Embed Size (px)
Citation preview

Conflitto d’interesse:Contratto con Biosense Webster per
lo sviluppo di nuove tecnologie
Ospedale “F. Miulli”
Acquaviva delle Fonti - Bari
Massimo Grimaldi
Cardiologia Universitaria
Foggia
Spunti di innovazione tecnologica nell’ablazione della fibrillazione atriale

100 pazienti con FA ( 51 parossistica) sottoposti ad ablazione ostiale o circonferenziale
84% recidive
97 % recidiva di conduzione di 1.8 +1 (circonferenziale) vs 1.9 +0.8 (ostiale) delle vene
Am Heart J, 2004

Perché l’ablazione di fibrillazione atriale è difficile
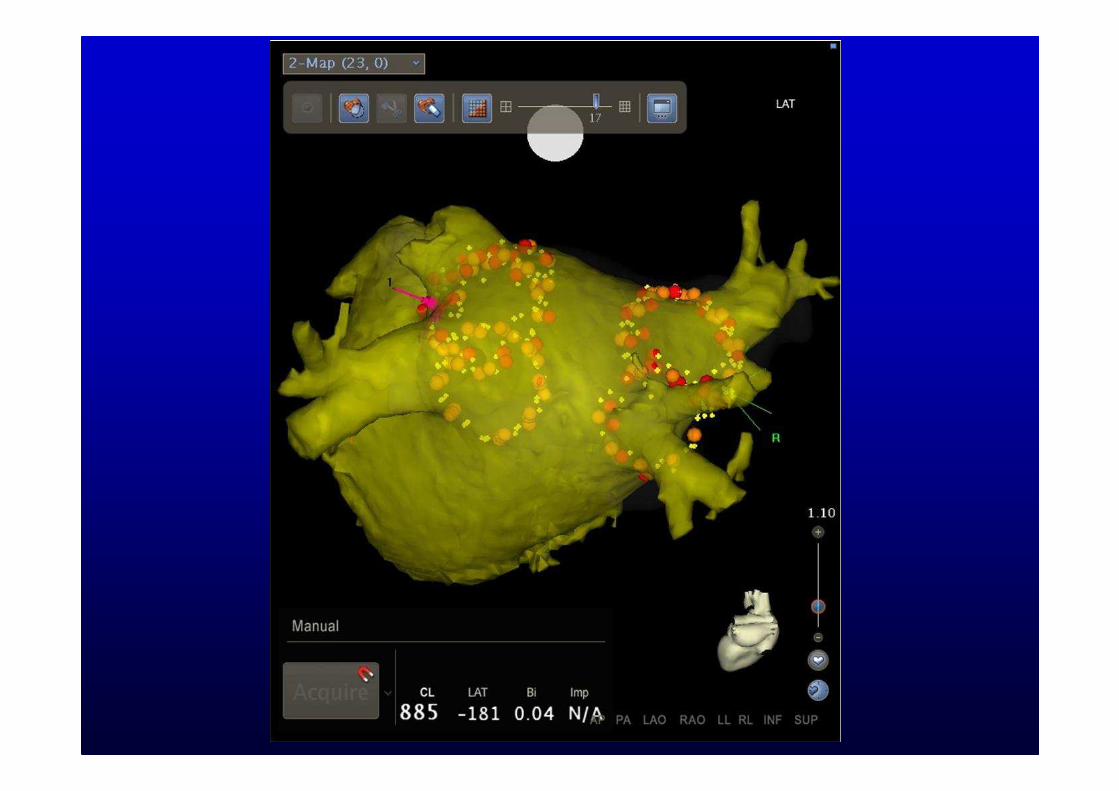
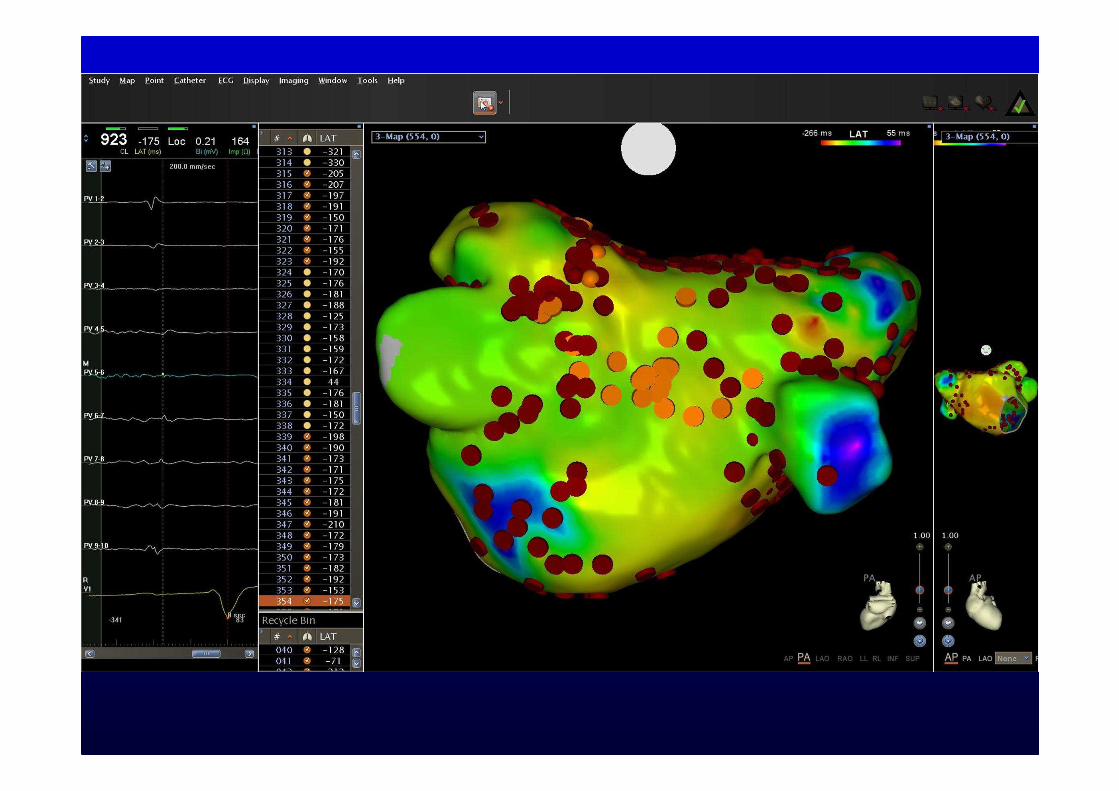
Corretto riconoscimento delle strutture anatomiche
Corretta interpretazione dei potenziali elettrici
Posizionamento dell’elettrodo ablatore
Stabilizzazione dell’elettrodo ablatore
Applicazione della RF con la giusta forza sul tessuto e per il giusto tempo

Crio Pallone

Nuova tecnologia

Arctic Front 174,0 113,8 45,3
Arctic Front Advance (US) 146,4 93,8 36,1
Arctic Front Advance (EU) 129,0 85,0 24,0
Dati Medtronic al 20 Nov 2012; AFB: N = 7787; AFA US: N = 865; AFA EU: N = 390
Tempi procedurali e di fluoroscopia


Assenza di recidive a 12 mesi
Andrade, Heart Rhythm 2011
Assenza di recidive a 12 mesi: 72,8 %Assenza di differenze statisticamente significative con RF

Europace, Feb 2013

COMPLICANZE

Laser Ballon lesione video-guidata
ENDOSCOPIC VIEW
Aiming ArcPV

§ VGLB– 2nd Generationl Compliant, adjustable diameterl 2Fr endoscopel 300 adjustable aiming arcl Diode laser (980nm) for ablation
VGLB – 2nd Generation

Studio in vivo
RSPV
LSPV
Ablation Lesions
Chronic Histology (10 PVs/120 sections)
• Circumferentiality 100%
• Transmurality = 99.0±5.5%
• 96.7% of sections were transmuralDukkipati SR, d’Avila A, Reddy VY et al.
Circ Arrhythm Electrophysiol. 2010,3:266-73




Heart Rhythm 2012; 9: 919–925
N = 56
# PV Isolated (%) 202/206 (98.1%)# Attempts to isolate/PV, mean 1.3
Fluoroscopy Time, mean±sd, min (limits) 23±15 (7 – 85)
# Ablation Lesions per Patient, mean±sd 143±33
Ablation Time, mean±sd, min (limits) 113±38 (46 – 221)
Procedure Time, mean±sd, min (limits) 198±43 (120 – 285)
# Catheters per Patient 1.05

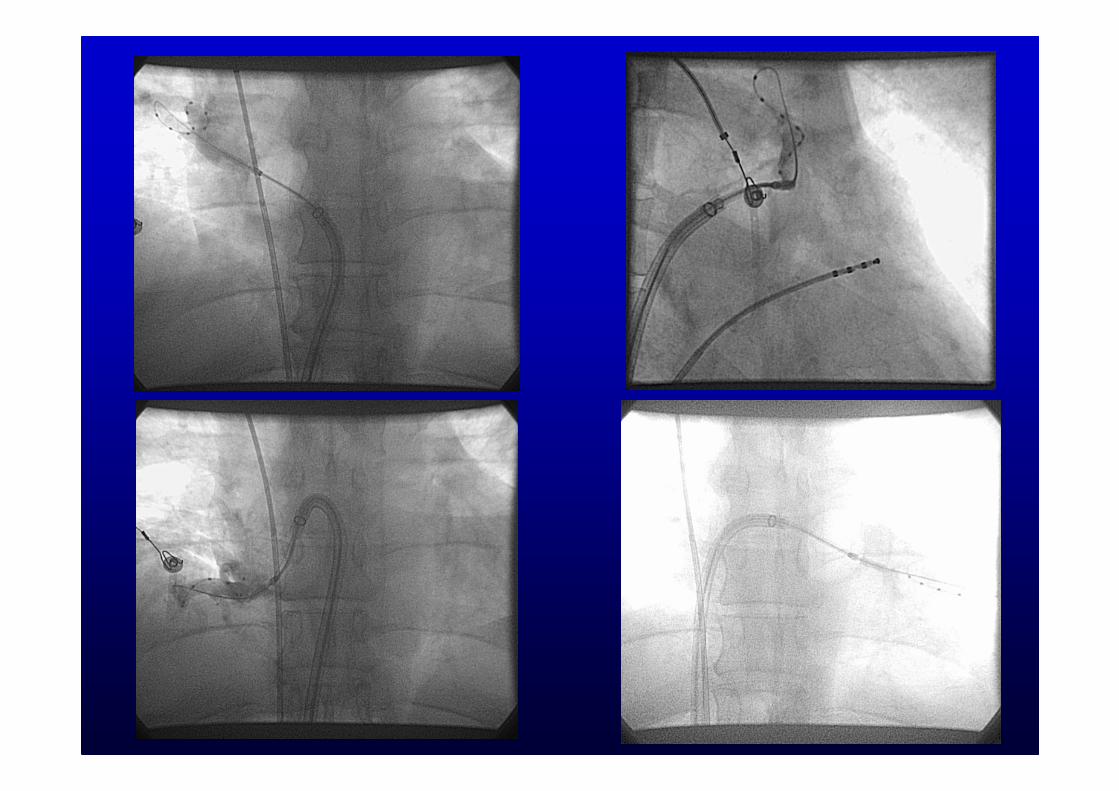
Catetere ablatore circolare con tecnologia “over the wire”
10 elettrodi eroganti radiofrequenza unipolare e bipolareGeneratore di radiofrequenza dedicato

1 Bittner, A.,Randomized study comparing duty-cycled bipolar and unipolar radiofrequency with point by point ablation in PVs isolation, HR
2011.
2. Choo WK, Experience of AF Ablation in a New Cardiac Centre using 3D Mapping and Multielectrode Duty-Cycled RFCA.ArchCardiovascDis 2011
3. Bulava A, Catheter Ablation for PAF: A Randomized Comparison between Multielectrode Catheter and Point-by-Point Ablation. PACE 2010
4. Rypko J. PV isolation to treat PAF: conventional versus multi-electrode RFCA, J Int C Elect 2012
Efficacia in studi randomizzati

Radiofrequency Catheter Ablation of Atrial Fibrillation: A Cause of Silent Thromboembolism?
Gaita, Circulation 2010
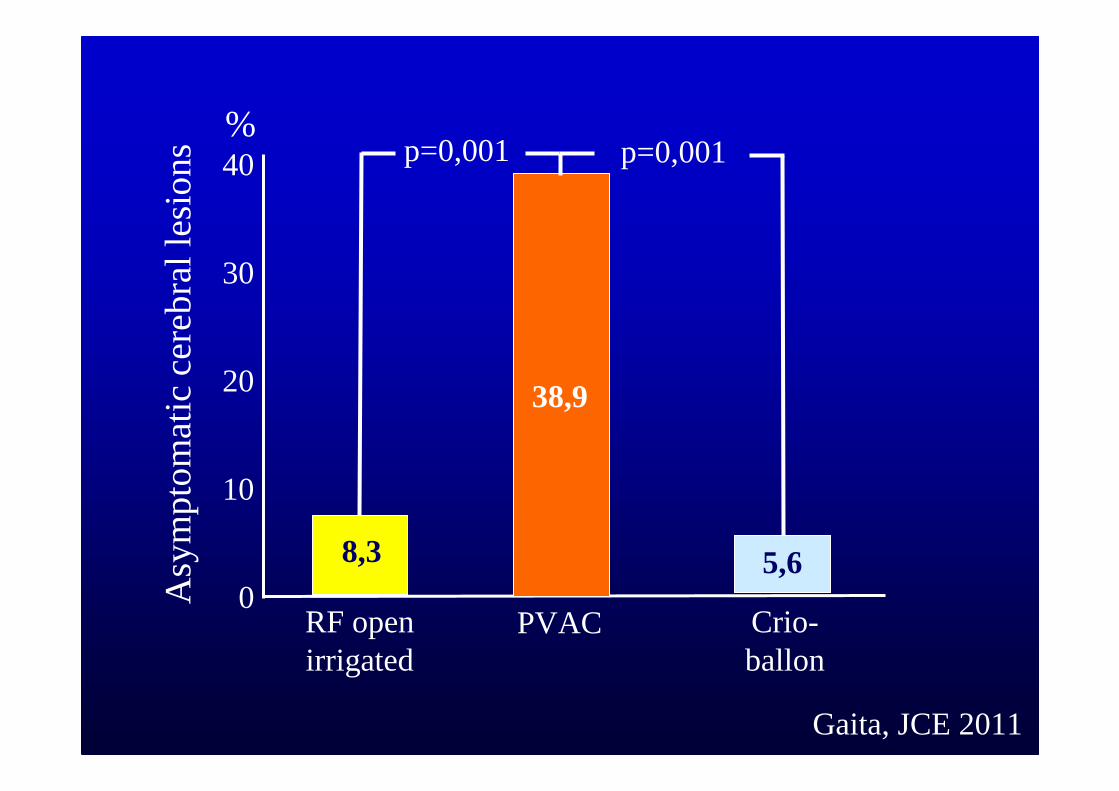
Gaita, JCE 2011
0
40
30
20
10
RF open irrigated
PVAC Crio-ballon
p=0,001
38,9
%
Asy
mp
tom
atic
cer
eb
ral l
esio
ns
8,3 5,6
p=0,001

Rilievo di lesioni cerebrali silenti in 33 di 86 pazienti (38%)Numero medio di lesioni per paziente: 3,6
Esame neurologico normale in tutti i pazienti
Heart Rhythm, 2011

Ablatore circolare a radiofrequenza unipolare e bipolare irrigata

Unipolar vs bipolar RF lesions
Uni 25W 25W
Bi 15W 15W

#67604 R4
Distal Distal
- Depth at Distal Electrode: 5.2 mm- Depth at Proximal Electrode: 5.3 mm- Lesion Length (Long Axis Diameter): 14.0 mm- Lesion Width (Short Axis Diameter): 7.9 mm
Unipolar and Bipolar Ablation
Long Axis TransactionShort Axis Transactionat Max Depth PortionSurface


Visualizzazione del catetere mediante sistema di mappaggio
Radiofrequenza unipolare Radiofrequenza bipolare



Posterior box isolation

Posterior wall dissociated beat

REVOLUTION Investigators
BELGIUMMattias Duytschaever, MD. Brugge
CZECHJosef Kautzner, MD. Prague
DENMARKPeter Steen Hansen, MD. Värde
FRANCE
Christian De Chillou, MD. Nancy
Pierre Jaïs, MD. Pessac
GERMANY
Gerhard Hindricks, MD. Leipzig
ITALY
Claudio Tondo, MD. Milan
Massimo Grimaldi, MD. Bari

Results – Acute Effectiveness
Site # of PV targets (%)
Site 01 24/32 (75%)
Site 02 59/59 (100%)
Site 03 12/12 (100%)
Site 04 35/51 (68.6%)
Site 05 102/111 (92%)
Site 06 3/4 (75%)
Site 07 39/78 (50%)
Site 08 107/107 (100%)
All Sites 381/454 (84%)
Results shown for effectiveness cohort; generator version 2.0
Targets successfully isolated without the use of focal touch-up

Results – Acute EffectivenessAcute Pulmonary Vein Isolation documented by confirmed entrance block
N=111
ACUTE SUCCESS 110/110* (100%)
First Ablation 110/110 (100%)
Second Ablation 16/16 (100%)
Third Ablation 2/2 (100%)
Results shown for effectiveness cohort; generator version 2.0
*Missing data for 1 patient
Confirmation of first ablation PVI with:Circular nMARQ 57.7% LASSO 36.0%Other 6.3% (crescent, combination of circular and
crescent, thermocool)

Results – Primary Endpoint -Safety
Cardiac Tamponade 2/161 (1.2%)
Diaphragmatic paralysis 1/161 (0.6%)
TIA 1/161 (0.6%)
Hospitalization 5/161 (3.1%)
Injection site hematoma 1/161 (0.6%)
Headache 1/161 (0.6%)
Inguinal hematoma 1/161 (0.6%)
Atrial flutter 1/161 (0.6%)
Artery-venous fistula 1/161 (0.6%)
Pericardial Effusion 1/161 (0.6%)
Early Onset Primary AEs 10/161 (6.2%)

Barium

RIPV
Unipolar RF: 18 WBipolar RF: 15 W
Stop RF
Time (seconds)
Temp. (°C)

Posterior wall
Unipolar RF: 18 WBipolar RF: 15 W
Temp. (°C)

Objective:
Evaluation for evidence of intracerebral microemboli and associated neurological deficits following RF ablation
Methods:
nMARQTM (test-group) vs. NAVISTAR® THERMOCOOL®
(control group)
Pre-ablation neurological examination and MRI
<48 hour pre-ablation
Post-ablation neurological examination and MRI
during day 1-2 post-ablation
REVOLUTION – Subpopulation Neurological Assessment (SNA)

Results Hospital F. Miulli:
REVOLUTION – Subpopulation Neurological Assessment (SNA)
nMARQTM (*) THERMOCOOL® New neurological findings post-ablation
0/12 (0%) 0/11 (0%) None
SNA population 100% lesion-free. No subjects observed with intracerebral microembolic lesions post-ablation
No new neurological deficits observed post-ablation
(*) Subjects on WarfarinTarget INR ≥ 2.0Target ACT≥325s

Acute safety and efficacy of a novel multipolar irrigated radiofrequency ablation catheter for pulmonary vein isolation
Lesioni silenti nel 33% dei pzDiametro medio 2,3 mm (1-9 mm)
Deneke, JCE 2013

Esophago-pericardial fistula complicating atrial fibrillation ablation using a novel irrigated radiofrequency multipolar ablation catheter
Deneke, JCE 2013

CONCLUSIONI
Nella terapia ablativa della fibrillazione atriale le nuove tecnologie devono garantire la sicurezza prima dell’efficacia
Malgrado le nuove tecnologie, l’efficacia e la sicurezza sono ancora operatore dipendenti:
L’operatore accorto impara dai propri erroriL’operatore stolto non impara dai propri erroriL’operatore saggio impara dagli errori degli altri
Nell’ablazione della fibrillazione atriale la prima prevenzione dell’errore nasce dal corretto inquadramento del paziente e dalla corretta indicazione ad eseguire l’ablazione, che non sempre è la scelta migliore





























