Embed Size (px)
Citation preview

STATISTICAL BACKGROUND FOR CBER PROPOSALS FOR ACCEPTABLE PROCESS CONTROL PLANS
John Scott, Ph.D.
Division of Biostatistics
FDA / CBER / OBE
October 19, 2012

Outline
Statistical Quality Control overview Sampling for quality control Single-stage sampling plans
Binomial plans Hypergeometric plans
Double-stage sampling plans Binomial plans Hypergeometric plans
Further possibilities
2

Statistical Quality Control Overview3

4
What is quality control?
Quality = “fitness for purpose” Many aspects to assessing quality, e.g.
Performance, reliability, durability, serviceability, aesthetics, features, perceived quality, conformance to standards
Much of the quality control literature centers on reduction of variability
We’re focused on assessing conformance Non-conformance is the end result of
uncontrolled variability

Methods of statistical quality control
Statistical process control methods Describe and explain variability in an
ongoing process Methods focus on graphical displays –
simple plots, Pareto charts, control charts
Experimental design methods Systematically assess sensitivity of
outputs to changes in input Acceptance sampling methods
Inspect and test final product for conformance
5

Some SPC graphs
Stem and leaf plot
Box plot Pareto chart The decimal point is 2 digit(s) to the left of the |
87 | 13
87 | 69
88 | 11233334
88 | 6788999
89 | 000011111223344444
89 | 556666677788888888889999
90 | 00001111112233344
90 | 5555666677778888
91 | 000000011122333333344
91 | 555556778
92 | 24444
92 | 6
Do
no
r
Op
era
tor
Filt
er
RBC Recovery Failures
Fre
qu
en
cy
05
10
15
20
0%
20
%4
0%
60
%8
0%
10
0%
Cu
mu
lativ
e P
erc
en
tag
e
6

Control charts
Control charts map samples of a product characteristic over time to identify when a process might be out of control
Features: A center line corresponding to the
average “in control” value Upper and lower control limits Out of control values or unusual runs
may be signals for investigation or action
7

Control chart example
RBC Recovery Control
Sample
% R
BC
Re
cove
ry
1 3 5 7 9 11 13 15 17 19 21 23 25
0.8
90
0.8
95
0.9
00
0.9
05
0.9
10
0.9
15
0.9
20
LCL
UCL
CL
8

Sampling for QC9
PopulationPopulation
Sample

Conformance to standards
The plateletpheresis and leukoreduction Guidances each recommend: Standards for QC testing of individual units A maximum acceptable proportion of non-
conforming units A minimum confidence level
Only process failures are counted as non-conforming Non-process failures (failures due to
uncontrollable parameters) are replaced in QC testing
10

Leukoreduction standards11
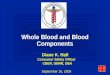
Plateletpheresis standards12

Maximum process failure rates 5% for:
Residual WBC content Content recovery / retention pH
25% for: Platelet yield
13

Minimum confidence levels
In each case, the Guidances recommend establishing a process failure rate below the maximum “with 95% confidence”
That means: if the true process failure rate for a given month is at the maximum allowable level, there’s: A 95% chance that QC testing will detect a problem,
or A 5% chance that the problem will go erroneously
undetected 95% confidence in a 95% success rate is
called “95%/95% acceptance” 95% confidence in a 75% success rate is
“95%/75% acceptance”
14
How to get to 95% confidence There’s an “easy” way to have 100%
confidence: test every unit. E.g.: Suppose you produce 200 units of RBC, LR
in a given month You test residual WBC content on every unit All but 8 units meet WBC < 5.0 x 106 The failure rate is 8/200 = 4% with 100%
confidence When testing every unit is impractical
(i.e. usually), you can use statistical sampling to get to 95% confidence
15

The logic of statistical sampling The population is what you
want to draw a conclusion about E.g. this month’s RBC units
Take a random sample, measure failure rate in the sample, use probability models to make inference about population rate Yields an estimate of population
rate Estimate has some uncertainty
because sample is incomplete
Population
Sam-ple
16

Acceptance sampling
Acceptance sampling consists of taking a sample from a lot and making a decision to accept or reject the lot based on the sample
Not the same as SPC for blood establishments A month’s worth of units is not a “lot” A month’s worth of units will not be
discarded on failed QC Common methods of acceptance
sampling do correspond to FDA recommendations
17

Acceptance sampling translations In order to use acceptance
sampling terminology, we need a couple translations
“Accept” = Pass QC testing for the month No further action required
“Reject” = Fail QC testing for the month Launch a failure investigation
18

Single-stage sampling plans
19
0.00 0.02 0.04 0.06 0.08 0.10
0.0
0.2
0.4
0.6
0.8
1.0

Single-stage sampling plans
In a given month, N units will be produced In a single-stage sampling plan:
A sample of n units is tested If more than c process failures, reject;
otherwise accept E.g. n = 60, c = 0 means:
We test a sample of 60 units If no process failures, accept If at least 1 process failure, reject, launch a
failure investigation n and c need to be chosen to provide
recommended confidence
20

Binomial single-stage sampling The Guidances recommend that n and c
be chosen such that the probability of accepting is at most 5% when the true failure rate is at the maximum allowed
We need a probability model to calculate the probability of accepting
For large N we usually use the binomial distribution Called “Type B sampling” in SPC literature
The binomial distribution assumes a random sample is taken with replacement from an infinite population
21

*The binomial distribution
Assume: The true failure rate is p The sample size is n The acceptance number is c
Then, under binomial sampling, the probability of accepting is given by:
For example, p = .05, n = 60, c = 0 gives
a probability of accepting of
22
0
!(1 )
!( )!
ck n k
k
np p
k n k
160
0
60!.05 (.95 .0)
!( )46
60 !k k
k k k

Operating characteristic curves For any sampling plan, we can ask:
what’s the probability of accepting at any given true failure rate? Recall that the Guidances recommend,
e.g., 5% probability of accepting at a true residual WBC failure rate of 5%
We also care about the probability of accepting at a “good” failure rate
An operating characteristic (OC) curve plots the probability of accepting against the true failure rate
23

OC curve examples24
0.00 0.02 0.04 0.06 0.08 0.10
0.0
0.2
0.4
0.6
0.8
1.0
OC Curves for type B sampling plans, n=93
Proportion of process failures
Pro
ba
bili
ty o
f acc
ep
tan
ce c=0, n=93c=1, n=93c=2, n=93
Practical binomial single-sampling Very few binomial single-stage sampling
plans are useful in practice Once you choose c, the smallest
allowable n is the best choice For 95%/95%:
1. c = 0, n = 59*2. c = 1, n = 933. c = 2, n = 124
*note that the Guidances mention c = 0, n = 60; establishments often prefer the round number, but c = 0, n = 59 is also acceptable
25
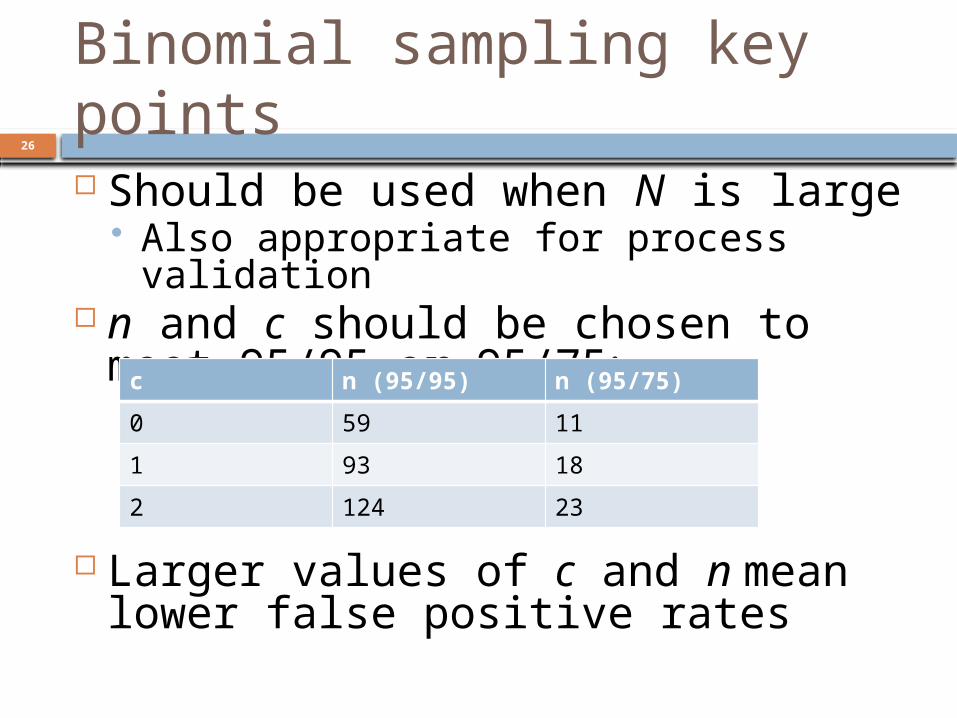
Binomial sampling key points Should be used when N is large
Also appropriate for process validation n and c should be chosen to meet
95/95 or 95/75:
Larger values of c and n mean lower false positive rates
26
c n (95/95) n (95/75)
0 59 11
1 93 18
2 124 23

Hypergeometric single-stage sampling The binomial distribution assumes
an infinite population You don’t produce an infinite number of
units, but this works well enough for large N
If the population is small, we can use the hypergeometric distribution instead Called “Type A sampling” in SPC
literature The hypergeometric distribution
assumes a random sample is taken without replacement from a finite population of size N
27

*The hypergeometric distribution Assume:
The population size is N The population number of successes is m
(m ≥ (1-p)N) The sample size is n The acceptance number is c
Under hypergeometric sampling, the probability of accepting is given by:
28
0
! ( )!!( )! ( )!( )!
!!( )!
c
k
m N mk m k n k N m n k
Nn N n

Hypergeometric OC curve examples
29
0.00 0.02 0.04 0.06 0.08 0.10
0.0
0.2
0.4
0.6
0.8
1.0
OC Curves for type A sampling plans (N=100)
Proportion of process failures
Pro
ba
bili
ty o
f acc
ep
tan
ce c=0, n=45c=1, n=65c=2, n=81

Binomial vs. hypergeometric plans Hypergeometric plans have
logistical difficulties: You need to know N (or put upper
bound on N) QC process may change from month to
month or component to component Binomial plans require larger
samples As N gets large, difference between
binomial and hypergeometric approaches narrows Almost no difference when N is at least
10 times bigger than n
30

Hypergeometric key points
Useful when N is small Sampling plan depends on knowing
N You may need to plan around an upper
bound on N Can’t be used for process validation For each N, you can choose n and c
to meet 95/95 or 95/75. E.g. for N = 100:
31
C n (95/95) n (95/75)
0 45 10
1 65 16
2 81 22
Single-stage sampling issues The sampling plan needs to be
prespecified Not acceptable to plan on c=1, n=93, then get
to 59 with no process failures and accept without further testing
You need to sample in such a way that you’ll have enough tests to meet QC acceptance rule With a c=1, n=93 sampling plan, if you have 1
process failure in 80 tests in a month, 95%/95% hasn’t been met
For small N, hypergeometric plans may involve testing almost 100% of units You may need to test consecutively from start
of month Potentially problematic if something changes
mid-month
32

Double-stage sampling plans
33
0.00 0.02 0.04 0.06 0.08 0.10
0.0
0.2
0.4
0.6
0.8
1.0

Double-stage sampling plans In a double-stage sampling plan:
A sample of n1 units is tested If c or fewer process failures are observed,
accept If c+2 or more process failures are
observed, reject If c+1 process failures are observed:
A second sample of n2 units is tested If no more process failures are observed,
accept If one or more process failures are observed,
reject c, n1 & n2 are chosen to meet
recommended criteria (e.g. 95%/95%, 95%/75%)
34

Binomial double-stage plans
For large N, we calculate probability of acceptance using the binomial distribution
Some acceptable double-stage sampling plans:
35
C 95/95 95/75
N1 n2 n1 n2
0 60 71 11 11
1 94 75 18 8
2 125 69 23 17

Double vs. single-stage sampling
36
0.00 0.02 0.04 0.06 0.08 0.10
0.0
0.2
0.4
0.6
0.8
1.0
OC Curves for single- vs. double-sampling
Proportion of process failures
Pro
ba
bili
ty o
f acc
ep
tan
ce c=0, n=59c=0, n1=60, n2=71c=1, n=93c=1, n1=94, n2=75c=2, n=124c=2, n1=125, n2=69

Flexibility in double-stage plans There are more choices with
double-stage plans All of these meet 95%/95%:
c n1 n2 Pr(accept) if p = 1%
Avg. total n if p = 1%
Max n
0 59 90 69% 89 149
0 60 71 71% 84 131
0 61 61 72% 82 122
0 62 55 73% 81 117
37

Hypergeometric double-sampling As with single-stage sampling,
binomial double-stage sampling is pretty efficient if N is large
For small N, hypergeometric double-stage sampling may allow smaller samples
You need to know N (or be able to put an upper bound on it)
The calculations are a little complicated; Appendix A of the leukoreduction guidance provides a table
38

Hypergeometric double-stage sampling examples
39

Double-stage sampling issues As with single-stage sampling:
Pre-specification required Need to ensure enough units are tested
Note that many hypergeometric plans have a second stage of 100% (“ALL”) or almost 100% You can’t get to 100% if you skipped any For N=50, c=0, n1=31, n2=18, you may be
done with testing two weeks into the month Will you catch issues late in the month? Supplemental testing may be advisable
40

Double-stage sampling key points Adopting a double-stage sampling
plan: Gives you a chance to “rescue” a
process in the event of a failed test Reduces risk of false positives
Binomial plans are appropriate for large N
Hypergeometric plans yield smaller sample sizes for small N Can’t be used for process validation
Plans should be pre-specified
41

Other Possibilities42
Multiple-stage sampling
Double-stage sampling can be generalized: The second stage can be designed
to allow for 1 or more process failures
Third, fourth, or … stages can be added
None of these techniques are likely to lead to practical sample sizes in the blood establishment setting
43

Chain sampling
In chain sampling, a sample of size n would be taken each month
If 0 process failures, accept If 2 process failures, reject If 1 process failure:
Accept if there have been 0 process failures in the past i months
Otherwise reject Hasn’t been proposed, to my
knowledge
44

Scan statistics
Scan statistics can be used to continuously monitor an ongoing process to look for event clusters
How it works: N tests over a year Look at every possible sequence of m
consecutive tests (a “window”) If there are more than k failures in a
window, the process is out of control N, m and k chosen to achieve probability of
declaring: In control at a “good” failure rate, p1 (e.g. 1%) Out of control at a “bad” failure rate, p2 (e.g.
5%)
45

Scan statistic pros and cons
A natural way to look at blood product QC Months are arbitrary (although c.f. CFR)
Avoids issues related to non-random sampling
Mathematically & logistically complex No free lunch!
Added flexibility of the scan statistic comes at a price
If you want 95%/95% for any scan window, large N (e.g. N > 1000) required, or false positives high
Compare to 60/month binomial N = 720
46

Thanks!47