-
7/28/2019 State of the Art and Science of Endodontics
1/13
2005;136;41-52J Am Dent Assoc
SCIENTIFIC AFFAIRS COMMITTEEENDODONTICS RESEARCH ANDAMERICAN
ASSOCIATION OFOF AND CONSULTANTS TO THESHAHROKH SHABAHANG and
MEMBERSState of the art and science of endodontics
jada.ada.org ( this information is current as of July 28, 2008
):
The following resources related to this article are available
online at
http://jada.ada.org/cgi/content/full/136/1/41
found in the online version of this article at:including
high-resolution figures, can beUpdated information and services
http://jada.ada.org/cgi/collection/endodonticsEndodontics
:subject collectionsThis article appears in the following
http://www.ada.org/prof/resources/pubs/jada/permissions.asp
reproduce this article in whole or in part can be found at:of
this article or about permission toreprintsInformation about
obtaining
2008 American Dental Association. The sponsor and its products
are not endorsed by the ADA.
onJuly28,2008
jada.ada.org
Downloadedfrom
http://jada.ada.org/cgi/content/full/136/1/41http://www.ada.org/prof/resources/pubs/jada/permissions.asphttp://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://www.ada.org/prof/resources/pubs/jada/permissions.asphttp://jada.ada.org/cgi/content/full/136/1/41
-
7/28/2019 State of the Art and Science of Endodontics
2/13
State of the art andscience of endodontics
SHAHROKH SHABAHANG, D.D.S., M.S., Ph.D.;AND MEMBERS OF AND
CONSULTANTS TO THEAMERICAN ASSOCIATION OF ENDODONTICSRESEARCH AND
SCIENTIFIC AFFAIRS COMMITTEE
The past 10 years have witnessed significantchanges in the art
and science of endodontics.The advances in the science of this
specialtyhave allowed for better understanding ofendodontic disease
processes and have led to
development of treatment modalities aimed at restoringhealth to
the pulp and periradicular tissues. Technolog-ical discoveries in
instruments and materials have madeit possible to achieve treatment
objectives that once
were considered unattainable. Thisarticle reviews the advances
in endodon-tics during the past decade, focusing on
both basic and clinical research.
BASIC RESEARCH
The microbial nature of endodonticdisease. While the mechanical
andmanual challenges of root canal dbride-ment and obturation
remain, it hasbecome increasingly clear that thelargest proportion
of endodontic disease,both pulpal and periradicular, is due tothe
presence of microorganisms. There-fore, treatment success is
related very
closely to the ability to remove theseirritants and to prevent
reinfection.The polymicrobial nature of endo-
dontic infections contributes to the increased overallbacterial
irritation that is associated with the develop-ment of certain
virulent bacterial combinations.1-3 Thepresence of certain
microorganisms, such as members ofthe black-pigmented gram-negative
bacteria, in rootcanals of teeth with necrotic pulp has been
associatedwith increased clinical symptoms.4-6
Development of DNA- and RNA-based microbiologicaltechniques has
allowed researchers in endodontics to
ABSTRACT
JADA, Vol. 136, January 2005 41
A better
understandingof the
pathogenesis
of pulp and
periradicular
diseases will
improve
patient care
and result in
preservation of
natural tissues.
JA D A
C
O
NT
INU
ING E DU
CAT
IO
N
R E S E A R C H
Background.Advances in the art and
science of endodontics have
facilitated better under-
standing of disease pro-
cesses and have led todevelopment of treat-
ment modalities aimed to
restore health to the pulp
and periradicular tissues.
This article presents a summary
of both basic and clinical breakthroughs
in endodontics.
Results. The author indicates that, on
the basis of the reviewed literature, pulp
and periradicular diseases are primarily
microbial. Basic research has led to devel-
opment of methodologies that have allowedfor specific and
accurate identification of
pathogens that are likely to cause persis-
tent infections. Close examination of clin-
ical data shows that meticulous dbride-
ment of the infected root canal system will
result in a high probability of successful
treatment outcome. Progress in visualiza-
tion, mechanical and chemical disinfection,
and biological seal of portals of entry will
improve quality of care further.
Conclusions and Clinical
Implications.A better understanding of
the pathogenesis of pulp and periradicular
diseases, inflammation and healing, as well
as of pain pathways, will improve patient
care and result in preservation of natural
tissues.
Key Words. Endodontics; endodontic
technology; basic endodontic research.
ARTICLE
1
JA D A
C
O
NT
INU
ING E DU
CAT
IO
N
identify new species of bacteria7,8 andto develop a more
elaborate descrip-
tion of the microbial diversity in rootcanal infections.9,10
Owing toincreased sensitivity and the abilityto detect uncultivable
microorgan-isms, researchers identified severalfastidious or
uncultivable microor-ganisms in root canal infections,using
techniques based on the poly-merase chain reaction to amplify
thebacterial 16S rRNA gene.8
Researchers cultured gram-positive bacteria,
particularlyEntero-
COVER STORY
Copyright 2005 American Dental Association. All rights
reserved.
onJuly28,2008
jada.ada.org
Downloadedfrom
http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/
-
7/28/2019 State of the Art and Science of Endodontics
3/13
coccus faecalis, from the root canals of teeth withpersistent
periradicular lesions.11-13 Furthermore,other researchers cultured
fungimostlybelonging to the genus Candidafrom nearly7 percent of
retreatment cases that have cul-
tivable microorganisms.14 It is not yet clearwhether these
microorganisms cause the treat-ment failure or are favored by the
environment ofpreviously treated root canals.
The endodontic literature has devoted muchattention to the
question of whether microorgan-isms are present within
periradicular lesions.Techniques using in situ staining methods
haverevealed the presence of bacteria, mainlybelonging to the
genusActinomyces, in sometherapy-resistant cases.15 Usingcareful
sampling techniques,
researchers have detected bacteria16or bacterial DNA17,18 in
periradicularlesions. More recently, researchershave linked
symptomatic periradic-ular lesions to an increased preva-lence of
human cytomegalovirus andEpstein-Barr virus.19
Inflammation of the pulp.Inflammation of the dental pulp is
abasic biological response that takesplace in a unique
low-compliance environmentand is the result, at least initially, of
bacterial
toxins acting well in advance of any direct micro-bial invasion.
The initial innate component of theresponse is largely vascular and
due to therelease, initiated by cytokines and mediators,
ofneuropeptides20,21 from the multitude of pulpalnerves via axon
reflexes.22A three-dimensionalstudy has revealed widespread
anastomoses andloops23 that help limit the potentially
damagingsequelae of inflammation. In this regard, exami-nation of a
microvascular study24 showed clearlythat mechanisms in the
capillary bed limit thedangers of increasing tissue fluid pressure
such
that capillary collapse occurs only at a late stagein untreated
inflammation. Researchers also havemapped out the immunological
component of thetissue response in detail,25 starting with
antigen-presenting cells that greet the penetrating irri-tants as
they reach the odontoblastic layer andculminating in nonspecific
and specific responsesby phagocytes and lymphocytes,
respectively.
Inflammation and infection of the periradiculartissues are an
extension of the processes in thepulp but are not identical to
them. What practi-tioners detect most often clinically is bone
resorp-
tion. Hard-tissue dissolution is not a character-istic of pulpal
inflammation. The periradicularlesion has proven to be a productive
model for thestudy of inflammatory resorption.26,27 Cliniciansnow
have detailed descriptions of the inflamma-
tory cascade of cytokines released by bacterialtoxins from
macrophages and neutrophils, andthe recognition of a group of these
cytokines(interleukin-1 alpha, interleukin-2 beta, trans-forming
growth factor-1 alpha, transforminggrowth factor-2 beta) as the
osteoclast-activatingfactor is an important advance.
For most patients, pain is the most obvious andimportant
characteristic of inflammatory disease,and especially so when it is
within the tooth.
During inflammation, intrapulpalnerves sprout and gather
increased
amounts of neuropeptides20 andrelease transmitters in response
tostimulation by cytokines.21A- fiberterminals, in dentin
responding tohydrodynamic stimuli, and C fibers,in pulp responding
to inflammatorymediators, appear to have differen-tial roles in
pulpitis.28A relation-ship between symptoms and inflam-matory
molecules has been
demonstrated in all studies reporting the signifi-cance of
substance P.29-31 Inflammation and regen-
eration are closely related. The repair potential ofthe dental
pulp is well-known, and recent workusing growth factors suggests
that modulation ofthese proteins will be of great value in
extendingthe range of pulpal repair procedures.32,33
CLINICAL RESEARCH
Treatment outcomes. The most recent dataindicate that about 15.8
million primary endo-dontic procedures were performed in the
UnitedStates in 1999.34 Maintenance of the natural den-tition,
aided by endodontic, periodontal and
restorative procedures, is the preferred choice ofpatients and
remains a predictable treatmentplan. From the patients perspective,
retention ofa tooth in a functional and esthetic condition maybe
considered a favorable treatment outcome. Onthe other hand,
endodontists use more rigorousstandards to assess treatment
outcomes. Suc-cessful treatment to the specialist generally
issignified by clinical and radiographic absence ofdisease.
Researchers have reported outcome datain the endodontic literature
as complete healing,incomplete healing or an absence of healing.
Com-
42 JADA, Vol. 136, January 2005
R E S E A R C H
Inflammation andinfection of the
periradicular tissues
are an extension of
the processes in
the pulp but are not
identical to them.
Copyright 2005 American Dental Association. All rights
reserved.
onJuly28,2008
jada.ada.org
Downloadedfrom
http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/
-
7/28/2019 State of the Art and Science of Endodontics
4/13
plete restoration to health may be expected in 80percent35,36 to
more than 95 percent37 of cases,depending on the observation
period. It is impor-tant to note that while signs of initiated,
butincomplete, healing may be visible in early follow-
up periods, complete resolution of preoperativeradiolucent
lesions may require up to four yearsof healing time.38 Overall, the
criteria used forreporting endodontic treatment outcomes are
dif-ferent from and more rigorous than those used toreport the
survival rates of implants.
Evidence-based endodontics. Clinical deci-sion making is
becoming more complex today andrequires information from many
sources: primarydata and patient preferences, the clinicians
ownclinical and personal experiences, external rulesand
constraints, and scientific evidence. There
also has been an explosive increase in the amountand quality of
laboratory and clinical evidence.Fortunately, mechanisms such as
systematicreviews are emerging that will help us acquirethe best,
most compelling and most current evi-dence that addresses defined
clinical questions.
In 1999, the American Association of Endodon-tists (AAE) Board
of Directors elected to use anevidence-based approach to its
decision makingand embrace lifelong learning as an essential
ele-ment in the practice of the highest standards ofendodontics.
Trained AAE members, active in
education and research, conducted systematicreviews in selected
topics that were reported atthe 2002 AAE Annual Session in Chicago.
Theorganization established an Evidence-basedEndodontics Standing
Committee to consideraction on the following
recommendations:dconstruction of a critically approved databaseof
identified articles;ddevelopment of an electronic journal from
thedatabase;dcontribution to other databases such as theCochrane
Collaboration;d
continued training of reviewers to conduct sys-tematic reviews
on additional clinical questions;dcreation of a standardized
report-writingformat;drevision of the standards of the
AmericanDental Association Commission on Dental
Accreditation to include instruction in conductingsystematic
reviews.
CLINICAL PRACTICE
Diagnosis.Accurate and efficient diagnosis isthe cornerstone of
endodontic therapy. Experi-
enced clinicians long have recognized that thepatients chief
complaint and history of illness arethe first, and arguably the
most, important piecesof the diagnostic puzzle. Some investigators
viewhistory of moderate-to-severe pain as a good indi-
cator of irreversible pulpal pathosis.39 Nonethe-less, clinical
signs and symptoms alone are unreli-able predictors of pulp and
periradiculardiseases.40,41 Thermal (cold and heat) and elec-trical
pulp testing (EPT) are simple tests but arenot completely reliable.
Heat as a pulp test has arelatively high sensitivity but is the
least accu-rate overall of the three common pulp tests owingto low
specificity.42 Cold testing withtetraflouroethane, ethyl chloride
or carbon dioxide(CO2) snow is relatively reliable and
generallymore accurate than heat. Cold testing is pre-
sumed to be more reliable than EPT in teeth withincomplete root
formation. Since thermal testsare not 100 percent accurate, EPT is
especiallyuseful for confirming a questionable pulpaldiagnosis.
A major limitation of thermal testing and EPTis that these tests
measure only pulpal nerveresponse, not pulpal blood flow. Since the
truemeasure of pulp vitality is blood flow, laserDoppler flowmetry
(LDF) and pulse oximetrydevices have been adapted for experimental
usein assessing pulp vitality.43-46 These devices seem
particularly well-suited for evaluating the vitalityof
traumatized teeth and for evaluating teeth inareas that may require
orthognathic surgery.47
Some investigators have attempted to identifybiological factors
that may determine the healthstatus of the pulp tissue more
accurately.48,49 Iden-tification of the 20,000 to 25,000 genes of
thehuman genome has paved the way for associationof specific genes
with known pathological find-ings. Microarray technology has
enabledresearchers to identify and study a large array ofgenes and
proteins that are affected during dis-
ease formation and healing.
50,51
Canal instrumentation. The goals of dbride-ment are to remove
irritants from the root canalsystem and to create a
three-dimensional shapethat can be obturated.52 Nickel titanium
(NiTi)files have become a mainstay in most endodonticprocedures.
Thanks to this metal, practitionerscan use rotary instruments
effectively in curvedcanals. Many file designs and shapes can be
usedfor dbridement. Varying the taper of the instru-ment leads to a
more efficient preparation of theroot canal space. Many of these
types of files fea-
JADA, Vol. 136, January 2005 43
R E S E A R C H
Copyright 2005 American Dental Association. All rights
reserved.
onJuly28,2008
jada.ada.org
Downloadedfrom
http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/
-
7/28/2019 State of the Art and Science of Endodontics
5/13
ture a U-shaped groove and a radial land thathelps prevent
perforations and instrumentlocking and separation. They also
usually have anoncutting tip that helps to decrease transporta-tion
of the canal space.
While it can reduce the bacterial count signifi-cantly,
mechanical dbridement does not disinfectthe root canal system
completely.53 Thus, a rootcanal irrigant is needed to aid in the
dbridementof the canals. Sodium hypochlorite (NaOCl) is themost
commonly used root canal irrigant. How-ever, NaOCl has some major
short-comings, including its inability toremove the smear
layer54,55 and tokill all bacteria present in infectedroot
canals.12,56,57 Recently, a mix-ture of a tetracycline isomer,
an
acid and a detergent known asMTAD has been introduced as afinal
rinse for disinfection of theroot canal system. This irrigant
isable to remove the smear layersafely,55 and it is a more
effectivedisinfectant than NaOCl evenagainst resistant bacteria
such asE. faecalis.58,59
Obturation: new delivery systems andimportance of coronal
restoration.Researchers have attributed failure of root canal
therapy largely to incomplete obturation of theroot canal
system.60After proper cleaning,shaping and disinfection of the root
canal system,proper filling of the canal is necessary to
preventreinfection. There are two basic methods of rootcanal
obturation, with a number of permutationsto these techniques. The
lateral condensationtechnique requires lateral compaction of
coldgutta-percha points to fill the space. Warm gutta-percha
techniques, also called vertical com-paction techniques, use warm
gutta-percha thatis made plastic and compacted apically. Both
techniques require addition of a cementlike sealerthat adheres
to the dentin walls and fills anyspace not obliterated by the
gutta-percha. Prop-erly prepared canalscleaned, disinfected
andtapered in shapealso should be cleared of thesmear layer. This
can be achieved by using a com-bination of ethylene diamine
tetra-acetic acid andNaOCl or MTAD.
Variations of the techniques described previ-ously use newer
devices, which are equippedwith a heated spreader/plugger that
warms thegutta-percha and acts as a plugger to compact
the plasticized mass. Use of solid-core carrierssuch as
Thermafil (Dentsply Tulsa Dental,Tulsa, Okla.) is another accepted
method ofobturating root canals. By this method, a centralcarrier
coated with alpha-phase gutta-percha is
warmed and plasticized in a special oven andinserted to the
appropriate depth in theprepared canal.
An apical third obturator acts as a terminalplug at the apical
portal of exit. The plug can bemade up of dentin chips formed from
the cleaned,
shaped and disinfected canal walls.Not only does the plug
preventoverfilling, but also dentin chipscan stimulate the
formation of acementumlike cap over the apex.61
Calcium hydroxide62 and mineral
trioxide aggregate (MTA)63 also canbe packed as an apical plug.
Theremainder of the canal space can befilled using sealer and a
gutta-percha gun such as Obtura II(Obtura Spartan, Fenton,
Mo.).
The lack of a coronal seal is animportant factor in the
develop-ment of periradicular lesions fol-lowing root canal
therapy.64 There-
fore, it is important to prevent coronal leakageafter completion
of root canal therapy.
A number of studies have investigated the lossof the provisional
restoration to determine howlong it takes for coronal leakage to
adverselyaffect the root canal seal.65-68 In one study,
leakageoccurred in as little as three days time.65 By day19 in
another study, more than 50 percent of theroot canals were
completely contaminated,66 andby day 30 in a third study, all
canals without acoronal seal were contaminated.68 While the
pres-ence of a temporary restoration may retard thisprocess, this
protection is short-lasting and a sub-stantial change occurs
between 28 and 90 days
after placement of a temporary restoration.
67
The loss of a provisional coronal access restora-tion most
likely results in a compromised rootcanal seal sometime during the
first month ofexposure to oral contaminants. Should there bean
extended period between the completion ofendodontic therapy and
definitive restorative orprosthodontic care, then a definitive
restorationshould be placed in the most coronal portion ofthe
access opening.
Adjuncts. Operating microscopes. Perhaps noarea of endodontic
practice has met with more
44 JADA, Vol. 136, January 2005
R E S E A R C H
The loss of a
provisional coronal
access restoration
most likely results ina compromised root
canal seal sometime
during the first month
of exposure to oral
contaminants.
Copyright 2005 American Dental Association. All rights
reserved.
onJuly28,2008
jada.ada.org
Downloadedfrom
http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/
-
7/28/2019 State of the Art and Science of Endodontics
6/13
excitement and controversy in the past decadethan the
introduction of the operating microscope(OM) to clinical practice.
In less than 10 years,the OM has progressed from a novelty item to
arequired training standard for specialty education
in endodontics.The OM is used most commonly to assist in
retrieving separated instruments, locating andnegotiating
calcified canals, and providing sur-gical root canal treatment.69
Proponents of OMsfeel strongly that they allow for more efficient
andsafe treatment of teeth that otherwise might beuntreatable or
treatable only with great difficulty.There is some evidence that
the use of OMs incombination with operator skill, prudent
caseselection, and other current technology andmaterials may lead
to improved surgical treat-
ment outcomes70 and the location of additionalcanals.71,72
Endoscopes, orascopes and magnifyingloupes with or without a
supplemental lightsource also can be employed to enhance
visualiza-tion of the operative field.73,74
Ultrasonic devices. Ultrasonic devices havebecome essential
tools for assisting in the removalof posts and separated
instruments, as well asroot-end preparation during surgical
treatment ofroot canals.75 Since heat is a byproduct of theenergy
generated by ultrasonic instruments, it isimportant to use a water
coolant spray and to
operate at the lowest setting possible consistentwith the task
(root-end preparation, for example,is a delicate procedure and
requires a lower set-ting than do post removal applications).
Manyspecially designed ultrasonic tips are availableand suitable
for specific situations such aspreparing root ends, removing posts,
removinginstrument fragments and searching for calcifiedcanals.
Ultrasonic tips specially designed for root-end preparation allow
for conservative and pre-cise preparation of the root end during
apicalsurgery.
Electronic apex locators. The task of deter-mining canal length
has moved into a new andmore precise era with the rapid evolution
of elec-tronic devices that measure the length of the rootcanal.
The first- and second-generation apex loca-tors were more difficult
to use and more prone toerroneous readings than are the
third-generationdevices now available.
Research and clinical experience support theclaim that apex
locators can assist accurately indetermining canal length in the
majority ofcases.76-78Apex locators also can be used to detect
perforations and root fractures. The use of elec-tronic apex
locators is contraindicated in patientswith cardiac pacemakers,
although the actualrisk to these patients is uncertain.79
Lasers. Lasers have various applications in
endodontics such as measuring pulp vitality,80
treating dentinal hypersensitivity,81 preparingand disinfecting
root canals,82,83 and performingapical surgery.84
Reports about these applications are con-flicting, owing to the
use of different types oflasers, energy levels and specimens used.
LDFhas the most promising application in endodon-tics. LDF was
developed to assess blood flow inmicrovascular systems.85 The
reliability of con-ventional pulp tests can vary in newly
eruptedand traumatized teeth, owing to incomplete for-
mation or trauma to the neural pulpal compo-nent, respectively.
LDF techniques are sensitiveand accurate for pulp vitality testing
becausethey reflect vascular rather than nervous respon-siveness
when compared with other methods.44
LDF is a useful research instrument, but a prac-tical clinical
device still is lacking.
The neodymium:yttrium-aluminum-garnet(Nd:YAG) laser is the most
popular system forcleaning and shaping the root canal
system,because the device offers a thin fiber-opticdelivery system
for entering narrow root canals.
Lasers can remove the smear layer and debris;however, it is
difficult to clean all root canal wallswith these devices, because
the linear emission ofthe laser beam makes it almost impossible to
irra-diate the lateral canal walls and leaves themrough and uneven.
Root canal spaces rarely arestraight; more often, they are curved
in at leasttwo dimensions. For lasers to be useful inendodontics,
it is necessary to improve the fibertip and the method so that the
laser irradiates allareas of root canal walls. Several studies
haveevaluated the sterilization of root canal systems
by means of CO286
and Nd:YAG lasers.
87
Althoughlasers used at high power have a bactericidaleffect,
that effect is dependent on each laser. Fur-thermore, using lasers
to disinfect root canals isproblematic, since it can inflict
thermal injury onperiodontal tissues.
Despite lasers approval for dental proceduresby the U.S. Food
and Drug Administration, moreresearch is required to develop lasers
for use inendodontics and to compare their efficacy withthat of
present treatment modalities.
JADA, Vol. 136, January 2005 45
R E S E A R C H
Copyright 2005 American Dental Association. All rights
reserved.
onJuly28,2008
jada.ada.org
Downloadedfrom
http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/
-
7/28/2019 State of the Art and Science of Endodontics
7/13
SPECIAL CASES
Nonsurgical retreatment (indications versussurgery). Despite the
availability of advancedtechnological tools and better
understanding ofthe biology of pulp and periradicular
diseases,clinicians often need to address posttreatmentendodontic
disease.88 Before commencing withany treatment, clinicians must
consider all inter-
disciplinary treatment options in terms of time,expense,
prognosis and patient satisfaction. If thechoice is endodontics,
then the goal of nonsurgicalretreatment is to remove materials from
the rootcanal space and to address any deficiencies orrepair
defects that are pathological or iatrogenicin origin.89 Many
significant advantages resultwhen endodontically failing teeth are
re-enterednonsurgically. Endodontic access provides theopportunity
to evaluate teeth for coronal leakage,fractures and missed
canalsand importantly,after disassembly procedures, these root
canal
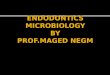
systems can be three-dimensionally cleaned,shaped and obturated
(Figure 1).90Advancementsin the field of nonsurgical endodontic
retreatmentare related directly to the introduction of thedental
OM, ultrasonic technology and relatedinstruments, NiTi rotary
shaping files and MTA.91
Nonsurgical retreatment of failed cases has asimilar success
rate to that of initial conventionaltreatment if the cause of
failure is identified andcorrected.92
Perforation repairs. Historically, the occur-rence of
perforations during root canal treatment
has reduced the long-term prognosis of theaffected tooth
significantly. The poor prognosis ofperforations is mostly due to
bacterial leakage orthe lack of biocompatibility of the repair
materi-als used.93 The important steps in the manage-
ment of a furcal perforation are immediate treat-ment, adequate
isolation, dbridement andsealing of the defect.94 Discovery of new
materialssuch as MTA95,96 has significantly improved theprognosis
for what once were considered hopelessteeth.97
Trauma and management of open apexes.Traumatic injuries in young
patients present aspecial challenge during endodontic treatment
interms of diagnosis and treatment planning, aswell as of managing
the open apex. Wheneverpossible, the goal should be preservation of
pulp
vitality to allow continued development alongthe entire root
length.98 MTA has the most desir-able properties for this purpose99
because it pro-vides a good seal,100 is biocompatible101 andinduces
hard-tissue formation.102 If the pulp isnecrotic, the treatment of
choice is root canaltherapy.103 However, in an immature tooth,
com-pletion of root canal therapy must be delayeduntil root-end
closure has been completed.104
Long-term calcium hydroxide therapy no longeris the treatment of
choice because of the vari-ability of its treatment outcomes and
its adverse
effects on dentin.105
Researchers have advocatedplacement of an artificial barrier as
an alterna-tive to long-term apexification
procedures.62,106,107
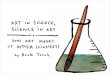
More recently, MTA has been shown to inducehard-tissue formation
more predictably than cal-cium hydroxide (Figure 2), while
bioactivematerials such as bone morphogenetic proteinshave
demonstrated no added advantage over cal-cium hydroxide.63
Evaluation of healing of intra-alveolar rootfractures in
patients between the ages of sevenand 17 years suggests that 77
percent of these
cases heal by means of development of a hard-tissue fragment,
development of periodontal liga-ment or a combination of the
two.108 Pulp vitality,degree of tooth development, presence or
absenceof response of the pulp to stimuli, type of injury,amount of
diastasis between the fragments andefforts to reposition the
displaced fragments havean influence on healing.108 However, the
efficacyof long-term splinting is questionable.108
To prioritize treatment of traumatic injuries,treatment delivery
has been divided into threegroups109: acute (treatment rendered
within a few
46 JADA, Vol. 136, January 2005
R E S E A R C H
Figure 1. Nonsurgical retreatment allows for three-
dimensional dbridement and obturation of the rootcanal
system.
Copyright 2005 American Dental Association. All rights
reserved.
onJuly28,2008
jada.ada.org
Downloadedfrom
http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/
-
7/28/2019 State of the Art and Science of Endodontics
8/13
hours), subacute (treatment rendered within thefirst 24 hours)
and delayed (treatment renderedafter the first 24 hours). A survey
of theavailable literature suggests the
followingrecommendations:dcrown and crown/root fracturessubacute
ordelayed treatment;droot fracturesacute or subacute
treatment;dconcussion and subluxationsubacutetreatment;dextrusion
and lateral luxationacute or suba-cute treatment;dintrusionsubacute
treatment;davulsionacute treatment if the tooth is notreplanted at
the time of injury, subacute treat-ment otherwise;dprimary tooth
injurysubacute treatment,
unless the primary tooth is displaced into the fol-licle of the
permanent tooth or occlusal problemsare present, in which cases
acute treatment isnecessary.
Surgical root canal therapy. Endodonticsurgery is not oral
surgery in the traditionalsense. Rather, it actually is endodontic
therapyperformed through a surgical flap. The main pur-pose of
performing periradicular surgery is toremove a portion of a root
with undbrided canalspace or to seal the canal when a complete
sealcannot be accomplished through a coronal
approach. With recent improvements in surgicalinstruments,
materials and techniques,endodontic surgery can provide a second
chanceto retain a tooth that otherwise would beextracted.
Endodontic surgery may be necessaryto address anatomical
complexities and pro-cedural complications associated with
difficultnonsurgical cases.110-113 The OM is the latest addi-tion
to this armamentarium, providing up to 32magnification of the
surgical field.114,115 The quan-tity and quality of light in the
working field is asimportant as magnification. The coaxial
lighting
and improved optics of an OM provide better dis-tinction between
tooth and bone. Identifyingminute canal openings, incipient
fracture linesand other important anatomical findings
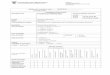
becomesroutine with the OM. For example, an isthmusfrequently runs
between two canals in themesiobuccal root of the maxillary first
molar.116,117
These small communications contain pulp tissueremnants and
should be included in root-endcavity preparations and fillings
during endodonticsurgery.118 The magnification and
illuminationafforded by the OM facilitates identification of
these ramifications, allowing them to be preparedand filled with
the main canals (Figure 3).
Enhanced magnification necessitates miniatur-ization of
endodontic surgical instruments.Microscalpels, piezoelectric
ultrasonic handpieces,surgical micromirrors and microsurgical
irriga-tors, together with miniature carriers, condensersand
pluggers, have been developed to accommo-
date the high level of magnification used rou-tinely in
endodontic surgical procedures.The miniaturized instruments allow
more pre-
cise performance of surgical procedures. Forinstance, the
root-end preparation is aligned par-allel to the long axis of the
root using speciallydesigned ultrasonic tips to a depth of 3
mm.119Avariety of root-end filling materials can be used,which
include Super EBA (Harry J. Bosworth,Skokie, Ill.), intermediate
restorative material,dentin bonding agents and, most
recently,MTA.118,120,121 The materials should be biocompat-
JADA, Vol. 136, January 2005 47
R E S E A R C H
Figure 2. A. Radiograph demonstrating a mandibular pre-molar
with an incompletely developed root and an openapex. B. Radiograph
demonstrating formation of a hard-tissue barrier at the root end of
the premolar after treat-ment with mineral trioxide aggregate as an
apical plug.
B
A
Copyright 2005 American Dental Association. All rights
reserved.
onJuly28,2008
jada.ada.org
Downloadedfrom
http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/
-
7/28/2019 State of the Art and Science of Endodontics
9/13
ible, provide a hermetic seal and, ideally, stimu-
late hard-tissue growth. MTA provides a superiorapical seal
compared with other root-end fillingmaterials and is not adversely
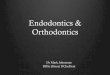
affected by bloodcontamination. In several studies,
histologicsections demonstrate the regeneration of newcementum over
the MTA root-end filling (Figure4), a phenomenon that is not seen
with other com-monly used root-end filling materials.
Clinical controversy: the smear layer.Studies have shown that
current methods ofcleaning and shaping root canals produce a
smearlayer that covers the instrumented walls.54,122-125
The smear layer contains inorganic and organicsubstances that
include fragments of odonto-blastic processes, microorganisms and
necroticmaterials.
Proponents of smear layer removal claim that
the presence of a smear layer can inhibit or signif-icantly
delay penetration of antimicrobial agentssuch as intracanal
irrigants and medications intothe dentinal tubules.126,127
Furthermore, removalof the smear layer may significantly
improveadhesion of obturation materials to the canalwalls128-132
and reduce microleakage.132-137
While some investigators have reported thatthe removal of the
smear layer does not have anysignificant effect on microleakage of
rootcanals,138-140 the opponents of smear layer removalhave shown
an increased level of leakage through
the obturated root canals141 with a 10- to 80-micrometer depth
of penetration.142-146
Despite controversy regarding the effect of thesmear layer on
the quality of instrumentationand obturation, it should be noted
that the smearlayer itself may be infected and may protect
thebacteria already present in the dentinaltubules.54,147,148
Because of these concerns, it maybe prudent to remove the initially
created smearlayer from infected root canals and allow penetra-tion
of intracanal medications into the dentinaltubules of these teeth.
After disinfection of the
root canal system, the smear layer can be recre-ated. Chemical,
mechanical and laser means canbe used to remove the smear
layer.
Management of pain, infection and anx-iety. Considerable
advances have occurred in themanagement of pain, infection and
anxiety in theendodontic patient.
Pain. Survey studies indicate that only about40 percent of
patients report pain after nonsur-gical root canal therapy, with
about 20 to 25 per-cent reporting moderate-to-severe pain.149
Thus,the clinician should tailor pain management
strategies to each patient. A survey of endodonticclinical
trials indicated that the presence of preop-erative pain or a
positive response to percussion isa consistent predictor of
patients most likely toreport postendodontic pain.150A systematic
reviewof nonsteroidal anti-inflammatory drugs used totreat pain in
endodontic patients reported goodanalgesic responses in patients
treated with either100 milligrams of flurbiprofen or the
combinationof flurbiprofen with 100 mg of tramadol.151
In the classic case of the difficult-to-anesthetizemandibular
molar, several studies have demon-
48 JADA, Vol. 136, January 2005
R E S E A R C H
Figure 4. Photomicrograph (original magnification 50,hemotoxylin
and eosin stain) demonstrating a completecementum layer over a
resected root end filled with min-eral trioxide aggregate.
Figure 3. Clinical photograph demonstrating an isthmusconnecting
the two canals in the mesial root of amandibular first molar.
Copyright 2005 American Dental Association. All rights
reserved.
onJuly28,2008
jada.ada.org
Downloadedfrom
http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/
-
7/28/2019 State of the Art and Science of Endodontics
10/13
strated that intraosseous anesthetics are effectivefor enhancing
the incomplete anesthesia thatoccurs after inferior alveolar nerve
blockinjection.152,153
Infection. Considerable progress has been made
with respect to the use of antibiotics in endo-dontic patients.
Susceptibility testing studieshave indicated that 80 to 95 percent
of cultivableendodontic microorganisms remain sensitive
topenicillin, supporting the selection of penicillin asan
antibiotic of first choice when indicated.154,155
Clindamycin is a good alternative for patientswho are unable to
take penicillin, since approxi-mately 87 to 100 percent of
cultivable endodonticmicroorganisms are sensitive to this
antibi-otic.154,155Although antibiotics are effective fortreating
endodontic infections, they appear to
have little effect on reducing pain.156 In addition,antibiotics
have no effect when prescribed to treatpain due to irreversible
pulpitis.157
Anxiety. Researchers have evaluated severalapproaches for
treating anxiety associated withendodontic care. In general, both
behavioral andpharmacological methods have proven to be effec-tive.
Oral triazolam (0.25 mg) may be superior tooral diazepam (5 mg) for
reducing anxiety asso-ciated with endodontic treatment.158
CONCLUSIONS AND FUTURE DIRECTIONS
The art and science of endodontics have under-gone significant
advances in the past decade.These changes have resulted in improved
treat-ment outcomes and an opportunity to preservethe natural
dentition. These objectives can beachieved with less morbidity and
more pre-dictability. The specialty of endodontics is dedi-cated to
the preservation of healthy natural denti-tion. Compilation of more
current clinical datathat are based on procedures performed
withmore advanced techniques will provide a moreaccurate rate of
healing after nonsurgical and
surgical endodontic therapy. The future holds thepromise of
continued growth of the body ofresearch knowledge, and systematic
reviews willprovide the most valuable thread of evidence
con-necting the patient, the clinician, the educator,the
researcher, the policy-maker, the editor, thebenefit purchaser and
the benefit provider in thedecision-making process. s
Dr. Shabahang is the chair, Research and Scientific Affairs
Com-mittee, Loma Linda University, Department of Endodontics, P.O.
Box1057, Loma Linda, Calif. 92354-1057, e-mail
[email protected]. Address reprint requests to Dr.
Shabahang.
This work was made possible by the contributions of the members
ofand consultants to the American Association of Endodontics
Researchand Scientific Affairs Committee who contributed to this
report: Drs.Leif K. Bakland, Mario DAddario, Mohamed F. Fayad,
Ashraf Fouad,Charles J. Goodacre, Kenneth M. Hargreave, G.R.
Holland, John I.Ingle, Bradford R. Johnson, Sergio Kuttler, Jeffrey
Lilly, Robert J.Loushine, Andre Mickel, Carl W. Newton, Ilan
Rotstein, Clifford J.
Ruddle, Charles L. Steffel and Mahmoud Torabinejad.
1. Baumgartner JC, Falkler WA Jr, Beckerman T.
Experimentallyinduced infection by oral anaerobic microorganisms in
a mouse model.Oral Microbiol Immunol 1992;7(4):253-6.
2. Sundqvist G. Associations between microbial species in dental
rootcanal infections. Oral Microbiol Immunol 1992;7(5):257-62.
3. Siqueira JF Jr, Magalhaes FA, Lima KC, de Uzeda
M.Pathogenicity of facultative and obligate anaerobic bacteria in
mono-culture and combined with eitherPrevotella intermedia
orPrevotellanigrescens. Oral Microbiol Immunol
1998;13(6):368-72.
4. Griffee MB, Patterson SS, Miller CH, Kafrawy AH, Newton
CW.The relationship ofBacteroides melaninogenicus to symptoms
asso-ciated with pulpal necrosis. Oral Surg Oral Med Oral
Pathol1980;50(5):457-61.
5. Yoshida M, Fukushima H, Yamamoto K, Ogawa K, Toda T.,Sagawa
H. Correlation between clinical symptoms and microorganismsisolated
from root canals of teeth with periapical pathosis. J
Endod1987;13(1): 24-8.
6. Sundqvist G, Johansson E, Sjgren U. Prevalence of
black-pigmentedBacteroides species in root canal infections. J
Endod1989;15(1):13-9.
7. Gharbia SE, Haapasalo M, Shah HN, et al. Characterization
ofPrevotella intermedia andPrevotella nigrescens isolates from
peri-odontic and endodontic infections. J Periodontol
1994;65(1):56-61.
8. Baumgartner JC, Bae KS, Xia T, Whitt J, David LL.
Sodiumdodecyl sulfate-polyacrylamide gel electrophoresis and
polymerasechain reaction for differentiation ofPrevotella
intermedia andPre-votella nigrescens. J Endod 1999;25(5):324-8.
9. Dymock D, Weightman AJ, Scully C, Wade WG. Molecular
anal-ysis of microflora associated with dentoalveolar abscesses. J
ClinMicrobiol 1996;34(3):537-42.
10. Munson MA, Pitt-Ford T, Chong B, Weightman A, Wade
WG.Molecular and cultural analysis of the microflora associated
withendodontic infections [published correction appears in J Dent
Res2003;82(1):69 and in J Dent Res 2003;82(3): 247]. J Dent
Res2002;81(11):761-6.
11. Molander A, Reit C, Dahlen G, Kvist T. Microbiological
status ofroot-filled teeth with apical periodontitis. Int Endod J
1998;31(1):1-7.
12. Sundqvist G, Figdor D, Persson S, Sjgren U. Microbiologic
anal-ysis of teeth with failed endodontic treatment and the outcome
of con-servative re-treatment. Oral Surg Oral Med Oral Pathol Oral
RadiolEndod 1998;85(1):86-93.
13. Hancock HH 3rd, Sigurdsson A, Trope M, Moiseiwitsch J.
Bac-teria isolated after unsuccessful endodontic treatment in a
NorthAmerican population. Oral Surg Oral Med Oral Pathol Oral
RadiolEndod 2001;91(5):579-86.
14. Waltimo TM, Siren EK, Torkko HL, Olsen I, Haapasalo MP.Fungi
in therapy-resistant apical periodontitis. Int Endod
J1997;30(2):96-101.
15. Happonen RP. Periapical actinomycosis: a follow-up study of
16surgically treated cases. Endod Dent Traumatol
1986;2(5):205-9.
16. Sunde PT, Olsen I, Lind PO, Tronstad L. Extraradicular
infec-tion: a methodological study. Endod Dent Traumatol
2000;16(2):84-90.
17. Gatti JJ, Dobeck JM, Smith C, White RR, Socransky SS, Skobe
Z.
Bacteria of asymptomatic periradicular endodontic lesions
identified byDNA-DNA hybridization. Endod Dent Traumatol
2000;16(5):197-204.18. Sunde PT, Tronstad L, Eribe ER, Lind PO,
Olsen I. Assessment of
periradicular microbiota by DNA-DNA hybridization. Endod
DentTraumatol 2000;16(5):191-6.
19. Sabeti M, Valles Y, Nowzari H, Simon JH, Kermani-Arab V,
SlotsJ. Cytomegalovirus and Epstein-Barr virus DNA transcription
inendodontic symptomatic lesions. Oral Microbiol Immunol
2003;18(2):104-8.
20. Byers MR, Narhi MV. Dental injury models: experimental
toolsfor understanding neuroinflammatory interactions and polymodal
noci-ceptor functions. Crit Rev Oral Biol Med 1999;10:4-39.
21. Goodis HE, Bowles WR, Hargreaves KM. Prostaglandin
E2enhances bradykinin-evoked iCGRP release in bovine dental pulp.
JDent Res 2000;79:1604-7.
22. Olgart L. Neural control of pulpal blood flow. Crit Rev Oral
BiolMed 1996;7:159-71.
JADA, Vol. 136, January 2005 49
R E S E A R C H
Copyright 2005 American Dental Association. All rights
reserved.
onJuly28,2008
jada.ada.org
Downloadedfrom
http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/
-
7/28/2019 State of the Art and Science of Endodontics
11/13
23. Takahashi K. Changes in the pulpal vasculature during
inflam-mation. J Endod 1990;16:92-7.
24. Heyeraas KJ, Berggreen E. Interstitial fluid pressure in
normaland inflamed pulp. Crit Rev Oral Biol Med 1999;10:328-36.
25. Jontell M, Okiji T, Dahlgren U, Bergenholtz G. Immune
defensemechanisms of the dental pulp. Crit Rev Oral Biol Med
1998;9:179-200.
26. Stashenko P, Teles R, DSouza R. Periapical inflammatory
responses and their modulation. Crit Rev Oral Biol Med
1998;9:498-521.27. Fouad A. Are antibiotics effective for
endodontic pain? An
evidence-based review. Endod Topics 2002;3:52-66.28. Narhi M,
Jyvasjarvi E, Virtanen A, Huopaniemi T, Ngassapa D,
Hirvonen T. Role of intradental A- and C-type nerve fibres in
dentalpain mechanisms. Proc Fin Dent Soc 1992;88:507-16.
29. Rodd HD, Boissonade FM. Substance P expression in humantooth
pulp in relation to caries and pain experience. Eur J Oral
Sci2000;108:467-74.
30. Awawdeh L, Lundy FT, Shaw C, Lamey PJ, Linden GJ, KennedyJG.
Quantitative analysis of substance P, neurokinin A and
calcitoningene-related peptide in pulp tissue from painful and
healthy humanteeth. Int Endod J 2002;35:30-6.
31. Bowles WR, Withrow JC, Lepinski AM, Hargreaves KM.
Tissuelevels of immunoreactive substance P are increased in
patients withirreversible pulpitis. J Endod 2003;29:265-7.
32. Goldberg M, Six N, Decup F, et al. Application of
bioactivemolecules in pulp-capping situations. Adv Dent Res
2001;15:91-5.
33. Smith AJ, Murray PE, Sloan AJ, Matthews JB, Zhao S.
Trans-dentinal stimulation of tertiary dentinogenesis. Adv Dent
Res2001;15:51-4.
34. American Dental Association. The 1999 survey of dental
servicesrendered. Chicago: American Dental Association;
2002:16.
35. Friedman S, Lost C, Zarrabian M, Trope M. Evaluation of
successand failure after endodontic therapy using a glass ionomer
cementsealer. J Endod 1995;21(7):384-90.
36. Caliskan MK, Sen BH. Endodontic treatment of teeth with
apicalperiodontitis using calcium hydroxide: a long-term study.
Endod DentTraumatol 1996;12(5):215-21.
37. Sjgren U, Hagglund B, Sundqvist G, Wing K. Factors
affectingthe long-term results of endodontic treatment. J Endod
1990;16(10):498-504.
38. rstavik D. Time-course and risk analyses of the
developmentand healing of chronic apical periodontitis in man. Int
Endod J1996;29(3):150-5.
39. Bender IB. Pulpal pain diagnosis: a review. J Endod
2000;26(3):
175-9.40. Hyman JJ, Cohen ME. The predictive value of endodontic
diag-
nostic tests. Oral Surg Oral Med Oral Pathol
1984;58(3):343-6.41. Michaelson PL, Holland GR. Is pulpitis
painful? Int Endod J
2002;35(10):829-32.42. Petersson K, Soderstrom C, Kiani-Anaraki
M, Levy G. Evaluation
of the ability of thermal and electrical tests to register pulp
vitality.Endod Dent Traumatol 1999;15(3):127-31.
43. Ingolfsson AR, Tronstad L, Hersh EV, Riva CE. Efficacy of
laserDoppler flowmetry in determining pulp vitality of human teeth.
EndodDent Traumatol 1994;10(2):83-7.
44. Evans D, Reid J, Strang R, Stirrups D. A comparison of
laserDoppler flowmetry with other methods of assessing the vitality
of trau-matised anterior teeth. Endod Dent Traumatol
1999;15(6):284-90.
45. Schnettler JM, Wallace JA. Pulse oximetry as a diagnostic
tool ofpulpal vitality. J Endod 1991;17(10):488-90.
46. Roebuck EM, Evans DJ, Stirrups D, Strang R. The effect of
wave-length, bandwidth, and probe design and position on assessing
the
vitality of anterior teeth with laser Doppler flowmetry. Int J
PaediatrDent 2000;10(3):213-20.47. Aanderud-Larsen K, Brodin P,
Aars H, Skjelbred P. Laser
Doppler flowmetry in the assessment of tooth vitality after Le
Fort Iosteotomy. J Craniomaxillofac Surg 1995;23(6):391-5.
48. Hahn CL, Falkler WA Jr, Siegel MA. A study of T and B cells
inpulpal pathosis. J Endod 1989;15(1):20-6.
49. Izumi T, Kobayashi I, Okamura K, Sakai H.
Immunohistochem-ical study on the immunocompetent cells of the pulp
in human non-carious and carious teeth. Arch Oral Biol
1995;40(7):609-14.
50. Tjderhane L, Pkknen V, Larmas M, Sulkala M, Salo T.
DNAmicroarray analysis of differential MMP expression in healthy
and car-ious tooth pulp tissue (abstract 537). J Dent Res 2003
(serial onCD-ROM).
51. Tsou R, Cole JK, Nathens AB, et al. Analysis of hypertrophic
andnormal scar gene expression with cDNA microarrays. J Burn
CareRehabil 2000;21(6):541-50.
52. Schilder H. Cleaning and shaping the root canal. Dent Clin
NorthAm 1974;18(2):269-96.
53. Pataky L, Ivanyi I, Grigar A, Fazekas A. Antimicrobial
efficacy ofvarious root canal preparation techniques: an in vitro
comparativestudy. J Endod 2002;28(6):603-5.
54. McComb D, Smith DC. A preliminary scanning electron
micro-scopic study of root canals after endodontic procedures. J
Endod
1975;1:238-42.55. Torabinejad M, Khademi AA, Babagoli J, et al.
A new solution forthe removal of the smear layer. J Endod
2003;29(3):170-5.
56. Sjgren U, Figdor D, Persson S, Sundqvist G. Influence of
infec-tion at the time of root filling on the outcome of endodontic
treatmentof teeth with apical periodontitis [published correction
appears in IntEndod J 1998;31(2):148]. Int Endod J
1997;30(5):297-306.
57. Shuping GB, rstavik D, Sigurdsson A, Trope M. Reduction
ofintracanal bacteria using nickel-titanium rotary instrumentation
andvarious medications. J Endod 2000;26:751-5.
58. Torabinejad M, Shabahang S, Aprecio R, Kettering JD.
Theantimicrobial effect of MTAD: an in vitro investigation. J
Endod2003;29(6):400-3.
59. Shabahang S, Torabinejad M. Effect of MTAD on
Enterococcusfaecalis-contaminated root canals of extracted human
teeth. J Endod2003;29(9):576-9.
60. Ingle JI. The Washington study of success and failure. In:
IngleJI, Bakland LK, eds. Endodontics. 5th ed. Hamilton, Ontario,
Canada:BC Decker; 2002:748.
61. Pitts DL, Jones JE, Oswald RJ. A histological comparison of
cal-cium hydroxide plugs and dentin plugs used for the control of
gutta-percha root canal filling material. J Endod
1984;10(7):283-93.
62. Schumacher JW, Rutledge RE. An alternative to apexification.
JEndod 1993;19(10):529-31.
63. Shabahang S, Torabinejad M, Boyne P, Abedi H, McMillan P.
Acomparative study of root-end induction using osteogenic
protein-1, cal-cium hydroxide, and mineral trioxide aggregate in
dogs. J Endod1999;24(1):1-5.
64. Snider D, Torabinejad M, Tang HM, Bakland LK. Effect of
rootcanal obturation and/or coronal seal on the success of root
canaltherapy (abstract 50). J Endod 1999;25:294.
65. Swanson K, Madison S. An evaluation of coronal microleakage
inendodontically treated teeth: part Itime periods. J Endod
1987;13(2):56-9.
66. Torabinejad M, Ung B, Kettering JD. In vitro bacterial
penetra-tion of coronally unsealed endodontically treated teeth. J
Endod1990;16(12):566-9.
67. Magura ME, Kafrawy AH, Brown CE Jr, Newton CW. Humansaliva
coronal microleakage in obturated root canals: an in vitro study.J
Endod 1991;17(7):324-31.
68. Khayat A, Lee SJ, Torabinejad M. Human saliva penetration
ofcoronally unsealed obturated root canals. J Endod
1993;19(9):458-61.
69. Mines P, Loushine RJ, West LA, Liewehr FR, Zadinsky JR. Use
ofthe microscope in endodontics: a report based on a questionnaire.
JEndod 1999;25(11):755-8.
70. Rubinstein RA, Kim S. Long-term follow-up of cases
consideredhealed one year after apical microsurgery. J Endod
2002;28(5):378-83.
71. Schwarze T, Baethge C, Stecher T, Geurtsen W. Identification
ofsecond canals in the mesiobuccal root of maxillary first and
secondmolars using magnifying loupes or an operating microscope.
AustEndod J 2002;28(2):57-60.
72. Buhrley LJ, Barrows MJ, BeGole EA, Wenckus CS. Effect of
mag-nification on locating the MB2 canal in maxillary molars. J
Endod2002;28(4):324-7.
73. von Arx T, Hunenbart S, Buser D. Endoscope- and
video-assisted
endodontic surgery. Quintessence Int 2002;33(4):255-9.74.
Bahcall JK, Barss JT. Fiberoptic endoscope usage for
intracanalvisualization. J Endod 2001;27(2):128-9.
75. von Arx T, Walker WA 3rd. Microsurgical instruments for
root-end cavity preparation following apicoectomy: a literature
review.Endod Dent Traumatol 2000;16(2):47-62.
76. Fouad AF, Reid LC. Effect of using electronic apex locators
onselected endodontic treatment parameters. J Endod
2000;26(6):364-7.
77. Fouad AF, Krell KV, McKendry DJ, Koorbusch GF, Olson
RA.Clinical evaluation of five electronic root canal length
measuringinstruments. J Endod 1990;16(9):446-9.
78. Dunlap CA, Remeikis NA, BeGole EA, Rauschenberger CR. An
invivo evaluation of an electronic apex locator that uses the ratio
methodin vital and necrotic canals. J Endod 1998;24(1):48-50.
79. Garofalo RR, Ede EN, Dorn SO, Kuttler S. Effect of
electronicapex locators on cardiac pacemaker function. J Endod
2002;28(12):831-3.
50 JADA, Vol. 136, January 2005
R E S E A R C H
Copyright 2005 American Dental Association. All rights
reserved.
onJuly28,2008
jada.ada.org
Downloadedfrom
http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/
-
7/28/2019 State of the Art and Science of Endodontics
12/13
80. Gazelius B, Olgart L, Edwall B, Edwall L. Non-invasive
recordingof blood flow in human dental pulp. Endod Dent Traumatol
1986;2(5):219-21.
81. Fayad MI, Carter JM, Liebow C. Transient effects of
low-energyCO2 laser irradiation on dentinal impedance: implications
for treat-ment of hypersensitive teeth. J Endod 1996;22:526-31.
82. Levy G. Cleaning and shaping the root canal with a Nd:YAG
laser
beam: a comparative study. J Endod 1992;18:123-7.83. Hardee MW,
Miserendino LJ, Kos W, Walia H. Evaluation of theantibacterial
effects of intracanal Nd:YAG laser irradiation. J
Endod1994;20:377-80.
84. Bader G, Lejeune S. Prospective study of two retrograde
endo-dontic apical preparations with and without the use of CO2
laser.Endod Dent Traum 1998;14:75-8.
85. Tronstad L. Recent development in endodontic research. Scand
JDent Res 1992;100:52-9.
86. Zakariasen KL, Dederich DN, Tulip J, DeCoste S, Jensen
SE,Pickard MA. Bactericidal action of carbon dioxide laser
radiation inexperimental dental root canals. Can J Microbiol
1986;32:942-6.
87. Ramskold LO, Fong CD, Stromberg T. Thermal effects
andantibacterial properties of energy levels required to sterilize
stainedroot canals with an Nd:YAG laser. J Endod
1997;23:96-100.
88. Scianamblo MJ. Endodontic failures: the retreatment of
previ-ously endodontically treated teeth. Revue DOdonto
Stomatologie1988;17(5):409-23.
89. Ruddle CJ. Nonsurgical endodontic retreatment. In: Cohen
S,
Burns RC, eds. Pathways of the pulp. 8th ed. St. Louis:
Mosby;2002:875-929.
90. Machtou P. La cavit daccs. In: Machtou P, Bensoussan D,
Hart-mann A, Mandel E, eds. Endodontie. Paris: Editions CdP;
1993;125-37.
91. Ruddle CJ. Microendodontic nonsurgical retreatment. Dent
ClinNorth Am 1997;41(3):429-54.
92. Bergenholtz G, Lekholm U, Milthon R, Heden G, Odesjo
B,Engstrom B. Retreatment of endodontic fillings. Scand J Dent
Res1979;87(3):217-24.
93. Arens DE, Torabinejad M. Repair of furcal perforations with
min-eral trioxide aggregate: two case reports. Oral Surg Oral Med
OralPathol Oral Radiol Endod 1996;82(1):84-8.
94. Bryan EB, Woollard G, Mitchell WC. Nonsurgical repair of
furcalperforations: a literature review. Gen Dent
1999;47(3):274-8.
95. Lee SJ, Monsef M, Torabinejad M. Sealing ability of a
mineral tri-oxide aggregate for repair of lateral root
perforations. J Endod 1993;19(11):541-4.
96. Ford TR, Torabinejad M, McKendry DJ, Hong CU,
Kariyawasam
SP. Use of mineral trioxide aggregate for repair of furcal
perforations.Oral Surg Oral Med Oral Pathol Oral Radiol Endod
1995;79(6):756-63.
97. Main C, Mirzayan N, Shabahang S, Torabinejad M. Repair of
rootperforations using mineral trioxide aggregate: a long-term
study. JEndod 2004;30(2):80-3.
98. Pitt Ford T, Shabahang S. Management of incompletely
formedroots. In: Principles of endodontics. 3rd ed. Philadelphia:
Saunders;2001:388-404.
99. Ford TR, Torabinejad M, Abedi HR, Bakland LK, KariyawasamSP.
Using mineral trioxide aggregate as a pulp-capping material.JADA
1996;127(10):1491-4.
100. Torabinejad M, Rastegar AF, Kettering JD, Pitt Ford TR.
Bacte-rial leakage of mineral trioxide aggregate as a root-end
filling material.J Endod 1995;21(3):109-12.
101. Torabinejad M, Hong CU, Pitt Ford TR, Kettering JD.
Cytotoxi-city of four root end filling materials. J Endod
1995;21(10):489-92.
102. Koh ET, Torabinejad M, Pitt Ford TR, Brady K, McDonald
F.Mineral trioxide aggregate stimulates a biological response in
human
osteoblasts. J Biomed Mater Res 1997;37(3):432-9.103. Seltzer S.
The root apex. In: Seltzer S, Krasner P, eds. Endodon-tology. 2nd
ed. Philadelphia: Lea & Febiger; 1988:1-30.
104. Frank A. Therapy for the divergent pulpless tooth by
continuedapical formation. JADA 1966;72(1):87-93.
105. Andreasen JO, Farik B, Munksgaard EC. Long-term
calciumhydroxide as a root canal dressing may increase risk of root
fracture.Dent Traumatol 2002;18(3):134-7.
106. Coviello J, Brilliant JD. A preliminary clinical study on
the useof tricalcium phosphate as an apical barrier. J Endod
1979;5(1):6-13.
107. Brandell DW, Torabinejad M, Bakland LK, Lessard GM.
Dem-ineralized dentin, hydroxylapatite and dentin chips as apical
plugs.Endod Dent Traumatol 1986;2(5):210-4.
108. Cvek M, Andreasen JO, Borum MK. Healing of 208
intraalveolarroot fractures in patients aged 7-17 years. Dent
Traumatol 2001;17:53-62.
109. Andreasen JO, Andreasen FM, Skeie A, Hjorting-Hansen E,
Schwartz O. Effect of treatment delay upon pulp and
periodontalhealing of traumatic dental injuries: a review article.
Dent Traumatol2002;18:116-28.
110. Gutmann JL, Harrison JW. Surgical endodontics. Boston:
Black-well Scientific; 1991.
111. Bellizzi R, Loushine R. A clinical atlas of endodontic
surgery.Chicago: Quintessence; 1991.
112. Arens DE, Torabinejad M, Chivian N, Rubinstein R.
Practicallessons in endodontic surgery. Chicago: Quintessence;
1998.113. Kim S. Color atlas of microsurgery in endodontics.
Philadelphia:
Saunders; 2001.114. Pecora G, Andreana S. Use of dental
operating microscope in
endodontic surgery. Oral Surg Oral Med Oral Path
1993;75:751-8.115. Mounce RE. Surgical operating microscopes in
endodontics: the
paradigm shift. Gen Dent 1995;43(4):346-9.116. Weller RN,
Niemczyk SP, Kim S. Incidence and position of the
canal isthmus: part 1mesiobuccal root of the maxillary first
molar. JEndod 1995;21:380-3.
117. Carr G. Ultrasonic root end preparation. Dent Clin of North
Am1997;41(3):541-54.
118. Torabinejad M, Watson TF, Pitt Ford TR. Sealing ability of
amineral trioxide aggregate when used as a root end filling
material. JEndod 1993;19:591-5.
119. Gilheany PA, Figdor D, Tyas MJ. Apical dentin permeability
andmicroleakage associated with root end resection and retrograde
filling.J Endod 1994;20(1):22-6.
120. Dorn SO, Gartner AH. Retrograde filling materials: a
retrospec-tive success-failure study of amalgam, EBA, and IRM. J
Endod 1990;16(8):391-3.
121. Rud J, Rud V, Munksgaard EC. Long-term evaluation of
retro-grade root filling with dentin-bonded resin composite. J
Endod 1996;22:90-3.
122. Moodnik RM, Dorn SO, Feldman MJ, Levey M, Borden BG.
Effi-cacy of biomechanical instrumentation: a scanning electron
microscopicstudy. J Endod 1976;2:261-6.
123. Mader CL, Baumgartner JC, Peters DD. Scanning
electronmicroscopic investigation of the smeared layer on root
canal walls. JEndod 1984;10:477-83.
124. Cengiz T, Aktener BO, Piskin B. The effect of dentinal
tubuleorientation on the removal of smear layer by root canal
irrigants: ascanning electron microscopic study. Int Endod J
1990;23:163-71.
125. Pashley DH. Smear layer: overview of structure and
function.Proc Finn Dent Soc 1992;88(supplement l):215-24.
126. rstavik D, Haapasalo M. Disinfection by endodontic
irrigants
and dressings of experimentally infected dentinal tubules. Endod
DentTraumatol 1990;6:142-9.
127. Bystrm A, Sundqvist G. The antibacterial action of
sodiumhypochlorite and EDTA in 60 cases of endodontic therapy. Int
Endod J1985;18:35-40.
128. Abramovich A, Goldberg F. The relationship of the root
canalsealer to the dentine wall: an in vitro study using the
scanning electronmicroscope. J Br Endod Soc 1976;9(2):81-6.
129. Tidmarsh BG. Acid-cleansed and resin-sealed root canals.
JEndod 1978;4:117-21.
130. White R, Goldman M, Lin PS. The influence of the
smearedlayer upon dentinal tubule penetration by plastic filling
materials. JEndod 1984;10:558-62.
131. Gettleman BH, Messer HH, ElDeeb ME. Adhesion of
sealercements to dentin with and without the smear layer. J Endod
1991;17:15-20.
132. Economides N, Liolios E, Kolokuris I, Beltes P. Long-term
evalu-ation of the influence of smear layer removal on the sealing
ability of
different sealers. J Endod 1999;25:123-5.133. Kennedy WA, Walker
WA, Gough RW. Smear layer removaleffects on apical leakage. J Endod
1986;12:21-7.
134. Cergneux M, Ciucchi B, Dietschi JM, Holz J. The influence
ofthe smear layer on the sealing ability of canal obturation. Int
Endod J1987;20:228-32.
135. Vassiliadis L, Liolios E, Kouvas V, Economides N. Effect
ofsmear layer on coronal microleakage. Oral Surg Oral Med Oral
PatholOral Radiol Endod 1996;82:315-20.
136. Taylor JK, Jeansonne BG, Lemon RR. Coronal leakage: effects
ofsmear layer, obturation technique, and sealer. J Endod
1997;23:508-12.
137. Karagz-Kkay I, Bayirli G. An apical leakage study in
thepresence and absence of the smear layer. Int Endod J
1994;27:87-93.
138. Evans JT, Simon JH. Evaluation of the apical seal produced
byinjected thermoplasticized gutta-percha in the absence of smear
layerand root canal sealer. J Endod 1986;12:100-7.
139. Chailertvanitkul P, Saunders WP, Mackenzie D. The effect
of
JADA, Vol. 136, January 2005 51
R E S E A R C H
Copyright 2005 American Dental Association. All rights
reserved.
onJuly28,2008
jada.ada.org
Downloadedfrom
http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/
-
7/28/2019 State of the Art and Science of Endodontics
13/13
smear layer on microbial coronal leakage of gutta-percha root
fillings.Int Endod J 1996;29:242-8.
140. Madison S, Krell KV. Comparison of ethylenediamine
tetraceticacid and sodium hypochlorite on the apical seal of
endodonticallytreated teeth. J Endod 1984;10:499-503.
141. Timpawat S, Vongsavan N, Messer HH. Effect of removal of
thesmear layer on apical microleakage. J Endod 2001;27:351-3.
142. Loel DA. Use of acid cleanser in endodontic therapy.
JADA1975;90:148-51.143. Gutirrez JH, Herrera VR, Berg EH, Villena
F, Jofr A. The risk
of intentional dissolution of the smear layer after mechanical
prepara-tion of root canals. Oral Surg Oral Med Oral Pathol
1990;70:96-108.
144. Pallars A, Faus V, Glickman GN. The adaptation of
mechani-cally softened gutta-percha to the canal walls in the
presence orabsence of smear layer: a scanning electron microscopic
study. IntEndod J 1995;28:266-9.
145. Kouvas V, Liolios E, Vassiliadis L, Parissis-Messimeris S,
Bout-sioukis A. Influence of smear layer depth of penetration of
threeendodontic sealers: an SEM study. Endod Dent Traumatol
1998;14:191-5.
146. Genoglu N, Samani S, Gnday M. Dentinal wall adaptation
ofthermoplasticized gutta-percha in the absence or presence of
smearlayer: a scanning electron microscopic study. J Endod
1993;19:558-62.
147. Brannstrm M. Smear layer: pathological and treatment
consid-erations. Oper Dent 1984;3(supplement):35-42.
148. Pashley DH. Smear layer: physiological considerations.
Oper
Dent 1984;3(supplement):13-29.
149. Georgopoulou M, Anastassiadis P, Sykaras S. Pain after
chemo-mechanical preparation. Int Endod J 1996;19:309-14.
150. Hargreaves KM, Hutter JW. Endodontic pharmacology. In:Cohen
S, Burns R, eds. Pathways of the pulp. St Louis:
Mosby;2002:665-82.
151. Holstein A, Hargreaves KM, Neiderman R. Evaluation ofNSAIDs
for treating post-endodontic pain: a systematic review. Endod
Topics 2002;3:3-13.152. Reader A, Nusstein J. Local anesthesia
for endodontic pain.Endod Topics 2002;3:14-30.
153. Hargreaves KM, Keiser K. Local anesthetic failure in
endodon-tics: mechanisms and management. Endod Topics
2002;1:26-39.
154. Khemaleelakul S, Baumgartner JC, Pruksakorn S.
Identifica-tion of bacteria in acute endodontic infections and
their antimicrobialsusceptibility. Oral Surg Oral Med Oral Pathol
Oral Radiol Endod2002;94:746-55.
155. Baumgartner JC, Xia T. Antibiotic susceptibility of
bacteriaassociated with endodontic abscesses. J Endod
2003;29:44-7.
156. Fouad AF, Barry J, Caimano M, et al. PCR-based
identificationof bacteria associated with endodontic infections. J
Clin Microbiol2002;40:3223-31.
157. Nagle D, Reader A, Beck M, Weaver J. Effect of systemic
peni-cillin on pain in untreated irreversible pulpitis. Oral Surg
Oral MedOral Pathol Oral Radiol Endod 2000;90:636-40.
158. Ehrich D, Lundgren J, Dionne R, Nicoll B, Hutter J.
Comparisonof triazolam, diazepam and placebo as outpatient oral
premedication
for endodontic patients. J Endod 1997;23:181-4.
52 JADA, Vol. 136, January 2005
R E S E A R C H
Copyright 2005 American Dental Association. All rights
reserved.
onJuly28,2008
jada.ada.org
Downloadedfrom
http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/http://jada.ada.org/