Embed Size (px)
Citation preview

www.elsevier.com/locate/jpedsurg
Journal of Pediatric Surgery (2009) 44, 2037–2042
Pediatric surgical images
Sonographic evaluation of gastrointestinal obstruction ininfants: a pictorial essayPraveen Maheshwari⁎, Abdussalam Abograra, Omran Shamam
Department of Radiology, Tripoli Medical Center, Tripoli, Libya
Received 1 April 2009; revised 9 May 2009; accepted 11 May 2009
C
0d
Key words:USG;Gastrointestinalobstruction;
Infants
Abstract Traditionally, gastrointestinal contrast studies have been the mainstay of evaluating infantilegastrointestinal problems. Because of technological advancements, good ultrasonography (USG) machinescan provide high-resolution images with graphic anatomical clarity, especially in infants and children andthus change the traditional diagnostic trends. In this article, we illustrate the USG appearances of variouscauses of gastrointestinal obstruction in infants and discuss the role of USG in their evaluation.© 2009 Elsevier Inc. All rights reserved.
Vomiting is the first presenting feature of upper gastro-intestinal (GI) obstructions. It can be bilious or nonbilious.Common causes of nonbilious vomiting in infants includegastroesophageal reflux (GER) and hypertrophic pyloricstenosis. Patients with bilious vomiting may have anobstruction in the duodenum distal to the ampulla of Vateror the obstruction may be in small bowel or large bowel.Appendicitis and Meckel's diverticulum are rare causes ofbilious vomiting in infants. Lower GI obstructions presentmainly with constipation, and vomiting may be a subsequentfeature. In this article, we illustrate the USG appearances ofvarious causes of gastrointestinal obstruction in infants anddiscuss the role of USG in their evaluation.
1. Gastroesophageal reflux
Some infants reflux forcefully or in large amounts, and itcan be clinically difficult to distinguish pure GER from GIobstruction. Ultrasonography can be used to rule out GI
⁎ Corresponding author. A-10, Century Staff Qts., P.B. Marg, Near T.V.enter, Worli, Mumbai, 400030, India. Tel.: + 91 22 24921299.E-mail address: [email protected] (P. Maheshwari).
022-3468/$ – see front matter © 2009 Elsevier Inc. All rights reserved.oi:10.1016/j.jpedsurg.2009.05.019
obstruction or detect as a primary diagnosis, GER. Bariumstudy, scintigraphy, endoscopy, and pH monitoring havebeen used as diagnostic tests in GER [1]. However, USG canbe used as a single and adequate diagnostic test for GER.Ultrasonographic diagnosis of GER is based on the length ofintraabdominal esophagus and visualization of cephaladpassage of gastric contents in the esophagus during a 10-minute period [2] (Fig. 1).
2. Congenital hypertrophic pyloric stenosis
Congenital hypertrophic pyloric stenosis (CHPS) ischaracterized by hypertrophy of circular smooth muscle ofthe pylorus. Ultrasonography is the primary imaging methodfor CHPS and has generally replaced the contrast study as thefirst-line diagnostic test. An antropyloric muscle thickness ofmore than 3 mm is considered to be diagnostic of CHPS.Muscle thickness of less than 2 mm is unequivocally normaland muscle thickness between 2 and 3 mm is abnormal butnot specifically diagnostic of pyloric stenosis. Sonographicappearance of pylorospasm can overlap that of pyloricstenosis. However, pylorospasm shows considerable

Fig. 1 Gastroesophageal reflux. A, Longitudinal sonogram ofgastroesophageal junction showing reflux of gastric fluid in theesophagus. B, Gastroesophageal junction in a healthy subject.Arrow points at gastroesophageal junction.
2038 P. Maheshwari et al.
variation in thickness and image appearance for a periodduring the study [3]. Ultrasonography for CHPS can beperformed accurately in a very short time frame with anaccuracy approaching 100% [4]. Inadequate distension ofgastric antrum with fluid can result in a contracted antrumand may result in the appearance of a false impression ofthickened smooth muscle. Muscle thickness should bemeasured in true cross section because a tangential viewcan give a false interpretation of increased thickness (Fig. 2).
Fig. 2 Congenital hypertrophic pyloric stenosis. Sonogramdepicting thick-walled pylorus (arrow) in longitudinal section (A)and cross section (B).
3. Duodenal obstruction
Neonates showing evidence of complete duodenal obstruc-tion on plain abdominal radiographs generally do not requireany further radiologic investigation. The classic radiographicfinding of the “double bubble sign,” with no gas distally,suggests the diagnosis of complete duodenal obstruction mostlikely because of duodenal atresia. Partial duodenal obstruc-
tion can be because of duodenal web, duodenal stenosis,malrotation (and its associated features such as midgutvolvulus, Ladd's bands), preduodenal portal vein, duplicationcyst, and annular pancreas [5]. Ultrasonography can be veryhelpful in differentiating between these conditions. Ultra-sonography is best performed when patient presents with anacute obstruction. With the insertion of nasogastric tube anddrainage of gastric contents, the classical signs of obstructionmay become less evident on USG because of lack of a properacoustic window, gaseous artifacts, and partial relief ofobstruction. A fluid-filled stomach might be required to avoida false-negative scan (Figs. 3, 4).
4. Malrotation
Sonographic diagnosis of malrotation is based ondemonstrating a reversal of the normal relationship of thesuperior mesenteric artery (SMA) and superior mesentericvein (SMV). The possibility of malrotation must be

Fig. 3 Duodenal stenosis. A, Transverse sonogram depicting fluid-filled distended second part of duodenum (Du) with gradual tapering.B, Upper GI contrast study showing tapering of distended second partof duodenum and stenosis (arrow) of the third part of duodenum.
2039Sonographic evaluation of GI obstruction in infants
considered whenever inversion of SMA and SMV is noted.However, a normal anatomy of the SMA and SMV does notrule out malrotation, and therefore, an upper GI contraststudy remains the gold standard about the diagnosis of thiscondition [6] (Fig. 5).
Fig. 4 Duodenal web. A, Transverse sonogram depicting gasdistended tapered second part of duodenum with echogenic gasbubbles seen passing through a narrow channel (arrow). B, UpperGI contrast study depicting distended second part of duodenum,with a membranous defect (arrow) in the third part.
5. Midgut volvulus
Midgut volvulus occurs when the bowel twists around theSMA. This leads to a whirlpool-like appearance on cross-sectional imaging. The SMV and its tributaries wrap aroundthe SMA in a clockwise direction as a result of the volvulus.The direction of the volvulus should be clockwise because acounterclockwise whirlpool can be seen in patients withenteritis. At some institutions, ultrasonographic diagnosis ofvolvulus suffices for the need to proceed to surgery, but someinstitutions require confirmation with an upper GI contrast
examination [7]. In the study of Shimanuki et al [8],sensitivity, specificity, and positive predictive value ofclockwise whirlpool sign for midgut volvulus were 92%,100%, and 100%, respectively. Midgut volvulus can alsoappear beyond the neonatal period and with a variety ofclinical presentations, making the clinical diagnosis in suchpatients very difficult. Ultrasonography can correctly suggestthe diagnosis in such atypical clinical presentations ofmidgut volvulus [9] (Fig. 6).
6. Distal small bowel or large bowel obstruction
In distal small bowel or large bowel obstruction, USGdemonstrates multiple fluid-filled bowel loops all over theabdomen. Sonography may be useful in differentiatingmeconium ileus and ileal atresia. In meconium, ileus bowel
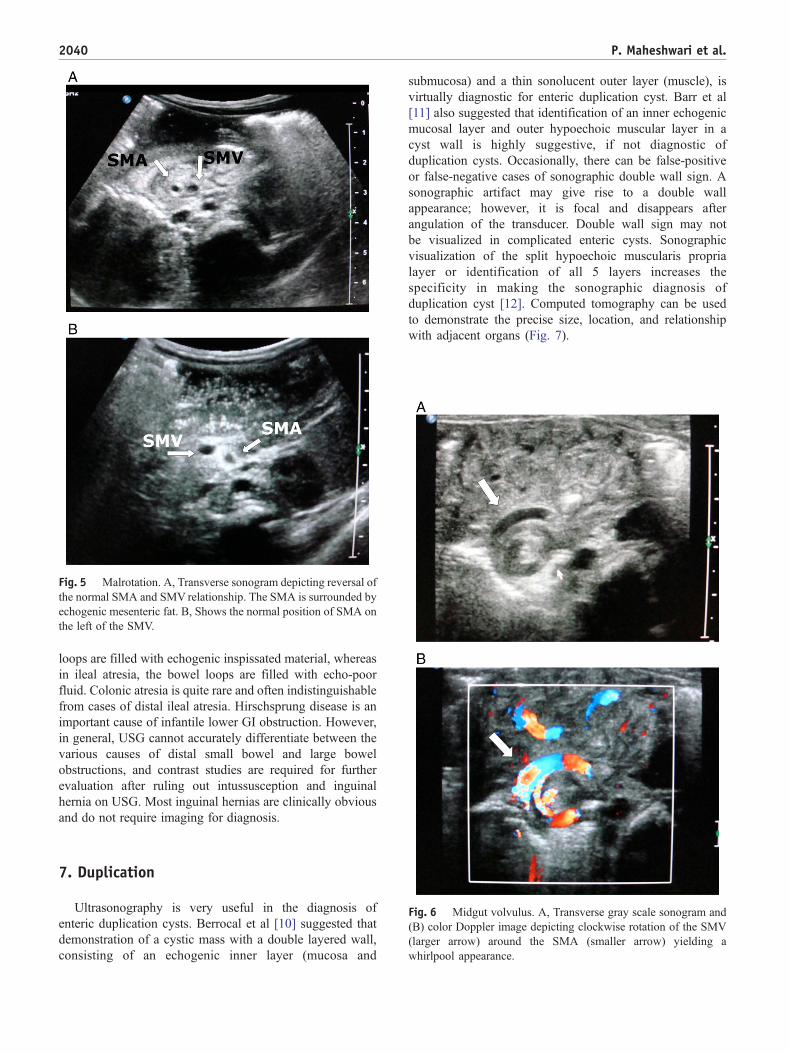
Fig. 5 Malrotation. A, Transverse sonogram depicting reversal ofthe normal SMA and SMV relationship. The SMA is surrounded byechogenic mesenteric fat. B, Shows the normal position of SMA onthe left of the SMV.
2040 P. Maheshwari et al.
loops are filled with echogenic inspissated material, whereasin ileal atresia, the bowel loops are filled with echo-poorfluid. Colonic atresia is quite rare and often indistinguishablefrom cases of distal ileal atresia. Hirschsprung disease is animportant cause of infantile lower GI obstruction. However,in general, USG cannot accurately differentiate between thevarious causes of distal small bowel and large bowelobstructions, and contrast studies are required for furtherevaluation after ruling out intussusception and inguinalhernia on USG. Most inguinal hernias are clinically obviousand do not require imaging for diagnosis.
Fig. 6 Midgut volvulus. A, Transverse gray scale sonogram and(B) color Doppler image depicting clockwise rotation of the SMV(larger arrow) around the SMA (smaller arrow) yielding awhirlpool appearance.
7. Duplication
Ultrasonography is very useful in the diagnosis ofenteric duplication cysts. Berrocal et al [10] suggested thatdemonstration of a cystic mass with a double layered wall,consisting of an echogenic inner layer (mucosa and
submucosa) and a thin sonolucent outer layer (muscle), isvirtually diagnostic for enteric duplication cyst. Barr et al[11] also suggested that identification of an inner echogenicmucosal layer and outer hypoechoic muscular layer in acyst wall is highly suggestive, if not diagnostic ofduplication cysts. Occasionally, there can be false-positiveor false-negative cases of sonographic double wall sign. Asonographic artifact may give rise to a double wallappearance; however, it is focal and disappears afterangulation of the transducer. Double wall sign may notbe visualized in complicated enteric cysts. Sonographicvisualization of the split hypoechoic muscularis proprialayer or identification of all 5 layers increases thespecificity in making the sonographic diagnosis ofduplication cyst [12]. Computed tomography can be usedto demonstrate the precise size, location, and relationshipwith adjacent organs (Fig. 7).

2041Sonographic evaluation of GI obstruction in infants
8. Intussusception
Ultrasonography is a reliable imaging tool for rapid andaccurate diagnosis of intussusception. It is seen as a thickhypoechoic rim and hyperechoic core (doughnut sign) intransverse section and a central elongated hyperechoic coresurrounded by hypoechoic rim on both sides (sandwich sign)in longitudinal sections. Occasionally, feces in the colon maymimic intussusception. Verschelden et al [13] demonstrated asensitivity of 100%, specificity of 88%, and a negativepredictive value of 100% in their study (Fig. 8).
9. Conclusion
Ultrasonography is a noninvasive, rapid, and very usefulmodality in the evaluation of gastrointestinal obstruction ininfants. Present-day advanced ultrasound machines provide
Fig. 7 Enteric duplication. A, USG showing gut signature of thecyst wall (inner hyperechoic mucosal layer and outer hypoechoicmuscular layer). B, Multiplanar reconstructed computed tomo-graphic image of the same patient.
Fig. 8 Intussusception. A, Transverse gray scale sonogramdepicting the doughnut sign of intussusception (thick hypoechoicouter rim and hyperechoic core). Intussusceptum is marked as“I.” B, Longitudinal section showing sandwich sign (centralelongated hyperechoic core surrounded by hypoechoic rim onboth sides).
excellent anatomical details in infants. Ultrasonography cansuggest the correct diagnosis or significantly narrow downthe differential diagnosis and guide further appropriateevaluation, thus, reducing radiation exposure in pediatricpatients. The availability of modern ultrasound technologyand equipment (machine) and skilled sonologists (uservariability) are the main limiting factors.
References
[1] Mehdizadeh M, Zandie F, Janati J, et al. A comparison between thediagnostic value of sonography vs barium swallow in gastroesopha-geal reflux in children. Iran J Radiol 2003:147-9.
[2] Koumanidou C, Vakaki M, Pitsoulakis G, et al. Sonographicmeasurement of the abdominal esophagus length in infancy: adiagnostic tool for gastroesophageal reflux. AJR 2004;183:801-7.

2042 P. Maheshwari et al.
[3] Gupta AK, Guglani B. Imaging of congenital anomalies of thegastrointestinal tract. Indian J Pediatr 2005;72(5):403-14.
[4] Schulman H. Infantile hypertrophic pyloric stenosis. Radiology 2003;227:319-31.
[5] Berrocal T, Torres I, Gutierrez J, et al. Congenital anomalies of theupper gastrointestinal tract. Radiographics 1999;19(4):855-72.
[6] Zerin JM, DiPietro MA. Superior mesenteric vascular anatomy at USin patients with surgically proved malrotation of the midgut. Radiology1992;183:693-4.
[7] Epelman M. The whirlpool sign. Radiology 2006;240:910-1.[8] Shimanuki Y, Aihara T, Takano H, et al. Clockwise whirlpool sign at
color Doppler US: an objective and definite sign of midgut volvulus.Radiology 1996;199:261-4.
[9] Taori K, Sanyal R, Attarde V, et al. Unusual presentations ofmidgut volvulus with the whirlpool sign. J Ultrasound Med 2006;25:99-103.
[10] Berrocal T, Lamas M, Gutierrez J, et al. Congenital anomalies of thesmall intestine, colon and rectum. Radiographics 1999;19(4):1219-36.
[11] Barr LL, Hayden Jr CK, Stansberry SD, et al. Enteric duplication cystsin children: are their ultrasonographic wall characteristics diagnostic.Pediatr Radiol 1990;20:326-8.
[12] Cheng G, Soboleski D, Daneman A, et al. Sonographic pitfalls in thediagnosis of enteric duplication cysts. AJR 2005;184:521-5.
[13] Verschelden P, Filiatrault D, Garel L, et al. Intussusception in children:reliability of US in diagnosis. Radiology 1992;184:741-4.





























