Embed Size (px)
Citation preview

– 846 –
Chinese Journal of Natural Medicines 2018, 16(11): 08460855
doi: 10.3724/SP.J.1009.2018.00846
Chinese Journal of Natural Medicines
Sodium tanshinone IIA sulfonate attenuates cardiac dysfunction and improves survival of rats with cecal ligation and
puncture-induced sepsis
MENG Zheng-Jie1, 2, WANG Chao3, MENG Ling-Tong2, BAO Bei-Hua4,
WU Jin-Hui2*, HU Yi-Qiao2* 1 College of Biotechnology and Pharmaceutical Engineering, Nanjing Tech University, Nanjing 211816, China; 2 State Key Laboratory of Pharmaceutical Biotechnology, Medical School, Nanjing University, Nanjing 210093, China; 3 School of Pharmaceutical Sciences, Nanjing Tech University, Nanjing 211816, China; 4 Jiangsu Key Laboratory for High Technology of Traditional Chinese Medicine Formulae Research, College of Pharmacy, Nan-jing University of Chinese Medicine, Nanjing 210023, China
Available online 20 Nov., 2018
[ABSTRACT] Cardiac dysfunction, a common consequence of sepsis, is the major contribution to morbidity and mortality in patients. Sodium tanshinone IIA sulfonate (STS) is a water-soluble derivative of Tanshinone IIA (TA), a main active component of Salvia miltiorrhiza Bunge, which has been widely used in China for the treatment of cardiovascular and cerebral system diseases. In the pre-sent study, the effect of STS on sepsis-induced cardiac dysfunction was investigated and its effect on survival rate of rats with sepsis
was also evaluated. STS treatment could significantly decrease the serum levels of C-reactive protein (CRP), procalcitonin (PCT),
cardiac troponin I (cTn-I), cardiac troponin T (cTn-T), and brain natriuretic peptide (BNP) in cecal ligation and puncture (CLP)-induced) septic rats and improve left ventricular function, particularly at 48 and 72 h after CLP. As the pathogenesis of septic
myocardial dysfunction is attributable to dysregulated systemic inflammatory responses, several key cytokines, including tumor ne-crosis factor-α (TNF-α), interleukin-1β (IL-1β), interleukin-6 (IL-6), interleukin-10 (IL-10) and high mobility group protein B1 (HMGB1), were detected to reveal the possible mechanism of attenuation of septic myocardial dysfunction after being treated by STS.
Our study showed that STS, especially at a high dose (15 mgkg–1), could efficiently suppress inflammatory responses in myocardium
and reduce myocardial necrosis through markedly reducing production of myocardial TNF-α, IL-6 and HMGB1. STS significantly improved the 18-day survival rate of rats with sepsis from 0% to 30% (P < 0.05). Therefore, STS could suppress inflammatory re-sponses and improve left ventricular function in rats with sepsis, suggesting that it may be developed for the treatment of sepsis.
[KEY WORDS] Sodium tanshinone II A sulfonate; Sepsis; Cardiac dysfunction; Cytokine; Cecal ligation and puncture model
[CLC Number] R965 [Document code] A [Article ID] 2095-6975(2018)11-0846-10
Introduction
Sepsis is a pathological state that results from a harmful
or damaging host response to infection. Overproduction of
host inflammatory cytokines, such as TNF-α and IL-1β, could
be induced by invasion of microorganisms into the blood
stream or absorption of toxins (such as LPS) in a local site,
[Received on] 18-May-2017 [*Corresponding author] Tel: 86-25-83596143, E-mail: wuj@nju. edu.cn (WU Jin-Hui); Tel: 86-25-83596143, E-mail: huyiqiao@nju. edu.cn (HU Yi-Qiao) These authors have no conflict of interest to declare.
which up-regulate the expression of other inflammatory cyto-
kines in turn [1]. Sepsis is characterized by hypotension, hy-
poperfusion and organ dysfunction, while the abnormal ex-
cessive accumulation of multiple inflammatory cytokines
contribute to multiple organ failure, hypotension, hypoperfu-
sion and mortality. It is shown that sepsis is the most common
cause of death among critically ill patients in non-coronary
intensive care units (ICU) [2], and the annual cost of hospital
treatment of sepsis is very high. Therefore, sepsis is an im-
portant public health problem.
Salvia miltiorrhiza Bunge is traditionally used to treat
cardiovascular and cerebral system diseases in China [3-5].
Four decades of research has revealed that Tanshinone IIA (TA)

MENG Zheng-Jie, et al. / Chin J Nat Med, 2018, 16(11): 846855
– 847 –
is not only the important quality control compound [6-10], but
also a major active compound for Salvia miltiorrhiza Bunge
and its formulations [11-16]. However, clinical use of TA is
limited by its hydrophobicity. Thus, Sodium tanshinone IIA
sulfonate (STS), a water-soluble derivative of TA, is developed.
It is found that STS possesses similar pharmacological activi-
ties to TA and can also be used to treat cardiovascular and
cerebral system diseases, such as cardiomyocyte hypertrophy [17],
myocardial infarction, myocardial ischemia-reperfusion
injury [18], myocardial fibrosis [19], and stroke [20]. Additionally,
STS is further found to have multiple pharmacological effects,
including anti-dyslipidemia, inhibition of fatty acid beta-
oxidation [18], modulation of ROS, anti-fibrotic effect [19],
enhancement of mesenteric perfusion [21], and reduction of
inflammatory cytokines [22]. These performances reflect the
medical application of STS being no longer limited in angio-
cardiopathy. Pulmonary edema, pulmonary arterial hyperten-
sion [23], hepatitis [24] and diabetic neuropathy [25] have be-
come the new indications of STS.
The abnormal accumulation of various inflammatory cy-
tokines plays a key role in the pathophysiology of sepsis and
cardiac dysfunction is the most important cause for mortality
in sepsis. Previous studies have shown that STS can reduce
the secretion of some inflammatory cytokines and has an
excellent protective effect on cardiac myocytes [18]. It seems
that STS could be used for the treatment of septic cardiac
dysfunction. However, to the best of our knowledge, there are
few studies available on the efficacy of STS in sepsis rats, and
the mechanisms of the protective effects of STS in septic
cardiac dysfunction have not yet revealed. In the present study,
the therapeutic capacity of STS on sepsis-induced cardiac
dysfunction and sepsis related inflammatory cytokines were
systematically evaluated in animal model of cecal ligation and
puncture (CLP)-induced sepsis. Furthermore, the effect of STS
on the survival rate of the rats with sepsis was also evaluated.
Materials and Methods
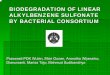
Chemicals and reagents STS was prepared by Shanghai No. 1 Biochemical &
Pharmaceutical Co. Ltd., Shanghai, China (Purity 99.1%, Product number: DS-1210001) according to chemical reactions shown in Fig. 1A. Briefly, 2.4 mL of glacial acetic acid and 4 mL of acetic anhydride were added into 1 g TA (Xi’an Hon-son Biotechnology Co., Ltd., Xi’an, China; Batch number: 100401, Purity 95.9%, Fig. 1B). The mixture was kept at 10 °C with agitation, and 2 mL of the mixed liquor (Vsulphuric acid : Vglacial acetic acid = 1 : 1) was added into the mixture dropwise. Then the reaction mixture was kept at room temperature for 1 h with agitation. After that, the reaction mixture was poured into equal-volume distilled water very slowly, to which 20 mL of saturated sodium chloride solution was added immediately. The mixture was centrifugated; the semi-finished product was obtained, washed twice with saturated sodium chloride solu-
tion, and dried on a water bath. The dried semi-finished product was refluxed with chloroform for 8 h to remove un-sulfonated liposoluble components, and sodium chloride was removed by refluxed with dehydrated alcohol. Finally, the refined STS was prepared by recrystallization using dehy-drated methanol, and its purity was analyzed by a Dionex HPLC (Ultimate 3000, Thermo Fisher Scientific, Shanghai, China). The data are shown in Fig. 1C. To prepare the regent used in the present study, 5 mg STS was dissolved into 1 mL of saline as a stock solution. The stock solution was sterilized by passing through a membrane filter with pore size of 220 nm.
ELISA kits for the detection of rat brain natriuretic pep-tide (BNP), C-reactive protein (CRP), procalcitonin (PCT), cardiac troponin-I (cTn-I), cardiac troponin-T (cTn-T), inter-leukin-1β (IL-1β), interleukin-6 (IL-6), interleukin-10 (IL-10), tumor necrosis factor-α (TNF-α), and high-mobility group protein B1 (HMGB1) were purchased from Bio-Swamp Life Science (Shanghai, China). HPLC Analysis
All samples were analyzed by a Dionex HPLC (Ultimate 3000, Thermo Fisher Scientific, Shanghai, China) equipped with a quaternary pump, a vacuum degasser, an UV detector, a column heater-cooler, and Chrome Leon software system. For TA analysis, an ODS2 C18 column (250 mm × 4.6 mm id, 5.0 µm particle size, Hypersil, Thermo Fisher Scientific, Shanghai, China) was used at room temperature, and mobile phase consisted of water and methanol (V/V = 25 : 75) at a flow rate of 1.0 mL·min−1. The detection wavelength was set at 270 nm. For STS analysis, a Hyper 0DS2 C18 column (250 mm × 4.6 mm id, 5.0 µm particle size) was used at room temperature, and mobile phase consisted of water, 0.1% phosphoric acid solution and alcohol (V/V/V = 80 : 10 : 10) at a flow rate of 1.0 mL·min−1. The detection wavelength was set at 220 nm. Standard TA and STS were purchased from National Institutes for Food and Drug Control (Beijng, China). Cecal ligation and puncture model of sepsis
All the animals were housed and handled in accordance to a protocol approved by Laboratory Animal Care and Use Committee of Jiangsu Province [SYXK (SU) 2014-0001]. CLP was performed on Sprague-Dawley (SD) specific patho-gen-free (SPF) rats (half male and half female) aged 8 weeks (weighing 220−280 g) [26]. All of SPF rats were purchased from Qinglongshan Animal Breeding Center, Nanjing, China, and were reared under SPF conditions at a rodent production facility in Jiangsu Provincial Institute of Materia Medica, (Nanjing, China). The rats were acclimated for 1 week with free access to food and tap water prior to CLP. Briefly, the rats were anesthetized with isoflurane, and the cecum was isolated via laparotomy. Approximately 30% of the cecum from the cecal tip was ligated using a 4-0 silk suture. Cecum was through- and-through punctured with a 21-gauge needle from mesenteric toward antimesenteric direction after ligation and gently squeezed to express approximately 1 mm column of feces. Wound closure was performed by applying simple

MENG Zheng-Jie, et al. / Chin J Nat Med, 2018, 16(11): 846855
– 848 –
running sutures to the abdominal musculature and skin. In sham-operated rats (Sham group), the cecum was isolated, but neither ligation nor punctured was performed. After surgery, all the rats were immediately received prewarmed normal saline
subcutaneously (37 °C, 5 mL/100 g). At the end of the surgi-cal procedure, the rats were returned to cages in a tempera-ture-controlled room (22 °C) immediately, with free access to tap water and food.
Fig. 1 A, The synthetic route of sodium tanshinone IIA sulfonate. B, HPLC analysis for tanshinone IIA. C, HPLC analysis for sodium tanshinone II A sulfonate
Treatment
120 SD rats (SPF grade) were randomly divided into the following four groups and underwent surgery and drug ad-ministration accordingly (n = 30): Sham group (equal volume of normal saline), CLP group (equal volume of normal saline),
STS low dose group [CLP + STS low dose, 5 mgkg–1 (1 mL·kg−1), equal to the lowest effective dosage in humans], STS high
dose group [CLP + STS high dose, 15 mgkg–1 (3 mL·kg−1), equal to three times as much as the lowest effective dosage in humans]. All the animals received the first drug administra-tion right after the surgery via caudal vein injection, repeated every 24 h for 3 days. Ten rats from each group were ran-domly selected at 24, 48, and 72 h after drug administration
for determination of cardiac function and measurement of levels of cytokines in heart tissue and serum. Heart tissues were collected for histologic analysis of myocardial damage. Details of heart tissue sample solutions and serum sample preparation and histologic analysis of heart tissues were listed in the following sections. Determination of cardiac function
The right carotid artery was exposed, and the distal end of the artery was ligatured. A small incision was then made in the artery and the polyethylene (PE)-50 catheter filled with heparin-saline was inserted into the artery, and the catheter was attached to a pressure transducer. After recording the mean arterial pressure (MAP) of the rat for 10 min, the PE-50

MENG Zheng-Jie, et al. / Chin J Nat Med, 2018, 16(11): 846855
– 849 –
catheter was then inserted into the left ventricle of rat to col-lect hemodynamic parameters, including dp/dtmax, –dp/dtmax, LVSP and LVEDP. The heart rates of rats were recorded throughout the experiment. Measurement of serum biomarkers
The rats were anesthetized by i.p. injection of 2% (W/W)
pentobarbital sodium [40 mgkg–1 (2 mL·kg−1)] and then were sacrificed by bleeding after cardiac function determination experiments, and blood samples were collected. Serum levels of CRP, PCT, BNP, cTn-I, and cTn-T were measured with ELISA assay kits. Measurement of myocardial inflammatory cytokines
100 mg myocardium collected from each of the rats after cardiac function determination experiments was homogenized in 900 µL of precooled normal saline via a homogenizer at 0 °C.
Myocardial homogenates were then centrifugated at 6000 rmin–1 for 10 min at 4 °C. Supernatants were collected for the meas-urement of cytokines, including IL-1β, IL-6, IL-10, TNF-α, and HMGB1. Histologic analysis of myocardial damage
At the end of cardiac function determination, the rats were killed with an overdose of diethyl ether, and part of heart of each rat was removed for histological study. The hearts were immediately washed in precooled PBS (1 ×, 4 °C) to remove blood clot, fixed in 4% paraformaldehyde at least for 24 h, and then embedded in paraffin. The heart tissues were sectioned at 4-µm thick and mounted on glass slides. The slides were stained with hematoxylin-eosin (H&E). For each
rat, at least 10 high power (400 ×) fields were examined. All the sections were examined in a blinded manner. A semiquan-titative grading system described by Nyska [27] was employed to evaluate the extent of cardiac inflammation: minimal (grade 1) changes involved 1%–10% of the section; mild (grade 2) involved 11%–40%; moderate (grade 3) involved 41%–80%; and severe (grade 4) involved 81%–100%. Survival analysis
Additional 40 SD rats (SPF grade) were chosen for survival experiment. Grouping (n = 10 in each group) and drug admini-stration procedures were the same as above. The treatments lasted for 18 days with no antibiotic treatment provided and survival was monitored every day throughout the experiment. Statistical analysis
All the data were presented as means ± SD (standard de-viation). Differences in cardiac function, serum and myocar-dial inflammatory cytokines among the groups were deter-mined with one-way analysis of variance (ANOVA). Kaplan- Meier survival curves were compared using a log-rank test. A P value < 0.05 was considered statistically significant.
Results
Effects of STS on cardiac function To determine the therapeutic effects of STS on myocar-
dial dysfunction in the CLP rats, cardiac hemodynamics were determined, and the results are shown in Fig. 2. In the sham group, the hemodynamics, such as mean arterial pressure (MAP), maximal rate of rise of left ventricular pressure (dp/dtmax),
Fig. 2 Dose-dependent effects of sodium tanshinone II A sulphonate (STS) on the cardiac function during sepsis. STS at doses of
5 and 15 mgkg–1 or equal volume of normal saline were i.v. administered immediately post-CLP or sham surgery. Drug/saline administration was repeated every 24 h for 3 days. The rats were randomly selected for cardiac hemodynamics assay at 24, 48 and 72 h post-CLP or sham surgery. Values are means ± SD, n = 10. †P < 0.05, ††P < 0.01 vs sham group; *P < 0.05, **P < 0.01 vs CLP group

MENG Zheng-Jie, et al. / Chin J Nat Med, 2018, 16(11): 846855
– 850 –
decline of the left ventricular pressure (–dp/dtmax), ventricular systolic pressure (LVSP), left ventricular end-diastolic pressure (LVEDP) and heart rate (HR), remained stable throughout the entire postoperative observation, which indicated that sham operation had no significant effect on cardiac function. Com-pared with the sham group, the CLP surgery showed damages to the cardiac functions; the longer the postoperative time, the worse the outcome, such as continuing decrease in MAP (P < 0.01 at 24, 48, and 72 h) and HR (P < 0.05 at 24 and 48 h, P < 0.01 at 72 h). The hemodynamic parameters in the CLP group also indicated left ventricular dysfunction, such as decreased LVSP (P < 0.05 at 24 h, P < 0.01 at 48 and 72 h), reduced dp/dtmax (P < 0.05 at 48 h, P < 0.01 at 72 h) and –dp/dtmax (P < 0.01 at 48 and 72 h), and increased LVEDP (P < 0.01 at 24 h, P < 0.05 at 48 h, and 72 h). The low dose of STS partially improved cardiac function, showing increased MAP level at 48 h (P < 0.05), increased dp/dtmax at 72 h (P < 0.05), in-creased –dp/dtmax at 24 h (P < 0.05) and 72 h (P < 0.01), and decreased LVEDP at 24 h (P < 0.05). Compared with the low dose STS, high dose of STS had much better effects on heart dysfunction, showing significantly increased MAP level (P < 0.01 at 24 h, P < 0.01 at 48 h and P < 0.05 at 72 h) and sig-nificantly decreased LVEDP throughout the whole postopera-tive period (P < 0.05 at 24, 48, and 72 h), and increased dp/dtmax (P < 0.05 at 72 h) and –dp/dtmax (P < 0.05 at 48 h and P < 0.01 at 72 h). Besides these results, the LVSP value was markedly increased at the 72 h for the high dose STS group (P < 0.05). Thus, it could be concluded that STS had the ability to
enhance the left ventricular systolic and diastolic functions. Effects of STS on serum biomarkers
The results of our study indicated that the serum concen-trations of CRP and PCT in the CLP rats increased signifi-cantly (Figs. 3A and 3B, P < 0.05 at 24 and 48 h, P < 0.01 at 72 h), while the two biomarkers remained stable in the sham group during the entire postoperative period. Such significant alterations of serum CRP and CLP levels suggested that se-vere septic status was achieved via CLP operation in our ex-periment. As shown in Figs. 3A and 3B, STS treatment re-duced the the CRP and PCT levels at 48 h after surgery. The low dose STS significantly reduced the plasma concentration of CRP at 48 and 72 h (P < 0.05), and the PCT level at 72 h (P < 0.01). The similarly therapeutic effects were observed in high dose group, with significant reduction of the PCT level at 48 h (P < 0.05) and much lower level of CRP and PCT at each time point compared with that of the low dose group. These results suggested that STS treatment could attenuate the severity of sepsis.
Myocardial dysfunction often accompanies severe sepsis. In order to evaluate this dysfunction in the CLP rats and monitor the therapeutic effects of STS on myocardial dys-function, cTn and BNP levels were detected in different groups. Although cardiac troponin is composed of three sub-units C, I and T, only cTn-I and cTn-T are ideally suited for the detection of myocardial damage since these two cytokines are expressed as cardio-specific isoforms [28]. CLP surgery significantly increased the serum concentrations of cTn-I and
Fig. 3 Effects of sodium tanshinone II A sulphonate (STS) on serum biomarkers levels in rats with sepsis. STS at doses of 5 and
15 mgkg–1 or equal volume of normal saline were i.v. administered immediately post-CLP or sham surgery. Drug/saline admini-stration was repeated every 24 h for 3 days. Blood samples were collected at 24, 48, and 72 h post-CLP or sham surgery. Serum levels of biomarkers are shown as means ± SD, n = 10. †P < 0.05, ††P < 0.01 vs sham group; *P < 0.05, **P < 0.01 vs CLP group

MENG Zheng-Jie, et al. / Chin J Nat Med, 2018, 16(11): 846855
– 851 –
cTn-T, which indicated a severe myocardial dysfunction. The low dose STS treatment had limited attenuating effects on cTn-I and cTn-T, and only could significantly reduce the cTn-T level at 48 h (P < 0.05), and the cTn-I levels were still significantly higher than that in the sham group (P < 0.05 at 24 and 48 h). The high dose STS treatment significantly de-creased the serum concentration of cTn-T at the three time points (P < 0.05), and also remarkably lowered the cTn-I level at 72 h (P < 0.05). The serum concentration of cTn-I and cTn-T in the high dose STS group approached to the levels seen in the sham group. The beneficial effects of high dose STS on cTn-I and cTn-T levels were better than that of low dose STS at 48 and 72 h after surgery.
BNP is another diagnostic marker for myocardial dys-function which is also a useful predictor of mortality in sepsis [29]. CLP surgery increased the BNP level at 24, 48, and 72 h (P < 0.01). Although low dose STS reduced the BNP serum con-centration during the whole experiment, and even signifi-cantly decreased the BNP level at 24 h (P < 0.01), compared with the CLP group, the BNP level at all the time points were still higher than that in the sham group. On the contrary, com-pared with CLP group, high dose STS treatment remarkably decreased the BNP level (P < 0.01 at 24 h, P < 0.05 at 48 and 72 h). No significant differences in BNP levels were observed between the sham group and the STS high dose group. Altera-tions of cTn-I level and BNP level in STS treatment groups suggested that STS might lessen myocardial dysfunction in the CLP rats. Taking the effects of STS on cardiac function
into consideration, STS could actually attenuate cardiac dys-function in CLP rats. Effects of STS on myocardial inflammatory cytokines
CLP surgery significantly increased the levels of TNF-α, IL-1β, IL-6 IL-10 and HGMB1 at each time point, indicating severe inflammation in myocardium (Fig. 4, P < 0.01 or P < 0.05). High dose STS treatment began to remarkably decrease the TNF-α concentration in myocardium at 48 h (Fig. 4A, P < 0.05), and the therapeutic effect lasted to 72 h (P < 0.01). Both low dose and high dose STS could decrease the myo-cardial IL-1β level. The effect of STS on IL-6 secretion was similar to that on IL-1β secretion, except for a significant decreasing effect of high dose STS observed at 48 h (Fig. 4C, P < 0.05) and 72 h (P < 0.05). STS treatment had no effect on IL-10 secretion (Fig. 4D). The myocardial IL-10 levels in the CLP group and treatment groups were still at the same level after drug administration. Compared with the CLP group, high dose STS could markedly decrease the myocardial HMGB1 level in a continuous mode throughout the experi-ment (Fig. 4E, P < 0.05). The results from this experiment revealed that STS could decrease the concentrations of pro-inflammatory cytokines (TNF-α, IL-1β and IL-6) and HMGB1 in myocardium, which was beneficial for the con-trol of myocardial inflammation and could lessen the degree of damage to the myocardium. It was also noteworthy that STS treatment had little influence on IL-10 levels, indicat-ing that it might have limited effects on proinflammatory cytokine feedback system.
Fig. 4 Effects of sodium tanshinone II A sulphonate (STS) on myocardial inflammatory cytokine levels in rats with sepsis. STS at doses of 5 and 15 mgkg–1 or equal volume of normal saline were i.v. administered immediately post-CLP or sham surgery. Drug/saline administration was repeated every 24 h for 3 days. Heart samples were collected at 24, 48, and 72 h post-CLP or sham surgery. Myocardial homogenates were prepared for measurement of inflammatory cytokine levels. Cytokine levels are shown as means ± SD, n=10. †P < 0.05, ††P < 0.01 vs sham group; *P < 0.05, **P < 0.01 vs CLP group

MENG Zheng-Jie, et al. / Chin J Nat Med, 2018, 16(11): 846855
– 852 –
Effects of STS on myocardial damage The results of histopathological evaluation are shown in
Fig. 5, and the inflammation scores are shown in Fig. 5M. In the sham group, minimal histological changes could be found, such as few acidophilic degenerations, and there was no in-flammation associated with sham surgery at the three time points (Figs. 5A, 5E, and 5I). The inflammation almost in-creased to grade 3 at the 24 h after CLP surgery (Fig. 5M).
Myocardial interstitial edema and inflammatory infiltration were obviously observed in the CLP group (Fig. 5B). The longer the postoperative time, the severer the inflammation in the CLP group. The inflammation increased to about grade 4 at 72 h (Fig. 5M), and necrosis was found (Figs. 5F and 5J). Low dose STS could attenuate the myocardial damage, which was represented as lower inflammatory scores and absence of necrosis.
Fig. 5 From A to L, Representative histopathology of heart tissue. After CLP surgery, there were significant inflammatory infil-tration, disorganization of cardiomyocytes, myocardial interstitial edema and necrosis in the CLP group, while only few aci-dophilic degenerations were observed in the sham group. Sodium tanshinone II A sulphonate (STS) attenuated the sepsis-induced myocardial damage in a dose-dependent manner. Black arrow, acidophilic degeneration; blue arrow, inflammatory infiltration; green arrow, myocardial interstitial edema; yellow arrow, necrosis (hematoxylin & eosin, original magnification × 200, n = 10). M, Inflammatory score of heart tissues. Each slide was stained with hematoxylin-eosin (H&E). At least 10 high power (400 ×) fields were examined. All sections were examined in a blinded manner. Values are means ± SD, n = 10. †P < 0.05, ††P < 0.01 vs sham group; *P < 0.05, **P < 0.01 vs CLP group
However, the therapeutic effect of low dose STS was
limited, inflammatory infiltration and myocardial interstitial edema still could be found (Figs. 5C, 5G, and 5K). Compared with the CLP group, high dose STS significantly decreased the inflammation scores at 48 and 72 h (Fig. 5M, P < 0.01). No obvious inflammatory infiltration and necrosis were found, and only mild interstitial edema and few acidophilic degen-erations were noted (Figs. 5D, 5H, and 5L). Effects of STS on survival ratse of rats with CLP-induced sepsis
No rat died in sham group throughout the survival ex-
periment. On the contrary, all the rats treated with normal
saline alone in CLP group died within 8 days after CLP sur-
gery (Fig. 6). However, compared with the CLP group, 60%
of rats in low dose STS group and 50% of rats in high dose
STS group died by Day 8 after surgery, and the survival rate
of the high dose STS group was significantly higher than that
of CLP group (P < 0.05). As the experiment went on, the rats
from the two STS treatment groups died, and the survival rate
fell to 20% and 30% by Day 18, respectively (Fig. 6). The
difference in overall survival rate between CLP group and
high dose group was significant (P < 0.05).
Discussion
Sepsis resulting from bacterial, viral, fungal and parasitic
Fig. 6 Effects of sodium tanshinone II A sulfonate (STS) on survival of rats with CLP-induced sepsis. STS at doses of 5 and 15 mgkg–1 or equal volume of normal saline were i.v. administered immediately post-CLP or sham surgery. Drug/saline administration was repeated every 24 h for 18 days. Survival of the rats was monitored at intervals of 24 h for 18 days. The overall difference in survival rate between the group treated with high dose of STS and the CLP control group was significant (*P < 0.05 vs CLP group), n = 10

MENG Zheng-Jie, et al. / Chin J Nat Med, 2018, 16(11): 846855
– 853 –
infections triggers the release of various inflammatory me-diators and induces cellular and organic dysfunction in the affected host [30]. There are three phases in the pathogenesis of sepsis: (1) infection of pathogenic microorganism and release of toxins; (2) release of cytokines; and (3) destructive effects of excessive specific cytokines [30]. CRP is a sensitive sys-temic marker of inflammation and tissue damage, and PCT increases markedly in serum of humans and animals with sepsis. It has been shown that PCT serum level is associated with the mortality in sepsis, and it can be a useful prediction marker in sepsis. According to 2012 international guidelines for management of severe sepsis and septic shock, plasma CRP coupled with the plasma PCT is a considerable inflam-matory variable in the diagnosis of sepsis [31]. In the present study, the serum levels of PCT and CRP in the CLP group were about two standard deviation (SD) above the level of the sham group, and the two indicators were significantly de-creased after STS treatment. It indicated that the STS could relieve inflammatory reactions in septic rats.
Cardiac dysfunction is a well-recognized complication of severe sepsis and septic shock [32]. It is also a major contribu-tor to morbidity and mortality in patients with sepsis. Cardiac dysfunction is characterized by reduced contractility, decrease in ejection fraction, and ventricular dilatation. The LVSP and the dp/dtmax are two important parameters of the left ventricu-lar systolic function, while the LVEDP and the maximal rate of –dp/dtmax predict the left ventricular diastolic function. In the present study, sepsis caused an increase in LVEDP and decreases in LVSP, ±dp/dtmax, MAP and HR in the CLP group, suggesting an early stage of heart failure. STS could signifi-cantly attenuate the cardiac dysfunction in rats with sepsis. In addition to these macroscopical changes in hemodynamic parameters, decreases in serum biomarkers, such as cTn-I, cTn-T and BNP, were also monitored after treatment with STS. It has been shown that cTn-I and cTn-T are expressed as cardio-specific isoforms, and they are predictors for the de-tection of myocardial damage [33]. BNP, secreted from atria and ventricles in response to volume load and myocardial wall stress, is another sensitive indicator for the diagnosis of cardiac dysfunction, especially for left ventricular dysfunction [34]. The results from the present study indicated that the STS could actually attenuate the cardiac dysfunction.
A critical question was then raised: what mechanism re-sulted in STS attenuating sepsis-induced cardiac dysfunction? As sepsis is associated with the abnormal host immune func-tion in response to invading pathogens and the “cytokine storm” is thought to be responsible for triggering the inflam-mation in sepsis, the effects of STS on various cytokines in myocardial tissue, including TNF-α, IL-1β, IL-6, IL-10 and HMGB1, were examined in the present study to reveal its mechanism on attenuating sepsis-induced cardiac dysfunction. Cytokines TNF-α and IL-1β are primarily secreted by macrophages and act as proinflammatory mediators. Both cytokines play a major role in initiation and regulation of
inflammation and immunity response. TNF-α and IL-1β are “proximal” cytokines, which are secreted early in sepsis [32]. Previous researches have indicated that high concentration of TNF-α induces myocardial cell apoptosis [35], has a negative inotropic effect on isolated cardiac myocytes, and decreases myofilament sensitivity to Ca2+, and that IL-1β has also been shown to increase the activity of Na+−Ca2+ exchanger [32]. Cardiomyocyte TNF-α and IL-1β secretion is responsible for myocardial depression and haemodynamic abnormalities [32]. Furthermore, these two proximal cytokines stimulate the production of IL-6, a “distal” cytokines. Unlike IL-1β and TNF-α, IL-6 does not induce cytokine expression and its main effects are to act in synergy with IL-1β and TNF-α to augment the response of immune cells to other cytokines. In addition, IL-6 can activate the coagulation system and function as a pyrogen. Inhibition of TNF-α and IL-1β expression results in a decrease in IL-6 production. In the present study, STS, par-ticularly at high dose, significantly decreased the myocardial TNF-α and IL-6 levels. However, it only decreased the myo-cardial IL-1β level slightly, and no significant differences were observed between treatment groups and CLP group. The alleviating effect of STS on IL-6 could be mainly due to its efficient decrease in TNF-α.
HMGB1 is another important proinflammatory cytokine in the pathophysiology of sepsis. HMGB1 protein is origi-nally described as a nuclear DNA-binding protein in the gene expression and transcriptional regulation. It has been func-tionally characterized as an “danger signal” or “alarmin”, and is released from activated monocytes and macrophages, pi-tuicytes, enterocytes, hepatocytes, and necrotic damaged cells [36]. Recent studies in mouse and rat models of sepsis have shown that HMGB1 can be secreted by dying or necrotic cardiomyo-cytes. Even viable cardiac myocytes have the ability of HMGB1 secretion [37]. HMGB1 modulates the membrane calcium influx and thus decreases calcium availability in car-diac myocytes. It acts as a myocardial depressant factor and has an obvious negative impact on myocardial contractile function, which is mainly manifested as decreasing LVDP, left ventricular (LV) +dP/dtmax and absolute value of LV –dP/dtmax, and increasing LV end-diastolic pressure [38]. Furthermore, HMGB1 plays a critical role in mediating organ damage in sepsis [37, 39], and HMGB1 antagonists exhibit protective roles against lethal sepsis [1]. In the present study, high dose STS significantly inhibited the myocardial HMGB1 secretion, which was beneficial to enhance the cardiac function and protecting rats with sepsis from death. As HMGB1 secretion can be affected by endotoxin or various proinflammatory cytokines, such as TNF-α and IL-1β, the suppressive effect of STS on HMGB1 secretion might be partially attributed to its excellent inhibition of myocardial TNF-α. In addition, unlike steroidal and nonsteroidal anti-inflammatory drugs, ster-oid-like STS dose-dependently attenuated endotoxin-induced HMGB1 secretion, which might also make a contribution to alleviating myocardial HMGB1 level in rats with sepsis.

MENG Zheng-Jie, et al. / Chin J Nat Med, 2018, 16(11): 846855
– 854 –
Conclusion
In conclusion, STS treatment could inhibit overproduc-tion of proinflammatory cytokines, including TNF-α, IL-6 and HMGB1, alleviating inflammatory reactions and enhanc-ing cardiac function. Therefore, STS treatment could improve the survival rate of rats with CLP-induced sepsis. The find-ings suggested that STS may be a useful candidate drug for the treatment of septic myocardial dysfunction.
Abbreviations
CRP C-reactive protein
PCT Procalcitonin
BNP Brain natriuretic peptide
cTn-I Cardiac troponin I
cTn-T Cardiac troponin T
TNF-α Tumor necrosis factor-α
IL-1β Interleukin-1β
IL-6 Interleukin-6
IL-10 Interleukin-10
HMGB1 High mobility group protein B1
ICAM-1 Intercellular adhesion molecule 1
VCAM-1 Vascular cell adhesion molecule 1
LPS Lipopolysaccharides
ROS Reactive oxygen species
LVSP Ventricular systolic pressure
LVEDP Left ventricular end-diastolic pressure
MAP Mean arterial blood pressure
HR Heart rate
dp/dtmax Maximal rate of rise of left ventricular pressure
–dp/dtmax Decline of the left ventricular pressure
ELISA Enzyme-linked immunosorbent assay
PBS Phosphate buffered saline
H&E Hematoxylin-eosin
Acknowledgments
Here we thank Professor HE Bing-Fang and all members of her research group for providing assistance in our ELISA assays. We also thank Mr. ZHONG Ye-Zhang and Miss CHEN Ying for their aids in histological analysis.
References
[1] Aziz M, Jacob A, Yang WL, et al. Current trends in inflammatory and immunomodulatory mediators in sepsis [J]. J Leukoc Biol, 2013, 93(3): 329-342.
[2] Mikkelsen ME, Shah CV, Meyer NJ, et al. The epidemiology of acute respiratory distress syndrome in patients presenting to the emergency department with severe sepsis [J]. Shock, 2013, 40(5): 375-381.
[3] Li MH, Chen JM, Peng Y, et al. Investigation of Danshen and related medicinal plants in China [J]. J Ethnopharmacol, 2008,
120(3): 419-426. [4] Su CY, Ming QL, Rahman K, et al. Salvia miltiorrhiza: Tradi-
tional medicinal uses, chemistry, and pharmacology [J]. Chin J Nat Med, 2015, 13(3): 163-182.
[5] Zhang XZ, Qian SS, Zhang YJ, et al. Salvia miltiorrhiza: A source for anti-Alzheimer’s disease drugs [J]. Pharm Biol, 2016, 54(1): 18-24.
[6] Yang DF, Liang ZS, Liu JL. LC fingerprinting for assessment of the quality of the lipophilic components of Salvia miltior-rhiza [J]. Chromatographia, 2009, 69: 555-560.
[7] Yang DF, Liang ZS, Duan QM, et al. Quality assessment of cardiotonic pills by HPLC fingerprinting [J]. Chromatographia 2007, 66: 509-514.
[8] Liu AH, Lin YH, Yang M, et al. Development of the finger-
prints for the quality of the roots of Salvia miltiorrhiza and its
related preparations by HPLC-DAD and LC-MS(n) [J]. J
Chromatogr B, 2007, 846(1-2): 32-41.
[9] Zhou L, Chow M, Zuo Z. Improved quality control method for
Danshen products--consideration of both hydrophilic and
lipophilic active components [J]. J Pharm Biomed Anal, 2006,
41(3): 744-750.
[10] Gu M, Zhang S, Su Z, et al. Fingerprinting of Salvia miltior-
rhiza Bunge by non-aqueous capillary electrophoresis com-
pared with high-speed counter-current chromatography [J]. J
Chromatogr A, 2004, 1057(1-2): 133-140.
[11] Gu M, Zhang G, Su Z, et al. Identification of major active
constituents in the fingerprint of Salvia miltiorrhiza Bunge de-
veloped by high-speed counter-current chromatography [J]. J
Chromatogr A, 2004, 1041(1-2): 239-243.
[12] Xu G, Zhao W, Zhou Z, et al. Danshen extracts decrease blood
C reactive protein and prevent ischemic stroke recurrence: a
controlled pilot study [J]. Phytother Res, 2009, 23(12): 1721-
1725. [13] Qiao Z, Ma J, Liu H. Evaluation of the antioxidant potential of
Salvia miltiorrhiza ethanol extract in a rat model of ische-mia-reperfusion injury [J]. Molecules, 2011, 16(12): 10002- 10012.
[14] Hatfield MJ, Tsurkan LG, Hyatt JL, et al. Modulation of esteri-fied drug metabolism by tanshinones from Salvia miltiorrhiza ("Danshen") [J]. J Nat Prod, 2013, 76(1): 36-44.
[15] Lin TY, Lu CW, Huang SK, et al. Tanshinone IIA, a constituent of Danshen, inhibits the release of glutamate in rat cerebrocor-tical nerve terminals [J]. J Ethnopharmacol, 2013, 147(2): 488- 496.
[16] Ren-an Q, Juan L, Chuyuan L, et al. Study of the protective mechanisms of Compound Danshen Tablet (Fufang Danshen Pian) against myocardial ischemia/reperfusion injury via the Akt-eNOS signaling pathway in rats [J]. J Ethnopharmacol, 2014, 156: 190-198.
[17] Li SS, Feng J, Zheng Z, et al. Effect of sodium tanshinone II A sulfonate on phosphorylation of extracellular signal-regulated kinase 1/2 in angiotensin II-induced hypertrophy of myocardial cells [J]. Chin J Integr Med, 2008, 14(2): 123-127.
[18] Wei B, You MG, Ling JJ, et al. Regulation of antioxidant sys-tem, lipids and fatty acid beta-oxidation contributes to the car-dioprotective effect of sodium tanshinone IIA sulphonate in isoproterenol-induced myocardial infarction in rats [J]. Athero-sclerosis, 2013, 230(1): 148-156.
[19] Yang L, Zou XJ, Gao X, et al. Sodium tanshinone IIA sul-fonate attenuates angiotensin II-induced collagen type I ex-

MENG Zheng-Jie, et al. / Chin J Nat Med, 2018, 16(11): 846855
– 855 –
pression in cardiac fibroblasts in vitro [J]. Exp Mol Med, 2009, 41(7): 508-516.
[20] Tan X, Yang Y, Cheng J, et al. Unique action of sodium tan-shinone II-A sulfonate (DS-201) on the Ca2+ dependent BK(Ca) activation in mouse cerebral arterial smooth muscle cells [J]. Eur J Pharmacol, 2011, 656(1-3): 27-32.
[21] Liu J, Morton J, Miedzyblocki M, et al. Sodium tanshinone IIA sulfonate increased intestinal hemodynamics without systemic circulatory changes in healthy newborn piglets [J]. Am J Physiol Heart Circ Physiol, 2009, 297(4): H1217-1224.
[22] Zhang Y, Li W, Zhu S, et al. Tanshinone IIA sodium sulfonate facilitates endocytic HMGB1 uptake [J]. Biochem Pharmacol, 2012, 84(11): 1492-1500.
[23] Wang J, Lu W, Wang W, et al. Promising therapeutic effects of sodium tanshinone IIA sulfonate towards pulmonary arterial hypertension in patients [J]. J Thorac Dis, 2013, 5(2): 169-172.
[24] Xu Y, Feng D, Wang Y, et al. Sodium tanshinone IIA sulfonate protects mice from ConA-induced hepatitis via inhibiting NF-kappaB and IFN-gamma/STAT1 pathways [J]. J Clin Im-munol, 2008, 28(5): 512-519.
[25] Liu Y, Wang L, Li X, et al. Tanshinone IIA improves impaired nerve functions in experimental diabetic rats [J]. Biochem Biophys Res Commun, 2010, 399(1): 49-54.
[26] Holthoff JH, Wang Z, Patil NK, et al. Rolipram improves renal perfusion and function during sepsis in the mouse [J]. J Phar-macol Exp Ther, 2013, 347(2): 357-364.
[27] Nyska A, Murphy E, Foley JF, et al. Acute hemorrhagic myo-cardial necrosis and sudden death of rats exposed to a combi-nation of ephedrine and caffeine [J]. Toxicol Sci, 2005, 83(2): 388-396.
[28] Agewall S, Giannitsis E, Jernberg T, et al. Troponin elevation in coronary vs. non-coronary disease [J]. Eur Heart J, 2011, 32(4): 404-411.
[29] Perman SM, Chang AM, Hollander JE, et al. Relationship between B-type natriuretic peptide and adverse outcome in pa-
tients with clinical evidence of sepsis presenting to the emer-gency department [J]. Acad Emerg Med, 2011, 18(2): 219-222.
[30] Sagy M, Al-Qaqaa Y, Kim P. Definitions and pathophysiology of sepsis [J]. Curr Probl Pediatr Adolesc Health Care, 2013, 43(10): 260-263.
[31] Dellinger RP, Levy MM, Rhodes A, et al. Surviving Sepsis Campaign: international guidelines for management of severe sepsis and septic shock, 2012 [J]. Intensive Care Med, 2013, 39(2): 165-228.
[32] Flynn A, Chokkalingam Mani B, Mather PJ. Sepsis-induced cardiomyopathy: a review of pathophysiologic mechanisms [J]. Heart Fail Rev, 2010, 15(6): 605-611.
[33] Agewall S, Giannitsis E. Troponin elevation in coronary ischemia and necrosis [J]. Curr Atheroscler Rep, 2014, 16(3): 396.
[34] Nishikimi T. Do plasma levels of brain natriuretic peptide (BNP) and N-terminal proBNP (NT-proBNP) increase in dia-stolic dysfunction as well as in systolic dysfunction? [J]. Circ J, 2012, 76(11): 2540-2541.
[35] Xue WL, Bai X, Zhang L. rhTNFR: Fc increases Nrf2 expres-sion via miR-27a mediation to protect myocardium against sepsis injury [J]. Biochem Biophys Res Commun, 2015, 464(3): 855-861.
[36] Andrassy M, Volz HC, Igwe JC, et al. High-mobility group box-1 in ischemia-reperfusion injury of the heart [J]. Circula-tion, 2008, 117(25): 3216-3226.
[37] Tzeng HP, Fan J, Vallejo JG, et al. Negative inotropic effects of high-mobility group box 1 protein in isolated contracting car-diac myocytes [J]. Am J Physiol Heart Circ Physiol, 2008, 294(3): H1490-1496.
[38] Hagiwara S, Iwasaka H, Uchino T, et al. High mobility group box 1 induces a negative inotropic effect on the left ventricle in an isolated rat heart model of septic shock: a pilot study [J]. Circ J, 2008, 72(6): 1012-1017.
[39] Klune JR, Dhupar R, Cardinal J, et al. HMGB1: endogenous danger signaling [J]. Mol Med, 2008, 14(7-8): 476-484.
Cite this article as: MENG Zheng-Jie, WANG Chao, MENG Ling-Tong, BAO Bei-Hua, WU Jin-Hui, HU Yi-Qiao. Sodium tanshinone IIA sulfonate attenuates cardiac dysfunction and improves survival of rats with cecal ligation and puncture-induced sepsis [J]. Chin J Nat Med, 2018, 16(11): 846-855.