Embed Size (px)
Citation preview
American Journal of Medical Genetics 59:139-142 (1995)
Spondyloperipheral Dysplasia
G. Sorge, M. Ruggieri, and R.S. Lachman Clinica Pediatrica, Universita di Catania, Catania, Italy (G.S., M.R.); and International Skeletal Dysplasia Registry, Cedars Sinai Medical Center, UCLA School of Medicine, Los Angeles, California (R.S.L.)
We present a patient with spondyloperiph- eral dysplasia, a rare skeletal dysplasia which is characterized by vertebral body abnormalities (platyspondyly, end-plate in- dentations) and brachydactyly. Our patient also manifested a characteristic “pugilistic” face, sensorineural deafness and mental re- tardation. This chondroosseous dysplasia appears to be inherited as an autosomal dominant disorder. It appears that there is considerable clinical variability in spondy- loperipheral dysplasia. 0 1995 Wiley-Liss, Inc.
KEY WORDS: skeletal dysplasia, brachy- dactyly, fish mouth vertebrae, acromelia, acromesomelia
INTRODUCTION In 1977, Kelly et al. reported a new skeletal dysplasia
which they termed spondyloperipheral dysplasia. To their three cases in 1 family were added 2 large families by Sybert et al. [19791 and Vanek [19831, as well as one isolated case [Vanek, 19831. We are presenting the sev- enteenth case of this rare disorder in a family with 3 af- fected individuals.
CLINICAL REPORT Patient IV-9
P.B., a 20-year-old male, was the sixth child born to unrelated parents (Fig. 1, IV-9). The parents noted short stature and short hands at about age 2 years: this was considered insignificant because of short stature in several other family members. At about the same time, the mother noticed mild hearing loss and chronic nasal andlor airway obstruction without previous trauma.
The young man was the product of a full-term un- complicated pregnancy. There was no history of med- ication or drug use during the pregnancy. Newborn data regarding length and weight are not available; however, developmental milestones were delayed. He
Received for publication May 16, 1994; revision received March 27, 1995.
Address reprint requests to Ralph Lachman, M.D., Interna- tional Skeletal Dysplasia Registry, Suite 1001, 444 South San Vicente Blvd., Los Angeles, CA 90048.
0 1995 Wiley-Liss, Inc.
walked at 16 months and spoke at age 2 years. Poor school performance resulted in permanent interruption of studies after primary school education. During the teen years, medical examination disclosed bilateral sensorineural hearing loss and nasal septum deviation.
A detailed family history in 5 generations was ob- tained (see Fig. 1). A great-grandmother (1-1) was re- ported with short stature and a barrel-shaped chest. There were no other historically abnormal features as- certained in the rest of generations I or 11. In genera- tion 111, the proband’s father (111-3) is clinically normal with a very different facial appearance from the proband. The unaffected siblings (IV-2,4) have been personally examined and are also clinically normal. At the level of generation V, both children (V-1,2) have been personally examined and are normal. No family members, other than the proband, have mental retar- dation or hearing loss. The remainder of affected indi- viduals will be separately discussed.
Following an increase in nasallupper airway obstruc- tion, the young man was referred for diagnosis and ther- apy at age 20 years. On physical examination he was
I
Iy
Y 1 2 1 2
Fig. 1. Family pedigree. 1-1: Short stature and barrel shaped chest. 111-3: 160 cm. 111-4: 158 cm, midface hypoplasia, small flat nose, short distal phalanges. IV-2: 173 cm. IV-4: 174 cm. IV-6: 157 cm, small flat nose and bilateral short thumbs with bulbous tips. IV-7: 158 cm, unilateral short distal phalanx of thumb with bulbous tip. IV-8: 162 cm. IV-9: proband.
140 Sorge et al.
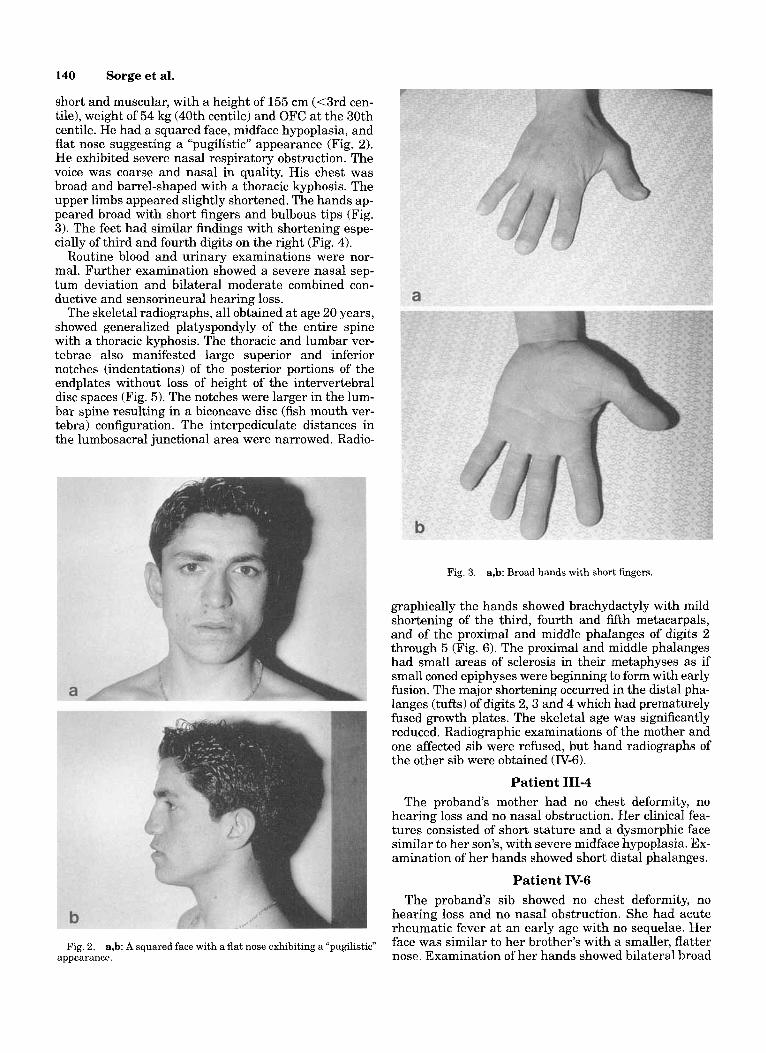
short and muscular, with a height of 155 cm (<3rd cen- tile), weight of 54 kg (40th centile) and OFC at the 30th centile. He had a squared face, midface hypoplasia, and flat nose suggesting a “pugilistic” appearance (Fig. 2). He exhibited severe nasal respiratory obstruction. The voice was coarse and nasal in quality. His chest was broad and barrel-shaped with a thoracic kyphosis. The upper limbs appeared slightly shortened. The hands ap- peared broad with short fingers and bulbous tips (Fig. 3). The feet had similar findings with shortening espe- cially of third and fourth digits on the right (Fig. 4).
Routine blood and urinary examinations were nor- mal. Further examination showed a severe nasal sep- tum deviation and bilateral moderate combined con- ductive and sensorineural hearing loss.
The skeletal radiographs, all obtained at age 20 years, showed generalized platyspondyly of the entire spine with a thoracic kyphosis. The thoracic and lumbar ver- tebrae also manifested large superior and inferior notches (indentations) of the posterior portions of the endplates without loss of height of the intervertebral disc spaces (Fig. 5). The notches were larger in the lum- bar spine resulting in a biconcave disc (fish mouth ver- tebra) configuration. The interpediculate distances in the lumbosacral junctional area were narrowed. Radio-
Fig. 3. a,b: Broad hands with short fingers
graphically the hands showed brachydactyly with mild shortening of the third, fourth and fifth metacarpals, and of the proximal and middle phalanges of digits 2 through 5 (Fig. 6). The proximal and middle phalanges had small areas of sclerosis in their metaphyses as if small coned epiphyses were beginning to form with early fusion. The major shortening occurred in the distal pha- langes (tufts) of digits 2 ,3 and 4 which had prematurely fused growth plates. The skeletal age was significantly reduced. Radiographic examinations of the mother and one affected sib were refused, but hand radiographs of the other sib were obtained (IV-6).
Patient 111-4 The proband‘s mother had no chest deformity, no
hearing loss and no nasal obstruction. Her clinical fea- tures consisted of short stature and a dysmorphic face similar to her son’s, with severe midface hypoplasia. Ex- amination of her hands showed short distal phalanges.
Patient IV-6 The proband’s sib showed no chest deformity, no
hearing loss and no nasal obstruction. She had acute rheumatic fever at an early age with no sequelae. Her face was similar to her brother’s with a smaller, flatter nose. Examination of her hands showed bilateral broad
Fig. 2, a,b: A squared face with a flat appearance.
exhibiting a ~~pugilistic~~
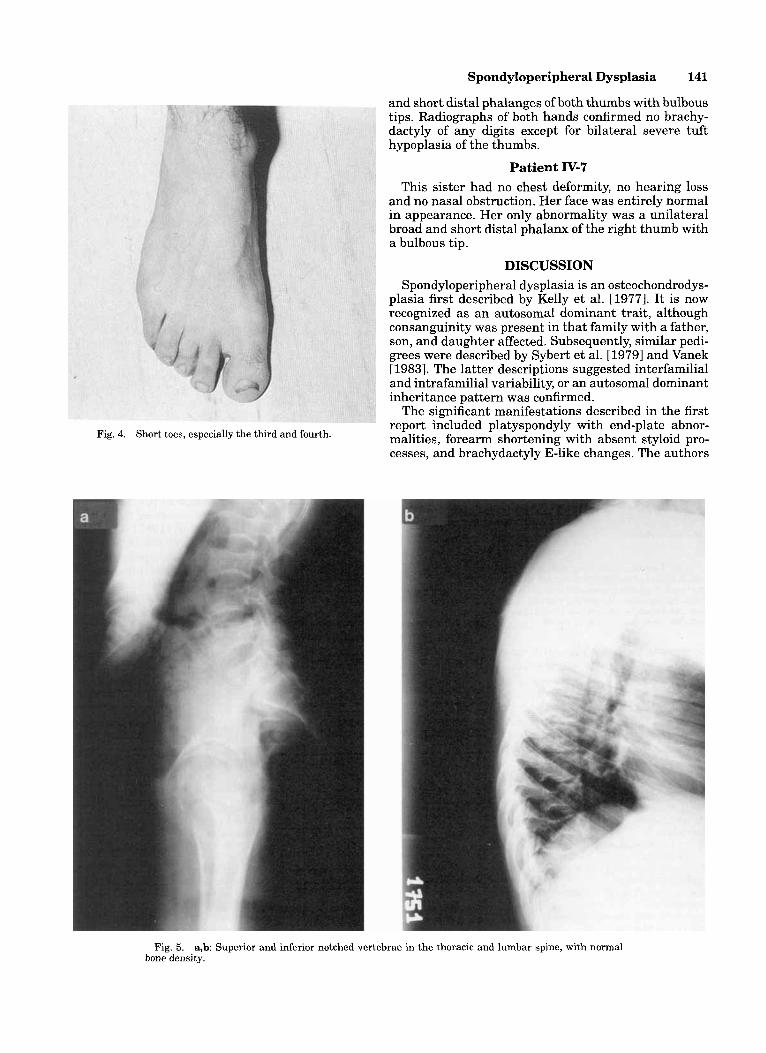
Fig. 4. Short toes, especially the third and fourth.
Spondyloperipheral Dysplasia 141
and short distal phalanges of both thumbs with bulbous tips. Radiographs of both hands confirmed no brachy- dactyly of any digits except for bilateral severe tuft hypoplasia of the thumbs.
Patient IV-7 This sister had no chest deformity, no hearing loss
and no nasal obstruction. Her face was entirely normal in appearance. Her only abnormality was a unilateral broad and short distal phalanx of the right thumb with a bulbous tip.
DISCUSSION Spondyloperipheral dysplasia is an osteochondrodys-
plasia first described by Kelly et al. [1977]. It is now recognized as an autosomal dominant trait, although consanguinity was present in that family with a father, son, and daughter affected, Subsequently, similar pedi- grees were described by Sybert et al. [1979] and Vanek [19831. The latter descriptions suggested interfamilial and intrafamilial variability, or an autosomal dominant inheritance pattern was confirmed.
The significant manifestations described in the first report included platyspondyly with end-plate abnor- malities, forearm shortening with absent styloid pro- cesses, and brachydactyly E-like changes. The authors
Fig. 5. a,b Superior and inferior notched vertebrae in the thoracic and lumbar spine, with normal bone density.

142 Sorge et al.
Fig. 6. Left hand and wrist radiograph at age 20 years revealing marked tuft shortening of the second, third and fourth digits which have fused (probably precociously) and sclerosis of many proximal and middle metaphyses, suggesting central fusing. The bone age is 14 years and 6 months, and greater than 4 standard deviations below the mean. No ulnar abnormality is noted.
preferred to delineate this entity as an unusual spondy- loepiphyseal dysplasia, although distinctive epiphyseal changes were not present except in the 60-year-old proband (degenerative arthrosis of the hips).
The condition described by Sybert et al. [1979] also ap- peared to have a spondyloperipheral dysplasia without platyspondyly but with (undescribed) vertebral notching and brachydactyly E-like changes. Some ulnar shorten-
TABLE I. Minimal Diagnostic Criteria: Spondyloperipheral Dysplasia
*Short stature *Platyspondyly, inferior-superior notching (“fish mouth
vertebrae”) *Broad hands with short fingers; short, broad thumbs with
bulbous tips *Markedly shortened distal phalanges, short proximal and
middle phalanges Face: normal, “round,” or flattened profile with “pugilistic”
appearance Chest deformity (barrel-shaped) Mental retardation Sensorineural deafness
*Major features
ing was also described in several patients, some of whom also exhibited lack of ulnar styloid development. Their cases showed significant interfamilial variability.
The family and sporadic case described by Vanek [1983] showed similar manifestations. The spinal changes were those of normal height with mild platyspondyly and biconcave end-plate abnormalities in most affected members, and brachydactyly E-like digital changes. Significant ulnar abnormalities were not noted. Marked interfamilial variability was noted.
The “epiphyseal abnormalities” in all reports are lim- ited to the capital femoral epiphyseal region and seem to represent degenerative arthrosis without significant epiphyseal abnormalities.
Our patient exhibits clinical and radiographic changes similar to the previous reports of spondyloperipheral dysplasia, especially to those described by Sybert et al. [ 19791 and Vanek [ 19831. No ulnar shortening or styloid hypoplasia were present in this patient, although his upper limbs appeared to be slightly short. Clinically, this patient had a characteristic face which is best charac- terized as “pugilistic” in appearance (square, severe mid- face hypoplasia and flattened non-enlarged nose). The nose is not the large, broad and flat ethnic North African nose seen typically in many Sicilian families. The face in the other reports is said to be normal or “round.” The il- lustrations in Kelly et al. [1977] have some similarity to our patient’s face. The sensorineural deafness found in our patient is also not mentioned in previous reports. Mental retardation was also not described by others.
A report by Goldblatt and Behari [19871 of a “Unique Skeletal Dysplasia with Absence of the Distal Ulnae” could represent variability in spondyloperipheral dys- plasia as their patient did not manifest brachydactyly, although similar spine and forearm changes were pre- sent. A recent report of “An Unclassifiable Type of Spondyloperipheral Epiphyseal Dysplasia Associated With 21 Trisomy” [Ioan, 19931 represents an entirely different disorder.
Table I describes what we conceive as the minimal diagnostic criteria for the diagnosis of spondylope- ripheral dysplasia. The family described here with at least 4 affected members exhibited marked interfamil- ial variability.
ACKNOWLEDGMENT This work was supported in part by NIH Program
Project Grant No. POI-HD 22657-08.
REFERENCES Goldblatt J , Behari D (1987): Unique skeletal dysplasia with absence
of the distal ulnae. Am J Med Genet 28:625-630. Ioan DM (1993): An unclassifiable type of spondyloperipheral epiphy-
seal dysplasia associated with 21 trisomy . Genetic Counseling 4: 59-62.
Kelly TE, Lichtenstein JR, Dorst JP (1977): An unusual familial spondyloepiphyseal dysplasia: Spondyloperipheral dysplasia. Birth Defects OAS 13 (3B):149-165.
Sybert VP, Byers PH, Hall JC (1979): Variable expression in a domi- nantly inherited skeletal dysplasia with similarities to Brachy- dactlyly E and Spondyloepiphyseal-spondyloperipheral Dysplasia. Clin Genet 15:160-166.
Vanek J (1983): Spondyloperipheral Dysplasia. J Med Genet 20: 117-12 1.