Embed Size (px)
Citation preview

REVIEWS
Sorafenib: Where Do We Go from Here?Abby B. Siegel, Sonja K. Olsen, Arthur Magun, and Robert S. Brown, Jr
The approval of sorafenib as the first effective drug for the treatment of hepatocellular car-cinoma (HCC) represents a milestone in the treatment of this disease. A better understand-ing of HCC pathogenesis has led to the development of several novel targeted treatments.HCC is treated in a uniquely multidisciplinary way requiring surgeons, hepatologists,interventional radiologists, and oncologists. This review describes the molecular pathoge-nesis of HCC, explores current and future treatments based on these pathways, anddescribes how these new therapies may augment existing approaches to HCC treatmen-t.(HEPATOLOGY 2010;52:360-369)
Hepatocellular carcinoma (HCC) is the thirdmost common cause of cancer-relateddeaths.1 HCC usually occurs in the setting of
underlying liver diseases, including hepatitis B and C,nonalcoholic fatty liver disease, and alcohol-inducedcirrhosis. The incidence of HCC in the United Stateshas almost doubled in recent decades because of theincreased prevalence of chronic hepatitis C, migrationfrom endemic areas, and, increasingly, nonalcoholicfatty liver disease.2,3 Until recently, there were no sys-temic treatment options that clearly improved survivalfor those with advanced HCC. Because of the diverseetiologies underlying HCC, there is likely no one
genetic mutation or molecular pathway crucial for allHCC tumorigenesis.The vast majority of HCC cases develop in the setting
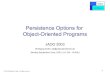
of chronic hepatitis or cirrhosis and may take over 30years to develop. Initially, hepatocytes proliferate in thesetting of increased levels of cytokines such as tumor ne-crosis factor a. Genetic and epigenetic changes then leadto dysplastic hepatocytes and finally HCC.4 Hepatitis Bmay act as a direct carcinogen by integrating into thehost genome and leading to genomic instability. Cirrho-sis is not always a necessary intermediate, and patientsmay have excellent underlying liver function; this leadsto different treatment possibilities (e.g., the resection oflarge tumors). Hepatitis C virus (HCV) infection isalmost always associated with cirrhosis when HCC hasdeveloped. Both cirrhosis and HCV may act on differ-ent pathways to enhance cancer development. Forinstance, HCV has been shown to act as a Wnt ligand,which can up-regulate cell signaling pathways, whereascirrhosis leads to many changes, including oxidativestress, which may contribute to carcinogenesis.5 HCC isa particularly heterogeneous disease, and many patho-genic processes contribute to carcinogenesis. However,several carcinogenic pathways have now been identifiedin the development and progression of HCC, andthey provide new molecular targets for HCC treatment(Fig. 1).We summarize several promising targets and drugs
that affect these pathways, including the vascular endo-thelial growth factor receptor (VEGFR), epidermalgrowth factor receptor (EGFR), and mammalian targetof rapamycin (mTOR) pathways. We discuss ways toconceptualize combining these agents alone and withvarious other treatment modalities, including locore-gional therapies, resection, and transplantation. Wediscuss novel pathways involving fibroblast growth fac-tor receptor (FGFR), insulin-like growth factor
Abbreviations: AFP, alpha-fetoprotein; AKT, protein kinase B; c-MET,mesenchymal epithelial transition factor; CP, Child-Pugh; DCE, dynamiccontrast-enhanced; EGF, epidermal growth factor; EGFR, epidermal growthfactor receptor; FGFR, fibroblast growth factor receptor; GEMOX, gemcitabineand oxaliplatin; HCC, hepatocellular carcinoma; HCV, hepatitis C virus;HDAC, histone deacetylase; HER, human epidermal growth factor receptor;IGF, insulin growth factor; IGF1R, insulin-like growth factor 1 receptor;IGFR, insulin-like growth factor receptor; MEK, mitogen-activated proteinkinase kinase; MRI, magnetic resonance imaging; mTOR, mammalian targetof rapamycin; PDGFR, platelet-derived growth factor receptor; PI3K,phosphoinositide 3-kinase; SHARP, Sorafenib HCC Assessment RandomizedProtocol; SRC, sarcoma; TRAIL, tumor necrosis factor–related apoptosis-inducing ligand; ULN, upper limit of normal; VEGF, vascular endothelialgrowth factor; VEGFR, vascular endothelial growth factor receptor.From the Departments of Medicine and Surgery, Columbia University College
of Physicians and Surgeons, New York, NY.Received January 8, 2010; accepted February 17, 2010.This study was supported by a Clinical and Translational Science Award/
National Cancer Institute K12 Career Development Award (KL2 RR024157-03 to Abby B. Siegel).Address reprint requests to: Abby B. Siegel, Center for Liver Disease and
Transplantation, NewYork–Presbyterian Hospital, 622 West 168th Street, PH14 105-C, New York, NY 10032-3784. E-mail: [email protected]; fax:212-305-4343.CopyrightVC 2010 by the American Association for the Study of Liver Diseases.Published online in Wiley InterScience (www.interscience.wiley.com).DOI 10.1002/hep.23633Potential conflict of interest: Dr. Siegel received grants from Bayer, Bristol-
Myers Squibb, and Imclone.
360

receptor (IGFR) signaling, and modulation of apopto-sis. Finally, we examine how molecular studies inHCC are helping to define new targets for HCC treat-ment and prevention.
VEGFR/EGFR Pathway
VEGFR. HCC is one of the most vascular solidtumors known. Vascular endothelial growth factor(VEGF) is a primary mediator of angiogenesis inHCC.6,7 Antiangiogenic drugs such as sorafenib(which acts in part by blocking the VEGF tyrosine ki-nase receptor) and bevacizumab have already shownsignificant clinical activity in HCC, and sorafenib isnow the first Food and Drug Administration–approvedagent for patients with advanced HCC.8,9
Sorafenib is a tyrosine kinase inhibitor directedagainst several targets, including VEGFR2 and Raf ki-nase. It has now been studied in two large, multicenter,randomized controlled trials in patients with advanced,unresectable HCC. In the Sorafenib HCC AssessmentRandomized Protocol (SHARP) study, 602 primarilyEuropean patients were randomized to sorafenib (400mg twice daily) or placebo. Patients with advanced dis-ease in this study were defined as being ineligible for,or having disease progression after, surgical or locore-gional therapies. They also had an Eastern CooperativeOncology Group performance status of 2 or less, andChild-Pugh (CP) liver function class A disease. Thesorafenib group had a median overall survival time of10.7 months versus 7.9 months in the placebo arm (P� 0.001).9
In a second randomized study conducted in Asia,271 patients were again randomized to sorafenib orplacebo. The median survival time in the sorafenibgroup was 6.5 months versus 4.2 months for the pla-cebo group (hazard ratio ¼ 0.68, P ¼ 0.014).10 Thisworsened survival may have been due to moreadvanced disease on presentation, but the degree ofbenefit from sorafenib in each study was almost identi-cal. The results of these studies led to the approval ofsorafenib for treatment of advanced HCC in patientsin the United States and Europe in 2007. These trialsboth demonstrated a clear overall survival advantage inthe setting of a randomized controlled trial, the end-point with the highest level of evidence to support it.Overall, sorafenib is usually well tolerated. Major
side effects include hand-foot syndrome (5%-8% inthe US study and 11% in the Asian study), fatigue(8%-10%), and diarrhea (9%). Although there was nosignificant increase in serious bleeding events seen ineither of the phase III trials, this complication may de-velop more commonly in patients with CP class B orC disease.11
These two pivotal trials of sorafenib both studiedpatients with preserved liver function. Less is knownabout the drug’s effects in patients with decompensatedliver disease, although sorafenib is approved in theUnited States for everyone with unresectable HCC.Abou-Alfa and colleagues12 looked at the use of sorafe-nib in a phase II study of 137 patients, 39 of whomhad CP class B disease, and found no difference in thetolerability of sorafenib in patients with CP class A orB disease. A retrospective study evaluated sorafenib in59 patients, 23 of whom were classified as having CPclass B disease and 10 of whom had CP class C disease.
Fig. 1. Molecularly targeted ther-apy in HCC.
HEPATOLOGY, Vol. 52, No. 1, 2010 SIEGEL ET AL. 361

The median survival times for patients with CP classA, B, and C disease were 8.3, 4.3, and 1.5 months,respectively (P ¼ 0.0001). The authors concluded thatthere was no benefit from systemic therapy in patientswith very advanced liver disease.11 Subsequently pub-lished work has suggested that the dosage of sorafenibshould be reduced to 200 mg twice daily in patientswith bilirubin levels >1.5 times but <3 times theupper limit of normal (ULN); for patients with levels�3 times ULN but less than 10 times ULN, even 200mg every 3 days was not tolerated.13 The use of sorafe-nib in patients with decompensated liver disease needsto be studied prospectively in larger numbers ofpatients to better assess its efficacy.To date, few predictive biomarkers have been shown
to definitively correlate with the response to sorafenib.Expression of phosphorylated extracellular signal-regu-lated kinase by immunohistochemistry was associatedwith improved progression-free survival in a subset ofpatients treated in a phase II trial of sorafenib inHCC.12 These data were validated in abstract form inthe SHARP trial.14 Several biomarkers are beingactively studied, including circulating endothelial cellsand plasma cytokines, but none has yet shown definitepredictive or prognostic value. Imaging studies usingdynamic contrast-enhanced (DCE) magnetic resonanceimaging (MRI) have shown that decreased angiogenesisis at least one mechanism of efficacy for sorafenib, butthe relative contributions of blockading the other path-ways is unknown.15 As we move forward with usingsorafenib in HCC, defining mechanisms of action andbiomarkers that predict response will be crucial fordeveloping individualized and cost-effective care.Bevacizumab is a recombinant humanized monoclo-
nal antibody directed against VEGF-A. It is approvedfor the treatment of several malignancies in the UnitesStates, including non–small cell lung cancer, breast can-cer, kidney cancer, and colon cancer. Bevacizumab’smechanism of action may include normalization ofleaky tumor vasculature in addition to the reduction ofthe actual number of blood vessels seen withintumors.16 Bevacizumab has been studied as a singleagent in the treatment of HCC. In a multicenter phaseII study of 46 patients with compensated liver diseaseand unresectable HCC, we reported 6-month progres-sion-free survival in 65% of patients, with 13% experi-encing a partial response to treatment (a 30% decreasein the sum of the longest diameters of the targetlesions). This response rate compares favorably to thatseen in the sorafenib trials, in which only 2% to 3% ofpatients had objective radiological responses. The crite-ria for advanced disease in this trial differed from those
in the SHARP trial. Patients in our study wereexcluded if they had greater than 50% involvement ofthe liver parenchyma by a tumor, invasion of the mainportal vein or vena cava, or extrahepatic disease. Onthe other hand, 26% of the patients in the bevacizu-mab study had CP class B disease. The study waspowered for a primary endpoint of 6-month progres-sion-free survival of 60%, which it met; the medianprogression-free survival time with bevacizumab was6.9 months, and the overall survival rate was 53% at 1year. A major side effect of bevacizumab was bleeding,with 11% of patients having serious bleeding complica-tions, including one fatal variceal bleed early in thestudy. After modifying the protocol to perform upperendoscopy and banding of esophageal varices prior tousing bevacizumab, we no longer saw this complica-tion.8 It is possible that we saw more serious bleedingevents because more of our patients had CP class B dis-ease, in contrast to the pivotal sorafenib trials discussed,in which almost all patients had CP class A disease.Issues related to heterogeneous patient selection in
HCC trials have now been discussed as part of anAmerican Association for the Study of Liver Diseasesconference in 2006, and guidelines were published in2008.17 These guidelines call for standardization ofpopulations studied with novel targeted therapies, andsuggest the use of the Barcelona Clinic Liver Cancercriteria to define advanced disease. The conference par-ticipants also discussed standardization of clinical end-points; they moved away from the response rate as aprimary measure of outcome and suggested random-ized phase II trials with a time to event endpoint asone way of moving forward in clinical trials in HCCwith less potential selection bias.17
Bevacizumab has also been studied in conjunctionwith chemotherapy for the treatment of unresectableHCC. In a phase II study of 33 patients, almost halfof whom had metastatic disease, treatment with beva-cizumab and gemcitabine and oxaliplatin (GEMOX)resulted in a 20% response rate with an overall mediansurvival time of 9.6 months.18 In a phase II trial ofGEMOX alone, a response rate of 18% was seen inHCC, and this suggested little clinical benefit with theaddition of bevacizumab.19
Sunitinib is another oral tyrosine kinase inhibitorthat blocks several receptors, including VEGFR1,VEGFR2, VEGFR3, platelet-derived growth factor re-ceptor a (PDGFRa), PDGFRb, and stem cell factorreceptor (KIT). Like sorafenib, it is approved for thetreatment of another particularly vascular tumor, renalcell carcinoma. Its clinical spectrum overlaps that ofsorafenib, and it has been studied in two separate
362 SIEGEL ET AL. HEPATOLOGY, July 2010

phase II trials in HCC using different dose sched-ules.20,21 The first study by Zhu and colleagues20
showed a response rate of 2.9% in 34 patients, withan average overall survival time of 9.8 months. Theirprimary outcome was progression-free survival. Thedosage was 37.5 mg daily for 28 days followed by 14days of rest in 6-week cycles. The authors found thathigher levels of inflammatory biomarkers such as inter-leukin-6 predicted worsened outcome, and DCE MRIimaging could predict delayed recurrence. Faivre andcolleagues21 studied a higher dose of sunitinib, 50 mgdaily for 4 weeks followed by a 2-week rest, in 37patients from France and Asia. The primary outcome,the response rate, was at 2.7%, and toxicity was highwith this dose schedule, with 10% of patients dyingfrom treatment-related causes. There is currently anongoing international phase III trial comparing sorafe-nib with sunitinib in advanced HCC patients.EGFR. EGFR is an active target for several onco-
logical chemotherapeutics. The receptor may beattacked extracellularly through the use of antibodiesthat block the receptor or intracellularly via binding tothe adenosine triphosphate binding site of the recep-tor’s tyrosine kinase domain. Cetuximab and panitu-mumab are antibodies targeted against EGFR, andthey are used for the treatment of advanced colorectalcancer and head and neck cancers.22-24 Gefitinib anderlotinib target the EGFR tyrosine kinase, and areused in the treatment of lung and pancreatic can-cers.25,26 EGFR is overexpressed in 40% to 70% ofHCCs,27 and activation of the receptor is also involvedin HCC pathogenesis.28,29 Fluorescence in situ hybrid-ization showed extra EGFR gene copies in about halfof HCCs in one study, and this was accompanied bygains in chromosome 7, which suggested balancedpolysomy rather than gene amplification.27 EGFRinhibitors prevent the development of HCC in animalmodels,28,30 and tyrosine kinase inhibitors againstEGFR have shown some activity in HCC to date.Erlotinib is an orally administered small molecule
EGFR inhibitor that targets the tyrosine kinase do-main. It has been studied as a single agent in HCC intwo US phase II trials at a dose of 150 mg daily. Inone study of 38 patients with unresectable HCC, 8%of patients had partial responses, 32% were progres-sion-free at 6 months, and the median overall survivaltime was 13 months.31 Erlotinib was studied inanother trial of 40 patients with Child A or B cirrhosisand advanced HCC. In this trial, there were no com-plete or partial responses, with a median overall sur-vival time of 10.8 months.32 Recently, Thomas andcolleagues33 evaluated the combination of erlotinib
with bevacizumab in a phase II study of 40 patients.With progression-free survival as the primary outcome,the combination yielded a 25% objective response ratewith a provocative median overall survival time of15.6 months. Patients in this study were slightly lessadvanced in terms of Barcelona Clinic Liver Cancerstaging than those in the SHARP trial, although morehad CP class B disease, and more were previouslytreated. Side effects of this regimen included gastroin-testinal bleeding (12.5%) and fatigue (20%). Thiscombination is currently being compared to sorafenibin a multicenter phase II trial.In contrast to erlotinib, cetuximab is a monoclonal
antibody directed against the epidermal growth factor(EGF) receptor. Like bevacizumab, it has become animportant component of standard therapy for manypatients with advanced, K-ras wild-type colorectal can-cer. Unlike erlotinib, it has not shown evidence of sig-nificant tumor responses in HCC. In one phase II trial,it was given to 30 patients with unresectable HCC fora period of 6 weeks. Although the regimen was welltolerated, no objective tumor responses were seen.34 In45 treatment-naı̈ve patients with advanced HCC, thecombination of GEMOX with cetuximab was associ-ated with progression-free survival of 4.7 months, over-all survival of 9.5 months, and a 40% 1-year survivalrate.35 Given the efficacy of the GEMOX combinationwithout the additional agent, the benefit of cetuximabremains uncertain. Similarly, lapatinib, a dual tyrosinekinase inhibitor against EGFR and human epidermalgrowth factor receptor 2 (HER2; another member ofthe EGFR family and an important target for breastand gastric cancer treatment), did not show significantactivity in a multicenter phase II trial.36
Unfortunately, no specific biological predictors ofresponse to EGF antagonists have been found to datefor HCC patients. Specific activating mutations ofEGFR have been found in lung cancer and have beenshown to predict response to some EGFR tyrosine ki-nase inhibitors,25 but they have not been seen inHCC.37 Similarly, although K-ras mutations have pre-dicted insensitivity to EGFR blockade in several tumortypes, these also have not yet been well studied inHCC.38 Interestingly, development of a skin rash hasbeen shown to predict response to all inhibitors of theEGFR pathway, and there is a suggestion that thismay also be the case in HCC.31
mTOR Pathway
The EGF and insulin growth factor (IGF) signalingpathways activate several downstream proteins,
HEPATOLOGY, Vol. 52, No. 1, 2010 SIEGEL ET AL. 363

including phosphoinositide 3-kinase (PI3K), proteinkinase B (AKT), and mTOR. AKT is an oncogenethat regulates several processes, including cell growthvia the mTOR pathway. In one large study, aberrantmTOR signaling was seen in about half of HCCcases, and this was associated with insulin-like growthfactor and EGF activation. Blockage of mTOR signal-ing in a cell culture and a xenograft model with ever-olimus decreased tumor growth.39
Sirolimus (rapamycin) is an mTOR inhibitor withimmunosuppressive properties that may be used insolid organ transplant patients. It has recently beendemonstrated to have antitumor properties via inhibi-tion of m-TOR signaling.40-42 In a retrospective studyof 73 patients who underwent liver transplantation forHCC outside the Milan criteria, those who receivedsirolimus had better survival than those who weregiven tacrolimus-based immunosuppression, and thiswas thought to be due to later and possibly fewerrecurrences.43 The use of sirolimus is associated withan increased risk of hepatic artery thrombosis andpoor wound healing, primarily in the immediate post-transplant period, and this limits its use as initialimmunosuppression.Sirolimus has also been studied outside transplanta-
tion in patients with primary liver tumors. Forinstance, in a small pilot study of 21 patients withHCC, 6 patients either had stable disease or had a par-tial remission.44 Further studies need to be performedto assess the role of sirolimus in the treatment ofHCC in both pretransplant and posttransplant set-tings. Everolimus is another mTOR inhibitor that hasbeen shown to have activity against HCC in xenograftsand is now being studied in phase II trials in meta-static disease.45 Everolimus has also been studied inconjunction with sorafenib treatment with promisingearly results.46
New Directions
The identification of sorafenib marks a majoradvance in the field as the first effective targeted ther-apy for HCC. Sorafenib is now approved for the treat-ment of advanced HCC in the United States andEurope, and its role in treatment is being studied indifferent contexts. For instance, it is being evaluated asadjuvant and neoadjuvant therapy in patients under-going locoregional treatment and as adjuvant therapyin patients undergoing surgical resection. Our institu-tion is pilot-testing sorafenib in high-risk HCCpatients (i.e., patients defined as being outside theMilan criteria or having aggressive features on explant
pathology) after transplantation to assess safety in thissetting. There is also consideration of its use as a che-mopreventive in patients with cirrhosis. The patientnumbers and resources needed to complete such a trialwould be large, however, and there are also concernsabout possible long-term toxicities, such as squamouscell carcinoma, which has been reported with sorafenibuse and may possibly be related to the hyperkeratosisthat is a side effect of the drug.47
In addition to evaluating sorafenib in these differentcontexts, there are several ways to conceptualize HCCtherapy for advanced disease. First, there is broad inter-est in evaluating existing drugs that affect other patho-genic pathways and comparing these directly to sorafe-nib. Second, studies are underway that are evaluatingvertical blockade, in which the same pathway is inter-rupted at different points by, for example, bevacizumab(an antibody to VEGF) and sorafenib (a small moleculetyrosine kinase inhibitor against VEGFR). The idea oftargeting the same pathway at several levels is appealingbecause it may lead to more complete blockade, blockfeedback loops, and have nonoverlapping resistance pat-terns.48 Horizontal blockade, in contrast, refers to theuse of different drugs that interrupt different signalingpathways, such as bevacizumab with erlotinib, whichtargets EGFR. Many of these combinations have pre-clinical evidence of synergy and/or block proposedresistance pathways seen in one of the drugs.49 Addi-tionally, blockade at different pathways may providefewer overlapping toxicities. Combinations of sorafenibwith chemotherapy are also being investigated, with anintergroup trial in the United States studying doxorubi-cin with sorafenib on the basis of phase II data.50
It is not clear which of these conceptualizations oftreatment will be more effective or whether consecu-tive sequencing of drugs will provide better efficacy incomparison with giving drugs simultaneously. Becauseof the importance of angiogenic signaling in HCC, itmay be that more complete blockade of this pathwaywill be particularly beneficial. There are data from aphase I study using sorafenib and bevacizumab to-gether that show a promising response rate of 59%,but at the cost of significant toxicity, including hand-foot syndrome, hypertension, and diarrhea.51 Thiscombination is currently being studied in a NationalCancer Institute–sponsored trial in HCC. It is alsoknown that responses can be seen through the sequen-tial use of a VEGFR tyrosine kinase inhibitor after thefailure of other antiangiogenic drugs in renal cell carci-noma, and this raises the question whether survivalmight be the same as (or better than) that with simul-taneous drug treatment with less toxicity.52,53
364 SIEGEL ET AL. HEPATOLOGY, July 2010

Data for the horizontal approach with targetedtherapies, although it is appealing conceptually, havebeen mixed so far in other cancer types. For instance,a single-arm phase II trial using bevacizumab and erlo-tinib in renal cell carcinoma looked promising, but asubsequent randomized phase II trial of bevacizumabwith or without erlotinib in this disease showed no sig-nificant clinical benefit with the addition of erloti-nib.54,55 In colorectal cancer, two large randomized tri-als used combinations of bevacizumab and anti-EGFRantibodies and showed significant toxicity and wors-ened outcomes in patients treated with both targetedagents simultaneously.56,57 In contrast, sequencingthese antibodies has been shown to provide clear sur-vival benefits in patients with metastatic colon can-cer.58 The phase II trial performed in HCC with beva-cizumab and erlotinib is encouraging, however, andhas been expanded into a larger multicenter study. Acareful evaluation of all these paradigms—verticalblockade, horizontal blockade, and sequential thera-pies—is needed to determine which options providethe best outcomes. These options will likely differaccording to the goals of therapy. For instance, in apatient who may be able to be downstaged prior toresection or transplantation, a rapid response rate maybe the most important endpoint, whereas for a meta-static patient, prolonged survival with minimal toxicitymay warrant different treatment options.New pathways are increasingly being examined as
possible targets for HCC treatment. These includeresistance pathways, apoptotic pathways, signal trans-duction pathways, and cell cycle pathways. One poten-tially promising approach involves targeting the FGFRpathway, which is thought to play a role in resistanceto VEGF blockade.59 Brivanib alanate is a dual inhibi-tor of VEGFR and FGFR tyrosine kinases. Brivanibhas shown preclinical activity in animal models60 andhas shown preliminary evidence of activity in HCCpatients who have progressed on previous antiangio-genic therapy.61 To test this hypothesis clinically, alarge randomized phase III trial is being conducted inwhich brivanib is being studied as second-line therapyin HCC patients who have progressed on sorafenib.Apoptosis pathways are also attractive targets for
modulation in anticancer therapies. Tumor necrosisfactor–related apoptosis-inducing ligand (TRAIL) ini-tiates apoptosis by joining two death receptors, deathreceptor 4 and death receptor 5. Akazawa and col-leagues62 have shown that in malignant liver cell lines,death receptor 5 undergoes endocytosis with traffickingto lysosomes and allows protease release into the cyto-sol and apoptosis. There are currently trials underway
that are using different TRAIL agonists with sorafenibin HCC.There is also a great deal of interest in examining
the IGFR inhibitors in HCC. Features of metabolicsyndrome, including diabetes, obesity, and insulin re-sistance, are related to both HCC development andmortality, and dysregulation of the IGF axis is seen inall of these disorders.63,64 Preclinical studies suggestthat blockade of the IGFR receptors block HCC cellgrowth, and at least 30% to 40% of HCCs overexpressinsulin-like growth factor 1 receptor (IGF1R).65-67
Culture models suggest that HCC cells may overcomeIGF1R via up-regulation of HER3, the main ligand ofEGFR, and this suggests the possible synergistic effectsof blocking both targets.67 Several companies aredeveloping IGF receptor antibodies, and phase II trialsusing these drugs in HCC are currently ongoing. Ta-ble 1 shows some of the targeted molecular therapiescurrently being tested in HCC.
Molecular Studies in HCC and theRole of Inflammation
Currently, there is no single molecular frameworkfor classifying all HCC, but much work is underwayto determine molecular predictors of outcome andresponse to therapies. Using HCC samples, Lee andThorgeirsson68 reported initial array data, clusteringtumors into two categories based on survival. Theyfound that genes associated with antiapoptosis and cellproliferation were more prevalent in tumors of patientswith poorer survival. They then found that HCCswith phenotypic markers of hepatic progenitor cellsalso had a worsened prognosis.69
Hoshida and colleagues70 have attempted to createunifying molecular subclasses of HCC incorporatingboth biological and clinical criteria. The group col-lected eight publicly available gene expression data setsand identified three robust subclasses of HCC. Thefirst subclass was associated with higher rates of recur-rence and more vascular invasion; molecularly, thesetumors exhibited activation of WNT signaling path-ways. Subclass 2 tumors were larger than the others,had the highest alpha-fetoprotein (AFP) levels, andoften exhibited AKT activation. Subclass 3 tumorstended to be smaller and were associated with a goodsurvival signature. Studies such as these point the waytoward novel targets for therapy and also better selec-tion of specific therapies for subtypes of HCC.By examining gene expression in liver tissue sur-
rounding tumors, Hoshida and colleagues71,72 were able
HEPATOLOGY, Vol. 52, No. 1, 2010 SIEGEL ET AL. 365

to show an association between a 132-gene profile, laterecurrence of tumors, and survival. This argues for afield effect and predicts that those with a more inflam-matory underlying liver are more prone to develop sec-ond primaries (confirmed genetically to be differentthan the primary tumors).Finally, molecular markers are also being examined
as possible predictors of response to therapy. Ji andcolleagues73 investigated micro-RNA patterns in 455resected HCC patients and found that expression ofmicro-RNA 26 was both predictive and prognostic,with lower expression being associated with responseto interferon in the adjuvant setting but lower overallsurvival. Expression of this micro-RNA was also linkedto inflammatory signaling cascades.Inflammatory signaling pathways also play a role in
HCC development and may ultimately yield chemo-prevention opportunities. For instance, Haybaeck andcolleagues74 found that the inflammatory cytokineslymphotoxin a and lymphotoxin b induced inflamma-tion and HCC in a mouse model, and inhibition ofthe lymphotoxin receptor in a transgenic mouse modelsuppressed HCC formation. These data raise the ques-tion whether antilymphotoxin agents (which arealready being studied in rheumatoid arthritis) may beexamined in the future as chemopreventives in patientsat risk for HCC.75
Novel Predictive and Prognostic Biomarkers
In addition to identifying molecular subtypes ofHCC, noninvasive biomarkers such as imaging tech-nologies and plasma markers that will not require tissuefor analysis will be crucial for tailoring HCC treatment.Functional imaging is one attractive way of assessingthe overall prognosis and response to therapy. Ratherthan evaluating the response on the basis of tumordiameters, the European Association for the Study ofthe Liver criteria have been proposed for assessingenhancement patterns of clinical responses from treat-ment rather than just tumor sizes.76 Similarly, for anti-angiogenic agents, DCE MRI has been studied as acorrelate of tumor response.8,20 All of these modalitiesrequire further study, standardization, and validation.Other peripheral biomarkers are beginning to be
evaluated as predictors of outcome. Chan and col-leagues77 evaluated serum AFP levels in 188 patientsrandomized to either doxorubicin or a combination ofolder chemotherapies called PIAF (doxorubicin, cispla-tin, 5-FU, and interferon alpha). They found that of117 patients who had elevated AFP levels (>20 lg/L),47 patients had an AFP response defined as a >20%decrease in AFP after two cycles of chemotherapy. AnAFP response was independently associated with over-all survival in a multivariable model. It is unclearwhether the AFP response will be useful as a predictiveor prognostic marker for novel targeted therapies.77
Similarly, plasma biomarkers such as VEGF, fibroblastgrowth factor, interleukin-6, and circulating endothe-lial cells are being studied as novel biomarkers ofresponse to antiangiogenic drugs. To date, none ofthese has been conclusively validated.
Summary
There are several challenges facing the hepatology,transplant, and oncological community in the treat-ment of HCC. First, additional work is required toclarify the molecular pathogenesis of HCC and iden-tify key targets for therapeutic intervention. The devel-opment of sorafenib underscores the potential for tar-geting additional receptors and other mediators inoncogenic pathways.Second, we need to ensure that various therapies are
studied in combination with each other and also insuccession. Specifically, the role of sorafenib as adjunc-tive therapy needs to be evaluated both before and af-ter surgery and with locoregional therapies.Third, study design needs to be critically evaluated,
particularly in the age of molecular therapies. As dis-cussed previously, the American Association for the
Table 1. Selected Targeted Therapies for HCC with TrialsUnderway
Mechanism Target Drug
Angiogenesis VEGFR (1-3) Sorafenib, sunitinib,
brivanib, linifanib, BIBF 1120,
AZD 2171 (cediranib),
TSU68, E7080
VEGF Bevacizumab
FGFR Brivanib, BIBF 1120,
TSU68
PDGFR Sunitinib, sorafenib
Tie-2 Bay 73-4506, AMG 386
Signal transduction EGFR Erlotinib, cetuximab
IGFR IMC-A12, cixutumumab,
BIIB022
mTOR Rapamycin, everolimus,
temsirolimus, AZD 8055
c-MET ARQ 197
c-KIT Dasatinib
MEK AZD 6244
Apoptosis TRAIL Mapatumumab, CS-1008
Chromatin remodeling HDAC PDX-101, 4SC 201
Cell migration SRC Dasatinib
Abbreviations: c-MET, mesenchymal epithelial transition factor; HDAC, histone
deacetylase; MEK, mitogen-activated protein kinase kinase; SRC, sarcoma viral
oncogene homolog; Tie-2, tyrosine kinase with immunoglobulin-like and EGF-
like domains 2.
366 SIEGEL ET AL. HEPATOLOGY, July 2010

Study of Liver Diseases has recently convened a panelof multidisciplinary experts to comment on the designof clinical trials for HCC. This group suggested thatrandomized phase II trials designed to determine theantitumor activity of a particular agent be encouragedand that the time to progression, not the responserate, might be a more useful endpoint in these trials.This thinking is underscored by data showing that sur-vival advantages can be seen in the absence of large tu-mor response rates and that response rates may notcapture the benefit of a molecular therapy as theywould with an intervention such as chemoemboliza-tion or radiofrequency ablation.17
Finally, because transplantation remains the primarymethod of treating HCC and the underlying liver dis-ease in the West, every effort needs to be made tostreamline the process of referring eligible HCCpatients to transplant centers.78
Further study must also focus on identifying predictiveand prognostic biomarkers to guide our use of this newarmamentarium against HCC. In addition to improvedtreatment modalities, improved methods for HCC sur-veillance in at-risk populations are critically important.Despite their deficiencies, surveillance programs havebeen proven to improve survival in those with HCC.The treatment of HCC is complicated by the wide
variety of underlying liver diseases associated with thedevelopment of this tumor as well as the various thera-peutic modalities available to patients. The identifica-tion of sorafenib and the survival benefit that it confersto patients with unresectable HCC represents a newera in the treatment of HCC. Studies are underway toassess additional molecular targets and to determineoptimal combinations and sequencing of treatmentmodalities to maximize patient outcome in this new,rapidly shifting landscape.
Acknowledgment: The authors thank Dr. PaulBerk, Dr. Gregory Gores, and Dr. Balazs Halmos fortheir careful critical readings of the manuscript and fortheir mentorship.
References1. Parkin DM. Global cancer statistics in the year 2000. Lancet Oncol
2001;2:533-543.
2. El-Serag HB, Mason AC. Rising incidence of hepatocellular carcinomain the United States. N Engl J Med 1999;340:745-750.
3. El-Serag HB, Rudolph KL. Hepatocellular carcinoma: epidemiologyand molecular carcinogenesis. Gastroenterology 2007;132:2557-2576.
4. Thorgeirsson SS, Grisham JW. Molecular pathogenesis of human hepa-tocellular carcinoma. Nat Genet 2002;31:339-346.
5. Fukutomi T, Zhou Y, Kawai S, Eguchi H, Wands JR, Li J. Hepatitis Cvirus core protein stimulates hepatocyte growth: correlation with upreg-ulation of wnt-1 expression. HEPATOLOGY 2005;41:1096-1105.
6. Yoshiji H, Kuriyama S, Yoshii J, Yamazaki M, Kikukawa M, TsujinoueH, et al. Vascular endothelial growth factor tightly regulates in vivo de-velopment of murine hepatocellular carcinoma cells. HEPATOLOGY 1998;28:1489-1496.
7. Moon WS, Rhyu KH, Kang MJ, Lee DG, Yu HC, Yeum JH, et al.Overexpression of VEGF and angiopoietin 2: a key to high vascularityof hepatocellular carcinoma? Mod Pathol 2003;16:552-557.
8. Siegel AB, Cohen EI, Ocean A, Lehrer D, Goldenberg A, Knox JJ,et al. Phase II trial evaluating the clinical and biologic effects of bevaci-zumab in unresectable hepatocellular carcinoma. J Clin Oncol 2008;26:2992-2998.
9. Llovet JM, Ricci S, Mazzaferro V, Hilgard P, Gane E, Blanc JF, et al.Sorafenib in advanced hepatocellular carcinoma. N Engl J Med 2008;359:378-390.
10. Cheng AL, Kang YK, Chen Z, Tsao CJ, Qin S, Kim JS, et al. Efficacyand safety of sorafenib in patients in the Asia-Pacific region withadvanced hepatocellular carcinoma: a phase III randomised, double-blind, placebo-controlled trial. Lancet Oncol 2009;10:25-34.
11. Pinter M, Sieghart W, Graziadei I, Vogel W, Maieron A, Konigsberg R,et al. Sorafenib in unresectable hepatocellular carcinoma from mild toadvanced stage liver cirrhosis. Oncologist 2009;14:70-76.
12. Abou-Alfa GK, Schwartz L, Ricci S, Amadori D, Santoro A, Figer A,et al. Phase II study of sorafenib in patients with advanced hepatocellu-lar carcinoma. J Clin Oncol 2006;24:4293-4300.
13. Miller AA, Murry DJ, Owzar K, Hollis DR, Kennedy EB, Abou-AlfaG, et al. Phase I and pharmacokinetic study of sorafenib in patientswith hepatic or renal dysfunction: CALGB 60301. J Clin Oncol 2009;27:1800-1805.
14. Llovet J. Biomarkers predicting outcome in patients with hepatocellularcarcinoma: results from random biopsies from the SHARP trial. Pre-sented at: 59th Annual Meeting of the American Association for theStudy of Liver Diseases; October 2008; San Francisco, CA.
15. Hahn OM, Yang C, Medved M, Karczmar G, Kistner E, Karrison T,et al. Dynamic contrast-enhanced magnetic resonance imaging pharma-codynamic biomarker study of sorafenib in metastatic renal carcinoma.J Clin Oncol 2008;26:4572-4578.
16. Willett CG, Boucher Y, di Tomaso E, Duda DG, Munn LL, Tong RT,et al. Direct evidence that the VEGF-specific antibody bevacizumab hasantivascular effects in human rectal cancer. Nat Med 2004;10:145-147.
17. Llovet JM, Di Bisceglie AM, Bruix J, Kramer BS, Lencioni R, ZhuAX, et al. Design and endpoints of clinical trials in hepatocellular carci-noma. J Natl Cancer Inst 2008;100:698-711.
18. Zhu AX, Blaszkowsky LS, Ryan DP, Clark JW, Muzikansky A, HorganK, et al. Phase II study of gemcitabine and oxaliplatin in combinationwith bevacizumab in patients with advanced hepatocellular carcinoma.J Clin Oncol 2006;24:1898-1903.
19. Louafi S, Boige V, Ducreux M, Bonyhay L, Mansourbakht T, de BaereT, et al. Gemcitabine plus oxaliplatin (GEMOX) in patients withadvanced hepatocellular carcinoma (HCC): results of a phase II study.Cancer 2007;109:1384-1390.
20. Zhu AX, Sahani DV, Duda DG, di Tomaso E, Ancukiewicz M, Cata-lano OA, et al. Efficacy, safety, and potential biomarkers of sunitinibmonotherapy in advanced hepatocellular carcinoma: a phase II study.J Clin Oncol 2009;27:3027-3035.
21. Faivre S, Raymond E, Boucher E, Douillard J, Lim HY, Kim JS, et al.Safety and efficacy of sunitinib in patients with advanced hepatocellularcarcinoma: an open-label, multicentre, phase II study. Lancet Oncol2009;10:794-800.
22. Van Cutsem E, Kohne CH, Hitre E, Zaluski J, Chang Chien CR,Makhson A, et al. Cetuximab and chemotherapy as initial treatmentfor metastatic colorectal cancer. N Engl J Med 2009;360:1408-1417.
23. Vermorken JB, Mesia R, Rivera F, Remenar E, Kawecki A, Rottey S,et al. Platinum-based chemotherapy plus cetuximab in head and neckcancer. N Engl J Med 2008;359:1116-1127.
24. Van Cutsem E, Peeters M, Siena S, Humblet Y, Hendlisz A, Neyns B,et al. Open-label phase III trial of panitumumab plus best supportivecare compared with best supportive care alone in patients with
HEPATOLOGY, Vol. 52, No. 1, 2010 SIEGEL ET AL. 367

chemotherapy-refractory metastatic colorectal cancer. J Clin Oncol2007;25:1658-1664.
25. Lynch TJ, Bell DW, Sordella R, Gurubhagavatula S, Okimoto RA,Brannigan BW, et al. Activating mutations in the epidermal growth fac-tor receptor underlying responsiveness of non-small-cell lung cancer togefitinib. N Engl J Med 2004;350:2129-2139.
26. Moore MJ, Goldstein D, Hamm J, Figer A, Hecht JR, Gallinger S,et al. Erlotinib plus gemcitabine compared with gemcitabine alone inpatients with advanced pancreatic cancer: a phase III trial of theNational Cancer Institute of Canada Clinical Trials Group. J ClinOncol 2007;25:1960-1966.
27. Buckley AF, Burgart LJ, Sahai V, Kakar S. Epidermal growth factor re-ceptor expression and gene copy number in conventional hepatocellularcarcinoma. Am J Clin Pathol 2008;129:245-251.
28. Schiffer E, Housset C, Cacheux W, Wendum D, Desbois-Mouthon C,Rey C, et al. Gefitinib, an EGFR inhibitor, prevents hepatocellular car-cinoma development in the rat liver with cirrhosis. HEPATOLOGY 2005;41:307-314.
29. Altimari A, Fiorentino M, Gabusi E, Gruppioni E, Corti B, D’ErricoA, et al. Investigation of ErbB1 and ErbB2 expression for therapeutictargeting in primary liver tumours. Dig Liver Dis 2003;35:332-338.
30. Nakopoulou L, Stefanaki K, Filaktopoulos D, Giannopoulou I. C-erb-B-2 oncoprotein and epidermal growth factor receptor in human hepa-tocellular carcinoma: an immunohistochemical study. Histol Histopa-thol 1994;9:677-682.
31. Philip PA, Mahoney MR, Allmer C, Thomas J, Pitot HC, Kim G,et al. Phase II study of erlotinib (OSI-774) in patients with advancedhepatocellular cancer. J Clin Oncol 2005;23:6657-6663.
32. Thomas MB, Chadha R, Glover K, Wang X, Morris J, Brown T, et al.Phase 2 study of erlotinib in patients with unresectable hepatocellularcarcinoma. Cancer 2007;110:1059-1067.
33. Thomas MB, Morris JS, Chadha R, Iwasaki M, Kaur H, Lin E, et al.Phase II trial of the combination of bevacizumab and erlotinib inpatients who have advanced hepatocellular carcinoma. J Clin Oncol2009;27:843-850.
34. Zhu AX, Stuart K, Blaszkowsky LS, Muzikansky A, Reitberg DP, ClarkJW, et al. Phase 2 study of cetuximab in patients with advanced hepa-tocellular carcinoma. Cancer 2007;110:581-589.
35. Asnacios A, Fartoux L, Romano O, Tesmoingt C, Louafi SS, Mansou-bakht T, et al. Gemcitabine plus oxaliplatin (GEMOX) combined withcetuximab in patients with progressive advanced stage hepatocellularcarcinoma: results of a multicenter phase 2 study. Cancer 2008;112:2733-2739.
36. Bekaii-Saab TS, Roda JM, Guenterberg KD, Ramaswamy B, YoungDC, Ferketich AK, et al. A phase I trial of paclitaxel and trastuzumabin combination with interleukin-12 in patients with HER2/neu-express-ing malignancies. Mol Cancer Ther 2009;8:2983-2991.
37. Su M, Lien H, Jeng Y. Absence of epidermal growth factor receptorexon 18-21 mutation in hepatocellular carcinoma. Cancer Lett 2005;224:117-121.
38. Karapetis CS, Khambata-Ford S, Jonker DJ, O’Callaghan CJ, Tu D,Tebbutt NC, et al. K-ras mutations and benefit from cetuximab inadvanced colorectal cancer. N Engl J Med 2008;359:1757-1765.
39. Villanueva A, Chiang DY, Newell P, Peix J, Thung S, Alsinet C, et al.Pivotal role of mTOR signaling in hepatocellular carcinoma. Gastroen-terology 2008;135:1972-1983.
40. Heuer M, Benko T, Cicinnati VR, Kaiser GM, Sotiropoulos GC, BabaHA, et al. Effect of low-dose rapamycin on tumor growth in twohuman hepatocellular cancer cell lines. Transplant Proc 2009;41:359-365.
41. Toso C, Meeberg GA, Bigam DL, Oberholzer J, Shapiro AM, Gut-freund K, et al. De novo sirolimus-based immunosuppression after livertransplantation for hepatocellular carcinoma: long-term outcomes andside effects. Transplantation 2007;83:1162-1168.
42. Nocera A, Andorno E, Tagliamacco A, Morelli N, Bottino G, Ravaz-zoni F, et al. Sirolimus therapy in liver transplant patients: an initial ex-perience at a single center. Transplant Proc 2008;40:1950-1952.
43. Zhou J, Wang Z, Wu ZQ, Qiu SJ, Yu Y, Huang XW, et al. Sirolimus-based immunosuppression therapy in liver transplantation for patientswith hepatocellular carcinoma exceeding the Milan criteria. TransplantProc 2008;40:3548-3553.
44. Rizell M, Andersson M, Cahlin C, Hafstrom L, Olausson M, LindnerP. Effects of the mTOR inhibitor sirolimus in patients with hepatocel-lular and cholangiocellular cancer. Int J Clin Oncol 2008;13:66-70.
45. Huynh H, Chow KP, Soo KC, Toh HC, Choo SP, Foo KF, et al.RAD001 (everolimus) inhibits tumor growth in xenograft models ofhuman hepatocellular carcinoma. J Cell Mol Med 2009;13:1371-1380.
46. Huynh H, Ngo VC, Koong HN, Poon D, Choo SP, Thng CH, et al.Sorafenib and rapamycin induce growth suppression in mouse modelsof hepatocellular carcinoma. J Cell Mol Med 2009;13:2673-2683.
47. Arnault JP, Wechsler J, Escudier B, Spatz A, Tomasic G, Sibaud V,et al. Keratoacanthomas and squamous cell carcinomas in patientsreceiving sorafenib. J Clin Oncol 2009;27:e59-e61.
48. Sosman JA, Puzanov I, Atkins MB. Opportunities and obstacles tocombination targeted therapy in renal cell cancer. Clin Cancer Res2007;13:764s-769s.
49. Camp ER, Summy J, Bauer TW, Liu W, Gallick GE, Ellis LM. Molec-ular mechanisms of resistance to therapies targeting the epidermalgrowth factor receptor. Clin Cancer Res 2005;11:397-405.
50. Abou-Alfa G, Johnson J, Knox JJ, Davidenko I, Lacava J, Leung T,et al. Final results from a phase II randomized, double-blind study ofsorafenib plus doxorubicin versus placebo plus doxorubicin in patientswith advanced hepatocellular carcinoma. Paper presented at: Gastroin-testinal Cancers Symposium; January 2008; Orlando, FL.
51. Azad NS, Posadas EM, Kwitkowski VE, Steinberg SM, Jain L, Annun-ziata CM, et al. Combination targeted therapy with sorafenib and beva-cizumab results in enhanced toxicity and antitumor activity. J ClinOncol 2008;26:3709-3714.
52. Rini BI, Michaelson MD, Rosenberg JE, Bukowski RM, Sosman JA,Stadler WM, et al. Antitumor activity and biomarker analysis of suniti-nib in patients with bevacizumab-refractory metastatic renal cell carci-noma. J Clin Oncol 2008;26:3743-3748.
53. Tamaskar I, Garcia JA, Elson P, Wood L, Mekhail T, Dreicer R, et al.Antitumor effects of sunitinib or sorafenib in patients with metastaticrenal cell carcinoma who received prior antiangiogenic therapy. J Urol2008;179:81-86.
54. Hainsworth JD, Spigel DR, Farley C, Thompson DS, Shipley DL,Greco FA. Phase II trial of bevacizumab and erlotinib in carcinomas ofunknown primary site: the Minnie Pearl Cancer Research Network.J Clin Oncol 2007;25:1747-1752.
55. Bukowski RM, Kabbinavar FF, Figlin RA, Flaherty K, Srinivas S,Vaishampayan U, et al. Randomized phase II study of erlotinib com-bined with bevacizumab compared with bevacizumab alone in meta-static renal cell cancer. J Clin Oncol 2007;25:4536-4541.
56. Hecht JR, Mitchell E, Chidiac T, Scroggin C, Hagenstad C, Spigel D,et al. A randomized phase IIIB trial of chemotherapy, bevacizumab,and panitumumab compared with chemotherapy and bevacizumabalone for metastatic colorectal cancer. J Clin Oncol 2009;27:672-680.
57. Tol J, Koopman M, Cats A, Rodenburg CJ, Creemers GJ, SchramaJG, et al. Chemotherapy, bevacizumab, and cetuximab in metastaticcolorectal cancer. N Engl J Med 2009;360:563-572.
58. Meyerhardt JA, Mayer RJ. Systemic therapy for colorectal cancer.N Engl J Med 2005;352:476-487.
59. Casanovas O, Hicklin DJ, Bergers G, Hanahan D. Drug resistance byevasion of antiangiogenic targeting of VEGF signaling in late-stage pan-creatic islet tumors. Cancer Cell 2005;8:299-309.
60. Huynh H, Ngo VC, Fargnoli J, Ayers M, Soo KC, Koong HN, et al.Brivanib alaninate, a dual inhibitor of vascular endothelial growth fac-tor receptor and fibroblast growth factor receptor tyrosine kinases,induces growth inhibition in mouse models of human hepatocellularcarcinoma. Clin Cancer Res 2008;14:6146-6153.
61. Raoul J, Finn R, Kang Y, Park J, Harris R, Coric V, et al. An open-labelphase II study of first- and second-line treatment with brivanib in patientswith hepatocellular carcinoma (HCC). J Clin Oncol 2009;27(Suppl):15S.
368 SIEGEL ET AL. HEPATOLOGY, July 2010

62. Akazawa Y, Mott JL, Bronk SF, Werneburg NW, Kahraman A, Guic-ciardi ME, et al. Death receptor 5 internalization is required for lysoso-mal permeabilization by TRAIL in malignant liver cell lines.Gastroenterology 2009;136:2365-2376.
63. Scharf JG, Braulke T. The role of the IGF axis in hepatocarcinogenesis.Horm Metab Res 2003;35:685-693.
64. Siegel AB, Zhu AX. Metabolic syndrome and hepatocellular carcinoma:two growing epidemics with a potential link. Cancer 2009;115:5651-5661.
65. Hopfner M, Huether A, Sutter AP, Baradari V, Schuppan D, ScherublH. Blockade of IGF-1 receptor tyrosine kinase has antineoplastic effectsin hepatocellular carcinoma cells. Biochem Pharmacol 2006;71:1435-1448.
66. Cantarini MC, de la Monte SM, Pang M, Tong M, D’Errico A, Trevi-sani F, et al. Aspartyl-asparagyl beta hydroxylase over-expression inhuman hepatoma is linked to activation of insulin-like growth factorand notch signaling mechanisms. HEPATOLOGY 2006;44:446-457.
67. Desbois-Mouthon C, Baron A, Blivet-Van Eggelpoel MJ, Fartoux L,Venot C, Bladt F, et al. Insulin-like growth factor-1 receptor inhibitioninduces a resistance mechanism via the epidermal growth factor recep-tor/HER3/AKT signaling pathway: rational basis for cotargeting insu-lin-like growth factor-1 receptor and epidermal growth factor receptorin hepatocellular carcinoma. Clin Cancer Res 2009;15:5445-5456.
68. Lee JS, Thorgeirsson SS. Genome-scale profiling of gene expression inhepatocellular carcinoma: classification, survival prediction, and identifi-cation of therapeutic targets. Gastroenterology 2004;127:S51-S55.
69. Lee JS, Heo J, Libbrecht L, Chu IS, Kaposi-Novak P, Calvisi DF, et al.A novel prognostic subtype of human hepatocellular carcinoma derivedfrom hepatic progenitor cells. Nat Med 2006;12:410-416.
70. Hoshida Y, Nijman SM, Kobayashi M, Chan JA, Brunet JP, ChiangDY, et al. Integrative transcriptome analysis reveals common molecular
subclasses of human hepatocellular carcinoma. Cancer Res 2009;69:7385-7392.
71. Hoshida Y, Villanueva A, Kobayashi M, Peix J, Chiang DY, CamargoA, et al. Gene expression in fixed tissues and outcome in hepatocellularcarcinoma. N Engl J Med 2008;359:1995-2004.
72. Hoshida Y, Villanueva A, Llovet JM. Molecular profiling to predict he-patocellular carcinoma outcome. Expert Rev Gastroenterol Hepatol2009;3:101-103.
73. Ji J, Shi J, Budhu A, Yu Z, Forgues M, Roessler S, et al. MicroRNAexpression, survival, and response to interferon in liver cancer. N EnglJ Med 2009;361:1437-1447.
74. Haybaeck J, Zeller N, Wolf MJ, Weber A, Wagner U, Kurrer MO,et al. A lymphotoxin-driven pathway to hepatocellular carcinoma. Can-cer Cell 2009;16:295-308.
75. Villanueva A, Savic R, Llovet JM. Lymphotoxins: new targets for hepa-tocellular carcinoma. Cancer Cell 2009;16:272-273.
76. Bruix J, Sherman M, Llovet JM, Beaugrand M, Lencioni R, BurroughsAK, et al. Clinical management of hepatocellular carcinoma. Conclu-sions of the Barcelona-2000 EASL conference. European Associationfor the Study of the Liver. J Hepatol 2001;35:421-430.
77. Chan SL, Mo FK, Johnson PJ, Hui EP, Ma BB, Ho WM, et al. Newutility of an old marker: serial alpha-fetoprotein measurement in pre-dicting radiologic response and survival of patients with hepatocellularcarcinoma undergoing systemic chemotherapy. J Clin Oncol 2009;27:446-452.
78. Siegel AB, McBride RB, El-Serag HB, Hershman DL, Brown RS Jr,Renz JF, et al. Racial disparities in utilization of liver transplantationfor hepatocellular carcinoma in the United States, 1998-2002. Am JGastroenterol 2008;103:120-127.
HEPATOLOGY, Vol. 52, No. 1, 2010 SIEGEL ET AL. 369