Embed Size (px)
Citation preview

1 !
Spine Symposium ACDF with plating in multilevels CSM Cervical Spondylotic Myelopathy (CSM) Clinical Evaluation and Management Korku Chiengthong M.D. Chiang Mai Thailand 7th C.M.U. Neurosurgery Forum 2015 !
CSM CSM is define as spinal cord dysfunction secondary to extrinsic compression of the cord or its vascular supply or both that is caused by degenerative disease of cervical spine. !
Pathophysiology CSM may be associated with congenital or developmental stenosis of cervical canal. The problem begins with degenerative change in the disk and secondary changes in the adjacent osseous and soft tissue structures .caused - Direct cord compression - Impair blood supply !
Natural History =Nuric 1970s Benign disorder in old age was the risk factor operative or non-operative = no difference =Symon – Lavendar and Sadacivian 1993. CSM –Progressive deterioration with no stabilization of symptoms - Early operation even mildly symptomatic patients =Sampath 2002 =Multicenter prospective trial 503 nonrandomized -Significant improvements in functional status of patients undergoing surgical treatment - Comparison with patients who were conservative treated !
Mechanism of ischemia 1. Canal narrowing and chondro-osseous spur or mass 2. Compression of foraminal or radicular feeder artery of cord by osteophyte or ligametum flavum 3. Morphologic change can produce pincer mechanism in normal motion !
LIG,FLAVUM!
FACET!
OSTEOPHYTE!
FACET !
LUSHKA !UNCOVERTEBRAL!
Encroachment on the available space !

2 !
Diameter of cervical spinal canal Sagittal diameter of C-spinal canal =17-18 mm Diameter less than 12 mm =myelopathy 1972 Nurick =11.3 in male . = 9.9 in female 2000 Korku and Pomsil measure the sagittal
diameter of cervical spinal canal=10.80+-1.27 and spinal cord =7.60+-0.56 mm
The Thai journal of orthopaedic surgery 2006 !
Level of C-spine Sagittal diameter
of cervical vertebra (mm)
Sagittal diameter of cervical spinal canal
(mm) Sagittal diameter
of cervical spinal cord (mm)
C3 15.00±2.00 11.20±1.20 7.86±0.62
C4 15.00±1.80 10.70±1.38 7.80±0.60
C5 16.00±2.00 11.00±1.40 7.70±0.60
C6 16.00±1.80 11.00±1.40 7.70±0.60
C7 16.00±2.00 11.00±1.30 7.70±0.60
Mean 15.50±1.73 10.80±1.27 7.60±0.56
Table 2. Sagittal diameters (mean ±SE) of the vertebral body, spinal canal, and the spinal cord at different cervical spine.
Compensatory zone 4 mm !
Clinical evaluation History Neck pain, difficulty in walking, pain numbness, paresthesia motor weakness radicular symptom and cord signs Natural history 1.No pathognomonic clues to permit the disease progression Almost all pt worsen clinically 2. 50% progress to severe disability !
Clinical evaluation Physical examination 1. Uppers in the lowers and lowers in the uppers 2. Upper in the upper extremity caudad to the lesion !
Clinical evaluation Physical examination Upper motor neuron dysfunction 1. DTR hyperactive 2. Hoffman sign positive ,IVR positive 3. Lhermitte sing positive 4. Babinski test Dosiflexion (severe myelopathy) 5. Gait disturbance and incoordination during turns !
Clinical evaluation Motor finding 1. Corticospinal tract dysfunction Lower extremity weakness and spastic gait Upper ext clumsiness 2. Anterior horn cells pathology Lower motor neuron finding Intrinsic atrophy !
3 !
Clinical evaluation Sensory finding Nerve root involvement Pain, paresthesia Loss of vibration sense and proprioception !
Clinical evaluation Reflex finding 1. Long tract sing positive 2. Hypo tone = nerve root compression 3. Jaw jerk to R/O pathology above foramen magnum !
Clinical Classifications Numerous scales for grading the severity of CSM 1. Nurick Disability Score 2. JOA score and Modified JOA score 3. Cooper Scale, Harsh scale, Prolo scale ++++ Visual analog scale All scales and scores are used in research Not in every day clinical practice !
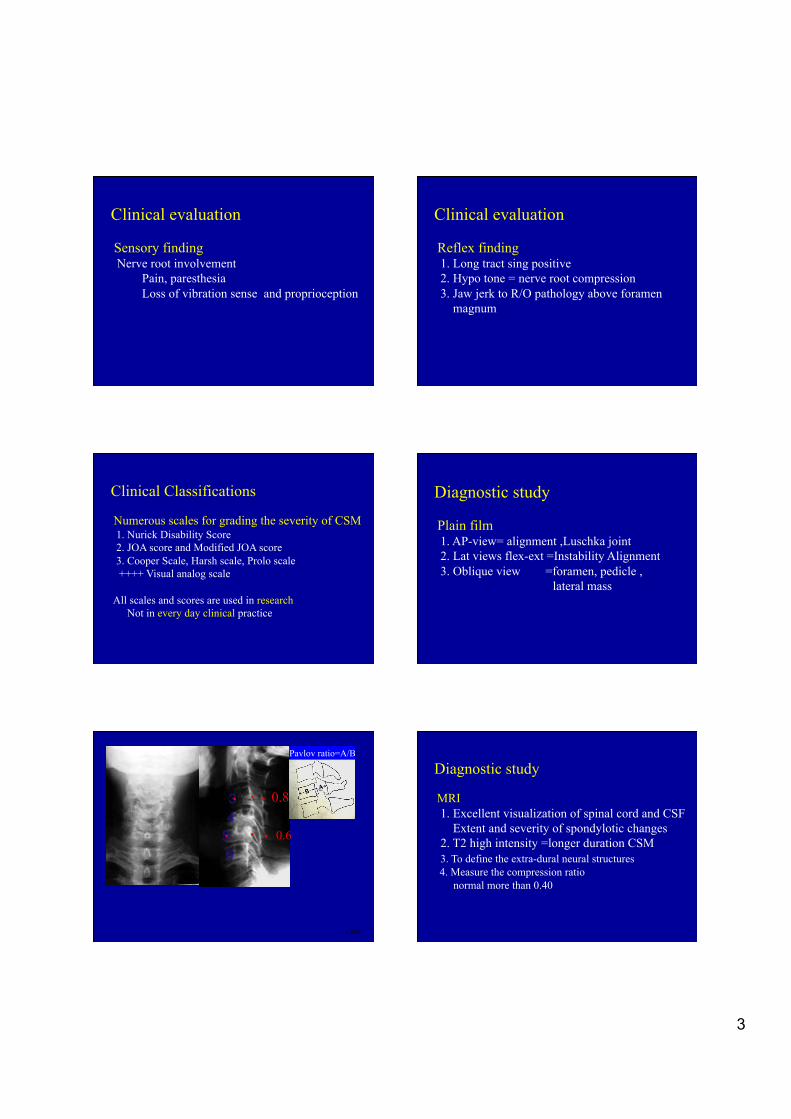
Diagnostic study Plain film 1. AP-view= alignment ,Luschka joint 2. Lat views flex-ext =Instability Alignment 3. Oblique view =foramen, pedicle , lateral mass !
CSM !
Pavlov ratio=A/B !
.! .! .! 0.8!
.! .! .! 0.6!
Diagnostic study MRI 1. Excellent visualization of spinal cord and CSF Extent and severity of spondylotic changes 2. T2 high intensity =longer duration CSM 3. To define the extra-dural neural structures 4. Measure the compression ratio normal more than 0.40 !

4 !
CSM ! CSM !
CT! CT!
CSM !
CT!
Differential diagnosis 1. MS 2. Spinal cord tumor 3. Syringomyelia 4. C-disc with myelopathy 5. Medical myelopathy !
CSM !
!1. Immobilization (collar) !2. Analgesic NSAIDs (Some benefit) !3. Physical therapy (No traction ) !4. F.U.every 6 mo for check up ( Useless) !!
Nonoperative treatment Mild myelopathy and high risk !
CSM !
- Progression of neurological deficit !- Failure of neurological improvement !- Compression ratio less than 0.4 !- Transverse area less than 40 mm2 !- Increase signal intensity TW2
- The goal of surgery is to prevent deterioration - Stabilization of motion segments - not complete resolution of symptoms !
Surgical Indication !
5 !
CSM !
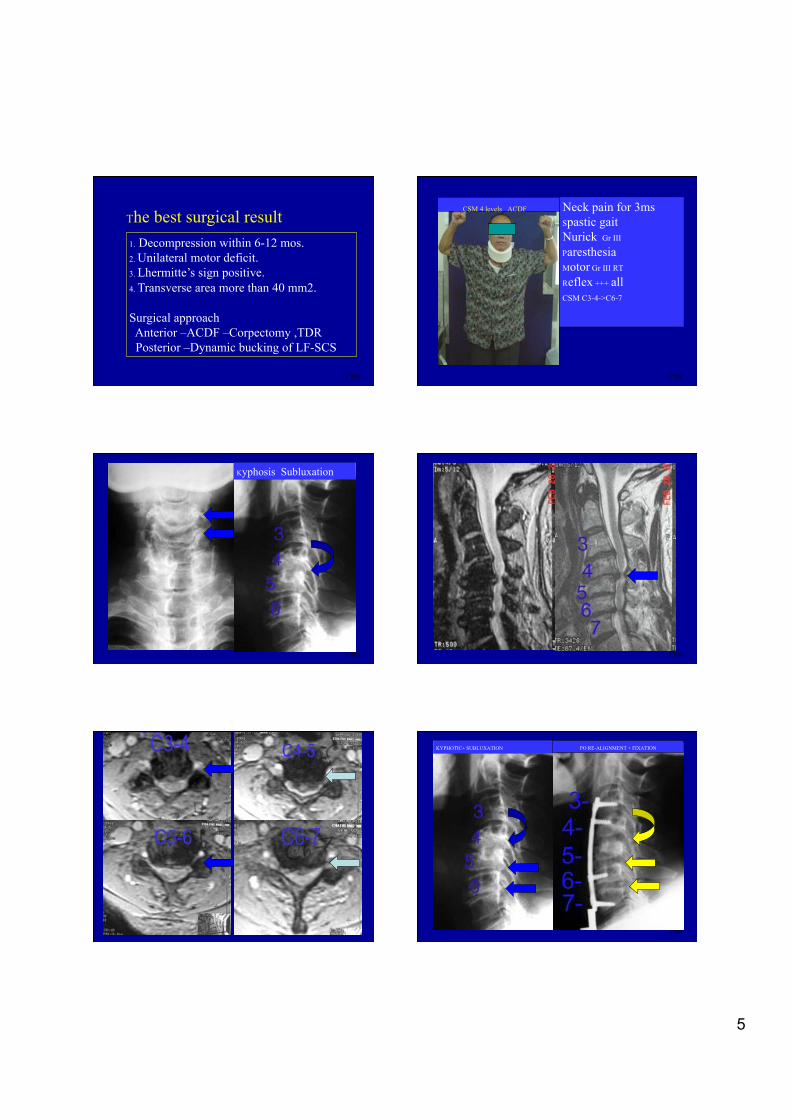
1. Decompression within 6-12 mos. !2. Unilateral motor deficit. !3. Lhermitte’s sign positive. !4. Transverse area more than 40 mm2. Surgical approach Anterior –ACDF –Corpectomy ,TDR Posterior –Dynamic bucking of LF-SCS !
The best surgical result !
CSM !
Neck pain for 3ms !Spastic gait !Nurick Gr III!Paresthesia!Motor Gr III RT !Reflex +++ all!CSM C3-4->C6-7 !!
CSM 4 levels ACDF !
CSM !
Kyphosis Subluxation !
CSM !
CSM ! CSM !
KYPHOTIC+ SUBLUXATION! PO RE-ALIGNMENT + FIXATION!

6 !
Outcomes of ACDF with Plating in multi levels CSM
Torphong Bunmaprasert, MD. Korku Chiengthong, MD. *
Aurmporn Oberdorfer, MD. ** *Department of Orthopaedic Surgery,
**Department of Pediatrics Faculty of Medicine, CMU.
Methodology • January 2001 – August 2002 • Number of patients = 40 • Age 40-80 yrs, M=27 / F=13 • Hx, PE, Plain X-rays, MRI, Nurick’s score • Operation: ACDF (Smith-Robinson technique), anterior plating , 3 or more levels • Follow-up: Nurick’s score, Plain X-rays at the 1st , 3rd,
6th , 12th month.
Comparative study between the preoperative & postoperative Nurick’s score at the final follow-up
(12th month) ! Improve 24 (=60% ) No change 12 (=30%) Worsening 4 (=10%)
Statistically-significance improvement at the 6th month
(P=0.033)* and 12th month (P<0.01) * * Wilcoxon-Signed Rank test
Results Results (Cont.)
0
10
20
30
40
Number
of Patients
1st
month
3rd
month
6th
month
12th
month
Time
Improve
No change&Worsening
Graph : Outcomes of the operation Improve =24. No change&worsening= 16
CSM !
Complication !
CSM !
!!
Complication !Post-op!
Quadri paresis !Causes Cord injury
Ant spinal artery stretching !Methyl prednisolone
! 4 wks post-op
Motor ,sensory recovery !12 wks hospital stay !
Pt can walk with support!!!!!

7 !
.!
Complications Spinal cord injury 1 out of 40 patients (=2.5%) Implant loosening 1 out of 40 patients (=2.5%) Pseudarthrosis 1 out of 40 patients(=2.5%) !Recommendation. Adequate decompression ,Proper grafting & Anterior plating technique ACDF could be the alternative treatment for patients with multi- levels CSM Simple, stable, easy to correct deformity !!
Conclusions Pathology of CSM is anterior Surgical treatment for CSM should be -Adequate anterior decompression ,Proper auto graft & anterior plating technique -ACDF is one of the best treatment for patients with multi- levels CSM - Simple, stable, easy to correct deformity -PO neck motion adequate for normal daily activity - Corpectomy more difficult technique & longer time - Laminoplasty - need more time, P.O. neck pain, instability and also need posterior fixation ( more difficult ) !!
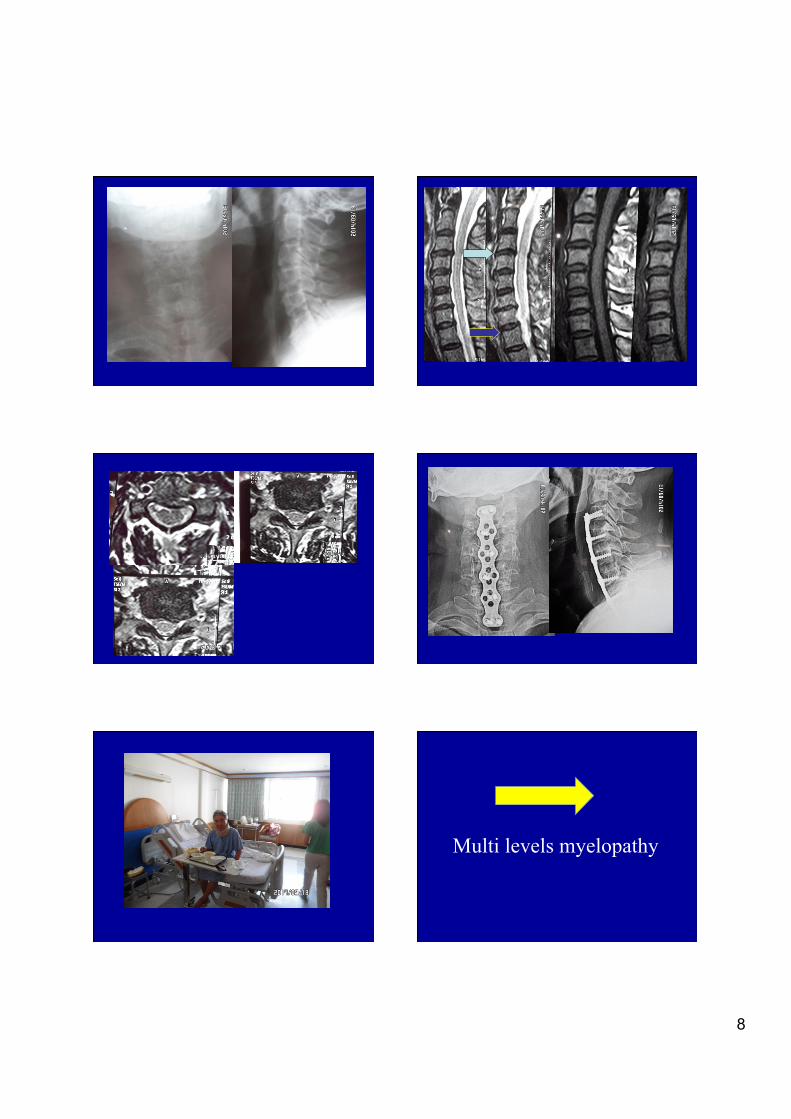
Multi levels myelopathy !
Multi – Levels Myelopathy !
8 !
Multi levels myelopathy !

9 !
C-Myelopathy PO ACDF 5 Levels!C2-3 ----C6-7 ! Post-op order
First and
Second day PO
Swallowing Problems!
Multi levels myelopathy !
C-Myelo-Radiculopathy!

10 !
PO ? =CORPECTOMY! 2 wks PO Fever severe neck pain quadriparesis !
8 Months post revision ! Basic surgical procedures are !
1.ACDF ( autograft ) +fixation 2. ACF remove uncus, restore foramen volume (not all) Facet osteophytes cannot 3.Laminectomy /foraminotomy (uncus, facets ) direct nerve root decompression 4.Laminoplasty ( no direct nerve root decompression) 5.TDR- Expensive, Final result = same as ACDF
Adequate neural decompression is the most important !
VDO =ACDF AUTOGRAFT PLATE FIXATION !
VDO !

11 !
Finally for spine surgeon 1.Symptoms and sign =Diagnosis ( PE )
2.X-rays MRI and other investigation + conferm 3.Diagnosis +Indication = Brain cells 4.Surgical technique need learning curve Routine work = SPINAL CORD function Spine surgeon MUST have a very good SPINAL CORD FUNCTION !
Cervical Myelopathy Cervical Radiculo-Myelopathy Anterior Pathology I prefer Anterior Surgery !
Thank you For your attention !
Case Discussion !
KORKU!

12 !
2 !4 !5 !6 !7 !
13 !
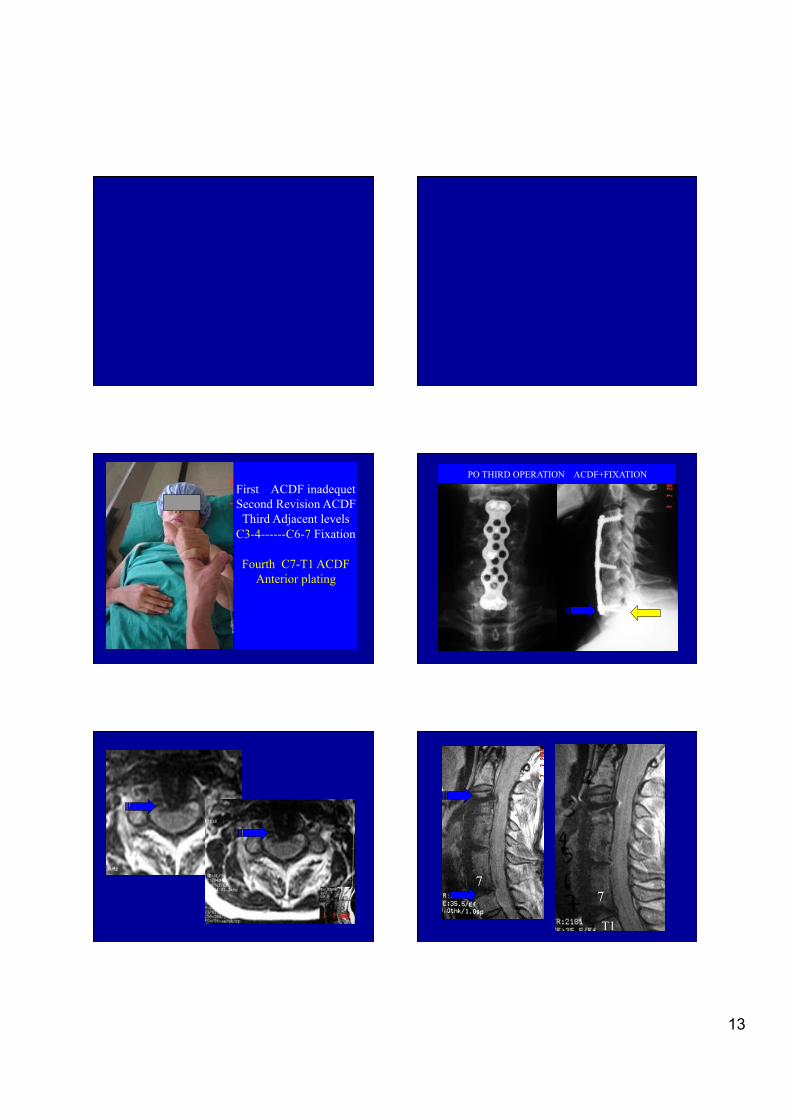
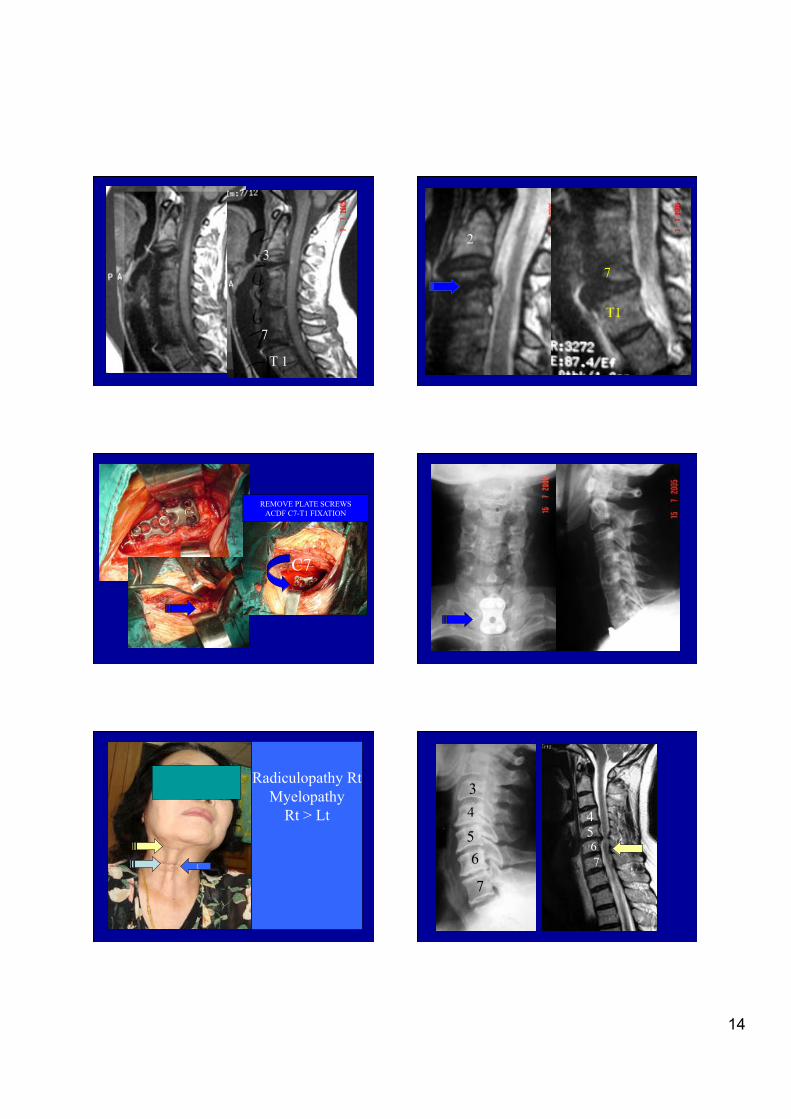
First ACDF inadequet Second Revision ACDF Third Adjacent levels
C3-4------C6-7 Fixation
Fourth C7-T1 ACDF Anterior plating
!
PO THIRD OPERATION ACDF+FIXATION!
7!7!
T1 !
14 !
7!
T 1!
3!2!
T1 !
7!
REMOVE PLATE SCREWS ACDF C7-T1 FIXATION !
C7!
Radiculopathy Rt Myelopathy
Rt > Lt !
1!
34
5!6!
7
45!67!

15 !
PO – ACDF First op!
3!
7!
4!
6 ms post-op Axial pain +Myelopathy !
3! 3!
3!
2!Ant revision !









![Original Article Impact of over distraction on occurrence ...Anterior cervical discectomy and fusion (ACDF) was first proposed for cervical spondylosis in 1958 [7]. Since then, ACDF](https://img.dokumen.tips/doc/110x75/601b12821ec12c5b586f0605/original-article-impact-of-over-distraction-on-occurrence-anterior-cervical.jpg)



















