Embed Size (px)
Citation preview

Klinik für Urologie, Uro-Onkologie, spezielle urologische und roboter-assistierte Chirurgie
Stellenwert der Lokaltherapie beim metastasierten hormonnaiven Prostatakarzinom
Axel Heidenreich

2 Klinik für Urologie, Uro-Onkologie, spezielle urologische und roboter-assistierte Chirurgie
Rationale der zytoreduktiven Therapie
• Elimation therapieresistenter, metastasierungs-
fähiger Tumorzellklone
• erster Schritt einer multimodalen Therapie
mit dem Ziel
Verbesserung des progressionsfreien und des
Gesamtüberlebens
Prävention der lokalen Progression und der
assoziierten Morbiditäten

3 Klinik für Urologie, Uro-Onkologie, spezielle urologische und roboter-assistierte Chirurgie
Lokale Primärtherapie des metastasierten
Prostatakarzinoms

4 Klinik für Urologie, Uro-Onkologie, spezielle urologische und roboter-assistierte Chirurgie
RPE als Monotherapy bei pN1
Zwergel U et al.,
J Urol 2004

5 Klinik für Urologie, Uro-Onkologie, spezielle urologische und roboter-assistierte Chirurgie
Engel J et al.,Eur Urol 2010
Overall Survival

6 Klinik für Urologie, Uro-Onkologie, spezielle urologische und roboter-assistierte Chirurgie
» N=377 pts with M0 PCa treated with RP alone (1987-2009)
» Mean age: 62 years; extracapsular extension: 95%; Gleason
Score≥7: 99%; seminal vesical invasion: 45%
Mazzola C. Eur Urol Suppl 2011;10(2):324(abs.1049)
RP alone can offer long-term freedom from biochemical recurrence to 30% of men with
lymph node positive PCa
Long-term outcome for PCa patients with positive LN after RP without adjuvant treatment
Survival outcomes

9 Klinik für Urologie, Uro-Onkologie, spezielle urologische und roboter-assistierte Chirurgie
„Radikale Prostatektomie ist bei LK-
Metastasen mit einem signifikanten
Überlebensbenefit verbunden„

10 Klinik für Urologie, Uro-Onkologie, spezielle urologische und roboter-assistierte Chirurgie
Lokale Primärtherapie des metastasierten
Prostatakarzinoms

11 Klinik für Urologie, Uro-Onkologie, spezielle urologische und roboter-assistierte Chirurgie
• Orthotopes Mausmodell: PC3-Zellen per injectionem in Prostata von SCID-Mäusen
• Gruppe 1: Injektion ohne weitere Therapie
• Gruppe 2: Injektion und ZRP an Tag 30 nach Ausbildung von Metastasen
Surgical cytoreduction of the primary tumor reduces metastatic progression in a mouse model of prostate cancer. Cifuentes FF et al., Oncol Rep 2015; 34: 2837 - 2844

12 Klinik für Urologie, Uro-Onkologie, spezielle urologische und roboter-assistierte Chirurgie
Tumor cytoreduction results in better response to androgen ablation—a preliminary report of palliative transurethral resection of the prostate in metastatic hormone sensitive prostate cancer. Qin XJ et al., Urol Oncol 2012; 30: 145 - 149

13 Klinik für Urologie, Uro-Onkologie, spezielle urologische und roboter-assistierte Chirurgie Seite 13
Might Men Diagnosed with Metastatic Prostate Cancer Benefit from
Definitive Treatment of the Primary Tumor? A SEER-Based Study.
Culp SH et al., Eur Urol 2014; 65: 1058 - 1066

14 Klinik für Urologie, Uro-Onkologie, spezielle urologische und roboter-assistierte Chirurgie
• n=32 zRPE versus n=38 Standard ADT
• identische biologisch, klinische und onkologische
Parameter zwischen den beiden Gruppen
• Vergleich der Zeit bis PSA-Rezidiv, klinischer
Progression, Entwicklung CRPC, Gesamt- und
tumorspezifisches Überleben
Cytoreductive radical prostatectomy in men with prostate
cancer and low volume skeletal metastases. Heidenreich A et al., J Urol 2015; 193: 832 - 838

15 Klinik für Urologie, Uro-Onkologie, spezielle urologische und roboter-assistierte Chirurgie
Cytoreductive radical prostatectomy in men with prostate
cancer and low volume skeletal metastases. Heidenreich A et al., J Urol 2015; 193: 832 - 838
“Einschlusskriterien” zRPE
• Lokal resezierbares Prostatakarzinom (=> mpMRI)
• ≤3 Metastasen in Skelettszintigraphie
• Pelvine Lymphknotenmetastasen ≤3 cm
• keine retroperitonealen Lymphknotenmetastasen
• Keine viszeralen Metastasen
Therapieplan
• Neoadjuvante ADT (LHRH analogues) für 6 Monate
• PSA < 0.4 ng/ml zRPE + epLAD
• ADT für 2 Jahre

16 Klinik für Urologie, Uro-Onkologie, spezielle urologische und roboter-assistierte ChirurgieHussain M et al., J Clin Oncol 2006; 24: 3984; SWOG Trial 9346
PSA nach 6 Monaten Surrogatmarker
des Überlebens

17 Klinik für Urologie, Uro-Onkologie, spezielle urologische und roboter-assistierte Chirurgie
Cytoreductive radical prostatectomy in men with prostate
cancer and low volume skeletal metastases. Heidenreich A et al., J Urol 2015; 193: 832 - 838
Daten RPE
OP-Zeit, Minuten (range) 127 (115–165)
Blutverlust, ml (range) 335 (250–600)
Transfusionsrate, % 0
Haemoglobin, g/dl (range)
Präoperativ
Postoperativ
13.1 (11.5–14.2)
11.8 (19.9–12.5)
Hospitalisation, Tage (range) 7.8 (6–13)
Patenz Anastomose, Tag 5 n/n (%) 30/32 (91.3%)
DK - Liegezeit, Tage (range) 5.6 (5–12)
18 Klinik für Urologie, Uro-Onkologie, spezielle urologische und roboter-assistierte Chirurgie
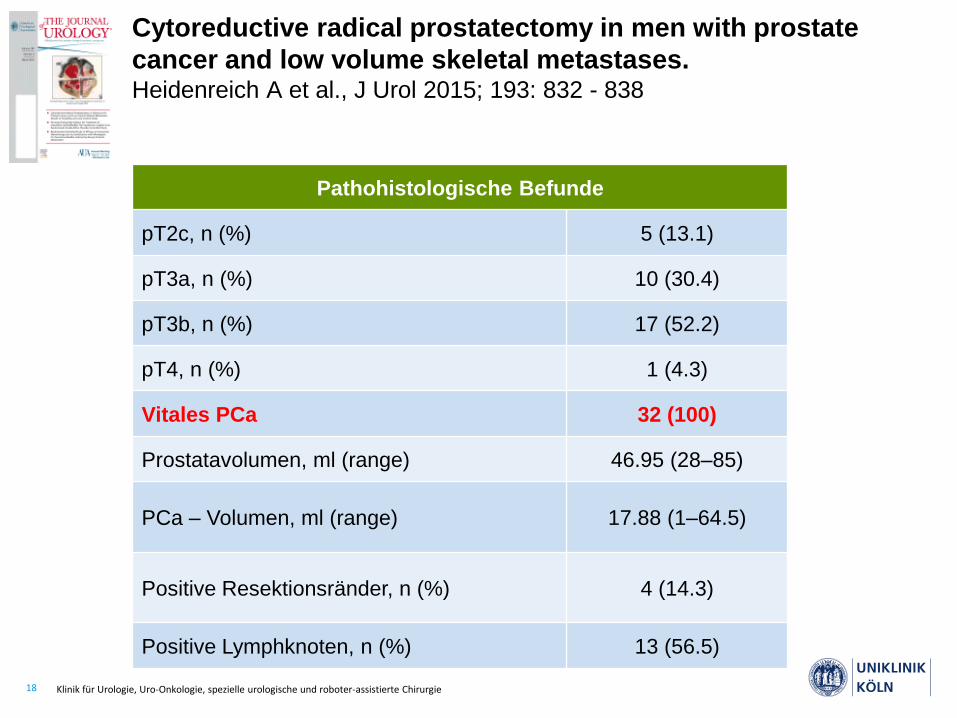
Cytoreductive radical prostatectomy in men with prostate
cancer and low volume skeletal metastases. Heidenreich A et al., J Urol 2015; 193: 832 - 838
Pathohistologische Befunde
pT2c, n (%) 5 (13.1)
pT3a, n (%) 10 (30.4)
pT3b, n (%) 17 (52.2)
pT4, n (%) 1 (4.3)
Vitales PCa 32 (100)
Prostatavolumen, ml (range) 46.95 (28–85)
PCa – Volumen, ml (range) 17.88 (1–64.5)
Positive Resektionsränder, n (%) 4 (14.3)
Positive Lymphknoten, n (%) 13 (56.5)

19 Klinik für Urologie, Uro-Onkologie, spezielle urologische und roboter-assistierte Chirurgie
Cytoreductive radical prostatectomy in men with prostate
cancer and low volume skeletal metastases. Heidenreich A et al., J Urol 2015; 193: 832 - 838

20 Klinik für Urologie, Uro-Onkologie, spezielle urologische und roboter-assistierte Chirurgie
Cytoreductive radical prostatectomy in men with prostate
cancer and low volume skeletal metastases. Heidenreich A et al., J Urol 2015; 193: 832 - 838
21 Klinik für Urologie, Uro-Onkologie, spezielle urologische und roboter-assistierte Chirurgie
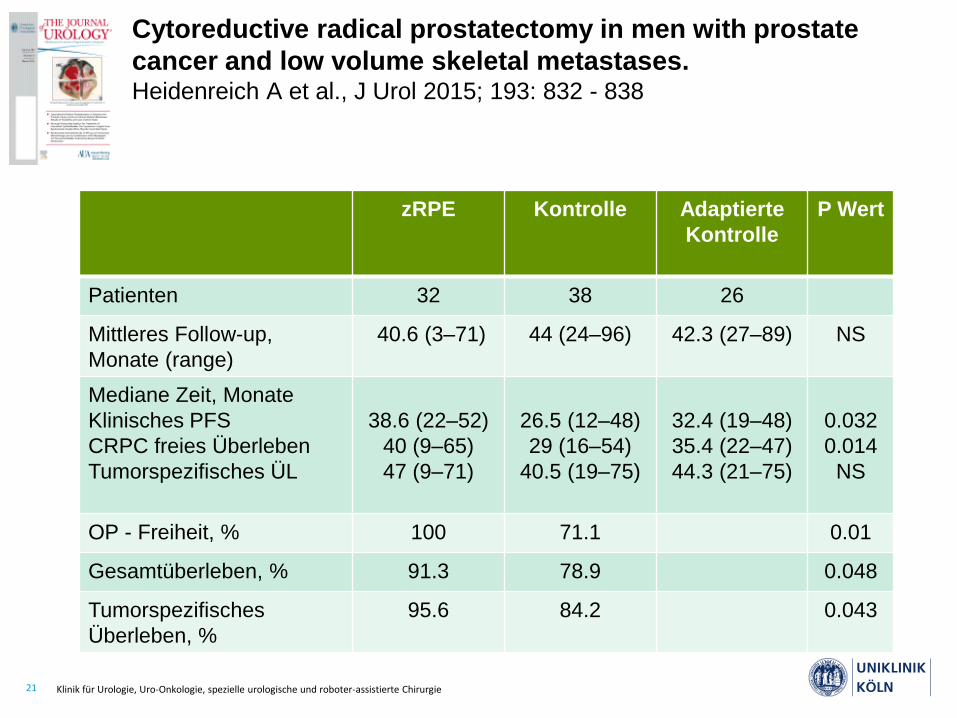
Cytoreductive radical prostatectomy in men with prostate
cancer and low volume skeletal metastases. Heidenreich A et al., J Urol 2015; 193: 832 - 838
zRPE Kontrolle Adaptierte
Kontrolle
P Wert
Patienten 32 38 26
Mittleres Follow-up,
Monate (range)
40.6 (3–71) 44 (24–96) 42.3 (27–89) NS
Mediane Zeit, Monate
Klinisches PFS
CRPC freies Überleben
Tumorspezifisches ÜL
38.6 (22–52)
40 (9–65)
47 (9–71)
26.5 (12–48)
29 (16–54)
40.5 (19–75)
32.4 (19–48)
35.4 (22–47)
44.3 (21–75)
0.032
0.014
NS
OP - Freiheit, % 100 71.1 0.01
Gesamtüberleben, % 91.3 78.9 0.048
Tumorspezifisches
Überleben, %
95.6 84.2 0.043

22 Klinik für Urologie, Uro-Onkologie, spezielle urologische und roboter-assistierte Chirurgie
Cytoreductive radical prostatectomy in men with prostate
cancer and low volume skeletal metastases. Heidenreich A et al., J Urol 2015; 193: 832 - 838
cRPE Control P Wert
Patients 32 38
complications, n (%)
Grad I & II 8 (26.1)* 11 (28.8%) NS
Grad IIIa 2 (8.7) 2 (5.4%) NS
Grad IIIb 1 (4.3) 9 (23.7%)** 0.04
Grad IVa - V 0 (0) 0 (0)
*n=2 anastomotic insufficiency, n=2 urinary tract infection
**only in patients with biopsy Gleason Score 8–10

23 Klinik für Urologie, Uro-Onkologie, spezielle urologische und roboter-assistierte Chirurgie
The role of cytoreductive radical prostatectomy (cRP) in 113 men with hormone-sensitive, metastatic prostate cancer(mPCA). Heidenreich A et al., GU ASCO 2017
Margin status Positive 57 (54.3)
Negative 48 (45.7)
postoperative T stage T0/Tx 2 (1.9)
T2 21 (19.8)
T3a 14 (13.2)
T3b 57 (53.8)
T4 12 (11.3)
postoperative N stage Nx 4 (3.8)
N0 26 (24.5)
N1 76 (71.7)

24 Klinik für Urologie, Uro-Onkologie, spezielle urologische und roboter-assistierte Chirurgie
Time from surgery (months)
96.0084.0072.0060.0048.0036.0024.0012.00.00
Ov
era
ll S
urv
iva
l
1.0
0.8
0.6
0.4
0.2
0.0
The role of cytoreductive radical prostatectomy (cRP) in 113 men with hormone-sensitive, metastatic prostate cancer(mPCA). Heidenreich A et al., GU ASCO 2017
Gesamtüberleben: nicht erreicht

25 Klinik für Urologie, Uro-Onkologie, spezielle urologische und roboter-assistierte Chirurgie
Time from surgery (months)
96.0084.0072.0060.0048.0036.0024.0012.00.00
Cli
nic
al
rec
urr
en
ce
-fre
e s
urv
iva
l1.0
0.8
0.6
0.4
0.2
0.0
Page 1
Mean clinical relapse-free survival: 72.3 months
The role of cytoreductive radical prostatectomy (cRP) in 113 men with hormone-sensitive, metastatic prostate cancer(mPCA). Heidenreich A et al., GU ASCO 2017
26 Klinik für Urologie, Uro-Onkologie, spezielle urologische und roboter-assistierte Chirurgie
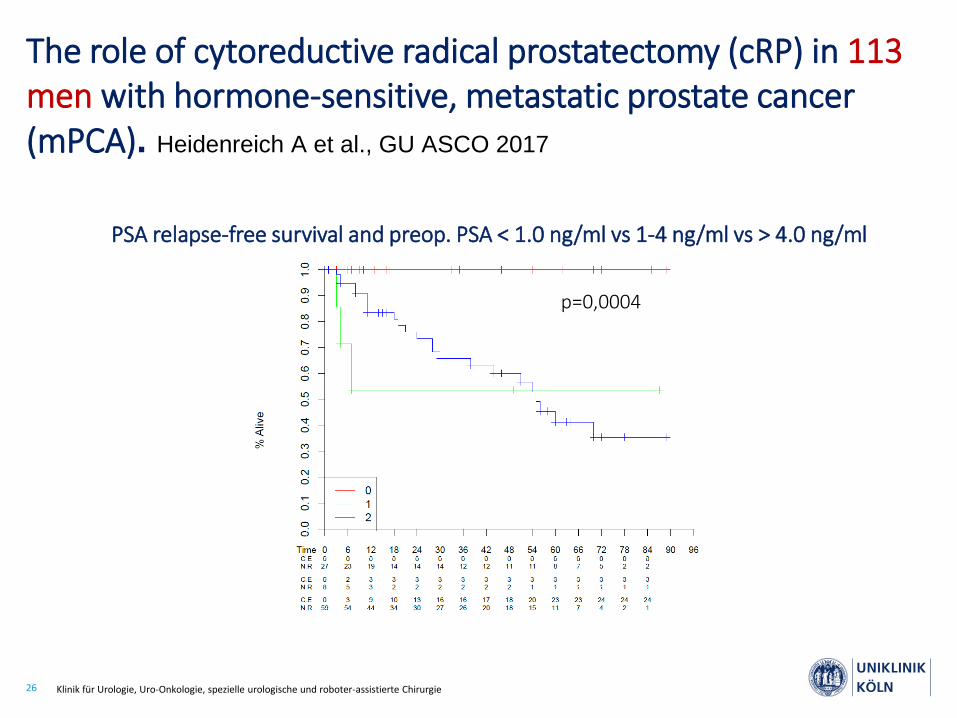
PSA relapse-free survival and preop. PSA < 1.0 ng/ml vs 1-4 ng/ml vs > 4.0 ng/ml
p=0,0004
The role of cytoreductive radical prostatectomy (cRP) in 113 men with hormone-sensitive, metastatic prostate cancer(mPCA). Heidenreich A et al., GU ASCO 2017

27 Klinik für Urologie, Uro-Onkologie, spezielle urologische und roboter-assistierte Chirurgie
n complications Non-significant Significant* p
Low volume diseaseHigh volume disease
8528
26 (30.6%)14 (50.0%)
20 (23.5%)5 (17.8%)
6 (7.1%)9 (32.1%)
< 0.05
PSA < 4 ng/mlPSA > 4 ng/ml
6647
17 (25.7%)23 (48.9%)
13 (19.7%)12 (25.5%)
4 (6.1%)11 (47.8%)
p < 0.05
neoadj. ADTno neoadj. Tx
8033
21 (26.3%)19 (57.6%)
14 (17.5%)11 (33.3%
7 (8.75%)8 (24.2%)
p < 0.05
*insignificant: Clavien Dindo I-IIIA*significant: Clavien-Dindo IIIB-V
The role of cytoreductive radical prostatectomy (cRP) in 113 men with hormone-sensitive, metastatic prostate cancer(mPCA). Heidenreich A et al., GU ASCO 2017

28 Klinik für Urologie, Uro-Onkologie, spezielle urologische und roboter-assistierte Chirurgie
Improved Survival With Prostate Radiation in Addition to
ADTfor Men With Newly Diagnosed Metastatic Prostate Cancer. Rusthoven CG et al., J Clin Oncol 2016; 34: 2835 - 2842
• National Cancer Database 2004 - 2012: mPCA treated with
ADT with w/o RT
• n = 6382 pts of whom 538 (8.4%) received RT
• n = 5844 (91.6%) with ADT alone
• n = 538 (8.4%) with ADT and RT
• median follow-up 5.1 years

29 Klinik für Urologie, Uro-Onkologie, spezielle urologische und roboter-assistierte Chirurgie
Improved Survival With Prostate Radiation in Addition to
ADTfor Men With Newly Diagnosed Metastatic Prostate Cancer. Rusthoven CG et al., J Clin Oncol 2016; 34: 2835 - 2842
30 Klinik für Urologie, Uro-Onkologie, spezielle urologische und roboter-assistierte Chirurgie
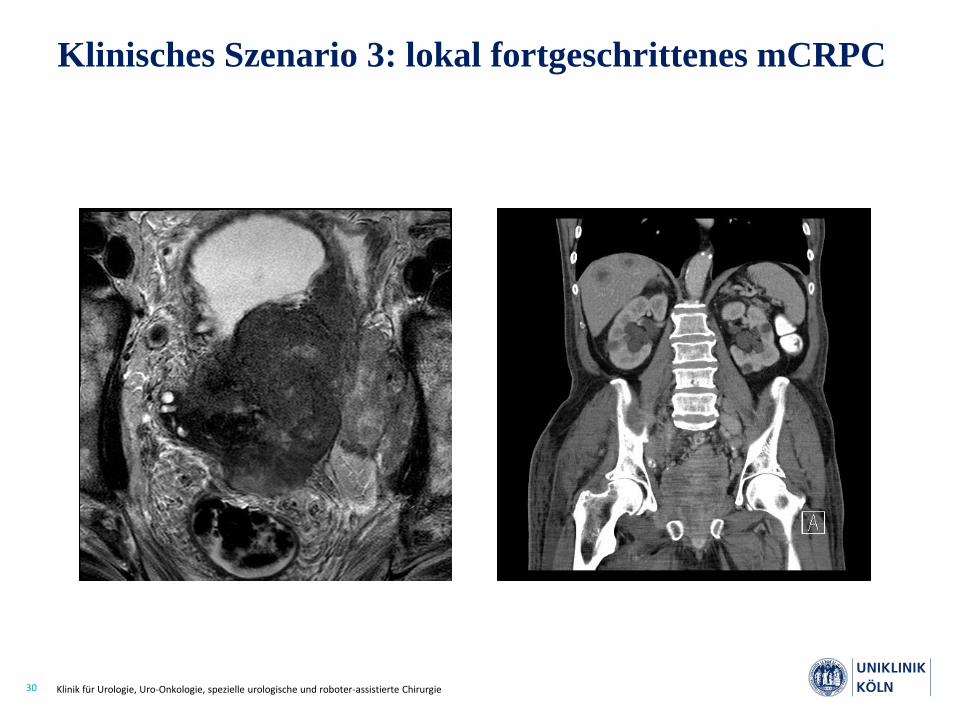
Klinisches Szenario 3: lokal fortgeschrittenes mCRPC

31 Klinik für Urologie, Uro-Onkologie, spezielle urologische und roboter-assistierte Chirurgie
Ventral Situs Dorsal Situs
Klinisches Szenario 3: lokal fortgeschrittenes mCRPC
32 Klinik für Urologie, Uro-Onkologie, spezielle urologische und roboter-assistierte Chirurgie
Seite 32
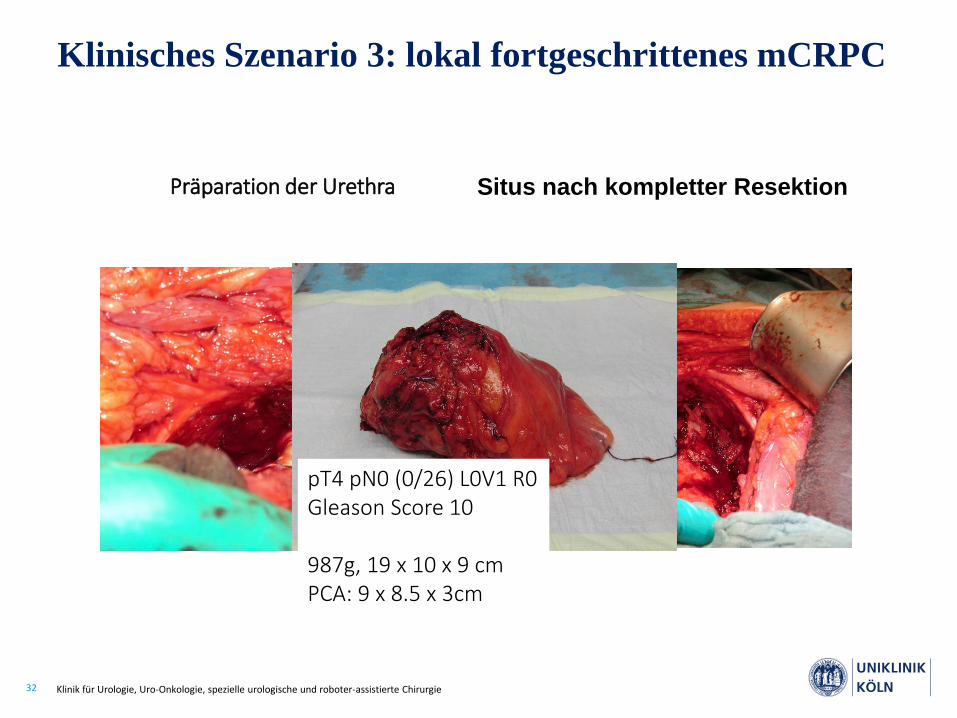
Präparation der Urethra Situs nach kompletter Resektion
pT4 pN0 (0/26) L0V1 R0Gleason Score 10
987g, 19 x 10 x 9 cmPCA: 9 x 8.5 x 3cm
Klinisches Szenario 3: lokal fortgeschrittenes mCRPC

33 Klinik für Urologie, Uro-Onkologie, spezielle urologische und roboter-assistierte Chirurgie
n = 72 Patienten
refraktäre pelvine Schmerzen
subvesikale Obstruktion
rezidivierende Makrohämaturie,
Transfusionen und Blasen-
tamponaden
radikale Tumorchirurgie aus
palliativer Intention?
radikale Prostatektomie (9)
radikale Zystoprostatektomie &
Harnableitung(57)
anteriore & posteriore Exenteration
(6)
mitlleres F-up: 24.8 (2-104) Mon
symptomfreies ÜL
1year 88.8%
3 years 65.6%
5 years 56.3%
tumorspezifisches ÜL 1 year 89.3%
3 years 42.4%
Porres D, Pfister D, Heidenreich A
DGU 2016
Klinisches Szenario 3: lokal fortgeschrittenes mCRPC

34 Klinik für Urologie, Uro-Onkologie, spezielle urologische und roboter-assistierte Chirurgie
Seite 34
signifikanter ÜL-Benefit der radikalen Prostatektomie bei Patienten mit
pelviner Lymphknotenmetastasierung im Vergleich zur alleinigen ADT
zytoreduktive RP könnte eine Therapieoption bei Patienten mit
günstiger Prognose nach neoadjuvanter ADT darstellen
100% vitales & potentiell letale intraprostatische PCA Klone
Risiko des Lokalrezidivs und lokaler Komplikationen
geringe therapieassoziierte Morbidität
radikale Tumorchirurgie aus palliativer Indikation hocheffektiv bei gut
ausgewählten Patienten
Zusammenfassung
35 Klinik für Urologie, Uro-Onkologie, spezielle urologische und roboter-assistierte Chirurgie
Offene Fragen der zytoreduktiven
Therapie
• Patientenauswahl
– Performance Status, konsumierende Erkrankung
– Comorbiditäten
• Metastasenlokalisation
– Knochen- versus Weichteilmetastasen
– Viszerale versus Hirnmetastasen
• neoadjuvante Therapie
– systemische Vortherapie und Chirurgie bei Response?




![Epidemiologische Studie an 202 metastasierten ... · Schleimhäute, Leptomeningen, Uvea oder Retina des Auges sowie Kochlea oder Labyrinth des Innenohrs [35]. Extrakutane Primärtumoren](https://img.dokumen.tips/doc/110x75/5d4b257788c99372718b6907/epidemiologische-studie-an-202-metastasierten-schleimhaeute-leptomeningen.jpg)
























