Embed Size (px)
Citation preview

Journal of The Association of Physicians of India ■ Vol. 69 ■ September 2021104
the IgM antibody by ELISA method. Out of 1911 samples, 562 samples were screened for NS1 ELISA. The overall positivity rate for dengue infection was 22% (419/1911). IgM seropositivity was 28% (390/1349) and NS1 positivity was 5.1% (29/562). These results have shown similarit ies with previous studies conducted in other areas.2,5
The most common symptoms among dengue posi t ive cases were fever (85.3%), followed by headache (62.3%), body pain (55.6%), joint pain (45.3%), vomiting (34.3%), retro-orbital pain (27.4%). The percentage positivity rate for dengue infection was 40.6% (48/118) in 2017 (October to December), 27.26% (232/851) in 2018, and 27.8% (111/398) in 2019 (until September ). Amongst dengue positive cases, 52.5% (205/390) were males and 47.5 % (185/390) were females. The mean age group was 28.7 years.
It was observed that about 51.6% (31 /60) o f dengue pos i t ive cases belonged to Wada block (04 PHCs), 49% (46/94) from Vasai (8 PHCs), 35% (7/20) from Talasari, 33% (6/18) from Mokhada of Palghar district. Thirty-eight percent (5/13) of NS1 positivity was observed in Wada block (January to September 2019). The seropositivity for dengue infection was observed in all the age groups, with the highest (40.3%) in age group of 6-10 years. The age and month-wise distribution of the seropositive cases are illustrated in Figure 1. Out of 390 cases who were positive for dengue, 79.4% (310/390) had a recorded travel history. Of 310, 26.1% (81/310) had shown travel history to places outside of Palghar district. However, 73.8% (229/310) cases had no travel history, and it indicates that the dengue virus is circulating in the Aedes vectors prevalent in Palghar district.
Among the 240 case records, 90.8% ( 2 1 8 / 2 4 0 ) o f t h e m h a d m o s q u i t o infestation in their area. Two hundred and twenty case records mentioned that 74% of (163/220) people were using plastic drums with a lid for the storage of water which is the most preferred site for the Aedes vector observed in Maharashtra.6 Eight (16.3%) of the 49 samples tested by RT-PCR analysis for dengue virus were positive. DENV- 3 (87.5%) (7/8) was the predominant sero type in Pa lghar fo l lowed by DENV-2 (12.5%) (1/8). The majority of the DENV-3 positive cases were less than 25 years of age. Circulation
of these serotypes was also identified in the Pune and Nashik regions of Maharashtra.7
To the best of our knowledge, this is the first study that has revealed 28% of prevalence and circulation of multiple dengue serotypes (DENV 3 & 2) in Palghar district. Therefore, the existence of multiple serotypes of the virus in the rural area of Palghar district increases the risk of Dengue Haemorrhagic fever/Dengue shock s y n d r o m e a n d f u t u r e o u t b r e a k s could lead to increased morbidity and mortality. The current situation warrants a robust surveillance system and control of Aedes spp breeding could prevent outbreak in the future.Acknowledgments
The authors are sincerely thankful to NVBDCP, New Delhi , and the National Institute of Virology, Pune for providing NS1 and IgM Dengue ELISA kits. The authors are thankful to the ICMR - Department of Health Research. Dr. Arun Yadav, Dr. Prabhkar Bhoye, Dr. Balaji Hengne, Dr. Abhijit Chavan from Sub District Hospital, Dahanu, Public Health Department, G o ve r n m e n t o f M a h a r a s h t r a a r e s i n c e r e l y a c k n o wl e d g e d f o r t h e help in obtaining samples. We also acknowledge Miss Ruchita Surve, Mrs. Pranali Kadu, and Mrs. Roshni Kadu for their help in data entry and sample collection during the study period. Mrs. Swati is also acknowledged for assistance in statistical analysis. Contributions
IKC, RK NS & SC : Conceptualization, design, planning and implementation of the study and manuscript preparation. IKC, KAN,NNK: Data co l lec t ion , interpretation of data, data analysis. SP facilitated sample collection from Palghar district. NS: contributed to c l inical inputs and review of the manuscript. All authors reviewed the manuscript.Funding
This study was financially supported by Intramural funds of the Model Rural Health Research Unit, Dahanu.
References1. Brady OJ, Gething PW, Bhatt S, Messina JP, Brownstein JS,
Hoen AG, Moyes CL, Farlow AW, Scott TW, Hay SI. Refining the global spatial limits of dengue virus transmission by evidence-based consensus. PLoS Negl Trop Dis 2012; 6:e1760.
2. Chakravarti A, Arora R, Luxemburger C. Fifty years of dengue in India. Trans R Soc Trop Med Hyg 2012; 106:273-82.
3. The National Vector Borne Disease Control Programme. Dengue cases and deaths in the country since 2015. https://nvbdcp.gov.in/index4.php?lang=1&level=0&linkid=431&lid=3715.
4. Lanciotti RS, Calisher CH, Gubler DJ, Chang GJ, Vorndam AV. Rapid detection and typing of dengue viruses from clinical samples by using reverse transcriptase-polymerase chain reaction. J Clin Microbiol 1992; 30:545-51.
5. Rahman M, Sharma A, Patgiri S, Hussain E, Borah AK, Saikia L. Serotyping of dengue viruses circulating during 2014-2015 in Assam, India. Indian J Med Microbiol 2018; 36:429-431.
6. Fulmali PV, Walimbe A, Mahadev PV. Spread, establishment & prevalence of dengue vector Aedes aegypti (L.) in Konkan region, Maharashtra, India. Indian J Med Res 2008; 127:589-601.
7. Patil JA, Alagarasu K, Kakade MB, More AM, Gadekar KA, Jadhav SM, Parashar D, Shah PS. Emergence of dengue virus type 1 and type 3 as dominant serotypes during 2017 in Pune and Nashik regions of Maharashtra, Western India. Infect Genet Evol 2018; 66:272-283.
Spinal Intramedullary Neurocysticercosis- An Unusual Cause of ParaparesisDivya M Radhakrishnan1, Ankith Bhasi2, Saurya Saurya3, Ritu Shree4, Niraj Kumar5
1Assistant Professor, Department of Neurology, 2Junior Resident, Department of Medicine, 3Junior Resident, Department of Radiology, All India Institute of Medical Sciences, Rishikesh, Uttarakhand; 4Assistant Professor, Department of Neurology, Post Graduate Institute of Medical Education & Research, Chandigarh; 5Additional Professor, Department of Neurology, All India Institute of Medical Sciences, Rishikesh, Uttarakhand
Sir,
Sp i n a l c y s t i c e r c o s i s i s a r a r e manifestation of neurocysticercosis
(NCC) accounting for 0.7 to 5.85% of all cases.1,2 Spinal intramedullary cyst icercos is ( IMC) i s infrequent when compared to extra-medullary ( intradural or extradural ) forms; constituting only 20% of spinal cases.2
A 40 -year-old male presented with one-month history of low back pain, which was fol lowed by weakness of lower limbs. The weakness was asymmetrical (right > left), associated with reduced sensations in both the lower limbs and urinary retention. Neurological examination revealed power of MRC grade 3/5 (right) and 4-/5 (left) in lower limbs (LL) with brisk deep tendon jerks and bilateral extensor plantar response. He had 50% reduced pan sensory loss below L1.
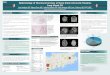
C o n t r a s t - e n h a n c e d m a g n e t i c resonance imaging (CEMRI) of the s p i n e r e ve a l e d a f o c a l e c c e n t r i c lesion (8x 5mm) with peripheral rim enhancement in conus medullaris at D11 vertebral body level suggestive of NCC in granular nodular stage (Figure 1). CEMRI of brain and cerebrospinal fluid analysis (CSF) were essentially

Journal of The Association of Physicians of India ■ Vol. 69 ■ September 2021 105
normal. ELISA for anti–T solium Ig G immunoglobulin was positive in serum.
The patient was started on oral dexamethasone in a dose of 0.1 mg/kg/day followed by a 2-week course of oral albendazole (15 mg/kg/day) 12th hourly. At the time of discharge, he showed significant improvement in power to 4/5 in both lower limbs along with improved sensations. At two months follow up; he had complete resolution of neurological features.
Hematogenous spread and CSF d i s s e m i n a t i o n v i a v e n t r i c u l a r - s u b a r a c h n o i d p a t h wa y s a r e t h e speculated mechanisms of spinal involvement1.The common clinical presentations include pain, paraparesis, s p a s t i c i t y , b o w e l a n d b l a d d e r incontinence and sexual dysfunction.2
Contrast enhanced MRI shows a cystic lesion with signal intensities similar to CSF on both T1-weighted and T2-weighted images.1,3 The scolex, when present, can be identified on T1- weighted images, as mural nodule isointense to cord parenchyma.1,3 A positive serology, preferably antibody
by ELISA, either in cerebrospinal fluid or in serum further strengthens the suspicion.1,3
T r e a t m e n t o f s p i n a l N C C includes both medical (Albendazole/ P r a z i q u a n t e l ) a n d / o r s u r g i c a l m a n a g e m e n t . A l b e n d a z o l e monotherapy is preferred in selected patients with IMC with stable clinical course.3 Dexamethasone should be given along with medical therapy as it increases the drug levels in blood and reduces the therapy associated inf lammatory react ions. 1 Surgical intervention is required when patients present with severe and progressive neurological deficits regardless of medical therapy.3
Acknowledgment
Authors acknowledge their patient and Department of Radiology at AIIMS Rishikesh
References1. Ahmad FU, Sharma BS. Treatment of intramedullary spinal
cysticercosis: report of 2 cases and review of literature. Surgical Neurology 2007; 67:74-7.
2. Agale SV, Bhavsar S, Barnik Choudhury VM. Isolated intramedullary spinal cord cysticercosis. Asian Journal of
Neurosurgery 2012; 7:90.
3. Maste PS, Lokanath YK, Mahantshetti SS, Soumya S. Isolated intramedullary spinal cysticercosis: A case report with review of literature of a rare presentation. Asian Journal of Neurosurgery 2018; 13:154.
Upper Gastrointestinal Bleed in Acute Mercury Chloride PoisoningPazhanivel MohanDepartment of Gastroenterology, Jawaharlal Institute of Postgraduate Medical Education and Research, Puducherry
Sir,
I read with interest the pictorial CME on Imaging Appearances following
Oral and Parenteral Mercury Poisoning by Deepashree T et al.1
I would like to discuss a case of a 27-year old lady with acute mercury chloride poisoning who had an upper gastrointestinal bleed.
A 27-year old woman was admitted following consumption of mercuric chloride swallowed in a capsule. She developed acute kidney injury and
Fig. 1: MRI dorso lumbar spine- Sagittal T1 W (A); Sagittal T2 W (B); STIR (C); Axial T2W (D)- images showing a focal tiny eccentric lesion in conus medullaris at D11 vertebral body level appearing hypointense on T1 and T2 W AND STIR images. On post contrast T1W Image (E) the lesion shows peripheral rim enhancement. No perilesional edema is seen. Findings are suggestive of partly calcified peripherally enhancing lesion in conus medularis –consistent with NCC in granular nodular stage
Fig. 1: Upper gastrointestinal endoscopy in a woman with acute mercury chloride poisoning showing (A) large areas of necrotic mucosa in the distal body of the stomach; (B) ulceration in the antrum extending to the pylorus and focal areas of hemorrhagic gastric mucosa

![Meta-analysis of plate fixation versus intramedullary fixation ......intramedullary fixation (IF), the common devices in clinics are Knowles pinning [14,15], elastic stable intramedullary](https://img.dokumen.tips/doc/110x75/60ec8dbb516bc21c1e0f6489/meta-analysis-of-plate-fixation-versus-intramedullary-fixation-intramedullary.jpg)









![Clinical Diagnoses of Neurocysticercosis · Clinical Diagnoses of Neurocysticercosis 281 extraparenchymal location [88%), in comparison with the parenchymal location (10%). [12] When](https://img.dokumen.tips/doc/110x75/5e76ff60412a36576f46bf82/clinical-diagnoses-of-neurocysticercosis-clinical-diagnoses-of-neurocysticercosis.jpg)