Embed Size (px)
Citation preview

ST Segment Elevation Myocardial Infarction
Elliott Antman, MD Cardiovascular Division
May 1, 2013
Disclosure
Accumetrics, Inc. Amgen, Inc. AstraZeneca Pharmaceuticals LP Baxter Bayer Healthcare LLC Beckman Coulter, Inc. Biosite Incorporated Bristol-Myers Squibb CardioKinetix CV Therapeutics, Inc. Daiichi-Sankyo Eli Lilly and Company FoldRx GlaxoSmithKline INO Therapeutics LLC Inotek Pharmaceuticals Corporation
The National Institutes of Health Integrated Therapeutics Corporation KAI Pharmaceuticals Merck & Co., Inc. Millennium Pharmaceuticals, Inc. Novartis Pharmaceuticals Nuvelo, Inc. Ortho-Clinical Diagnostics, Inc. Pfizer, Inc. Roche Diagnostics Corporation Roche Diagnostics GmbH Sanofi-Aventis Sanofi-Synthelabo Recherche Schering-Plough Research Institute St Jude Medical
The TIMI Study Group has received research / grant support in the past 2 yrs through the Brigham & Women’s Hospital with funding from (in alphabetical order):

127:e6-e245,2013
127:e362-425,2013

2013 STEMI GL
MI
NSTEMI
STEMI
Steiner C HCUP Projections Report # 2012-02.

Life’s Simple Seven
http://mylifecheck.heart.org
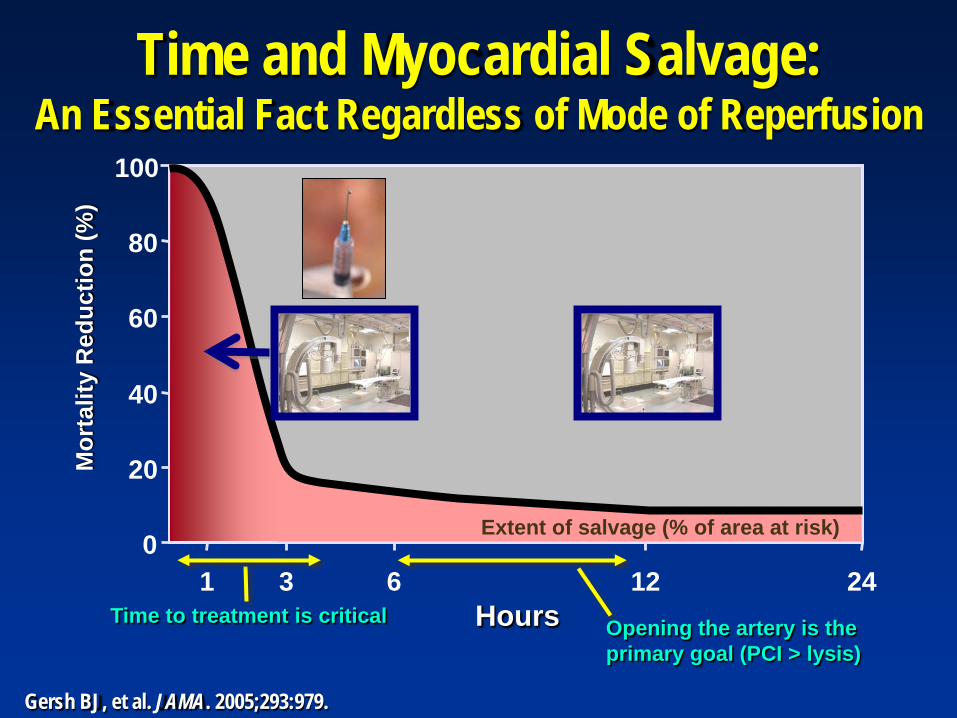
Time and Myocardial Salvage: An Essential Fact Regardless of Mode of Reperfusion
0
20
40
60
80
100
1 3 6 12 24 Hours
Mor
talit
y R
educ
tion
(%)
Extent of salvage (% of area at risk)
Time to treatment is critical Opening the artery is the primary goal (PCI > lysis)
Gersh BJ, et al. JAMA. 2005;293:979.

Checklist to Improve Door-Device Time
2013 STEMI GL

Door To Balloon Time and Mortality
NCDR---43,801 pts with STEMI In-Hospital Mortality after Prim PCI
Rathore BMJ 338: b1807,2009

Regional Systems of STEMI Care, Reperfusion Therapy, and Time-to-
Treatment Goals
All communities should create and maintain a regional system of STEMI care that includes assessment and continuous quality improvement of EMS and hospital-based activities. Performance can be facilitated by participating in programs such as Mission: Lifeline and the D2B Alliance.
I IIa IIb III
Performance of a 12-lead ECG by EMS personnel at the site of FMC is recommended in patients with symptoms consistent with STEMI.
I IIa IIb III
2013 STEMI GL

260 systems
Cardiac

Reperfusion Therapy for Patients with STEMI
2013 STEMI GL
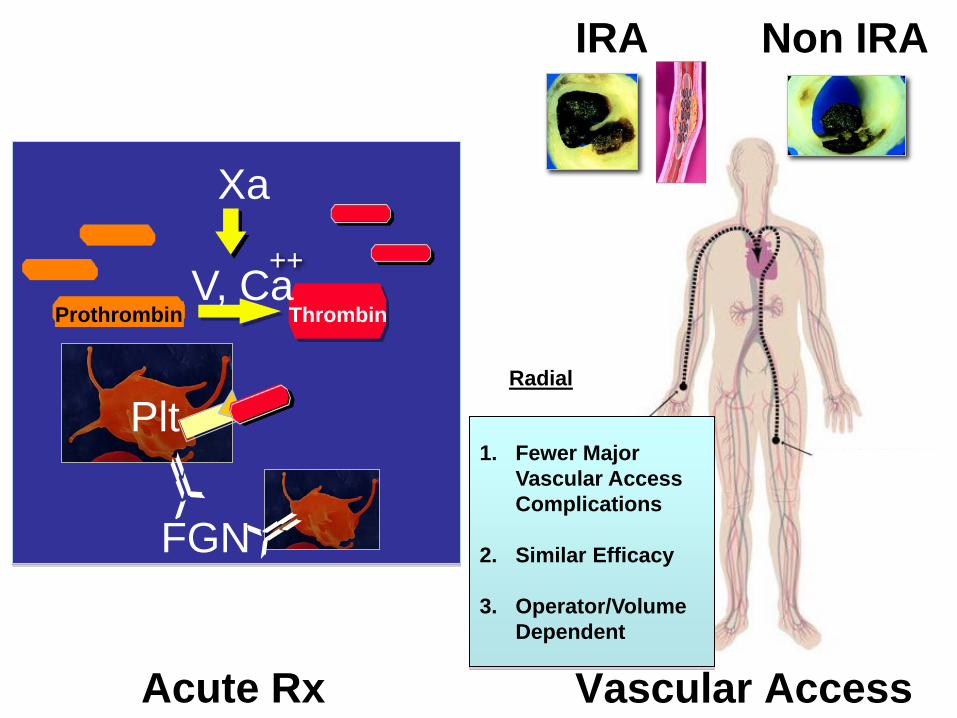
Vascular Access
1. Fewer Major Vascular Access Complications
2. Similar Efficacy
3. Operator/Volume Dependent
Radial
Prothrombin Thrombin
Xa
V, Ca ++
.
FGN
Plt
Acute Rx
IRA Non IRA

Prothrombin Thrombin
Xa
X TF/VIIa
V, Ca2+
Xa inhibitors LMWH UFH
LMWH UFH DTIs
WARFARIN
ASA P2Y12 inhib.
IV GP IIb/IIIa Inhibitor

Anticoagulant Scorecard UFH ENOX FONDA BIVAL
Route IV (SC) IV, SC SC (IV) IV
Monitor aPTT, ACT
No No aPTT, ACT
UA/NSTEMI Yes Yes Yes Yes
STEMI Yes Yes Yes Yes
Bleeding Yes Yes Less ? Less
PCI Yes Yes Need anti IIa Rx
Yes
CABG Yes No No Possible
Antidote Protamine Protamine None None

Antiplatelet Scorecard Clopidogrel Prasugrel Ticagrelor
Route PO PO PO
Monitor Uncertain Not Necessary
Dose LD,MD 600 / 75 mg 60/10 mg 180 / 90 mg BID
UA/NSTEMI Yes Yes Yes
STEMI Yes PCI PCI
Bleeding Yes Yes Yes
PCI DAPT with ASA
DC for CABG 5-7 days 7-10 days ? 2-3 days
Issues Irreversible Variable Resp.
Irreversible 5 mg MD ?
Reversible (Compliance)

Evolution of PCI for STEMI
Balloon Antiplatelet Rx
Stent
DES
GP IIb/IIIa Inhibitor
ASA P2Y12 inhib.
Thrombus Removal;
Embolization Protection
Devices Antman + Van de Werf Circ 109:2480,2004
I IIa IIb III
2013 STEMI GL
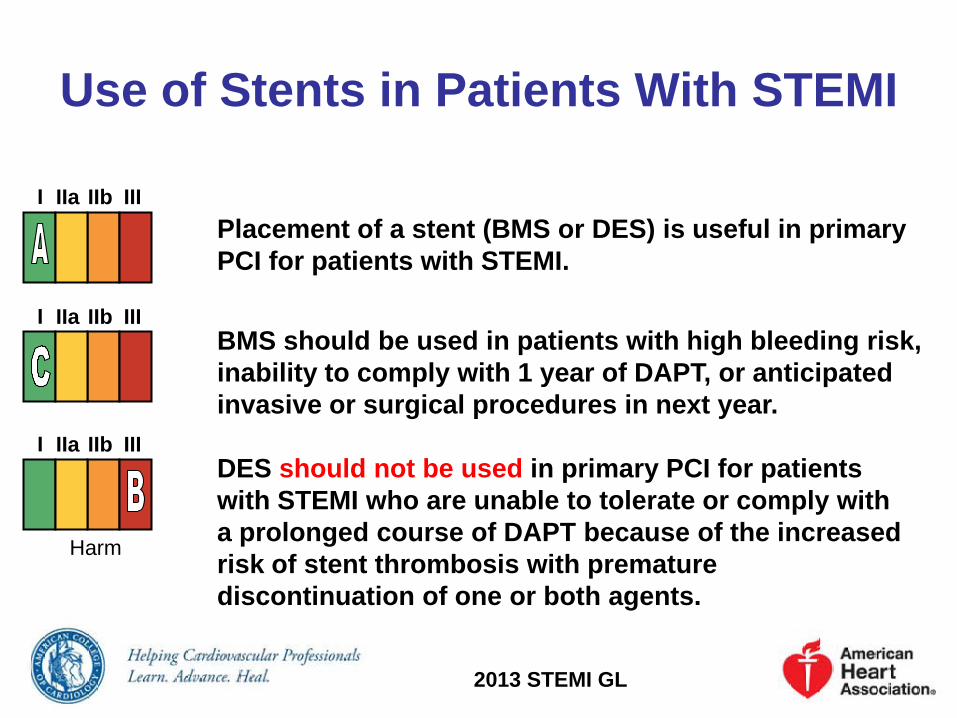
Use of Stents in Patients With STEMI
Placement of a stent (BMS or DES) is useful in primary PCI for patients with STEMI.
I IIa IIb III
BMS should be used in patients with high bleeding risk, inability to comply with 1 year of DAPT, or anticipated invasive or surgical procedures in next year.
I IIa IIb III
DES should not be used in primary PCI for patients with STEMI who are unable to tolerate or comply with a prolonged course of DAPT because of the increased risk of stent thrombosis with premature discontinuation of one or both agents.
I IIa IIb III
Harm
2013 STEMI GL

GP IIbIIIa Therapy to Support Primary PCI for STEMI
It is reasonable to start treatment with an intravenous GP IIb/IIIa receptor antagonist at the time of primary PCI (with or without stenting or clopidogrel pretreatment) in selected patients with STEMI who are receiving UFH.
• Double-bolus eptifibatide: 180 mcg/kg IV bolus, then 2 mcg/kg/min; a 2nd 180-mcg/kg bolus is administered 10 min after the 1st bolus.
• Abciximab: 0.25 mg/kg IV bolus, then 0.125 mcg/kg/min (maximum 10 mcg/min); or
• High-bolus-dose tirofiban: 25 mcg/kg IV bolus, then 0.15 mcg/kg/min; or
I IIa IIb III
I IIa IIb III
I IIa IIb III
2013 STEMI GL

Primary PCI in STEMI
2013 STEMI GL
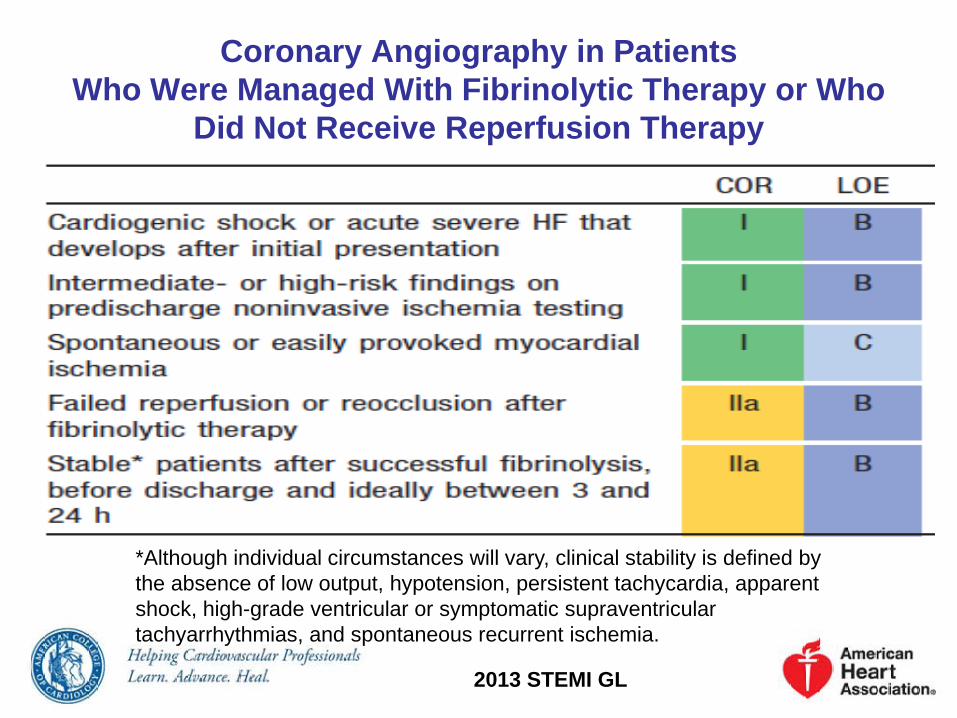
Coronary Angiography in Patients Who Were Managed With Fibrinolytic Therapy or Who
Did Not Receive Reperfusion Therapy
*Although individual circumstances will vary, clinical stability is defined by the absence of low output, hypotension, persistent tachycardia, apparent shock, high-grade ventricular or symptomatic supraventricular tachyarrhythmias, and spontaneous recurrent ischemia.
2013 STEMI GL

PCI of an Infarct Artery in Patients Who Were Managed With Fibrinolytic Therapy or Who Did Not Receive
Reperfusion Therapy
*Although individual circumstances will vary, clinical stability is defined by the absence of low output, hypotension, persistent tachycardia, apparent shock, high-grade ventricular or symptomatic supraventricular tachyarrhythmias, and spontaneous recurrent ischemia.
2013 STEMI GL

Beta-Blockers
Oral beta-blockers should be initiated within 1st 24 h for pts without contraindications
I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III IIa IIa IIa IIb IIb IIb III III III
It is reasonable to administer intravenous beta blockers at presentation for hypertension to pts without contraindications
I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III IIa IIa IIa IIb IIb IIb III III III
Containdications: 1) signs of HF 2) evidence of a low-output state, 3) increased risk for cardiogenic shock (Age >70,SBP < 120, HR> 110 or < 60, prolonged time from onset of symptoms) 4) other relative contraindications (PR > 0.24 s, 2nd or 3rd degree heart block, active asthma, or reactive airway disease).
Patients w initial contraindications to use of beta blockers in first 24 h should be reevaluated to determine subsequent eligibilty
I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III I I I IIa IIa IIa IIb IIb IIb III III III IIa IIa IIa IIb IIb IIb III III III
2013 STEMI GL

“Warning Arrhythmias”
(From Antman EM, Rutherford JD: Coronary Care Medicine. Boston, Martinus Nijhoff Publishing, 1986)
K 4.5 Mg 2.0

Combined Conduction Defects
Anterior MI with RBBB, LAFB
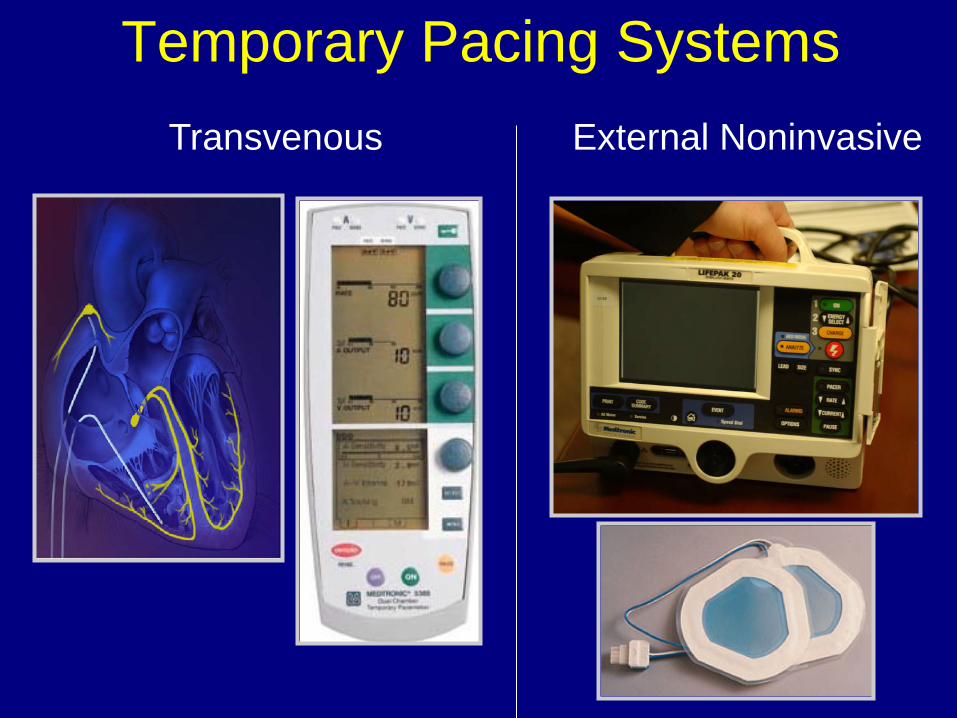
Temporary Pacing Systems Transvenous External Noninvasive

Primary Prevention of SCD ICD Implantation After STEMI
At Least 40 days After STEMI; No Spontaneous VT or VF 48 hours post-STEMI
Assess LVEF and NYHA Functional Status
No ICD
LVEF > 40%
ICD
LVEF < 30-40% NHYA Class II-III
LVEF < 30-35% NHYA Class I
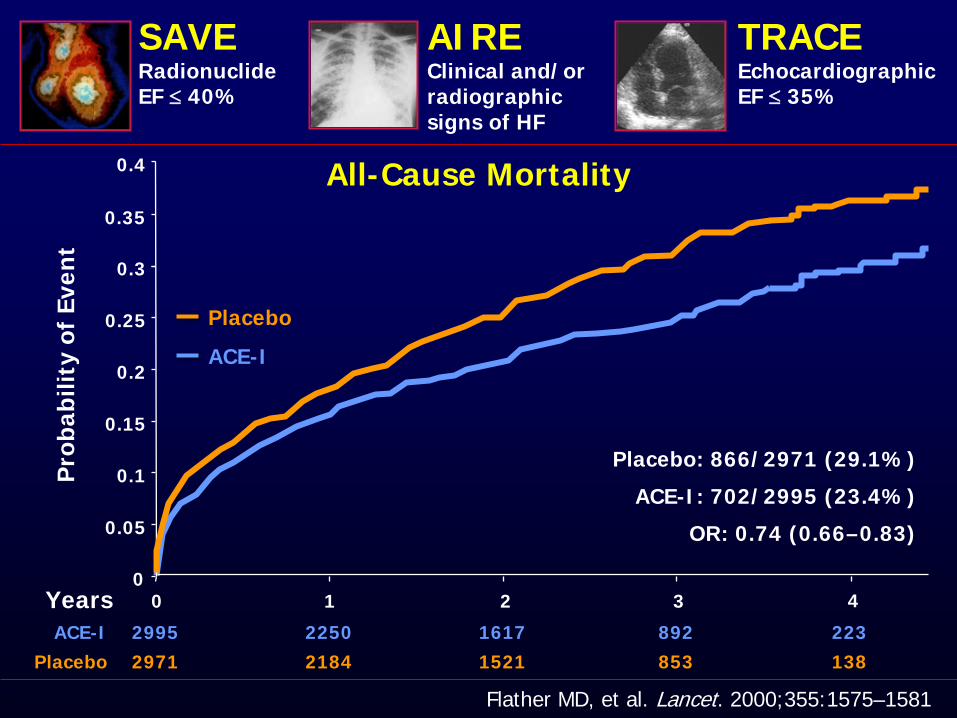
All-Cause Mortality
Years
Pro
babi
lity
of E
vent
0
0.05
0.1
0.15
0.2
0.25
0.3
0 1 2 3
0.35
0.4
4
ACE-I
Placebo
ACE-I 2995 2250 1617 892 223 Placebo 2971 2184 1521 853 138
Flather MD, et al. Lancet. 2000;355:1575–1581
OR: 0.74 (0.66–0.83)
ACE-I: 702/2995 (23.4%)
Placebo: 866/2971 (29.1%)
TRACE Echocardiographic EF ≤ 35%
AIRE Clinical and/or radiographic signs of HF
SAVE Radionuclide EF ≤ 40%
4
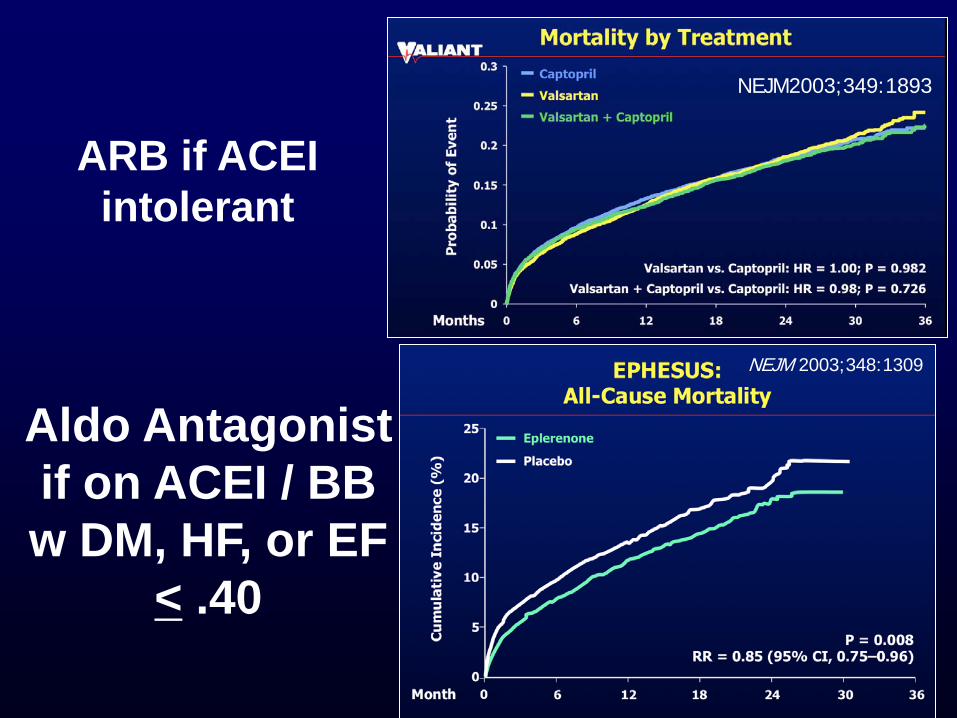
ARB if ACEI intolerant
Aldo Antagonist if on ACEI / BB w DM, HF, or EF
< .40
NEJM 2003;348:1309
NEJM2003;349:1893
Management of LV Dysfunction
• General Ventilation Correct Acidosis Anticoagulation
• Pharmacologic Support Inotropes Vasopressors Vasodilators
• Revascularization
• Mechanical Support

Right Ventricular Infarction Clinical findings:
Shock with clear lungs, elev JVP Kussmaul sign
Hemodynamics: Increased RA pressure (y descent) Square root sign in RV tracing
ECG: ST elev in R sided leads
Echo: Depressed RV function
Rx: Maintain RV preload Lower RV afterload (PA---PCW) Inotropic support Reperfusion
V4R Wellens NEJM 340: 381,1999

Ventricular Septal Rupture
Mitral Regurgitation (Pap. M. dysfunction)
Incidence 1-2% 1-6% 1-2% Timing 3-5 d p MI 3-6 d p MI 3-5 d p MI Phy Exam murmur 90% JVD, EMD murmur 50% Thrill Common No Rare Echo Shunt Peric. Effusion Regurg. Jet PA cath O2 step up Diast Press Equal. c-v wave in PCW
Images:Courtesy of W D Edwards (Mayo Foundation) Data: Lavocitz CV Rev Rpt 5:948,1984; Birnbaum NEJM 347:1426 ,2002
Free Wall Rupture

Aneurysm Formation after STEMI
From Shah PK “ Complications of acute MI” In Cardiology (Parmley et al 1987)

Regeneration of the Myocardium
Source
Endpoint(s) of Trial
Preparation
Timing
Delivery System
Duration of Followup
Enhancement Strategies
Dimmeler Circ 121:325, 2010

Myoblasts
Bone-Marrow Derived Cells
Mesenchymal Stem Cells
Cardiac Progenitor
Clinical Trials of Cardiac Regeneration
Siu + Tse Lancet 379:870, 2012

Dimmeler AHA 2012

SCIPIO
Absolute Change in EF
% Change in Viable Tissue in Infarct Region by CMR
12 Month Data: Lancet 2011;378:1847 24 Month Data: R. Bolli AHA 2012

SCIPIO
Change in NYHA Score
Change in Minnesota HF Score
12 Month Data: Lancet 2011;378:1847 24 Month Data: R. Bolli AHA 2012

Δ Scar Mass (g) 12 mos.
CADUCEUS
Δ Viable Mass (g) 12 mos.
Systolic Wall Thickening (%)
6 mos.
Makkar RR et al Lancet 379: 895, 2012
All bars represent +/- 1 SEM
Controls CDCs
-20
-10
0
10
20
p = 0.02
-30
-15
0
15
30
p = 0.001
0
20
40
60
p = 0.015

Secondary Prevention and Long Term Management
Smoking Goal: Complete Cessation
Blood pressure control: Goal: < 140/90 mm Hg
Physical activity: Goal:30 minutes minimum 5 days per week;Optimal daily
Diabetes: Goal: HbA1c < 7%
Weight management: Goal:BMI 18.5 -24.9 Waist circumference: Women: < 35 in. Men: < 40 in.
Circ 124: 2458, 2011
NSAIDs: Stepped Care Approach
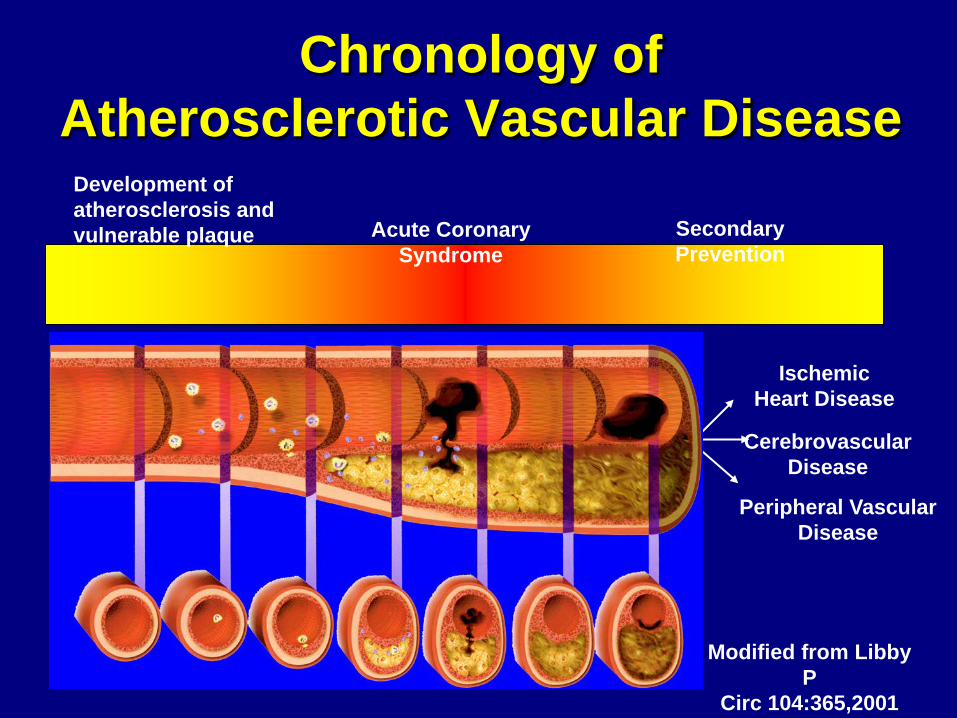
Chronology of Atherosclerotic Vascular Disease
Development of atherosclerosis and vulnerable plaque Acute Coronary
Syndrome Secondary Prevention
Ischemic Heart Disease
Cerebrovascular Disease
Peripheral Vascular Disease
Modified from Libby P
Circ 104:365,2001




























