Embed Size (px)
Citation preview

ST Segment Elevation Nothing is ever as hard (or easy) as it looks
Cameron Guild, MD
Division of Cardiology
University of Mississippi Medical Center
February 17, 2012
1. Describe the electrical changes within the myocardium that lead to ST elevation on ECG.
2. Demonstrate groups of ECG leads effected by various regions of myocardial ischemia.
3. Review examples of ECG’s showing STEMI and show the corresponding coronary angiograms.
4. Identify non-ischemic causes of ST elevation that mimic STEMI.
Objectives

Review of Important Terms
J point
Intervals include waves
Segments are distances between waves
PR segment- time between atrial depolarization and ventricular depolarization
ST segment- time between ventricular depolarization and repolarization
TP segment- time where all of heart is repolarized and awaiting next depolarization
J point- the “junction” of the QRS with the ST segment
PR segment ST segment TP segment
PR interval QRS interval
QT interval

Why is there “ST elevation” in STEMI?
“isoelectric” points are where the action potential is zero (no “flow” of current). ST segment- all cells of LV are depolarized
TP segment- all cells of LV are polarized
Injured myocytes cannot produce energy to maintain electrical gradients (repolarize); thus, in constant state of full/partial depol.
Thus, the only isoelectric point in an ischemic heart is the ST segment where all cells are depolarizing. Technically, that means the ST segment is really the baseline with TP and PR
depression… not ST elevation!

0-30 min 0-12 hrs 1-12 hrs 1-5 days wks-mths
Evolution of “Current of Injury”
• Highly variable timing of above (not all stages every time)
• Reperfusion usually accelerates evolution of changes

ECG while CP free
ECG within 2 min of CP onset
Hyperacute T waves

ECG baseline & 2 hours later

5/10 CP on arrival
10/10 CP 1hr later
ECG during bad & worse chest pain
Post PCI
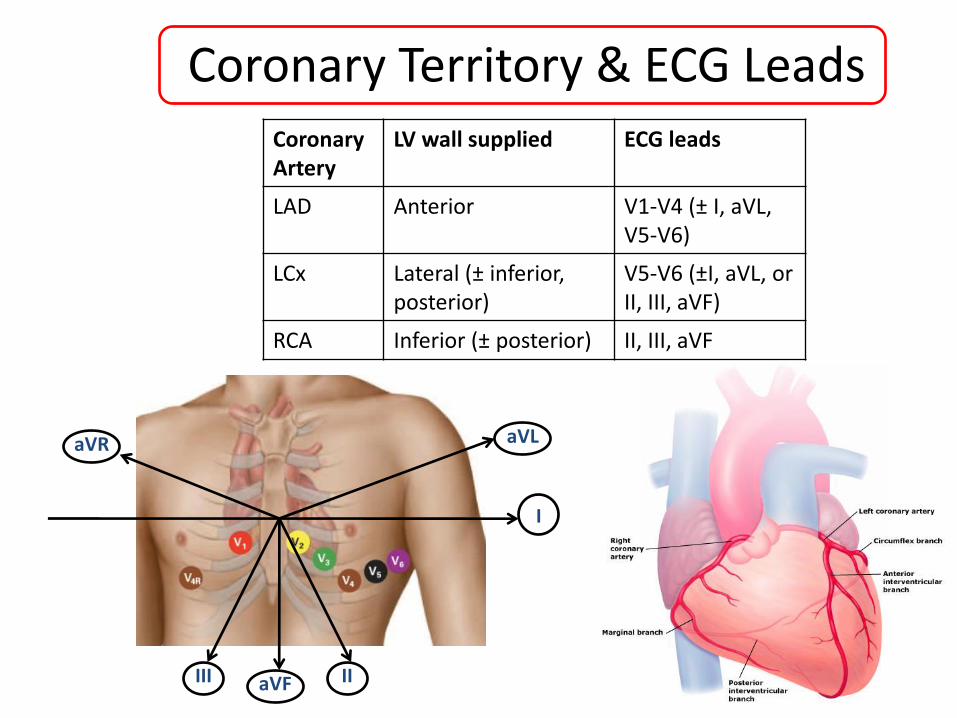
aVR
I
II III aVF
aVL
Coronary Artery
LV wall supplied ECG leads
LAD Anterior V1-V4 (± I, aVL, V5-V6)
LCx Lateral (± inferior, posterior)
V5-V6 (±I, aVL, or II, III, aVF)
RCA Inferior (± posterior) II, III, aVF
Coronary Territory & ECG Leads

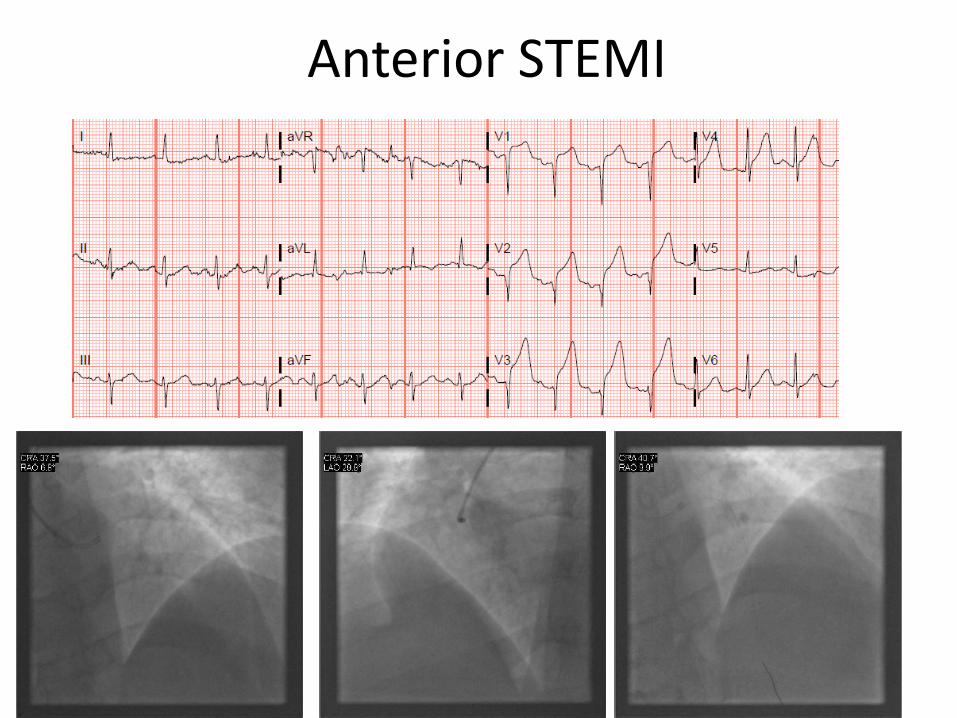
Anterior STEMI
ST V2-V4 (±V5,V6)
• ST V1 if proximal to first septal perforator.
• ST in I, aVL if proximal to first diagonal
Occlusion of proximal LAD

Lateral STEMI
Occlusion of proximal LCx
(or 1st obtuse marginal or diagonal branch)
ST I, aVL (±V5,V6)

Inferior STEMI
Occlusion of PDA
ST II, III, aVF • Due to occlusion of the PDA
- PDA can be supplied by RCA ~85%, LCx ~15%, or even the terminal LAD (<5%)
• Can involve “posterior” wall - Due to occlusion of posterolateral branches - ST in V1-V3 (or ST in V7-V9)
• Consider RV infarction - Lead V4R (≥0.5mm ST)
RCA LCx

Anterior STEMI

Inferior STEMI

Anterior STEMI (with IVCD)

Anterior STEMI

Silent LCx

Lateral STEMI
Anterior STEMI
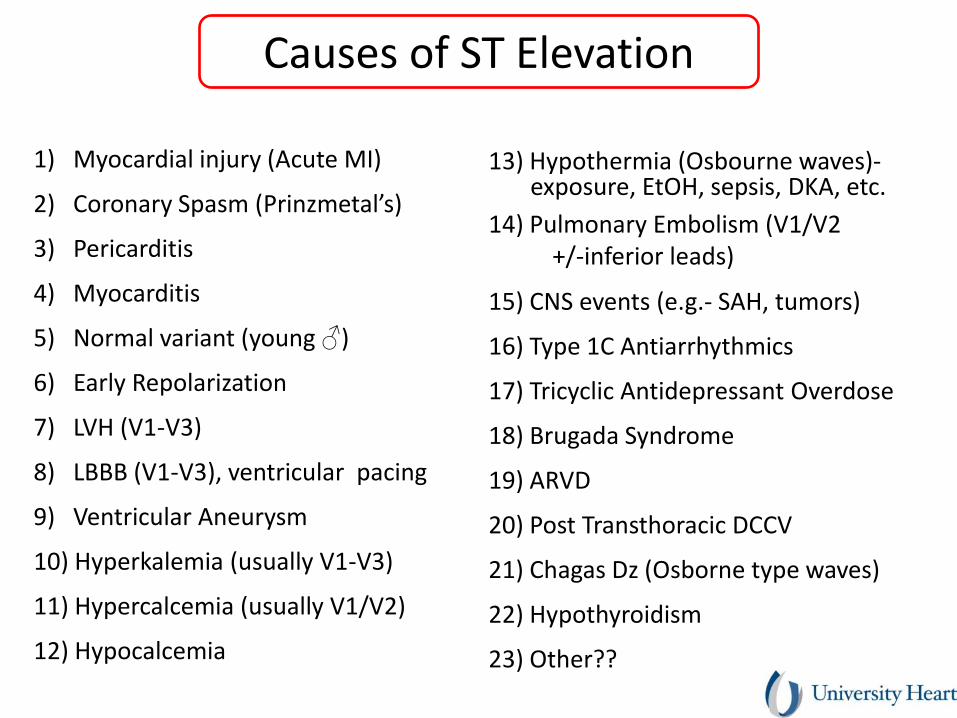
1) Myocardial injury (Acute MI)
2) Coronary Spasm (Prinzmetal’s)
3) Pericarditis
4) Myocarditis
5) Normal variant (young ♂)
6) Early Repolarization
7) LVH (V1-V3)
8) LBBB (V1-V3), ventricular pacing
9) Ventricular Aneurysm
10) Hyperkalemia (usually V1-V3)
11) Hypercalcemia (usually V1/V2)
12) Hypocalcemia
13) Hypothermia (Osbourne waves)- exposure, EtOH, sepsis, DKA, etc.
14) Pulmonary Embolism (V1/V2 +/-inferior leads)
15) CNS events (e.g.- SAH, tumors)
16) Type 1C Antiarrhythmics
17) Tricyclic Antidepressant Overdose
18) Brugada Syndrome
19) ARVD
20) Post Transthoracic DCCV
21) Chagas Dz (Osborne type waves)
22) Hypothyroidism
23) Other??
Causes of ST Elevation

Brady WJ et al. An Emerg Med 2001
Retrospective review of 902 adult pt’s c/o CP.
1) LVH with repolarization abnormality (25%)
2) LBBB with repolarization abnormality (15%)
3) Acute MI (15%)
4) Early repolarization (12%)
5) “undefined” BBB (5%)
6) LV aneurysm (3%)
7) Ventricular paced rhythm (1%)
8) Pericarditis (1%)
9) Other/Undefined (1%)
Statistics of ST in the ER

Condition ECG findings
Normal 1-2 mm concave ST V1-V3 (most in V2) Present in ~90% of healthy, young males
STEMI (Prinzmetal’s)
Convex ST with Reciprocal ST Corresponds to coronary region Evolves over time
Early repolarization
Concave ST, mostly precordial leads (most in V4) “Notch” at J point, resolves with exercise (HR) Usually tall R and T waves
Pericarditis Diffuse concave ST (usually just 1-3mm), PR (ST in aVR; V1 usually isoelectric) T waves don’t invert until ST’s back to baseline
LVH “with strain” V1-V2 with deep S waves, concave ST Other features of LVH (e.g. voltage)
Differentiating Causes of ST Elevation
• Clinical scenario
• Reciprocal ST depression
• Evolution over time (minutes)
• Wall motion on echo

Early Repol
Concave ST “notch” at J point Tall R’s and T’s

2006
2008
Still just Early Repol 2006
2006
2006 2006

Pericarditis
Diffuse, concave, ST (ST aVR)
PR
No loss of R waves (T’s don’t invert until ST’s at baseline)

LVH with “strain”
Concave ST in V1-V3 (assoc. with deep S wave)
Essentially opposite V4-V6 with tall R’s & ST

STEMI vs. Hyperkalemia
STEMI
K+
STEMI: T’s are broad, rounded, minimal ST segment
Hyperkalemia: T’s are narrow, pointy, discrete ST segment

STEMI with IVCD vs. Hyperkalemia
STEMI
K+
Clinical setting, QRS complexes of K+ run into each other

There are many causes of ST The majority are not STEMI’s
ECG’s are neither 100% sensitive nor specific for STEMI You will miss some STEMI’s, you will cath some normals
Sometimes your best just isn’t good enough
The clinical setting is the most important factor Common sense often rules the day
Symptoms, risk factors for CAD
ECG morphology can also be helpful, but not foolproof!! ST with STEMI is usually convex, regional, recip ST, dynamic
Beware subtle inferior STEMI’s!
Serial ECG’s can help keep you out of trouble
Summary





























