Embed Size (px)
Citation preview

One of the greatest challengesin clinical nursing education is pro-viding an orientation program thatmeets the needs of critical care nurseswith various backgrounds and levelsof experience within a relevant andstimulating format. Since the 1990s,a major shift has occurred within theculture of intensive care units (ICUs)to employ, orient, and mentor new
graduate nurses. Formerly, aftergraduation, the standard progres-sion for all critical care nurses wasat least 1 year of medical-surgicalexperience in a general care area.The gradual transition from medical-surgical nursing into the criticalcare environment that once existedhas changed in response to thedwindling supply of nurses in theworkforce. Concurrently, the popu-lation of patients in ICUs hasincreased, the severity of illness hasincreased, and the length of stay hasdecreased. Critical care educatorsare challenged to accommodategraduate nurses into ICUs whilemaintaining competence and ensur-ing the highest quality of care. Inthis article, we describe how wefaced that challenge and exceededall expectations.
Assessment of OrientationThe previous program of orien-
tation for critical care nurses atNorthwestern Memorial Hospital,
Chicago, Illinois, consisted of 2primary methods: classroom edu-cation and clinical instruction witha preceptor. Nurses were hired intoany of our 5 ICUs: medical, surgi-cal, cardiothoracic, neurosciences,and coronary care. The length oforientation ranged from 8 to 12weeks, depending on the nurse’snumber of years in nursing andlevel of experience.
Each new nurse was enrolled inthe Critical Care Course, a 31⁄2 daycourse that included lectures cover-ing a basic review of cardiac dys-rhythmias, pulmonary disorders,renal failure, interpretation ofblood gas analyses, and monitoringhemodynamic parameters. Beforeimplementation of our new criticalcare orientation program, mostICUs did not accept new graduates.All new nurses, regardless of experi-ence, were required to either attendthe classes offered every 2 monthsor test out of the classes via writtenexamination. Task competency was
http://ccn.aacnjournals.org CRITICALCARENURSE Vol 27, No. 6, DECEMBER 2007 37
Linda L. Morris, PhD, APN, CCNSPamela B. Pfeifer, RN, MS, CCNSRene Catalano, RN, MSRobert Fortney, RN, MS, CNRNEdith L. Hilton, DSN, PhD, APRN, BCJulia McLaughlin, RN, BSN, CCRNGreta Nelson, RN, MS, CNA, BCJanet Palamone, RN, MSN, APRN, BC, CCRN, CNRNRobb Rabito, BARebecca Wetzel, RN, BSNLindsay Goldstein, RN, BSN
Designing a ComprehensiveModel for Critical Care Orientation
StaffDevelopment
This article has been designated for CE credit. A closed-book, multiple-choice examination follows this article, which tests your knowledge of the following objectives:
1. Examine the role and challenges of criticalcare educators in integrating diverse levels ofnursing experience into an orientation model
2. Describe the educational and training needsof preceptors assisting with implementationof a critical care orientation program
3. Discover the benefits of a critical care modelof orientation on the unit, the staff, and thehospital
by AACN on January 24, 2019http://ccn.aacnjournals.org/Downloaded from

validated at the bedside by a precep-tor, who used a standardized check-list. Select units also providedclasses that focused on the units’specific population of patients. Writ-ten materials were made available tothe orientees, but no designatedtime outside of the orientees’assigned orientation hours forpatients’ care was given to reviewand discuss these materials.
Because of numerous concernsabout content and consistency ofclasses as well as the need to pro-mote critical-thinking skills in theorientees, the managers and staffeducators requested support fromNorthwestern Memorial Academy,the training and development sec-tion of the human resources depart-
ment. The academy, in turn, askedthe clinical nurse specialist (CNS)for the department of respiratorycare, who held dual certification asa critical care CNS and in continu-ing education and staff develop-ment, to assess the program andrecommend revisions.
Assessment of the CriticalCare Orientation Program
In our traditional approach,when a new nurse was hired, themanager of the ICU was discon-nected from the educational part ofthe orientation and focused on thedepartmental orientation from ahuman resource perspective. Thestaff educator took on the bulk ofthe role of determining compliance
with the mandatory hospital-wideeducational programs, the unit-based classes, online learning mod-ules, scheduling of orientation, andfollow-up. The preceptor’s role wasto “shepherd” the orientee thoughthe critical care orientation andensure completion of the orientee’scompetency-based skills lists.
A comprehensive assessment ofthe critical care orientation was per-formed during the last quarter of2003 and into the first quarter of2004. The CNS identified 3 primaryareas of inconsistencies in our pre-vious orientation program: instruc-tional reliability, teaching materials,and scheduling. We defined instruc-tional reliability as the ability of 2different instructors to teach an
38 CRITICALCARENURSE Vol 27, No. 6, DECEMBER 2007 http://ccn.aacnjournals.org
Linda L. Morris is the clinical nurse specialist for respiratory care at Northwestern Memorial Hospital and assistant professor of clinicalanesthesiology for the Feinberg School of Medicine at Northwestern University, Chicago, Illinois.Pamela B. Pfeifer has held several clinical and management positions, including staff nurse, assistant nurse manager, advanced practicenurse, and program director for the Critical Care Institute ( formerly education consultant). She is currently the interim manager with theNorthwestern Memorial Academy.Rene Catalano, with 11 years of experience in the development and implementation of education programs, is the staff educator in thecoronary care unit at Northwestern Memorial Hospital.Robert Fortney is the director of neurosciences nursing at Northwestern Memorial Hospital. As the former nurse manager of the neurospine intensive care unit, he recently expanded the unit from 12 beds to 23 beds and was intimately involved with the new orientationprogram for training all the newly hired nurses.Edith L. Hilton was an advanced practice nurse in the neurosciences at Northwestern Memorial Hospital. She has an extensive clinicalbackground in the neurosciences and rehabilitation; her research interests are chronic illness and disability.Julia McLaughlin was a staff educator in the medical intensive care unit at Northwestern Memorial Hospital and began DePaul-Evanston’snurse anesthetist program in the fall of 2006.Greta Nelson is the program administrator of home hospice at Northwestern Memorial Hospital and the former nurse manager of themedical intensive care unit. With 25 years of nursing practice, she has an extensive background in critical care and management, includ-ing experience as an educator, a manager, a director, and a consultant in healthcare.Janet Palamone is a staff educator in the neuro spine intensive care unit at Northwestern Memorial Hospital with 18 years of experiencein critical care.Robb Rabito is a senior project coordinator at the American College of Chest Physicians in Northbrook, Illinois. He has worked in educa-tion administration for 8 years.Rebecca Wetzel is currently the staff educator in the cardiac transplant unit at Northwestern Memorial Hospital, which expanded from11 to 23 beds, incorporating transplantation of solid organs.Lindsay Goldstein is a staff nurse in the neurosurgical intensive care unit at Rush University Medical Center in Chicago and a graduatestudent in the nurse practitioner program at Rush University College of Nursing.
Authors
Corresponding author: Linda L. Morris, PhD, APN, CCNS, Northwestern Memorial Hospital and Feinberg School of Medicine, Northwestern University, 251 E Huron St,Feinberg Pavilion, Ste 8-330, Chicago, IL 60611 (e-mail: [email protected]).
To purchase reprints, contact The InnoVision Group, 101 Columbia, Aliso Viejo, CA 92656. Phone, (800) 899-1712 or (949) 362-2050 (ext 532); fax, (949) 362-2049; e-mail, [email protected].
StaffDevelopment
by AACN on January 24, 2019http://ccn.aacnjournals.org/Downloaded from

identical session with equal results.In other words, participants whoattended identical sessions taughtby different instructors should havethe same understanding or grasp ofthe material. However, we foundthat equal results were not the case.Teaching materials consisted prima-rily of standardized PowerPoint pre-sentations, and sometimes outdatedwritten materials were used. Occa-sionally, instructors (usually thestaff educators) were not availableto teach scheduled classes becauseof unit staffing needs and classeshad to be canceled. Because classeswere offered bimonthly, they didnot always coincide with the start oforientation sessions; therefore, newnurses were inconsistently sched-uled for these classes.
In addition to inspecting theteaching materials used in the criticalcare classes, the CNS evaluated eachinstructor’s teaching skills and themethods used to elicit class partici-pation. She assessed each instructor’sability to present the information,noting whether he or she simplyread from notes or had a more activerole in interacting with the partici-pants. The CNS also taught sessionsof the Critical Care Course, whichallowed her to evaluate the teachingmaterials from the instructor’s per-spective. Next, the CNS developed4 separate assessment tools, oneeach for new orientees, preceptors,the unit-based staff educators, andthe nurse managers. These assess-ment tools were based on her expe-rience with the development andevaluation of previous orientationprograms. The tools consisted pri-marily of open-ended questionsand were distributed to each ofthe 4 groups.
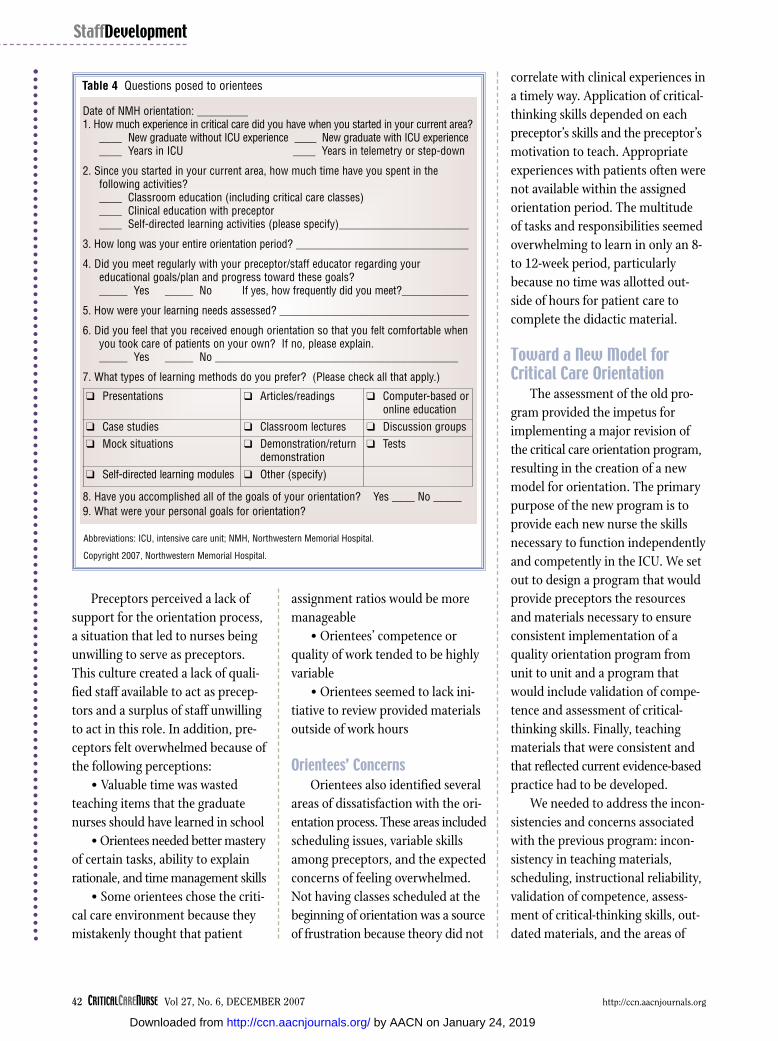
The staff educators, managers,and preceptors were asked about theirperceptions regarding the amount oftime spent preparing to orient newstaff, new nurses’ level of motivationto learn, barriers to the effectivenessof preceptors, resources to improvefunction of preceptors, preceptors’satisfaction, helpfulness of the cur-rent critical care orientation classesin introducing critical care concepts,level of satisfaction with the criticalcare orientation program itself, andsuggestions for improvement. Inaddition, recent orientees were askedabout how much time they spentin classroom education, in clinicalorientation with a preceptor, and inself-directed activities. They werealso asked about how their learningneeds were assessed, whether theymet regularly with the staff educatorsto discuss goals, the orientees’ pre-ferred learning methods, andwhether the orientees accomplishedtheir goals of orientation. Tables 1
through 4 list the specific questionsasked of each group. Many of thesequestions were duplicated through-out the groups to provide a compre-hensive picture of the current stateof the orientation process.
To identify repetitive themes, theCNS analyzed the results of thesequestionnaires and the course evalu-ations of the previous year’s criticalcare orientation program. A proposalwas submitted in early 2004 withrecommendations for improvement.The areas to be addressed includedthe previously discussed inconsis-tencies in teaching methods, sched-uling, and education.
Staff Educators’ ConcernsResults from the staff educators
indicated inconsistencies in the waythe program was implemented fromICU to ICU. In some units, orienteeswere allowed to test out of classes ifthey had critical care experience; inother units, they were required to
http://ccn.aacnjournals.org CRITICALCARENURSE Vol 27, No. 6, DECEMBER 2007 39
Table 1 Questions posed to staff educators
1. How many preceptors are on your unit?
2. How often are they expected to be a preceptor?
3. On the average, how much time do they spend in preparation for orientation (eg,developing teaching materials, searching Web sites)?
4. What is the experience level of most of your orientees (new graduate, experiencednon–critical care, experienced critical care)?
5. How motivated to learn are the new employees?
6. What barriers or obstacles hinder the preceptor's ability to function effectively?
7. How helpful is the critical care orientation course in introducing critical care concepts?
8. Do your preceptors seem satisfied with the precepting experience? Why or why not?
9. What other resources would help them function as effective preceptors?
10. On a scale of 0-10, how satisfied are you with the clinical orientation process? (0 = not at all satisfied; 10 = totally satisfied)
11. On a scale of 0-10, how satisfied are you with the critical care orientation course as part of the orientation process? (0 = not at all satisfied; 10 = totally satisfied)
12. If the current critical care orientation course is revised, what suggestions do you have for improvement?
Copyright 2007, Northwestern Memorial Hospital.
by AACN on January 24, 2019http://ccn.aacnjournals.org/Downloaded from

attend all classes regardless of theirexperience level. In addition, the cri-teria for competence varied fromunit to unit. For example, in one unit,competence was assumed once anorientee had achieved an acceptable
score on the posttest, whereas inother units, skills checklists wereused, but not consistently.
Staff educators were also con-cerned that orientees sometimescompleted their orientation period
needing more time to apply theinformation in the clinical setting.In addition, no formal method wasavailable to determine readiness topractice independently in an ICUwithout direct supervision.
The CNS also noted missedopportunities to assess the critical-thinking skills of the orientees andinconsistency in the way didacticcontent was taught. Experiencedclassroom instructors knew how tofacilitate discussion on a topic toensure that the material was under-stood; inexperienced instructorswere unable to do so.
Preceptors’ ConcernsResults from the preceptors’
assessments revealed several con-cerns. These themes included vari-ability or inconsistencies in the skillsof the preceptors and negative per-ceptions of the precepting experience.Preceptors were selected on the basisof “who did it last,” rather than onthe basis of which person was themost appropriate. Selection was alsobased on schedule availability, yearsof work on the unit, and previousexperience as a preceptor.
Preceptors’ teaching skills tendedto be highly variable. The preceptorcurriculum, a course that is suggestedbut not mandatory for preceptors,consists of six 2-hour sessions offeredin a 3-month period. The classesinclude assessment and feedback,effective communication, criticalthinking, new learner issues, plan-ning instruction, and the challeng-ing learner. Although the in-housepreceptor curriculum includes dis-cussion of instructional resources, notall preceptors attended these sessions,so some preceptors had more infor-mation on teaching than others did.
40 CRITICALCARENURSE Vol 27, No. 6, DECEMBER 2007 http://ccn.aacnjournals.org
StaffDevelopment
Table 2 Questions posed to managers
1. How many preceptors are in your unit?
2. How often are they expected to be preceptors?
3. On the average, how much time do they spend in preparation for orientation (eg, developing teaching materials, searching Web sites)?
4. What is the experience level of most of your orientees (new graduate, experienced non–critical care, experienced critical care)?
5. How motivated to learn are the new employees?
6. What barriers or obstacles hinder the preceptor's ability to function effectively?
7. How helpful is the critical care orientation course in introducing critical care concepts?
8. Do your preceptors seem satisfied with the precepting experience? Why or why not?
9. What other resources would help them function as effective preceptors?
10. On a scale of 0-10, how satisfied are you with the clinical orientation process? (0 = not at all satisfied; 10 = totally satisfied)
11. On a scale of 0-10, how satisfied are you with the critical care orientation course as part of the orientation process? (0 = not at all satisfied; 10 = totally satisfied)
12. If the current critical care orientation course is revised, what suggestions do you have for improvement?
Copyright 2007, Northwestern Memorial Hospital.
Table 3 Questions posed to preceptors
1. How long have you been a preceptor?
2. How often are you asked to be a preceptor?
3. On the average, how much time do you spend in preparation for orientation (eg, developing teaching materials, searching Web sites)?
4. What is the experience level of most of your orientees (new graduate, experienced non–critical care, experienced critical care)?
5. How motivated to learn are the new employees?
6. What barriers or obstacles hinder your ability to function as an effective preceptor?
7. How helpful is the critical care orientation course in introducing critical care concepts?
8. Do you enjoy being a preceptor? Why or why not?
9. What other resources would help you function as an effective preceptor?
10. On a scale of 0-10, how satisfied are you with your experience as a preceptor? (0 = not at all satisfied; 10 = totally satisfied)
11. On a scale of 0-10, how satisfied are you with the critical care orientation course as part of the orientation process? (0 = not at all satisfied; 10 = totally satisfied)
12. If the current critical care orientation course is revised, what suggestions do you have for improvement?
Copyright 2007, Northwestern Memorial Hospital.
by AACN on January 24, 2019http://ccn.aacnjournals.org/Downloaded from
Preceptors perceived a lack ofsupport for the orientation process,a situation that led to nurses beingunwilling to serve as preceptors.This culture created a lack of quali-fied staff available to act as precep-tors and a surplus of staff unwillingto act in this role. In addition, pre-ceptors felt overwhelmed because ofthe following perceptions:
• Valuable time was wastedteaching items that the graduatenurses should have learned in school
• Orientees needed better masteryof certain tasks, ability to explainrationale, and time management skills
• Some orientees chose the criti-cal care environment because theymistakenly thought that patient
assignment ratios would be moremanageable
• Orientees’ competence orquality of work tended to be highlyvariable
• Orientees seemed to lack ini-tiative to review provided materialsoutside of work hours
Orientees’ ConcernsOrientees also identified several
areas of dissatisfaction with the ori-entation process. These areas includedscheduling issues, variable skillsamong preceptors, and the expectedconcerns of feeling overwhelmed.Not having classes scheduled at thebeginning of orientation was a sourceof frustration because theory did not
correlate with clinical experiences ina timely way. Application of critical-thinking skills depended on eachpreceptor’s skills and the preceptor’smotivation to teach. Appropriateexperiences with patients often werenot available within the assignedorientation period. The multitudeof tasks and responsibilities seemedoverwhelming to learn in only an 8-to 12-week period, particularlybecause no time was allotted out-side of hours for patient care tocomplete the didactic material.
Toward a New Model for Critical Care Orientation
The assessment of the old pro-gram provided the impetus forimplementing a major revision ofthe critical care orientation program,resulting in the creation of a newmodel for orientation. The primarypurpose of the new program is toprovide each new nurse the skillsnecessary to function independentlyand competently in the ICU. We setout to design a program that wouldprovide preceptors the resourcesand materials necessary to ensureconsistent implementation of aquality orientation program fromunit to unit and a program thatwould include validation of compe-tence and assessment of critical-thinking skills. Finally, teachingmaterials that were consistent andthat reflected current evidence-basedpractice had to be developed.
We needed to address the incon-sistencies and concerns associatedwith the previous program: incon-sistency in teaching materials,scheduling, instructional reliability,validation of competence, assess-ment of critical-thinking skills, out-dated materials, and the areas of
42 CRITICALCARENURSE Vol 27, No. 6, DECEMBER 2007 http://ccn.aacnjournals.org
Table 4 Questions posed to orientees
Date of NMH orientation: _________1. How much experience in critical care did you have when you started in your current area?
____ New graduate without ICU experience ____ New graduate with ICU experience____ Years in ICU ____ Years in telemetry or step-down
2. Since you started in your current area, how much time have you spent in the following activities?____ Classroom education (including critical care classes)____ Clinical education with preceptor____ Self-directed learning activities (please specify)_______________________
3. How long was your entire orientation period? _______________________________
4. Did you meet regularly with your preceptor/staff educator regarding your educational goals/plan and progress toward these goals?_____ Yes _____ No If yes, how frequently did you meet?____________
5. How were your learning needs assessed? __________________________________
6. Did you feel that you received enough orientation so that you felt comfortable when you took care of patients on your own? If no, please explain._____ Yes _____ No ___________________________________________
7. What types of learning methods do you prefer? (Please check all that apply.)
8. Have you accomplished all of the goals of your orientation? Yes ____ No _____9. What were your personal goals for orientation?
� Presentations � Articles/readings � Computer-based or online education
� Case studies � Classroom lectures � Discussion groups� Mock situations � Demonstration/return
demonstration� Tests
� Self-directed learning modules � Other (specify)
Abbreviations: ICU, intensive care unit; NMH, Northwestern Memorial Hospital.
Copyright 2007, Northwestern Memorial Hospital.
StaffDevelopment
by AACN on January 24, 2019http://ccn.aacnjournals.org/Downloaded from

dissatisfaction among the preceptorsand orientees. This model also had toaddress the learning needs of nurseswith different levels of experience.
A new model of critical care ori-entation was created that draws onBenner’s “novice to expert” model.1
This model has 5 levels of mastery:novice, advanced beginner, compe-tent, proficient, and expert. Withinthis framework are 3 aspects of skillacquisition that we used to guide thecritical care orientation curriculumand help nurses adjust to their rolein the ICU1:
1. Movement from reliance onabstract principles to use of pastexperiences
2. Change in the learner’s per-ception of the situation in terms ofequally relevant bits of informationto a complete whole in which onlycertain parts are relevant
3. Passage from detached observerto involved performer
For new ICU nurses to gain asense of confidence and demon-strate competence in complex nurs-ing skills, the program must includetime for preparation, resources richin critical care concepts, and prac-tice in real-life or simulated situa-tions. These characteristics give newICU nurses the best opportunities topractice independently.1 The foun-dation of our program provides flex-ibility for nurses entering the ICUregardless of their previous knowl-edge or performance level. In sup-porting the foundation of ourprogram, we provided preceptorswith the necessary resources andmaterials to ensure that a qualityorientation program is implementedconsistently from unit to unit.
Our new model builds on thelearner’s experiences, provides a
variety of learning methods, uses task-oriented problem-solving approachesto learning, and uses self-directedlearning as an option when advanta-geous. These methods encompassBenner’s model and the 3 aspects ofskill performance, therefore encour-aging nurses to advance to a higherlevel of clinical aptitude.
The new model of critical careorientation was developed first(Figure 1). This model has an over-arching umbrella that representsthe use of a consistent approach toorientation from unit to unit. Ourprimary theme of critical thinking
infused the entire program as itchanged from one of traditionalpedagogy (teacher-centered meth-ods) to andragogy (adult-centeredlearning).2-4 With adult-learning theory as a framework,5-8 the newmodel builds on a learner’s experi-ences; provides a variety of learningmethods; uses task-oriented, problem-solving approaches tolearning; and uses self-directed learn-ing as an option when possible. Thismodel offers constant opportunityfor assessment and evaluation of alearner’s ability to apply the knowl-edge in real and simulated situations.
http://ccn.aacnjournals.org CRITICALCARENURSE Vol 27, No. 6, DECEMBER 2007 43
Figure 1 New model of critical care orientation.
Abbreviations: CCO, critical care orientation; ECCO, Essentials of Critical Care Orientation; PACEP, Pulmonary Artery Catheter Education Project.
Copyright 2007, Northwestern Memorial Hospital.
Testing/retesting
Demonstration/returndemonstration
Knowledge and skill
COMPETENCY
High-fidelitysimulation
Casestudies
Screening for experience
Learning needs assessment
New model of critical care orientation
CRITICAL
THINKING
CRITICAL
THINKING
Online learning
• PACEP
• ECCO
Clinical experience
with preceptor
Classroom
CCO, neuro, trauma Videos Articles
Games
Quizzes
Mockevents
by AACN on January 24, 2019http://ccn.aacnjournals.org/Downloaded from

Our challenge has been to providestimulating learning experiences for3 distinct groups: experienced criti-cal care nurses, experienced non–critical care nurses, and graduatenurses. Relevant learning opportu-nities were planned to meet individ-ual needs. As a result of our efforts,the traditional learning methods oflecture-based classes in combina-tion with assignment to a preceptorhave been replaced with a variety oflearning methods.
Learning MethodsDepending on each nurse’s expe-
rience, learning needs are identifiedin different ways (see the section“Implementation of the Model”). Avariety of learning methods are used,depending on the results of theseinitial assessments. The primarylearning methods used in the newapproach include online learning,case studies, a human simulator, andclinical time with a preceptor. Thestaff educator and preceptor deter-mine what other learning methodsare appropriate for each orientee.These other methods can includeservice-based classroom lectures(eg, the neurosciences orientationclasses for the nurses working in theneurosciences ICU), quizzes, games,videos, mock events, articles fromcritical care journals, and demon-stration/return demonstration.
Online MethodsIn our new model, most of the
traditional classroom lectures havebeen replaced with the Web-basedlearning programs Essentials ofCritical Care Orientation (ECCO)9
and Pulmonary Artery Catheter Edu-cation Project (PACEP).10 ECCO is acomprehensive Web-based learning
program developed by the AmericanAssociation of Critical-Care Nursesand consists of 8 system-based modules: cardiovascular, pulmonary,neurological, renal, endocrine, hema-tological, gastrointestinal, and multi-system. Each module contains a basicreview of anatomy and physiology,assessment, monitoring, diagnosticor invasive procedures, and specificdisorders relevant to that body sys-tem. A variety of media formats areused in ECCO, including text, audio,video, animation, and tests. The pro-gram also includes managementoversight ability, in which approvedindividuals are able to check theprogress of the staff, checking thenumber of modules completed, aver-age scores on tests, and all aspects oforientees’ progress in completion ofthe modules.
PACEP was designed to providea free Web-based state-of-the-arteducational program on monitoringhemodynamic parameters and usingpulmonary artery catheters. PACEPwas developed in collaboration withseveral professional societies: theAmerican Association of Critical-CareNurses, the American Association ofNurse Anesthetists; the AmericanCollege of Chest Physicians; theAmerican Society of Anesthesiolo-gists; the American Thoracic Society;the National Heart, Lung, and BloodInstitute; the Society of Cardiovas-cular Anesthesiologists; and theSociety of Critical Care Medicine.Topics are divided into 2 levels ofdifficulty; each topic includes physi-ological concepts, interpretation ofdata, waveform analysis, and techni-cal aspects of monitoring hemody-namic parameters. Content includeseffects of medications on hemody-namic values, recognizing trends in
data, and identifying abnormalhemodynamic profiles such as shock,heart failure, and tamponade.
When a nurse completes bothECCO and PACEP, he or she receives64 contact hours of continuing edu-cation credit. Web-based learningstrategies provide current content ina consistent manner that can bereviewed at scheduled times or atthe convenience of the user. Thisarrangement helped us correct oneof our concerns, instructional relia-bility; however, we also needed amethod to assess how each orienteeapplies this information to specificsituations. We assess application ofthe theory learned by reviewing casestudies and simulations of real-lifeexperience with the human simulator,which mimics real-life experiences.
Case StudiesCase studies are excellent meth-
ods for assessing critical-thinkingability.11 This type of assessment isespecially important when assessingthe competence of any new nurse.Case studies contain a patient situa-tion, including assessment data, aninherent problem, results, andimplications. After being presentedwith a situation, the participantbegins by relaying his or her con-cerns about potential problems and“talks it through” with the guidanceof a leader. The leader, usually astaff educator or an advanced prac-tice nurse, allows the participant to“care for” a patient aloud in the par-ticipant’s thoughts, but gives theparticipant more information alongthe way. At the end of the exercise,the leader promotes discussion toevaluate the way the participant caredfor the patient, including strengthsand weaknesses. This feedback allows
44 CRITICALCARENURSE Vol 27, No. 6, DECEMBER 2007 http://ccn.aacnjournals.org
StaffDevelopment
by AACN on January 24, 2019http://ccn.aacnjournals.org/Downloaded from

participants to learn in a nonthreat-ening manner.
The case studies were developedby critical care advanced practicenurses and staff educators at North-western Memorial Hospital to meetthe learning needs of orientees atincreasing levels of complexity inorder to challenge nurses at all levelsof experience. Each case study wasdeveloped to illustrate specificteaching points. Table 5 is an exam-ple of a case study that can be usedindependently by an orientee (blank),and Table 6 is a case study that canbe used by a preceptor with an ori-entee (with answers). The latterexample includes answers so thatthe preceptor can coach the orienteetoward the correct answers. The ori-entee is continuously evaluated onhis or her ability to discuss theappropriate care within the contextof these case studies.
Human SimulatorMany of the case studies are
presented in a real-time learningenvironment. This method allowsevaluation of critical thinking byplacing the orientees in a more life-like learning environment throughthe use of a computerized humansimulator (Medical Education Tech-nologies, Inc, Sarasota, Florida). Thissimulator, nicknamed “Cosmo,” isowned by the department of anes-thesiology and has been an effectivetool in the education of anesthesiaresidents, who are expected to man-age actual patients safely with a verylow margin of error. This methodallows orientees to learn, and simul-taneously the instructor can evaluatethe orientees’ response to real-life,real-time patient situations in a risk-free environment. The simulator can
be set up to emulate an operatingroom, an ICU, or a delivery room.
Scenarios were developed bycritical care advanced practice nursesand staff educators so that an orien-tee gains exposure to numerousemergency situations that can occurin the ICU. Simulator scenariosinclude a dislodged tube in a newversus an older tracheostomy, admin-istration of medication to and syn-chronized cardioversion of a patientwith supraventricular tachycardia,symptomatic bradycardia with exter-nal pacing, symptomatic andasymptomatic ventricular tachycar-dia, resuscitation of a patient fromventricular fibrillation and pulselesselectrical activity, and inability toresuscitate a patient from asystole.
Learning with simulator tech-nology is beneficial because the
technology can be used to do thefollowing12:
• Provide real-life critical carescenarios
• Allow assessment of perform-ance in a risk-free environment
• Provide immediate feedbackon performance evaluation
• Provide an opportunity toevaluate critical thinking in action
• Allow videotaping with feed-back on performance
• Offer the opportunity to “stoptime” to provide a teachable momentduring a scenario
The simulator promotes critical-thinking skills in a real-time envi-ronment and assists educators inidentifying individual qualities suchas motivation and readiness to learnas well as cognitive processes. Theresult of critical thinking is decision
46 CRITICALCARENURSE Vol 27, No. 6, DECEMBER 2007 http://ccn.aacnjournals.org
Table 5 Example of case study, participant version (blank)
Cardiac Case Studies A
A 69-year-old female presented to the ED with c/o severe, substernal chest pain. BP 150/96, HR = 100 irregularly irregular. PMH: dyslipidemia; hypertension (controlled onenalapril); osteoporosis w/ multiple vertebral fractures; GERD. Initial ECG: ST elevationin anterior leads. Patient was taken immediately to cath lab where she underwent emer-gent cardiac catheterization and PTCA w/ stent. After the procedure she was taken tothe CCU, where her stay was unremarkable with no further c/o CP. She was dis-charged directly from the CCU on the morning of Day 3.
1. What coronary artery was probably stented?
2. What medications does the patient receive post-intracoronary stent?
3. What are nursing routines/orders that must be performed for the post-cath patientto prevent complications?
4. Name four (cardioprotective) drugs that this patient will probably be dischargedon and their importance.
5. What information/patient education information would you review with this patientand document on MPET prior to discharge?
6. Although this patient has been on Coumadin [warfarin] for a while because of heratrial fib, what should you review with her about this drug before she goes home?
Abbreviations: BP, blood pressure; cath, catheterization; CCU, coronary care unit; c/o, complaints of; CP,chest pain; ECG, electrocardiogram; ED, emergency department; fib, fibrillation; GERD, gastroesophagealreflux disease; HR, heart rate; MPET, Multidisciplinary Patient Education Tool; PMH, prior medical history;PTCA, percutaneous transluminal coronary angiography; w/, with.
Copyright 2007, Northwestern Memorial Hospital.
StaffDevelopment
by AACN on January 24, 2019http://ccn.aacnjournals.org/Downloaded from

making. This type of critical think-ing is called “thinking in action” or“reasoning in action.”13
These methods also supportBenner’s 3 aspects of skill perform-ance. Our method of using casestudies, computerized simulations,and other learning tools help learn-ers move from conceptual principlesto true-life experiences. These expe-riences help change the orientees’perception that each aspect of apatient’s care is not about individualentities, but about the patient as awhole with significant findings. Alearner passes from a “detachedobserver to involved performer” by
practicing with a clinical preceptorand compiling pertinent informationfor problem solving.1 Our new modeloffers constant opportunity forassessment and evaluation of an ori-entee’s ability to apply the knowledgein real and simulated situations.
Implementation of the ModelExperienced Versus InexperiencedCritical Care Nurses
Figure 2 illustrates the 3 separateorientation pathways for critical carenurses with different experience lev-els: experienced critical care nurses,experienced nurses without criticalcare experience, and graduate nurses.
All nurses undergo a general nursingorientation during their first week.Table 7 provides information on thecontent given to all nurses duringthe first week of orientation.
Experienced Critical Care Nurses.At the start of orientation, each expe-rienced critical care nurse is screenedby using the Basic Knowledge Assess-ment Tool (BKAT, Version 7.0).14
The BKAT is a well-designed com-prehensive test that covers a widevariety of critical care topics: cardio-vascular, pulmonary, neurology, mon-itoring catheters, endocrine, renal,gastrointestinal/parenteral, and
http://ccn.aacnjournals.org CRITICALCARENURSE Vol 27, No. 6, DECEMBER 2007 47
Table 6 Example of case study, facilitator version (answers)
Cardiac Case Studies A: STEMI (anterior)
A 69-year-old female presented to the ED with c/o severe, substernal chest pain. BP 150/96, HR = 100 irregularly irregular. PMH: dys-lipidemia; hypertension (controlled on enalapril); osteoporosis w/ multiple vertebral fractures; GERD. Initial ECG: ST elevation in ante-rior leads. Patient was taken immediately to cath lab, where she underwent emergent cardiac catheterization and PTCA with stent. Postprocedure she was taken to the CCU, where her stay was unremarkable with no further c/o CP. She was discharged directly from theCCU on the morning of Day 3.
1. What coronary artery was probably stented?(probably LAD)
2. What medications does the patient receive post-intracoronary stent?(Plavix [clopidogrel bisulfate], Reopro [abciximab], non-enteric coated ASA)
3. What are nursing routines/orders that must be performed for the post-cath pt. to prevent complications?
Check pulses (DP/PT), VS—per cath lab orders (how do you assess and document pulse checks)Prevent vascular complication at sheath site: sheet tuck to keep leg straight, on bedrest per order, don’t cough, etc.Hydrate, monitor urine outputTeach pt about complications, when to call RN/MD (if going home soon), importance of medicationsIf in unit that pulls sheaths, can discuss technique
4. Name four (cardioprotective) drugs that this patient will probably be discharged on and their importance.(ASA, BB, ACEI, statin)
5. What information/patient education information would you review with this patient and document on MPET prior to discharge?(see if patient has ACS packet from CCU)
6. Although this patient has been on Coumadin [warfarin] for a while because of her atrial fib, what should you review with her about this drug before she goes home?Drug interaction; instruct her to tell all new MDs, health care practitioners she is on CoumadinConsistent dietLimit alcohol intakeKnow frequency for checking INR (make sure they know terminology)Prevent against falls, trauma—seek medical assistance with injury, bleeding
Abbreviations: ACEI, angiotensin-converting enzyme inhibitors; ACS, acute coronary syndrome; ASA, acetylsalicylic acid; BB, β-blockers; BP, blood pressure; cath,catheterization; CCU, coronary care unit; c/o, complaints of; CP, chest pain; DP, dorsalis pedis; ECG, electrocardiogram; ED, emergency department; fib, fibrillation;GERD, gastroesophageal reflux disease; HR, heart rate; INR, international normalized ratio; LAD, left anterior descending artery; MD, physician; MPET, MultidisciplinaryPatient Education Tool; PMH, prior medical history; pt, patient; PT, posterior tibial; PTCA, percutaneous transluminal coronary angiography; RN, registered nurse; VS,vital signs; w/, with.
Copyright 2007, Northwestern Memorial Hospital.
by AACN on January 24, 2019http://ccn.aacnjournals.org/Downloaded from
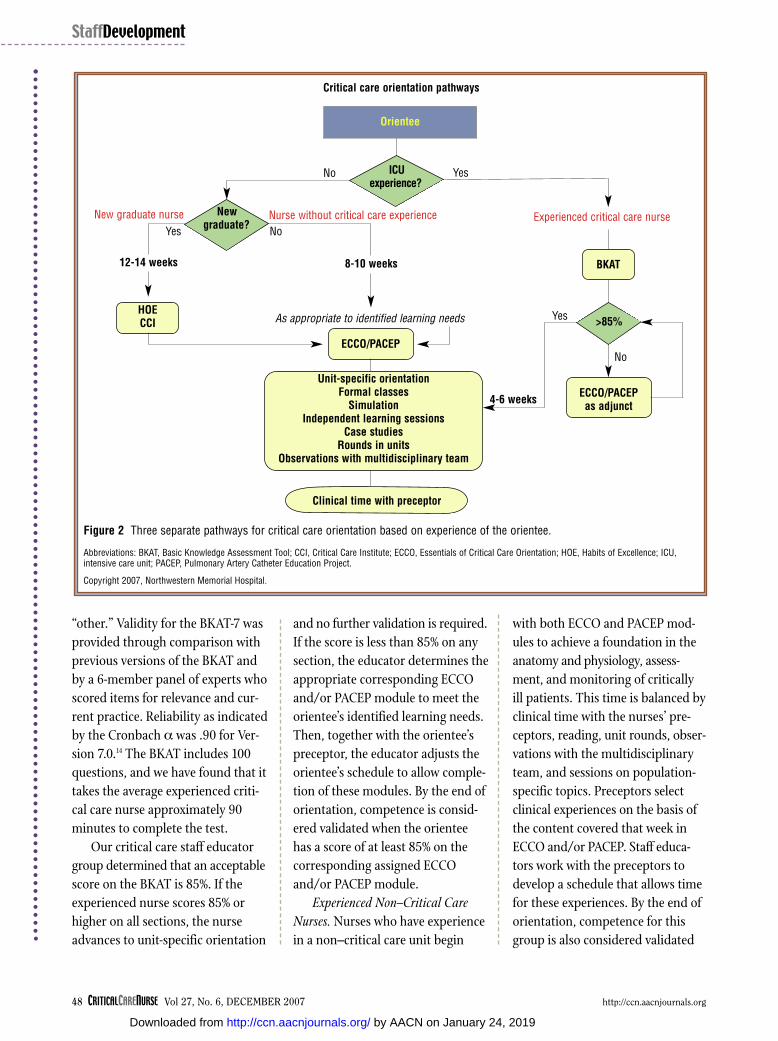
“other.” Validity for the BKAT-7 wasprovided through comparison withprevious versions of the BKAT andby a 6-member panel of experts whoscored items for relevance and cur-rent practice. Reliability as indicatedby the Cronbach α was .90 for Ver-sion 7.0.14 The BKAT includes 100questions, and we have found that ittakes the average experienced criti-cal care nurse approximately 90minutes to complete the test.
Our critical care staff educatorgroup determined that an acceptablescore on the BKAT is 85%. If theexperienced nurse scores 85% orhigher on all sections, the nurseadvances to unit-specific orientation
and no further validation is required.If the score is less than 85% on anysection, the educator determines theappropriate corresponding ECCOand/or PACEP module to meet theorientee’s identified learning needs.Then, together with the orientee’spreceptor, the educator adjusts theorientee’s schedule to allow comple-tion of these modules. By the end oforientation, competence is consid-ered validated when the orienteehas a score of at least 85% on thecorresponding assigned ECCOand/or PACEP module.
Experienced Non–Critical CareNurses. Nurses who have experiencein a non–critical care unit begin
with both ECCO and PACEP mod-ules to achieve a foundation in theanatomy and physiology, assess-ment, and monitoring of criticallyill patients. This time is balanced byclinical time with the nurses’ pre-ceptors, reading, unit rounds, obser-vations with the multidisciplinaryteam, and sessions on population-specific topics. Preceptors selectclinical experiences on the basis ofthe content covered that week inECCO and/or PACEP. Staff educa-tors work with the preceptors todevelop a schedule that allows timefor these experiences. By the end oforientation, competence for thisgroup is also considered validated
48 CRITICALCARENURSE Vol 27, No. 6, DECEMBER 2007 http://ccn.aacnjournals.org
ICUexperience?
Orientee
HOECCI
ECCO/PACEP
ECCO/PACEPas adjunct
Critical care orientation pathways
4-6 weeks
No
New graduate nurse Nurse without critical care experience Experienced critical care nurseNo
No
Yes
Yes
YesAs appropriate to identified learning needs
12-14 weeks 8-10 weeks BKAT
>85%
Unit-specific orientationFormal classes
SimulationIndependent learning sessions
Case studiesRounds in units
Observations with multidisciplinary team
Figure 2 Three separate pathways for critical care orientation based on experience of the orientee.
Abbreviations: BKAT, Basic Knowledge Assessment Tool; CCI, Critical Care Institute; ECCO, Essentials of Critical Care Orientation; HOE, Habits of Excellence; ICU,intensive care unit; PACEP, Pulmonary Artery Catheter Education Project.
Copyright 2007, Northwestern Memorial Hospital.
Clinical time with preceptor
New graduate?
StaffDevelopment
by AACN on January 24, 2019http://ccn.aacnjournals.org/Downloaded from

when the orientee has a score of atleast 85% on all ECCO and PACEPmodules.
New Graduate Nurses. Expansionof several of our ICU areas promptedthe units’ managers to consider hir-ing graduate nurses, something thathad rarely been done at this institu-tion. These managers approachedthe Northwestern Memorial Acad-emy to develop a program to sup-port these hiring efforts. Afterseveral discussions with the direc-tors, managers, and staff educatorsfrom the ICUs, an 8-week programcalled the Critical Care Institute (CCI)was designed to facilitate the inte-gration and socialization of graduatenurses into the critical care environ-ment. Goals of this program are toensure basic nursing skill competen-cies and to support the preceptors inproviding critical care informationso that the graduate nurses are ableto function safely when placed in a
critical care envi-ronment.
Critical CareInstitute
The struc-ture of the CCIis shown in Fig-ure 3; it consistsin a series ofinterrelatedmodules, eachwith a focus ona particularbody system.The modules,based on thelessons foundin ECCO andPACEP, areintroduced in
the program according to theincreasing complexity of that bodysystem as seen in critically illpatients. Each module builds on theknowledge and skills learned in theprevious modules; the final moduleis a culmination of all modules thataddresses a patient with multisys-tem failure. The goal of the CCI is todevelop a graduate nurse into acompetent advanced beginner.
Integrated within the first 2weeks of the CCI is the Habits ofExcellence program: 5 days of gen-eral hospital nursing orientation forall graduate nurses designed specifi-cally to address general issues ofpatient care. The Habits of Excel-lence program allows all of the hos-pital’s graduate nurses to reviewand safely demonstrate the general
50 CRITICALCARENURSE Vol 27, No. 6, DECEMBER 2007 http://ccn.aacnjournals.org
Figure 3 Structure of the Critical Care Institute.
Abbreviations: ECG, electrocardiography; PACEP, Pulmonary Artery Catheter Education Project.
Copyright 2007, Northwestern Memorial Hospital.
Module 2:Cardiovascular
Module 3:Hemodynamics
PACEP
Module 4:Pulmonary
Module 5:Neurology
Module 6:Renal
Module 7:Gastrointestinal
Module 8:Endocrine
Module 9:Hematology
Module 10:Multisystem
Module 1:ECG basics
Table 7 Content reviewed during the first week of hospitalorientation for all new nurses (Professional Clinical Orientation)
Nursing Orientation Week 1
Day 1
Day 2
Day 3
Day 4
Day 5
General hospital orientation for all new employees
EquipmentResource centerComputerized documentation
Infection controlSafetyRisk managementLifting and movingEmergency responseBlood administrationPharmacyRespiratory therapyCommunicationOrgan and tissue donation
Intravenous therapyPhlebotomyCentral venous access devices
Cardiopulmonary resuscitation (if needed)Unit-specific orientation
Copyright 2007, Northwestern Memorial Hospital.
StaffDevelopment
by AACN on January 24, 2019http://ccn.aacnjournals.org/Downloaded from

skills covered in nursing orientationunder the guidance of a clinicalinstructor, who is either one of thestaff educators or an experiencedstaff nurse.
Clinical instructors demonstrateand review skills in a simulated envi-ronment during the morning. In theafternoon, they take a small group ofgraduate nurses out to various patientcare areas, enabling practical applica-tion of the content presented in themorning session. Traditional unitboundaries are disregarded in order toprovide maximal exposure to complexexamples of altered physiology. Man-agers have reported that graduatenurses who have been through thisprocess demonstrate increased clinicalcompetence, confidence, and prob-lem-solving skills to then start the CCI.
During this time, and continuingfor the next 8 weeks, the graduate
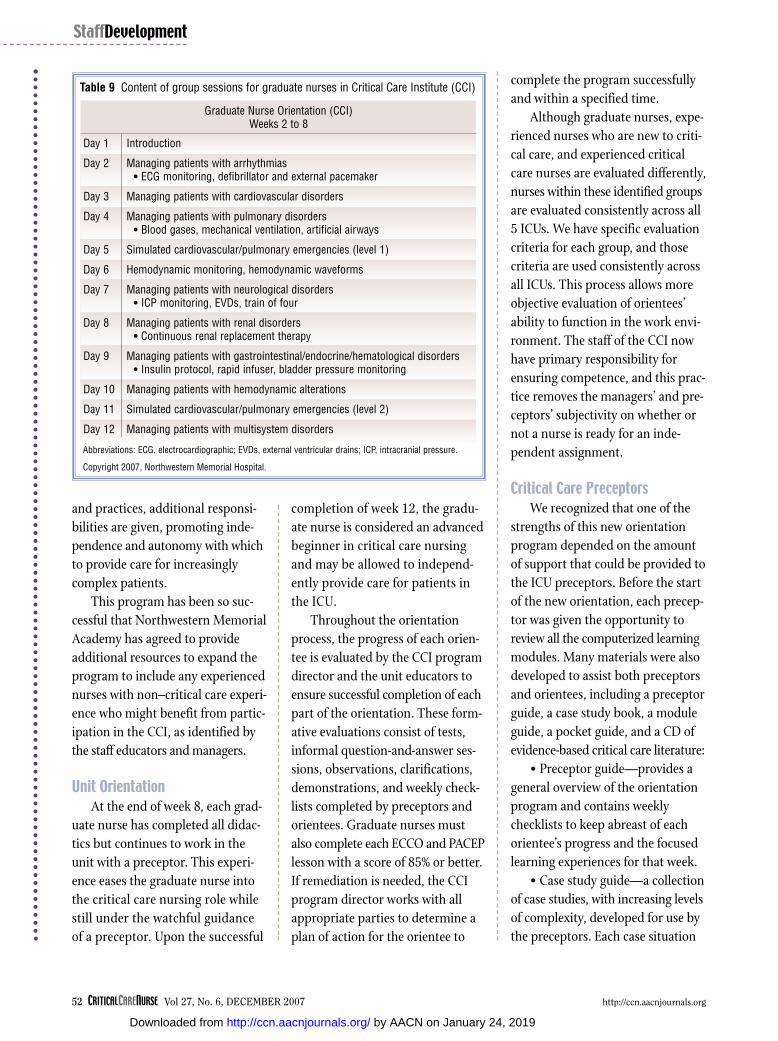
nurses in the ICU begin to learncritical care nursing with the ECCOand PACEP modules. A sampleschedule is shown in Table 8. Eachweek the new nurses attend at least1 group session focused on applica-tion of the critical care informationreviewed in the corresponding mod-ule. This process is also integratedwith appropriate patient assign-ments when the orientees are in theunit with the preceptors. Detailedschedules are developed by the CCIdirector and the staff educators sothat each graduate nurse’s time isdivided between unit-based activi-ties, completion of assigned onlinemodules, clinical group sessions,and corresponding time in the unitwith the preceptor.
During the clinical group sessions,critical care concepts (eg, in the res-piratory module, managing a patient
with an artificial airway) are illus-trated by a variety of methods,including case study discussionswith expert nurses, simulateddemonstrations, and teachingrounds in any critical care unit.Table 9 lists the content covered inthe group sessions. When a newnurse graduate is scheduled towork in a unit, immediate applica-tion of knowledge and skills learnedin the critical care group sessions isensured by the nurse’s preceptor,who chooses patient assignmentsthat correlate with the conceptsreviewed. Each week is built toincorporate concepts from the pre-vious weeks so that the orienteegradually assimilates to the ICUenvironment through experienceswith the preceptor, colleagues, andpatients. As the graduate nursedemonstrates mastery of concepts
http://ccn.aacnjournals.org CRITICALCARENURSE Vol 27, No. 6, DECEMBER 2007 51
Table 8 Critical care orientation schedule for new graduate nurses
Monday Tuesday Wednesday Thursday Friday
2
General employee orientation
3
Professional ClinicalOrientation
4
Professional ClinicalOrientation
5
Professional ClinicalOrientation
6
CPRIn unitaECCO
9
ECCOIn unit
10
HOE
11
ECCOIn unit
12
HOE
13
ECCOCCI
16
ECCOIn unit
17
HOE
18
HOE
19
HOE
20
ECCOCCI
Weeks 4-8Variable: Days divided between ECCO, PACEP, CCI, and In unit
Weeks 9-12Variable: Days in unit
Abbreviations: CCI, Critical Care Institute classes; ECCO, Essentials of Critical Care Orientation; HOE, Habits of Excellence orientation for all new graduate nurses;PACEP, Pulmonary Artery Catheter Education Program computer lessons.a In unit indicates time with preceptor.
Copyright 2007, Northwestern Memorial Hospital.
by AACN on January 24, 2019http://ccn.aacnjournals.org/Downloaded from
and practices, additional responsi-bilities are given, promoting inde-pendence and autonomy with whichto provide care for increasinglycomplex patients.
This program has been so suc-cessful that Northwestern MemorialAcademy has agreed to provideadditional resources to expand theprogram to include any experiencednurses with non–critical care experi-ence who might benefit from partic-ipation in the CCI, as identified bythe staff educators and managers.
Unit OrientationAt the end of week 8, each grad-
uate nurse has completed all didac-tics but continues to work in theunit with a preceptor. This experi-ence eases the graduate nurse intothe critical care nursing role whilestill under the watchful guidanceof a preceptor. Upon the successful
completion of week 12, the gradu-ate nurse is considered an advancedbeginner in critical care nursingand may be allowed to independ-ently provide care for patients inthe ICU.
Throughout the orientationprocess, the progress of each orien-tee is evaluated by the CCI programdirector and the unit educators toensure successful completion of eachpart of the orientation. These form-ative evaluations consist of tests,informal question-and-answer ses-sions, observations, clarifications,demonstrations, and weekly check-lists completed by preceptors andorientees. Graduate nurses mustalso complete each ECCO and PACEPlesson with a score of 85% or better.If remediation is needed, the CCIprogram director works with allappropriate parties to determine aplan of action for the orientee to
complete the program successfullyand within a specified time.
Although graduate nurses, expe-rienced nurses who are new to criti-cal care, and experienced criticalcare nurses are evaluated differently,nurses within these identified groupsare evaluated consistently across all5 ICUs. We have specific evaluationcriteria for each group, and thosecriteria are used consistently acrossall ICUs. This process allows moreobjective evaluation of orientees’ability to function in the work envi-ronment. The staff of the CCI nowhave primary responsibility forensuring competence, and this prac-tice removes the managers’ and pre-ceptors’ subjectivity on whether ornot a nurse is ready for an inde-pendent assignment.
Critical Care PreceptorsWe recognized that one of the
strengths of this new orientationprogram depended on the amountof support that could be provided tothe ICU preceptors. Before the startof the new orientation, each precep-tor was given the opportunity toreview all the computerized learningmodules. Many materials were alsodeveloped to assist both preceptorsand orientees, including a preceptorguide, a case study book, a moduleguide, a pocket guide, and a CD ofevidence-based critical care literature:
• Preceptor guide—provides ageneral overview of the orientationprogram and contains weeklychecklists to keep abreast of eachorientee’s progress and the focusedlearning experiences for that week.
• Case study guide—a collectionof case studies, with increasing levelsof complexity, developed for use bythe preceptors. Each case situation
52 CRITICALCARENURSE Vol 27, No. 6, DECEMBER 2007 http://ccn.aacnjournals.org
Table 9 Content of group sessions for graduate nurses in Critical Care Institute (CCI)
Graduate Nurse Orientation (CCI)Weeks 2 to 8
Day 1
Day 2
Day 3
Day 4
Day 5
Day 6
Day 7
Day 8
Day 9
Day 10
Day 11
Day 12
Introduction
Managing patients with arrhythmias• ECG monitoring, defibrillator and external pacemaker
Managing patients with cardiovascular disorders
Managing patients with pulmonary disorders• Blood gases, mechanical ventilation, artificial airways
Simulated cardiovascular/pulmonary emergencies (level 1)
Hemodynamic monitoring, hemodynamic waveforms
Managing patients with neurological disorders• ICP monitoring, EVDs, train of four
Managing patients with renal disorders• Continuous renal replacement therapy
Managing patients with gastrointestinal/endocrine/hematological disorders• Insulin protocol, rapid infuser, bladder pressure monitoring
Managing patients with hemodynamic alterations
Simulated cardiovascular/pulmonary emergencies (level 2)
Managing patients with multisystem disorders
Abbreviations: ECG, electrocardiographic; EVDs, external ventricular drains; ICP, intracranial pressure.
Copyright 2007, Northwestern Memorial Hospital.
StaffDevelopment
by AACN on January 24, 2019http://ccn.aacnjournals.org/Downloaded from

contains relevant patient data and aseries of questions with answers sothat the preceptor can easily guidean orientee to the correct answers.It also contains a blank copy of thesituation without answers so thatthe orientee can complete it inde-pendently and review it later withthe preceptor or staff educator.Tables 5 and 6 provide examples ofboth versions.
• Module guide—content out-lines and references for each Web-based module. Refer to the ECCOsite9 for more information about thecontent of the modules.
• Pocket guide—a collection ofcritical care reference material suchas normal and abnormal pulmonaryartery and intracranial pressurewaveforms, normal ranges of resultsof laboratory tests, dysrhythmias,and acid-base disturbances. It is sizedto accommodate data fitting on 3 ×5-in index cards, easily fits into apocket, and allows orientees to addextra pages of information. Table 10provides an example of a page fromthe pocket guide.
• CD—a collection of more than350 articles on evidence-based prac-tice in critical care, graphics, andPowerPoint presentations about avariety of critical care topics. It wasstarted by the CNS, and materialswere added by the staff educators.Under the fair use copyright guide-lines, these CDs can be used onlyfor educational purposes with ournurses, and they contain a dis-claimer indicating so. In addition,each ICU has a folder on the CDthat can also include the unit’s orien-tation manual or other unit-specificinformation.
The staff educators and themanagers are responsible for coor-dinating the orientation schedulebetween each preceptor and gradu-ate nurse. Each preceptor is given acopy of the schedule that detailswhen the preceptor’s graduate nurseis in group sessions, at the com-puter, or in the unit. Graduatenurses are also given detailed check-lists containing the objectives foreach group session that they need tocomplete in the unit with their
preceptors. It is the responsibilityof each graduate nurse to meetweekly with his or her preceptor toreview checklist completion; thechecklist is then reviewed by theCCI program manager during thenurse’s group sessions. This systemallows communication of progressbetween the CCI instructors, thegraduate nurses, and the precep-tors—and communication back tothe managers. This arrangement isespecially helpful when a graduatenurse is assigned to more than asingle preceptor.
Table 11 is an example of agraduate nurse’s checklist. Precep-tors and educators involved in theHabits of Excellence program wereallowed to adjust their schedules,enabling them to assume the addi-tional responsibilities required forsuccessful implementation of theorientation.
Management PerspectivesAlthough the goal of an effective
orientation program is to produce acompetent critical care nurse, theICU nurse managers must alsoaddress fiscal and human resourceissues: How quickly can graduatenurses be moved from orientationto the regular work force? How manyorientees can a unit accommodateat one time? How can this intensivenew program be initiated withoutaddressing the learning needs ofcurrent staff members who wereoriented under a different model?
One ICU nurse manager notedthat graduate nurses in the ICUhave a “steep learning curve” andusually do not demonstrate criticalthinking and astute assessmentskills until after they have been outof orientation for 6 months to 1
http://ccn.aacnjournals.org CRITICALCARENURSE Vol 27, No. 6, DECEMBER 2007 53
Table 10 Example of a page from the pocket guide
Endotracheal tube management
Assess cuff pressure: >20 mm Hg increases risk for tracheal damage<15 mm Hg increases risk of aspiration around cuff
Assess ventilation: • Auscultate the lateral aspect of the chest midaxillary line for presence of breath
sounds, inspect chest for equal expansion• Auscultate over the epigastric area
• Gurgling sounds indicate esophageal intubation—remove tube and reintubate• End-tidal carbon dioxide monitor to evaluate effectiveness of ventilation
• Result should be within 5 mm Hg of PaCO2• A result >5 mm Hg indicates increased dead space (eg, pulmonary embolism)
Use minimal occlusive technique:• Place stethoscope at larynx• Slowly remove air (in 0.2-mL amounts) from cuff until air leak is heard• Slowly reinsert (in 0.2-mL amounts) until the inspiratory leak stops
Refer to Policy #18.13, Endotracheal (ET) Intubation and Policy #18.12, Endotracheal (ET) Extubation
Copyright 2007, Northwestern Memorial Hospital.
by AACN on January 24, 2019http://ccn.aacnjournals.org/Downloaded from

year. By their 1-year anniversary inthe unit, the graduate nurses haveusually developed clinical compe-tence but are not confident in theirpractice. The manager has called thesecond year of new graduate nurses’ICU career their “confidence curve,”the time during which they developconfidence in themselves. At the
same time, their peers and the med-ical staff develop confidence in thenurses’ assessments, clinical skills,and decisions related to patient care.
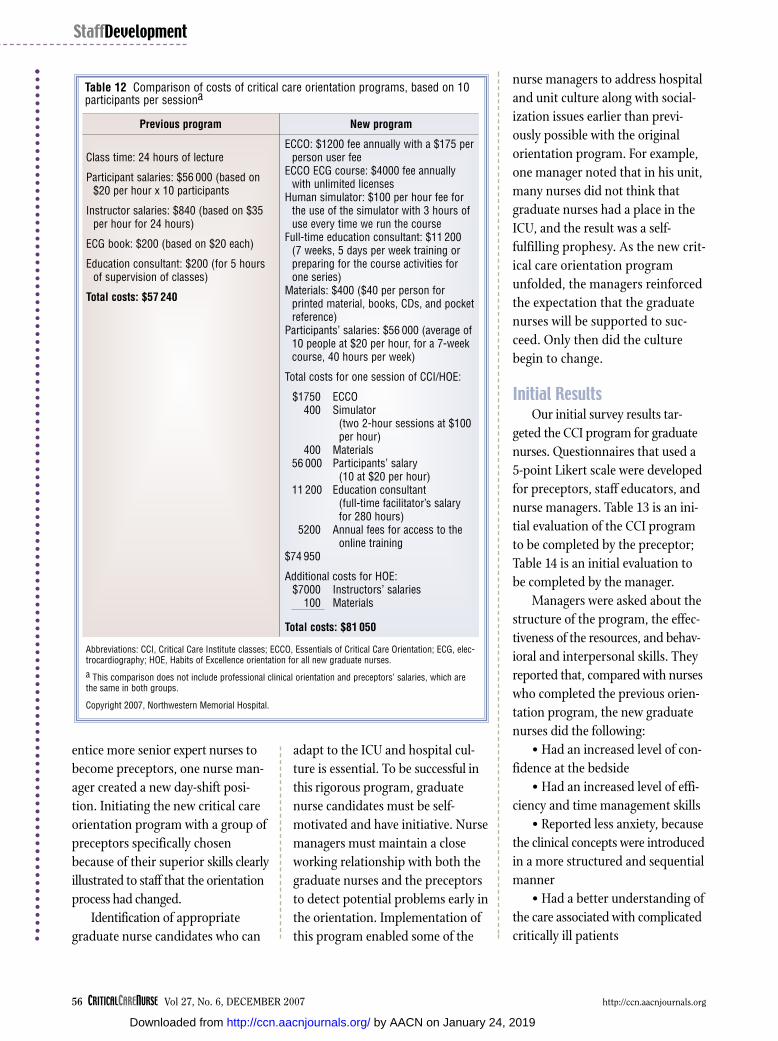
The managers in each ICU sup-ported the implementation of thenewly designed program by absorb-ing the financial costs involved,facilitating space for computerized
learning in theunit, and allow-ing more clinicalteaching timefor the educa-tors outside theunit. Table 12shows the costsof the newmodel of criticalcare orientation.Although thesecosts are signifi-cant, they mustbe weighedagainst the ben-efits of the pro-gram.
Nurse man-agers noted thata primary con-cern in formu-lating anorientation pro-gram based oncompetency wasidentifying acadre of precep-tors who aremotivated toteach, as indi-cated in the pre-ceptors’ annualperformancegoals. Each pre-ceptor musthave excellentcommunication
skills and at least 2 years of acutecare experience (without perform-ance issues), with one of those yearsin critical care clinical experience inthe preceptor’s current unit. Precep-tor workshops were designed tosolidify these skills to enable thepreceptors to evaluate and validateorientees’ accomplishments. To
54 CRITICALCARENURSE Vol 27, No. 6, DECEMBER 2007 http://ccn.aacnjournals.org
Table 11 Example of a page from the weekly checklist for the arrhythmias module
ECG Module Observation Form Demonstrate beginning competence in the management of the patient with ECG monitoring.
Reference: NCP # 2.08, 18.06, 18.11 NAP #2.08, PCP# 5.67
Nurse observed: __________________________________
Goals: • To identify basic cardiac rhythms• To recognize emergency arrythmias and respond appropriately• To set up the Marquette system for telemetry monitoring• To identify the components of a LifePak defibrillator• To identify basic cardiac electronic paced rhythms
Demonstrates knowledge of basic arrythmia recognition.
1 Identifies the following rhythms on an ECG monitor:
Normal sinus rhythm
Sinus bradycardia
Sinus tachycardia
Atrial tachycardia
Atrial flutter
Atrial fibrillation
1st degree A-V block
2nd degree A-V block
3rd degree A-V block
Junctional rhythm
Ventricular tachycardia
Ventricular fibrillation
Asystole
2 Determines heart rate and measures PR, QRS, and QT intervals on ECG rhythm strip
Not o
bser
ved
Does
not
de
mon
stra
teDe
mon
stra
tes
whe
n cu
ed
Dem
onst
rate
s
Revi
ewed
0 1 2 3 4
� � � � �
� � � � �
� � � � �
� � � � �
� � � � �
� � � � �
� � � � �
� � � � �
� � � � �
� � � � �
� � � � �
� � � � �
� � � � �
� � � � �
Abbreviations: A-V, atrioventricular; ECG, electrocardiographic; NAP, nursing administration policy; NCP, nursing care policy; PCP, patientcare procedure.
Copyright 2007, Northwestern Memorial Hospital.
StaffDevelopment
by AACN on January 24, 2019http://ccn.aacnjournals.org/Downloaded from
entice more senior expert nurses tobecome preceptors, one nurse man-ager created a new day-shift posi-tion. Initiating the new critical careorientation program with a group ofpreceptors specifically chosenbecause of their superior skills clearlyillustrated to staff that the orientationprocess had changed.
Identification of appropriategraduate nurse candidates who can
adapt to the ICU and hospital cul-ture is essential. To be successful inthis rigorous program, graduatenurse candidates must be self-motivated and have initiative. Nursemanagers must maintain a closeworking relationship with both thegraduate nurses and the preceptorsto detect potential problems early inthe orientation. Implementation ofthis program enabled some of the
nurse managers to address hospitaland unit culture along with social-ization issues earlier than previ-ously possible with the originalorientation program. For example,one manager noted that in his unit,many nurses did not think thatgraduate nurses had a place in theICU, and the result was a self-fulfilling prophesy. As the new crit-ical care orientation programunfolded, the managers reinforcedthe expectation that the graduatenurses will be supported to suc-ceed. Only then did the culturebegin to change.
Initial ResultsOur initial survey results tar-
geted the CCI program for graduatenurses. Questionnaires that used a5-point Likert scale were developedfor preceptors, staff educators, andnurse managers. Table 13 is an ini-tial evaluation of the CCI programto be completed by the preceptor;Table 14 is an initial evaluation tobe completed by the manager.
Managers were asked about thestructure of the program, the effec-tiveness of the resources, and behav-ioral and interpersonal skills. Theyreported that, compared with nurseswho completed the previous orien-tation program, the new graduatenurses did the following:
• Had an increased level of con-fidence at the bedside
• Had an increased level of effi-ciency and time management skills
• Reported less anxiety, becausethe clinical concepts were introducedin a more structured and sequentialmanner
• Had a better understanding ofthe care associated with complicatedcritically ill patients
56 CRITICALCARENURSE Vol 27, No. 6, DECEMBER 2007 http://ccn.aacnjournals.org
Table 12 Comparison of costs of critical care orientation programs, based on 10participants per sessiona
Previous program
Class time: 24 hours of lecture
Participant salaries: $56 000 (based on$20 per hour x 10 participants
Instructor salaries: $840 (based on $35per hour for 24 hours)
ECG book: $200 (based on $20 each)
Education consultant: $200 (for 5 hoursof supervision of classes)
Total costs: $57 240
New program
ECCO: $1200 fee annually with a $175 perperson user fee
ECCO ECG course: $4000 fee annuallywith unlimited licenses
Human simulator: $100 per hour fee forthe use of the simulator with 3 hours ofuse every time we run the course
Full-time education consultant: $11 200 (7 weeks, 5 days per week training orpreparing for the course activities forone series)
Materials: $400 ($40 per person forprinted material, books, CDs, and pocketreference)
Participants’ salaries: $56 000 (average of10 people at $20 per hour, for a 7-weekcourse, 40 hours per week)
Total costs for one session of CCI/HOE:
$1750 ECCO400 Simulator
(two 2-hour sessions at $100 per hour)
400 Materials56 000 Participants’ salary
(10 at $20 per hour)11 200 Education consultant
(full-time facilitator’s salary for 280 hours)
5200 Annual fees for access to the online training
$74 950
Additional costs for HOE:$7000 Instructors’ salaries
100 Materials
Total costs: $81 050
Abbreviations: CCI, Critical Care Institute classes; ECCO, Essentials of Critical Care Orientation; ECG, elec-trocardiography; HOE, Habits of Excellence orientation for all new graduate nurses.a This comparison does not include professional clinical orientation and preceptors’ salaries, which arethe same in both groups.
Copyright 2007, Northwestern Memorial Hospital.
StaffDevelopment
by AACN on January 24, 2019http://ccn.aacnjournals.org/Downloaded from

• Developed more critical-thinking skills as case scenarioswere reviewed
• Developed better networkingskills with other ICUs and the abilityto use resources in those other units,because the clinical experiences were
not limited to their home unit andthey had access to the resources ofthe entire facility
After the first 15 months, 116nurses had completed the new crit-ical care orientation program: 68graduate nurses, 33 experienced
non–criticalcare nurses,and 15 experi-enced criticalcare nurses.The staff educa-tors and pre-ceptorsreported thatthe new criticalcare orientationprogram wasless labor inten-sive than theprevious pro-gram becausethey did nothave to spendtime preparingand teachingcritical careclasses; insteadthe majority ofthe classes werereplaced bycomputer-basedcontent and self-paced learning.Because clearand concisewritten materi-als were pro-vided, orientees,preceptors, andstaff educatorshad fewer ques-tions aboutdaily schedulesand expecta-tions. Graduate
nurses appreciated that educationalmaterials were provided in bothwritten and computer-based for-mats. Preceptors reported that theywere able to spend more time con-centrating on issues of patient carerather than on explaining critical
http://ccn.aacnjournals.org CRITICALCARENURSE Vol 27, No. 6, DECEMBER 2007 57
Table 13 Sample of form used by preceptors for evaluation of the Critical Care Institute
In general, I believe that the Critical CareInstitute program:
Not at all true
1
No
2
Yes
3
To a great extent
4
Not applicable
51. Was useful in preparing new graduate
nurses for the intensive care unit (ICU)
2. Resulted in orientees who were more prepared to complete orientation with their preceptors
3. Resulted in orientees who demonstrated more confidence
4. Resulted in orientees with lower levels of anxiety
5. Provided information that was useful to new graduates entering the ICU
6. Provided information so that review by preceptors was not necessary
In general, I believe the following about theCritical Care Institute program:
Not at all true
1
No
2
Yes
3
To a great extent
4
Not applicable
57. The structure of the modules was
logical
8. The preceptor guide was a useful tool for providing clinical focus for times when the orientee was on the unit
9. The amount of information provided inthe orientation was appropriate
10. The topics covered in the Critical Care Institute were appropriate
What additional information do you think should be covered in the Critical Care Institute?
What information could be deleted from the Critical Care Institute?
Increase Neither increase nor decrease
Decrease
11. In general, I believe the Critical Care Institute will __________ the amount of time new graduate nurses will spend in orientation.
I have precepted ___________ new graduate nurses in the past 2 years.I have practiced as a nurse for approximately _____ years and _____ months.
Copyright 2007, Northwestern Memorial Hospital.
by AACN on January 24, 2019http://ccn.aacnjournals.org/Downloaded from

care concepts such as hemodynam-ics or interpretation of electrocar-diograms. And finally, additionalrecruitment opportunities arosefrom word-of-mouth knowledge ofthis new orientation model.
For a while, we continued tooffer the “old” orientation program,until we had fully implemented the
new orientation model. This overlapallowed us a unique opportunity tocompare groups. The managers’impressions were that CCI groupsdid the following:
• Seemed to be more “hands-on”early on, and had more inclination toparticipate actively in patients’ care
• Appeared to integrate theo-
retical knowl-edge into clini-cal practicemore readily
• Seemedmore flexible,perhapsbecause manyof the experi-ences wereobtained out-side the groupmembers’ ownclinical spe-cialty areas
• Appearedto develop asense of cama-raderie, estab-lishingthemselves as acohort andthereby facili-tating socializa-tion into thelarger institution
In addition,we observedthat with theaid of the CCI,graduate nurseshad excellentclinical andassessmentskills immedi-ately after orientation.Compared with
our previous orientees, nurses inthe CCI group demonstrated critical-thinking skills, greater confidence in their decisions, andimproved problem-solving abilitiesmore quickly. Nurse managers noware fully committed to the CCI asthe orientation program for gradu-ate nurses.
58 CRITICALCARENURSE Vol 27, No. 6, DECEMBER 2007 http://ccn.aacnjournals.org
Table 14 Sample of form used by managers for evaluation of the Critical Care Institute
In general, I believe that the Critical Care Institute program was useful in:
Not at all1
Somewhat2
Mostly3
To a great extent 4
Not appli-cable 5
1. Decreasing the amount of anxiety felt by the preceptors
Comments:
2. Decreasing the amount of burnout felt by the preceptors
Comments:
3. Decreasing the amount of time spent in orientation
Comments:
3. a. If the Critical Care Institute decreased the amount of time spent in orientation, by how much time was orientation shortened?
3. b. If the Critical Care Institute increased the amount of time spent in orientation, by how much time was orientation lengthened?
Of the remaining questions, please indicate howtrue you believe the following statements to be.Use the scale to the right to indicate your choice.
Very false
1
False
2
Neither truenor false
3
True
4
Very true
5
4. The amount of information covered in the Critical Care Institute was appropriate
Comments:5. The balance of time devoted to the didactic
portion of the program (the computer and class time) and time in the unit was appropriate
Comments:6. The amount of time devoted to online
computer learning (ECCO) was appropriateComments:7. The amount of resources my unit devoted to
the Critical Care Institute was appropriateComments:8. Overall, I am satisfied with the Critical Care
InstituteComments:9. I believe that the Critical Care Institute should
be continuedComments:
Abbreviation: ECCO, Essentials of Critical Care Orientation.
Copyright 2007, Northwestern Memorial Hospital.
StaffDevelopment
by AACN on January 24, 2019http://ccn.aacnjournals.org/Downloaded from

Lessons Learned With Implementation
Although this new process wasvery well received, some lessonswere still learned during the earlyperiod after implementation. Thesecan be summarized as follows:
• Initially, preceptors were con-fused with the new process for thegraduate nurses. As a result, theNorthwestern Memorial Academy’seducation consultant spent timewith each preceptor, reviewing thenew model of orientation and allthe teaching tools available.
• Preceptors needed to revisetheir schedules to match the orien-tee’s schedules. Scheduling con-straints for preceptors sometimesresulted in an orientee having multi-ple preceptors.
• Learning content provided bythe central CCI program sometimesoverlapped with that of the unit-specific orientation programs.
• The workload for the staff edu-cators was increased to accommo-date the Habits of Excellenceprogram and those orientees whowere not able to participate in theentire program.
• Preceptors did not hold expe-rienced non-ICU nurses to the sameschedule as that followed by thegraduate nurses, so the orientationexperience of experienced non-ICUnurses was more fragmented, similarto the limitations of our previouscritical care orientation program.
We found that the graduate nurseswere quite eager to participate in thenew program and verbalized theirmotivation to develop and improvetheir clinical skills. Although theyexpressed frustration in managingthe overwhelming amount of didac-tic information and resources, they
realized the value of the content.The case studies that were reviewedwith the graduate nurses during thegroup time or time with their pre-ceptors helped alleviate some of thenurses’ anxieties when clinical expe-riences were lacking.
The experienced ICU nursesfound the new orientation programa helpful refresher for their currentknowledge base. However, the non-ICU experienced nurses felt the dis-connection between the self-pacedcomputer learning and the clinicalexperience because these nurses werenot initially included in the groupsessions. To provide a more coordi-nated orientation effort, educatorsand managers now encourage thepreceptors to follow the same sched-ule of orientation for the non-ICUexperienced nurses as that used fornew graduate nurses.
A concern surfaced when clinicalexperiences were not always available.For example, at times the unit con-tained only a single patient with adisease process or procedure thatcoincided with the topic of that week.With multiple new critical care nursescompeting for this same clinicalexperience, the limitations includedhaving respect for the patient’s needsand privacy while balancing theoptimal clinical learning experiencefor the new nurses. The review ofpolicies and procedures was notreceived as well as other strategieswere until we reformatted it to coin-cide with the hands-on experiences.
Preceptors initially reported theirpersistent need to give additionalinformation to graduate nurses. Wefound it beneficial to reinforce withthe preceptors that the graduatenurses are coming to the units pre-pared with more critical care infor-
mation, and the preceptors shouldnow serve as role models for gradu-ate nurses to demonstrate what itmeans to “be a nurse.” The precep-tors realize now that they still needto provide information, but the focushas shifted from reviewing criticalcare concepts to demonstrating theprocess of patient care.
Detailed communication of theCCI program was the most challeng-ing aspect of this program becauseof the scope of the program and thenumber of people involved. Whenas few as 2 or as many as 6 newgraduates began every 4 weeks, theeducators found juggling schedulesbetween orientees and preceptors achallenge, especially because of theconstraints already in place withthe structured schedule. This cas-cading effect exhausted the avail-able resources.
We have just begun to expandthe CCI program to incorporateexperienced nurses with non-ICUbackgrounds into sessions with thegraduate nurses. We anticipate thatthis change will have an impact onresource allocation, making it vitalto be cognizant of the constraintson ICU resources as we accommo-date the larger number of partici-pants. At the very least, we expectthat a schedule similar to that of thegraduate nurses will further enhancethe experience for new orientees.
ConclusionOur new model of critical care
orientation allowed us to addresssome of the challenges facing criti-cal care educators in integratingnurses with a variety of experiencelevels into the critical care setting.The new program has resulted in amore coordinated, consistent
http://ccn.aacnjournals.org CRITICALCARENURSE Vol 27, No. 6, DECEMBER 2007 59
by AACN on January 24, 2019http://ccn.aacnjournals.org/Downloaded from

orientation experience for all orientees and for precep-tors as well. We foster the knowledge and skill necessaryfor new nurses to function independently and compe-tently in the ICU, and for the preceptors to have the nec-essary resources and materials needed to ensureconsistent implementation of the orientation program.
The foundation of the CCI is also proving importantin areas of the hospital other than the education of grad-uate nurses; it is serving as a template for major changesto the way orientation is provided in other nursing units.Using this new educational process as a foundation, wehave successfully expanded two of our ICUs from 12-bedto 23-bed units. The structure of the new orientationprogram can be applied to any learning curve and canincorporate nurses at any skill level. The options havebecome limitless as we continue to develop and perfectthe CCI. Now, with the initial implementation phasecomplete, we plan to expand the program and perfect itas variables in the profession and the workplace con-tinue to evolve.
AcknowledgmentsWe thank all the people involved in making this program successful: hospitaland nursing administration for their support of the proposal and the meansto implement it, members of the Northwestern Memorial Academy for theirexpertise in curriculum development and leadership during implementationof the program, and the staff of the Patient Safety Simulator Center for theirassistance in creation and implementation of the simulation scenarios.Finally, we appreciate the support of all the critical care preceptors and staff ofthe ICUs at Northwestern Memorial Hospital, especially during the initialphases of implementation. It has truly been a team effort in which we can alltake pride.
Financial DisclosuresNone reported.
References1. Benner P. From Novice to Expert: Excellence and Power in Clinical Nursing
Practice. Commemorative ed. Upper Saddle River, NJ: Prentice Hall; 2001.2. Waight C, Stewart B. Valuing the adult learner in e-learning: a conceptual
model for corporate settings. In: Morris M, ed. Proceedings AHRD Confer-ence 2005. Bowling Green, OH: Academy of Human Resource Develop-ment; 2005:1118-1123. www.ahrd.org. Accessed September 10, 2007.
3. Houde J. Andragogy and motivation: an examination of the principlesof andragogy through two motivation theories. In: Nafukho FM, ed.Proceedings AHRD Conference 2006. Bowling Green, OH: Academy ofHuman Resource Development; 2006:90-97. www.ahrd.org. AccessedSeptember 10, 2007.
4. Clardy A. Andragogy: Adult Learning and Education at Its Best? Bronx,NY: HW Wilson Co; 2006.
5. Brundage D, Macher D. Adult Learning Principles and Their Application toProgram Planning. Toronto, ON: Ministry of Education; 1980.
6. Knowles MS. The Modern Practice of Adult Education: From Pedagogy toAndragogy. River Grove, IL: Follett Publishing Co; 1980.
7. Darkenwald G, Merriam S. Adult Education: Foundations of Practice.New York, NY: Harper & Row; 1982.
8. Chaves C. Involvement, development and retention: theoretical foun-dations and potential extensions for adult community college students.Community Coll Rev. 2006; 34(2):139-152.
9. American Association of Critical-Care Nurses. Essentials of critical careorientation. http://aacn.org/AACN/conteduc.nsf/vwdoc /EccoHome.Accessed September 4, 2007.
10. Pulmonary Artery Catheter Education Project Collaborative. Pulmonaryartery catheter education project. http://www.pacep.org. AccessedSeptember 4, 2007.
11. Tomey A. Learning with cases. J Contin Educ Nurs. 2003;34(1):34-38.12. Gordon J. High-fidelity patient simulation: a revolution in medical edu-
cation. In: Dunn W, ed. Simulators in Critical Care and Beyond. DesPlaines, IL: Society of Critical Care Medicine; 2004:3-6.
13. Schumacher L. Simulation in critical care nursing education: concep-tual and practical perspectives. In: Dunn W, ed. Simulators in CriticalCare and Beyond. Des Plaines, IL: Society of Critical Care Medicine;2004: 114-118.
14. Toth JC. The Basic Knowledge Assessment Tool, Version Seven (BKAT-7) forAdult Critical Care Nursing. Limited circulation. Washington, DC:Catholic University of America; 2006.
60 CRITICALCARENURSE Vol 27, No. 6, DECEMBER 2007 http://ccn.aacnjournals.org
StaffDevelopment
by AACN on January 24, 2019http://ccn.aacnjournals.org/Downloaded from

CE Test Test ID C0762: Designing a Comprehensive Model for Critical Care OrientationLearning objectives: 1. Examine the role and challenges of critical care educators in integrating diverse levels of nursing experience into an orientation model2. Describe the educational and training needs of preceptors assisting with implementation of a critical care orientation program 3. Discover the benefits of a critical care model of orientation on the unit, the staff, and the hospital
Program evaluationYes No
Objective 1 was met � �Objective 2 was met � �Objective 3 was met � �Content was relevant to my
nursing practice � �My expectations were met � �This method of CE is effective
for this content � �The level of difficulty of this test was: � easy � medium � difficult
To complete this program, it took me hours/minutes.
Test answers: Mark only one box for your answer to each question. You may photocopy this form.
1. In intensive care units (ICUs) since the 1990s, what factors havechanged requiring critical care educators to reevaluate orientation programs?a. Longer length of stay and increased severity of illnessb. Shorter length of stay and increased severity of illness c. Decreased severity of illness and shorter length of stayd. Decreased severity of illness and stable length of stay
2. What were the major concerns of managers and educators regardingthe training and development of the program?a. Critical thinking skills and individualized course contentb. Practice skills and content consistencyc. Critical thinking and practice skillsd. Content and consistency of course and critical thinking skills
3. What inconsistencies were found in the initial assessment of the existing orientation program?a. PowerPoint slides, instructor’s level of education, and schedulingb. Instructional reliability, teaching materials, and instructor’s critical
thinking skillsc. Teaching materials, educational techniques, and program lengthd. Scheduling, instructional reliability, and teaching materials
4. What was the main purpose of the new orientation program?a. To increase the educator’s job satisfactionb. To improve ICU staffingc. To promote independent and competent ICU staffd. To provide new staff skills to function
5. The new orientation program was based on what nursing model?a. Benner’s novice to expert modelb. Roy’s adaptation modelc. Benner’s expert to novice modeld. The Synergy Model
6. The human simulator used in the orientation model is valuable inassessing what?a. Benner’s level of masteryb. Critical thinking skillsc. Preceptor effectivenessd. Nursing school attended
7. How many separate orientation pathways are present in the new critical care orientation algorithm?a. 6b. 4c. 3d. 2
8. What are the primary learning methods in the new orientationmodel?a. Online learning, precepted clinical time, and outside conferencesb. Case studies, online learning, and precepted clinical timec. Precepted clinical time, tests, and online learningd. Outside conferences, online preceptors, and case studies
9. What are some of the reported benef its for graduate nurses afterthe implementation of the orientation program?a. Increased level of confidence and critical thinking skillsb. Increased use of evidence-based practice and confidencec. Increased level of confidence and knowledge of administrative
expectationsd. Increased use of evidence-based practice and level of confidence
10. What is the length of orientation for a new graduate nurse?a. 8 weeksb. 1 yearc. 4 weeksd. 12 weeks
11. Within the clinical orientation of graduate nurses, how were theyexposed to examples of altered physiology?a. Emergency department rotationsb. Simulator usec. Mentor-mediated experiencesd. Disregarding traditional unit boundaries
12. What tool was used to assess experienced critical care nurses’knowledge level?a. ECCO modulesb. Basic Knowledge Assessment toolc. SATd. CCRN certificate
For faster processing, takethis CE test online at
http://ccn.aacnjournals.org(“CE Articles in this issue”)or mail this entire page to:
AACN, 101 Columbia Aliso Viejo, CA 92656.
Test ID: C0762 Form expires: December 1, 2009 Contact hours: 1.0 Fee: AACN members, $0; nonmembers, $10 Passing score: 9 correct (75%) Category: A, SynergyCERP A Test writer: Patti McCluskey-Andre, RN, MSN, ACNP-C/CCNS
9. �a�b�c�d
8. �a�b�c�d
7. �a�b�c�d
6. �a�b�c�d
5. �a�b�c�d
4. �a�b�c�d
3. �a�b�c�d
2. �a�b�c�d
1. �a�b�c�d
11. �a�b�c�d
12. �a�b�c�d
10. �a�b�c�d
Name Member #
Address
City State ZIP
Country Phone
RN Lic. 1/St RN Lic. 2/St
Payment by: � Visa � M/C � AMEX � Discover � Check
Card # Expiration Date
SignatureThe American Association of Critical-Care Nurses is accredited as a provider of continuing nursing education by the American Nurses Credentialing Center’s Commission on Accreditation.
AACN has been approved as a provider of continuing education in nursing by the State Boards of Nursing of Alabama (#ABNP0062), California (#01036), and Louisiana (#ABN12). AACN programming meets the standards for most other states requiring mandatory continuing education credit for relicensure.
by AACN on January 24, 2019http://ccn.aacnjournals.org/Downloaded from

Greta Nelson, Janet Palamone, Robb Rabito, Rebecca Wetzel and Lindsay GoldsteinLinda L. Morris, Pamela B. Pfeifer, Rene Catalano, Robert Fortney, Edith L. Hilton, Julia McLaughlin,Designing a Comprehensive Model for Critical Care Orientation
http://ccn.aacnjournals.org/Published online Copyright © 2007 by the American Association of Critical-Care Nurses
37-60 27 2007;Crit Care Nurse
http://ccn.aacnjournals.org/cgi/external_ref?link_type=PERMISSIONDIRECTPersonal use only. For copyright permission information:
http://ccn.aacnjournals.org/subscriptions/Subscription Information
http://ccn.aacnjournals.org/misc/ifora.xhtmlInformation for authors
http://www.editorialmanager.com/ccn Submit a manuscript
http://ccn.aacnjournals.org/subscriptions/etoc.xhtmlEmail alerts
362-2049. Copyright ©2016 by AACN. All rights reserved. bimonthly by AACN, 101 Columbia, Aliso Viejo, CA 92656. Telephone: (800) 899-1712, (949) 362-2050, ext. 532. Fax: (949) Critical Care Nurse is an official peer-reviewed journal of the American Association of Critical-Care Nurses (AACN) published
by AACN on January 24, 2019http://ccn.aacnjournals.org/Downloaded from





























