Embed Size (px)
Citation preview

J Neurosurg 121:1380–1387, 2014
1380 J Neurosurg / Volume 121 / December 2014
©AANS, 2014
ChroniC subdural hematomas (CSDHs) are gener-ally regarded to be consequences of head trauma. The most commonly accepted pathophysiological
explanation of CSDH is that mild head trauma leads to tearing of bridging veins with subsequent bleeding be-tween the inner layer of the dura mater and the arachnoid, or between the outer and inner layers of the dura, thus creating the hematoma.5,14,28,29 Further and chronic en-
largement of the subdural hematoma is believed to be due to microbleedings from fragile walls of sprouting vessels, accumulation of fluid in this newly created space follow-ing an osmotic gradient created by blood degradation products, or a combination of these events.5,10 In older pa-tients, mechanical forces related to brain atrophy enable formation and growth of CSDH. A history of mild head trauma in many older patients is suggestive of trauma as a causative agent. In younger patients, brain atrophy is generally not so prominent and a history of head trauma is often not present.
Triggered by our experience with a young man with recurrent CSDH whose recurrence only stopped after
Spinal cerebrospinal fluid leak as the cause of chronic subdural hematomas in nongeriatric patients
Clinical articleJürgen Beck, M.D.,1 Jan gralla, M.D., M.Sc.,2 chriStian Fung, M.D.,1 chriStian t. ulrich, M.D.,1 PhiliPPe Schucht, M.D.,1 JenS Fichtner, M.D.,1 lukaS anDereggen, M.D.,1 Martin goSau, M.D.,4 elke hattingen, M.D.,5 kleMenS gutBroD, M.D.,3 Werner J. Z’graggen, M.D.,1,3 Michael reinert, M.D.,1,6 Jürg hüSler, Ph.D.,7 chriStoPh oZDoBa, M.D.,2 anD anDreaS raaBe, M.D.1
Departments of 1Neurosurgery, 2Neuroradiology, and 3Neurology, Bern University Hospital, Bern, Switzerland; 4Department of Cranio-Maxillo-Facial Surgery, University Medical Center, Regensburg, Germany; 5Institute of Neuroradiology, University of Frankfurt, Frankfurt/Main, Germany; 6Department of Neurosurgery, Ospedale Cantonale di Lugano, Switzerland; and 7Institute of Mathematical Statistics and Actuarial Science, University of Bern, Switzerland
Object. The etiology of chronic subdural hematoma (CSDH) in nongeriatric patients (≤ 60 years old) often re-mains unclear. The primary objective of this study was to identify spinal CSF leaks in young patients, after formulat-ing the hypothesis that spinal CSF leaks are causally related to CSDH.
Methods. All consecutive patients 60 years of age or younger who underwent operations for CSDH between September 2009 and April 2011 at Bern University Hospital were included in this prospective cohort study. The pa-tient workup included an extended search for a spinal CSF leak using a systematic algorithm: MRI of the spinal axis with or without intrathecal contrast application, myelography/fluoroscopy, and postmyelography CT. Spinal patholo-gies were classified according to direct proof of CSF outflow from the intrathecal to the extrathecal space, presence of extrathecal fluid accumulation, presence of spinal meningeal cysts, or no pathological findings. The primary outcome was proof of a CSF leak.
Results. Twenty-seven patients, with a mean age of 49.6 ± 9.2 years, underwent operations for CSDH. Hema-tomas were unilateral in 20 patients and bilateral in 7 patients. In 7 (25.9%) of 27 patients, spinal CSF leakage was proven, in 9 patients (33.3%) spinal meningeal cysts in the cervicothoracic region were found, and 3 patients (11.1%) had spinal cysts in the sacral region. The remaining 8 patients (29.6%) showed no pathological findings.
Conclusions. The direct proof of spinal CSF leakage in 25.9% of patients suggests that spinal CSF leaks may be a frequent cause of nongeriatric CSDH.(http://thejns.org/doi/abs/10.3171/2014.6.JNS14550)
key WorDS • chronic subdural hematoma • spinal CSF leak • geriatric • vascular disorders • meningeal cyst
Abbreviations used in this paper: CSDH = chronic subdural hematoma; mRS = modified Rankin Scale; SIH = spontaneous intra-cranial hypotension; SPACE = sampling perfection with application of optimized contrasts using different flip angle evolutions.
Unauthenticated | Downloaded 02/20/22 12:10 AM UTC

J Neurosurg / Volume 121 / December 2014
Spinal CSF leakage and chronic subdural hematoma
1381
a spinal CSF leak was sealed, we started to include the search for spinal CSF leakage into a prospective proto-col for all consecutive nongeriatric CSDH patients. Our primary objectives were to identify spinal CSF leaks and spinal meningeal cysts in our cohort with the hypothesis that spinal CSF leaks are causally related to CSDH. In this paper we report our findings on the frequency of this condition.
MethodsStudy Design
This prospective cohort study was approved by the local ethics committee of Bern University Hospital. All consecutive patients ≤ 60 years old with CSDH verified by CT or MRI who underwent operations between Sep-tember 1, 2009, and April 12, 2011, were eligible for the study. After formulation of our hypothesis that spinal CSF egress may be a cause of CSDH in younger patients, we distributed the study protocol among all staff of the Departments of Neurosurgery and Neuroradiology at sev-eral meetings and conferences that took place beginning 4 months prior to study initiation. Beginning September 1, 2009, all staff from both departments began to screen for patients who underwent operations for CSDH. Fur-thermore, we used the daily interdisciplinary neurosurgi-cal-neuroradiological conferences, where all elective and emergency cases were presented, as a second screening platform. Patients operated on for a CSDH who were 60 years of age or younger were eligible for spinal imaging workup. We excluded patients who died early (< 48 hours) due to epilepsy, who presented with recurrent SDH, who were not compliant during spinal imaging, who had recent brain surgery (< 6 months), or who had a shunt system for CSF diversion. As a next step, the computerized and writ-ten log books of all operating theaters were screened for patients with CSDH who had not been included in the study. A flow diagram of the number of patients at each stage of the study is provided in Fig. 1. An idealized dia-gram for how imaging modalities can be used, in order of increasing invasiveness, is shown in Fig. 2.Spinal Imaging
For MRI, a Magnetom Avanto 1.5-T or Magnetom Verio 3-T (Siemens) machine was used. The following sequences were employed: T1-weighted, T2-weighted, magnetization-prepared rapid acquisition gradient echo (MPRAGE), and sampling perfection with application of optimized contrasts using different flip angle evolutions (SPACE) with multiplanar reconstructions. In cases of intrathecal contrast application, gadopentetate dimeglu-mine (Magnevist, Bayer) at a standard dose of 0.5 ml dissolved in 9.5 ml CSF was administered via a lumbar puncture at the L3–5 level.
Myelography was performed using a Siemens Artis Zee Monoplan System (Siemens). A maximum dosage of 30 ml of iodine contrast material was administered after lumbar puncture using an atraumatic puncture kit. Post-myelography CT was performed on a LightSpeed Ultra scanner (GE) immediately after myelography and again 4 hours later in selected cases.
Stepwise Protocol of the SearchAfter a review of existing imaging results or sug-
gestions of CSF leaks, 3-T SPACE imaging of the com-plete spinal axis was conducted. Next, 0.5 ml of contrast medium (Magnevist) was injected intrathecally, and T1-weighted MRI of the spinal axis was completed. Myelog-raphy was then performed, and finally, postmyelography CT was completed. If a CSF leak was identified, the im-aging algorithm was stopped with the least invasive study. Example images from a patient are provided in Fig. 3; following the diagnosis of a CSDH (Fig. 3A), spinal im-aging without contrast demonstrated extrathecal fluid ac-cumulation (Fig. 3B). The CSF fistula was then proven by fluoroscopy (Fig. 3C) and postmyelography CT (Fig. 3D).
Classification of Spinal Imaging FindingsWe classified the findings of the spinal imaging ac-
cording to the likelihood of pathological CSF outflow from the intrathecal to the extrathecal space on a scale from 0 to 5 in an ascending manner (Table 1): no path-ological findings (category 0), detection of spinal men-ingeal cysts in the sacral region (category 1), detection of spinal meningeal cysts in the cervicothoracic region (category 2), detection of extrathecal fluid accumulation on spinal MRI without intrathecal contrast application (category 3), detection of extrathecal contrast (Magnev-ist/iopamidol 300 [Iopamiro, Bracco]) on spinal MRI or postmyelography CT after intrathecal administration of contrast (category 4), and direct visualization of outflow of intrathecally administered contrast (iodine) from the intrathecal to the extrathecal space under fluoroscopy (category 5). The proof of an existing CSF leak (catego-ries 4 and 5) was defined as the primary outcome.
Surgery for CSDHWhenever possible, the patients were operated on un-
der local anesthesia via the 2-bur-hole technique;18 drain insertion was performed if it was considered safe, after careful rinsing with large amounts of normal saline so-lution.26 For nonliquified space-occupying blood clots, open craniotomy under general anesthesia was the first procedure or a backup procedure.
Postsurgical CareAll patients were admitted to the intermediate care
unit or the intensive care unit after surgery. The drains were left in place, restricted to 10 ml/hr and 120 ml/day, for a maximum of 48 hours. Mobilization of patients was started on the day of surgery.
Treatment of Spinal CSF LeakIn cases in which a spinal CSF leak was detected, the
following treatment algorithm was used: 1) bed rest for as long as 3 days; 2) undirected blood patch at the L3–4 level (with an option to repeat the treatment if necessary); 3) directed blood patch under fluoroscopy or CT guid-ance (with an option to repeat the treatment if necessary); and 4) microsurgical exposure and closure of the CSF leak. For treatment options 3 and 4, the exact site of the
Unauthenticated | Downloaded 02/20/22 12:10 AM UTC

J. Beck et al.
1382 J Neurosurg / Volume 121 / December 2014
CSF leak had to be known. Depending on the severity of symptoms, the escalation from an undirected treatment (1 or 2) to a directed treatment (3 or 4) was accelerated, in-cluding emergency neuroradiological workup to find the spinal CSF leak and to enable directed treatment.
Patient OutcomeOutcome was assessed after 6 months during regu-
larly scheduled follow-up visits in the outpatient clinics. Patient outcome was based on the modified Rankin scale (mRS) score, working status, major neurological deficits, dependency, and living situation.
Statistical AnalysisFor descriptive statistics, data are expressed for con-
tinuous variables as means, standard deviations, and me-dians. Associations between categorical variables such as multiple recurrence, bilateral hematoma, head trauma, and CSF leak were calculated using a 2-sided Fisher exact test. Multiple logistic regression analysis was applied to
consider the event of a CSF leak or of a recurrent CSDH in relation to explanatory variables by forward selection. Because the sample size and the number of events were small, only a few explanatory variables and no interac-tions could be investigated together. The statistical analy-sis was conducted using SAS Enterprise Guide (version 4.3). A p value < 0.05 was considered indicative of a sig-nificant result.
ResultsPatient Characteristics and Clinical Findings
Nineteen men and 8 women, with a mean age of 49.6 ± 9.2 years (median 52.0 years), were included in the study (Table 2). Patient 1, who presented in November 2008 and whose clinical course led to the formation of our hypothesis, was included in the final analysis. The leading symptoms included headaches, neurological defi-cits, cranial nerve deficits, decreased level of conscious-ness, and seizures (Table 2). Fifteen patients (55.6%) had
Fig. 1. Flow chart showing the number of patients at each stage of this prospective cohort study. Two hundred twenty-one patients were screened and 27 patients underwent spinal imaging and were included in the final analysis.
Unauthenticated | Downloaded 02/20/22 12:10 AM UTC

J Neurosurg / Volume 121 / December 2014
Spinal CSF leakage and chronic subdural hematoma
1383
a history of head trauma, 1 patient was taking oral antico-agulants, and 4 patients were taking aspirin. Orthostatic headaches prevailed in 1 patient and were retrospectively documented in 2 additional cases. Thus, although the chief complaint of 15 patients was headache, for 12 of these patients the headache was not orthostatic; overall, 24 patients had no orthostatic symptoms.
Characteristics and Treatment of CSDHChronic SDHs were unilateral in 20 patients (74.1%)
and bilateral in 7 patients (25.9%; Table 2). Initial treat-ment was via 2-bur-hole trephination (25 cases), via 2-bur-hole trephination with conversion to craniotomy (1 case), and craniotomy (1 case). One patient showed a yel-lowish subdural fluid collection (hygroma, 3.7%), and 26 (96.3%) showed typical hematomas. Ten patients (37.0%) had recurrent CSDH treated with a total of 14 procedures. All patients who underwent operations for multiple recur-rences had a proven CSF leak (3 of 7 with a leak vs 0 of 20 without a leak; p = 0.012).
Results of Spinal ImagingAccording to our classification system (Table 1),
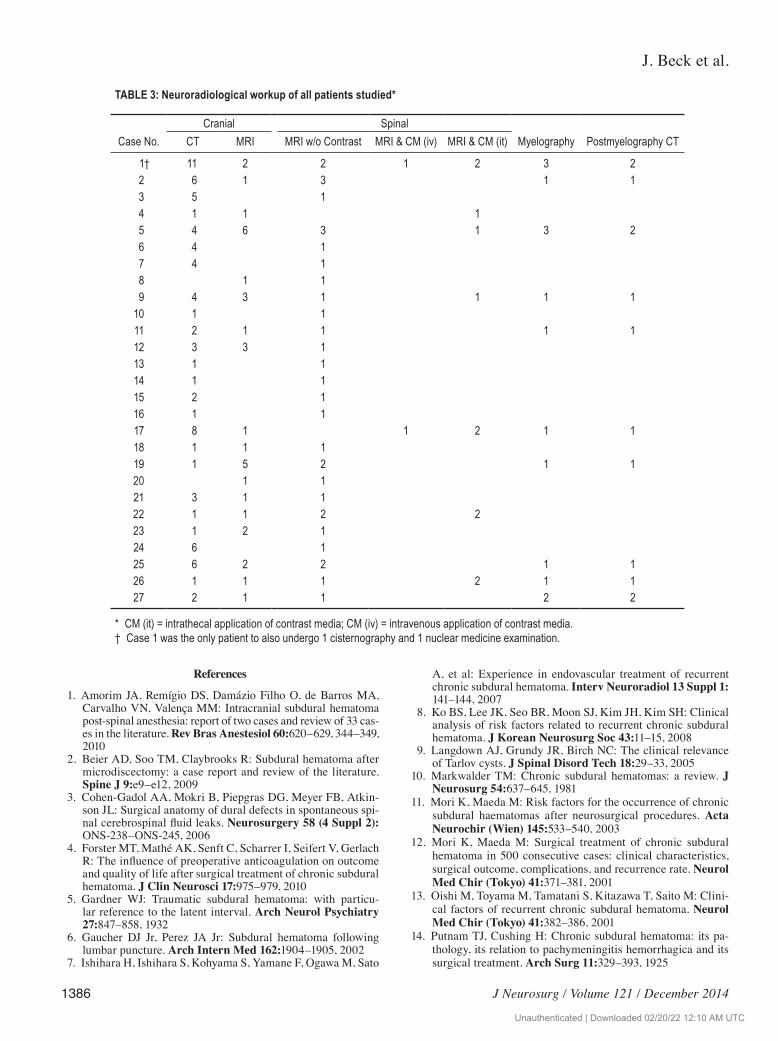
5 patients had a spinal CSF leak proven by direct visu-alization of contrast material outflow (category 5) and 2 patients had a spinal CSF leak proven by extrathecal contrast material accumulation after intrathecal applica-tion (category 4), resulting in 25.9% of patients with a proven CSF leak as the primary outcome. Spinal cervi-cothoracic meningeal cysts (category 2) were found in 9 patients (33.3%), including patients with multiple cysts. Cysts in the sacral region only (category 1) were detected in 3 cases (11.1%). No pathology (class 0) was found in 8 patients (29.6%). The specific imaging findings and imag-ing modalities used per patient are listed in Tables 2 and
3. Three (43%) of the 7 patients with proven CSF leaks had a history of head trauma as compared with 15 (75%) of 20 patients without a proven leak (p = 0.175). Imaging comprised 46 spinal MRI procedures, 15 myelographies, 13 postmyelography CT scans, 1 cisternography, and 1 nuclear medicine examination.
Treatment of Spinal CSF LeaksEight patients, including 7 with proven CSF leaks
and 1 without spinal pathology but with recurrent CSDH, were treated with 13 epidural blood-patching procedures. Three patients underwent 4 spinal microsurgical opera-tions for closure of the leak. Two of these patients needed microsurgery after repeated blood patching.
Patient OutcomeOutcome according to the mRS score at 6 months
was a score of 0 for 15 patients, a score of 1 for 9 pa-tients, and a score of 2 for 3 patients (Table 2). One of the
Fig. 2. Flow chart for spinal imaging. The diagram shows how we believe that imaging modalities can be used, in order of increasing inva-siveness, during the search for spinal CSF leaks and spinal meningeal cysts.
Fig. 3. Images from a patient with CSDH. Extrathecal fluid accu-mulation (arrowheads) was demonstrated by axial T2-weighted (A) and sagittal SPACE 3-T MRI (B). The spinal CSF leak was proven by direct visualization of the passage of contrast material from the intra- to the extrathecal space by anterior-posterior projection fluoroscopy (C). The leak is located in the thoracic spine (arrow) at the T10–11 level (C). The extradural accumulation of contrast material (arrow) is also demon-strated by postmyelography axial CT (D).
Unauthenticated | Downloaded 02/20/22 12:10 AM UTC

J. Beck et al.
1384 J Neurosurg / Volume 121 / December 2014
patients with an mRS score of 2 had suffered an ische-mic stroke 8 years earlier with persistent hemiparesis. All 27 patients lived independently at home and 25 (92.6%) returned to their previous work status. All patients were available for follow-up.
Multiple Logistic RegressionThe dependence of a CSF leak event was considered
with respect to the following variables: sex, trauma, or-thostatic headache, oral anticoagulation/aspirin, and bilat-eral CSDH. Only the lack of orthostatic headache (OR = 0.030, p = 0.030) and the presence of bilateral CSDH (OR = 21.33, p = 0.017) had significant impacts on the occur-rence of a CSF leak. The model assumptions and fit were checked (area under the curve = 0.836). The same model assumptions were used for the recurrence event with the same variables and also CSF leak. In this case, the pres-ence of bilateral CSDH (OR = 17.8, p = 0.03) and lack of trauma (OR = 0.059, p = 0.023) were significant factors. The model assumptions and fit were also checked (area un-der the curve = 0.889). Because of the small sample size with not many events in the explanatory variables, these results should be considered with caution. Multiple recur-rences were also considered, but because there were only 3 such events among the 27 patients, a multiple logistic regression did not produce an acceptable result. However, this event was dependent on CSF leak (p = 0.012, Fisher exact test) and trauma (p = 0.029, Fisher exact test).
DiscussionWith this prospective search for spinal pathologies
in a consecutive neurosurgical series of nongeriatric pa-tients with CSDH, we found an unexpectedly high rate of spinal CSF leaks (25.9%). Although spinal CSF leaks have been described as a potential cause of CSDH in rare cases, spinal CSF leakage has not been regarded as a fre-quent diagnosis and is therefore not included in a standard workup. Our findings suggest that investigation of spinal CSF leakage should be a mandatory part of a dedicated workup. In addition to the 25.9% of patients with directly proven CSF leaks, 33.3% of patients were found to have spinal cervicothoracic meningeal cysts. These cysts have been proposed as the cause or likely cause for spinal CSF outflow.20
Cerebrospinal Fluid Leakage as a Cause of CSDHsSpinal outflow of CSF may lead to sagging of the
brain,19 which may tear congested bridging veins and thus enable formation of a CSDH. A causal relationship between CSF outflow and CSDH is supported by the for-mation of CSDH as a complication of lumbar puncture,6 spontaneous intracranial hypotension (SIH),19,21 neurosur-gical shunting procedures,11,15 spinal anesthesia,1 spinal microdiscectomy with a dural tear,2 or any neurosurgical procedure associated with excessive CSF outflow.11
Until now, the clinical relevance and incidence of spi-nal CSF outflow for nongeriatric patients with CSDH has not been documented and is very likely underestimated. The prevailing diagnostics focus on iatrogenic mecha-nisms (such as spinal tap or CSF shunts) leading to CSF loss, whereas an occult, idiopathic, or acquired form of spinal CSF leakage that leads to CSDH is currently not regarded as a relevant differential diagnosis and is thus not routinely investigated. To our knowledge, a systematic study of spinal CSF leakage in patients with CSDH has never been performed or reported.
Because SIH is a possible diagnosis leading to CSDH, we specifically inquired about orthostatic symptoms at admission, and again during outpatient follow-up visits, including questioning of relatives. This led to identifica-tion of 3 patients (11%) with some orthostatic component. The majority of subdural fluid collections in SIH report-ed in the literature are hygromas (which do not usually require evacuation); in contrast, in our series there were only 4% hygromas and the remaining 96% were hemato-mas.3,23 Both disorders, CSDH and SIH, occur with the same incidence of about 5 per 100,000 people.16,19 Thus, it is extremely unlikely that a simultaneous occurrence of these disorders would happen by chance in 25.9% of a group of patients.
The presence of a spinal CSF leak might lead to dif-ferent clinical phenotypes (SIH or CSDH), which raises pathophysiological considerations. Whether there are dif-ferent kinds of spinal CSF leaks with specific anatomical or functional (flow) characteristics, with some leading to SIH and others to CSDH, or whether the clinical mani-festations change over time or represent a spectrum of a disease, is unknown.
Relevance of Spinal Meningeal CystsThe incidence and natural history of spinal meninge-
TABLE 1: Classification of imaging findings and the likelihood of spinal CSF leakage
Category Imaging Finding Imaging Modality Intrathecal Contrast Material Interpretation
0 no suggestion of CSF loss MRI, myelography, CT, cisternography Gd, iodine, radionuclide no CSF fistula1 spinal meningeal cyst, sacral region MRI, myelography, CT Gd, iodine CSF fistula unlikely2 spinal meningeal cyst, cervicothoracic region MRI, myelography, CT Gd, iodine CSF fistula likely3 extrathecal fluid detection w/o intrathecal
contrastMRI (T2 SPACE) — CSF fistula very likely
4 extrathecal contrast accumulation after intra- thecal contrast application
CT/MRI Gd, iodine CSF fistula proven
5 direct visualization of contrast passage from intrathecal to extrathecal space
fluoroscopy (myelography) iodine CSF fistula proven
Unauthenticated | Downloaded 02/20/22 12:10 AM UTC

J Neurosurg / Volume 121 / December 2014
Spinal CSF leakage and chronic subdural hematoma
1385
al cysts are not exactly known. Small perineural cysts in the region of the sacrum appear to have a benign course.9 Spinal meningeal cysts have been regarded as the source of CSF outflow,3,22 and Schievink and his group suggested that these are, together with imaging and clinical features, a diagnostic criterion for spinal CSF leaks.20 Spinal CSF leaks in combination with anticoagulation treatment were recently suggested as a cause of CSDH, particularly in elderly patients.22 Interestingly, all 3 reported patients in
that study had spinal cervicothoracic cysts (33.3%, com-parable to the current cohort) but none had a proven CSF leak. To take this into consideration, our classification dif-ferentiates proven CSF outflow (categories 4 and 5) from the mere presence of spinal cysts (categories 1 and 2).
Patient Profile and Risk FactorsThe reported incidence of recurrent CSDH varies
from 3% to 39%,4,17,24,27,30 with reports of second or mul-tiple recurrence ranging from 2% to 9%.4,7,18,24–26 Our series showed a high rate of first (33.3%), second (11.1%), and third recurrences (3.7%), but no reference group of nongeriatric patients with CSDH is available for comparison. Multiple recurrences occurred significantly more often in patients with proven CSF leaks (categories 4 and 5) as compared with patients without such leaks. What makes the multiple recurrences noteworthy is the fact that in 4 of the 7 current cases, the recurrence of the CSDH only stopped after the CSF leak was sealed. This finding supports the hypothesis of a causal relationship between CSF outflow and CSDH.
Other researchers have reported that patients with recurrent CSDH have a lower incidence of head trauma than patients without recurrent CSDH,13 as was also the case in the current series. In addition, bilateral CSDH and young age appear to involve a higher risk of recur-rence.8,12,26,27 The current report describes an association of bilateral hematomas, orthostatic headaches, and mul-tiple CSDH recurrences with a proven CSF leak. Based on our current observations, we suggest that criteria such as young age, early or multiple CSDH recurrence, con-tinuing or unexplained clinical deterioration, orthostatic headaches, or the presence of bilateral CSDH should ini-tiate the search for spinal CSF leaks.
ConclusionsSpinal imaging results are challenging the pathoge-
netic concept of CSDH in nongeriatric patients. Our re-sults support the hypothesis that spinal CSF leakage is a frequent cause of CSDH in young patients, which could influence the diagnostic and therapeutic management of these patients. Potential spinal CSF leaks should be me-thodically investigated in young patients and in patients with certain risk factors.
Disclosure
The authors report no conflict of interest concerning the mate-rials or methods used in this study or the findings specified in this paper.
Author contributions to the study and manuscript prepara-tion include the following. Conception and design: Beck, Raabe. Acquisition of data: Beck, Gralla, Fung, Ulrich, Schucht, Fichtner, Andereggen, Gutbrod, Z’Graggen, Reinert, Ozdoba, Raabe. Analysis and interpretation of data: Beck, Gralla, Fung, Ulrich, Gosau, Hattingen, Z’Graggen, Hüsler, Ozdoba, Raabe. Drafting the article: Beck, Fung, Gosau, Hattingen, Z’Graggen, Hüsler, Ozdoba, Raabe. Critically revising the article: all authors. Reviewed submit-ted version of manuscript: all authors. Approved the final version of the manuscript on behalf of all authors: Beck. Statistical analysis: Hüsler, Beck. Study supervision: Beck.
TABLE 2: Patient characteristics
Variable Value
age (yrs) mean ± SD 49.6 ± 9.2 median 52.0males (n = 19) mean age ± SD (yrs) 48.1 ± 9.7 median age 51.0females (n = 8) mean age ± SD (yrs) 53.1 ± 7.1 median age 55.5leading symptoms (multiple) headache 15 somnolence 4 coma 1 seizure 2 mydriasis 1 hemiparesis 3 ataxia 2 apraxia 2 perseveration 1 paresthesia 1 cranial nerve deficit 2 cognitive decline 1 delirium 1location of CSDH rt 11 lt 9 bilat 7category of spinal CSF leak 0 8 1 3 2 9 3 0 4 2 5 5warfarin therapy 1aspirin 4mRS score at 6 mos 0 15 1 9 2 3
Unauthenticated | Downloaded 02/20/22 12:10 AM UTC
J. Beck et al.
1386 J Neurosurg / Volume 121 / December 2014
References
1. Amorim JA, Remígio DS, Damázio Filho O, de Barros MA, Carvalho VN, Valença MM: Intracranial subdural hematoma post-spinal anesthesia: report of two cases and review of 33 cas-es in the literature. Rev Bras Anestesiol 60:620–629, 344–349, 2010
2. Beier AD, Soo TM, Claybrooks R: Subdural hematoma after microdiscectomy: a case report and review of the literature. Spine J 9:e9–e12, 2009
3. Cohen-Gadol AA, Mokri B, Piepgras DG, Meyer FB, Atkin-son JL: Surgical anatomy of dural defects in spontaneous spi-nal cerebrospinal fluid leaks. Neurosurgery 58 (4 Suppl 2): ONS-238–ONS-245, 2006
4. Forster MT, Mathé AK, Senft C, Scharrer I, Seifert V, Gerlach R: The influence of preoperative anticoagulation on outcome and quality of life after surgical treatment of chronic subdural hematoma. J Clin Neurosci 17:975–979, 2010
5. Gardner WJ: Traumatic subdural hematoma: with particu-lar reference to the latent interval. Arch Neurol Psychiatry 27:847–858, 1932
6. Gaucher DJ Jr, Perez JA Jr: Subdural hematoma following lumbar puncture. Arch Intern Med 162:1904–1905, 2002
7. Ishihara H, Ishihara S, Kohyama S, Yamane F, Ogawa M, Sato
A, et al: Experience in endovascular treatment of recurrent chronic subdural hematoma. Interv Neuroradiol 13 Suppl 1: 141–144, 2007
8. Ko BS, Lee JK, Seo BR, Moon SJ, Kim JH, Kim SH: Clinical analysis of risk factors related to recurrent chronic subdural hematoma. J Korean Neurosurg Soc 43:11–15, 2008
9. Langdown AJ, Grundy JR, Birch NC: The clinical relevance of Tarlov cysts. J Spinal Disord Tech 18:29–33, 2005
10. Markwalder TM: Chronic subdural hematomas: a review. J Neurosurg 54:637–645, 1981
11. Mori K, Maeda M: Risk factors for the occurrence of chronic subdural haematomas after neurosurgical procedures. Acta Neurochir (Wien) 145:533–540, 2003
12. Mori K, Maeda M: Surgical treatment of chronic subdural hematoma in 500 consecutive cases: clinical characteristics, surgical outcome, complications, and recurrence rate. Neurol Med Chir (Tokyo) 41:371–381, 2001
13. Oishi M, Toyama M, Tamatani S, Kitazawa T, Saito M: Clini-cal factors of recurrent chronic subdural hematoma. Neurol Med Chir (Tokyo) 41:382–386, 2001
14. Putnam TJ, Cushing H: Chronic subdural hematoma: its pa-thology, its relation to pachymeningitis hemorrhagica and its surgical treatment. Arch Surg 11:329–393, 1925
TABLE 3: Neuroradiological workup of all patients studied*
Cranial SpinalCase No. CT MRI MRI w/o Contrast MRI & CM (iv) MRI & CM (it) Myelography Postmyelography CT
1† 11 2 2 1 2 3 22 6 1 3 1 13 5 14 1 1 15 4 6 3 1 3 26 4 17 4 18 1 19 4 3 1 1 1 1
10 1 111 2 1 1 1 112 3 3 113 1 114 1 115 2 116 1 117 8 1 1 2 1 118 1 1 119 1 5 2 1 120 1 121 3 1 122 1 1 2 223 1 2 124 6 125 6 2 2 1 126 1 1 1 2 1 127 2 1 1 2 2
* CM (it) = intrathecal application of contrast media; CM (iv) = intravenous application of contrast media.† Case 1 was the only patient to also undergo 1 cisternography and 1 nuclear medicine examination.
Unauthenticated | Downloaded 02/20/22 12:10 AM UTC

J Neurosurg / Volume 121 / December 2014
Spinal CSF leakage and chronic subdural hematoma
1387
15. Samuelson S, Long DM, Chou SN: Subdural hematoma as a complication of shunting procedures for normal pressure hy-drocephalus. J Neurosurg 37:548–551, 1972
16. Santarius T, Hutchinson PJ: Chronic subdural haematoma: time to rationalize treatment? Br J Neurosurg 18:328–332, 2004
17. Santarius T, Kirkpatrick PJ, Ganesan D, Chia HL, Jalloh I, Smielewski P, et al: Use of drains versus no drains after burr-hole evacuation of chronic subdural haematoma: a ran-domised controlled trial. Lancet 374:1067–1073, 2009
18. Santarius T, Kirkpatrick PJ, Kolias AG, Hutchinson PJ: Work-ing toward rational and evidence-based treatment of chronic subdural hematoma. Clin Neurosurg 57:112–122, 2010
19. Schievink WI: Spontaneous spinal cerebrospinal fluid leaks and intracranial hypotension. JAMA 295:2286–2296, 2006
20. Schievink WI, Maya MM, Louy C, Moser FG, Tourje J: Di-agnostic criteria for spontaneous spinal CSF leaks and intra-cranial hypotension. AJNR Am J Neuroradiol 29:853–856, 2008
21. Schievink WI, Maya MM, Moser FG, Tourje J: Spectrum of subdural fluid collections in spontaneous intracranial hypo-tension. J Neurosurg 103:608–613, 2005
22. Schievink WI, Maya MM, Pikul BK, Louy C: Spontaneous spinal cerebrospinal fluid leaks as the cause of subdural he-matomas in elderly patients on anticoagulation. Report of 3 cases. J Neurosurg 112:295–299, 2010
23. Sencakova D, Mokri B, McClelland RL: The efficacy of epidural blood patch in spontaneous CSF leaks. Neurology 57:1921–1923, 2001
24. Smely C, Madlinger A, Scheremet R: Chronic subdural hae-matoma–a comparison of two different treatment modalities. Acta Neurochir (Wien) 139:818–826, 1997
25. Stroobandt G, Fransen P, Thauvoy C, Menard E: Pathogenetic factors in chronic subdural haematoma and causes of recur-rence after drainage. Acta Neurochir (Wien) 137:6–14, 1995
26. Tahsim-Oglou Y, Beseoglu K, Hänggi D, Stummer W, Steiger HJ: Factors predicting recurrence of chronic subdural haema-toma: the influence of intraoperative irrigation and low-mo-lecular-weight heparin thromboprophylaxis. Acta Neurochir (Wien) 154:1063–1068, 2012
27. Torihashi K, Sadamasa N, Yoshida K, Narumi O, Chin M, Ya-magata S: Independent predictors for recurrence of chronic subdural hematoma: a review of 343 consecutive surgical cases. Neurosurgery 63:1125–1129, 2008
28. Trotter W: Chronic subdural haemorrhage of traumatic origin, and its relation to pachymeningitis haemorrhagica interna. Br J Surg 2:271–291, 1914
29. Virchow R: Das haematom der dura mater. Verh Phys Med Ges Würzburg 7:134–142, 1857
30. Weigel R, Schmiedek P, Krauss JK: Outcome of contempo-rary surgery for chronic subdural haematoma: evidence based review. J Neurol Neurosurg Psychiatry 74:937–943, 2003
Manuscript submitted September 26, 2013.Accepted June 9, 2014.Please include this information when citing this paper: pub-
lished online July 18, 2014; DOI: 10.3171/2014.6.JNS14550.Address correspondence to: Jürgen Beck, M.D., Department of
Neurosurgery, Bern University Hospital, Freiburgstrasse 10, Bern 3010, Switzerland. email: [email protected].
Unauthenticated | Downloaded 02/20/22 12:10 AM UTC





























