Embed Size (px)
Citation preview

43ISSN: 2171-4703© 2014 SECOIRSociedad Española de Cirugía Ocular Implanto-Refractiva
Spontaneous acute corneal hydrops in a patient with previously undetected unilateral
pellucid marginal degenerationBlanco Domínguez I, MD1; Garcia-Valcarcel Gonzalez B, MD1; Rojas Lozano P, MD1;
Baeza Autillo A, MD1; Balado Vazquez P, MD1
ABSTRACT: Acute corneal hydrops is a rare complication caused by a rupture in Descemet’s membrane as a result of progressive corneal thinning, normally due to advanced forms of corneal ectatic disorders.We report a case of unilateral pellucid marginal degeneration (PMD) which presented as acute corneal hydrops in a 56-year-old woman with no history of ocular or systemic disease.
J Emmetropia 2014; 5: 43-46
Submitted: 09/16/2013Revised: 01/19/2014Accepted: 02/04/20141 Corneal and Ocular Surface section; Department of Ophthalmology. Hospital General Universitario Gregorio Marañón, Madrid, Spain.
Financial disclosure: The authors do not have any financial interest in any of the products mentioned.
Corresponding Author: Irene Blanco Domínguez. Oftalmología Hospital General Universitario Gregorio Marañón. C/ Doctor Esquerdo, nº 46, 28007, Madrid, Spain.E-mail: [email protected]
CASE REPORT
Pellucid marginal degeneration (PMD) is a rare, bilateral, slowly progressing, non-inflammatory corneal ectatic disorder, characterised by inferior corneal thinning and transparency of the affected tissue1-6.
Acute corneal hydrops is an uncommon complication in clinical practice. It can occur in different corneal ectatic disorders, normally in advanced forms, but it is unusual for it to appear in a situation without underlying corneal disease.
CASE REPORT
A 56-year-old woman with no significant systemic or ophthalmological history was referred from the emergency department with a 24-hour history of pain, hyperaemia and intense photophobia in the left eye (OS), accompanied by loss of vision (uncorrected visual acuity [uVA] 0.05; 1.00 in the contralateral eye [decimal]). She did not report any previous trauma or other possible causes.
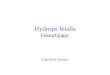
Biomicroscopy of the OS showed an ectatic area in the inferior peripheral cornea with localised oedema and intact epithelium. There were no areas of vascularisation, lipid or haemosiderin deposits. A crescent-shaped band of scarring was observed in the upper edge of the affected area. The central corneal thickness was normal and sensitivity was not compromised. The anterior segment of the right eye (OD) was normal (Figure 1).
Topography (Zeiss Humphrey Systems Atlas Version A11.2) could not initially be performed in the OS due to the condition of the cornea. Astigmatism of 0.25 dioptres (D) was detected in the OD (k1: 42.37 D 90°; k2: 42.12 D 180°), with no criteria for ectasia (corneal irregularity measurement [CIM]: 1.20; Shape Factor [SF]: 0.25; toric corneal measurement [TKM]: 43). Nevertheless, it should be noted that both the CIM and TKM values were just within the reference ranges (Figure 2).
A diagnosis of corneal hydrops in inferior keratectasia was made, and conservative topical treatment with various eyedrops was initiated, as follows: medroxyprogesterone acetateandtetryzoline hydrochloride (Colircusi Medrivas® eyedrop solution 20/5 mg/ml, Alcon Cusí S.A.), one drop every 6 hours; sodium chloride (Colircusi® Antiedema eyedrop solution 50 mg/ml, Alcon Cusí S.A.), one drop every 4 hours; timolol maleate (Timoftol® 0.5%, MSD de España S.A.), one drop every 12 hours; moxifloxacin hydrochloride (Vigamox® 5 mg/ml, Alcon Cusí S.A.), one drop every 8 hours; and hydration with ocular lubricants (Vitadrop®, Laboratorios Llorens S.A. and Lacrilube®, Allergan S.A.), alternating every 4 hours. After two weeks of treatment, the patient

44
JOURNAL OF EMMETROPIA - VOL 5, JANUARY-MARCH
showed clinical improvement, Medrivas® tapering was therefore commenced (decrease of 1 drop every 7 days). The Vigamox® eyedrops were discontinued one week later. The other treatments were continued until the hydrops had completely resolved, approximately 10 weeks later (Figure 3).
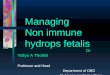
After resolution of the oedema, topography of the OS was performed (Zeiss Humphrey Systems Atlas Version A11.2), revealing a butterfly pattern characteristic of PMD, with corneal flattening along the vertical meridian and an increase in the horizontal curvature with inferior prolongation (astigmatism of 20.5 D; k1:34.50 D 100°; k2:55 D 10°). The patient presented criteria for keratectasia (CIM: 9.05; SF: 0.69 and TKM: 47.3) (Figure 4).
The final diagnosis was acute corneal hydrops in unilateral PMD. After the hydrops had resolved, the patient’s corrected VA was 0.40 in the OS, while uncorrected vision in the OD remained at 1.00 (decimal).
DISCUSSION
PMD is, by definition, a bilateral, often asymmetric condition3,4,6. Although, unilateral cases, such as that observed in our patient, have been described, there is usually topographic evidence of PMD or another ectatic disorder in the contralateral eye3. This case therefore is a rare, atypical form of PMD. One of the few references in the literature is the case described by Toriyama et al.2
Recent studies suggest that the condition is more prevalent in males, and usually occurs in the fourth or fifth decade of life, manifesting as decreased visual acuity due to against-the-rule astigmatism3.
On biomicroscopy, PMD appears as a peripheral sulcus (1/3 or less of the normal thickness), at a distance of about 2-4 mm parallel to the lower limbus, typically at between 4 and 8 o´clock, with intact epithelium and preserved corneal sensitivity. The peripheral cornea between the limbus and sulcus is clear, non-leucomatous and free of lipid deposits and
Figure 1. Biomicroscopy A) Normal anterior segment of the OD. B) Image of keratectasia and hydrops in the OS. C) Amplification of the image of the hydrops with a slit lamp section.
Figure 2. A) Keratometry and Placido discs images of the OD, showing a regular cornea. B) Topography of the OD showing a nor-mal surface pattern.
Figure 3. A) Biomicroscopic appearance of the OS after hydrops resolution. B) The same image with a slit lamp section, allowing a clearer view of the area of inferior corneal thinning and ectasia.
CASE OF CORNEAL HYDROPS IN UNILATERAL PMD

JOURNAL OF EMMETROPIA - VOL 5, JANUARY-MARCH
45
vascularisation. The appearance and thickness of the central cornea remain normal, protruding just above the area of thinning, and may be depressed or ectatic at the junction2-6. Some authors have described a deep crescent-shaped band of corneal scarring along the upper edge of the sulcus4.
These features must be taken into account to make a good differential diagnosis, allowing to rule out other ectatic phenomena, such as keratoconus or Terrien’s marginal degeneration (Table 1).
A pattern of against-the-rule astigmatism with vertical oval distribution of Placido mires is confirmed on topography. The horizontal “butterfly wings” at the maximum horizontal curvature are deflected downwards to form a notch and attach to the inferior peripheral areas of the maximum curvature to form the so-called “loop cylinder”. Peripheral compression of the lower mires causes the lower flattened vertical sector to close in a “teardrop” shape, while the upper sector fans out4.
Corneal hydrops is caused by a gradual build-up in pressure that eventually produces a tear in the Descemet’s membrane that enlarges with the influx of aqueous humour into the stroma. The patient experiences pain, significant photophobia and loss of vision. In most cases, it is a self-limiting process that tends to resolve fully within 6 weeks to 6 months5. The endothelial barrier is gradually restored by polymorphism and polymegathism induced by
Figure 4. A) Keratometry and Placido discs images of the OS, show-ing an irregular cornea with severe against-the-rule astigmatism of 20.5D. B) Topography of the OS showing corneal flattening along the vertical meridian with an increase in the “butterfly wing” hori-zontal curvature.
Table 1. Typical characteristics (mainly biomicroscopic) of pellucid marginal degeneration (PMD), keratoconus and Terrien’s marginal degeneration for differential diagnosis of ectatic disorders
PMD Keratoconus Terrien’s marginal degeneration
Typical location of thinning
Peripheral sulcus parallel to the inferior limbus, around 2-4 mm from
same, typically between 4 and 8 o´clock
Central or just below the visual axis
Superior or superior nasal, separated from the limbus by
a narrow transparent area
Central corneal thickness Usually unchanged Central corneal thinning
Unchanged
Corneal sensitivity Unchanged May be decreased Decreases in the sulcus and is suppressed in
the ectatic area, usually unchanged in the centre
Vogt’s striae Absent Present AbsentFleischer´s ring Absent May be present at
the base of the coneAbsent
Vascularization Absent (except hydrops sequelae)
Absent (except hydrops sequelae)
Present
Lipid deposits Absent Absent Present
CASE OF CORNEAL HYDROPS IN UNILATERAL PMD

46
JOURNAL OF EMMETROPIA - VOL 5, JANUARY-MARCH
REFERENCES
1. Vanathi M, Behera G, Vengayil S, Panda A, Khokhar S. Intracameral SF6 injection and anterior segment OCT-based documentation for acute hydrops management in pellucid marginal corneal degeneration. Cont Lens Anterior Eye. 2008; 31:164-6.
2. Toriyama K, Inoue T, Suzuki T, Higashiura R, Maeda N, Ohashi Y. Spontaneous Bleb Formation in a Presumed Pellucid Marginal Corneal Degeneration With Acute Hydrops. Cornea. 2013; 32:839-41.
3. Jinabhai A, Radhakrishnan H, O’ Donnell C. Pellucid corneal marginal degeneration: A review. Cont Lens Anterior Eye. 2011; 34:56-63.
4. Barraquer RI. Distrofias y degeneraciones corneales. Atlas y Texto.Barcelona: Espaxs; 2004:317-26.
5. Kaushal S, Sharma N, Vajpayee RB. Treatment of acute corneal hydrops with intracameral C3F8 in a patient of pellucid marginal degeneration with keratoglobus. Clin Exp Ophthalmol. 2007; 35:697-9.
6. Taboureau E, Berthout A, Turut P, Milazzo S. Acute spontaneous corneal hydrops in a patient with pellucid marginal corneal degeneration. J Fr Ophtalmol. 2006;29:e13.
7. Carter JB, Jones DB, Wilhelmus KR. Acute hydrops in pellucid marginal corneal degeneration. Am J Ophthalmol. 1989;107:167-70.
8. Lucarelli MJ, Gendelman DS, Talamo JH. Hydrops and spontaneous perforation in pellucid marginal corneal degeneration. Cornea. 1997; 16:232-4.
9. Poyales-Galán F, Fernández-Aitor-García A, Garzón-Jiménez N, Ortiz-De-Zárate B, Elipe-Gosálvez V. Tratamiento de la rotura de la membrana de Descemet mediante SF6 intracamerular en Hydrops agudo. Arch Soc Esp Oftalmol. 2009; 84:533-6.
First author:
Irene Blanco Domínguez, MD
Hospital General Universitario Gregorio Marañón, Madrid, Spain
healthy neighbouring endothelial cells in the affected area, repairing the defect and allowing regeneration of Descemet’s membrane5, 8, 9. It can be associated with complications such as perforation, infection, malignant glaucoma, corneal neovascularisation and residual leukomas1, 5. Only 27% of patients with ectasia who do not undergo surgery after an episode of acute hydrops maintain an acceptable range of VA1.
Medical treatment is basically symptomatic, although attempts can be made to improve the healing time. New therapeutic options involving the intracameral injection of gases such as SF6 or C3F8 have recently been described. These aim to reposition the Descemet’s membrane against the stroma, thereby reducing symptom duration1, 5, 6, 9.
In all the articles on corneal hydrops in PMD that we reviewed1, 2, 5-8, patients were being monitored for an ectatic disorder or had a previous history of severe astigmatism in the affected eye. This case is remarkable in that there was no history of disease, no known astigmatism and no history of optical correction. Furthermore, the patient was unaware of any decreased vision in the affected eye prior to the onset of hydrops.
In conclusion, PMD is a rare disorder, by definition bilateral and often asymmetric. Unilateral cases are atypical and rarely documented in the scientific literature. Corneal hydrops is a rare acute complication, usually self-limiting, that can appear in various, normally advanced, ectatic disorders, and it is rare for the underlying condition to present in the manner we describe here. A good differential diagnosis is of particular importance in keratectasia, for which biomicroscopy and topography are fundamental tools.
CASE OF CORNEAL HYDROPS IN UNILATERAL PMD