Embed Size (px)
Citation preview

VOL. 21, NO. 4, 1995 Speech and LanguageDisorders in Childrenand Adolescents WithSchizophrenia
677
by Christiane AM Baltaxe andJames Q. Simmons III
Abstract
This study examines communica-tion characteristics and specificlanguage deficits in 47 childrenand adolescents diagnosed withearly-onset schizophrenia usingDSM-HI-R criteria. All had beenreferred for speech and languageservices because of apparentcommunication problems. Stand-ardized tests and formal meas-ures were used to identify im-pairment in discrete areas ofcommunication, including prag-matics, receptive and expressivevocabulary and syntax, abstractlanguage, auditory processing,and speech production. Resultsshowed that these discrete areaswere variably involved, withpragmatics, prosody, auditoryprocessing, and abstract languagehaving the greatest involvement.The communication deficits iden-tified in the early-onset groupclosely resembled the phenome-nology reported in studies of thecommunication characteristics ofadults with schizophrenia. Thiscomparison thus lends furthersupport to the presence of thesame disorder as seen in adults.The roles of gender, mental re-tardation, and seizure disordersare also discussed as additionalrisk factors in the developmentof communication problems andschizophrenia.
Schizophrenia Bulletin, 21(4):677-692, 1995.
Speech and language disordershave been demonstrated to coexistwith a wide range of childhoodand adolescent psychiatric condi-tions, including infantile autism(Baltaxe and Simmons 1981;Prizant et al. 1990), attention defi-
cit disorder (Baker and Cantwell1992), and other behavioral andemotional disorders (Beitchman etal. 1986; Baltaxe and Simmons1988, 1990).
One such condition is schizo-phrenia with onset in childhood oradolescence, a relatively rare disor-der affecting approximately 3youngsters in 10,000 (Graham1986). The diagnosis of schizophre-nia in childhood and adolescencehas not been uniquely defined andis made using diagnostic criteriafor the adult disorder. Thus, thediagnostic criteria for schizophreniainclude the presence of a thoughtdisorder, hallucinations, motilitydisturbances, and disturbances insocial relationships. In childhood,thought disorders and hallucina-tions are among the main differen-tial criteria that distinguish schizo-phrenia from other psychiatricconditions, particularly autism, per-vasive developmental disorder (nototherwise specified), and schizoty-pal personality disorder. Additionalconsiderations in differentiatingschizophrenia from these otherconditions involve the age at onsetand family history (Cohen et al.1986; Rutter and Schopler 1987).
Because a thought disorder man-ifests itself in language, the charac-teristics of language have alwaysbeen among the key diagnosticfeatures of schizophrenia(Kraepelin 1919/1971; Bleuler1911/1950; Andreasen 1979a, 1979b;American Psychiatric Association1987). A thought disorder can takethe form of incoherence, marked
Reprint requests should be sent toDr. C.A.M. Baltaxe, UCLA Neuropsy-chiatric Institute and Hospital, Centerof the Health Sciences, 760 WestwoodPlaza, Los Angeles, CA 90024-1759.
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/21/4/677/1883961 by guest on 21 D
ecember 2021

678 SCHIZOPHRENIA BULLETIN
loosening of associations, illogi-cality, and poverty of content ofspeech (formal thought disorder).It can also manifest itself in delu-sions of various types (content ofthought disorder). Closely associ-ated are prodromal and residuallinguistic symptoms of schizophre-nia, which include language that ischaracterized as digressive, vague,overelaborate, circumstantial, andimpoverished in content as well asoutput, according to DSM-UI—R(American Psychiatric Association1987).
The linguistic manifestations ofthought disorder in adults andchildren have been studiedthrough instruments with knownvalidity and reliability (Andreasen1979a, 1979b; Arboleda and Holz-man 1985; Caplan et al. 1990;Caplan 1994) and through formaldiscourse analysis, an aspect ofpragmatics (Rochester and Martin1979). Considered from the per-spective of pragmatics (or the useof language in a social context),most manifestations of thought dis-order in persons with schizophre-nia have been identified as a dys-function in a speaker-hearer rolerelationship (Andreasen 1979a,1979b; Rochester and Martin 1979;Baltaxe and Simmons 1987). Theemergence of these impairments incommunication are assumed to co-incide with the onset of the schiz-ophrenic disorder (DSM-III-R;American Psychiatric Association1987).
In addition to delays and abnor-malities in behavioral, emotional,and motor development, a signifi-cant number of children also ap-pear to have delays and abnor-malities in language development(Beitchman 1983; Graham 1986).Direct and indirect evidence forthe existence of developmental lan-
guage delays and abnormalitiesyears before the onset of schizo-phrenia is documented in severalsources. One source is retrospec-tive and followup studies of schiz-ophrenia in childhood and adoles-cence. Although many of thesestudies make no reference to earlylanguage characteristics, delays,and abnormalities, others discussthese briefly as part of the generaldevelopmental picture (Bender andFaretra 1972; Eggers 1978; Kyddand Werry 1982; Green et al. 1984;Garralda 1985; Watkins et al.1987). Another source of datacomes from risk factor studies inwhich early developmental indica-tors including language are dis-cussed (Mednick and Schulsinger1965; Harvey et al. 1982; Fish1987; Sameroff et al. 1987; Wein-traub 1987). And finally, a thirdsource is studies relating to chil-dren with schizophrenia with earlyautistic symptomatology (Benderand Faretra 1972; Petty et al. 1984;Watkins et al. 1987). These studiesgenerally distinguish between earlylanguage delay and abnormalitiesand the subsequent verbal man-ifestation of a thought disorder.All clearly indicate that in a sig-nificant number of children andadolescents, early language delaysand abnormalities were prominentamong the premorbid symptoms ofschizophrenia. The delays and ab-normalities noted in these studiesare summarized and further dis-cussed by Baltaxe and Simmons(submitted for publication). Theseauthors concluded that languagedysfunction may be an early andsignificant neurodevelopmental in-dicator of schizophrenia.
Because of the retrospective na-ture of most of the studies, noneused formal tests to assess earlycommunication behaviors in their
schizophrenia subjects. Therefore, itis not clear to what extent discreteareas of speech and language wereseriously disturbed early in de-velopment. It is also not clear towhat extent disturbances in dis-crete areas of communication areidentifiable after the schizophreniahas been diagnosed. The presentstudy is designed to examine thespecific communication characteris-tics and deficits in children andadolescents diagnosed with schizo-phrenia and referred for speechand language services because ofobvious communication involvement.
Standardized and formal meas-ures will be used to identify dys-functions in discrete areas of com-munication and to examine theirrelevance to schizophrenia. Theseare areas usually considered inchildren suspected of communica-tion handicaps. Most of theseareas have also been those investi-gated separately in studies ofadult schizophrenia. Because of thepaucity of specific information cur-rently available on communicationdeficits in early-onset schizophre-nia, the findings from this studywill be examined from the per-spective of what is known aboutthese areas in adult schizophrenia.Deficits similar to those seen inadults may provide additional evi-dence for the presence of the samedisorder in childhood.
Methods
Subjects. The subjects were 47patients admitted to the child andadolescent inpatient services of theUniversity of California, Los An-geles, Neuropsychiatric Institute, anacute care psychiatric facility. Theyoungsters ranged in age from 6.9through 17.2 years; their mean agewas 13 years, 4 months (standard
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/21/4/677/1883961 by guest on 21 D
ecember 2021

VOL. 21, NO. 4, 1995 679
deviation [SD] = 3 years, 10months). Eight of trie subjectswere under the age of 10 years,and 39 were 10 years and older.Seventy percent (n = 33) weremale, and 30 percent (n = 14)were female. Sixty-seven percent(n = 25) were white, 24 percent (n= 8) black, and 8 percent (n = 3)Hispanic. Seven subjects had anadditional diagnosis of mental re-tardation (5 mild, 1 moderate, and1 severe). Five were also diag-nosed with a seizure disorder. Allwere fluent in English and all hadbeen referred for speech and lan-guage services because of obviousor suspected communicationinvolvement.
Psychiatric Assessment. The psy-chiatric diagnoses were based ondata obtained by structured andsemistructured psychiatric inter-views with the children and theirparents. Psychiatric diagnoses weremade according to the diagnosticcriteria specified in DSM-III-R. Di-agnoses were made independentlyby a psychiatrist and an inter-disciplinary treatment team; issuesconcerning the diagnoses were re-solved by consensus between thepsychiatrist and the interdisciplin-ary treatment team.
Communication Assessment. Allsubjects received a completespeech and language evaluation bya speech pathologist. Assessmenttools included standardizedspeech / language tests and formalprocedures for analyzing spon-taneous speech samples. Areas ofspeech (including articulation, flu-ency, voice, and prosody) and lan-guage (including abstract language,syntax, vocabulary [expression, re-ception], auditory processing, andpragmatics) were assessed. Defini-tions of each of these areas of lan-
guage are presented in the appen-dix. All subjects were cooperativeduring testing, and none were onmedications when they weretested.
In general, impairment in anarea of language functioning wasoperationally defined as standard-ized test scores 1 or more SDs be-low the norm for the child's agelevel. For the seven youngsterswho had mental retardation (i.e., asignificant discrepancy betweenchronological age and mental agelevels), language impairments werediagnosed in relation to non-language mental age (i.e., perform-ance intelligence) levels. Specificexplanations of how each area oflanguage was assessed in the pres-ent study -and operational defini-tions of what constituted a deficitin each area in the present studyare provided in the appendix.
Results
Table 1 indicates the numbers andpercentages of youngsters with
schizophrenia who were impairedin the various areas of speech andlanguage assessed. As this tableshows, pragmatics (or the interac-tional use of language) was thearea of language impaired in thegreatest number of youngsters—83percent. The other two areas oflanguage most frequently impairedwere prosody (or the melody ofspeech), which was impaired in 81percent of the youngsters, and au-ditory processing, which was im-paired in 72 percent.
Approximately two-thirds of allsubjects (64%) were impaired inunderstanding and formulating ab-stract language. Receptive and ex-pressive vocabulary was deficientin close to two-thirds of the sub-jects (62%). Receptive and expres-sive syntax (i.e., the understandingand use of different sentencetypes) were impaired in approx-imately one-half of the subjects(51%), as was speech fluency(53%). Fewer impairments wereseen in speech articulation and
Table 1. Discrete areas of communication impairment in 47youngsters with schizophrenia
Areas of communicationNo.
impaired Impaired
Pragmatics
Language
Receptive vocabularyReceptive syntaxExpressive vocabularyExpressive syntaxAbstract language
Auditory processing
SpeechArticulationFluencyVoiceProsody
39
2924292430
34
18251238
83
6251625164
72
38532681
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/21/4/677/1883961 by guest on 21 D
ecember 2021
680 SCHIZOPHRENIA BULLETIN
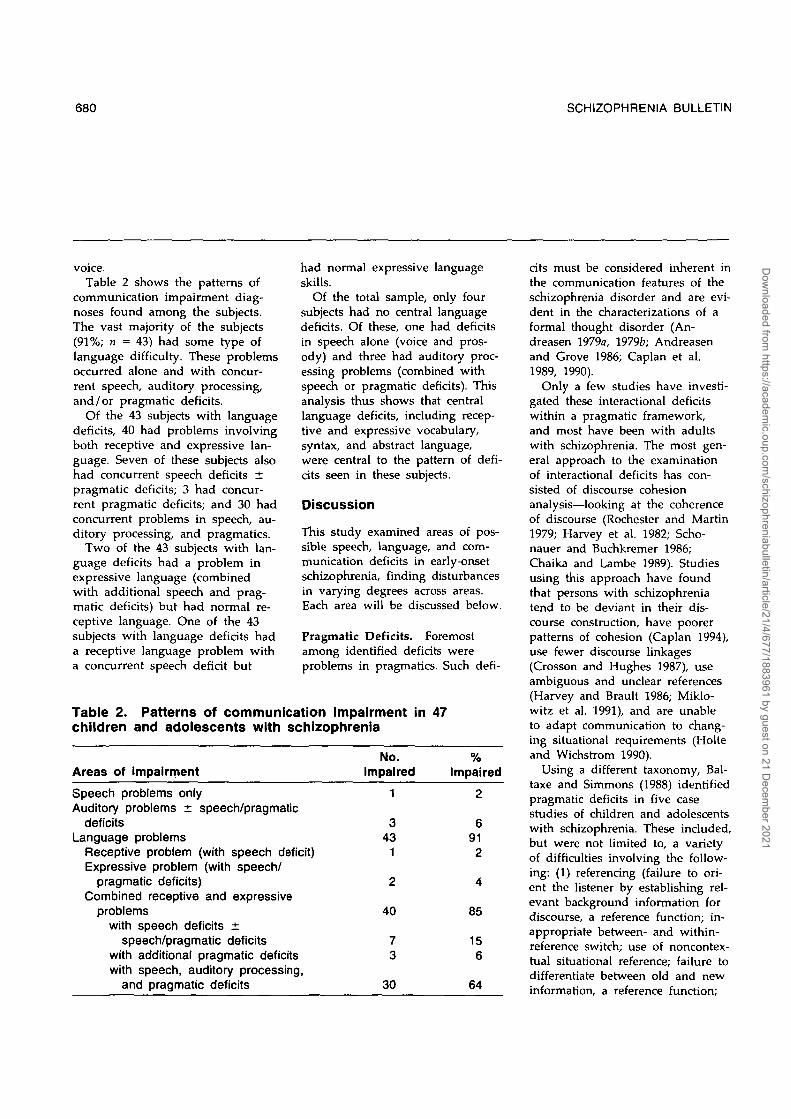
voice.Table 2 shows the patterns of
communication impairment diag-noses found among the subjects.The vast majority of the subjects(91%; n = 43) had some type oflanguage difficulty. These problemsoccurred alone and with concur-rent speech, auditory processing,and /or pragmatic deficits.
Of the 43 subjects with languagedeficits, 40 had problems involvingboth receptive and expressive lan-guage. Seven of these subjects alsohad concurrent speech deficits ±pragmatic deficits; 3 had concur-rent pragmatic deficits; and 30 hadconcurrent problems in speech, au-ditory processing, and pragmatics.
Two of the 43 subjects with lan-guage deficits had a problem inexpressive language (combinedwith additional speech and prag-matic deficits) but had normal re-ceptive language. One of the 43subjects with language deficits hada receptive language problem witha concurrent speech deficit but
had normal expressive languageskills.
Of the total sample, only foursubjects had no central languagedeficits. Of these, one had deficitsin speech alone (voice and pros-ody) and three had auditory proc-essing problems (combined withspeech or pragmatic deficits). Thisanalysis thus shows that centrallanguage deficits, including recep-tive and expressive vocabulary,syntax, and abstract language,were central to the pattern of defi-cits seen in these subjects.
Discussion
This study examined areas of pos-sible speech, language, and com-munication deficits in early-onsetschizophrenia, finding disturbancesin varying degrees across areas.Each area will be discussed below.
Pragmatic Deficits. Foremostamong identified deficits wereproblems in pragmatics. Such defi-
Table 2. Patterns of communication impairment in 47children and adolescents with schizophrenia
Areas of impairment
Speech problems onlyAuditory problems ± speech/pragmatic
deficitsLanguage problems
Receptive problem (with speech deficit)Expressive problem (with speech/
pragmatic deficits)Combined receptive and expressive
problemswith speech deficits ±
speech/pragmatic deficitswith additional pragmatic deficitswith speech, auditory processing,
and pragmatic deficits
No.impaired
1
343
1
2
40
73
30
%Impaired
2
6912
4
85
156
64
cits must be considered inherent inthe communication features of theschizophrenia disorder and are evi-dent in the characterizations of aformal thought disorder (An-dreasen 1979a, 1979fc; Andreasenand Grove 1986; Caplan et al.1989, 1990).
Only a few studies have investi-gated these interactional deficitswithin a pragmatic framework,and most have been with adultswith schizophrenia. The most gen-eral approach to the examinationof interactional deficits has con-sisted of discourse cohesionanalysis—looking at the coherenceof discourse (Rochester and Martin1979; Harvey et al. 1982; Scho-nauer and Buchkremer 1986;Chaika and Lambe 1989). Studiesusing this approach have foundthat persons with schizophreniatend to be deviant in their dis-course construction, have poorerpatterns of cohesion (Caplan 1994),use fewer discourse linkages(Crosson and Hughes 1987), useambiguous and unclear references(Harvey and Brault 1986; Miklo-witz et al. 1991), and are unableto adapt communication to chang-ing situational requirements (Holteand Wichstrom 1990).
Using a different taxonomy, Bal-taxe and Simmons (1988) identifiedpragmatic deficits in five casestudies of children and adolescentswith schizophrenia. These included,but were not limited to, a varietyof difficulties involving the follow-ing: (1) referencing (failure to ori-ent the listener by establishing rel-evant background information fordiscourse, a reference function; in-appropriate between- and within-reference switch; use of noncontex-tual situational reference; failure todifferentiate between old and newinformation, a reference function;
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/21/4/677/1883961 by guest on 21 D
ecember 2021

VOL. 21, NO. 4, 1995 681
and lack of reference and inap-propriate ellipsis of reference); (2)topic selection, maintenance, andswitch (difficulties establishingtopic of discourse, inappropriatetopic switch, inappropriate topicexpansion, topic switch to self); (3)sequencing of discourse (difficultiesdescribing events in time and log-ically sequencing utterances withina discourse); and (4) turn-takingproblems. The pragmatic deficitsseen in the present study mirroredthe deficits discussed above relat-ing to reference and difficultieswith changing register, topic, se-quencing, and turn taking. Prag-matic deficits seen in children withschizophrenia thus appear to mir-ror those reported for adults withschizophrenia.
Receptive and Expressive Vo-cabulary and Syntax. The find-ings in this study showed thatmore than half the subjects wereimpaired in receptive and expres-sive vocabulary and syntax. Littleinformation is currently availableon the receptive language skills ofchildren with schizophrenia. How-ever, the results appear to agreewith what little information isavailable, primarily in adults. Also,Waterhouse and Fein (1984) dem-onstrated lower receptive and ex-pressive vocabulary scores for thegroup of children with schizophre-nia they studied compared withnormal controls. Similarly, Fish(1987), in her study of children atrisk for schizophrenia, noted adrop in vocabulary scores in sevenof her subjects and in comprehen-sion scores on the Wechsler Intel-ligence Scale for Children-Revised(Wechsler 1974) comprehensionsubtest in five of her subjects be-tween 10 and 15 years of age.However, these findings are in
contrast with those of Schneiderand Asarnow (1987), who foundno such difference between thechildren with schizophrenia andthe normal controls they studied.
With respect to receptive syntax,Morice and McNicol (1985) investi-gated the comprehension of com-plex grammatical structures inadults with schizophrenia, using amodified version of the Token Test(DiSimoni 1978). Their results dem-onstrated an impairment of com-prehension that was proportionalto a reduction in the syntacticcomplexity of their spoken lan-guage. These investigators found asignificant correlation between theschizophrenia patients' receptiveand expressive skills.
The existence of deficits in theexpressive syntax of adults withschizophrenia has been shown in aseries of studies using computer-assisted linguistic analysis of freespeech samples (Fraser et al. 1986;Thomas et al. 1987; Fraser et al.1989; King et al. 1990; Thomas etal. 1990). These studies showedthat the syntactic structures ofspeech in adult schizophrenia sub-jects were less complex than thoseof normal controls. Patients withschizophrenia used less clausal em-bedding, fewer reduced relativeclauses, more syntactically and se-mantically deviant sentences, andmore syntactic errors.
The above investigators alsodemonstrated that syntactic and se-mantic errors were state-dependentfeatures associated with positiveschizophrenia symptoms, whereasa reduction in syntactic complexitywas associated with the presenceof negative symptoms. Expressivesyntax also appeared to deteriorateas a function of the schizophrenicprocess. Differences in the freespeech samples of acute and
chronic subjects with schizophreniawere seen on measures of syntac-tic complexity, integrity (errors),and fluency, with acute patientsperforming less well than the nor-mal controls but better than thechronic patients. The authors con-cluded that linguistic deteriorationin their adult subjects was relatedto the illness process.
Although comparable studies inearly-onset schizophrenia are stilllacking, the results of the presentstudy appear to parallel those inthe above adult studies with re-spect to receptive and expressivevocabulary, syntax, and fluency.The subjects showed lower agescores and demonstrated more er-rors in receptive and expressivevocabulary, less syntactic complex-ity than expected for their ages,and a considerable amount of dys-fluency. It cannot be determined inthe context of the present studywhether these receptive and ex-pressive deficits were developmen-tal in origin or whether they are afunction of the schizophrenicprocess.
Receptive/Expressive AbstractLanguage. The current studyidentified deficits in the under-standing and use of abstract lan-guage in close to two-thirds of thesubjects. Difficulties with abstractlanguage have been shown to existin adults with schizophrenia andhave been considered a characteris-tic of the disorder. Thus, Goldstein(1944) noted that "expressions ofabnormal concreteness" are charac-teristic of schizophrenia; Arieti(1974) described the language im-pairment in schizophrenia as "animpairment in the ability to ab-stract"; Kasanin (1944) referred toa reduced ability "to think ab-stractly"; and Moran (1953) re-
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/21/4/677/1883961 by guest on 21 D
ecember 2021

682 SCHIZOPHRENIA BULLETIN
ferred to a "lesser capacity to dealwith abstract analogies."
Difficulties with abstract lan-guage have been found in a num-ber of empirical studies of adultswith schizophrenia. Cutting et al.(1987) used four tests of categori-cal thinking and found that thosewith schizophrenia showed ele-vated rates of conceptual looseningand overcategorization. Cuttingand Murphy (1990) studied de-notative and connotative meaningsand found elevated rates of diffi-culty with metaphorical meaning.
Deficits in abstract language arealso characteristic of children withcommunication handicaps (deAjuriaguerra et al. 1976; Nippoldand Fey 1983). Abstract languagethus appears to be an area wherelanguage characteristics expected inchildren and adolescents withschizophrenia and language charac-teristics of those with languagedisorders intersect. Within the cur-rent context, it is not possible todetermine if deficits in abstractlanguage are more closely associ-ated with communication impair-ment or schizophrenia. However,deficits in abstract language againappeared to mirror the adult phe-nomenology of schizophrenia.
Auditory Processing. Almostthree-fourths of the current sub-jects showed significant deficits inthe auditory processing of lan-guage. Deficient auditory process-ing in its various designations hasbeen associated with schizophrenia,communication handicaps, andlearning disorders. In its broadestsense, attentional deficits, includingthe auditory channel, have beenregarded as characteristic of theschizophrenic disorder since itsearliest description (Kraepelin1919/1971). Although there is no
direct evidence that attentional def-icits predispose to schizophrenia(Rutter and Garmezy 1983), thesedeficits also were the most consis-tent findings in high-risk studies(Erlenmeyer-Kimling et al. 1984).The attentional and informationprocessing deficits described byWeintraub (1987) for children ofmothers with schizophrenia in-cluded an inability to maintain at-tention and to ignore irrelevant in-formation. Everett et al. (1989)noted that subjects with schizo-phrenia have difficulty maintainingselective attention over time. Man-schreck et al. (1988) suggested anattentional deficit hypothesis forschizophrenic language functioningbased on the results of a study ofsemantic priming in those withschizophrenia who have thoughtdisorders. More recently, Barchand Berenbaum (1994) proposedthat reduced processing capacitymay underlie the decreased syn-tactic complexity, decreasedverbal output, and increasedpause length reported in thosewith schizophrenia.
With respect to auditory mem-ory, Weiss et al. (1988) concludedthat auditory information overloadseverely disrupted the performanceon digit recall of those with schiz-ophrenia. Wood and Flowers(1990) determined an auditorymemory deficit for narrative prosethat they associated with a uniquelanguage-related focal deficit inschizophrenia. Huang et al. (1990)described possible conflicting re-sults. In a study of recall and lan-guage characteristics via storyschemata they showed that adultswith schizophrenia did not havean impaired ability to recall storyschemata.
Auditory memory deficits werealso found by Goldberg et al.
(1989), who compared adults withschizophrenia with other neuro-psychiatric and normal controls byusing a selective reminding testand by Goldberg et al. (1990) in astudy of monozygotic twins discor-dant for schizophrenia. These in-vestigators also found deficits invigilance and concept formation.Auditory memory deficits in schiz-ophrenia were found by Silversteinet al. (1988).
Asarnow et al. (1987) concludedthat children with schizophreniahad problems in the recruitmentand allocation of this momentaryprocessing capacity. Limitations inrecruitment and allocation of proc-essing capacity have also beenconsidered core impairments inadult schizophrenia (Nuechterleinand Dawson 1984). Soares andCollet (1988) concluded that thosewith schizophrenia showed an al-teration in the cognitive processesunderlying the processing and re-constitution of simple messages.Rund (1988) noted that attentionfocusing and information process-ing seemed to be the most con-spicuous disturbances in schizo-phrenia. Similarly, a dysfunctionalauditory information processingsystem was posited by Wale andCarr (1988) in a study of dichoticlistening asymmetries in schizo-phrenia. Finally, in a study of theN400 component of event-relatedpotentials in patients with schizo-phrenia, Grillon et al. (1991) sug-gested that N400 amplitude abnor-malities identified in adults withschizophrenia suggested a delay ininformation processing.
A number of studies have alsoassociated auditory processing defi-cits with communication handicaps(Heins et al. 1976; Keith et al.1989). However, recent studieshave also shown that higher level
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/21/4/677/1883961 by guest on 21 D
ecember 2021

VOL. 21, NO. 4, 1995 683
language deficits are not attributa-ble to difficulties in the more pre-liminary analysis of acoustic stim-uli (Akshoomoff et al. 1989). Thus,although auditory processing defi-cits show a high co-occurrencewith language deficits, they do notappear to be essential for the de-velopment of communicationdisorders.
The above studies seem toprovide evidence that auditoryprocessing deficits in those withschizophrenia and the communica-tion handicapped are not uni-dimensional. Rather, these deficitsmay range over a number of indi-vidual components associated withthe auditory processing of informa-tion as this term is defined in theappendix. It is of interest that onlythree subjects in the current studyhad auditory processing deficitswithout central language deficitwhile in all other instances, theauditory processing deficits co-occurred with central languageproblems. The deficits seen in thepresent study were based on theimmediate recall of digits, unre-lated words, and sentences. In thecurrent context, it cannot be deter-mined whether these deficits weremore closely associated with theschizophrenic process or the lan-guage disorder. Rutter (1987) notedthat deficits in the ability to proc-ess incoming information may leadto subsequent biases and distor-tions in cognitive processing andbe associated with social and emo-tional malfunction.
Speech Disorders. Only foursubjects had problems in speech(i.e., articulation, voice, fluency,and prosody) without also havingconcurrent central languagedeficits.
Voice. The deficient vocal
characteristics found includedhypo- and hypernasality, breathi-ness, whispering, and subvocaliza-tion. These difficulties have notbeen discussed specifically in theliterature on schizophrenia. How-ever, Cantor et al. (1981) describedhypotonic children and adolescentswith schizophrenia, and we knowhyponasality is often a vocal corre-late of hypotonia. Similarly, Bickand Kinsbourne (1987) describedsubvocalizations in adults withschizophrenia (and subvocalizationmay reflect a voice disorder).
Voice disorders may also occuras an aspect of a communicationdisorder picture. It is not clearwhether the voice disorders identi-fied here uniformly relate moreclosely to the schizophrenic proc-ess or to the communication disor-der pattern.
Fluency. This study found thatsomewhat more than half the sub-jects had speech fluency problems.Fluency problems have been de-scribed in adult schizophrenia inseveral ways. Andreasen (1979a,1979b) described three distinct for-mal thought disorders, which in-clude a fluency factor and affectthe flow of speech: thought block-ing, distractible speech, and pres-sure of speech. In thought block-ing the speaker's train of thoughtis interrupted and the flow ofspeech is interrupted, sometimesby pauses lasting from seconds tominutes in which the patient can-not recall what he is saying orwhat he meant to say. In distract-ible speech the patient stops talk-ing in the middle of a sentence oridea and changes the subject in re-sponse to the intrusion of anotherstimulus. Dysfluency occurs in theform of pausing, false starts, anddisruptions by changes in topic orlack of sentence completion. Dis-
ruptions may occur at the soundand syllable level, but are morelikely to occur at the word,phrase, or sentence level. In pres-sure of speech, sentences may beleft incomplete because of the pa-tient's eagerness to get an ideaacross. The speaker may also usefalse starts and perseverations andalter the speed of speech flow.
A fluency factor was also recog-nized by Holzman et al. (1986),who included a "fragmentation"parameter in their revised ThoughtDisorder Index (Solovay et al.1986). Also, fluency tests are in-cluded in many neuropsychologicalstudies of schizophrenia (Goldberget al. 1988; Gruzelier et al. 1988;Williamson et al. 1989; Sagawa etal. 1990; Cleghorn et al. 1991).
As noted above, dysfluency hasalso been found to be a significantfactor in linguistic studies ofadults with schizophrenia (Thomaset al. 1990). Dysfluency also occursin isolation and as part of a moregeneral communication disorderpicture. However, the incidence ofthe dysfluencies in communication-disordered populations does notappear to be as high as that seenin the present results. The resultsappear to show a phenomenologysimilar to that of adults withschizophrenia who show consider-able fluency problems.
Prosody. More than four-fifthsof the subjects also had disturb-ances in expressive prosody. Pro-sodic disturbances are frequentlymentioned as part of the abnor-malities seen in schizophrenicspeech (Alpert 1981) and often ap-pear in the guise of affective flat-tening or blunting (Andreasen1982; American Psychiatric Associa-tion 1987). Bleuler (1911/1950) de-scribed distortions in the pitch,loudness, and duration of speech
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/21/4/677/1883961 by guest on 21 D
ecember 2021

684 SCHIZOPHRENIA BULLETIN
as well as in the incongruence ofaffective intonation with the con-tent of the message. Ostwald(1980) used spectrographic analysisto identify anomalous patterns ofvocal behavior in schizophrenia.
Prosody in schizophrenia hasgenerally been associated with pro-duction characteristics. For exam-ple, Fricchione et al. (1986) studiedaprosodia in eight subjects withschizophrenia and found thatseven had aprosodia with associ-ated motor components. On theother hand, Murphy and Cutting(1990) studied both prosodic com-prehension and expression inschizophrenia and showed thatthose with schizophrenia were sig-nificantly inferior to normal con-trols on emotional prosody com-prehension and had a significantinferiority in emotional prosodyexpression.
From the perspective of com-munication handicaps, prosodic ab-normalities are most often seen inneurological disturbances wherethey are associated with righthemisphere lesions (Borod et al.1989). Prosodic disturbances do notappear to occur with great fre-quency in children and adolescentswith pure communication hand-icaps. When they are seen, thesedisturbances generally are second-ary to motor speech disturbancessuch as dysarthria or apraxia. Theexception is obvious abnormalitiesin verbal children with autism.The high incidence of prosodicdisturbances in the current sample,again, appears to parallel the phe-nomenology of adult schizophrenia.
In summary, the results of thepresent study reveal a close paral-lel to the speech, language, andcommunication characteristics re-ported in adult schizophrenia. Onthe other hand, several of the
characteristics also appear to sup-port the notion of a spectrum ofdisorders affecting social communi-cation (Tanguay 1990). Close paral-lels to the communication deficitsseen in high-functioning autistic in-dividuals are discussed by Baltaxeand Simmons (1992a).
Concerning the issue of genderand the presence of mental retar-dation and seizure disorders, thisstudy used a referred clinical sam-ple, so these factors were not con-trolled. However, they are impor-tant because they have beenidentified as possible risk factorsfor both communication disordersand schizophrenia.
Retrospective, followup, andhigh-risk studies had indicated thata significant number of childrenand adolescents with early-onsetschizophrenia had communicationdelays and abnormalities, oftenpreceding the disorder. It is notcurrently clear to what degreeearlier deficits continue to exist atthe time of full-blown schizophre-nia and to what degree they re-flect aspects of the schizophreniaitself. This may be a difficult ques-tion to answer because the riskfactors associated with the onset ofschizophrenia, such as pregnancy,birth complications, and illnessesaffecting the central nervous sys-tem, are also the risk factors re-lated to the development of com-munication handicaps (Rutter andGarmezy 1983; Shaffer 1985).
Gender. Although schizophreniain the adult population is dis-tributed approximately evenlyamong the sexes (American Psychi-atric Association 1987), in youngerage groups the disorder is morecommonly seen in males (Graham1986). The current results, with amale-to-female ratio of approx-
imately 2.3:1, are in agreementwith these findings. However,Beitchman (1983), in a review ofthe literature, noted that the gen-der ratio of schizophrenia in chil-dren varied widely, depending onthe particular study. Because de-velopmental communication hand-icaps occur more frequently inmales than females, the greatermale prevalence in the presentsample may be due to the pres-ence of communication handicapsin all subjects (Baltaxe and Sim-mons 1992b). We suggest thatpresence or absence of a com-munication handicap may also ac-count for the inconsistencies ingender ratios reported by Beitch-man (1983). The potential com-pounding effect of language dis-abilities on the gender variable inearly-onset schizophrenia thereforedeserves further scrutiny.
Mental Retardation. Seven of thesubjects had a diagnosis of mentalretardation. Rutter et al. (1970) hadnoted that psychiatric disturbancesin childhood are often associatedwith a low IQ. Corbett (1985) ob-served that, etiologically, it is morelikely for low IQ to antedate thepsychiatric disorder. However, ageneral deterioration in cognitivefunction can be expected with thedevelopment of schizophrenia(American Psychiatric Association1987).
Mental retardation results in de-lays in language development.However, because mental retarda-tion may be associated with a va-riety of underlying causes, addi-tional language problems can alsobe expected beyond the delay as-sociated with a lower mental age(Miller 1981). It is not possiblehere to determine whether the ad-ditional communication handicaps
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/21/4/677/1883961 by guest on 21 D
ecember 2021

VOL 21, NO. 4, 1995 685
in the seven mentally retardedsubjects were associated with un-derlying causes, which may alsohave played a role in the develop-ment of the schizophrenia or theschizophrenia process itself.
Seizure Disorders. The presentsample included five youngsterswho, in addition to the diagnosisof schizophrenia, also had a sei-zure disorder. Shaffer (1985) notedthat individuals with such disor-ders are at particular risk for de-veloping psychiatric disorders.Graham (1986) observed that chil-dren with long-standing temporallobe epilepsy seemed to be atgreater risk for the development ofschizophrenia. Several authors havealso suggested that the develop-ment of a psychosis, includingschizophrenia, is particularly evi-dent when epilepsy begins duringpuberty (Slater et al. 1963). The in-crease of other developmental ab-normalities early in life often re-ported for individuals with early-onset schizophrenia may be an ad-ditional risk factor for the develop-ment of the schizophrenic disorder(Beitchman 1983; Graham 1986).Such developmental abnormalitiesare frequently further linked withan increased incidence of en-cephalitis, neoplasms, irradiation,prenatal trauma, and seizure disor-ders. An excess of obstetric com-plications appears to characterizethe histories of patients with schiz-ophrenia in general (O'Callaghanet al. 1990). Wilcox and Nasrallah(1987) also reported an increasedincidence of head trauma beforethe age of 10 for individuals withearly-onset schizophrenia. Associ-ated chronic brain syndromes mayplace some children and adoles-cents at greater risk for schizo-phrenia (Steinberg 1985). Such un-
derlying causes are frequently alsoassociated with communicationhandicaps (McGee et al. 1984).Communication-handicapped chil-dren commonly show a history ofprenatal and perinatal difficultiesand encephalitic and other diseaseprocesses affecting the brain. Sei-zure disorders, in particular tem-poral lobe epilepsy, are oftenlinked to communication hand-icaps. Again, the exact interrela-tionship between the three typesof disorders—schizophrenia, seizuredisorder, and communicationhandicap—cannot be determinedwithin the scope of the presentstudy.
In summary, the above studydemonstrates that children and ad-olescents with early-onset schizo-phrenia show a broad variety ofcommunication deficits. Most ofthese parallel deficits also seen inadult schizophrenia seem to pre-sent further evidence in support ofthe continuity of the schizophreniadisorder from childhood to adoles-cence. However, this investigationalso points up linguistic similaritiesto such developmental disorders asautism and pervasive developmen-tal disorder (not otherwise spec-ified) particularly in pragmaticdeficits, prosodic disturbances, dys-fluencies, and deficits with abstractlanguage, but also in receptive andexpressive syntax. The presentfindings thus appear to supportthe notion of a spectrum of disor-ders, all affecting social communi-cation. It is not clear to what ex-tent the deficits seen in thecurrent study also have their rootsin an earlier developmental delayand, perhaps, contribute to theearly onset of the schizophreniadisorder. Future studies areneeded to focus on these andother issues to further explore the
areas of communication deficitsidentified above and to comparethe differences between early-onsetschizophrenia subjects with clearlyidentified communication deficitsand those with less obvious signsof communication impairment.
References
Akshoomoff, N.; Courchesne, E.;Yeung-Courchesne, R.; and Cos-tello, J. Brainstem auditory evokedpotentials in receptive developmen-tal language disorders. Brain andLanguage, 37(3):409^18, 1989.
Alpert, M. Speech and disturb-ances of affect. In: Darby, J., ed.Speech Evaluation in Psychiatry.New York, NY: Grune & Stratton,1981. pp. 359-367.
American Psychiatric Association.DSM-II1-R: Diagnostic and Statisti-cal Manual of Mental Disorders. 3rded., revised. Washington, DC: TheAssociation, 1987.
Andreasen, N.C. Thought, lan-guage, and communication disor-ders: I. Definition of terms andtheir reliability. Archives of GeneralPsychiatry, 36(12):1315-1321, 1979a.
Andreasen, N.C. Thought, lan-guage, and communication disor-ders: II. Diagnostic significance.Archives of General Psychiatry,36(12):1325-1330, 1979b.
Andreasen, N.C. Negative symp-toms of schizophrenia. Archives ofGeneral Psychiatry, 39:784-788,1982.
Andreasen, N.C, and Grove, W.M.Thought, language, and communi-cation in schizophrenia: Diagnosisand prognosis. Schizophrenia Bul-letin, 12(3):348-359, 1986.
Arboleda, C, and Holzman, P.S.Thought disorder in children atrisk for psychosis. Archives of Gen-
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/21/4/677/1883961 by guest on 21 D
ecember 2021

686 SCHIZOPHRENIA BULLETIN
eral Psychiatry, 42(10):1004-1013,1985.
Arieti, S. Interpretation of Schizo-phrenia. New York, NY: BasicBooks, 1974.
Asarnow, R.; Tanguay, P.; Bott, L.;and Freeman, B. Patterns of intel-lectual functioning in non-retardedautistic and schizophrenic children.Journal of Child Psychology andPsychiatry, 28(2):273-280, 1987.
Baker, L., and Cantwell, D.P. At-tention deficit disorder andspeech / language disorder. Com-prehensive Mental Health Care, 2:3-16, 1992.
Baltaxe, C.A.M., and Simmons, J.Q.Disorders of language in childhoodpsychosis: Current concepts andapproaches. In: Darby, J., ed.Speech Evaluations in Psychiatry.New York, NY: Grune & Stratton,1981. pp. 285-328.
Baltaxe, C.A.M., and Simmons, J.Q.Communication deficits in the ado-lescent with autism, schizophrenia,and language-learning disabilities.In: Layton, T., ed. Language andTreatment of Autistic and Develop-mentally Disordered Children.Springfield, IL: Charles C Thomas,1987. pp. 155-186.
Baltaxe, C.A.M., and Simmons, J.Q.Communication deficits in pre-school children with psychiatricdisorders. Seminars in Speech andLanguage, 9(1):81-91, 1988.
Baltaxe, C.A.M., and Simmons, J.Q.The differential diagnosis of com-munication disorders in child andadolescent psychopathology. Topicsin Language Disorders, 10(4):17-31,1990.
Baltaxe, C.A.M., and Simmons, J.Q.A comparison of language issuesin high-functioning autism and re-lated disorders with onset in child-hood and adolescence. In: Schopler,
E., and Mesibov, G.B., eds. Com-munication and Autism. New York,NY: Plenum Press, 1992a.pp. 201-225.
Baltaxe, C.A.M., and Simmons, J.Q.Gender-related vulnerability tocommunication disorders in chil-dren and adolescents with psychi-atric disorders. Journal of BrainDysfunction, 5:239-252, 1992b.
Baltaxe, C.A.M., and Simmons, J.Q."Age Related Differences in Com-munication Disorders of Childrenand Adolescents With PsychiatricDisorders." Submitted forpublication.
Barch, D., and Berenbaum, H. Therelationship between informationprocessing and language produc-tion. Journal of Abnormal Psychol-ogy, 103:241-250, 1994.
Beitchman, J. Childhood schizo-phrenia: A review and comparisonwith adult onset schizophrenia.Psychiatric journal of the Universityof Ottawa, 8:25-37, 1983.
Beitchman, J.; Nair, R.; Clegg, M;Ferguson, B.; and Patel, P. Preva-lence of psychiatric disorders inchildren with speech and languagedisorders. Journal of the AmericanAcademy of Child Psychiatry,25:528-535, 1986.
Bender, L., and Faretra, G. The re-lationship between childhood andadult schizophrenia. In: Kaplan, A.,ed. Genetic Factors in Schizophrenia.Springfield, IL: Charles C Thomas,1972. pp. 28-64.
Bick, P.A., and Kinsbourne, M.Auditory hallucinations and sub-vocal speech in schizophrenic pa-tients. American Journal of Psychia-try, 144(2):222-225, 1987.
Bleuler, E. Dementia Praecox or theGroup of Schizophrenias. (1911)Translated by J. Zinkin. New York,
NY: International UniversitiesPress, 1950.Borod, J.C.; Alpert, M; Brozgold,A.; Martin, C; Welkowitz, J.; Dil-ler, L.; Peselow, E.; Angrist, B.;and Lieberman, A. A preliminarycomparison of flat affect schizo-phrenics and brain-damaged pa-tients on measures of affectiveprocessing. Journal of Communica-tion Disorders, 22(2):93-104, 1989.
Cantor, S.; Pearce, J.; Pezzot-Pearce, T.; and Evans, J. Thegroup of hypotonic schizophrenics.Schizophrenia Bulletin, 7(1):1—11,1981.
Caplan, R. Thought disorder inchildhood. Journal of the AmericanAcademy of Child Psychiatry,33:605-615, 1994.
Caplan, R.; Guthrie, D.; Fish, B.;Tanguay, P.E.; and David-Lando,G. The Kiddie Formal ThoughtDisorder Scale (K-FTDS). Clinicalassessment, reliability, and validity.Journal of the American Academy ofChild Psychiatry, 28:208-216, 1989.
Caplan, R.; Perdue, S.; Tanguay,P.E.; and Fish, B. Formal thoughtdisorder in childhood onset schizo-phrenia and schizotypal personalitydisorder. Journal of Child Psychol-ogy and Psychiatry, 31(7):1103-1114,1990.
Carrow-Woolfolk, E. Test for Audi-tory Comprehension of Language —Revised (TACL-R). Allen, TX: DLMTeaching Resources, 1985.
Chaika, E., and Lambe, R.A. Cohe-sion in schizophrenic narratives,revisited. Journal of CommunicationDisorders, 22(6):407-421, 1989.
Cleghorn, J.M.; Kaplan, R.D.;Szechtman, B.; Szechtman, H.;Brown, G.M.; and Franco, S. Sub-stance abuse and schizophrenia:Effect on symptoms but not onneurocognitive function. Journal of
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/21/4/677/1883961 by guest on 21 D
ecember 2021

VOL. 21, NO. 4, 1995 687
Clinical Psychiatry, 52(l):26-30,1991.
Cohen, D.; Volkmar, R.; and Paul,R. Issues in the classification ofpervasive developmental disorders:History and current status ofnosology. Journal of the AmericanAcademy of Child Psychiatry,25:158-161, 1986.
Corbett, J. Mental retardation: Psy-chiatric aspects. In: Rutter, M., andHersov, L., eds. Child and Adoles-cent Psychiatry: Modern Approaches.Oxford, England: Blackwell Scien-tific Publications, 1985. pp. 661-678.
Crosson, B., and Hughes, C.W.Role of the thalamus in language:Is it related to schizophrenicthought disorder? SchizophreniaBulletin, 13(4):605-621, 1987.
Cutting, J.; David, A.; and Mur-phy, D. The nature of overinclu-sive thinking in schizophrenia. Psy-chopathology, 20(3-4):213-219, 1987.
Cutting, J., and Murphy, D. Prefer-ence for denotative as opposed toconnotative meanings in schizo-phrenics. Brain and Language,39(3):459-468, 1990.
de Ajuriaguerra, J.; Jaeggi, A.;Guignard, F.; Kocher, F.; Maquard,M.; Rother, S.; and Schmidt, E.The development and prognosis ofdysphasia in children. In: More-head, D.M., and Morehead, A.E.,eds. Normal and Deficient ChildLanguage. Baltimore, MD: Univer-sity Park Press, 1976. pp. 345-385.
DiSimoni, F. The Token Test forChildren. Boston, MA: Teaching Re-sources, 1978.
Dunn, L.M., and Dunn, L.M. Pea-body Picture Vocabulary Test-Revised. Circle Pines, MN: Ameri-can Guidance Service, 1981.
Eggers, C. Course and prognosisof childhood schizophrenia. Journalof Autism and Childhood Schizophre-nia, 8(l):21-35, 1978.
Erlenmeyer-Kimling, L.A.; Marcuse,Y.; Cornblatt, B.; Friedman, D.;Rainder, J.D.; and Rutschmann, J.The New York High Risk Project.In: Watt, N.; Anthony, E.J.;Wynne, L.C.; and Rolf, J., eds.Children at Risk for Schizophrenia:A Longitudinal Perspective. NewYork, NY: Cambridge UniversityPress, 1984. pp. 169-189.
Everett, J.; Laplante, L; andThomas, J. The selective attentiondeficit in schizophrenia. Limitedresources or cognitive fatigue?Journal of Nervous and Mental Dis-ease, 177(12):735-738, 1989.
Fish, B. Infant predictors of thelongitudinal course of schizo-phrenic development. SchizophreniaBulletin, 13(3):395-i09, 1987.
Fraser, W.I.; King, K.; and Thomas,P. Computer-assisted linguisticanalysis of two mentally retardedpsychotic female's texts. Journal ofMental Deficiency Research,33(5):429-435, 1989.
Fraser, W.I.; King, K.; Thomas, P.;and Kendell, R. The diagnosis ofschizophrenia by language analysis.British Journal of Psychiatry, 148:275-278, 1986.
Fricchione, G.; Sedler, M.J.; andShukla, S. Aprosodia in eightschizophrenic patients. AmericanJournal of Psychiatry, 143(11):1457-1459, 1986.
Gardner, M.F. Expressive One WordPicture Vocabulary Test-Revised.Novato, CA: Academic TherapyPublications, 1983.
Gardner, M.F. Test of Auditory Per-ceptual Skills (TAPS). San Fran-cisco, CA: Children's Hospital ofSan Francisco, 1985.
Garralda, M. Characteristics of thepsychoses of late onset in childrenand adolescents: A comparativestudy of hallucinating children.Journal of Adolescence, 8:195-208,1985.
Goldberg, T.E.; Kelsoe, J.R.; Wein-berger, D.R.; Pliskin, N.H.; Kirwin,P.D.; and Berman, K.F. Perform-ance of schizophrenic patients onputative neuropsychologial tests offrontal lobe function. InternationalJournal of Neuroscience, 42(1-2):51-58, 1988.
Goldberg, T.E.; Ragland, J.D.; Tor-rey, E.F.; Gold, J.M.; Bigelow, L.B.;and Weinberger, D.R. Neuropsy-chological assessment of mono-zygotic twins discordant for schiz-ophrenia. Archives of GeneralPsychiatry, 47(11): 1066-1072, 1990.
Goldberg, T.E.; Weinberger, D.R.;Pliskin, N.H.; Berman, K.F.; andPodd, M.H. Recall memory deficitin schizophrenia: A possible man-ifestation of prefrontal dysfunction.Schizophrenia Research, 2(3):251-257,1989.
Goldman, R., and Fristoe, M. Gold-man Fristoe Test of Articulation.Circle Pines, MN: American Guid-ance Service, 1986.
Goldstein, K. Methodological ap-proach to the study of schizo-phrenic thought disorder. In: Ka-sanin, J.S., ed. Language andThought in Schizophrenia. NewYork, NY: W.W. Norton & Com-pany, 1944. pp. 17-78.
Graham, P. Child Psychiatry: A De-velopmental Approach. Oxford, Eng-land: Oxford Medical Publications,1986.
Green, W.; Campbell, M.; Hard-esty, A.; Grega, D.; Padron-Gayol,M.; Shell, M; and Erlenmeyer-Kimling, L. A comparison of schiz-ophrenic and autistic children.
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/21/4/677/1883961 by guest on 21 D
ecember 2021

688 SCHIZOPHRENIA BULLETIN
Journal of the American Academy ofChild Psychiatry, 23:399-409, 1984.
Grillon, C; Ameli, R.; and Glazer,W.M. N400 and semantic categori-zation in schizophrenia. BiologicalPsychiatry, 29(5):467-480/ 1991.
Gruzelier, J.; Seymour, K.; Wilson,L.; Jolley, A.; and Hirsch, S. Im-pairments on neuropsychologictests of temporohippocampal andfrontohippocampal functions andword fluency in remitting schizo-phrenia and affective disorders.Archives of General Psychiatry,45(7):623-629, 1988.
Hammill, D.D. Detroit Tests ofLearning Aptitude (DTLA-2). Aus-tin, TX: Pro-Ed, 1985.
Harvey, P.D., and Brault, J. Speechperformance in mania and schizo-phrenia: The association of positiveand negative thought disordersand reference failures. Journal ofCommunication Disorders, 19(3):161-173, 1986.
Harvey, P.D.; Weintraub, S.; andNeale, J.M. Speech competence ofchildren vulnerable to psycho-pathology. Journal of AbnormalChild Psychology, 10(3):373-387,1982.
Heins, E.D.; Hallahan, D.P.; andTarver, S.G. Relationship betweencognitive tempo and selective at-tention in learning disabled chil-dren. Perceptual and Motor Skills,42:233-234, 1976.
Holte, A., and Wichstrom, L. Dis-confirmatory feedback in familiesof schizophrenics. ScandinavianJournal of Psychology, 31(3):198-211,1990.
Holzman, P.S.; Shenton, M.E.; andSolovay, M.R. Quality of thoughtdisorder in differential diagnosis.Schizophrenia Bulletin, 12(3):360-371,1986.
Huang, C.Z.; Huang, H.L.; Chang,J.F.; Young, S.S.; and Lee, G.H. Astudy of recall and languagecharacteristics in schizophrenia viastory schema analysis. Kao-Hsiung1 Hsueh Ko Hsueh Tsa Chih Kaoh-siung Journal of Medical Sciences,6(l):22-29, 1990.
Kasanin, J., ed. Language andThought in Schizophrenia. NewYork, NY: W.W. Norton & Com-pany, 1944.
Keith, R.W.; Rudy, J.; Donahue,P.A.; and Katbamna, B. Com-parison of SCAN results withother auditory and language meas-ures in a clinical population. Earand Hearing, 10(6):382-386, 1989.
King, K.; Fraser, W.; Thomas, P.;and Kendell, R. Re-examination ofthe language of psychotic subjects.British Journal of Psychiatry,156:211-215, 1990.
Kraepelin, E. Dementia Praecox andParaphrenia. (1919) Translated byR.M. Barclay. New York, NY:Robert E. Krieger Publishing Com-pany, 1971.Kydd, R., and Werry, J. Schizo-phrenia in children under 16years. Journal of Autism and De-velopmental Disorders, 12(4):343-357,1982.
Manschreck, T.C.; Maher, B.A.;Milavetz, ].].; Ames, D.; Weisstein,C.C.; and Schneyer, ML. Semanticpriming in thought disorderedschizophrenic patients. Schizophre-nia Research, l(l):61-66, 1988.
McGee, R.; Williams, S.; and Silva,P. Background characteristics ofaggressive, hyperactive, and ag-gressive, hyperactive boys. Journalof the American Academy of ChildPsychiatry, 23:280-284, 1984.
Mednick, S.A., and Schulsinger, F.A longitudinal study of childrenwith a high risk for schizophrenia:
A preliminary report. In: Vanden-berg, S., ed. Methods and Coals inHuman Behavior Genetics. NewYork, NY: Academic Press, 1965.pp. 255-296.
Miklowitz, D.J.; Velligan, D.I.;Goldstein, M.J.; Nuechterlein, K.H.;Gitlin, M.J.; Ranlett, G.; andDoane, J.A. Communication de-viance in families of schizophrenicand manic patients. Journal of Ab-normal Psychology, 100(2): 163-173,1991.
Miller, ]. Assessing Language Pro-duction in Children: ExperimentalProcedures. Baltimore, MD: Univer-sity Park Press, 1981.
Moran, L.J. Vocabulary knowledgeand usage among normal andschizophrenic subjects. PsychologicalMonographs, 67(20):l-19, 1953.
Morice, R., and McNicol, D. Thecomprehension and production ofcomplex syntax in schizophrenia.Cortex, 21(4):567-580, 1985.
Murphy, D., and Cutting, ]. Pro-sodic comprehension and expres-sion in schizophrenia. Journal ofNeurology, Neurosurgery and Psychi-atry, 53(9):727-730, 1990.
Nippold, M., and Fey, S. Meta-phoric understanding in pre-adolescents having a history oflanguage acquisition difficulties.Language, Speech and Hearing Serv-ices in the Schools, 14:171-180,1983.
Nuechterlein, K.H., and Dawson,M.E. Information processing andattentional functioning in the de-velopmental course of schizo-phrenic disorders. SchizophreniaBulletin, 10(2): 160-203, 1984.
O'Callaghan, E.; Larkin, C; andWaddington, J.L. Obstetric com-plications in schizophrenia and thevalidity of maternal recall. Psycho-logical Medicine, 20(l):89-94, 1990.
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/21/4/677/1883961 by guest on 21 D
ecember 2021

VOL. 21, NO. 4, 1995 689
Ostwald, P. Speech and schizo-phrenia. In: Darby, J., ed. SpeechEvaluations in Psychiatry. NewYork, NY: Grune & Stratton, 1980.pp. 329-338.
Petty, L.; Ornitz, E.; Michelman, J.;and Zimmerman, E. Autistic chil-dren who become schizophrenic.Archives of General Psychiatry,41:129-135, 1984.
Prizant, B.; Audet, L.; Burke, G.;Hummel, L.; Maher, S.; and The-odore, G. Communication disordersand emotional/behavioral disordersin children and adolescents, journalof Speech and Hearing Disorders,55:179-192, 1990.
Prutting, C.A., and Kirchner, D.M.A clinical appraisal of the pragma-tic aspects of language, journal ofSpeech and Hearing Disorders,52:105-119, 1987.
Rochester, S., and Martin, J. CrazyTalk: A Study in the Discourse ofSchizophrenic Speakers. New York,NY: Plenum Press, 1979.
Rund, B.R. Cognitive disturbancesin schizophrenics: What are they,and what is their origin? Ada Psy-chiatrica Scandinavica, 77(2):113-123,1988.
Rutter, M. The role of cognition inchild development and disorder.British journal of Medical Psychol-ogy, 60:1-6, 1987.
Rutter, M., and Garmezy, N. De-velopmental psychopathology. In:Hetherington, E.M., ed. Socializa-tion, Personality, and Social Develop-ment: Handbook of Child Psychology.Vol. 4. New York, NY: John Wiley& Sons, 1983. pp. 775-911.
Rutter, M., and Schopler, E. Au-tism and pervasive developmentaldisorders: Concepts and diagnosticissues, journal of Autism and De-velopmental Disorders, 17(2):159-187,1987.
Rutter, M.; Tizard, J.; and Whit-more, K. eds. Education, Health,and Behavior. London, England:Longmans, 1970.
Sagawa, K.; Kawakatsu, S.;Shibuya, I.; Oiji, A.; Morinobu, S.;Komatani, A.; Yazaki, M.; and Tot-suka, S. Correlation of regionalcerebral blood flow with perform-ance on neuropsychological tests inschizophrenic patients. Schizophre-nia Research, 3(4):241-246, 1990.Sameroff, A.; Seifer, R.; Zax, M.;and Barocas, R. Early indicators ofdevelopmental risk: Rochester lon-gitudinal study. Schizophrenia Bul-letin, 13(3):383-394, 1987.
Schneider, S.G., and Asarnow, R.F.A comparison of cognitive/neuro-psychological impairments of non-retarded autistic and schizophrenicchildren, journal of Abnormal ChildPsychology, 15(1):29^5, 1987.
Schonauer, K., and Buchkremer, G.Some linguistic aspects of thoughtdisorder in non-acute schizophre-nia. European Archives of Psychiatryand Neurological Sciences, 236(3):179-186, 1986.
Semel, E.; Wiig, E.H.; and Secord,W. Clinical Evaluation of LanguageFundamentals-Revised (CELF-R).San Antonio, TX: PsychologicalCorporation, 1987.
Shaffer, D. Brain damage. In: Rut-ter, M., and Hersov, L., eds. Childand Adolescent Psychiatry: ModernApproaches. Oxford, England: Black-well Scientific Publications, 1985.pp. 129-151.
Silverstein, M.L.; McDonald, C;and Meltzer, H.Y. Differential pat-terns of neuropsychological deficitin psychiatric disorders, journal ofClinical Psychology, 44(3):412^115,1988.
Slater, E.; Beard, A.W.; andClithero, E. The schizophrenia-like
psychoses of epilepsy. British Jour-nal of Psychiatry, 109:95-105, 1963.
Soares, I., and Collet, L. Relation-ships between verbal intelligence,educational level and reconstitutionof linguistic messages in schizo-phrenia. International Journal ofNeuroscience, 38:69-74, 1988.
Solovay, M.R.; Shenton, M.E.; Gas-peretti, C; Coleman, M.; Kestn-baum, E.; Tyler Carpenter, J.; andHolzman, P.S. Scoring manual forthe Thought Disorder Index. Schiz-ophrenia Bulletin, 12(3):483- i96,1986.
Steinberg, D. Psychotic and otherdisorders in adolescence. In: Rut-ter, M., and Hersov, L., eds. Childand Adolescent Psychiatry: ModernApproaches. Oxford, England: Black-well Scientific Publications, 1985.pp. 567-583.
Tanguay, P. Infantile autism andsocial communication spectrum dis-orders. [Editor's note] Journal ofAmerican Academy of Child and Ad-olescent Psychiatry, 29:854, 1990.
Thomas, P.; King, K.; and Fraser,W.I. Positive and negative symp-toms of schizophrenia and linguis-tic performance. Acta PsychiatricaScandinavica, 76(2):144-151, 1987.
Thomas, P.; King, K.; Fraser, W.I.;and Kendell, R.E. Linguistic per-formance in schizophrenia: A com-parison of acute and chronic pa-tients. British Journal of Psychiatry,156:204-210, 214-215, 1990.
Wale, J., and Carr, V. Dichotic lis-tening asymmetries and psychoticsymptoms in schizophrenia: A pre-liminary report. Psychiatry Research,25(l):31-39, 1988.
Waterhouse, L., and Fein, D. De-velopmental trends in cognitiveskills for children diagnosed as au-tistic and schizophrenic. Child De-velopment, 55:236-248, 1984.
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/21/4/677/1883961 by guest on 21 D
ecember 2021

690 SCHIZOPHRENIA BULLETIN
Watkins, ].; Asarnow, R.; and Tan-guay, P. Symptom development inchildhood onset schizophrenia.Journal of Child Psychology andPsychiatry, 29(6):865-878/ 1987.
Wechsler, D. Wechsler IntelligenceScale for Children-Revised. NewYork, NY: Psychological Corpora-tion, 1974.
Weintraub, S. Risk factors in schiz-ophrenia: The Stony Brook High-Risk Project. Schizophrenia Bulletin,13(3):439^150, 1987.
Weiss, K.M.; Vrtunski, P.B.; andSimpson, D.M Information over-load disrupts digit recall perform-ance in schizophrenics. Schizophre-nia Research, l(4):299-303, 1988.
Wiig, E., and Secord, W. Test ofLanguage Competence-Expanded Edi-tion (TLC-E). San Antonio, TX:Psychological Corporation, 1988.
Wiig, E., and Semel, E. LanguageAssessment and Intervention for theLearning Disabled. (2nd ed.) Co-lumbus, OH: Charles E. MerrillPublishing Company, 1984.
Wilcox, ]., and Nasrallah, H.Childhood head trauma and psy-chosis. Psychiatry Research, 21:303-306, 1987.
Williamson, P.C.; Kutcher, S.P.;Cooper, P.W.; Snow, W.G.; Szalai,J.P.; Kaye, H.; Morrison, S.L.;Willinshky, R.A.; and Mamelak, M.Psychological, topographic EEG,
and CT scan correlates of frontallobe function in schizophrenia.Psychiatry Research, 29(2):137-149,1989.
Wood, F.B., and Flowers, D.L. Hy-pofrontal vs. hypo-Sylvian bloodflow in schizophrenia. SchizophreniaBulletin, 16(3):413-124, 1990.
The Authors
Christiane A.M. Baltaxe, Ph.D., isAdjunct Professor of Psychiatryand Biobehavioral Sciences, andJames Q. Simmons III, M.D., isProfessor of Clinical Psychiatry,University of California, Los An-geles, CA.
Appendix:Definitions andOperationalDefinitions ofSpeech/LanguageTerms
A. Language Terms
Language. Language is a conven-tional system of arbitrary symbolsused as a code for representingand communicating messages. Itinvolves two major functions: re-ception (i.e., understanding, com-prehension, or receptive language)and expression (i.e., communicat-ing, expressing, or expressive lan-guage). Specific areas of languageinclude vocabulary, syntax, andabstract language. In the presentstudy, language disorder was oper-ationally defined as (1) scores inthe deficit range in both vocabu-lary and syntax and/or (2) scoresin the deficit range for abstractlanguage, expressive language, orreceptive language.
Abstract language. Abstract lan-guage is a receptive/expressivelinguistic function involving theabilities to discern implied infor-mation or information requiring in-
ferences and logical conclusions; toobserve unspoken cause and effectrelationships; to use and under-stand proverbs, metaphors, idioms,and complex analogies; to resolvelinguistic ambiguities; to form as-sociations between words; and todiscriminate between fact and fic-tion and fact and opinion (Wiigand Semel 1984).
A deficit in abstract languagewas defined operationally in thepresent study as scores in the def-icit range on the following threesubtests of the Test of LanguageCompetence (Wiig and Secord1988): the making inferences sub-test, the sentence ambiguities sub-test, and the figurative languagesubtest.
Auditory processing. Auditoryprocessing refers to the capacityfor processing language that isheard (i.e., through the auditorychannel). The psycholinguisticprocesses involved in auditory
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/21/4/677/1883961 by guest on 21 D
ecember 2021

VOL. 21, NO. 4, 1995 691
processing are not understood, andthere is some controversy aboutwhether they are purely linguisticprocesses or larger cognitive proc-esses (Barch and Berenbaum 1994).Various component skills havebeen hypothesized, including selec-tive attention, auditory attention,discrimination of speech versusbackground noise, discriminationof individual speech sounds, mem-ory for auditory information, se-quencing of auditory information,and cognitive information process-ing (Wiig and Semel 1984). In thepresent work, an auditory process-ing deficit was operationally de-fined by scores in the deficit rangeon the following tests and sub-tests: (1) the word sequences sub-test and the sentence imitationsubtest of the Detroit Tests ofLearning Aptitude-Revised (DTLA-R; Hammill 1985) and (2) theword memory subtest, the auditorynumber memory subtest, and thesentence memory subtest of thesubtests of the Test of AuditoryPerceptual Skill-Revised (TAPS-R;Gardner 1985).
Pragmatics. Pragmatics relates tothe rules for using language in asocial context. Pragmatic behaviorsor the interactive use of languagewere assessed in the present studyusing a protocol (Baltaxe and Sim-mons 1987) adapted from Pruttingand Kirchner (1987). The followingareas of functioning and specificproblems were rated: (1) Generaldiscourse features, that is, failingto orient the listener by establish-ing relevant background informa-tion, ignoring relevant backgroundinformation, having difficulties re-lating coherent narratives, havingdifficulties sequencing events intime, having difficulties using con-cepts of time, and perseverating;
(2) difficulties relating to topic,that is, having difficulties establish-ing topics, maintaining topics, in-appropriately switching topics,failing to differentiate between oldand new information, using pro-nouns when introducing informa-tion for the first time, overusingnoun phrases when old informa-tion is offered, failing to identifyantecedent referents, inappropri-ately omitting information; inap-propriately switching from singularto plural or plural to singular, in-appropriately referring to situa-tions, inappropriately switchingbetween situations; (3) difficultiesrelating to turn taking, that is, notinitiating speech, paucity of re-sponses, interrupting, not repairingor revising turn-taking errors, re-fusal to allow other party to havea turn speaking, manipulating con-versation through use of rhetoricalexpressions; and (4) stylistic varia-tions, that is, the use of tone ofvoice or word choices inappropri-ate to the dialect or social groupinvolved in the communication.
Syntax. Syntax refers to thegrammatical subsystem of lan-guage, including the grammaticalcategories, and to the grammaticalrelations and rules required toform sentences and phrases. Adeficit in syntax was operationallydefined in the present study by(1) scores in the deficit range onthe oral directions subtest,the word classes subtest, thesemantic relations subtests of theClinical Evaluation of LanguageFundamentals-Revised (CELF-R;Semel et al. 1987), and on the Testfor Auditory Comprehension ofLanguage-Revised (Carrow-Woolfolk 1985) (assessing receptivesyntax); and /or (2) scores in thedeficit range on the formulated
sentences subtest, the sentence as-sembly subtest, and the recallingsentences subtests of the CELF-R(assessing expressive syntax); and(3) results of an analysis of aspontaneous language sampleusing published norms for gram-matical structures.
Vocabulary. Vocabulary consistsof the discrete units of languagethat represent concepts, ideas, andmeaningful relations. In the pres-ent study, vocabulary deficits wereoperationally defined by scores inthe deficit range on (1) the Pea-body Picture Vocabulary Test-Revised (Dunn and Dunn 1981)(assessing receptive vocabulary)and (2) the Expressive One WordPicture Vocabulary Test (Gardner1983) (assessing expressivevocabulary).
B. Speech Terms
Speech. Speech refers to the mo-tor act of expressing language andincludes articulation, fluency, pros-ody, and voice. In the presentstudy a disorder in any of theseareas was considered a "speechdisorder" and aspects of speechwere evaluated based on spon-taneous language samples and theclinical impressions of a speechpathologist.
Articulation. Articulation is themotor act of producing speechsounds in sequence and in variouscombinations to form words, sen-tences, and phrases. In addition toratings by a speech pathologist, ar-ticulation was assessed in the pres-ent study by using the Goldman-Fristoe Test of Articulation (Gold-man and Fristoe 1986).
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/21/4/677/1883961 by guest on 21 D
ecember 2021

692 SCHIZOPHRENIA BULLETIN
Fluency. Fluency includes paus-ing, hesitations, false starts, andrepetitions of sounds, syllables,words, and phrases as well asshifts in the speed of flow ofspeech.
Prosody. Prosody refers to the
melody of speech, including pat-terns of stress (loudness) andtones (intonation). Prosody is usedto communicate affective informa-tion such as sadness, happiness,anger, surprise, disapproval, doubt,irony, and other emotional shad-ings of a communication. Prosody
acts as a linguistic indicator of dif-ferent sentence types.
Voice. Voice refers to the mecha-nism by which speech sounds areproduced. It includes phonation,articulation-resonance, respiration,pitch, and loudness.
An Invitationto Readers
Providing a forum for a lively ex-change of ideas ranks high amongthe Schizophrenia Bulletin's objec-tives. In the section At Issue,readers are asked to comment onspecific controversial subjects thatmerit wide discussion. But remarksneed not be confined to the issueswe have identified. At Issue isopen to any schizophrenia-relatedtopic that needs airing. It is aplace for readers to discuss articlesthat appear in the Bulletin or else-where in the professional litera-ture, to report informally on
experiences in the clinic, labora-tory, or commmunity, and to shareideas—including those that mightseem to be radical notions. We wel-come all comments.—The Editors.
Send your remarks to:
At IssueResearch Projects and
Publications BranchNational Institute of Mental
Health5600 Fishers Lane, Rm. 18C-06Rockville, MD 20857
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/21/4/677/1883961 by guest on 21 D
ecember 2021