Embed Size (px)
Citation preview

Somatosensory SystemsSomatosensory Systems
Chapter 7 BlumenfeldChapter 7 BlumenfeldRobert Altman PGY 3Robert Altman PGY 3
Neurology, McGill UniversityNeurology, McGill UniversityOct 2009Oct 2009
OverviewOverview
Overview key afferent pathwaysOverview key afferent pathways Focusing on central course in spinal cord and brainFocusing on central course in spinal cord and brain
Dorsal Column Medial Lemniscal (DCML)Dorsal Column Medial Lemniscal (DCML) Spinothalamic and other anterolateral pathwaysSpinothalamic and other anterolateral pathways
Introduction to the thalamusIntroduction to the thalamus Neurology of bladder & bowel functionNeurology of bladder & bowel function
VERY briefVERY brief
Clinical examplesClinical examples Take-home messagesTake-home messages Jeopardy-Style Trivia, Round 2!Jeopardy-Style Trivia, Round 2!
General PrincipalsGeneral Principals
Somatotopy respected in Somatotopy respected in spinal cord, brainstem relay spinal cord, brainstem relay nucleii and cortexnucleii and cortex
Aids with localizability of Aids with localizability of lesionslesions
Touch is shared in both Touch is shared in both pathwayspathways DiscriminativeDiscriminative CrudeCrude
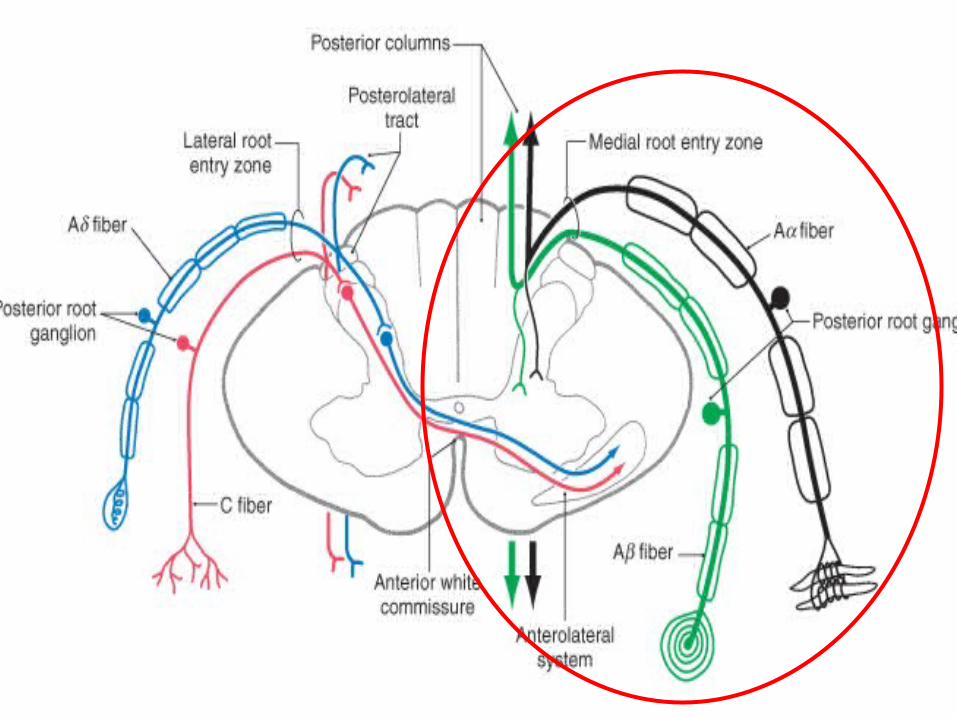
DRG; pseudo-unipolar neuronDRG; pseudo-unipolar neuron
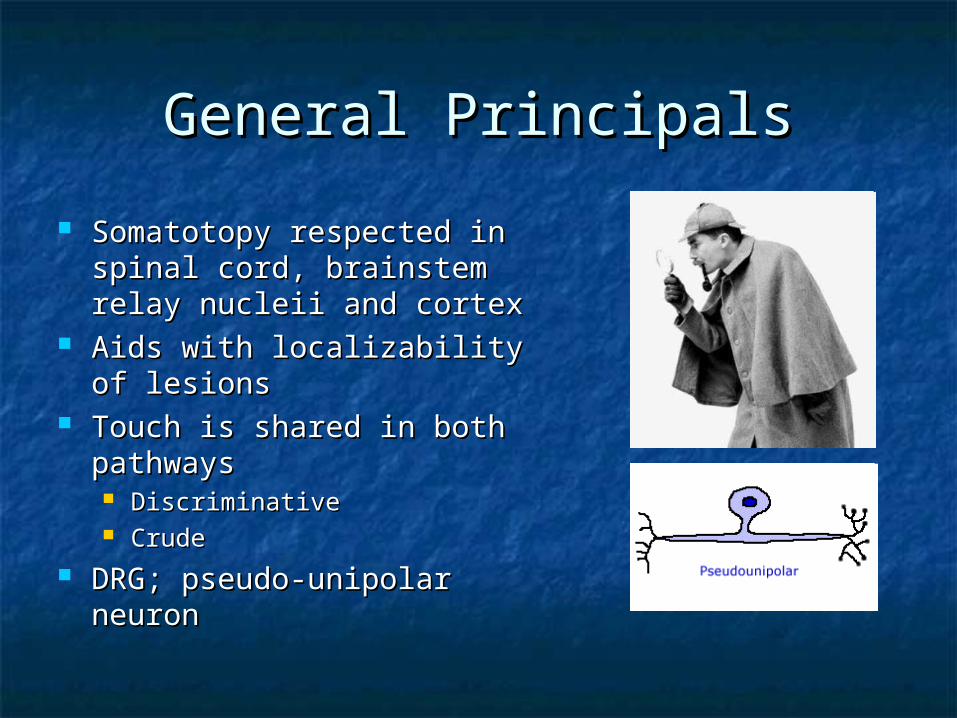
Sensory Neuron TypesSensory Neuron Types
NAMENAME DIAMETER (µm)DIAMETER (µm) MYELINATEDMYELINATED RECEPTORSRECEPTORS SENSORY SENSORY MODALITYMODALITY
A-A- (I) (I) 13-2013-20 YesYes Muscle spindle, golgi Muscle spindle, golgi tendon organtendon organ Proprioception Proprioception
A-A-ββ (II) (II) 6-126-12 YesYes
Muscle spindle, Muscle spindle, Meissner’s corpuscule, Meissner’s corpuscule, Merkel’s receptor, Merkel’s receptor, Pacinian corpuscule, Pacinian corpuscule, Ruffini ending, Hair Ruffini ending, Hair receptorreceptor
Proprioception, Proprioception, superficial touch, deep superficial touch, deep touch, vibration, touchtouch, vibration, touch
A-A-δδ (III) (III) 1-51-5 YesYes Bare nerve endingBare nerve ending Pain, temperature Pain, temperature (cool)(cool)
C (IV)C (IV) 0.2-1.50.2-1.5 NoNo Bare nerve endingBare nerve ending Pain, temperature Pain, temperature (warm), itch(warm), itch


DCMLDCML
DCMLDCML
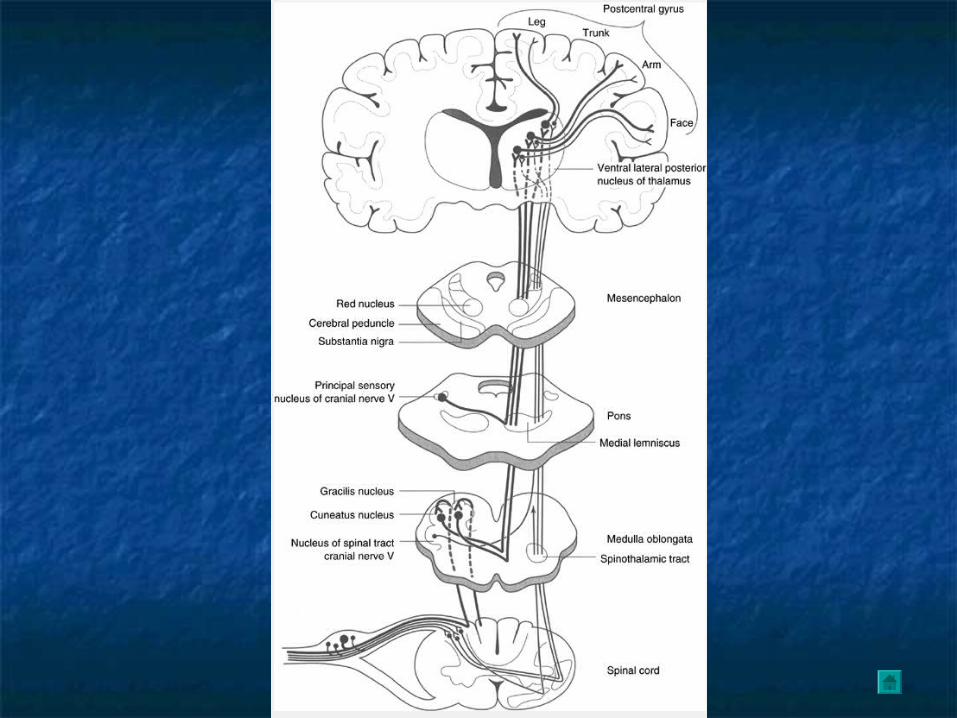
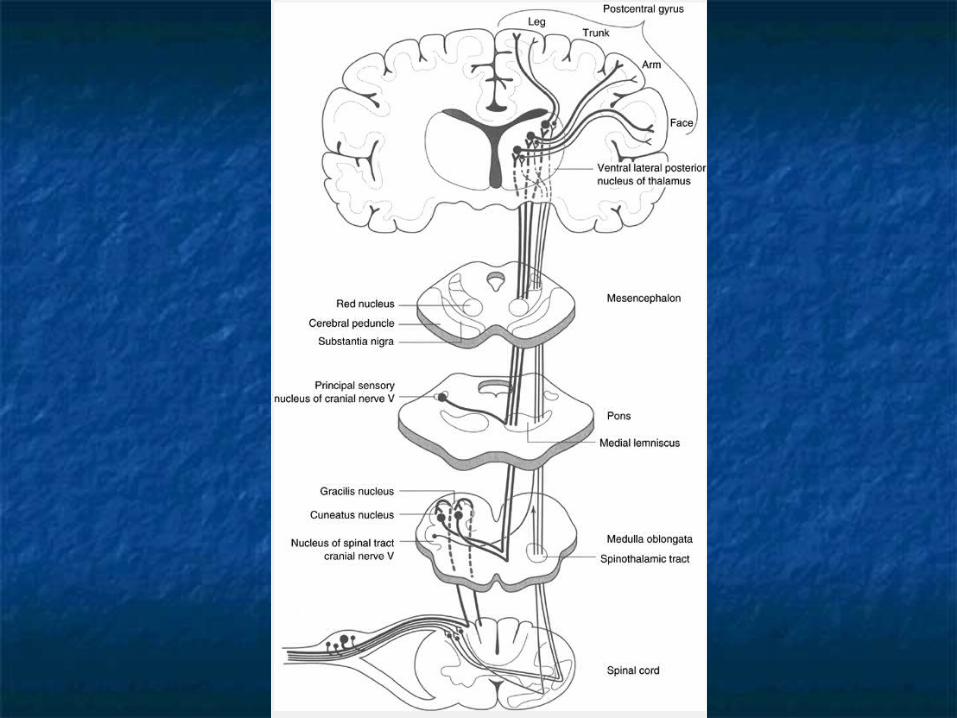
Most axons do not perform their 1Most axons do not perform their 1stst synapse until at n. gracilis or synapse until at n. gracilis or cuneatus in lower medulla (i.e. 1cuneatus in lower medulla (i.e. 1stst order) order)
22ndnd order neurons run to VPL order neurons run to VPL Somatotopy mnemonicSomatotopy mnemonic Lemniscus Lemniscus = tract = tract Gracile = Gracile = thinthin Cuneate = Cuneate = wedgewedge T6T6 Internal Arcuate fibersInternal Arcuate fibers Medial LemniscusMedial Lemniscus
VerticalVertical Lateral / inclined position in upper brainstemLateral / inclined position in upper brainstem
VPLVPL Posterior limb of IC to reach areas 3, 1, 2 of primary SS cortexPosterior limb of IC to reach areas 3, 1, 2 of primary SS cortex
Primarily layer IV > III > VI Primarily layer IV > III > VI

6 layers of the neocortex6 layers of the neocortexLayerLayer NameName FunctionFunction
II Molecular Layer / Plexiform LayerMolecular Layer / Plexiform Layer Dendrites and axons Dendrites and axons from other layersfrom other layers
IIII Small Pyramidal Layer / External Small Pyramidal Layer / External Granular LayerGranular Layer
Cortical-cortical Cortical-cortical connectionsconnections
IIIIII Medium Pyramidal layer / External Medium Pyramidal layer / External Pyramidal LayerPyramidal Layer
Cortical-cortical Cortical-cortical connectionsconnections
IVIV Granular Layer / Internal Granular Granular Layer / Internal Granular LayerLayer Input from thalamusInput from thalamus
VV Large Pyramidal Layer / Internal Large Pyramidal Layer / Internal Pyramidal LayerPyramidal Layer
Outputs to subcortical Outputs to subcortical structures besides structures besides thalamusthalamus
e.g. from giant cells of e.g. from giant cells of Betz in motor cortexBetz in motor cortex
VIVI Polymorphic Layer / Multiform LayerPolymorphic Layer / Multiform LayerCortical-Thalamic Cortical-Thalamic connections (Outputs to connections (Outputs to Thalamus)Thalamus)
Layers I through VI vary in thickness in different cortical regions. Layer IV is most pronounced in the sensory projection cortex and layer V is most pronounced in the primary motor cortex (pre-central
gyrus).

Sensory HomonculusSensory Homonculus

Anterolateral SystemsAnterolateral Systems

Anterolateral SystemsAnterolateral Systems
First synapse is immediate in the spinal cordFirst synapse is immediate in the spinal cord Dorsal horn of lamina I (marginal zone)Dorsal horn of lamina I (marginal zone) Lamina VLamina V
Lissauer’s tract allows some axon collaterals to Lissauer’s tract allows some axon collaterals to ascend or descend 2-4 segments before entering in ascend or descend 2-4 segments before entering in central graycentral gray
Second order neurons than traverse Second order neurons than traverse anterior anterior commisure (over 2-3 spinal segments)commisure (over 2-3 spinal segments) clinical clinical correlation to spinal lesionscorrelation to spinal lesions
Somatotopy (see next slide)Somatotopy (see next slide) Once reaches brainstem, remains lateral (b/w Once reaches brainstem, remains lateral (b/w
olives and ICP)olives and ICP)

Anterolateral SystemsAnterolateral Systems
Anterolateral systemAnterolateral system SpinothalamicSpinothalamic ( (I, VV))
Discriminative aspects of pain, location, intensityDiscriminative aspects of pain, location, intensity Synapse on VPL (different area than DCML), relay to Synapse on VPL (different area than DCML), relay to
specific SSC target (Brodmann 3,1,2)specific SSC target (Brodmann 3,1,2) SpinoreticularSpinoreticular ( (II, VIIII, VII, VI, VIIIVI, VIII))
Emotional and arousal aspects of painEmotional and arousal aspects of pain Ultimately RF projects to IL thalamic nuclei Ultimately RF projects to IL thalamic nuclei
(centromedian), which then project diffusely to the (centromedian), which then project diffusely to the entire cerebral cortex (behavioural arousal)entire cerebral cortex (behavioural arousal)
SpinomesencephalicSpinomesencephalic To PAG, SCTo PAG, SC Pain modulationPain modulation

Central Pathways Involved in Central Pathways Involved in Pain ModulationPain Modulation
Spinal cord circuitsSpinal cord circuits Gate theory (A-Gate theory (A-ββ) ) TENSTENS
““Long range” modulatory inputsLong range” modulatory inputs PAGPAG (MB) receives diffuse inputs from (MB) receives diffuse inputs from hypothalamus, hypothalamus,
amygdala, cortexamygdala, cortex Relays to nucleus raphe-magnus inRelays to nucleus raphe-magnus in RVM RVM (rostral ventral (rostral ventral
medulla)medulla) Subsequently relays (via 5HT neurons) to dorsal horn, Subsequently relays (via 5HT neurons) to dorsal horn, acting acting
as pain modulatoras pain modulator Also relays to Also relays to locus ceruleuslocus ceruleus (rostral pons) via substance P, (rostral pons) via substance P,
which in turn relay NE projections to dorsal horn, which in turn relay NE projections to dorsal horn, acting as acting as pain modulatorpain modulator

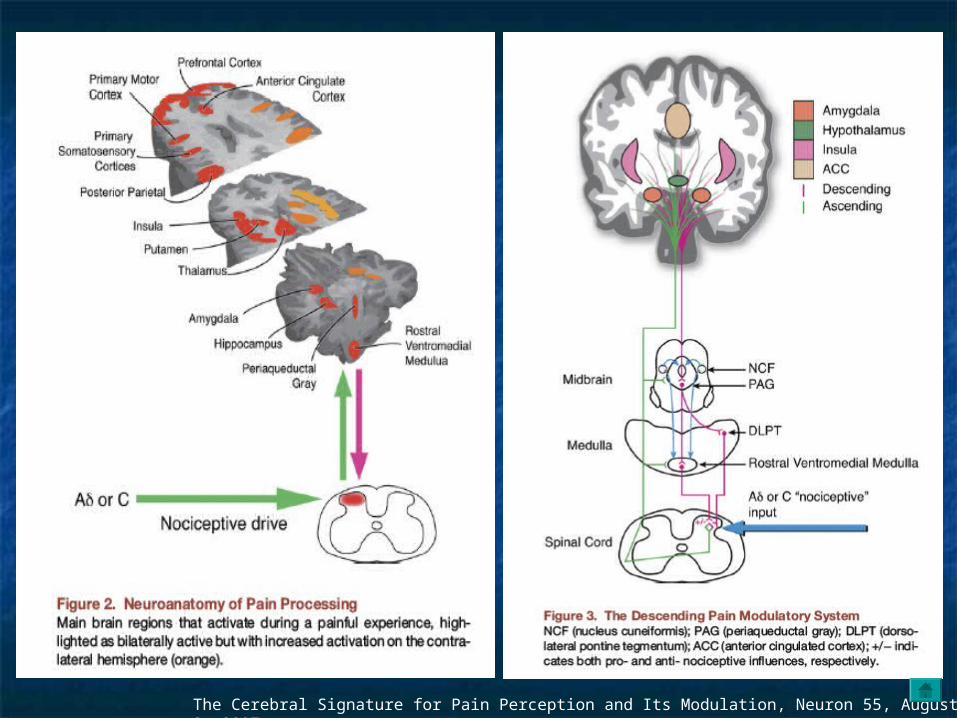
The Cerebral Signature for Pain Perception and Its Modulation, Neuron 55, August 2, 2007
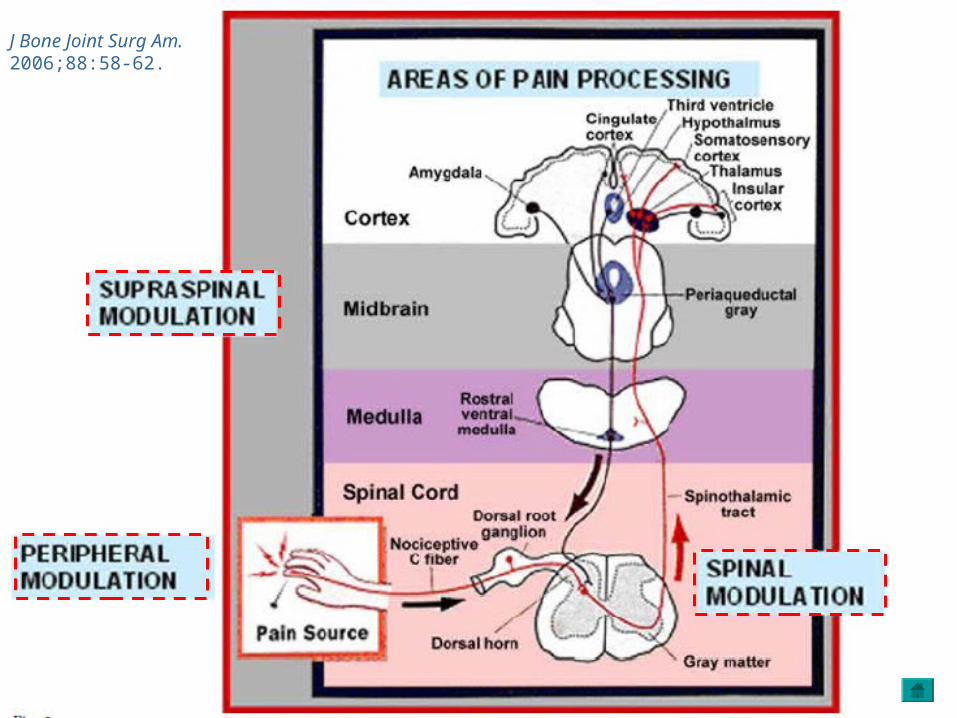
J Bone Joint Surg Am. 2006;88:58-62.

OpiodsOpiods
Receptors found on peripheral nerves Receptors found on peripheral nerves and diffusely in pain modulating and diffusely in pain modulating system.system. Enkephalins*Enkephalins* dynorphindynorphin* * ββ-endorphins**-endorphins**
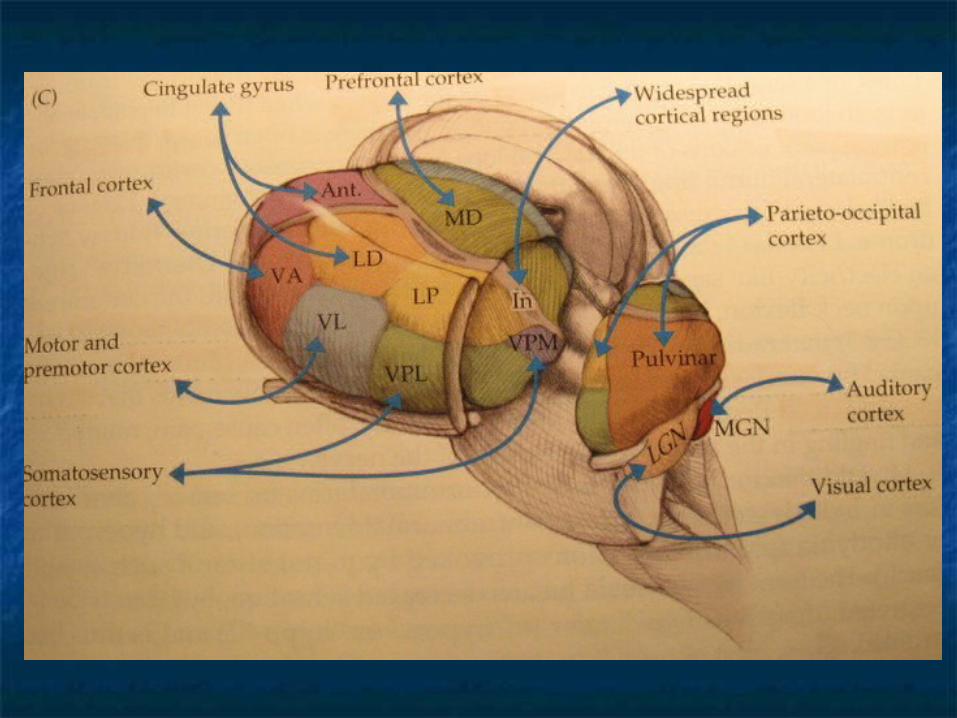
ThalamusThalamus
Brief overviewBrief overview
ThalamusThalamus
Master relay centerMaster relay center SensorySensory MotorMotor CerebellarCerebellar Basal gangliaBasal ganglia LimbicLimbic Behaviour, arousal, sleep-wake cycleBehaviour, arousal, sleep-wake cycle
Dense reciprocal feedback connections Dense reciprocal feedback connections between cortex and thalamus. between cortex and thalamus. Corticothalamic projections outnumber Corticothalamic projections outnumber
thalamocortical!thalamocortical!

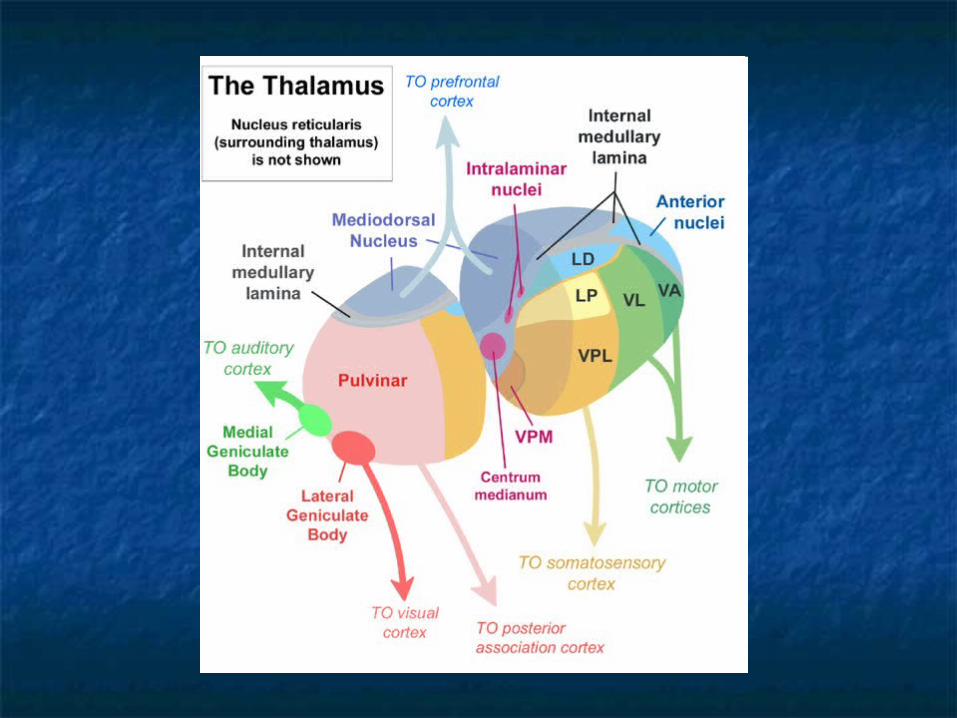
ThalamusThalamus
DiencephalonDiencephalon Divided by internal medullary laminaDivided by internal medullary lamina
MedialMedial LateralLateral AnteriorAnterior Intralaminar nucleiIntralaminar nuclei Midline thalamic nucleiMidline thalamic nuclei Thalamic reticular nucleusThalamic reticular nucleus
3 chief functions3 chief functions
1.1. RelayRelay SpecificSpecific Nonspecific (widely projecting)Nonspecific (widely projecting)
2.2. IntralaminarIntralaminar
3.3. ReticularReticular
Relay Nuclei Relay Nuclei
Lie mainly in lateral thalamusLie mainly in lateral thalamus All primary sensory modalities have relays in the lateral thalamus All primary sensory modalities have relays in the lateral thalamus
en route to their specific cortical target, with one exception*en route to their specific cortical target, with one exception* Reciprocal innervation w/ cortexReciprocal innervation w/ cortex Examples:Examples:
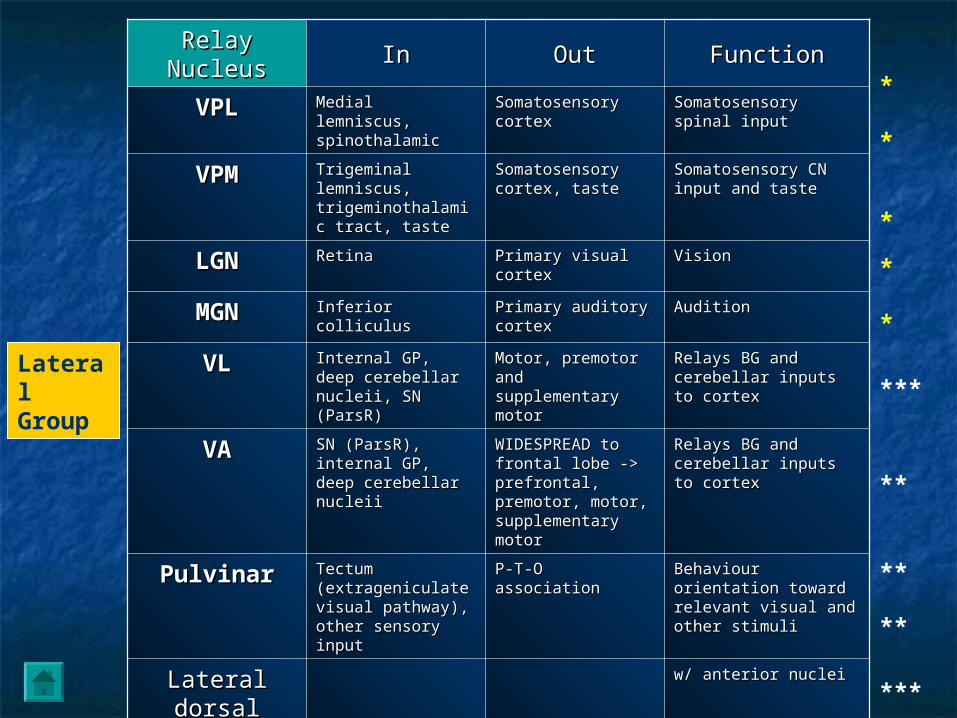
Relay Relay NucleusNucleus InIn OutOut FunctionFunction
VPLVPL Medial lemniscus, Medial lemniscus, spinothalamicspinothalamic
Somatosensory Somatosensory cortexcortex
Somatosensory spinal Somatosensory spinal inputinput
VPMVPM Trigeminal Trigeminal lemniscus, lemniscus, trigeminothalamic trigeminothalamic tract, tastetract, taste
Somatosensory Somatosensory cortex, tastecortex, taste
Somatosensory CN Somatosensory CN input and tasteinput and taste
LGNLGN RetinaRetina Primary visual Primary visual cortexcortex
VisionVision
MGNMGN Inferior colliculusInferior colliculus Primary auditory Primary auditory cortexcortex
AuditionAudition
VLVL Internal GP, deep Internal GP, deep cerebellar nucleii, cerebellar nucleii, SN (ParsR)SN (ParsR)
Motor, premotor Motor, premotor and supplementary and supplementary motormotor
Relays BG and Relays BG and cerebellar inputs to cerebellar inputs to cortexcortex
VAVA SN (ParsR), internal SN (ParsR), internal GP, deep cerebellar GP, deep cerebellar nucleiinucleii
WIDESPREAD to WIDESPREAD to frontal lobe -> frontal lobe -> prefrontal, prefrontal, premotor, motor, premotor, motor, supplementary supplementary motormotor
Relays BG and Relays BG and cerebellar inputs to cerebellar inputs to cortexcortex
PulvinarPulvinar Tectum Tectum (extrageniculate (extrageniculate visual pathway), visual pathway), other sensory inputother sensory input
P-T-O associationP-T-O association Behaviour orientation Behaviour orientation toward relevant visual toward relevant visual and other stimuliand other stimuli
Lateral Lateral dorsaldorsal
w/ anterior nucleiw/ anterior nuclei
Lateral Lateral posteriorposterior
w/ pulvinarw/ pulvinar
Ventral Ventral medialmedial
Midbrain reticular Midbrain reticular formationformation
Widespread to Widespread to cortexcortex
Maintain alert, Maintain alert, conscious stateconscious state
*
*
*
*
*
***
**
***
**
**
Lateral Group

Relay Relay NucleusNucleus InIn OutOut FunctionFunction
Medial group
Mediodorsal / Mediodorsal / dorsomedialdorsomedial
Amygdala, olfactory Amygdala, olfactory cortex, limbic cortex, cortex, limbic cortex, BGBG
Frontal cortexFrontal cortex Limbic pathways, major Limbic pathways, major relay to frontal cortexrelay to frontal cortex
Anterior group
Anterior Anterior nucleusnucleus
Mammillary bodies, Mammillary bodies, hippocampal hippocampal formationformation
Cingulate gyrusCingulate gyrus Limbic pathwaysLimbic pathways
Midline Thalamic groupParaventricular, Paraventricular,
parataenial, parataenial, intermediodorsalintermediodorsal
, rhomboid, , rhomboid, medial ventralmedial ventral
Hypothalamus, basal Hypothalamus, basal forebrain, amygdala, forebrain, amygdala, hippocampushippocampus
Amygdala, Amygdala, hippocampus, limbic hippocampus, limbic cortexcortex
Limbic pathwaysLimbic pathways
*
**
**
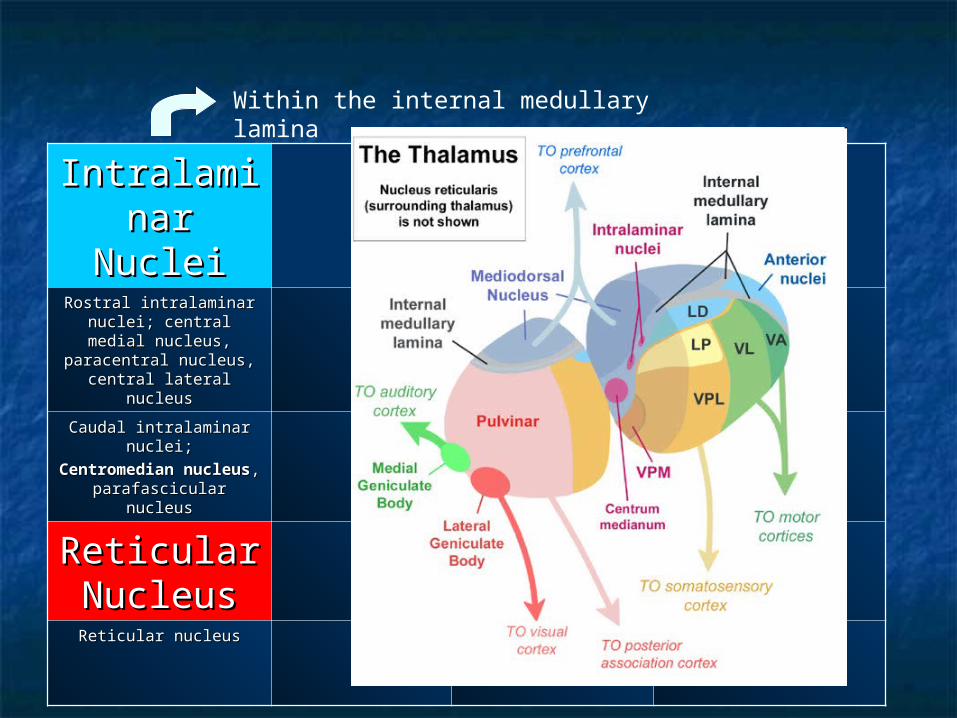
IntralaminIntralaminar Nucleiar NucleiRostral intralaminar Rostral intralaminar
nuclei; central medial nuclei; central medial nucleus, paracentral nucleus, paracentral
nucleus, central lateral nucleus, central lateral nucleusnucleus
Caudal intralaminar Caudal intralaminar nuclei;nuclei;
Centromedian Centromedian nucleusnucleus, parafascicular , parafascicular
nucleusnucleus
Reticular Reticular NucleusNucleusReticular nucleusReticular nucleus
Within the internal medullary lamina

IntralaminIntralaminar Nucleiar Nuclei InIn OutOut FunctionFunction
Rostral intralaminar nuclei;; central medial central medial nucleus, paracentral nucleus, paracentral
nucleus, central lateral nucleus, central lateral nucleusnucleus
Deep cerebellar Deep cerebellar nuclei, GP, nuclei, GP, brainstem, brainstem, ARASARAS, , sensory pathwayssensory pathways
Cerebral cortex, Cerebral cortex, striatumstriatum
Maintain alert Maintain alert consciousness; motor consciousness; motor relay for basal ganglia and relay for basal ganglia and cerebellumcerebellum
Caudal intralaminar Caudal intralaminar nucleinuclei;;
Centromedian Centromedian nucleusnucleus, parafascicular , parafascicular
nucleusnucleus
GP, ARAS, sensory GP, ARAS, sensory pathwayspathways
Striatum, cereral Striatum, cereral cortexcortex
Motor relay for BGMotor relay for BG
Reticular Reticular NucleusNucleusReticular nucleusReticular nucleus Cerebral cortex, Cerebral cortex,
thalamic relay and thalamic relay and intralaminar nuclei, intralaminar nuclei, ARASARAS
Thalamic relay and Thalamic relay and intralaminar nucleiintralaminar nuclei
Regulates state of other Regulates state of other thalamic nucleithalamic nuclei
***
***


Clinical Concept – dysfunction Clinical Concept – dysfunction in sensory pathwaysin sensory pathways
Negative = anasthesia, loss of Negative = anasthesia, loss of sensationsensation
Positive = added sensationPositive = added sensation Localizability of symptom descriptionLocalizability of symptom description
“numb”
Victor and Adams
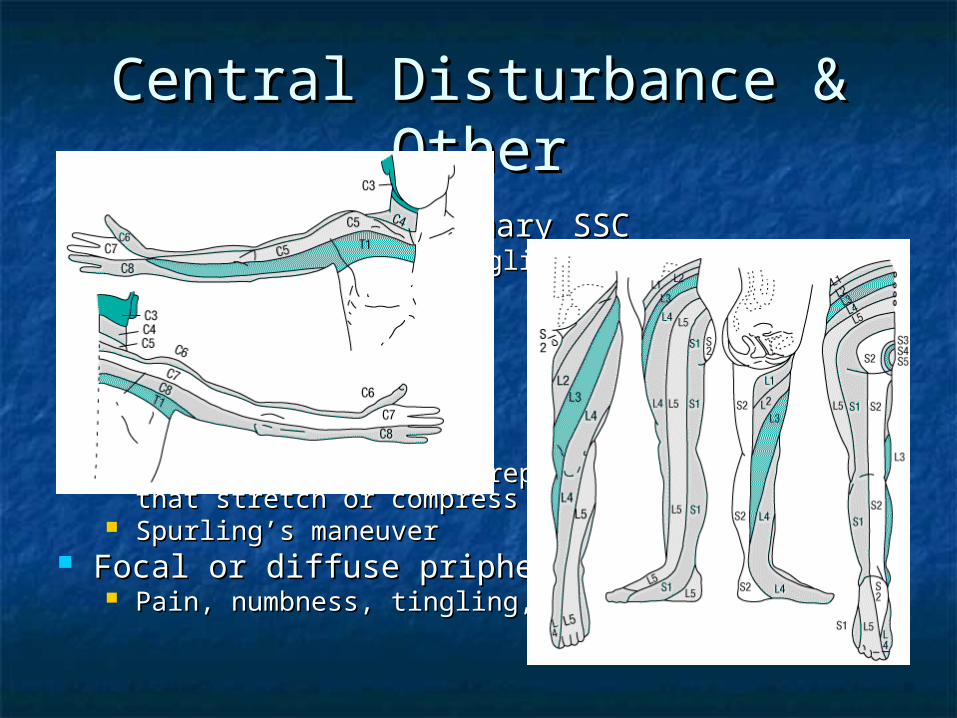
Central Disturbance & OtherCentral Disturbance & Other
Parietal lobe or primary SSCParietal lobe or primary SSC Contralateral numb tingling or painContralateral numb tingling or pain
ThalamicThalamic Dejerine-RoussyDejerine-Roussy
Cervial cordCervial cord LHermitte’s signLHermitte’s sign
RadicularRadicular Symptoms (dermatomal) reproduced by maneuvers that Symptoms (dermatomal) reproduced by maneuvers that
stretch or compress the NRstretch or compress the NR Spurling’s maneuverSpurling’s maneuver
Focal or diffuse pripheral n diseaseFocal or diffuse pripheral n disease Pain, numbness, tingling, etc…Pain, numbness, tingling, etc…
Spinal Cord LesionsSpinal Cord Lesions
MyelopathiesMyelopathies CompressiveCompressive Non-CompressiveNon-Compressive
Etiology multifactorialEtiology multifactorial VINDICATE, VITAMIN CD etc….VINDICATE, VITAMIN CD etc….
Most common causes = compressive due to Most common causes = compressive due to trauma, metasteses, degenerative changestrauma, metasteses, degenerative changes
Clinically evident by sensory level, motor Clinically evident by sensory level, motor dysfunction, reflex abnormalities, b/b dysfunction, reflex abnormalities, b/b incontinence, fever?incontinence, fever? Image above sensory level (2-4 levels)Image above sensory level (2-4 levels) And even if you suspect LS pathology, try and get whole And even if you suspect LS pathology, try and get whole
spine imagedspine imaged

Spinal ShockSpinal Shock
Acute flaccid paralysisAcute flaccid paralysis Absent DTRAbsent DTR HypotensionHypotension Sphincter / tone flacciditySphincter / tone flaccidity
Rule of thumb = 80% of patients treated for Rule of thumb = 80% of patients treated for CC after they are nonambulatory remain so. CC after they are nonambulatory remain so. However, 80% treated before losing However, 80% treated before losing mobility, remain so for the remainder of mobility, remain so for the remainder of their lives.their lives.

Clinical ExamplesClinical Examples
Primary somatosensory cortexPrimary somatosensory cortex Primary vs “cortical” sensory lossPrimary vs “cortical” sensory loss
VPL or VPM or Thalamic VPL or VPM or Thalamic somatosensory radiationssomatosensory radiations
Lateral Pons or lateral medullaLateral Pons or lateral medulla Medial medullaMedial medulla SCSC NR / Peripheral n.NR / Peripheral n.
Contra or ipsi, sensory loss, motor loss, other…
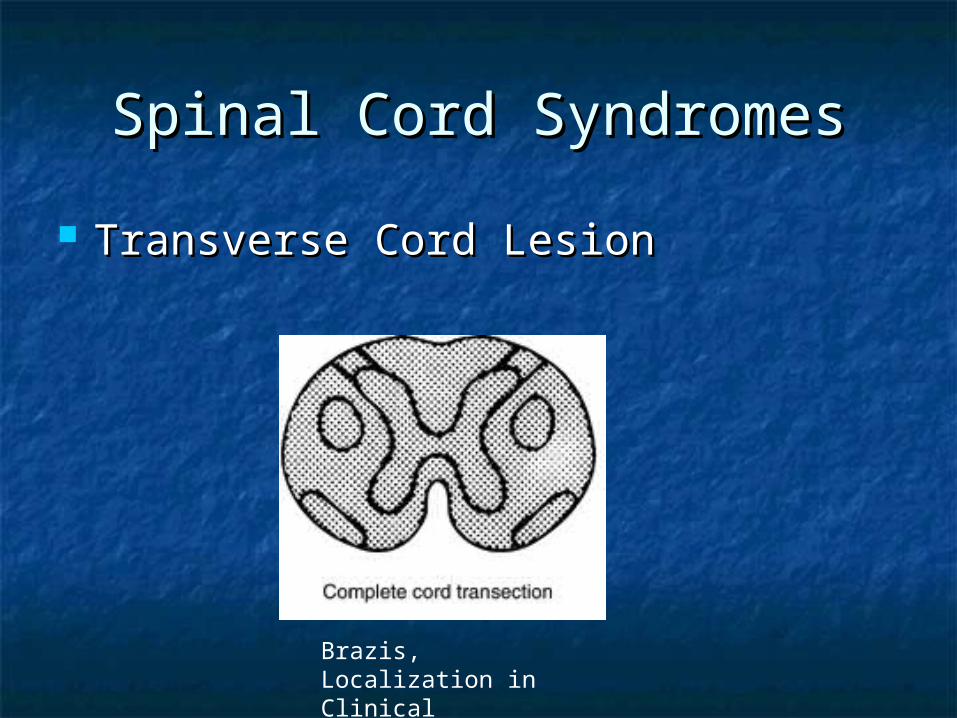
Spinal Cord SyndromesSpinal Cord Syndromes
Transverse Cord LesionTransverse Cord Lesion
Brazis, Localization in Clinical Neurology, 5th ed
Spinal Cord SyndromesSpinal Cord Syndromes
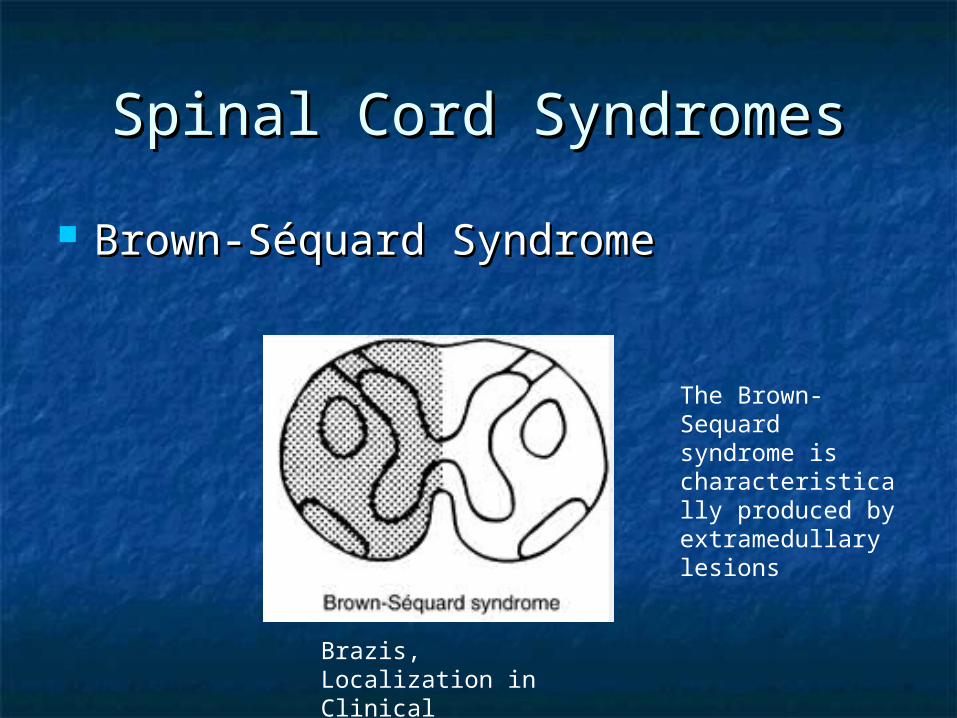
Brown-Séquard SyndromeBrown-Séquard Syndrome
Brazis, Localization in Clinical Neurology, 5th ed
The Brown-Sequard syndrome is characteristically produced by extramedullary lesions
Spinal Cord SyndromesSpinal Cord Syndromes
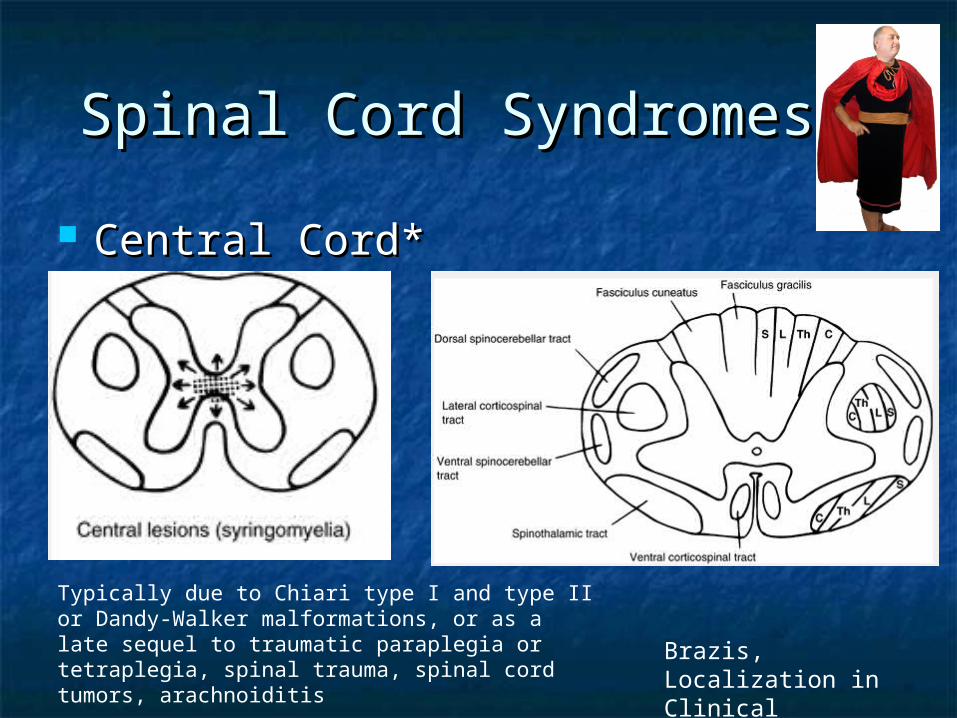
Central Cord*Central Cord*
Brazis, Localization in Clinical Neurology, 5th ed
Typically due to Chiari type I and type II or Dandy-Walker malformations, or as a late sequel to traumatic paraplegia or tetraplegia, spinal trauma, spinal cord tumors, arachnoiditis
SyringomyeliaSyringomyelia
The classic presentation is a central cord syndrome consisting of a dissociated sensory loss and areflexic weakness in the upper limbs. Loss of pain and temperature sensation with sparing
of touch and vibration in a distribution that is "suspended" over the nape of the neck, shoulders, and upper arms (cape distribution) or in the hands.
Begins asymmetrically with unilateral sensory loss in the hands that leads to injuries and burns that are not appreciated by the patient.

SyringomyeliaSyringomyelia
Muscle wasting in the lower neck, shoulders, arms, and hands with asymmetric or absent reflexes in the arms reflects expansion of the cavity into the gray matter of the cord.
As the cavity enlarges and further compresses the long tracts Spasticity and weakness of the legs Bladder and bowel dysfunction Horner's syndrome Facial numbness and sensory loss from damage to the
descending tract of the trigeminal nerve (C2 level or above). In cases with Chiari malformations, cough-induced headache and
neck, arm, or facial pain are reported. Extension of the syrinx into the medulla, syringobulbia, causes
palatal or vocal cord paralysis, dysarthria, horizontal or vertical nystagmus, episodic dizziness, and tongue weakness.

Spinal Cord SyndromesSpinal Cord Syndromes Central Cord & Central Cord & Sacral SparingSacral Sparing
http://www.neuroanatomy.wisc.edu/SClinic/Myelo/Myelbase.htm

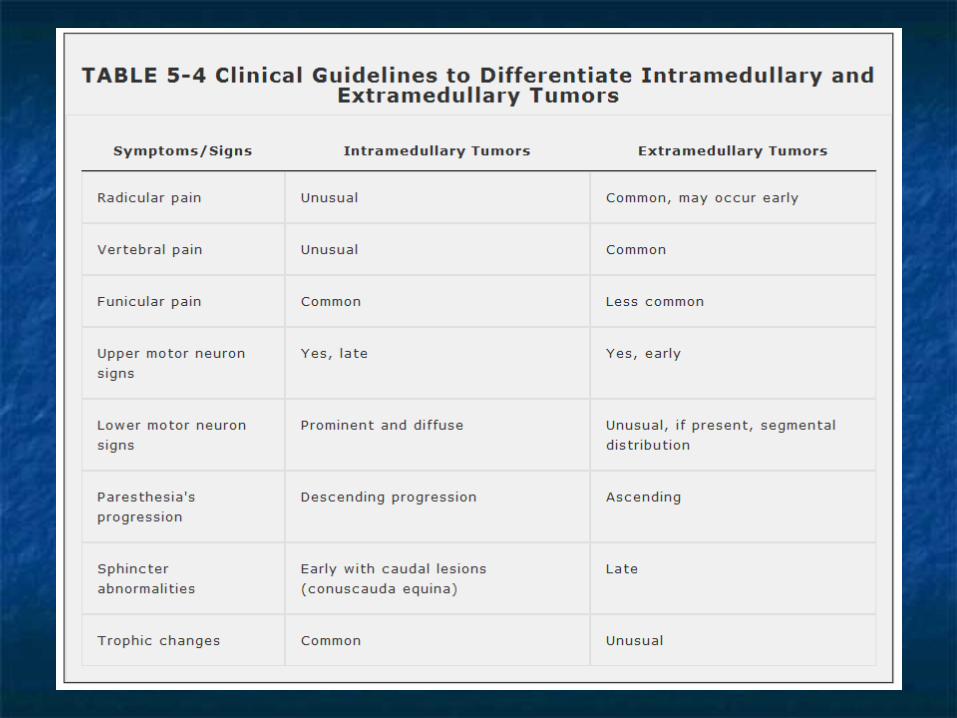
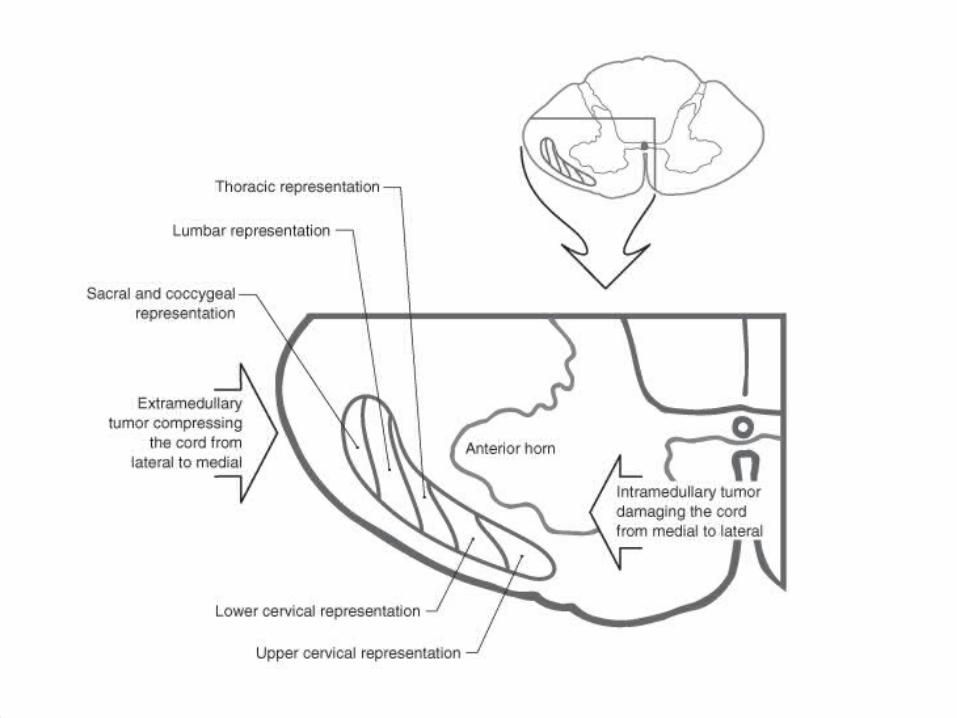
Intramedullary and Intramedullary and Extramedullary SyndromesExtramedullary Syndromes
Intramedullary vs Extramedullary processes Intra or external to cordcompresses the spinal cord or its
vascular supply. The differentiating features are only relative and serve as
clinical guides. With extramedullary lesions, radicular pain is often
prominent, and there is early sacral sensory loss (lateral spinothalamic tract) and spastic weakness in the legs (corticospinal tract) due to the superficial location of leg fibers in the corticospinal tract.
Intramedullary lesions tend to produce poorly localized burning pain rather than radicular pain and spare sensation in the perineal and sacral areas ("sacral sparing"), reflecting the laminated configuration of the spinothalamic tract with sacral fibers outermost; corticospinal tract signs appear later.
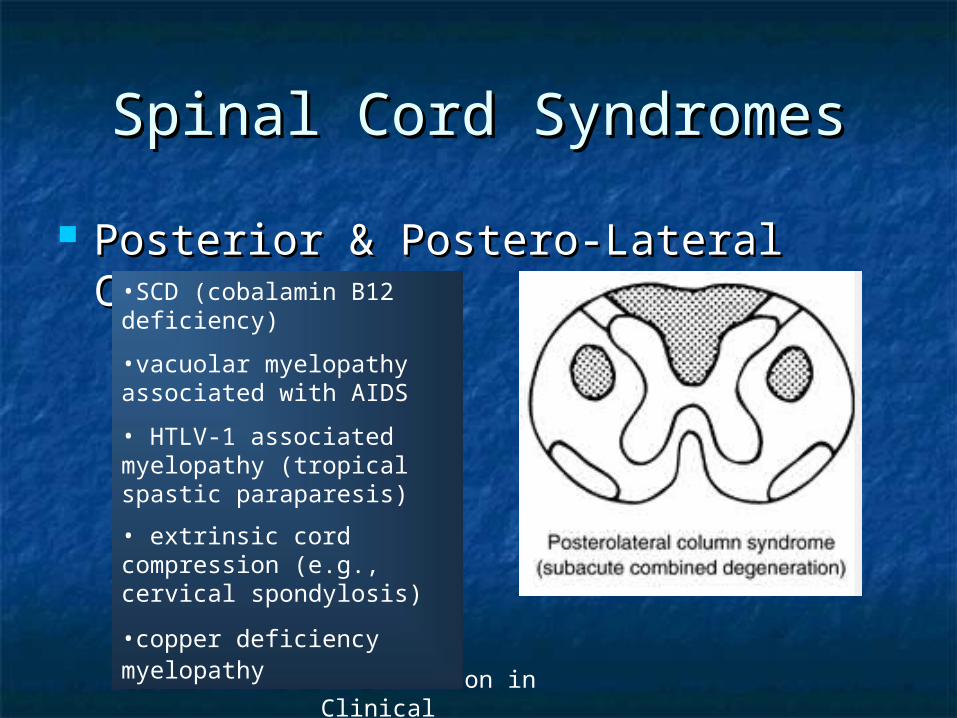
Spinal Cord SyndromesSpinal Cord Syndromes
Posterior & Postero-Lateral CordPosterior & Postero-Lateral Cord
Brazis, Localization in Clinical Neurology, 5th ed
•SCD (cobalamin B12 deficiency)
•vacuolar myelopathy associated with AIDS
• HTLV-1 associated myelopathy (tropical spastic paraparesis)
• extrinsic cord compression (e.g., cervical spondylosis)
•copper deficiency myelopathy

Spinal Cord SyndromesSpinal Cord Syndromes
Anterior CordAnterior Cord
Brazis, Localization in Clinical Neurology, 5th ed
Anterior Spinal Artery Syndrome
•Back of neck pain of sudden onset•Rapidly progressive flaccid and areflexic paraplegia•Loss of pain and temperature to a sensory level•Preservation of JPS and vibration sensation•Urinary incontinence
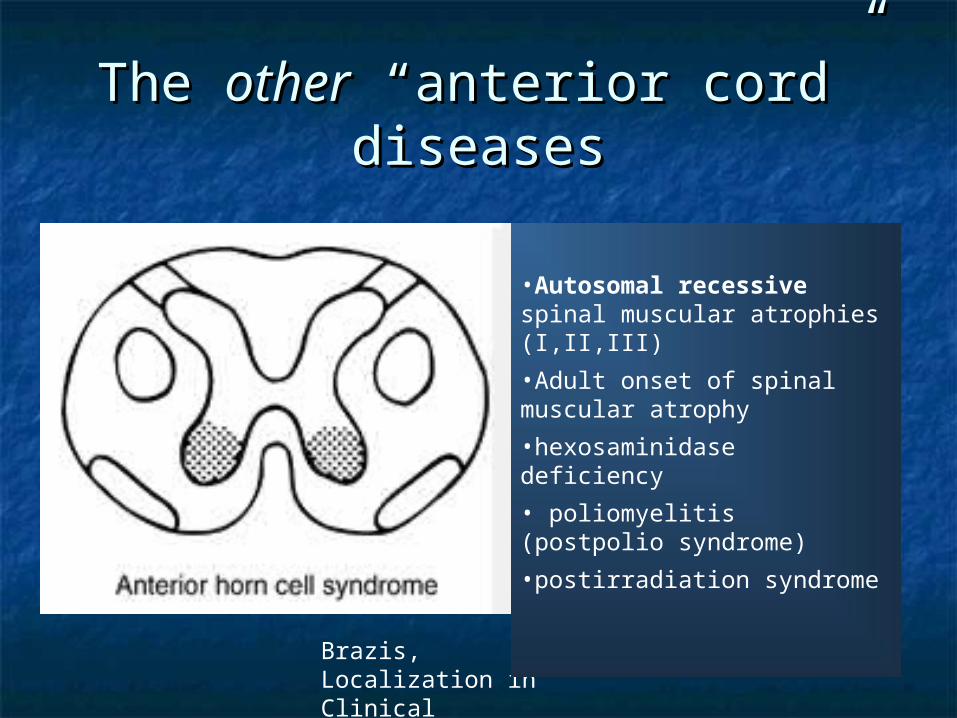
The The otherother “anterior cord” “anterior cord” diseasesdiseases
Brazis, Localization in Clinical Neurology, 5th ed
•Autosomal recessive spinal muscular atrophies (I,II,III)
•Adult onset of spinal muscular atrophy
•hexosaminidase deficiency
• poliomyelitis (postpolio syndrome)
•postirradiation syndrome
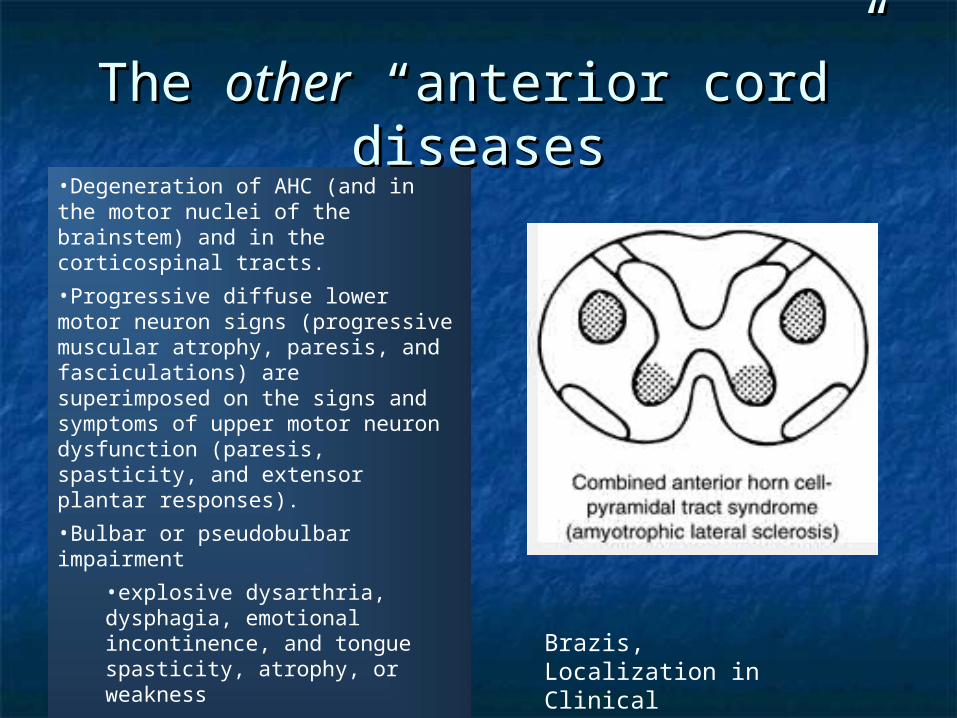
The The otherother “anterior cord” “anterior cord” diseasesdiseases
Brazis, Localization in Clinical Neurology, 5th ed
•Degeneration of AHC (and in the motor nuclei of the brainstem) and in the corticospinal tracts.
•Progressive diffuse lower motor neuron signs (progressive muscular atrophy, paresis, and fasciculations) are superimposed on the signs and symptoms of upper motor neuron dysfunction (paresis, spasticity, and extensor plantar responses).
•Bulbar or pseudobulbar impairment
•explosive dysarthria, dysphagia, emotional incontinence, and tongue spasticity, atrophy, or weakness
•Bowel / bladder unaffected
•“Intact” mentation
Anatomy of Bowel and Bladder Anatomy of Bowel and Bladder FunctionFunction
Complex interplay between sensory, motor (voluntary and Complex interplay between sensory, motor (voluntary and involuntary) and autonomic pathways at multiple levels of involuntary) and autonomic pathways at multiple levels of the nervous systemthe nervous system Frontal “micturition inhibiting area”, sensorimotor sphincter Frontal “micturition inhibiting area”, sensorimotor sphincter
control area, BG, vermis, pontine micturition centercontrol area, BG, vermis, pontine micturition center S2-S4 S2-S4
Sensory (bladder, rectum, urethra, genetalia)Sensory (bladder, rectum, urethra, genetalia) Ascends via Ascends via posteriorposterior & & anteralateralanteralateral columns columns
Motor (AHC Motor (AHC pelvic floor, pelvic floor, Onuf’s nucleus Onuf’s nucleus =sphincteromotor nucleus=sphincteromotor nucleus urethral and anal sphincters) urethral and anal sphincters)
Parasympathetics Parasympathetics detrusor contraction detrusor contraction Sympathetics T11-L1 (inermediolateral cell column)Sympathetics T11-L1 (inermediolateral cell column)
detrusor relaxation, bladder neck contractiondetrusor relaxation, bladder neck contraction Need Need bilateralbilateral pathways involved to get clinical syndrome pathways involved to get clinical syndrome

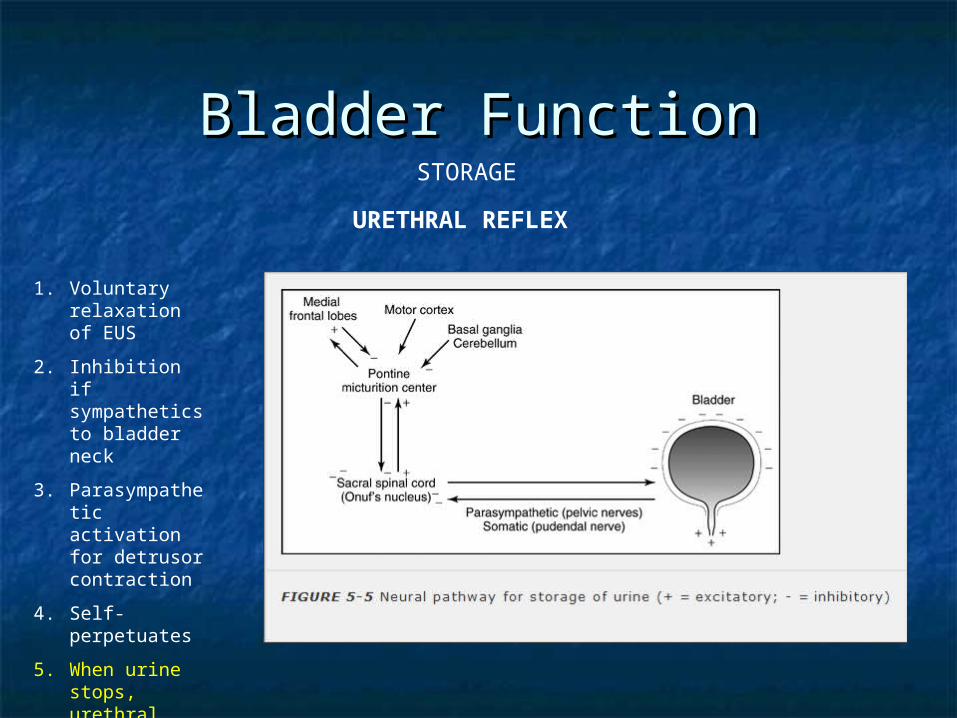
Bladder FunctionBladder FunctionVOIDING
DETRUSOR REFLEX
1. Voluntary relaxation of EUS
2. Inhibition if sympathetics to bladder neck
3. Parasympathetic activation for detrusor contraction
4. Self-perpetuates
Bladder FunctionBladder Function
1. Voluntary relaxation of EUS
2. Inhibition if sympathetics to bladder neck
3. Parasympathetic activation for detrusor contraction
4. Self-perpetuates
5. When urine stops, urethral sphincters contract triggering detrusor relaxation
STORAGE
URETHRAL REFLEX

SummarySummary
1.1. The cerebral loopThe cerebral loop involving the brainstem, cerebral cortex, and basal ganglia involving the brainstem, cerebral cortex, and basal ganglia
structuresstructures initiates and inhibitsinitiates and inhibits switching between filling and voiding states switching between filling and voiding states
2.2. Corticospinal pathways Corticospinal pathways motor cortex to pudendal motor neuronsmotor cortex to pudendal motor neurons concerned with the concerned with the voluntary controlvoluntary control of the sphincters and pelvic floor of the sphincters and pelvic floor
3.3. The urethral reflex loop The urethral reflex loop urethral afferents to pudendal motor neuronsurethral afferents to pudendal motor neurons maintains the sphincter tone when the maintains the sphincter tone when the detrusor is inactivedetrusor is inactive
4.4. The detrusor reflex loop The detrusor reflex loop detrusor afferents to pudendal motor neuronsdetrusor afferents to pudendal motor neurons sphincter relaxation when the sphincter relaxation when the detrusor is activedetrusor is active
5.5. The cord loop The cord loop brainstem structures to the conus medullarisbrainstem structures to the conus medullaris coordinatescoordinates detrusor and sphincter contraction and relaxation detrusor and sphincter contraction and relaxation
Lesion Location & Clinical Lesion Location & Clinical SyndromeSyndrome
Bilateral medial frontal lesion (parasaggital meningioma)Bilateral medial frontal lesion (parasaggital meningioma) Removal of conscious control over sphincter/bladder, when to Removal of conscious control over sphincter/bladder, when to
initiate/halt initiate/halt voiding, with intact reflex arcvoiding, with intact reflex arc Below pontine micturition center, above conusBelow pontine micturition center, above conus
Interrupt Interrupt pathways that are pathways that are inhibitoryinhibitory to the detrusor and those that to the detrusor and those that coordinate coordinate normal sphincter-detrusor activity normal sphincter-detrusor activity
Flaccid, acontractileFlaccid, acontractile evolves over wks to months evolves over wks to months Reflex contraction of uretheral sphincterReflex contraction of uretheral sphincterretentionretention Detrusor-sphincter dyssnergia; increased and uncoordinated, Detrusor-sphincter dyssnergia; increased and uncoordinated,
antagonisticantagonistic Examples: TM, MS, traumaExamples: TM, MS, trauma
Peripheral nerves or S2-S4Peripheral nerves or S2-S4 Flaccid, areflexic resembling acontractile typeFlaccid, areflexic resembling acontractile type Overflow + stress incontinenceOverflow + stress incontinence
Eg. DB, conus or cauda lesion Eg. DB, conus or cauda lesion Due toDue to
Loss of parasympatheticsLoss of parasympathetics Loss of afferents from urethra and bladderLoss of afferents from urethra and bladder

Bowel FunctionBowel Function
Also mediated by medial frontal lobesAlso mediated by medial frontal lobes Players:Players:
Internal smooth sphincter + GI motility Internal smooth sphincter + GI motility (parasympathetics)(parasympathetics)
External striated sphincter (Onuf)External striated sphincter (Onuf) Pelvic floor muscles (S2-S4 AHC)Pelvic floor muscles (S2-S4 AHC)
Etiologies: damage at any levelEtiologies: damage at any level Acute lesionsAcute lesions flaccid sphincter and loss flaccid sphincter and loss
of sacral PS of sacral PS constipation constipation
Take HomeTake Home
DCMLDCML ALSALS Thalamus; specific relaysThalamus; specific relays Somatosensory CortexSomatosensory Cortex
Somatotopy!Somatotopy! Lesions localizable and recognizableLesions localizable and recognizable Imaging and paraclinical will help Imaging and paraclinical will help
determine etiology of lesiondetermine etiology of lesion

ReferencesReferences
BlumenfeldBlumenfeld BrazisBrazis Pain articles:Pain articles:
Basic Science of Pain, J Bone Joint Surg Am. 2006;88:58-62.
The Cerebral Signature of Pain and its Modulation, Neuron, Aug 2nd, Vol 55, 2007
Cord Syndromes WebsiteCord Syndromes Website http://www.neuroanatomy.wisc.edu/
SClinic/Myelo/Myelbase.htm

Merci!Merci!
San Francisco, August 2009
Trivia TimeTrivia TimeSplit into 2 teams.Split into 2 teams.
Scorekeeper needed.Scorekeeper needed.
Multiple Multiple Choice Q’sChoice Q’s
The The ThalamusThalamus
SomatotopySomatotopy++
Cord Cord Syndromes Syndromes 11
MiscellaneoMiscellaneousus
Somatosensory JeopardySomatosensory Jeopardy
Easy
Medium
Hard
1
2
3
Easy Easy Easy Easy
Medium
Medium Medium Medium
Hard Hard Hard Hard
Points
MCQ 1MCQ 1
Name the different levels that pain Name the different levels that pain perception is modulatedperception is modulated
a)a) PeripheralPeripheral
b)b) SpinalSpinal
c)c) Supraspinal Supraspinal
d)d) None of the aboveNone of the above
e)e) All of the above (excluding choice D)All of the above (excluding choice D)

MCQ 2MCQ 2
Where does the 2Where does the 2ndnd order neuron in order neuron in the DCML system take off from, if I the DCML system take off from, if I were to touch my toe?were to touch my toe?
a)a) Clarke’s nucleusClarke’s nucleusb)b) Intermediolateral cell columnIntermediolateral cell columnc)c) ThalamusThalamusd)d) Rexed lamina IIRexed lamina IIe)e) Nucleus gracilisNucleus gracilis

MCQ 3MCQ 3
At which layer in the cerebral At which layer in the cerebral neocortex do most afferents neocortex do most afferents terminate in?terminate in?
1.1. IIII
2.2. IIIIII
3.3. IVIV
4.4. VIVI
5.5. VV
Thalamus 1Thalamus 1
What is the broad classification What is the broad classification scheme for thalamic projections?scheme for thalamic projections?
Thalamus 2Thalamus 2
Where does the pulvinar project to?Where does the pulvinar project to? BonusBonus
In what condition can we see the “pulvinar In what condition can we see the “pulvinar sign” on MRI?sign” on MRI?
Thalamus 3Thalamus 3
Name 5 specific relay nucleiName 5 specific relay nuclei
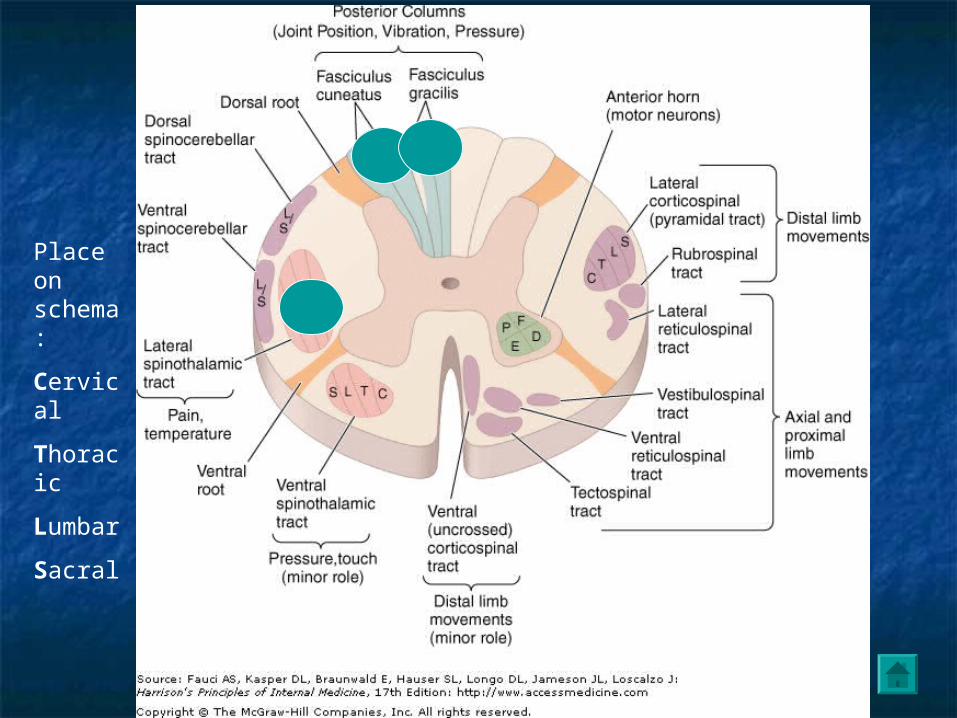
Somatotopy 1Somatotopy 1
Place on schema:
Cervical
Thoracic
Lumbar
Sacral

Somatotopy 2Somatotopy 2
Which pathway in the ALS convey’s Which pathway in the ALS convey’s the emotional and arousal aspects of the emotional and arousal aspects of pain?pain?
Somatotopy 3Somatotopy 3
What “built-in” system is heavily What “built-in” system is heavily involved in intrinsic pain modulation?involved in intrinsic pain modulation? Name 4 key players involved in pain Name 4 key players involved in pain
controlcontrol

Cord Syndromes 1Cord Syndromes 1
24 yo F, followed in psychiatry for schizoaffective 24 yo F, followed in psychiatry for schizoaffective d/od/o
3 mo Hx “walking on clouds”, can’t feel soles3 mo Hx “walking on clouds”, can’t feel soles Mild weakness in LE’sMild weakness in LE’s Impaired JPS, VibImpaired JPS, Vib + Romberg sign + Romberg sign
Where is the lesion?Where is the lesion? Ddx?Ddx?
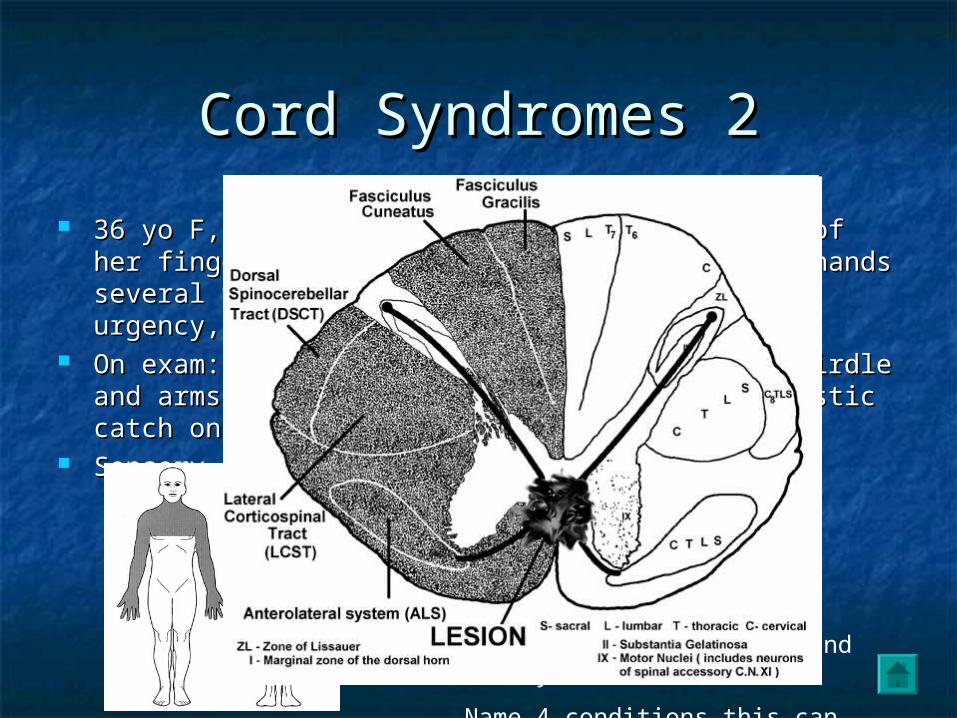
Cord Syndromes 2Cord Syndromes 2
36 yo F, complaining of not feeling the tips of her fingers, 36 yo F, complaining of not feeling the tips of her fingers, accidentally closed car door on hands several times. Also accidentally closed car door on hands several times. Also mentions some bladder urgency, and incontinence.mentions some bladder urgency, and incontinence.
On exam: atrophy of neck muscles / scapular girdle and On exam: atrophy of neck muscles / scapular girdle and arms, asymmetrically hyporeflexic UE, spastic catch on R arms, asymmetrically hyporeflexic UE, spastic catch on R biceps, R Horner’s syndromebiceps, R Horner’s syndrome
Sensory exam:Sensory exam: Where would you place the lesion ?
What segment to image first?
How do you explain the Horner’s?
How about the mixed UMN and LMN syndrome?
Name 4 conditions this can occur in?
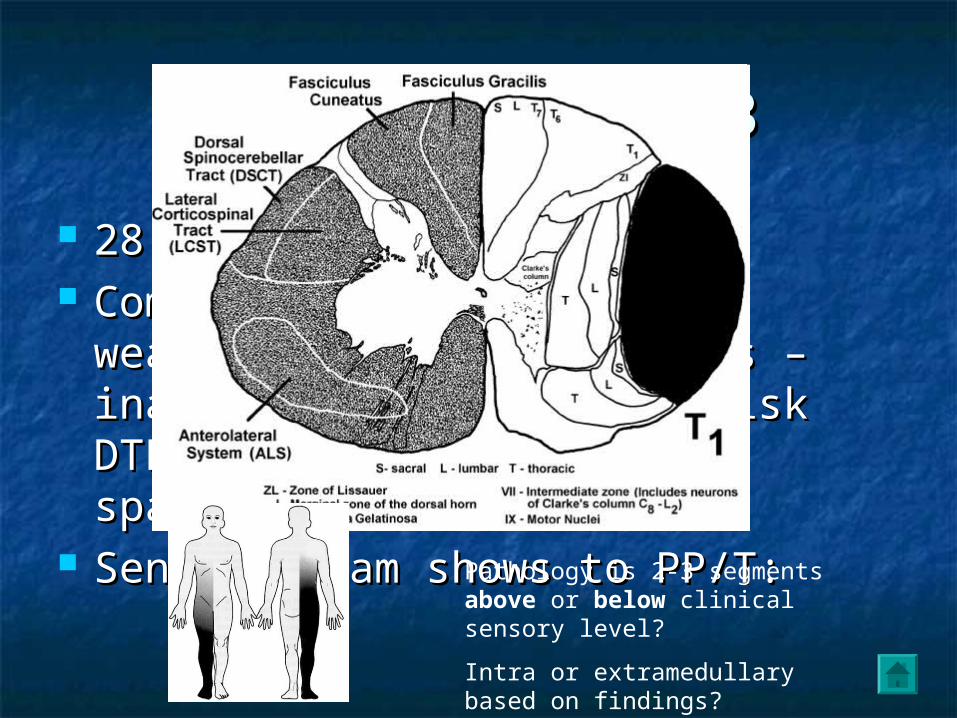
Cord Syndromes 3Cord Syndromes 3
28 yo M28 yo M Complaining of L sided weakness, Complaining of L sided weakness,
bladder fullness – inability to void. bladder fullness – inability to void. O/E brisk DTR’s on L HB, L sided O/E brisk DTR’s on L HB, L sided spacticityspacticity
Sensory exam shows to PP/T:Sensory exam shows to PP/T:Pathology is 2-3 segments above or below clinical sensory level?
Intra or extramedullary based on findings?

Miscellaneous 1Miscellaneous 1
63 yo M63 yo M HTN/DB/DLPDHTN/DB/DLPD Awoke yesterday with patchy numbness to Awoke yesterday with patchy numbness to
R face, hands, feetR face, hands, feet O/EO/E
R HB decreased sensationR HB decreased sensation No weakness appreciatedNo weakness appreciated Reflexes 2+ symmetric UE, LEReflexes 2+ symmetric UE, LE Plantars flexorPlantars flexor
L VPLL VPLWhere could you propose one lesion to account for these symptoms? Etiology?
Miscellaneous 2Miscellaneous 2
At what level is Onuf’s nucleus?At what level is Onuf’s nucleus? What is it’s function?What is it’s function?
Bonus: On a completely unrelated Bonus: On a completely unrelated questionquestion Where is the Where is the internal arcuate fibersinternal arcuate fibers??

Miscellaneous 3Miscellaneous 3
76 F76 F OA/ Cx and Lx DDD/HTN/DBOA/ Cx and Lx DDD/HTN/DB Complains of weakness in hands > legs x 2/12Complains of weakness in hands > legs x 2/12 Clumsy handsClumsy hands ProgressiveProgressive ““zinging” down spine when flexes head forwardzinging” down spine when flexes head forward Urinary frequency / some urge incontinenceUrinary frequency / some urge incontinence O/EO/E
Decreased PP/T on L from T4 distallyDecreased PP/T on L from T4 distally Decreased ST on R T2 distallyDecreased ST on R T2 distally Spastic catch R elbowSpastic catch R elbow Mild pyramidal weakness RUEMild pyramidal weakness RUE FDI, hand intrinsic atrophy+FDI, hand intrinsic atrophy+ Extensor plantar on R, diffusely brisk DTR’s on R HBExtensor plantar on R, diffusely brisk DTR’s on R HB
What segment of the CNS would you image?
What do you think is the pathophysiology?

Spondylotic myelopathySpondylotic myelopathy