Embed Size (px)
Citation preview

ITMIG DEFINITIONS AND POLICIES
Standard Report Terms forChest Computed Tomography Reports of
Anterior Mediastinal Masses Suspicious for Thymoma
Edith M. Marom, MD,* Melissa L. Rosado-de-Christenson, MD,†‡ John F. Bruzzi, FFRRCSI,§Masaki Hara, MD,� Joshua R. Sonett, MD,¶ and Loren Ketai, MD#
Key Words: Thymoma, Computed tomography, Structured report-ing, Staging.
(J Thorac Oncol. 2011;6: S1717–S1723)
There is a growing demand for structured reporting inradiology and for the formulation of standard terms to
be used by clinicians and radiologists alike. A studyfocusing on computed tomography (CT) reporting of lungnodules found inconsistency of the reporting of theirmargins and presence of calcifications.1 Another study,comparing imaging terms listed in the Fleischner SocietyGlossary2 with their use in medical lexicons including theInternational Classification of Diseases, 9th revision, ClinicalModification (Center of Medicare and Medicaid Services,Washington, DC), Systematized Nonmenclature of Medicine–Reference Terminology (SNOMED-RT) (College of Ameri-can Pathologists, Northfield, IL), and the Unified MedicalLanguage System (National Library of Medicine, Bethesda,MD), found low rates of utilization of Fleischner termsranging from 3 to 36%.3 On the other hand, when standard-ized reporting is implemented for imaging a specific disease,such as seen in the screening for breast cancer, this leads toimproved patient care. It is expected that the creation of astandardized terminology for the description of an anteriormediastinal mass suspicious for thymoma and the promotion of
its use will result in improved communication between theclinician and the radiologist and will ultimately positively im-pact patient care.
In addition to developing a common language, includ-ing pertinent information in the radiologic report that willinfluence therapy requires knowledge of the disease and isoften disease specific. Because of this, standardized reportinghas been created for specific diseases in a few organs and hasbeen proven useful. The American College of Radiologydeveloped the Breast Imaging Reporting and Data System4 tocharacterize breast lesions seen on mammography and breastultrasound in a standardized manner that correlates with theunderlying histologic findings. The Breast Imaging Reportingand Data System assigns a percentage probability of malig-nancy to each category and has gained worldwide acceptancein its use for guiding clinical management.5 A similar systemhas been developed for the ultrasound evaluation of thyroidnodules, stratifying them into those with imaging findingsmore likely to be malignant and those less likely to bemalignant with suggestions for appropriate clinical manage-ment called Thyroid Imaging and Reporting Data System.6
Although there is preliminary evidence to suggest thatcertain imaging findings in thymoma are important for staging orprognosis, further validation will require the prospective acqui-sition of data, which will be facilitated by the creation of astructured radiology report. The following guidelines containdescriptors that should be included in CT reports of patients withanterior mediastinal masses in whom thymoma is considered inthe differential diagnosis. Corresponding representative imagesare included for clarity and consistency. Pertinent negatives withregard to these descriptors are just as important. Consistent useof these descriptors will help establish a common reportinglanguage that will be used and accepted by clinicians as theymake management decisions regarding their patients with thy-moma and facilitate further research.
METHODSThe process used in development of this document was
designed to represent a broad consensus within the communityof clinicians and researchers interested in thymic diseases. Acore workgroup (Edith M. Marom, Melissa L. Rosado-de-Chris-tenson, John F. Bruzzi, Masaki Hara, Joshua R. Sonett, andLoren Ketai) reviewed the existing literature as well as existing
*Department of Radiology, The University of Texas, M. D. Anderson CancerCenter, Houston, Texas; †University of Missouri-Kansas City, KansasCity, Missouri; ‡Department of Radiology, Uniformed Services Univer-sity, Bethesda, Maryland; §Department of Radiology, Galway UniversityHospitals (GUH), Galway, Ireland; �Department of Radiology, NagoyaCity University Graduate School of Medical Sciences, Nagoya, Japan;¶Thoracic Surgery Department, Columbia University New York-Presby-terian Hospital, New York, New York; and #Department of Radiology,University of New Mexico Health Science Center, Albuquerque, NewMexico.
Disclosure: The authors declare no conflicts of interest.Address for correspondence: Edith M. Marom, MD, Department of Radiol-
ogy, The University of Texas, M. D. Anderson Cancer Center, Unit 1478,1515 Holcombe Blvd, Houston, TX 77030-4009. E-mail: [email protected]
Copyright © 2011 by the International Association for the Study of LungCancerISSN: 1556-0864/11/0607-1717
Journal of Thoracic Oncology • Volume 6, Number 7, Supplement 3, July 2011 S1717

standards for chest radiology that applied or could be adapted toachieving consistency in reporting imaging findings in anteriormediastinal masses. This group drafted proposed standard reportterms and definitions. These were refined at an InternationalThymic Malignancy Interest Group (ITMIG) Definition andTerminology workshop on November 16, 2010, which wassupported by the International Association for the Study of LungCancer. After distribution to all ITMIG members for comment,the final document was approved and adopted by ITMIG mem-bers in February 2011.
Review of Existing StudiesThe Masaoka staging system and its variants7,8 have
been shown to strongly correlate with prognosis,8–10 yetstaging is often only established postoperatively. Patientswith locally advanced thymoma may receive neoadjuvantchemotherapy to enable effective resection,9,11 as completeresection, even of advanced disease, improves survival.7,12
Currently, it is recommended that patients with stage III andIV thymoma should receive neoadjuvant therapy.13–18 Histor-ically, mediastinal imaging has been considered to havelimited value in the staging of patients with thymoma. Thismay have been due to the limitations of older imagingtechniques and the rarity of thymoma. These factors likelyinfluenced scientific publication and limited the number ofpublished case studies on the imaging of thymoma, which inturn decreased the statistical power of these studies.
CT is currently considered the preferred imaging mo-dality for the initial assessment and follow-up of patients withthymoma.19 In the last decade, CT technique has improveddramatically resulting in routine rapid acquisition of thin-section slices enabling high quality image reformations inmultiple planes. This resulted in improved visualization ofthese tumors, allowing assessment of internal lesion charac-teristics as well as detailed visualization of the tumor’srelationship to surrounding structures.
Promising studies have been published in the last decade,taking advantage of modern CT imaging techniques. Thesestudies have shown that some CT characteristics correlate withaggressive tumor behavior and higher stage. To the best of ourknowledge, only two have correlated the CT appearance ofthymoma with Masaoka staging.20,21,21a One study assessed 50patients with thymoma21,21a and found that invasive thymomaswere more likely to be larger and have low attenuation regions,calcifications, and lobulated and irregular contours when com-pared with low-stage thymomas. A later study assessed 99patients with thymoma20 and found multiple factors associatedwith advanced disease (stages III and IV): large size, lobulatedcontours, heterogeneous attenuation, calcifications, infiltration ofsurrounding mediastinal fat, tumor abutting �50% of a medi-astinal structure, adjacent lung abnormalities, and pleural effu-sion. However, after performing multivariate analysis, largertumor size, lobulated contours, and fatty infiltration surroundingthe tumor were the only imaging findings that were likely tocorrelate with higher stage disease, i.e., stage III or IV.20
Thymomas are classified histologically by the WorldHealth Organization (WHO) classification. Although the clin-ical use of the WHO classification is debatable because oflack of adequate reproducibility and clinical predictive value
that was found in some studies,10 several CT studies havecorrelated CT appearance with the WHO histologic classifi-cation. Two studies that evaluated 45 and 76 patients withthymoma22,23 found that lobulated and irregular tumor con-tours were associated with more aggressive disease, althoughthis was not confirmed by a third study24 that evaluated 48patients with thymoma.
The above imaging studies are promising. In fact, someclinicians already use large tumor size, tumor heterogeneity,and tumor lobulation to help identify patients who shouldreceive neoadjuvant therapy before attempted resection.However, much larger studies correlating the relationship ofimaging findings of thymoma with its biologic behavior areneeded. Such studies will have to be performed on an inter-national basis as despite thymoma being the most commonprimary neoplasm of the anterior mediastinum, it only ac-counts for less than 1% of all adult malignancies.25
RECOMMENDATIONSWe believe that each CT report of a mediastinal mass
suspicious for thymoma or of newly diagnosed thymoma shouldinclude the following data about the primary mass and itssurrounding structures: lesion location and size in the x, y, and zaxis, description of the lesion contour (smooth or lobulated),presence or absence of heterogeneous attenuation, calcifications,infiltration of surrounding mediastinal fat, and tumor abutting�50% of an adjacent mediastinal structure and direct invasioninto a vessel lumen. The following information regarding thesurrounding structures must also be included: diaphragmaticelevation (consistent with phrenic nerve involvement), adjacentlung abnormalities, pleural effusion, pleural nodule or nodules,lymph node enlargement, and findings suggestive of distantmetastatic disease (i.e., lung, liver, adrenal, or peritoneal nod-ules). If these variables are prospectively and consistently re-corded, they can be used to create a table or drop down menu tobe used in future structured reports (Tables 1 and 2). In addition,if all these data are routinely captured in radiologic reports ofcases of thymoma, retrospective studies could be performedusing the information contained in these reports.
Definitions of Thymoma Report TermsPrimary Tumor Size
We recommend documenting the three axes of tumorsize to mirror information that is consistently contained inpathology reports of excised thymomas. The axial slice cho-sen for measurement is that which demonstrates the longesttumor dimension. The short axis is perpendicular to the longaxis on the same slice (Figure 1). Because tumor orientationdoes not always conform to strict sagittal or coronal refor-mats, the superior-inferior dimension of the tumor should beobtained by subtracting the lowest from the highest bedposition in which the primary tumor is seen (Figure 1).
LocationIt is expected that most of these lesions will be located
in the prevascular anterior mediastinum. Some of these le-sions are unilateral, whereas others cross the midline involv-ing both sides of the mediastinum.
Marom et al. Journal of Thoracic Oncology • Volume 6, Number 7, Supplement 3, July 2011
Copyright © 2011 by the International Association for the Study of Lung CancerS1718

ContourA lesion contour is considered smooth in the absence of
spiculation, ill-defined borders, or lobulation. Smooth lesionsare typically spherical or ovoid in shape, but lesion contoursmay also conform to the shape of the adjacent mediastinum.A lobulated contour is one that exhibits one or more lobula-
tions, characterized as convex tumor contours with adjacentnotches between tumor lobules (Figure 2).
AttenuationThymomas may demonstrate homogeneous or hetero-
geneous attenuation. Heterogeneous attenuation often mani-fests as areas of low attenuation within the tumor and shouldbe assessed on soft tissue or mediastinal windows. Adminis-tration of contrast will help demonstrate tumor heterogeneityand is recommended if not contraindicated (Figure 3). Cysticthymomas exhibit intrinsic low attenuation manifesting ashomogeneous water attenuation surrounded by the soft tissuetumor capsule. These lesions may also exhibit internal softtissue septa. The presence of mural soft tissue nodules in acystic anterior mediastinal mass is one of the characteristicmanifestations of cystic thymoma.
CalcificationsCalcifications of any pattern, including curvilinear,
punctate, or coarse, have been associated with more advanceddisease and should be described and characterized. Viewingthe same image at a different window level, such as with bonewindow, may accentuate the differences between intravascu-lar contrast and tumor calcification (Figure 4).
Infiltration of Surrounding Mediastinal FatFor a tumor to be characterized as infiltrating the sur-
rounding fat, it needs to only infiltrate the fat in one location andnot necessarily along its entire circumference. Such neoplasmsmay exhibit irregular borders. Tumors that abut the mediastinal
TABLE 1. Documentation of Primary Tumor Characteristics
Variable Menu Option
Size (cm) x axis (longest dimension onaxial slice)
y axis (perpendicular to longestdimension)
z axis (craniocaudal dimension)
Contour Smooth
Lobulated
Internal density Homogenous
Heterogeneous
Cystic
Calcification Yes
No
Infiltration of surrounding fat Yes
No
Abutment of �50% of a mediastinal Yes (list which structure/s)
structure with loss of fat plane No
Additional mediastinal Yes (list)
structures the tumor abuts No
Direct vascular endoluminal Yes (list vessel name)
invasion No
TABLE 2. Documentation of Involvement of SurroundingStructures
Variable Menu Option
Abnormalities in adjacent lung parenchyma Yes
No
Presence of a pleural effusion Unilateral
Bilateral
No
Presence of a pleural nodule No
Unilateral/bilateral
1
2–5
�5/diffuse
Mediastinal lymph node enlargement(�1 cm in short axis on an axial image)
Yes (list location accordingto node map26)
No
Abutment at the expected location of thephrenic nerve
Yes
No
Elevated hemidiaphragm Yes
No
Presence of a pulmonary nodule Yes
No
Extrathoracic suspected metastases Yes (list location)
No
FIGURE 1. Tumor size measurement. The measurement isobtained on the axial slice that demonstrates the tumor’slargest diameter; in this case, the largest diameter is 4 cm.The short axis perpendicular to it is 3.5 cm. Tumor rangedin superior to inferior orientation from bed position 197 to149 (197�149 � 48 mm) and thus the superior to inferiordimension is 4.8 cm. Thus, tumor size should be reported as4.0 � 3.5 � 4.8 cm, with the last measurement represent-ing the superior to inferior dimension.
Journal of Thoracic Oncology • Volume 6, Number 7, Supplement 3, July 2011 Standard Report Terms for Chest CT
Copyright © 2011 by the International Association for the Study of Lung Cancer S1719

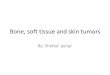
FIGURE 2. Schematic and computed tomography (CT) examples of contour. A, Smooth contour. B, Smooth contour con-forming to the mediastinal structure the lesion abuts without evidence of lobulation. C, Contrast-enhanced chest CT (soft tis-sue window) showing a tumor that conforms to the mediastinal structure it abuts. D, Lobulated contour with single sharpnotch. E, Contrast-enhanced chest CT (soft tissue window) showing lobulated tumor due to the lateral sharp notch (white ar-row) whereas medially the contour is smooth and conforms to the shape of the adjacent mediastinum (black arrowheads). F,Lobulated contour with multiple lobulations. G, CT image of a multilobulated tumor extending into lung parenchyma (whitearrows point at lobulations).
FIGURE 3. Attenuation. Contrast-enhanced chest com-puted tomography (CT) (soft tissue window) of a heteroge-neous thymoma at the level of the pulmonary trunk. Arrowspoint to two of the many small low attenuation regionswithin the mass.
FIGURE 4. Calcification. Contrast-enhanced chest computedtomography (CT) (soft tissue window) at levels set betweenbone and mediastinal window. Curvilinear high-density regions(black arrows) are due to calcifications as they do not conformto the expected morphology of an opacified blood vessel, andmost are of higher attenuation than opacified blood in the leftatrium (LA) and ascending aorta (Ao).
Marom et al. Journal of Thoracic Oncology • Volume 6, Number 7, Supplement 3, July 2011
Copyright © 2011 by the International Association for the Study of Lung CancerS1720

vessels without an intervening fat plane are not considered asinfiltrating of surrounding fat, as the mediastinal fat that typi-cally surrounds the vessel cannot be evaluated for infiltration ifit cannot be visualized (Figure 5).
Tumor Abutting >50% of Mediastinal StructureTo maintain consistency in imaging reports, vessel
abutment should be described as the percentage of the vessel
circumference that is touched by the adjacent tumor withoutan intervening tissue plane (Figure 6).
Direct Vascular InvasionVascular invasion is rarely seen but may manifest as
direct extension of the tumor into a vessel lumen (Figure 7).
FIGURE 5. Infiltration of mediastinal fat. Coronal obliquereformatted contrast-enhanced chest computed tomography(CT) (soft tissue window) shows the thymoma (T) with infil-tration of surrounding mediastinal fat (black arrows). Noticethat the attenuation of the mediastinal fat further away fromthe tumor (arrowheads) is lower than that immediately adja-cent to the lesion.
FIGURE 6. Abutment of vessels. Contrast-enhanced chest(CT) (soft tissue window) demonstrates the thymoma (T)nearly completely encasing the right brachiocephalic vein(white arrow), whereas only abutting about 30% of the aorta(A) circumference. Arrowhead: contrast filled collateral vein.
FIGURE 7. Vessel invasion. Contrast-enhanced chest com-puted tomography (CT) (soft tissue window) at the level ofthe pulmonary trunk (P) demonstrates a thymoma in theanterior mediastinum (arrowhead) with direct invasion (seenon a more superior slice) into the superior vena cava (whitearrow). Note soft tissue attenuation of the intracaval masssimilar to that of the primary tumor.
FIGURE 8. Lymph node enlargement. Contrast-enhancedchest computed tomography (CT) (soft tissue window) atthe level of the aortic arch (A) demonstrates the thymoma(T) and adjacent mildly enlarged ipsilateral mediastinallymph nodes (white arrows). At surgery, no malignancy wasfound within these lymph nodes.
Journal of Thoracic Oncology • Volume 6, Number 7, Supplement 3, July 2011 Standard Report Terms for Chest CT
Copyright © 2011 by the International Association for the Study of Lung Cancer S1721

When present, any appreciable narrowing or deformity of thevessel lumen should be described as well.
Mediastinal Lymph Node EnlargementThe presence and nodal stations of mediastinal lymph
node enlargement should be noted in the report,26 as removalof any enlarged lymph nodes at surgery is recommended.27
The definition of mediastinal lymph node enlargement is ashort-axis diameter of a lymph node greater than 1 cm on anaxial image (Figure 8).
Adjacent Lung AbnormalitiesAdjacent lung abnormalities such as intrapulmonary
extension of tumor are rarely appreciated on CT and areusually detected intraoperatively. The most common pulmo-nary abnormality seen on chest CT is compressive atelectasis
by the adjacent tumor, but this may be difficult to differen-tiate from direct extension of tumor into lung (Figure 9).
Pleural EffusionPleural effusions are not common in patients with
thymoma. However, presence or absence of pleural effusionsshould be documented on the report as they are more fre-quently associated with thymic carcinoma and metastaticpleural involvement by primary neoplasms other than thy-moma (Figure 9).
Diaphragmatic ElevationInclusion of the phrenic nerve in the resection may com-
promise pulmonary function and may lead to serious postoper-ative complications.28 Preoperative documentation of phrenicnerve involvement is of utmost importance as affected patientsmay receive preoperative chemotherapy before surgery to allowcomplete tumor resection of disease without resection of thephrenic nerve, thus leading to a favorable functional and survivalbenefit. Therefore, elevation of the hemidiaphragm should bedocumented in the report. In addition, tumor abutting the ana-tomic location of the course of the phrenic nerve should also bementioned. The phrenic nerve courses over the brachiocephalicartery, posterior to the subclavian vein, and then crosses anteriorto the hilum, over the pericardium covering the right atrium(right phrenic nerve) or left ventricle (left phrenic nerve) to thediaphragm, where it divides into branches which pierce thatmuscle and are distributed to its under surface (Figure 10).
Pleural NodulesMetastatic thymoma typically involves the pleura and
manifests as soft tissue pleural nodules that range from smalllentil-shaped nodules to large pleural masses and can prog-ress to circumferential nodular pleural thickening with in-volvement of the interlobar fissures. Solid pleural metastases(stage IVa) should be distinguished from pulmonary paren-chymal metastases (stage IVb). Pleural nodules are disposedalong the anatomic location of the pleural surfaces and arebest assessed on the lung window in cases of early disease.Intraparenchymal pulmonary nodules29 are completely sur-rounded by lung parenchyma (Figure 11).
FIGURE 9. Pulmonary parenchymal involvement. Contrast-enhanced chest computed tomography (CT) (soft tissue win-dow), at the level of the right pulmonary artery (rp), showsa thymoma (T) compressing the middle lobe bronchus withresultant atelectasis of the middle lobe. The atelectatic mid-dle lobe is seen between the tumor edge (black arrowheads)and the right major fissure (white arrows). It is difficult todetermine whether there is direct tumor invasion into thelung parenchyma at this site. Note the associated right pleu-ral effusion (e).
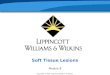
FIGURE 10. Phrenic nerve in-volvement. A, Posterior anteriorchest radiograph of newly diag-nosed thymoma demonstrates alarge mediastinal mass (M) withassociated elevation of the lefthemidiaphragm (arrowhead). B,Contrast-enhanced chest computedtomography (CT) (soft tissue win-dow) at the level of the left pulmo-nary artery (L) demonstrates thethymoma (M) abutting the entireleft side of the mediastinum ante-rior to the hilum, this location is inthe expected course of the leftphrenic nerve.
Marom et al. Journal of Thoracic Oncology • Volume 6, Number 7, Supplement 3, July 2011
Copyright © 2011 by the International Association for the Study of Lung CancerS1722

Distant MetastasesDistant metastases are uncommon at presentation and
constitute stage IVb disease. The most common site is thelung followed by the liver, lymph nodes, and bone.30
CONCLUSIONThis article provides a lexicon of terms that should be
consistently used for describing mediastinal masses suspectedof representing a thymoma. Knowledge of the imaging fea-tures of high-stage thymomas as well as the correct use ofthese terms will add value to the CT report, will facilitatecommunication between clinicians and radiologists, and willallow the radiologist to play an important role in helping theclinician make management decisions for their patients withthymoma including the use of preoperative therapy. Docu-mentation of the above imaging features of thymoma pro-vides the basis for structured reporting and a database forcollected newly diagnosed thymoma cases that permits fur-ther research.
REFERENCES1. Burns J, Haramati LB, Whitney K, et al. Consistency of reporting basic
characteristics of lung nodules and masses on computed tomography.Acad Radiol 2004;11:233–237.
2. Hansell DM, Bankier AA, MacMahon H, et al. Fleischner Society:glossary of terms for thoracic imaging. Radiology 2008;246:697–722.
3. Langlotz CP, Caldwell SA. The completeness of existing lexicons forrepresenting radiology report information. J Digit Imaging 2002;15(Suppl 1):201–205.
4. D-D’Orsi CJ, Mendelson EB, Ikeda DM, et al. Breast Imaging Reportingand Data System: ACR BI-RADS - Breast Imaging Atlas. Reston, VA,American College of Radiology, 2003.
5. Stavros AT, Thickman D, Rapp CL, et al. Solid breast nodules: use ofsonography to distinguish between benign and malignant lesions. Radi-ology 1995;196:123–134.
6. Horvath E, Majlis S, Rossi R, et al. An ultrasonogram reporting systemfor thyroid nodules stratifying cancer risk for clinical management.J Clin Endocrinol Metab 2009;94:1748–1751.
7. Blumberg D, Port JL, Weksler B, et al. Thymoma: a multivariateanalysis of factors predicting survival. Ann Thorac Surg 1995;60:908–913; discussion 914.
8. Masaoka A, Monden Y, Nakahara K, et al. Follow-up study of thymomaswith special reference to their clinical stages. Cancer 1981;48:2485–2492.
9. Casey EM, Kiel PJ, Loehrer PJ Sr. Clinical management of thymomapatients. Hematol Oncol Clin North Am 2008;22:457–473.
10. Suster S, Moran CA. Histologic classification of thymoma: the WorldHealth Organization and beyond. Hematol Oncol Clin North Am 2008;22:381–392.
11. Kim ES, Putnam JB, Komaki R, et al. Phase II study of a multidisciplinaryapproach with induction chemotherapy, followed by surgical resection,radiation therapy, and consolidation chemotherapy for unresectable malig-nant thymomas: final report. Lung Cancer 2004;44:369–379.
12. Elkiran ET, Abali H, Aksoy S, et al. Thymic epithelial neoplasia: a studyof 58 cases. Med Oncol 2007;24:197–201.
13. Falkson CB, Bezjak A, Darling G, et al. The management of thymoma: asystematic review and practice guideline. J Thorac Oncol 2009;4:911–919.
14. Girard N, Mornex F, Van Houtte P, et al. Thymoma: a focus on currenttherapeutic management. J Thorac Oncol 2009;4:119–126.
15. Myojin M, Choi NC, Wright CD, et al. Stage III thymoma: pattern offailure after surgery and postoperative radiotherapy and its implicationfor future study. Int J Radiat Oncol Biol Phys 2000;46:927–933.
16. Rea F, Sartori F, Loy M, et al. Chemotherapy and operation for invasivethymoma. J Thorac Cardiovasc Surg 1993;106:543–549.
17. Venuta F, Rendina EA, Longo F, et al. Long-term outcome aftermultimodality treatment for stage III thymic tumors. Ann Thorac Surg2003;76:1866–1872; discussion 1872.
18. Venuta F, Rendina EA, Pescarmona EO, et al. Multimodality treatmentof thymoma: a prospective study. Ann Thorac Surg 1997;64:1585–1591;discussion 1591–1592.
19. Marom EM. Imaging thymoma. J Thorac Oncol 2010;5:S296–S303.20. Marom EM, Milito MA, Moran CA, et al. Computed tomography
findings predicting invasiveness of thymoma. J Thorac Oncol 2011[Epub ahead of print].
21. Tomiyama N, Muller NL, Ellis SJ, et al. Invasive and noninvasivethymoma: distinctive CT features. J Comput Assist Tomogr 2001;25:388–393.
21a.Priola AM, Priola SM, Di Franco M, et al. Computed tomography andthymoma: distinctive findings in invasive and noninvasive thymoma andpredictive features of recurrence. Radiol Med 2010;115:1–21.
22. Jeong YJ, Lee KS, Kim J, et al. Does CT of thymic epithelial tumorsenable us to differentiate histologic subtypes and predict prognosis? AJRAm J Roentgenol 2004;183:283–289.
23. Tomiyama N, Johkoh T, Mihara N, et al. Using the World HealthOrganization Classification of thymic epithelial neoplasms to describeCT findings. AJR Am J Roentgenol 2002;179:881–886.
24. Sadohara J, Fujimoto K, Muller NL, et al. Thymic epithelial tumors:comparison of CT and MR imaging findings of low-risk thymomas, high-risk thymomas, and thymic carcinomas. Eur J Radiol 2006;60:70–79.
25. Duwe BV, Sterman DH, Musani AI. Tumors of the mediastinum. Chest2005;128:2893–2909.
26. Rusch VW, Asamura H, Watanabe H, et al. The IASLC lung cancerstaging project: a proposal for a new international lymph node map inthe forthcoming seventh edition of the TNM classification for lungcancer. J Thorac Oncol 2009;4:568–577.
27. Detterbeck FC, Moran CA, Huang J, et al. Which way is up? Policiesand procedures for surgeons and pathologists regarding resection spec-imens of thymic malignancy. J Thorac Oncol 2011;6:S1730–S1738.
28. Yano M, Sasaki H, Moriyama S, et al. Preservation of phrenic nerveinvolved by stage III thymoma. Ann Thorac Surg 2010;89:1612–1619.
29. Huang J, Detterbeck FC, Wang Z, et al. Standard outcome measures forthymic malignancies. J Thorac Oncol 2010;5:2017–2023.
30. Bott-Kothari T, Aron BS, Bejarano P. Malignant thymoma with metas-tases to the gastrointestinal tract and ovary: a case report and literaturereview. Am J Clin Oncol 2000;23:140–142.
FIGURE 11. Pleural and pulmonary metastasis. Contrast-enhanced chest computed tomography (CT) (lung window)demonstrates the thymoma (T) abutting the pulmonarytrunk (*). There is a pleural metastasis within the left majorfissure (PM), a left pleural effusion (e), and a pulmonarynodule (black arrow) surrounded by lung.
Journal of Thoracic Oncology • Volume 6, Number 7, Supplement 3, July 2011 Standard Report Terms for Chest CT
Copyright © 2011 by the International Association for the Study of Lung Cancer S1723