Embed Size (px)
Citation preview

1
SOUTH DAKOTA AND IOWA SUMMARY OF PHARMACY BENEFITS
DEFINITIONS Brand Name Drug A drug manufactured and marketed under a trademark or name by a specific drug manufacturer. Certification Process The process of obtaining certification for coverage of certain prescription drug products prior to their being dispensed, using guidelines approved by the Health Plan. Refer to the section on Drugs that Require Prospective (pre‐service) Review and Certification in this booklet. Clinic/Office/Hospital Outpatient Administered Injectables Injectable medications that may be given in a variety of settings but must be given by a healthcare professional. These drugs are considered to be a medical benefit with coverage at the deductible and coinsurance level. Copay (also known as Copayment) The specified charge (flat dollar amount or percentage) that the member is required to pay for a Prescription Drug Product. Covered Drugs The following types of drugs are covered unless subject to an exception listed below under “Excluded Drugs and Supplies:”
1. Federal Legend Drugs: any medicinal substance which bears the legend, “Caution: Federal Law prohibits dispensing without a prescription,” except for those medicinal substances classified as exempt narcotics pursuant to state law;
2. An injectable drug can be prescribed to either be self‐administered or administered by a healthcare professional. Covered injectable drugs include insulin. Refer to the Injectable Drug Listing in this book for additional covered drugs.
3. State Restricted Drugs: any medicinal substance which may only be dispensed with a prescription according to state law;
4. Compound Medications: any medicinal substance which must be mixed, compounded, or otherwise prepared by a registered pharmacist and has at least one ingredient that is a federal legend or state restricted drug in a therapeutic amount;
5. Diabetic Treatment: Items listed below are available in a 90 day supply. Each 30 day supply generates a generic copay (90 day supply equals 3 copays)
• needles • injectable insulin • syringes • lancets • test strips ‐ maximum amount of 205 strips per month with a healthcare practitioner order
6. Contraceptive devices: including but not limited to oral medications, IUDs, implantable and injectable birth control devices. This coverage rule is defined by the benefit package purchased by the Employer group and by State Insurance Regulations for coverage.
Drug Exclusion Sanford Health Plan reserves the right to maintain a drug listing in which medications are specifically not available for coverage under benefit packages per Plan policy. Payment for this list of drugs will be the member’s responsibility in full.

2
Members may request a review of an adverse determination based on issues of medical necessity as it relates to non‐covered medications, generic substitution, therapeutic interchanges and step‐therapy protocols. Refer to Drug Exclusion List and Grievance Procedure in this book. Drug Formulary A list which identifies those Prescription Drug Products which are preferred by the Plan for dispensing to members when appropriate. This list is subject to periodic review and modifications. Formulary Brand‐Name Drug A prescription drug that is available only as a name brand medication, is preferred by the Sanford Health Plan and is listed in the Drug Formulary. A formulary brand name drug is typically available at the 2nd tier copay in a 3‐ Tier or 4‐ Tier Formulary. Generic Drug Drugs that (1) are approved by the Food and Drug Administration (FDA) as a therapeutic equivalent to the Brand Name Drug, (2) contain the same active ingredient as the Brand Name Drug, and (3) cost less then the Brand Name equivalent. Maintenance Drug List A list of drug products, typically used for chronic conditions, approved by the Sanford Health Plan or Employer, allowed to be dispensed in 90 day quantities. Medical Benefit Refers to drugs which are covered at the deductible/coinsurance level instead of with a copay. Member An individual eligible for benefits under the Plan as determined by the Plan or Employer. Non‐Participating Pharmacy A pharmacy that does not have a contract with Express Scripts Inc., on behalf of Sanford Health Plan. If a Sanford Health Plan Member utilizes a Non‐Participating Pharmacy, except in an emergency, the member is responsible for the full cost of the prescription drug. Non‐Formulary Brand‐Name Drug Brand‐Name drug not on Sanford Health Plan’s Formulary. Requests for coverage of Non‐Formulary Brand‐Name Drugs will not be considered unless the Member has tried and failed a Formulary alternative. These drugs are provided at a higher cost share to the member. This is the 3rd or 4th Tier Copay in a 3‐Tier or 4‐ Tier Formulary. Oral Contraceptives Oral contraceptives are considered an optional or mandated benefit based on your employer group location due to state mandated benefits.
• South Dakota Members: Oral contraceptives are an optional benefit for your employer group to purchase on your behalf.
• Iowa Members: Oral contraceptives, diaphragms, IUDs, Implanon and injectable drugs for contraception are a mandated state benefit.
Over‐the‐Counter (OTC) Drug A drug product that does not require a prescription order under federal or state law. Sanford Health Plan does not cover any medications that can be obtained Over‐the‐Counter. Participating Pharmacy A pharmacy that has contracted with Express Scripts Inc., on behalf of Sanford Health Plan to deliver prescription drug services to members. The Participating Pharmacy may be a hospital, pharmacy or other facility that has contractually

3
accepted the terms and conditions set forth by the Health Plan. Refer to the Sanford Health Plan Participating Pharmacy Listing or Express Scripts website found on www.sanfordhealthplan.com. If a Sanford Health Plan Member does not utilize their prescription card, except in an emergency, the member is responsible for the full cost of the prescription drug. Pill‐Splitting Program Some medications come in different strengths that are all similarly priced. The Pill Splitting Program allows members to split the higher‐strength tablets in half, doubling their supply and saving money on copays. This allows the member to make only one trip to the pharmacy every other month. The pill splitting program is available at retail pharmacies only. The drugs eligible for this program are indicated with a (1/2 tab) designation on the Drug Formulary. Prescription Drug Product A medication, product or device approved by the Food and Drug Administration (FDA) and dispensed under federal or state law only, pursuant to a prescription order or refill. Reasonable Costs Costs that do not exceed the lesser of: (a) negotiated schedule of payment developed by the Plan which are accepted as payment in full by Participating Practitioner and/or Providers within the Plan’s Service Area or (b) the prevailing marketplace charges. Self‐Injectable Are self‐administered drugs that can be given at home by the patient or caregiver. Typically these drugs are covered under the pharmacy benefit. Specialty Drugs A prescription drug that is available as a name brand, is preferred by Sanford Health Plan, is typically used to treat a chronic condition, and is more costly than traditional treatment. Step Therapy Program Program using protocols that specify the order in which different drugs for a given condition are prescribed. If a member does not obtain the desired clinical effect or experiences side effects at one step, then the drug choice at another step may be tried. Step therapy requires the use of first‐line alternatives before more expensive second‐line drugs are covered by the pharmacy benefit. Supply • Drugs are routinely supplied in 30 day quantities at one time, for one copay, unless otherwise approved by the Plan.
In some instances, if more than a typical 30 day supply is dispensed an additional copay will be charged. Examples include: All brand name Proton Pump Inhibitors and Cymbalta.
• Maintenance drugs may be dispensed in a 90‐day supply, but a copayment applies to each 30‐day supply received.
SANFORD HEALTH PLAN FORMULARY It is agreed that this prescription drug rider is attached to and made a part of the contract between Sanford Health Plan and the group. However, nothing in this rider will alter or affect any of the terms of the contract, unless specifically stated. To be covered by the plan, drugs must be:
1. Prescribed by a physician, physician assistant, nurse practitioner, dentist, or optometrist (eye medications only);
2. Listed in the Plan Formulary, unless certification is given by the Plan; 3. Provided by a Participating Pharmacy except in the event of a medical emergency. If the prescription is
obtained at a Non‐Participating Pharmacy the member is responsible for the prescription drug cost in full. 4. Approved by the Federal Food and Drug Administration (FDA) for use in the United States.

4
This information about the Sanford Health Plan Formulary applies only to those drugs, including injectable drugs that may be covered under this Policy. The Sanford Health Plan Formulary is a list of medications that are the most effective for the treatment and diagnosis of disease and maintenance of health according to the clinical judgment of the physicians, pharmacists and other health care professionals who helped us develop the Formulary. For a complete listing of the formulary, pharmacy locator, health news, generic substitution information, drug side effect and interaction information, personal reminders, price check, benefit information and your current medication usage, please utilize www.sanfordhealthplan.com then link to the electronic formulary via the Express Scripts web link. Following the Sanford Health Plan Formulary, especially asking your healthcare practitioner for generic medications, will save you money and help control the costs of health care. If you request that you receive the brand‐name drug when there is an equivalent generic alternative available, you will be required to pay the price difference between the brand and the generic in addition to your copay. When your practitioner prescribes a drug for you, you can ask that he or she refer to the Sanford Health Plan Formulary for prescription options. All participating practitioners have received a copy of the Sanford Health Plan Formulary on your behalf. Sanford Health Plan has options of Open, Closed, 2‐Tier, 3‐Tier, and 4‐Tier formulary programs for your employer’s choice to best meet the needs of the company. Please refer to your Group Summary of Plan Benefits for the Formulary Benefit purchased. Open Formulary An Open Formulary is a list of medications that are recommended by Express Scripts Inc., on behalf of Sanford Health Plan. This list is used only to encourage practitioners to prescribe appropriate medications. All drugs are covered as defined by the benefit package. Closed Formulary A Closed Formulary is a list of certain medications that are covered and others that are not covered at all by Sanford Health Plan. If a prescription is written for a medication that is not on the formulary list, the member is responsible in full for the cost of the medication. If a member or their Practitioner feels that a certain drug is medically necessary for their condition an Exception to the Formulary process is available. Refer to the Exception to the Formulary Process in your Policy. Please note that Participating Practitioners have been given instructions on how to obtain exceptions to the formulary. If you receive an adverse determination for your request for a formulary exception, you may request a review of that decision through our Grievance (Appeal) Procedure (see next section or refer to your Policy for the Problem Resolution (Appeal Procedure)). 4‐Tier Formulary A 4‐Tier drug program uses a copayment structure that reduces your out‐of‐pocket costs when using Generic Drugs and Formulary Brand Name Drugs. When a prescription is filled, your copayment will be at least one of these tiers: Tier 1: Generic Drugs Tier 2: Formulary Brand Name Drugs Tier 3: Non‐Formulary Brand Name Drugs Tier 4: Specialty Name Brand Drugs 3‐Tier Formulary A 3‐Tier drug program uses a copayment structure that reduces your out‐of‐pocket costs when using Generic Drugs and Formulary Brand Name Drugs. When a prescription is filled, your copayment will be at least one of these tiers:
Tier 1: Generic Drugs Tier 2: Formulary Brand Name Drugs Tier 3: Non‐Formulary Brand Name Drugs

5
2‐Tier Formulary A 2‐Tier drug program uses a copayment structure that reduces your out‐of‐pocket costs when using Generic Drugs and Formulary Brand Name Drugs. When a prescription is filled, your copayment will be at one of these tiers: Tier 1: Generic Drugs Tier 2: All covered Brand Name Drugs *The higher the tier, the higher the copay
GRIEVANCE (APPEAL) PROCEDURE If you receive an adverse determination to your request for an exception to the formulary, please follow the grievance procedure and the external review rights in your Policy. This applies to requests for coverage of non‐covered medications, generic substitutions, therapeutic interchanges and step‐therapy protocols. South Dakota Members The Grievance Procedure for Adverse Determinations is followed when there has been a medical necessity adverse determination based on formulary design. Four types of grievance procedures are available to members and Practitioners and/or Providers to address concerns regarding adverse determinations based on a request for a pharmacy service, certification, or formulary exception: 1) 1st Level Grievances for Prospective (Pre‐service) or Retrospective (Post‐service) Reviews; 2) Expedited Grievance for Urgent Care Reviews; 3) Additional Voluntary (2nd Level) Reviews; and 4) Independent, External Review. A prospective (pre‐service) grievance is a request to change an Adverse Determination that the Plan must approve in whole or in part in advance of the Member obtaining care or services. A retrospective (post‐service) grievance is a request to change an Adverse Determination for care or services already received by the Member. An expedited grievance process is used when the condition is of an emergency or urgent nature. The decision to cover your request for an exception will be made by a pharmacist or a practitioner of the appropriate specialty given the member’s health condition. Iowa Members The Appeal Procedure for Medical Review Determination is followed when there has been a medical necessity denial based on formulary design. Two types of initial appeals are available to members and Practitioner and/or Providers to address concerns regarding medical determination and certification decisions based on a request for service or certification: an expedited appeal process and a standard appeal process. An expedited appeal process is used when the condition is of an emergency or urgent nature. The decision to cover your request for an exception will be made by a pharmacist or a practitioner of the appropriate specialty given the member’s health condition.
SANFORD HEALTH PLAN PHARMACY PROGRAM Please review the following information concerning the drug exclusion list, certification, quantity limits, step therapy and injectable medication programs. Additional drugs may be added throughout the year to any listing. Sanford Health Plan will notify you of any changes. If you have any questions or concerns, contact our Utilization Management Department at 1‐800‐805‐7938. Please note that you may always request a formulary exception or prior certification by the Plan for excluded drugs. Drugs that Require Prospective (Pre‐service) Review and Certification To be considered for coverage by Sanford Health Plan, the following medications require a written certification of medical necessity for a formulary exception. Fax the written certification of Medical Necessity to Utilization Management at (605) 328‐6813. Oral contraceptives are not covered by all benefit packages but may be authorized for a medical condition.

6
Medications • Byetta • Generic Terbinafine (Lamisil) and Generic Itraconazole (Sporanox) for fungal disease. A positive culture or
KOH preparation is required for certification to receive coverage for one of these products. • Lexapro; Available only with prior authorization, which will not be granted unless a 90 day trial of citalopram
40mg daily has been completed. Coverage is at third tier when drug approved. • Lovaza; Triglyceride level must greater than 500 • Testosterone Products (Androgen, Androgel, Testoderm, Testosterone Injectable) • Symlin • Zyvox
INJECTABLE DRUG PROGRAM Sanford Health Plan uses CuraScript for your injectable medication needs. CuraScript will ship your drug and all the supplies you need for your injection directly to your home or healthcare practitioner’s office within 24 to 48 hours after the request is approved and medication is ordered. Also, your administration supplies (syringes, needles etc.) are free; you do not pay additional co‐pays for them. Prior to all shipments, a Specialty Care staff member will contact you to discuss your co‐pay for your drug and arrange delivery. CuraScript offers toll‐free customer service available 24 hours a day, 365 days a year. Specially trained staff offers support services for you, your caregivers, and your practitioners that include:
• Injectable drug order information; • Consultation with an experienced, knowledgeable pharmacist; • Specially trained nurses available to answer questions about injectable drugs and disease states they treat.
To enroll in the CuraScript program, call toll‐free at 1‐888‐773‐7376 and a customer service representative will ask the following information:
• Your name and date of birth • Your phone number and address • The name of your injectable medication to be filled • Your doctor’s name and phone number
CuraScript will mail your practitioner a letter explaining the new program and how to send your prescriptions to CuraScript. By participating in Specialty Care, you are automatically enrolled in a drug therapy management program. This program entitles you to receive the following benefits at no additional charge:
• Access to nurses and pharmacists 24 hours/day, 7 days/week for questions related to your injectable drug and the illness the drug is treating.
• Injectable drug refills reminders if you forget to call for your refill, and convenient refill process. • Free delivery of your medication and supplies to your home, practitioner’s office or designated location.
Injectable and High Cost Medications • The following medications (injectable and high cost medications) must be obtained from CuraScript by calling
(888) 773‐7376. If these medications are obtained from a retail pharmacy or healthcare practitioner office without certification by Sanford Health Plan Utilization Management Department the member will be responsible for the full cost of the medication. All medications obtained from CuraScript are prior authorized by CuraScript using criteria approved by the Sanford Health Plan. Most of these medications are covered under the medical benefit and are subject to payment with deductible, coinsurance or a medical copay, dependent upon your benefit package.
NAME DISEASE STATE COVERAGE PREFERRED ALTERNATIVES
8‐MOP MISCELLANEOUS SPECIALTY CONDITIONS MEDICAL ABRAXANE CANCER MEDICAL ACTHAR H.P. MULTIPLE SCLEROSIS MEDICAL ACTIMMUNE IMMUNE DEFICIENCY MEDICAL

7
NAME DISEASE STATE COVERAGE PREFERRED ALTERNATIVES
ADAGEN ENZYME DEFICIENCIES MEDICAL ‐ LIMITED DISTRIBUTION
ADRIAMYCIN CANCER MEDICAL ADRUCIL CANCER MEDICAL ADVATE HEMOPHILIA MEDICAL ALDURAZYME ENZYME DEFICIENCIES MEDICAL ALFERON N CANCER MEDICAL ALIMTA CANCER MEDICAL ALKERAN CANCER MEDICAL ALPHANATE HEMOPHILIA MEDICAL ALPHANINE SD HEMOPHILIA MEDICAL AMEVIVE INFLAMMATORY CONDITIONS MEDICAL ANTAGON INFERTILITY PHARMACY 100% COPAY
APOKYN MISCELLANEOUS SPECIALTY CONDITIONS MEDICAL ‐ LIMITED DISTRIBUTION
ARALAST RESPIRATORY CONDITIONS MEDICAL ‐ LIMITED DISTRIBUTION
ARANESP BLOOD CELL DEFICIENCY PHARMACY ‐ TIER 3 EPOGEN, PROCRIT ‐ TIER 2
AREDIA CANCER MEDICAL
ARIXTRA ANTICOAGULANT PHARMACY ‐ AVAIL THRU RETAIL ‐ TIER 3
FRAGMIN, INNOHEP, LOVENOX ‐ TIER 2
ARRANON CANCER MEDICAL ‐ LIMITED DISTRIBUTION
ATGAM TRANSPLANT MEDICAL AUTOPLEX T HEMOPHILIA MEDICAL AVASTIN CANCER MEDICAL AVONEX MULTIPLE SCLEROSIS PHARMACY ‐ TIER 2 BAYGAM IMMUNE DEFICIENCY MEDICAL BAYHEP B HEPATITIS B PHARMACY ‐ TIER 3 NABI‐HB ‐ TIER 2 BAYRHO‐D IMMUNE DEFICIENCY MEDICAL BEBULIN VH IMMUNO HEMOPHILIA MEDICAL BENEFIX HEMOPHILIA MEDICAL
BETASERON MULTIPLE SCLEROSIS PHARMACY ‐ NOT COVERED WITHOUT MED REVIEW
AVONEX OR REBIF ‐ TIER 2
BEXXAR CANCER MEDICAL ‐ LIMITED DISTRIBUTION
BICNU CANCER MEDICAL BLENOXANE CANCER MEDICAL BLEOMYCIN SULFATE CANCER MEDICAL BONIVA (INJECTABLE) OSTEOPOROSIS MEDICAL BOTOX MISCELLANEOUS SPECIALTY CONDITIONS MEDICAL BRAVELLE INFERTILITY PHARMACY 100% COPAY BUSULFEX CANCER MEDICAL CAMPATH CANCER MEDICAL CAMPTOSAR CANCER MEDICAL CARBOPLATIN CANCER MEDICAL
CARIMUNE IMMUNE DEFICIENCY MEDICAL ‐ LIMITED DISTRIBUTION

8
NAME DISEASE STATE COVERAGE PREFERRED ALTERNATIVES
CELLCEPT INJ TRANSPLANT MEDICAL
CEREDASE ENZYME DEFICIENCIES MEDICAL ‐ LIMITED DISTRIBUTION
CEREZYME ENZYME DEFICIENCIES MEDICAL CERUBIDINE CANCER MEDICAL CETROTIDE INFERTILITY PHARMACY 100% COPAY CHOREX‐10 INFERTILITY PHARMACY 100% COPAY CHORIONIC GONADOTROPIN INFERTILITY PHARMACY 100% COPAY
CISPLATIN CANCER MEDICAL CLADRIBINE CANCER MEDICAL
COPAXONE MULTIPLE SCLEROSIS PHARMACY ‐ TIER 3 AVONEX, REBIF ‐ TIER 2
COPEGUS HEPATITIS C PHARMACY ‐ TIER 2 COSMEGEN CANCER MEDICAL CYCLOPHOSPHAMIDE CANCER MEDICAL CYCLOSPORINE INJ TRANSPLANT MEDICAL CYTARABINE CANCER MEDICAL CYTOGAM IMMUNE DEFICIENCY MEDICAL CYTOXAN CANCER MEDICAL DACARBAZINE CANCER MEDICAL DACOGEN CANCER MEDICAL DAUNORUBICIN HCL CANCER MEDICAL DAUNOXOME CANCER MEDICAL DDAVP ENDOCRINE DISORDERS MEDICAL DEFEROXAMINE MESYLATE IRON TOXICITY MEDICAL
DEPOCYT CANCER MEDICAL DESFERAL, MESYLATE IRON TOXICITY MEDICAL DESMOPRESSIN ACETATE ENDOCRINE DISORDERS MEDICAL
DEXRAZOXANE CANCER MEDICAL DIDRONEL OSTEOPOROSIS MEDICAL DOXIL CANCER MEDICAL DOXORUBICIN HCL CANCER MEDICAL DTIC‐DOME IV CANCER MEDICAL
ELAPRASE ENZYME DEFICIENCIES MEDICAL ‐ LIMITED DISTRIBUTION
ELIGARD CANCER MEDICAL ELITEK CANCER MEDICAL ELLENCE CANCER MEDICAL ELOXATIN CANCER MEDICAL ELSPAR CANCER MEDICAL ENBREL INFLAMMATORY CONDITIONS PHARMACY ‐ TIER 2 EPIRUBICIN CANCER MEDICAL EPOGEN BLOOD CELL DEFICIENCY PHARMACY ‐ TIER 2 ERBITUX CANCER MEDICAL ETHYOL CANCER MEDICAL ETOPOPHOS CANCER MEDICAL ETOPOSIDE CANCER MEDICAL EUFLEXXA OSTEOARTHRITIS MEDICAL

9
NAME DISEASE STATE COVERAGE PREFERRED ALTERNATIVES
EXJADE IRON TOXICITY MEDICAL ‐ LIMITED DISTRIBUTION
FABRAZYME ENZYME DEFICIENCIES MEDICAL FEIBA VH IMMUNO HEMOPHILIA MEDICAL FERTINEX INFERTILITY PHARMACY 100% COPAY FLEBOGAMMA IMMUNE DEFICIENCY MEDICAL
FLOLAN PULMONARY HYPERTENSION MEDICAL ‐ LIMITED DISTRIBUTION
FLOXURIDINE CANCER MEDICAL FLUDARA CANCER MEDICAL FLUDARABINE PHOSPHATE CANCER MEDICAL
FLUOROURACIL CANCER MEDICAL FOLLISTIM AQ INFERTILITY PHARMACY 100% COPAY FORTEO OSTEOPOROSIS PHARMACY ‐ TIER 2
FRAGMIN ANTICOAGULANT PHARMACY ‐ AVAIL THRU RETAIL ‐ TIER 2
FUDR CANCER MEDICAL FUZEON IMMUNE DEFICIENCY MEDICAL GAMASTAN S/D IMMUNE DEFICIENCY MEDICAL GAMIMUNE N IMMUNE DEFICIENCY MEDICAL GAMMAGARD IMMUNE DEFICIENCY MEDICAL GAMMAR‐P I.V. IMMUNE DEFICIENCY MEDICAL GAMUNEX IMMUNE DEFICIENCY MEDICAL GANIRELIX ACETATE INFERTILITY PHARMACY 100% COPAY GEMZAR CANCER MEDICAL
GENARC HEMOPHILIA MEDICAL ‐ LIMITED DISTRIBUTION
GENOTROPIN GROWTH DEFICIENCY MEDICAL GEREF, DIAGNOSTIC GROWTH DEFICIENCY MEDICAL GLEEVEC CANCER MEDICAL GONAL‐F INFERTILITY PHARMACY 100% COPAY HEALON OPHTHALMIC CONDITIONS MEDICAL HEALON GV OPHTHALMIC CONDITIONS MEDICAL HELIXATE FS HEMOPHILIA MEDICAL HEMOFIL M HEMOPHILIA MEDICAL HEPAGAM B HEPATITIS B PHARMACY ‐ TIER 3 NABI‐HB ‐ TIER 2 HERCEPTIN CANCER MEDICAL HUMATE‐P HEMOPHILIA MEDICAL HUMATROPE GROWTH DEFICIENCY MEDICAL HUMIRA INFLAMMATORY CONDITIONS PHARMACY ‐ TIER 2 ENBREL ‐ TIER 2 HYALGAN OSTEOARTHRITIS MEDICAL HYCAMTIN CANCER MEDICAL HYPERHEP S/D HEPATITIS B PHARMACY ‐ TIER 3 NABI‐HB ‐ TIER 2 HYPERRAB S/D IMMUNE DEFICIENCY MEDICAL HYPERRHO S/D IMMUNE DEFICIENCY MEDICAL IDAMYCIN PFS CANCER MEDICAL IDARUBICIN HCL CANCER MEDICAL IFEX CANCER MEDICAL IFEX/MESNEX CANCER MEDICAL

10
NAME DISEASE STATE COVERAGE PREFERRED ALTERNATIVES
IFOSFAMIDE CANCER MEDICAL IFOSFAMIDE/MESNA CANCER MEDICAL
IMMUNE GLOBULIN IMMUNE DEFICIENCY MEDICAL ‐ LIMITED DISTRIBUTION
IMOGAM RABIES‐HT IMMUNE DEFICIENCY MEDICAL INCRELEX GROWTH DEFICIENCY MEDICAL
INFERGEN HEPATITIS C PHARMACY ‐ TIER 3 INTRON A, ROFERON A‐TIER 2
INNOHEP ANTICOAGULANT PHARMACY ‐ AVAIL THRU RETAIL ‐ TIER 2
INTRON A CANCER PHARMACY ‐ TIER 2
IPLEX GROWTH DEFICIENCY MEDICAL ‐ LIMITED DISTRIBUTION
IRESSA CANCER MEDICAL IVEEGAM EN IMMUNE DEFICIENCY MEDICAL
KEPIVANCE CANCER MEDICAL ‐ LIMITED DISTRIBUTION
KINERET INFLAMMATORY CONDITIONS PHARMACY ‐ TIER 3 ENBREL ‐ TIER 2 KOATE‐DVI HEMOPHILIA MEDICAL KOGENATE FS HEMOPHILIA MEDICAL KUVAN PKU MEDICAL LETAIRIS PULMONLARY HYPERTENSION PHARMACY ‐ TIER 3 LEUCOVORIN CALCIUM CANCER MEDICAL LEUKINE BLOOD CELL DEFICIENCY MEDICAL LEUPROLIDE ACETATE CANCER MEDICAL LEUSTATIN CANCER MEDICAL
LOVENOX ANTICOAGULANT PHARMACY ‐ AVAIL THRU RETAIL ‐ TIER 2
LUPRON CANCER MEDICAL LUPRON DEPOT CANCER MEDICAL LUVERIS INFERTILITY PHARMACY 100% COPAY MENOPUR INFERTILITY PHARMACY 100% COPAY MESNA CANCER MEDICAL MESNEX CANCER MEDICAL METHOTREXATE CANCER PHARMACY ‐ TIER 1 MICRHOGAM IMMUNE DEFICIENCY MEDICAL
MICRHOGAM IMMUNE DEFICIENCY MEDICAL ‐ LIMITED DISTRIBUTION
MITOMYCIN CANCER MEDICAL MITOXANTRONE, HCL CANCER MEDICAL MONARC‐M HEMOPHILIA MEDICAL MONOCLATE‐P HEMOPHILIA MEDICAL MONONINE HEMOPHILIA MEDICAL MUSTARGEN CANCER MEDICAL MUTAMYCIN CANCER MEDICAL MYLOTARG CANCER MEDICAL MYOBLOC MISCELLANEOUS SPECIALTY CONDITIONS MEDICAL MYOZYME ENZYME DEFICIENCIES MEDICAL NABI‐HB HEPATITIS B PHARMACY ‐ TIER 2 NAGLAZYME ENZYME DEFICIENCIES MEDICAL NATRECOR MISCELLANEOUS SPECIALTY CONDITIONS MEDICAL

11
NAME DISEASE STATE COVERAGE PREFERRED ALTERNATIVES
NAVELBINE CANCER MEDICAL NEOSAR CANCER MEDICAL NEOSAR FOR INJECTION CANCER MEDICAL
NEULASTA BLOOD CELL DEFICIENCY PHARMACY ‐ TIER 3 NEUPOGEN – TIER 2
NEUMEGA BLOOD CELL DEFICIENCY MEDICAL NEUPOGEN BLOOD CELL DEFICIENCY PHARMACY ‐ TIER 2 NEXAVAR CANCER MEDICAL NIPENT CANCER MEDICAL NORDITROPIN GROWTH DEFICIENCY MEDICAL NOVANTRONE CANCER MEDICAL NOVAREL INFERTILITY PHARMACY 100% COPAY NOVOSEVEN HEMOPHILIA MEDICAL NUTROPIN, AQ, DEPOT GROWTH DEFICIENCY MEDICAL OCTAGAM IMMUNE DEFICIENCY MEDICAL OCTREOTIDE ACETATE ENDOCRINE DISORDERS MEDICAL OMNITROPE GROWTH DEFICIENCY MEDICAL ONCASPAR CANCER MEDICAL ONTAK CANCER MEDICAL ONXOL CANCER MEDICAL ORENCIA INFLAMMATORY CONDITIONS MEDICAL
ORFADIN ENZYME DEFICIENCIES MEDICAL ‐ LIMITED DISTRIBUTION
ORTHOCLONE OKT‐3 TRANSPLANT MEDICAL ORTHOVISC OSTEOARTHRITIS MEDICAL OTN PAMIDRONATE CANCER MEDICAL OVIDREL INFERTILITY PHARMACY 100% COPAY PACLITAXEL CANCER MEDICAL PAMIDRONATE DISODIUM CANCER
MEDICAL PANGLOBULIN NF IMMUNE DEFICIENCY MEDICAL PANRETIN MISCELLANEOUS SPECIALTY CONDITIONS MEDICAL PARAPLATIN CANCER MEDICAL PEGASYS HEPATITIS C PHARMACY ‐ TIER 2
PEG‐INTRON HEPATITIS C PHARMACY ‐ NOT COVERED WITHOUT MED REVIEW PEGASYS ‐ TIER 2
PHOTOFRIN CANCER MEDICAL PLENAXIS CANCER MEDICAL POLYGAM S/D IMMUNE DEFICIENCY MEDICAL PREGNYL INFERTILITY PHARMACY 100% COPAY PRIALT MISCELLANEOUS SPECIALTY CONDITIONS MEDICAL PROCRIT BLOOD CELL DEFICIENCY PHARMACY ‐ TIER 2 PROFASI INFERTILITY PHARMACY 100% COPAY PROFILNINE SD HEMOPHILIA MEDICAL PROGESTERONE IN OIL INFERTILITY PHARMACY 100% COPAY
PROGRAF TRANSPLANT MEDICAL ‐ LIMITED DISTRIBUTION
PROLASTIN RESPIRATORY CONDITIONS MEDICAL ‐ LIMITED DISTRIBUTION
PROLEUKIN CANCER MEDICAL

12
NAME DISEASE STATE COVERAGE PREFERRED ALTERNATIVES
PROPLEX T HEMOPHILIA MEDICAL PROTROPIN GROWTH DEFICIENCY MEDICAL PROVISC OPHTHALMIC CONDITIONS MEDICAL PULMOZYME RESPIRATORY CONDITIONS PHARMACY ‐ TIER 3 RAPTIVA INFLAMMATORY CONDITIONS PHARMACY ‐ TIER 2 REBETOL HEPATITIS C PHARMACY ‐ TIER 1 REBIF MULTIPLE SCLEROSIS PHARMACY ‐ TIER 2
RECLAST PAGETʹS DISEASE/ OSTEOPORSIS MEDICAL
ALENDRONATE‐ TIER 1, ACTONEL‐ TIER 2
RECOMBINATE HEMOPHILIA MEDICAL REFACTO HEMOPHILIA MEDICAL
REFLUDAN ANTICOAGULANT PHARMACY ‐ AVAIL THRU RETAIL
FRAGMIN, INNOHEP, LOVENOX ‐ TIER 2
REMICADE INFLAMMATORY CONDITIONS MEDICAL REMODULIN PULMONARY HYPERTENSION PHARMACY ‐ TIER 3 REPRONEX INFERTILITY PHARMACY 100% COPAY RETROVIR IV IMMUNE DEFICIENCY MEDICAL REVATIO PULMONARY HYPERTENSION PHARMACY ‐ TIER 3 REVLIMID CANCER MEDICAL RHOGAM IMMUNE DEFICIENCY MEDICAL RHOPHYLAC IMMUNE DEFICIENCY MEDICAL RIBAPAK HEPATITIS C PHARMACY ‐ TIER 1 RIBASPHERE HEPATITIS C PHARMACY ‐ TIER 1 RIBATAB HEPATITIS C PHARMACY ‐ TIER 1 RIBAVIRIN HEPATITIS C PHARMACY ‐ TIER 1 RILUTEK MISCELLANEOUS SPECIALTY CONDITIONS MEDICAL RITUXAN CANCER PHARMACY ‐ TIER 2 ROFERON‐A CANCER PHARMACY ‐ TIER 2 SAIZEN GROWTH DEFICIENCY MEDICAL SANDIMMUNE TRANSPLANT MEDICAL SANDOSTATIN, LAR ENDOCRINE DISORDERS MEDICAL SEROSTIM GROWTH DEFICIENCY MEDICAL SIMULECT TRANSPLANT MEDICAL SOLIRIS MISCELLANEOUS SPECIALTY CONDITIONS MEDICAL
SOMAVERT GROWTH DEFICIENCY MEDICAL ‐ LIMITED DISTRIBUTION
SPRYCEL CANCER MEDICAL SUPARTZ OSTEOARTHRITIS MEDICAL SUTENT CANCER MEDICAL SYNAGIS RSV PREVENTION MEDICAL SYNVISC OSTEOARTHRITIS MEDICAL TARABINE PFS CANCER MEDICAL TARCEVA CANCER MEDICAL TAXOL CANCER MEDICAL TAXOTERE CANCER MEDICAL TEMODAR CANCER MEDICAL TEV‐TROPIN GROWTH DEFICIENCY MEDICAL THALOMID CANCER MEDICAL

13
NAME DISEASE STATE COVERAGE PREFERRED ALTERNATIVES
THERACYS CANCER MEDICAL THIOTEPA CANCER MEDICAL
THYMOGLOBULIN TRANSPLANT MEDICAL ‐ LIMITED DISTRIBUTION
THYROGEN CANCER MEDICAL TOBI RESPIRATORY CONDITIONS PHARMACY ‐ TIER 3 TOPOSAR CANCER MEDICAL TORISEL CANCER MEDICAL TRACLEER PULMONARY HYPERTENSION PHARMACY ‐ TIER 3 TRELSTAR DEPOT CANCER MEDICAL TRELSTAR LA CANCER MEDICAL TRISENOX CANCER MEDICAL TYKERB CANCER MEDICAL TYSABRI MULTIPLE SCLEROSIS MEDICAL VANTAS CANCER MEDICAL VARICELLA‐ZOSTER IMM GLOBULIN IMMUNE DEFICIENCY
MEDICAL VECTIBIX CANCER MEDICAL VELCADE CANCER MEDICAL VENOGLOBULIN‐S IMMUNE DEFICIENCY MEDICAL
VENTAVIS PULMONARY HYPERTENSION MEDICAL ‐ LIMITED DISTRIBUTION
VIADUR CANCER MEDICAL VIDAZA CANCER MEDICAL VINBLASTINE SULFATE CANCER MEDICAL VINCRISTINE SULFATE CANCER MEDICAL VINORELBINE TARTRATE
CANCER MEDICAL
VITRAVENE OPHTHALMIC CONDITIONS MEDICAL VIVAGLOBIN IMMUNE DEFICIENCY MEDICAL VUMON CANCER MEDICAL WINRHO SDF IMMUNE DEFICIENCY MEDICAL XELODA CANCER MEDICAL XOLAIR RESPIRATORY CONDITIONS MEDICAL
XYREM MISCELLANEOUS SPECIALTY CONDITIONS MEDICAL ‐ LIMITED DISTRIBUTION
ZANOSAR CANCER MEDICAL ZANOSAR STERILE POWDER
CANCER MEDICAL
ZAVESCA ENZYME DEFICIENCIES MEDICAL
ZEMAIRA RESPIRATORY CONDITIONS MEDICAL ‐ LIMITED DISTRIBUTION
ZENAPAX TRANSPLANT MEDICAL ZEVALIN CANCER MEDICAL ZINECARD CANCER MEDICAL ZOLADEX CANCER MEDICAL ZOLINZA CANCER MEDICAL ZOMETA CANCER MEDICAL ZORBTIVE GROWTH DEFICIENCY MEDICAL

14
EXCLUDED DRUGS AND SUPPLIES The following medications are specifically EXCLUDED from coverage under the Plan unless mandated by state regulation or a formulary exception has been granted by the Plan or previous certification by the Plan was given: • Drugs not listed in the Sanford Health Plan Formulary; • Medications, equipment or supplies available over‐the‐counter (OTC) (except for insulin and select diabetic supplies,
e.g. syringes, , needles, test strips, and lancets) that by federal or state law do not require a prescription order and any medication that is equivalent to an OTC medication;
• Drugs and associated expenses and devices not approved by the FDA for a particular use except as required by law (unless the Practitioner certifies off‐label use with a letter of medical necessity).
• Birth control drugs and devices including but not limited to IUDs, implantable and injectable birth control devices (e.g. Implanon) except as may be covered by a supplemental prescription drug rider. This coverage rule is defined by the benefit package purchased by the Employer group and by State Insurance Regulations (NOTE: This exclusion does not apply to Iowa Members);
Medications that are used to treat infertility; • Weight management drugs except when medically necessary to treat morbid obesity and approved by the Plan(e.g.
Meridia, Xenical, tenuate, and phenteramine); • Replacement of a prescription drug due to loss, damage, or theft; • Outpatient Drugs dispensed in a Practitioner’s office or non‐retail pharmacy location; • Experimental or Investigational drugs; • Growth Hormone, except when medically indicated and approved by the Sanford Health Plan; • B‐12 Injections, except for pernicious anemia; • Immunological agents; • Acne Medication for Members over age thirty (30) such as Renova and Retin‐A Microgel; • Orthomolecular Therapy, including nutrients, vitamins (including but not limited to prenatal vitamins), multi‐
vitamins with iron and/or fluoride, food supplements and baby formula (except to treat PKU or otherwise required to sustain life), nutritional and electrolyte substances;
• Whole Blood and Blood Components Not Classified as Drugs in the United States Pharmacopoeia; • Smoking deterrent products such as Zyban and Chantix; • Drug Efficacy Study Implementation (“DESI”) drugs; • Drugs that may be received without charge under a federal, state, or local program; • Drugs for cosmetic purposes, including baldness, removal of facial hair, and pigmenting or antipigmenting of the
skin,(e.g. Propecia, and Vaniqa); • Refills of any prescription older than one year; and • Compound medications containing no legend (prescription) medication.
Drug Exclusion List The following drugs (and their generic equivalent, if listed) are excluded by the Health Plan policy, as there are similar drugs in this category available for coverage. Brand name products will not be covered when an A‐B rated generic is available. Excluded Drug Formulary Alternative Accolate Singulair Aciphex generic omeprazole, Prevacid, OTC
Prilosec Activella Prempro, Premphase, FemHRT Actonel generic alendronate Aerobid/‐M Flovent, Pulmicort Alamast Patanol Allegra/‐D OTC products (i.e. loratadine/‐D,
Zyrtec/‐D) Alocril Patanol Alomide Patanol
Excluded Drug Formulary Alternative Alora generics, Climara, Estraderm,
Vivelle Alrex Patanol Altoprev generic lovastatin Ambien, CR, PAK generic zolpidem (Ambien) Angelig Prempro/premphase, Fem HRT Ansaid (flurbiprofen)
generic ibuprofen, naproxen sodium
Anzemet generic ondansetron (Zofran) Antara generic gemfibrozil, fenofibrate,
Tricor
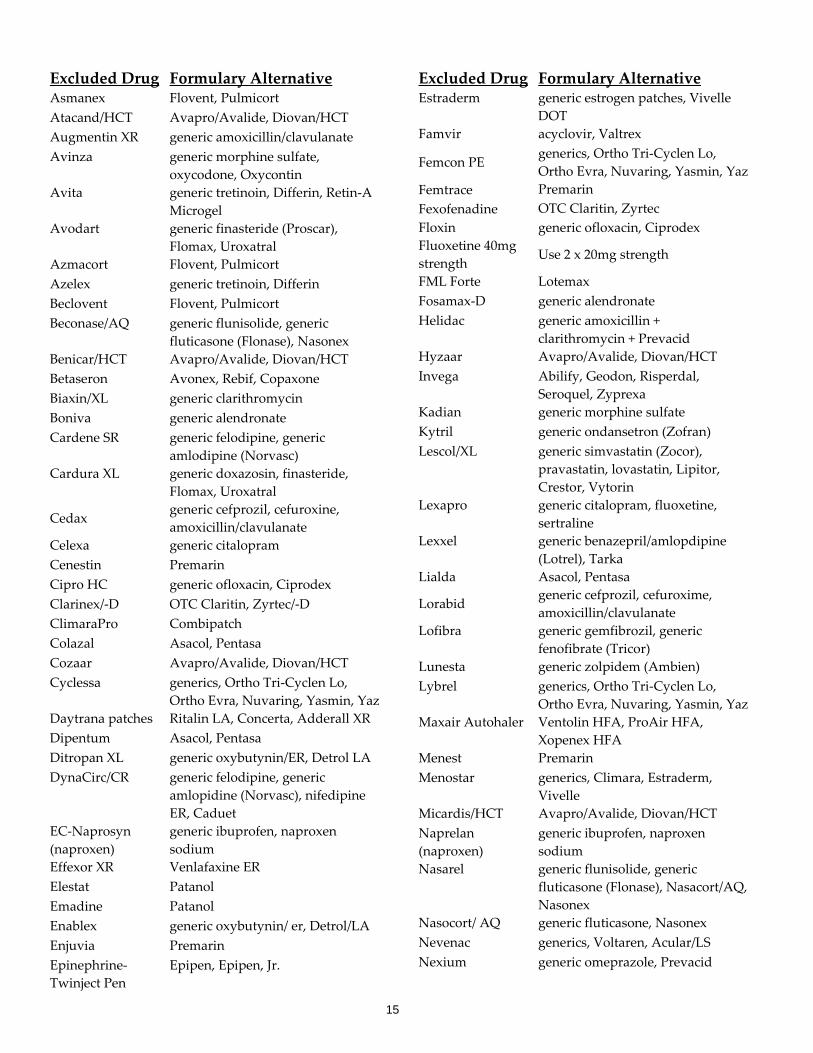
15
Excluded Drug Formulary Alternative Asmanex Flovent, Pulmicort Atacand/HCT Avapro/Avalide, Diovan/HCT Augmentin XR generic amoxicillin/clavulanate Avinza generic morphine sulfate,
oxycodone, Oxycontin Avita generic tretinoin, Differin, Retin‐A
Microgel Avodart generic finasteride (Proscar),
Flomax, Uroxatral Azmacort Flovent, Pulmicort Azelex generic tretinoin, Differin Beclovent Flovent, Pulmicort Beconase/AQ generic flunisolide, generic
fluticasone (Flonase), Nasonex Benicar/HCT Avapro/Avalide, Diovan/HCT Betaseron Avonex, Rebif, Copaxone Biaxin/XL generic clarithromycin Boniva generic alendronate Cardene SR generic felodipine, generic
amlodipine (Norvasc) Cardura XL generic doxazosin, finasteride,
Flomax, Uroxatral
Cedax generic cefprozil, cefuroxine, amoxicillin/clavulanate
Celexa generic citalopram Cenestin Premarin Cipro HC generic ofloxacin, Ciprodex Clarinex/‐D OTC Claritin, Zyrtec/‐D ClimaraPro Combipatch Colazal Asacol, Pentasa Cozaar Avapro/Avalide, Diovan/HCT Cyclessa generics, Ortho Tri‐Cyclen Lo,
Ortho Evra, Nuvaring, Yasmin, YazDaytrana patches Ritalin LA, Concerta, Adderall XR Dipentum Asacol, Pentasa Ditropan XL generic oxybutynin/ER, Detrol LA DynaCirc/CR generic felodipine, generic
amlopidine (Norvasc), nifedipine ER, Caduet
EC‐Naprosyn (naproxen)
generic ibuprofen, naproxen sodium
Effexor XR Venlafaxine ER Elestat Patanol Emadine Patanol Enablex generic oxybutynin/ er, Detrol/LA Enjuvia Premarin Epinephrine‐Twinject Pen
Epipen, Epipen, Jr.
Excluded Drug Formulary Alternative Estraderm generic estrogen patches, Vivelle
DOT Famvir acyclovir, Valtrex
Femcon PE generics, Ortho Tri‐Cyclen Lo, Ortho Evra, Nuvaring, Yasmin, Yaz
Femtrace Premarin Fexofenadine OTC Claritin, Zyrtec Floxin generic ofloxacin, Ciprodex Fluoxetine 40mg strength
Use 2 x 20mg strength
FML Forte Lotemax Fosamax‐D generic alendronate Helidac generic amoxicillin +
clarithromycin + Prevacid Hyzaar Avapro/Avalide, Diovan/HCT Invega Abilify, Geodon, Risperdal,
Seroquel, Zyprexa Kadian generic morphine sulfate Kytril generic ondansetron (Zofran) Lescol/XL generic simvastatin (Zocor),
pravastatin, lovastatin, Lipitor, Crestor, Vytorin
Lexapro generic citalopram, fluoxetine, sertraline
Lexxel generic benazepril/amlopdipine (Lotrel), Tarka
Lialda Asacol, Pentasa
Lorabid generic cefprozil, cefuroxime, amoxicillin/clavulanate
Lofibra generic gemfibrozil, generic fenofibrate (Tricor)
Lunesta generic zolpidem (Ambien) Lybrel generics, Ortho Tri‐Cyclen Lo,
Ortho Evra, Nuvaring, Yasmin, YazMaxair Autohaler Ventolin HFA, ProAir HFA,
Xopenex HFA Menest Premarin Menostar generics, Climara, Estraderm,
Vivelle Micardis/HCT Avapro/Avalide, Diovan/HCT Naprelan (naproxen)
generic ibuprofen, naproxen sodium
Nasarel generic flunisolide, generic fluticasone (Flonase), Nasacort/AQ, Nasonex
Nasocort/ AQ generic fluticasone, Nasonex Nevenac generics, Voltaren, Acular/LS Nexium generic omeprazole, Prevacid

16
Excluded Drug Formulary Alternative Opana, ER generic morphine sulfate,
oxycodone, Oxycontin Optivar Patanol Pataday Patanol Paxil CR generic paroxetine PCE generic erythromycin Peg Intron‐A Pegasys PrevPac generic clarithromycin +
amoxicillin + Prevacid Prefest Prempro, Premphase, FemHRT Prilosec generic omeprazole, Prevacid Pristiq generic bupropion, sertaline,
Effexor Protonix generic omeprazole, Prevacid Proventil HFA Ventolin HFA, Proair HFA,
Xopenex HFA Provigil Adderall, Concerta, Ritalin Prozac Weekly generic fluoxetine Quixin generics, Vigamox QVAR Flovent, Pulmicort Relenza Tamiflu Renova generic tretinoin, Retin‐A Microgel,
Differin Risperdal M Risperdal Rhinocort/AQ generic flunisolide, generic
fluticasone (Flonase), Nasonex Rozerem generic zolpidem (Ambien) Rynatan OTC Claritin‐D, Zyrtec‐D Sanctura generic oxybutynin/er, Detrol LA Sarafem generic fluoxetine
Excluded Drug Formulary Alternative
Seasonale generics, Ortho Tri‐Cyclen Lo, Ortho Evra, Nuvaring, Yasmin, Yaz
Sonata generic zolpidem (Ambien) Spectracef generic cefprozil, cefuroxime,
amoxicillin/clavulante
Sular generic felodipine, generic amlodipine (Norvasc)
Suprax generic cefprozil, cefuroxime, amoxicillin/clavulanate
Symbyax generic fluoxetine Testim Androgel, Androderm Teveten/HCT Avapro/Avalide, Diovan/HCT Travatan/Z Xalatan, Lumigan Triglide generic gemfibrozil, generic
fenofibrate (Tricor) Veramyst generic fluticasone (Flonase),
Nasonex Vexol Lotemax Vivelle Vivelle DOT Vytorin generic simvastatin (Zocor),
pravastatin, lovastatin, Lipitor, Crestor
Vyvanse generic methylphenidate, Adderall XR, Concerta, Ritalin LA
Xyzal OTC Zyrtec Zegerid generic omeprazole Ziana generic tretinoin, Differin, Retin‐A
Microgel Zymar generics, Vigamox Zyprexa Zydis Zyprexa
Quantity Limit List* The following drugs do not require certification but have a quantity limit: Amerge—9 tablets/prescription Anzemet—1 tablets/ prescription (not covered unless part of step therapy program) Axert—6 tablets/prescription butorphanol tartrate‐ nasal spray —2 spray bottles/ prescription Emend—3 pills/prescription (3rd tier copay) Frova—9 tablets/prescription Imitrex—9 tablets/ 6 nasal spray or 1 kit for injections/prescription or 2 injections Kytril—2 tablets/prescription (not covered unless medically necessary) Maxalt—6 tablets/prescription Maxalt MLT—9 tablets/prescription Migranal—4 ampules/spray/prescription Relpax—12 tablets/prescription Zomig—6 tablets for 2.5mg and 3 tablets for 5mg/ prescription Zomig—6 ampules/spray/prescription Zomig ZMT—6 tablets for 2.5 mg and 3 tablets for 5 mg/ prescription

17
*The Sanford Health Plan policy is a 30‐day prescription limit excluding maintenance medications. If you would like a complete listing or information about a specific drug please contact the Utilization Management Department at 1‐800‐805‐7938, or log onto the website: www.sanfordhealth.org. Special Quantity Limits The following drugs, when approved by authorization, are only available in quantities of 30 per prescription for one copay. Additional quantities will generate additional copays. Formulary Drugs: Cymbalta 60 mg daily limitation Prevacid Non‐Formulary Drugs Nexium Aciphex STEP THERAPY PROGRAM The step therapy program was developed to encourage the use of first‐line alternatives before more expensive second‐line medications. If a member does not obtain the desired clinical effect or experiences side effects at one step, then the drug choice at another step may be tried. If a step therapy rule is not met at the pharmacy, coverage will be determined by prospective (pre‐service) review. You can request prospective (pre‐service) review and/or certification by calling the Utilization Management Department at 1‐800‐805‐7938. The following step therapy programs are listed and their clinical criteria are as follows. Step Therapy
• Antidepressent Therapy (SSRI and SNRI) • Antiemetic (ondansetron hcl, Aloxi, Anzemet, Emend)—Applies only to Members receiving Chemotherapy. • Proton Pump Inhibitors (PPIs) omeprazole, Prevacid • Singulair • Zetia
Antidepressent (SSRI and SNRI) Step Therapy
1. One generic drug will be required before a brand name drug is authorized. Generic drugs will have to have been prescribed at an effective dose for a minimum of 30 days. Documentation of attempt and failure of a generic within the last 12 months will be considered as fulfilling this requirement. The daily effective doses are considered to be: • Fluoxetine 40 mg. • Paroxetine 20 mg. • Citalopram 40 mg. • Mirtazapine 30mg. • Bupropion sr 300mg. • Sertraline 150 mg. • Bupropion xl 150mg • Bupropion xl 300mg
2. Cymbalta will be covered (after a generic SSRI is tried a minimum of 30 days) at the 2nd tier copay level. 3. Venlafaxine ER 150 mg will be covered (after a generic drug is tried a minimum of 30 days) at the 2nd tier copay
level. • Any member using Venlafaxine ER 37.5mg or 75mg will pay 3rd tier for the medication after a 3 month
supply unless the total daily dose is 150mg or more.
Antiemetic Step Therapy (ondansetron hcl, Aloxi, Anzemet, Emend) This step therapy program only applies to Members receiving Chemotherapy.

18
1. ondansetron hcl is the preferred drug for Level 1 and Level 2 Chemotherapy agents. 2. ondansetron hcl will be the only covered outpatient oral agents that a Member can fill at a retail pharmacy
unless prior authorization is obtained with a letter of medical necessity from a healthcare practitioner. 3. Aloxi will not be covered for Level 1 and Level 2 Chemotherapy agents without prior authorization. 4. Aloxi will be covered for Chemotherapy agents in Levels 3, 4, and 5. Prior authorization is not required. 5. Anzemet will be covered for these agents if ondansetron hcl fails. 6. Emend will be covered for agents in Level 3, 4, and 5. Prior authorization is not required. Proton Pump Inhibitors (PPIs) omeprazole, Prevacid 1. A minimum of a 30 day trial of generic omeprazole is required; Prevacid will be covered thereafter with no
prior authorization required. Singulair Step Therapy 1. Certification for Singulair is approved for members with asthma, COPD, emphysema, chronic
bronchitis/bronchospasm, or acute respiratory syncytial virus (RSV) bronchiolitis. 2. For members with allergic rhinitis, Singulair is covered only after the member has tried and failed an
antihistamine and a nasal corticosteroid. 3. Members with chronic urticaria must have tried and failed one of the oral antihistamines such as OTC Zyrtec.
Zetia Step Therapy
1. The member must have tried and failed one of the following drugs (may be brand or generic) or combination of drugs at the following dosage:
2. The member has tried one of the drugs from the above list and cannot tolerate the side effects. 3. The member is taking or will be taking a medication that has drug interactions with a drug from the above
listing. 4. Children or adolescents <17 years of age must have tried a drug from the above list at the clinically
appropriate pediatric dose. 5. Members with severe renal impairment of creatinine clearance ≤30 mL/minute. 6. Homozygous familial hypercholesterolemia. 7. Homozygous familial sitosterolemia. 8. Pregnant women. 9. Active liver disease or unexplained persistent elevations of serum transaminases.
SVHP‐0351 1/09
Brand Name Daily Dose Advicor ≥2000 mg/40 mg Crestor ≥20mg Lescol ≥40 mg Lipitor ≥20 mg Lovastatin ≥40 mg Pravastatin ≥40 mg Simvastatin ≥40 mg

2009 SOUTH DAKOTA AND IOWA FORMULARY The following is a list of the most commonly prescribed drugs. It represents an abbreviated version of the drug formulary that is the core of your pharmacy benefit coverage. In addition to using this list, allowing substitution of generic products is encouraged when appropriate. If you are currently on a 3 or 4-tier pharmacy benefit program, the lowest co-payment is applied to all covered generic drugs. Generic drugs are indicated in bold. Tier 2 co-payment will apply to all of the covered brands listed on this formulary. Brand name drugs are listed in CAPITAL letters. This is NOT a complete listing of covered drugs. For a complete list of medications, you can go to www.sanfordhealthplan.com and then link to the electronic formulary via Express Scripts. Questions may be directed to a Sanford Health Plan representative at 1-800-805-7938. “PA Required” indicates that prior authorization is required on that specific medication. “Step therapy” indicates the medication requires the use of first-line alternatives before more expensive second-line drugs are covered by the pharmacy benefit. Drugs marked with an asterisk (*) must be obtained from CuraScript. Questions may be directed to a Sanford Health Plan Representative at 1-800-805-7938. If you are currently taking or are prescribed an injectable medication, please contact CuraScript Injectable Drug Program at 1-888-773-7376 to order your drugs. Refer to the 2009 Summary of Pharmacy Benefits for a complete listing of drugs and instructions. Questions regarding coverage can be directed to a Sanford Health Plan Representative at 1-800-805-7938.
TABLE OF CONTENTS Chapter Name Chapter 1 ANESTHETICS Chapter 2 ANTIINFECTIVES Chapter 3 ANTINEOPLASTIC/IMMUNOSUPPRESSANT DRUGS Chapter 4 CARDIOVASCULAR MEDICATIONS Chapter 5 AUTONOMIC & CNS MEDICATIONS Chapter 6 DERMATOLOGICAL MEDICATIONS Chapter 7 EAR-NOSE-THROAT MEDICATIONS Chapter 8 ENDOCRINE MEDICATIONS Chapter 9 GASTROINTESTINAL MEDICATIONS Chapter 10 IMMUNOLOGICALS & VACCINES Chapter 11 MUSCULOSKELETAL MEDICATIONS Chapter 12 NUTRITION, BLOOD Chapter 13 OBSTETRICAL & GYNECOLOGICAL MEDICATIONS Chapter 14 OPHTHALMIC MEDICATIONS Chapter 15 RESPIRATORY MEDICATIONS Chapter 16 UROLOGICAL MEDICATIONS Chapter 17 DIAGNOSTIC & MISCELLANEOUS MEDICATIONS – NOT APPLICABLE Chapter 18 MEDICAL (MISCELLANEOUS) SUPPLIES

SANFORD HEALTH PLAN 2009
TIER
DRUG NAME RESTRICTION 1 2 3
SUGGESTED PREFFERED
ALTERNATIVES
CHAPTER 1: ANESTHETICS
1.2 TOPICAL ANESTHETICS
lidocaine hcl, ‐viscous X
LIDODERM X
CHAPTER 2: ANTIINFECTIVES
2.1.1 CEPHALOSPORINS
cefaclor, er X
cefadroxil X
cefdinir X
cefpodoxime proxetil X
cefprozil X
cefuroxime X
cephalexin X
2.1.3 CLINDAMYCINS
clindamycin hcl X
clindamycin phosphate X
2.1.4 ERYTHROMYCINS
erythromycin ethylsuccinate X
erythromycin stearate X
2.1.4.1 OTHER MACROLIDES
azithromycin X
clarithromycin X
ZMAX X
2.1.4.2 KETOLIDES
KETEK, ‐PAK X
2.1.5 PENICILLINS amox tr‐potassium clavulanate X
amoxicillin X
ampicillin X
penicillin v potassium X
trimox X
2.1.6 SULFONAMIDES sulfamethoxazole‐ trimethoprim X
erythromycin w/sulfisoxazole X
GANTRISIN X
2.1.7 TETRACYCLINES
doxycycline hyclate X
doxycycline monohydrate X
minocycline hcl X
tetracycline hcl X
2.1.8 URINARY ANTIINFECTIVES nitrofurantoin, macrocrystal X
trimethoprim X
2.1.9 QUINOLONES
ciprofloxacin hcl X
AVELOX, ABC PACK X
LEVAQUIN X
2.2 TOPICAL ANTIBACTERIAL DRUGS
chlorhexidine gluconate X
gentamicin sulfate X
mupirocin 2% ointment X
silver sulfadiazine X
BACTROBAN X
2.3 ORAL ANTIFUNGAL DRUGS
clotrimazole troche X
fluconazole X
itraconazole PA, except derm X
ketoconazole X
nystatin X
terbinafine hcl PA, except derm X
SPORANOX SOLN PA, except derm X
2.4.1 VAGINAL ANTIFUNGALS
clotrimazole X
nystatin X
terconazole X
GYNAZOLE‐1 X
2.4.2 OTHER TOPICAL ANTIFUNGALS
ciclopirox X
clotrimazole X
econazole nitrate X
ketoconazole X
TIER
DRUG NAME RESTRICTION 1 2 3
SUGGESTED PREFFERED
ALTERNATIVES nystatin X
2.4.3 TOPICAL ANTIFUNGAL‐CORTICOSTEROID COMB. clotrimazole‐ betamethasone X nystatin‐triamcinolone X
2.5.1 ANTIRETROVIRALS & PROTEASE INHIBITORS
ALL PRODUCTS ARE COVERED X
2.5.2 OTHER ANTIVIRAL DRUGS
acyclovir X
amantadine hcl X
famciclovir X
ribavirin X
rimantadine X
FLUMADINE SYRUP X
TAMIFLU X
VALTREX X
2.7.2 ANTITUBERCULOSIS DRUGS
isoniazid X
rifampin X
2.7.3 PLASMODICIDES hydroxychloroquine sulfate X
quinine sulfate X
2.7.5 TRICHOMONOCIDES
metronidazole X
2.8 OTHER ANIINFECTIVE DRUGS
ZYVOX PA REQUIRED X
CHAPTER 3: ANTINEOPLASTIC/IMMUNOSUPPRESSANT DRUGS
3.0 ANTINEOPLASTIC/IMMUNOSUPPRESSANT DRUGS
azathioprine X
cyclosporine X
flutamide X
megestrol acetate X
mercaptopurine X
methotrexate X
tamoxifen citrate X
ARIMIDEX X
CASODEX X
CELLCEPT X
ELIGARD X
ENBREL PA REQUIRED* X
FEMARA X
HUMIRA PA REQUIRED* X
CHAPTER 4: CARDIOVASCULAR MEDICATIONS
4.1 CARDIAC GLYCOSIDES
digoxin X
LANOXIN X
4.2 CALCIUM ANTAGONISTS
amlodipine besylate X
cartia xt X
diltiazem er, hcl, xr X
felodipine er X
nicardipine hcl X
nifedipine, er X
verapamil hcl X
4.3.1 LOOP DIURETICS
bumetanide X
furosemide X
torsemide X
4.3.2 THIAZIDE AND RELATED DRUGS
hydrochlorothiazide X
indapamide X
metolazone X
4.3.3 POTASSIUM SPARING DIURETICS
amiloride hcl, w/hctz X
eplerenone X
spironolactone, w/hctz X
triamterene, w/hctz X
4.4 BETA‐ADRENERGIC ANTAGONIST DRUGS atenolol, w/chlorthalidone X
bisoprolol fumarate, w/hctz X
carvedilol X
labetalol hcl X
metoprolol succinate X

TIER
DRUG NAME RESTRICTION 1 2 3
SUGGESTED PREFFERED
ALTERNATIVES metoprolol tartrate, er, w/hctz X nadolol X propranolol hcl, la, w/hctz X
BYSTOLIC X generic atenolol, metoprolol
COREG CR X generic carvedilol INNOPRAN XL X generic propranolol 4.5.1 VASODILATOR ANTIHYPERTENSIVES doxazosin mesylate X hydralazine hcl X prazosin hcl X terazosin hcl X 4.5.2 CENTRALLY ACTING ANTIHYPERTENSIVES clonidine hcl X guanfacine hcl X methydopa X CATAPRES TTS X 4.5.4.1 ANGIOTENSIN CONVERTING ENZYME INHIBITORS (ACEIs) benazepril hcl, w/hctz X captopril, w/hctz X
enalapril maleate, w/hctz X lisinopril, w/hctz 1/2 tab incentive X moexipril hcl X ramipril X
4.5.4.2 ANGIOTENSIN II RECEPTOR ANTAGONISTS (ARBs)
AVALIDE X
AVAPRO 1/2 tab incentive X
DIOVAN 1/2 tab incentive X
DIOVAN HCT X
4.5.6 OTHER ANTIHYPERTENSIVES amlodipine besylate‐benazepril X
TARKA X
TEKTURNA X lisinopril, AVAPRO, DIOVAN
TEKTURNA HCT X lisinopril/hctz, AVALIDE, DIOVAN HCT
4.6.1 NITRATES
isosorbide dinitrate X
isosorbide mononitrate X
nitroglycerin X
4.8.1 HYPOLIPOPROTEINEMICS cholestyramine X
colestipol hcl X
fenofibrate X
gemfibrozil X
LOVAZA PA FOR TRIG>500 X
niacin, simvastatin, lovastatin
NIASPAN X niacin, simvastatin, lovastatin
TRICOR X
WELCHOL X cholestyramine, colestipol
ZETIA STEP THERAPY X
4.8.2 HMG‐COA REDUCTASE INHIBITORS
lovastatin X
pravastatin sodium X
simvastatin
$0 copay for 90 days if switch from brand ‐ expires 7/1/09 X
CRESTOR X
LIPITOR X
4.8.2.1 HMG‐COA COMBINATIONS
ADVICOR X
CADUET X
4.9 OTHER CARDIOVASCULAR DRUGS
pentoxifylline X
CHAPTER 5: AUTONOMIC AND CNS MEDICATIONS
5.1.1 ANALGESICS
tramadol hcl X
tramadol hcl‐acetaminophen X
5.1.1.1 CLASS II NARCOTICS
fentanyl X
fentanyl citrate X
hydromorphone hcl X
methadone hcl X
morphine sulfate, sa X
oxycodone hcl, w/APAP X
TIER
DRUG NAME RESTRICTION 1 2 3
SUGGESTED PREFFERED
ALTERNATIVES
OXYCONTIN X
OXYIR X
5.1.1.2 CLASS III NARCOTICS
acetaminophen‐codeine X
hydrocodone bit‐ibuprofen X hydrocodone‐ acetaminophen X
5.1.1.3 CLASS IV NARCOTICS
propoxyphene hcl‐apap X
propoxyphene napsylate‐apap X
5.1.2 DRUGS TO PREVENT AND TREAT HEADACHES
butalbital‐apap‐caffeine X
butalbital compound X
AMERGE X
IMITREX, MAXALT/MLT, RELPAX
AXERT X
IMITREX, MAXALT/MLT, RELPAX
FROVA X
IMITREX, MAXALT/MLT, RELPAX
IMITREX INJ limit 1 kit/rx X
IMITREX NASAL limit 6/rx X
IMITREX TABS limit 9/rx X
MIGRANAL NASAL limit 4/rx
MAXAL, MLT limit 9/rx X
RELPAX limit 12/rx X
ZOMIG, ZMT X
IMITREX, MAXALT/MLT, RELPAX
5.2.1 ANXIOLYTICS
alprazolam X
buspirone hcl X
diazepam X
lorazepam X
5.2.2 SEDATIVE/HYPNOTIC DRUGS
flurazepam hcl X
temazepam X
triazolam X
zolpidem tartrate X
5.3 ANTIMANIA DRUGS lithium carbonate, ‐citrate X
5.4.1 CARBAMAZEPINES
carbamazepine X
oxcarbazepine X
TEGRETOL XR X
5.4.2 ANTICONVULSANT BENZODIAZEPINES
clonazepam X
5.4.3 HYDANTOINS
phenytoin sodium, extended X phenytoin sodium, extended X
DILANTIN 30mg KAPSEALS X
DILANTIN 50mg INFATABS X
PHENYTEK X
5.4.4 VALPROIC ACID AND DERIVATIVES
divalproex sodium X
valproic acid X
DEPAKOTE ER X
5.4.6 ANTICONVULSANT BARBITURATES
phenobarbital X
primidone X
5.4.7 OTHER ANTICONVULSANTS
gabapentin X
lamotrigine X
levetiracetam X
zonisamide X
LYRICA X
TOPAMAX X
5.5.1.1 TERTIARY AMINES
amitriptyline hcl X
doxepin hcl X
imipramine hcl X
5.5.1.2 SECONDARY AMINES

TIER
DRUG NAME RESTRICTION 1 2 3
SUGGESTED PREFFERED
ALTERNATIVES
desipramine hcl X
nortriptyline hcl X
5.5.1.3 SELECTIVE SEROTONIN REUPTAKE INHIBITORS
citalopram hbr X
fluoxetine hcl X
fluvoxamine maleate X
paroxetine hcl X
sertraline hcl X
5.5.1.4 OTHER ANTIDEPRESSANTS
bupropion hcl, sr, xl X
mirtazapine X
trazodone hcl X
venlafaxine hcl X
CYMBALTA STEP THERAPY; MAX 60MG/DAY X
VENLAFAXINE ER
STEP THERAPY; TIER 2 AT APPROPRIATE DOSE X
5.6 ANTIVERTIGO AND ANTIEMETIC DRUGS
meclizine hcl X
ondansetron hcl, odt X
prochlorperazine maleate X
promethazine hcl X
promethegan X
trimethobenzamide hcl X
EMEND limit 3/rx X
5.7.1 ANTIPARKINSON ANTICHOLINERGIC DRUGS
benztropin meslyate X
5.7.2 OTHER ANTIPARKINSON DRUGS
bromocriptine mesylate X
carbidopa‐levodopa, er X
ropinirole hcl X
selegiline hcl X
AZILECT X
MIRAPEX X
5.8 ANTIPSYCHOTIC DRUGS
clozapine X
haloperidol X
risperidone X
thioridazine hcl X
ABILIFY X
GEODON X
SEROQUEL, XR X
ZYPREXA X
5.9.1 CNS STIMULANT DRUGS
amphetamine salt combo X
dexmethylphenidate hcl X dextroamphetamine sulfate X
methylin, er X
methylphenidate hcl, er X
ADDERALL XR X
CONCERTA X
METADATE CD X
generics, ADDERALL XR, CONCERTA, RITALIN LA
RITALIN LA X
5.9.3 ANTIDEMENTIA DRUGS
galantamine, er X
ARICEPT, ODT X
EXELON X
NAMENDA X
5.9.4 DRUGS TO TREAT MULTIPLE SCLEROSIS
AVONEX PA REQUIRED* X
COPAXONE PA REQUIRED* X AVONEX, REBIF
REBIF PA REQUIRED* X
5.9.6 OTHER DRUGS FOR ADHD
STRATTERA X
CHAPTER 6: DERMATOLOGICAL MEDICATIONS
6.1 TOPICAL CORTICOSTEROID DRUGS
betamethasone dipropionate, aug X
betamethasone valerate X
clobetasol propionate X
desonide X
desoximetasone X
fluocinonide X
TIER
DRUG NAME RESTRICTION 1 2 3
SUGGESTED PREFFERED
ALTERNATIVES fluticasone propionate oint X
mometasone furoate X
triamcinolone acetonide X
PRAMOSONE X
6.2 ANTIPRURITIC DRUGS
hydroxyzine hcl X
hydroxyzine pamoate X
6.3 ANTIACNE DRUGS
clindamycin phosphate X
erythromycin base X erythromycin‐benzoyl peroxide X
metronidazole X sodium sulfacetamine/ sulfur tf X
tretinoin AGE ≤ 30 OR DERM ONLY X
BENZACLIN X
BENZAMYCINPAK X
DIFFERIN X
DUAC CS X FINACEA X metronidazole 0.75% METROGEL X metronidazole 0.75%
NORITATE X
RETIN‐A MICRO AGE ≤ 30 OR DERM ONLY X
RETIN‐A MICRO PUMP AGE ≤ 30 OR DERM ONLY X
6.7 KERATOLYTIC DRUGS
CONDYLOX X
6.8 ANTIPSORIASIS AND ANTIECZEMA DRUGS
calcipotriene X
selenium sulfide X
sulfacetamide sodium X
DOVONEX X
TACLONEX COVERED FOR DERM ONLY X
TAZORAC X
6.9.2 TOPICAL DERMATOLOGICAL DRUGS
amonium lactate X
fluorouracil X
ALDARA X
CARAC X
ELIDEL X
LAC‐HYDRIN X
PROTOPIC X
6.9.3 SCABICIDES
lindane X
permethrin X
CHAPTER 7: EAR‐NOSE‐THROAT MEDICATIONS
7.1 DRUGS AFFECTING THE EAR
a‐b otic X
antipyrine w/benzocaine X
neomycin‐polymyxin‐hc X
ofloxacin X
CERUMENEX X
CIPRODEX X
7.2 DRUGS AFFECTING THE NOSE
fluticasone propionate X
ipratropium bromide X
ASTELIN X
NASONEX X
7.3 DRUGS AFFECTING THE THROAT AND MOUTH
chlorhexidine gluconate X
CHAPTER 8: ENDOCRINE MEDICATIONS
8.1.1 INSULIN
HUMALOG, MIX VIAL X
HUMULIN VIAL X
LANTUS VIAL X
LEVEMIR VIAL X
NOVOLIN VIAL X
NOVOLOG, MIX VIAL X
HUMALOG, MIX PEN/CARTIDGE X HUMULIN PEN/CARTRIDGE X

TIER
DRUG NAME RESTRICTION 1 2 3
SUGGESTED PREFFERED
ALTERNATIVES LANTUS PEN/SOLOSTAR X LEVEMIR PEN X NOVOLOG, MIX PEN/CARTRIDGE X 8.1.2 ORAL HYPOGLYCEMIC DRUGS acarbose X glimepiride X glipizide, ‐er, ‐xl, w/metformin X glyburide, ‐micronized, ‐w/metformin X metformin hcl, ‐er X PRANDIN X STARLIX X
8.1.3 INSULIN SENSITIZERS ACTOPLUS MET X
ACTOS X
AVANDAMET X ACTOPLUS MET AVANDARYL X sulfonylurea + ACTOS
AVANDIA X ACTOS DUETACT X glimepiride + ACTOS 8.1.4 AMYLIN ANALOGUES SYMLIN, PEN PA REQUIRED X 8.1.5.1 INCRETIN MIMETICS BYETTA PA REQUIRED X 8.1.5.2 DIPEPTIDYL PEPTIDASE‐IV INHIBITORS
JANUMET X
JANUVIA X
8.3.1 GLUCOCORTICOID DRUGS dexamethasone X hydrocortisone X methylprednisolone X prednisolone X prednisolone sodium phosphate X prednisone X 8.4.1 THYROID SUPPLEMENTS levothyroxine sodium X levoxyl X unithroid X
8.4.2 ANTITHYROID DRUGS
methimazole X
propylthiouracil X
8.6 OTHER ENDOCRINE DRUGS
alendronate sodium X
desmopressin acetate X etidronate disodium X FORTEO PA REQUIRED* X fortical X SENSIPAR PA REQUIRED* X
CHAPTER 9: GASTROINTESTINAL MEDICATIONS
9.2 ANTIDIARRHEAL DRUGS
diphenoxylate‐atropine X
9.3 ANTISPASMODICS/DRUGS AFFECT GI MOTILITY dicyclomine hcl X hyoscyamine sulfate X metoclopramide hcl X
9.4.1 OTHER ANTIULCER DRUGS misoprostol X sucralfate X
9.4.2 PROTON PUMP INHIBITORS
omeprazole
$0 FIRST FILL IF SWITCH FROM BRAND; limit 30/month X
PREVACID STEP THERAPY; limit 30/month X omeprazole
9.4.3 HELICOBACTER PYLORI DRUGS amox+clarithromycin+ PPI X
9.6 OTHER GI DRUGS hydrocortisone, ‐acetate X
sulfasalazine X ANALPRAM HC X
ASACOL X CANASA X CREON 5, ‐10, ‐20 X NULYTELY, ‐WITH FLAVOR PACKS X
PENTASA X
ULTRASE, ‐MT X
URSO, ‐FORTE X 9.7 IRRITABLE BOWEL DRUGS
TIER
DRUG NAME RESTRICTION 1 2 3
SUGGESTED PREFFERED
ALTERNATIVES
AMITIZA X
CHAPTER 10: IMMUNOLOGICALS AND VACCINES 10.2.1 MYELOID STIMULANTS
NEULASTA PA REQUIRED* X NEUPOGEN
NEUPOGEN PA REQUIRED* X 10.2.2 ERYTHROID STIMULANTS ARANESP PA REQUIRED* X EPOGEN, PROCRIT
EPOGEN PA REQUIRED* X
PROCRIT PA REQUIRED* X 10.2.3 INTERFERONS INTRON‐A * X AVONEX PA REQUIRED* X PEGASYS PA REQUIRED* X REBIF PA REQUIRED* X
CHAPTER 11: MUSCULOSKELETAL MEDICATIONS
11.1.1 SALICYLATES AND RELATED DRUGS
diflunisal X
salsalate X 11.1.2 NON‐STEROIDAL ANTIINFLAMMATORY AGENTS
diclofenac sodium X
etodolac X
ibuprofen X
indomethacin X
meloxicam X
nabumetone X
naproxen X
naproxen sodium X
piroxicam X
CELEBREX limit 30/month X
11.2 DRUGS TO PREVENT AND TREAT GOUT
allopurinol X
colchicine X
probenecid X
11.3.1 DIRECT MUSCLE RELAXANTS
baclofen X tizanidine hcl X
11.3.2 CNS MUSCLE RELAXANTS carisoprodol X
chlorzoxazone X cyclobenzaprine hcl X methocarbamol X orphenadrine citrate X
CHAPTER 12: NUTRITION,BLOOD 12.1 PHOSPHATE BINDERS PHOSLO X RENAGEL X RENVELA X 12.2 POTASSIUM SUPPLEMENTS
k‐dur X
klor‐con 10, ‐m10, m20 X
potassium chloride X 12.3.1 ORAL ANTICOAGULANTS, VITAMIN K warfarin sodium X 12.3.2 HEPARIN AND HEPARIN ANTAGONISTS
ARIXTRA X FRAGMIN, LOVENOX, INNOHEP
FRAGMIN X HEPARIN X INNOHEP X
LOVENOX X 12.4 ANTIPLATELET DRUGS cilostazol X dipyridamole X ticlopidine X AGGRENOX X PLAVIX X 12.7 BLOOD DETOXICANTS lactulose X CHAPTER 13: OBSTETRICAL & GYNECOLOGICAL MEDICATIONS 13.1.2 SPECIALIZED OB/GYN DRUGS LUPRON DEPOT X 13.3 ANDROGEN DRUGS ANDRODERM PA REQUIRED X ANDROGEL PA REQUIRED X
13.4 ESTROGEN DRUGS estradiol X estropipate X me‐testosterone/ estrogen, est X PREMARIN X VAGIFEM X VIVELLE‐DOT X

TIER
DRUG NAME RESTRICTION 1 2 3
SUGGESTED PREFFERED
ALTERNATIVES 13.4.1 ESTROGEN/PROGESTIN COMBINATIONS COMBIPATCH X FEMHRT X PREMPHASE X PREMPRO X 13.4.3 SELECTIVE ESTROGEN RECEPTOR MODULATOR
EVISTA X 13.5 PROGESTIN DRUGS
errin X
jolivette X medroxyprogesterone acetate X
nora‐be X norethindrone acetate X progesterone in oil X CRINONE X
ENDOMETRIN X PROCHIEVE X PROMETRIUM X 13.7 CONTRACEPTIVES
apri X
aviane X
camila X
cryselle X
enprese X
junel fe X
kariva X
lessina X
low‐ogestrel X
microgestin fe X
mononessa X
ocella X
ogestrel X
previfem X
sprintec X
trinessa X
tri‐previfem X
tri‐sprintec X
zovia X
NUVARING X
ORTHO EVRA X
ORTHO TRI‐CYCLEN LO X
PLAN B covered for rx only, no OTC X
YAZ X
CHAPTER 14: OPHTHALMIC MEDICATIONS
14.1.1 OPHTHALMIC TOPICAL ANTIBACTERIAL DRUGS
ciprofloxacin hcl X
erythromycin X
gentamicin sulfate X polymyxin b sul‐trimethoprim X
sulfacetamide sodium X
tobramycin sulfate X
VIGAMOX X
14.2 OPHTHALMIC CORTICOSTEROID DRUGS
prednisolone acetate X
LOTEMAX X
14.3 OPHTHALMIC ANTIINFECTIVE/CORTICOSTEROIDS neomycin‐polymyxin‐ dexameth X sulfacetamide/ prednisone X
tobramycin/dexameth X ZYLET X generics
14.5 ANTIGLAUCOMA DRUGS acetazolamide X brimonidine tartrate X
dorzolamide X
dorzolamide/timolol X
pilocarpine hcl X
timolol maleate X ALPHAGAN P X
AZOPT X generics BETIMOL X timolol
COMBIGAN X generic dorzolamide/ timolol
IOPIDINE X ALPHAGAN P
ISTALOL X timolol
LUMIGAN X
TIER
DRUG NAME RESTRICTION 1 2 3
SUGGESTED PREFFERED
ALTERNATIVES
XALATAN X
14.6 OTHER OPHTHALMIC DRUGS
atropine sulfate X
cromolyn sodium X
diclofenac sodium X
ACULAR, LS X
PATANOL X
RESTASIS X
VOLTAREN X
CHAPTER 15: RESPIRATORY MEDICATIONS 15.1.1 BETA‐2 ADRENERGIC DRUGS albuterol, sulfate X metaproterenol sulfate X terbutaline sulfate X BROVANA X albuterol soln FORADIL X PROAIR HFA X SEREVENT DISKUS X
VENTOLIN HFA X XOPENEX X albuterol soln XOPENEX HFA X 15.1.2 METHYL XANTHINE DRUGS aminophylline X theophylline, anhydrous X UNIPHYL X
15.1.3 OTHER DRUGS FOR ASTHMA
ipratropium bromide X
ipratropium‐albuterol X
ADVAIR DISKUS, HFA X
ATROVENT HFA X
COMBIVENT X
EPIPEN, JR X
FLOVENT DISKUS X
FLOVENT HFA X INTAL X
PULMICORT, FLEXHALER X
SPIRIVA X
SYMBICORT X
TILADE X
15.1.4 LEUKOTRIENE MODIFIERS SINGULAIR STEP THERAPY X
15.2.1 ANTIHISTAMINES
cyproheptadine hcl X
promethazine hcl X
15.2.3 ANTIHISTAMINE/DECONGESTANT COMBINATIONS promethazine vc X
15.3 ANTITUSSIVE AND EXPECTORANT DRUGS
benzonatate X
guaifenesin w/codeine X
guaifenex pse X hydrocodone w/guaifenesin X promethazine w/codeine X
promethazine w/dm X promethazine vc w/codeine X TUSSIONEX X
CHAPTER 16: UROLOGICAL MEDICATIONS 16.1.1 ANTICHOLINERGIC ANTISPASMODICS oxybutynin chloride X oxybutynin chloride er X DETROL/LA X VESICARE X
16.1.3 URINARY ANESTHETICS phenazopyridine hcl X 16.1.4 OTHER GENITOURINARY PRODUCTS finasteride X FLOMAX X UROXATRAL X
CHAPTER 17: DIAGNOSTIC & MISCELLANEOUS MEDICATIONS – NOT APPLICABLE
CHAPTER 18: MEDICAL (MISCELLANEOUS) SUPPLIES
18.1 DIABETIC SUPPLIES
ACCU‐CHEK ‐ ALL strips ‐ limit 205/rx X
FAST TAKE ‐ ALL strips ‐ limit 205/rx X
ONE TOUCH ALL strips ‐ limit 205/rx X
SURESTEP ALL strips ‐ limit 205/rx X

Index a‐b otic 7.1 ABILIFY 5.8 acarbose 8.1.2 ACCU‐CHEK ‐ ALL 18.1 acetaminophen‐codeine 5.1.1.2 acetazolamide 14.5 ACTOPLUS MET 8.1.3 ACTOS 8.1.3 ACULAR, LS 14.6 acyclovir 2.5.2 ADDERALL XR 5.9.1 ADVAIR DISKUS, HFA 15.1.3 ADVICOR 4.8.2.1 AGGRENOX 12.4 albuterol, sulfate 15.1.1 ALDARA 6.9.2 alendronate sodium 8.6 ALL PRODUCTS ARE COVERED 2.5.1 allopurinol 11.2 ALPHAGAN P 14.5 alprazolam 5.2.1 amantadine hcl 2.5.2 AMERGE 5.1.2 amiloride hcl, w/hctz 4.3.3 aminophylline 15.1.2 AMITIZA 9.7 amitriptyline hcl 5.5.1.1 amlodipine besylate 4.2 amlodipine besylate‐benazepril 4.5.6 amonium lactate 6.9.2 amox tr‐potassium clavulanate 2.1.5 amox+clarithromycin+PPI 9.4.3 amoxicillin 2.1.5 amphetamine salt combo 5.9.1 ampicillin 2.1.5 ANALPRAM HC 9.6 ANDRODERM 13.3 ANDROGEL 13.3 antipyrine w/benzocaine 7.1 apri 13.7 ARANESP 10.2.2 ARICEPT, ODT 5.9.3 ARIMIDEX 3 ARIXTRA 12.3.2 ASACOL 9.6 ASTELIN 7.2 atenolol, w/chlorthalidone 4.4 atropine sulfate 14.6 ATROVENT HFA 15.1.3 AVALIDE 4.5.4.2 AVANDAMET 8.1.3 AVANDARYL 8.1.3 AVANDIA 8.1.3 AVAPRO 4.5.4.2 AVELOX, ABC PACK 2.1.9 aviane 13.7 AVONEX 10.2.3 AVONEX 5.9.4 AXERT 5.1.2 azathioprine 3 AZILECT 5.7.2 azithromycin 2.1.4.1 AZOPT 14.5 baclofen 11.3.1 BACTROBAN 2.2 benazepril hcl, w/hctz 4.5.4.1 BENZACLIN 6.3 BENZAMYCINPAK 6.3 benzonatate 15.3 benztropin meslyate 5.7.1 betamethasone dipropionate, aug 6.1 betamethasone valerate 6.1 BETIMOL 14.5 bisoprolol fumarate, w/hctz 4.4 brimonidine tartrate 14.5 bromocriptine mesylate 5.7.2 BROVANA 15.1.1 bumetanide 4.3.1 bupropion hcl, sr, xl 5.5.1.4 buspirone hcl 5.2.1 butalbital compound 5.1.2
butalbital‐apap‐caffeine 5.1.2 BYETTA 8.1.5.1 BYSTOLIC 4.4 CADUET 4.8.2.1 calcipotriene 6.8 camila 13.7 CANASA 9.6 captopril, w/hctz 4.5.4.1 CARAC 6.9.2 carbamazepine 5.4.1 carbidopa‐levodopa, er 5.7.2 carisoprodol 11.3.2 cartia xt 4.2 carvedilol 4.4 CASODEX 3 CATAPRES TTS 4.5.2 cefaclor, er 2.1.1 cefadroxil 2.1.1 cefdinir 2.1.1 cefpodoxime proxetil 2.1.1 cefprozil 2.1.1 cefuroxime 2.1.1 CELEBREX 11.1.2 CELLCEPT 3 cephalexin 2.1.1 CERUMENEX 7.1 chlorhexidine gluconate 2.2 chlorhexidine gluconate 7.3 chlorzoxazone 11.3.2 cholestyramine 4.8.1 ciclopirox 2.4.2 cilostazol 12.4 CIPRODEX 7.1 ciprofloxacin hcl 14.1.1 ciprofloxacin hcl 2.1.9 citalopram hbr 5.5.1.3 clarithromycin 2.1.4.1 clindamycin hcl 2.1.3 clindamycin phosphate 6.3 clindamycin phosphate 2.1.3 clobetasol propionate 6.1 clonazepam 5.4.2 clonidine hcl 4.5.2 clotrimazole 2.4.1 clotrimazole 2.4.2 clotrimazole troche 2.3 clotrimazole‐betamethasone 2.4.3 clozapine 5.8 colchicine 11.2 colestipol hcl 4.8.1 COMBIGAN 14.5 COMBIPATCH 13.4.1 COMBIVENT 15.1.3 CONCERTA 5.9.1 CONDYLOX 6.7 COPAXONE 5.9.4 COREG CR 4.4 CREON 5, ‐10, ‐20 9.6 CRESTOR 4.8.2 CRINONE 13.5 cromolyn sodium 14.6 cryselle 13.7 cyclobenzaprine hcl 11.3.2 cyclosporine 3 CYMBALTA 5.5.1.4 cyproheptadine hcl 15.2.1 DEPAKOTE ER 5.4.4 desipramine hcl 5.5.1.2 desmopressin acetate 8.6 desonide 6.1 desoximetasone 6.1 DETROL/LA 16.1.1 dexamethasone 8.3.1 dexmethylphenidate hcl 5.9.1 dextroamphetamine sulfate 5.9.1 diazepam 5.2.1 diclofenac sodium 14.6 diclofenac sodium 11.1.2 dicyclomine hcl 9.3 DIFFERIN 6.3 diflunisal 11.1.1 digoxin 4.1
DILANTIN 30mg KAPSEALS 5.4.3 DILANTIN 50mg INFATABS 5.4.3 diltiazem er, hcl, xr 4.2 DIOVAN 4.5.4.2 DIOVAN HCT 4.5.4.2 diphenoxylate‐atropine 9.2 dipyridamole 12.4 divalproex sodium 5.4.4 dorzolamide 14.5 dorzolamide/timolol 14.5 DOVONEX 6.8 doxazosin mesylate 4.5.1 doxepin hcl 5.5.1.1 doxycycline hyclate 2.1.7 doxycycline monohydrate 2.1.7 DUAC CS 6.3 DUETACT 8.1.3 econazole nitrate 2.4.2 ELIDEL 6.9.2 ELIGARD 3 EMEND 5.6 enalapril maleate, w/hctz 4.5.4.1 ENBREL 3 ENDOMETRIN 13.5 enprese 13.7 EPIPEN, JR 15.1.3 eplerenone 4.3.3 EPOGEN 10.2.2 errin 13.5 erythromycin 14.1.1 erythromycin base 6.3 erythromycin ethylsuccinate 2.1.4 erythromycin stearate 2.1.4 erythromycin w/sulfisoxazole 2.1.6 erythromycin‐benzoyl peroxide 6.3 estradiol 13.4 estropipate 13.4 etidronate disodium 8.6 etodolac 11.1.2 EVISTA 13.4.3 EXELON 5.9.3 famciclovir 2.5.2 FAST TAKE ‐ ALL 18.1 felodipine er 4.2 FEMARA 3 FEMHRT 13.4.1 fenofibrate 4.8.1 fentanyl 5.1.1.1 fentanyl citrate 5.1.1.1 FINACEA 6.3 finasteride 16.1.4 FLOMAX 16.1.4 FLOVENT DISKUS 15.1.3 FLOVENT HFA 15.1.3 fluconazole 2.3 FLUMADINE SYRUP 2.5.2 fluocinonide 6.1 fluorouracil 6.9.2 fluoxetine hcl 5.5.1.3 flurazepam hcl 5.2.2 flutamide 3 fluticasone propionate 7.2 fluticasone propionate oint 6.1 fluvoxamine maleate 5.5.1.3 FORADIL 15.1.1 FORTEO 8.6 fortical 8.6 FRAGMIN 12.3.2 FROVA 5.1.2 furosemide 4.3.1 gabapentin 5.4.7 galantamine, er 5.9.3 GANTRISIN 2.1.6 gemfibrozil 4.8.1 gentamicin sulfate 2.2 gentamicin sulfate 14.1.1 GEODON 5.8 glimepiride 8.1.2 glipizide, ‐er, ‐xl, w/metformin 8.1.2 glyburide, ‐micronized, ‐w/metformin 8.1.2 guaifenesin w/codeine 15.3 guaifenex pse 15.3

guanfacine hcl 4.5.2 GYNAZOLE‐1 2.4.1 haloperidol 5.8 HEPARIN 12.3.2 HUMALOG, MIX PEN/CARTIDGE 8.1.1 HUMALOG, MIX VIAL 8.1.1 HUMIRA 3 HUMULIN PEN/CARTRIDGE 8.1.1 HUMULIN VIAL 8.1.1 hydralazine hcl 4.5.1 hydrochlorothiazide 4.3.2 hydrocodone bit‐ibuprofen 5.1.1.2 hydrocodone w/guaifenesin 15.3 hydrocodone‐acetaminophen 5.1.1.2 hydrocortisone 8.3.1 hydrocortisone, ‐acetate 9.6 hydromorphone hcl 5.1.1.1 hydroxychloroquine sulfate 2.7.3 hydroxyzine hcl 6.2 hydroxyzine pamoate 6.2 hyoscyamine sulfate 9.3 ibuprofen 11.1.2 imipramine hcl 5.5.1.1 IMITREX INJ 5.1.2 IMITREX NASAL 5.1.2 IMITREX TABS 5.1.2 indapamide 4.3.2 indomethacin 11.1.2 INNOHEP 12.3.2 INNOPRAN XL 4.4 INTAL 15.1.3 INTRON‐A 10.2.3 IOPIDINE 14.5 ipratropium bromide 7.2 ipratropium bromide 15.1.3 ipratropium‐albuterol 15.1.3 isoniazid 2.7.2 isosorbide dinitrate 4.6.1 isosorbide mononitrate 4.6.1 ISTALOL 14.5 itraconazole 2.3 JANUMET 8.1.5.2 JANUVIA 8.1.5.2 jolivette 13.5 junel fe 13.7 kariva 13.7 k‐dur 12.2 KETEK, ‐PAK 2.1.4.2 ketoconazole 2.3 ketoconazole 2.4.2 klor‐con 10, ‐m10, m20 12.2 labetalol hcl 4.4 LAC‐HYDRIN 6.9.2 lactulose 12.7 lamotrigine 5.4.7 LANOXIN 4.1 LANTUS PEN/SOLOSTAR 8.1.1 LANTUS VIAL 8.1.1 lessina 13.7 LEVAQUIN 2.1.9 LEVEMIR PEN 8.1.1 LEVEMIR VIAL 8.1.1 levetiracetam 5.4.7 levothyroxine sodium 8.4.1 levoxyl 8.4.1 lidocaine hcl, ‐viscous 1.2 LIDODERM 1.2 lindane 6.9.3 LIPITOR 4.8.2 lisinopril, w/hctz 4.5.4.1 lithium carbonate, ‐citrate 5.3 lorazepam 5.2.1 LOTEMAX 14.2 lovastatin 4.8.2 LOVAZA 4.8.1 LOVENOX 12.3.2 low‐ogestrel 13.7 LUMIGAN 14.5 LUPRON DEPOT 13.1.2 LYRICA 5.4.7 MAXAL, MLT 5.1.2 meclizine hcl 5.6
medroxyprogesterone acetate 13.5 megestrol acetate 3 meloxicam 11.1.2 mercaptopurine 3 METADATE CD 5.9.1 metaproterenol sulfate 15.1.1 me‐testosterone/estrogen, est 13.4 metformin hcl, ‐er 8.1.2 methadone hcl 5.1.1.1 methimazole 8.4.2 methocarbamol 11.3.2 methotrexate 3 methydopa 4.5.2 methylin, er 5.9.1 methylphenidate hcl, er 5.9.1 methylprednisolone 8.3.1 metoclopramide hcl 9.3 metolazone 4.3.2 metoprolol succinate 4.4 metoprolol tartrate, er, w/hctz 4.4 METROGEL 6.3 metronidazole 6.3 metronidazole 2.7.5 microgestin fe 13.7 MIGRANAL NASAL 5.1.2 minocycline hcl 2.1.7 MIRAPEX 5.7.2 mirtazapine 5.5.1.4 misoprostol 9.4.1 moexipril hcl 4.5.4.1 mometasone furoate 6.1 mononessa 13.7 morphine sulfate, sa 5.1.1.1 mupirocin 2% ointment 2.2 nabumetone 11.1.2 nadolol 4.4 NAMENDA 5.9.3 naproxen 11.1.2 naproxen sodium 11.1.2 NASONEX 7.2 neomycin‐polymyxin‐dexameth 14.3 neomycin‐polymyxin‐hc 7.1 NEULASTA 10.2.1 NEUPOGEN 10.2.1 NIASPAN 4.8.1 nicardipine hcl 4.2 nifedipine, er 4.2 nitrofurantoin, macrocrystal 2.1.8 nitroglycerin 4.6.1 nora‐be 13.5 norethindrone acetate 13.5 NORITATE 6.3 nortriptyline hcl 5.5.1.2 NOVOLIN VIAL 8.1.1 NOVOLOG, MIX PEN/CARTRIDGE 8.1.1 NOVOLOG, MIX VIAL 8.1.1 NULYTELY, ‐WITH FLAVOR PACKS 9.6 NUVARING 13.7 nystatin 2.3 nystatin 2.4.1 nystatin 2.4.2 nystatin‐triamcinolone 2.4.3 ocella 13.7 ofloxacin 7.1 ogestrel 13.7 omeprazole 9.4.2 ondansetron hcl, odt 5.6 ONE TOUCH ALL 18.1 orphenadrine citrate 11.3.2 ORTHO EVRA 13.7 ORTHO TRI‐CYCLEN LO 13.7 oxcarbazepine 5.4.1 oxybutynin chloride 16.1.1 oxybutynin chloride er 16.1.1 oxycodone hcl, w/APAP 5.1.1.1 OXYCONTIN 5.1.1.1 OXYIR 5.1.1.1 paroxetine hcl 5.5.1.3 PATANOL 14.6 PEGASYS 10.2.3 penicillin v potassium 2.1.5 PENTASA 9.6
pentoxifylline 4.9 permethrin 6.9.3 phenazopyridine hcl 16.1.3 phenobarbital 5.4.6 PHENYTEK 5.4.3 phenytoin sodium, extended 5.4.3 phenytoin sodium, extended 5.4.3 PHOSLO 12.1 pilocarpine hcl 14.5 piroxicam 11.1.2 PLAN B 13.7 PLAVIX 12.4 polymyxin b sul‐trimethoprim 14.1.1 potassium chloride 12.2 PRAMOSONE 6.1 PRANDIN 8.1.2 pravastatin sodium 4.8.2 prazosin hcl 4.5.1 prednisolone 8.3.1 prednisolone acetate 14.2 prednisolone sodium phosphate 8.3.1 prednisone 8.3.1 PREMARIN 13.4 PREMPHASE 13.4.1 PREMPRO 13.4.1 PREVACID 9.4.2 previfem 13.7 primidone 5.4.6 PROAIR HFA 15.1.1 probenecid 11.2 PROCHIEVE 13.5 prochlorperazine maleate 5.6 PROCRIT 10.2.2 progesterone in oil 13.5 promethazine hcl 5.6 promethazine hcl 15.2.1 promethazine vc 15.2.3 promethazine vc w/codeine 15.3 promethazine w/codeine 15.3 promethazine w/dm 15.3 promethegan 5.6 PROMETRIUM 13.5 propoxyphene hcl‐apap 5.1.1.3 propoxyphene napsylate‐apap 5.1.1.3 propranolol hcl, la, w/hctz 4.4 propylthiouracil 8.4.2 PROTOPIC 6.9.2 PULMICORT, FLEXHALER 15.1.3 quinine sulfate 2.7.3 ramipril 4.5.4.1 REBIF 10.2.3 REBIF 5.9.4 RELPAX 5.1.2 RENAGEL 12.1 RENVELA 12.1 RESTASIS 14.6 RETIN‐A MICRO 6.3 RETIN‐A MICRO PUMP 6.3 ribavirin 2.5.2 rifampin 2.7.2 rimantadine 2.5.2 risperidone 5.8 RITALIN LA 5.9.1 ropinirole hcl 5.7.2 salsalate 11.1.1 selegiline hcl 5.7.2 selenium sulfide 6.8 SENSIPAR 8.6 SEREVENT DISKUS 15.1.1 SEROQUEL, XR 5.8 sertraline hcl 5.5.1.3 silver sulfadiazine 2.2 simvastatin 4.8.2 SINGULAIR 15.1.4 sodium sulfacetamine/sulfur tf 6.3 SPIRIVA 15.1.3 spironolactone, w/hctz 4.3.3 SPORANOX SOLN 2.3 sprintec 13.7 STARLIX 8.1.2 STRATTERA 5.9.6 sucralfate 9.4.1

sulfacetamide sodium 6.8 sulfacetamide sodium 14.1.1 sulfacetamide/prednisone 14.3 sulfamethoxazole‐trimethoprim 2.1.6 sulfasalazine 9.6 SURESTEP ALL 18.1 SYMBICORT 15.1.3 SYMLIN, PEN 8.1.4 TACLONEX 6.8 TAMIFLU 2.5.2 tamoxifen citrate 3 TARKA 4.5.6 TAZORAC 6.8 TEGRETOL XR 5.4.1 TEKTURNA 4.5.6 TEKTURNA HCT 4.5.6 temazepam 5.2.2 terazosin hcl 4.5.1 terbinafine hcl 2.3 terbutaline sulfate 15.1.1 terconazole 2.4.1 tetracycline hcl 2.1.7 theophylline, anhydrous 15.1.2 thioridazine hcl 5.8 ticlopidine 12.4 TILADE 15.1.3 timolol maleate 14.5 tizanidine hcl 11.3.1 tobramycin sulfate 14.1.1 tobramycin/dexameth 14.3 TOPAMAX 5.4.7 torsemide 4.3.1 tramadol hcl 5.1.1 tramadol hcl‐acetaminophen 5.1.1 trazodone hcl 5.5.1.4 tretinoin 6.3 triamcinolone acetonide 6.1 triamterene, w/hctz 4.3.3 triazolam 5.2.2 TRICOR 4.8.1 trimethobenzamide hcl 5.6 trimethoprim 2.1.8 trimox 2.1.5 trinessa 13.7 tri‐previfem 13.7 tri‐sprintec 13.7 TUSSIONEX 15.3 ULTRASE, ‐MT 9.6 UNIPHYL 15.1.2 unithroid 8.4.1 UROXATRAL 16.1.4 URSO, ‐FORTE 9.6 VAGIFEM 13.4 valproic acid 5.4.4 VALTREX 2.5.2 VENLAFAXINE ER 5.5.1.4 venlafaxine hcl 5.5.1.4 VENTOLIN HFA 15.1.1 verapamil hcl 4.2 VESICARE 16.1.1 VIGAMOX 14.1.1 VIVELLE‐DOT 13.4 VOLTAREN 14.6 warfarin sodium 12.3.1 WELCHOL 4.8.1 XALATAN 14.5 XOPENEX 15.1.1 XOPENEX HFA 15.1.1 YAZ 13.7 ZETIA 4.8.1 ZMAX 2.1.4.1 zolpidem tartrate 5.2.2 ZOMIG, ZMT 5.1.2 zonisamide 5.4.7 zovia 13.7 ZYLET 14.3 ZYPREXA 5.8 ZYVOX 2.8
HP-0046 1/09





























