Embed Size (px)
Citation preview

Some observations on
observation practice
Professor Len Bowers

Overview

City-128: observation and outcomes
• 136 wards participated (6 months), in 67 hospitals in 26 Trusts. • PCC-SR: 47,000 end of shift reports were collected and scanned.
68 acute ward years of data• Also information on: patients admitted, service environment, and
physical environment• Additional measures:
– Attitude to Personality Disorder Questionnaire– Attitude to Containment Methods Questionnaire– Maslach Burnout Inventory– Multifactor Leadership Questionnaire– Team Climate Inventory– Ward Atmosphere Questionnaire (partial): order and organisation,
program clarity, staff control

Self-harm model
• Positive correlations (more self-harm with more of these):– Rate of admissions and admissions during shift– Locked ward door– Ethnicity of staff/patients
• Negative correlations (less self-harm with more of these):– Intermittent observation– Numbers of qualified staff on duty

Null findings
• Constant special observation was not related to self-harm rates
• Staff attitudes, morale, teamwork, leadership and ward atmosphere were not associated with self-harm rates in this analysis
• Security practices were not associated with self-harm rates

Substitution
• Wards with cctv and better general observation features used less intermittent observation
• A general surveillance function that stays static and is implemented in different ways
• Intermittent and constant observation use were inversely correlated, i.e. more of one meant less of the other
• CSO use was associated with more Bank/Agency staff. But not intermittent.

Acceptability of containment
6
12
18
24
30
net b
ed
mec
hani
cal r
estra
int
IM m
edica
tion
seclu
sion
man
ual r
estra
int
open
are
a se
clusio
n
PICU
cons
tant
obs
erva
tion
prn
med
icatio
n
time
out
inte
rmitte
nt o
bser
vatio
n
Patients
Staff

Conclusions on self-harm
• Premature to draw conclusions about the efficacy of special observation, but:– No indication that constant observation is effective– Startling and unexpected evidence on the possible efficacy of
intermittent observation– Intermittent observation preferred by patients
• Use of intermittent observation should be facilitated and/or increased
• Means of effect? NPSA data shows.• Enriching the nursing skill mix and increasing structured
patient activities may also help to reduce self-harm• Locking the ward door may have adverse consequences

The Tompkins Acute Ward Study
• Longitudinal study of 13 acute psychiatric wards and 3 PICUs over 5 years
• > 15k end of shift reports, all officially reported incidents, staffing deployment, PMVA training records, 191 patient interviews, 151 staff interviews, and over 500 staff questionnaires
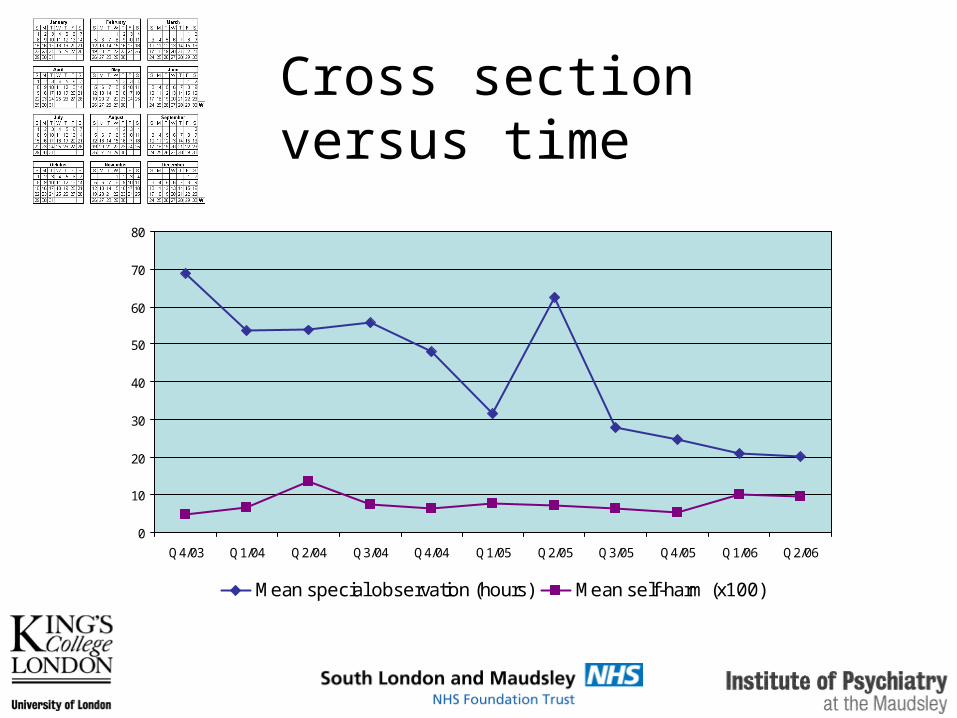
Cross section versus time
0
10
20
30
40
50
60
70
80
Q4/03 Q1/04 Q2/04 Q3/04 Q4/04 Q1/05 Q2/05 Q3/05 Q4/05 Q1/06 Q2/06
Mean special observation (hours) Mean self-harm (x100)

Constant SO associations
• Affective disorder admissions
• Self harm
• Physical aggression to others
• Bank/agency staffing use

TAWS conclusions
• Not clear whether use of lots of constant special observation has a good outcome
• Constant observation used for self-harm and also for aggression
Conflict and containment sequence study
• The sequence or order of conflict and containment events (PCC-CN)
• First two weeks of admission• Characteristics of patients• Acute psychiatric wards and psychiatric
intensive care units• Random sample of adult (18-65 years old)
patients • Final sample: 522 patients on 84 wards in 31
hospital locations

Three types of CSO use
• 86 patients (16%) received CSO1. 36 patients (7% of sample) were placed under
CSO at the point of admission2. The most common event immediately prior to
CSO was an end to intermittent SO (23%), prompted by self harm (8), absconding attempts (2) or physical violence (2)
3. Returning from absconding and aggression, particularly verbal aggression, and self-harm/suicide attempt were the next most frequent conflict behaviours to immediately precede initiation of CSO

Events during CSO use
• There was more aggression during CSO than before it
• Verbal aggression the most common event to occur during CSO
• Self-harm and suicide attempts also occurred• Lots of PRN medication given during CSO.• Sometimes show of force and manual restraint
were used• Patients with a previous history of self-harm
were more likely to be placed on CSO, but not patients with a history of harm to others

Conclusions
• Three circumstances of use: on admission, when intermittent observation fails, and post crisis
• Three behaviours targeted: aggression, self-harm and absconding
• Constant SO irritating and may prompt aggression
• Unclear what impact it has on self-harm or suicide attempts, as these still occur

NPSA suicide attempts
• 602 reports of attempted suicide• Between 01st January 2009 and 31st
December 2009 • In mental health inpatient units• Included only attempts made on the ward,
and attempts made off the ward where the actions of ward staff prevented the suicide.
• Aim: how were these prevented from becoming completed suicides
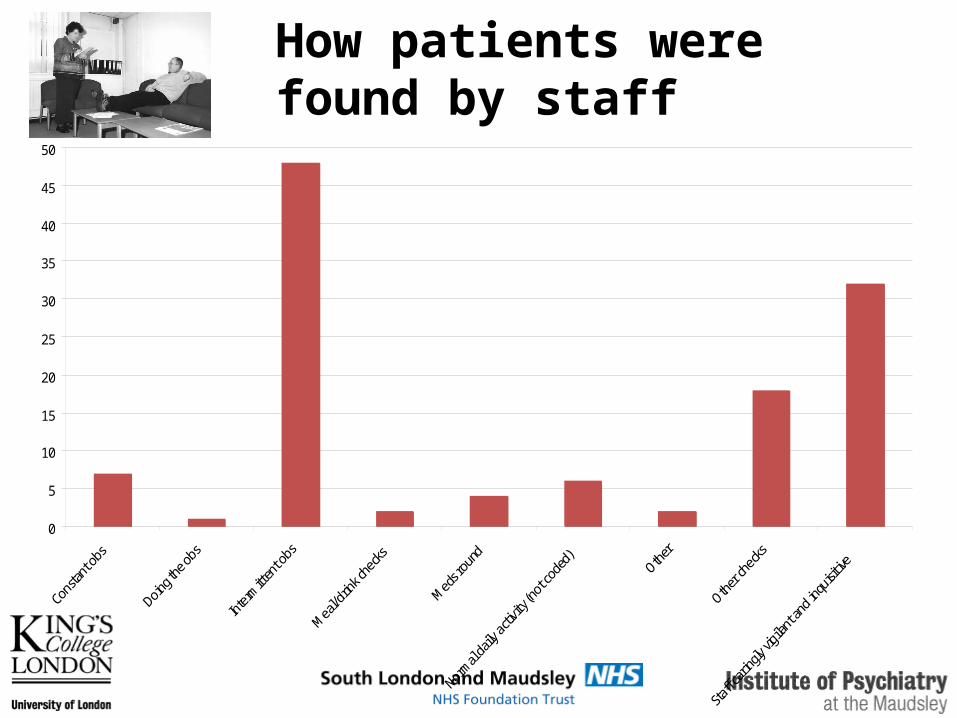
How patients were found by staff
0
5
10
15
20
25
30
35
40
45
50
CSO suicide attempts
• Ran into her bedroom, locking the door behind her, tying a ligature before access could be gained.
• Tying ligature underneath the bedclothes while in bed (n = 2)
• Allowed to go to the toilet unobserved while nurse waited outside the door, attempted suicide by suffocation while out of sight (n = 1), or by tying ligature (n = 2).
• Allowed to go to the toilet with door left open, but nurse stood to one side to give privacy. Ligature tied whilst out of sight.

Conclusions
• Intermittent observation is good
• CSO can be circumvented: be on your guard
• Be caringly vigilant and inquisitive

Literature review
• 1960-2009, 63 papers• 4-16% of patients placed on CSO• Mostly lasts 2 days or more• Reasons for use: self-harm/suicide,
absconding, aggression• What outcome information there is relates
to self-harm and suicide• No outcomes or studies of CSO for
aggression

Observations on observation for violence
• Two to one observation for violence:– No evidence on efficacy– Unusual practice– Justification on a PICU?
• Rationale?• What goes on during such observation?• Cost• Review. How do you know when to stop?

Summary
• Intermittent observation for self-harm and suicide prevention is good. There is evidence it works, and patients prefer it
• CSO for self-harm and suicide is less clear in terms of evidence, but common sense says it works
• No evidence on efficacy for absconding prevention
• What little evidence there is for aggression suggests observation may increase it

Inpatient suicide prevention course
• Baseline MCQs and Attitude to Suicide Prevention Scale
• General risk assessment and inpatient risk assessment (videos, case studies, practice)
• Routines to prevent (videos, online discussion)
• Constant and intermittent observation (research review, evaluate 8 new ideas on obs practice, review local policy, share ideas)
• Being Caringly Vigilant and Inquisitive (review public news stories and clinical cctv footage)
• Understanding the suicidal mind (Schneidman’s 10 commonalities, build empathy)
• Spending time with suicidal people (interaction skills explained by expert nurse)
• Outcome MCQs and Attitude to Suicide Prevention Scale
• http://www.youtube.com/watch?v=hBrs53ZsPIY

• www.kcl.ac.uk/mentalhealthnursing
• www.safewards.net





























