Embed Size (px)
Citation preview

Social support and health-related quality of life in chronic heart failure patients
S.J. Bennett1, S.M. Perkins2, K.A. Lane2, M. Deer3, D.C. Brater2 & M.D. Murray3,4
1Indiana University School of Nursing (E-mail: [email protected]); 2Indiana University School of Medicine;3Regenstrief Health Care Institute; 4Purdue University School of Pharmacy, Indianapolis, IN, USA
Accepted in revised form 5 October 2001
Abstract
Objectives: Objectives of this study were to: (1) describe perceived social support during a baseline hos-pitalization and 12 months later among heart failure patients; (2) examine differences in social support as afunction of gender and age (less than 65 and 65 years or older); and (3) examine social support as apredictor of health-related quality of life. Background: Social support is a predictor of well-being andmortality, but little is known about support patterns among heart failure patients and how they influencequality of life. Methods: The sample included 227 hospitalized patients with heart failure who completed theSocial Support Survey and the Chronic Heart Failure Questionnaire at baseline; 147 patients completedthese questionnaires again 12 months after baseline. Results: Mean baseline and 12-month total supportscores were 56 and 53, respectively, with a score of 76 indicating the most positive perceptions of support.The ANOVA indicated significant interactions of gender by age for total (F ¼ 5:04; p ¼ 0:03) and emo-tional/informational support (F ¼ 4:87; p ¼ 0:03) and for positive social interactions (F ¼ 4:43; p ¼ 0:04),with men under age 65 perceiving less support than men aged 65 and older and women in either age group.Baseline support did not predict 12-month health-related quality of life, but changes in social supportsignificantly predicted changes in health-related quality of life (R2 ¼ 0.14). Conclusions: Overall, percep-tions of support were moderate to high, but there was wide variation in perceptions over time. Men underage 65 reported less support than other groups of patients. Importantly, changes in social support weresignificant predictors of changes in health-related quality of life.
Key words: Heart failure, Quality of life, Social support
Introduction
Health outcomes remain poor for patients withheart failure. Mortality and morbidity rates arehigh and health-related quality of life is dimin-ished [1–4]. Improving health-related quality oflife is one of the major goals of therapy for per-sons with heart failure because of its debilitatingeffects and the inability to cure it [5]. Some con-sensus exists that health-related quality of life is amultidimensional construct comprised of biologi-cal and physiological domains, symptom status,functional status, health perceptions, and thequality of life overall [6]. Characteristics of the
individual (e.g., motivation and values) and of theenvironment (e.g., social and psychological sup-ports) are proposed to influence health-relatedquality of life [6].
Approximately half of the 4.8 million peoplewith heart failure in the United States are women[1]. Recent studies suggest that quality of life ispoorer for women than men with heart failure. Ina small focus group study with 23 patients withheart failure (7 women; 16 men) designed toidentify potential self-care interventions, womenpatients reported frequent episodes of crying,tearfulness, and sadness while the men patients didnot report these problems [7].
Quality of Life Research 10: 671–682, 2001.� 2001 Kluwer Academic Publishers. Printed in the Netherlands.
671

Riedinger et al. [8] conducted a secondaryanalysis of 1382 age-matched and ejection-frac-tion-matched women (50%) and men (50%) withheart failure enrolled in the Studies of Left Ven-tricular Dysfunction (SOLVD). After controllingfor New York Heart Association class, age, andejection fraction, the women with heart failure hadsignificantly lower quality of life scores than menin activities of daily living requiring moderate ex-ertion such as climbing stairs and in social activi-ties such as visiting friends or relatives. Chin andGoldman [9] reported that, among 435 patientshospitalized with heart failure, women (n ¼ 90)had significantly lower scores in vitality andphysical functioning than men. At 12 months afterbaseline, women had less improvement than menin their physical functioning, leading the investi-gators to conclude that women with heart failuremay need more assistance and specific interven-tions than men.
Physiological differences between women andmen with heart failure may contribute in part todifferences in life quality [10]. In a comprehensivereview of the literature, Richardson [10] summa-rized the differences in cardiac anatomy andphysiology of women compared to men as follows:smaller heart size and coronary arteries, smallermuscle fibers, increased vasospasm, higher restingejection fraction and heart rate, lower left ven-tricular end-diastolic pressure and volume, ejec-tion fraction less responsive to exercise, higherestrogen levels, potential difference in metabolismand clearance of drugs, and longer QTc intervals.Women with heart failure are more likely to havecomorbid conditions, including hypertension [11]and diabetes [12], than men with heart failure.Women with heart failure tend to be older thanmen due to the later onset of coronary arterydisease in women, and thus may be more likely tobe widowed and/or to live alone without adequatesupport systems. These differences present specialproblems for women with heart failure.
Social support is one variable proposed to in-fluence symptom and functional status, healthperceptions, and overall quality of life [6]. Socialsupport, as defined in this study, is functionalsupport that involves the degree to which one’sinterpersonal relationships serve specific functions,with the most common types of functions being
emotional support, appraisal support, socialcompanionship, tangible or instrumental support,and informational support [13, 14]. Social supportis a predictor of health outcomes in some popu-lations [15, 16]. The lack of perceived emotionalsupport at hospital admission was an independentpredictor of cardiovascular events in the year fol-lowing hospitalization among 292 elderly patientswith heart failure, with the odds ratio (OR) forwomen much higher than for men [17]. Friedmanand King [18] reported that, among 80 womenwith heart failure aged 55 years or older, greateremotional support was significantly associatedwith more positive affect and life satisfaction,while greater tangible support was associated withless negative affect.
Increasing social support might be one way toimprove the diminished health-related quality oflife experienced by heart failure patients. Increasedsupport might facilitate management of trouble-some symptoms such as fatigue and cognitive im-pairment. The self-care activities that thesepatients must perform, including adhering to amultiple medication regimen, following dietarysodium restrictions, and self-monitoring weight[19, 20], might be improved with adequate levels ofsocial support. Because their quality of life appearspoorer than men and they are more likely to livealone without adequate support, older womenwith heart failure might need relatively more socialsupport to manage their condition and improvetheir life quality.
A gap remains in what is known about the dif-ferences in social support and how it affects qualityof life between women and men with heart failureof varying ages. Therefore, we conducted this studyto (1) describe the levels of perceived social supportduring a baseline hospitalization and 12 monthslater among patients with heart failure; (2) examinethe differences in perceived social support as afunction of gender and of age (those less than65 years of age vs. age 65 years or older); and (3)examine perceived social support as a predictor ofhealth-related quality of life. Two hypotheses wereproposed: (1) women aged 65 years or older per-ceive significantly lower social support than womenyounger than 65 years or men in either age group;and (2) baseline social support significantly pre-dicts 12-month health-related quality of life.
672
Methods
Sample
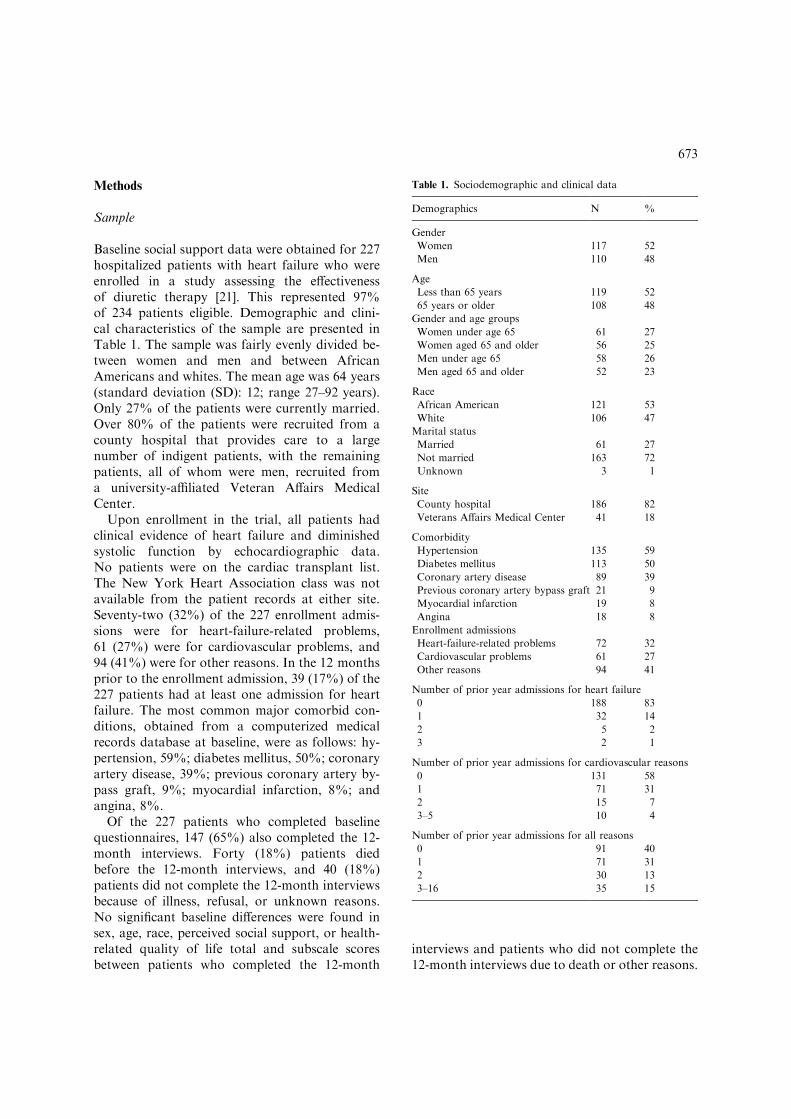
Baseline social support data were obtained for 227hospitalized patients with heart failure who wereenrolled in a study assessing the effectivenessof diuretic therapy [21]. This represented 97%of 234 patients eligible. Demographic and clini-cal characteristics of the sample are presented inTable 1. The sample was fairly evenly divided be-tween women and men and between AfricanAmericans and whites. The mean age was 64 years(standard deviation (SD): 12; range 27–92 years).Only 27% of the patients were currently married.Over 80% of the patients were recruited from acounty hospital that provides care to a largenumber of indigent patients, with the remainingpatients, all of whom were men, recruited froma university-affiliated Veteran Affairs MedicalCenter.
Upon enrollment in the trial, all patients hadclinical evidence of heart failure and diminishedsystolic function by echocardiographic data.No patients were on the cardiac transplant list.The New York Heart Association class was notavailable from the patient records at either site.Seventy-two (32%) of the 227 enrollment admis-sions were for heart-failure-related problems,61 (27%) were for cardiovascular problems, and94 (41%) were for other reasons. In the 12 monthsprior to the enrollment admission, 39 (17%) of the227 patients had at least one admission for heartfailure. The most common major comorbid con-ditions, obtained from a computerized medicalrecords database at baseline, were as follows: hy-pertension, 59%; diabetes mellitus, 50%; coronaryartery disease, 39%; previous coronary artery by-pass graft, 9%; myocardial infarction, 8%; andangina, 8%.
Of the 227 patients who completed baselinequestionnaires, 147 (65%) also completed the 12-month interviews. Forty (18%) patients diedbefore the 12-month interviews, and 40 (18%)patients did not complete the 12-month interviewsbecause of illness, refusal, or unknown reasons.No significant baseline differences were found insex, age, race, perceived social support, or health-related quality of life total and subscale scoresbetween patients who completed the 12-month
interviews and patients who did not complete the12-month interviews due to death or other reasons.
Table 1. Sociodemographic and clinical data
Demographics N %
Gender
Women 117 52
Men 110 48
Age
Less than 65 years 119 52
65 years or older 108 48
Gender and age groups
Women under age 65 61 27
Women aged 65 and older 56 25
Men under age 65 58 26
Men aged 65 and older 52 23
Race
African American 121 53
White 106 47
Marital status
Married 61 27
Not married 163 72
Unknown 3 1
Site
County hospital 186 82
Veterans Affairs Medical Center 41 18
Comorbidity
Hypertension 135 59
Diabetes mellitus 113 50
Coronary artery disease 89 39
Previous coronary artery bypass graft 21 9
Myocardial infarction 19 8
Angina 18 8
Enrollment admissions
Heart-failure-related problems 72 32
Cardiovascular problems 61 27
Other reasons 94 41
Number of prior year admissions for heart failure
0 188 83
1 32 14
2 5 2
3 2 1
Number of prior year admissions for cardiovascular reasons
0 131 58
1 71 31
2 15 7
3–5 10 4
Number of prior year admissions for all reasons
0 91 40
1 71 31
2 30 13
3–16 35 15
673

Instruments
Social support surveySocial support was conceptually defined as theperceptions a person has about the availability ofdifferent types of support and relationships thatserve particular functions [14]. The social supportsurvey developed by Sherbourne and Stewart [14]was used to measure social support. The first itemon this survey is an open-ended question onwhich respondents are asked to rate the numberof close friends and relatives they have. The re-maining 19 items each address a type of perceivedsocial support, with 5-point response scalesranging from 0 (none of the time) to 4 (all of thetime). For each item, respondents rate theamount of support they perceive is available tothem. The possible range of the total score isfrom 0 to 76, with higher scores indicating moreperceived support.
In addition to the total score, the social supportsurvey yields four subscale scores respectively la-beled emotional/informational support, tangiblesupport, positive social interaction, and affection-ate support. The authors of the survey operation-alized the dimensions of social support accordingto the following definitions. Emotional supportwas defined as being empathetic and understand-ing, having positive affect, and encouragingexpression of feelings. Offering information,guidance, and advice was considered informa-tional support. Tangible support was providingconcrete aid and assistance, such as financial,transportation, or housekeeping help. Positive so-cial interaction was defined as having people withwhom one can share social activities. Affectionatesupport was having someone who expresses loveand affection [14].
Reliability and validity of the instrument havebeen documented in patient populations, includ-ing patients with heart failure [14, 22, 23]. Theauthors specifically designed the survey to be dis-tinct from measures of health status and healthoutcomes and this distinctness was supported in astudy with 2987 patients [14]. In the current sam-ple, the Cronbach’s a internal consistency reli-ability estimates of the total and subscale scoreswere satisfactory, ranging from 0.80 to 0.95 atbaseline and from 0.84 to 0.97 at 12 months afterbaseline.
Chronic heart failure questionnaireThe chronic heart failure questionnaire by Guyattet al. [24] was used to measure disease-specifichealth-related quality of life, defined as valuedaspects of life related to one’s health in the contextof heart disease. This questionnaire contains 16items with 7-point response scales ranging from 1to 7. The possible range of the total health-relatedquality of life score is from 16 to 112, with a higherscore indicating better health-related quality oflife.
In addition to the total health-related quality oflife score, there are three subscales respectivelymeasuring dyspnea, fatigue, and emotional qual-ity of life. The first two subscales deal with thetwo most common symptoms of heart failure,dyspnea and fatigue. The emotional subscale hasitems about emotional symptoms associated withheart failure and affect [24]. Items on the emo-tional subscale do not overlap with items on thesocial support survey. Reliability and validityhave been satisfactory in past studies [25, 26]. Inthis study, the Cronbach’s a values ranged from0.78 to 0.88 at baseline and from 0.79 to 0.92,12 months later.
Procedure
The study was approved by the university institu-tional review board prior to implementation.During hospitalization, patients who agreed toparticipate were enrolled in a randomized clinicaltrial to compare two diuretic medications. Thesepatients also completed the social support surveyand the chronic heart failure questionnaire byface-to-face interviews during hospitalization.Some of the patients completed these question-naires a second time 12 months later by telephoneinterviews. All interviews were completed by thesame four trained and experienced research assis-tants and graduate nursing students.
Statistical analysis
Descriptive statistics (means and SDs) were com-puted for the social support total and subscalescores, the chronic heart failure questionnairescores, and change scores from baseline to12 months after baseline. Pearson correlation co-efficients were computed and graphical analyses
674
conducted to compare baseline and 12-monthscores. Age was analyzed as a dichotomous vari-able in order to examine differences between pa-tients under age 65 and those patients aged 65 andover. The rationale for using age 65 is that it is thecommonly used age in the United States to desig-nate persons as eligible for retirement and otherbenefits of older age. Mortality and morbidity areknown to be higher among people aged 65 yearsor older [27].
To test the hypothesis that women aged 65 yearsor older would perceive significantly less socialsupport than women younger than 65 years ormen in either age group at baseline, ANOVAswere conducted with gender, age, and a gender byage interaction. Following a significant interac-tion, Tukey’s pairwise comparisons were used tocompare the groups. A series of multiple linearregression analyses was conducted to test the hy-pothesis that social support at baseline wouldsignificantly predict health-related quality of life12 months later. The 12-month health-relatedquality of life total and subscale scores were usedas dependent variables. The baseline social supporttotal and subscale scores were entered separatelyinto the equations as independent variables. Inthese models, baseline health-related quality oflife, drug group, age (<65 vs. P65), gender, race,number of prior admissions, comorbidities, andsite were used as co-variates. The significance levelwas set at pO0:05 for all primary analyses. Ana-lyses were completed with the SAS computerprogram, version 6.12 [28].
Results
Social support
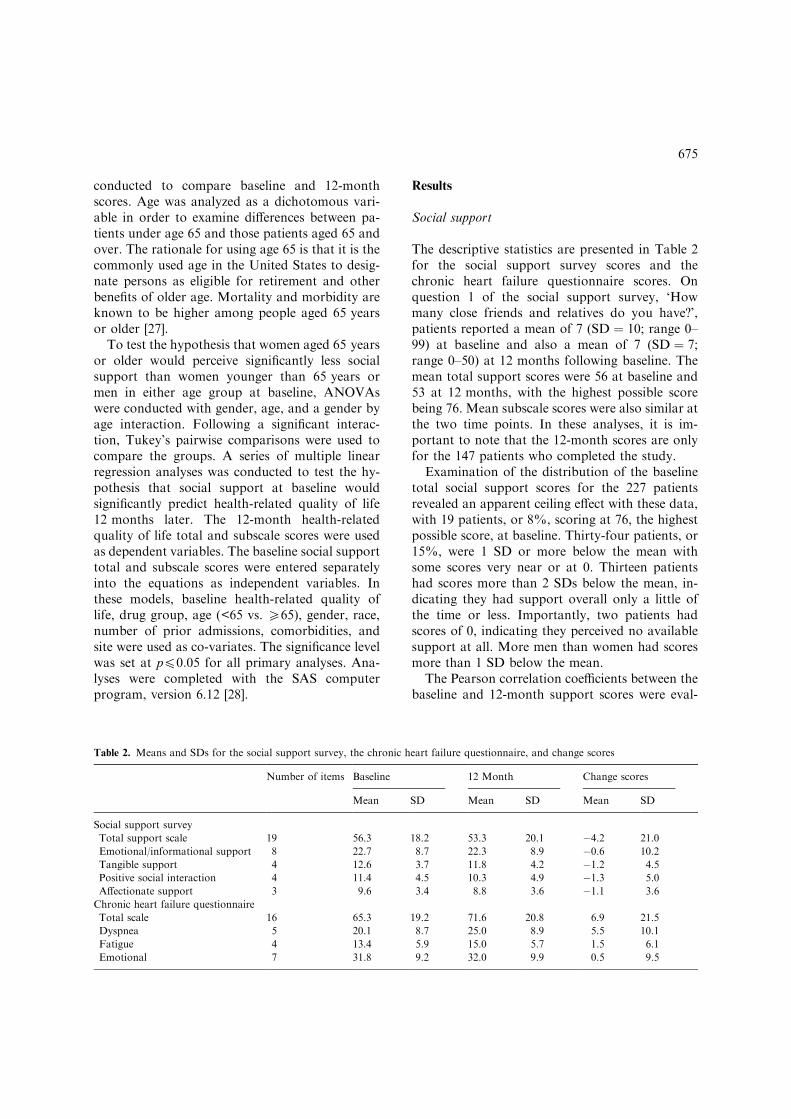
The descriptive statistics are presented in Table 2for the social support survey scores and thechronic heart failure questionnaire scores. Onquestion 1 of the social support survey, ‘Howmany close friends and relatives do you have?’,patients reported a mean of 7 (SD ¼ 10; range 0–99) at baseline and also a mean of 7 (SD ¼ 7;range 0–50) at 12 months following baseline. Themean total support scores were 56 at baseline and53 at 12 months, with the highest possible scorebeing 76. Mean subscale scores were also similar atthe two time points. In these analyses, it is im-portant to note that the 12-month scores are onlyfor the 147 patients who completed the study.
Examination of the distribution of the baselinetotal social support scores for the 227 patientsrevealed an apparent ceiling effect with these data,with 19 patients, or 8%, scoring at 76, the highestpossible score, at baseline. Thirty-four patients, or15%, were 1 SD or more below the mean withsome scores very near or at 0. Thirteen patientshad scores more than 2 SDs below the mean, in-dicating they had support overall only a little ofthe time or less. Importantly, two patients hadscores of 0, indicating they perceived no availablesupport at all. More men than women had scoresmore than 1 SD below the mean.
The Pearson correlation coefficients between thebaseline and 12-month support scores were eval-
Table 2. Means and SDs for the social support survey, the chronic heart failure questionnaire, and change scores
Number of items Baseline 12 Month Change scores
Mean SD Mean SD Mean SD
Social support survey
Total support scale 19 56.3 18.2 53.3 20.1 �4.2 21.0
Emotional/informational support 8 22.7 8.7 22.3 8.9 �0.6 10.2
Tangible support 4 12.6 3.7 11.8 4.2 �1.2 4.5
Positive social interaction 4 11.4 4.5 10.3 4.9 �1.3 5.0
Affectionate support 3 9.6 3.4 8.8 3.6 �1.1 3.6
Chronic heart failure questionnaire
Total scale 16 65.3 19.2 71.6 20.8 6.9 21.5
Dyspnea 5 20.1 8.7 25.0 8.9 5.5 10.1
Fatigue 4 13.4 5.9 15.0 5.7 1.5 6.1
Emotional 7 31.8 9.2 32.0 9.9 0.5 9.5
675

uated to determine the degree to which socialsupport changed over time in individual patients,even though mean scores remained similar (seeTable 3). The correlations ranged from 0.06 to0.53. Many of these correlations were statisticallysignificant, but the magnitude of the correlations islow to moderate and represents low associationsbetween the measures at the two time points. Themean scores for social support remained stableover time but there was little correlation betweenthe scores at the two time points. Graphical dataanalysis (not shown) indicated that quite a fewpatients perceived high support throughout thestudy. Some patients with low support at the onsetof the study experienced large increases in supportduring the 12 months. In contrast, other patientswith high support at the beginning of the studyreported large decreases at 12 months.
Health-related quality of life
The mean scores on the chronic heart failurequestionnaire were 65 at baseline and 72 at12 months, with the highest possible score being112 (Table 2). Overall, patients reported low tomoderate health-related quality of life overall. Themeans for the dyspnea and fatigue subscale scoresincreased over the 12 months, indicating a de-crease in these symptoms, while the emotionalhealth-related quality of life subscale mean re-mained the same.
Sex and age analysis
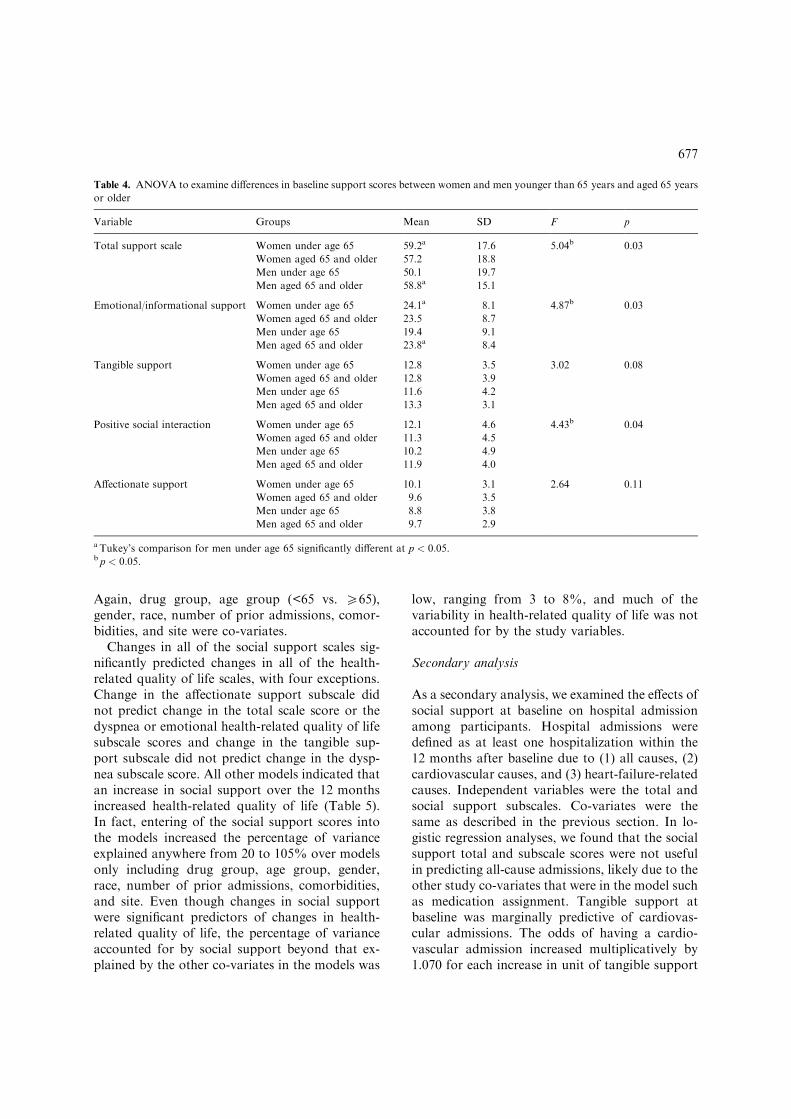
The ANOVA indicated significant interactions ofgender by age in perceptions of total support,
emotional/informational support, and positivesocial interaction at baseline (Table 4). Tukey’spost hoc analysis revealed that the men who wereunder age 65 perceived significantly less socialsupport than men aged 65 and over and womenunder age 65. There were no significant differencesin perceived support between women aged 65 orolder and any other group. Thus the hypothesisthat women aged 65 years and older would havesignificantly lower social support was rejected. Todetermine whether other variables influenced thesefindings, we conducted post hoc ANCOVA modelsadjusting for drug group, race, site, number ofprior hospitalizations, and comorbidities. Resultsindicated that there were no significant differencesbetween the four groups, although trends weresimilar to the ANOVA results.
Multiple regression analysis
Results of the multiple regression analysis indi-cated that baseline social support was not a sig-nificant predictor of 12-month health-relatedquality of life when other factors were controlled.Hypothesis 2 was not supported. Because of thechanges noted in social support scores during the12 months, we evaluated whether changes in socialsupport scores were associated with changes inhealth-related quality of life scores (Table 5). Forboth measures, the change scores were calculatedas the 12-month score minus the baseline score,and higher change scores indicated improvement.In regression analyses, the change scores for thehealth-related quality of life total and subscaleswere dependent variables. The social supportchange scores were the independent variables.
Table 3. Pearson’s correlation coefficients between baseline and 12-month support scores
All patients
N = 147
Women under
age 65 N = 41
Women aged 65
and older N = 34
Men under age
65 N = 40
Men aged 65 and
older N = 32
Total support scale r = 0.36 r = 0.45 r = 0.26 r = 0.27 r = 0.44
p < 0.0001 p = 0.0034 p = 0.1443 p = 0.0962 p = 0.0122
Tangible social support r = 0.28 r = 0.41 r = 0.31 r = 0.20 r = 0.06
p = 0.0005 p = 0.0070 p = 0.0761 p = 0.2171 p = 0.7409
Emotional/informational support r = 0.31 r = 0.41 r = 0.16 r = 0.24 r = 0.30
p = 0.0001 p = 0.0073 p = 0.3605 p = 0.1315 p = 0.0938
Affectionate support r = 0.39 r = 0.49 r = 0.19 r = 0.39 r = 0.53
p < 0.0001 p = 0.0012 p = 0.2928 p = 0.0125 p = 0.0016
Positive social interaction r = 0.40 r = 0.42 r = 0.43 r = 0.29 r = 0.51
p < 0.0001 p = 0.0059 p = 0.0120 p = 0.0746 p = 0.0031
676
Again, drug group, age group (<65 vs. P65),gender, race, number of prior admissions, comor-bidities, and site were co-variates.
Changes in all of the social support scales sig-nificantly predicted changes in all of the health-related quality of life scales, with four exceptions.Change in the affectionate support subscale didnot predict change in the total scale score or thedyspnea or emotional health-related quality of lifesubscale scores and change in the tangible sup-port subscale did not predict change in the dysp-nea subscale score. All other models indicated thatan increase in social support over the 12 monthsincreased health-related quality of life (Table 5).In fact, entering of the social support scores intothe models increased the percentage of varianceexplained anywhere from 20 to 105% over modelsonly including drug group, age group, gender,race, number of prior admissions, comorbidities,and site. Even though changes in social supportwere significant predictors of changes in health-related quality of life, the percentage of varianceaccounted for by social support beyond that ex-plained by the other co-variates in the models was
low, ranging from 3 to 8%, and much of thevariability in health-related quality of life was notaccounted for by the study variables.
Secondary analysis
As a secondary analysis, we examined the effects ofsocial support at baseline on hospital admissionamong participants. Hospital admissions weredefined as at least one hospitalization within the12 months after baseline due to (1) all causes, (2)cardiovascular causes, and (3) heart-failure-relatedcauses. Independent variables were the total andsocial support subscales. Co-variates were thesame as described in the previous section. In lo-gistic regression analyses, we found that the socialsupport total and subscale scores were not usefulin predicting all-cause admissions, likely due to theother study co-variates that were in the model suchas medication assignment. Tangible support atbaseline was marginally predictive of cardiovas-cular admissions. The odds of having a cardio-vascular admission increased multiplicatively by1.070 for each increase in unit of tangible support
Table 4. ANOVA to examine differences in baseline support scores between women and men younger than 65 years and aged 65 years
or older
Variable Groups Mean SD F p
Total support scale Women under age 65 59.2a 17.6 5.04b 0.03
Women aged 65 and older 57.2 18.8
Men under age 65 50.1 19.7
Men aged 65 and older 58.8a 15.1
Emotional/informational support Women under age 65 24.1a 8.1 4.87b 0.03
Women aged 65 and older 23.5 8.7
Men under age 65 19.4 9.1
Men aged 65 and older 23.8a 8.4
Tangible support Women under age 65 12.8 3.5 3.02 0.08
Women aged 65 and older 12.8 3.9
Men under age 65 11.6 4.2
Men aged 65 and older 13.3 3.1
Positive social interaction Women under age 65 12.1 4.6 4.43b 0.04
Women aged 65 and older 11.3 4.5
Men under age 65 10.2 4.9
Men aged 65 and older 11.9 4.0
Affectionate support Women under age 65 10.1 3.1 2.64 0.11
Women aged 65 and older 9.6 3.5
Men under age 65 8.8 3.8
Men aged 65 and older 9.7 2.9
a Tukey’s comparison for men under age 65 significantly different at p < 0:05.b p < 0:05.
677

(p ¼ 0:09). Tangible support did predict heart-failure-related admission (p ¼ 0:05), and a trendtoward significance was noted for total socialsupport (p ¼ 0:08) and positive social interaction(p ¼ 0:07). The odds of having a heart-failure-re-lated admission increased multiplicatively by 1.114for each unit increase in tangible support, 1.019 foreach increase in unit of total social support, and1.082 for each unit increase in positive social in-teraction.
We also examined the change scores for socialsupport to determine whether changes were pre-dictive of hospital admissions, and there was someevidence for this. The odds of all-cause admissiondecreased multiplicatively by 1.016 (p ¼ 0:10) for aunit increase in the change score for total socialsupport, 1.041 (p ¼ 0:04) for a unit increase in thechange score for emotional/informational support,and 1.081 (p ¼ 0:05) for a unit increase in thechange score for positive social interaction. Inaddition, the odds of cardiovascular admission
decreased multiplicatively by 1.032 (p ¼ 0:09) for aunit increase in emotional/informational support.Finally, the odds of heart-failure-related admissiondecreased multiplicatively by 1.019 (p ¼ 0:07) for aunit increase in the change score for total socialsupport, 1.092 (p ¼ 0:06) for a unit increase in thechange score for tangible support, and 1.094(p ¼ 0:04) for a unit increase in the change scorefor positive social interaction.
As detailed above, all logistic models for whichthe social support variable was significant at the0.10 level or less indicated that higher levels ofbaseline social support reflected increases in hos-pital admissions, and all logistic models for whichthe change in social support was significant at the0.10 level or less indicated that an increase in thechange score for social support reflected a decreasein hospital admissions. Representative logisticmodels, one each for baseline and change in socialsupport, are presented in Table 6. Note that onlysocial support, drug group, and angina as a com-
Table 5. Multiple linear regression analyses for change scores
Estimated effect Final model R2 Increase in R2 due to
addition of support scale
% Increase* p
Chronic heart failure questionnaire total scale
Total support scale 0.28 0.1447 0.0721 99 0.001
Tangible social support 1.16 0.1310 0.0584 80 0.003
Emotional/informational support 0.59 0.1486 0.0759 105 0.001
Affectionate support 0.74 0.0871 0.0145 20 0.149
Positive social interaction 1.11 0.1375 0.0649 89 0.002
Chronic heart failure questionnaire dyspnea subscale
Total support scale 0.10 0.1400 0.0437 45 0.01
Tangible social support 0.33 0.1180 0.0217 23 0.07
Emotional/informational support 0.22 0.1426 0.0463 48 0.01
Affectionate support 0.23 0.1030 0.0067 7 0.32
Positive social interaction 0.49 0.1550 0.0588 61 0.003
Chronic heart failure questionnaire fatigue subscale
Total support scale 0.06 0.1738 0.0436 33 0.01
Tangible social support 0.26 0.1666 0.0364 28 0.02
Emotional/informational support 0.11 0.1662 0.0359 28 0.02
Affectionate support 0.28 0.1567 0.0265 20 0.04
Positive social interaction 0.24 0.1687 0.0385 30 0.01
Chronic heart failure questionnaire emotional subscale
Total support scale 0.10 0.1243 0.0451 57 0.01
Tangible social support 0.48 0.1306 0.0514 65 0.006
Emotional/informational support 0.22 0.1330 0.0538 68 0.005
Affectionate support 0.14 0.0818 0.0026 3 0.54
Positive social interaction 0.33 0.1090 0.0298 38 0.04
* % Increase = 100% · (increase in R2 due to addition of support scores/(final model R2�increase in R2 due to addition of support
scale)).
678
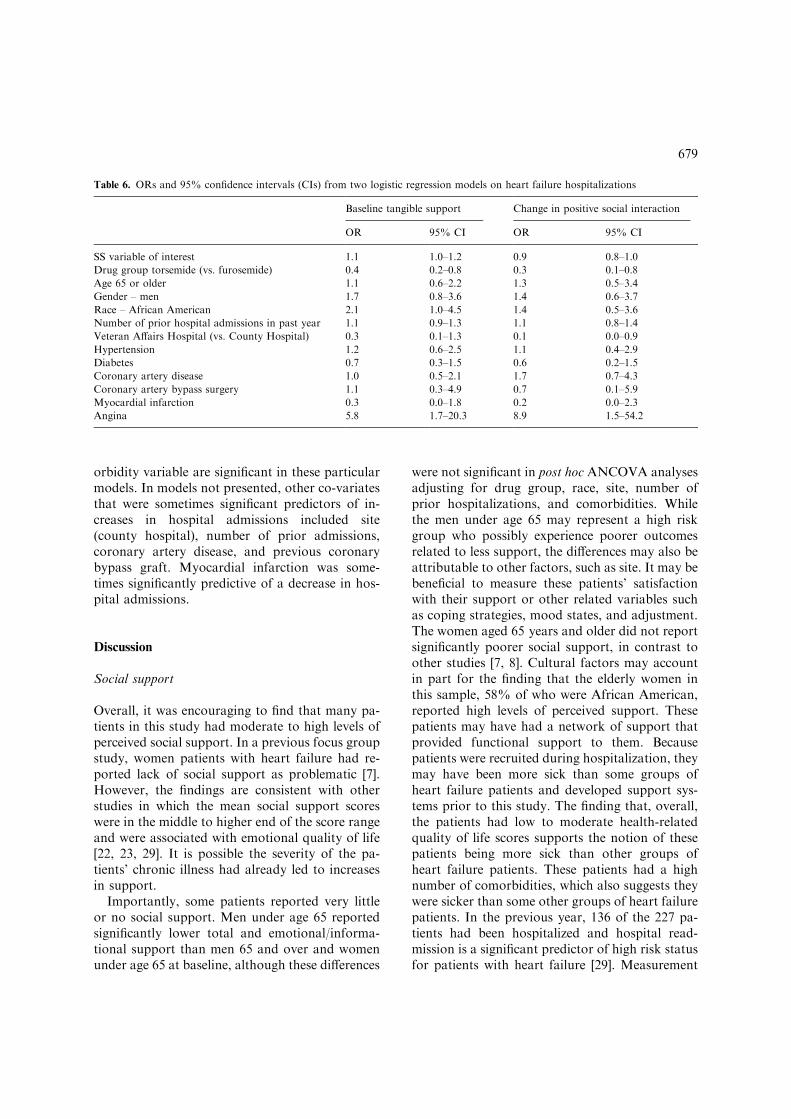
orbidity variable are significant in these particularmodels. In models not presented, other co-variatesthat were sometimes significant predictors of in-creases in hospital admissions included site(county hospital), number of prior admissions,coronary artery disease, and previous coronarybypass graft. Myocardial infarction was some-times significantly predictive of a decrease in hos-pital admissions.
Discussion
Social support
Overall, it was encouraging to find that many pa-tients in this study had moderate to high levels ofperceived social support. In a previous focus groupstudy, women patients with heart failure had re-ported lack of social support as problematic [7].However, the findings are consistent with otherstudies in which the mean social support scoreswere in the middle to higher end of the score rangeand were associated with emotional quality of life[22, 23, 29]. It is possible the severity of the pa-tients’ chronic illness had already led to increasesin support.
Importantly, some patients reported very littleor no social support. Men under age 65 reportedsignificantly lower total and emotional/informa-tional support than men 65 and over and womenunder age 65 at baseline, although these differences
were not significant in post hoc ANCOVA analysesadjusting for drug group, race, site, number ofprior hospitalizations, and comorbidities. Whilethe men under age 65 may represent a high riskgroup who possibly experience poorer outcomesrelated to less support, the differences may also beattributable to other factors, such as site. It may bebeneficial to measure these patients’ satisfactionwith their support or other related variables suchas coping strategies, mood states, and adjustment.The women aged 65 years and older did not reportsignificantly poorer social support, in contrast toother studies [7, 8]. Cultural factors may accountin part for the finding that the elderly women inthis sample, 58% of who were African American,reported high levels of perceived support. Thesepatients may have had a network of support thatprovided functional support to them. Becausepatients were recruited during hospitalization, theymay have been more sick than some groups ofheart failure patients and developed support sys-tems prior to this study. The finding that, overall,the patients had low to moderate health-relatedquality of life scores supports the notion of thesepatients being more sick than other groups ofheart failure patients. These patients had a highnumber of comorbidities, which also suggests theywere sicker than some other groups of heart failurepatients. In the previous year, 136 of the 227 pa-tients had been hospitalized and hospital read-mission is a significant predictor of high risk statusfor patients with heart failure [29]. Measurement
Table 6. ORs and 95% confidence intervals (CIs) from two logistic regression models on heart failure hospitalizations
Baseline tangible support Change in positive social interaction
OR 95% CI OR 95% CI
SS variable of interest 1.1 1.0–1.2 0.9 0.8–1.0
Drug group torsemide (vs. furosemide) 0.4 0.2–0.8 0.3 0.1–0.8
Age 65 or older 1.1 0.6–2.2 1.3 0.5–3.4
Gender – men 1.7 0.8–3.6 1.4 0.6–3.7
Race – African American 2.1 1.0–4.5 1.4 0.5–3.6
Number of prior hospital admissions in past year 1.1 0.9–1.3 1.1 0.8–1.4
Veteran Affairs Hospital (vs. County Hospital) 0.3 0.1–1.3 0.1 0.0–0.9
Hypertension 1.2 0.6–2.5 1.1 0.4–2.9
Diabetes 0.7 0.3–1.5 0.6 0.2–1.5
Coronary artery disease 1.0 0.5–2.1 1.7 0.7–4.3
Coronary artery bypass surgery 1.1 0.3–4.9 0.7 0.1–5.9
Myocardial infarction 0.3 0.0–1.8 0.2 0.0–2.3
Angina 5.8 1.7–20.3 8.9 1.5–54.2
679

issues may also explain differences in results. Someprevious studies used small samples and a focusgroup design [7], data obtained from clinical trialswhich may represent select groups of patients [8],or measures of emotional support that lackeddocumented reliability [7].
Although the mean level of perceived socialsupport remained stable over time, the variabilityin the change patterns was high. It will be impor-tant to identify prospectively which variables pre-dict the changes in social support in future studiesin order to develop targeted interventions. Forexample, how do family variables and the exis-tence or quality of marital relationships influencesuch changes? Measurement issues need to be ad-dressed, including how frequently social supportshould be measured to detect important changes,how ceiling effects influence results, and how dif-ferent modes of administration of instruments,such as face-to-face and telephone interviews,compare with one another.
Interventions
Although baseline social support did not predictfuture health-related quality of life, changes insocial support did predict changes in health-relatedquality of life. The results support Wilson andCleary’s [6] model in which social support is hy-pothesized to be a factor influencing the health-related quality of life domains of functional status,general health perceptions, and well-being. Fur-thermore, the results are consistent with previousstudies that have documented relationships be-tween social support and health-related quality oflife [8, 18, 22, 23]. This finding suggests that in-terventions designed for persons with low socialsupport might improve health-related quality oflife, particularly if we knew more about thechanges in social support.
In our secondary analysis, we found that higherlevels of social support at baseline predictedgreater odds of heart-failure-related hospital ad-missions. This finding is in contrast to past re-search by Krumholz et al. [17] who found that lackof emotional support was a significant predictor ofhospitalization, but his study involved elderly pa-tients (n ¼ 292, mean age 80 years) with heartfailure, was retrospective in part with some dataobtained from medical records, and the measure of
emotional and tangible support contained onlytwo questions respectively asking whether each ofthese types of support was available and two fol-low-up questions for patients who answered ‘yes’to either initial question. Patients in the currentstudy were recruited prospectively during a hos-pitalization, were younger with a mean age of64 years, and the measure of social support wasreliable. These factors may have contributed tothis difference in results. We also found evidence toindicate that positive changes in social supportpredicted decreases in all-cause and heart-failure-related hospital admission.
An important intervention for patients withmoderate to high levels of support might be as-sisting family members and others who are pro-viding care to these patients. A search of Medlineand the Cumulative Index for Nursing and AlliedHealth Literature (CINAHL) databases using thekeywords of congestive heart failure and caregiverburden yielded only one reference, which was astudy by Karmilovich, who found that caregiversof persons with heart failure reported high levels ofstress and caregiver burden [30]. In a study of 90patients with severe cardiomyopathy and theirspouses, Bohachick and Anton found that patientsand spouses reported different problems in ad-justment, and they recommended interventions tosupport both the patients and their spouses [31]. Ina focus group study with 23 patients with heartfailure and 18 family members, family membersdiscussed difficulties in dealing with many trou-bling symptoms and behaviors [7]. Studies ofcaregiver burden might suggest interventions thatwould assist caregivers in providing care and ulti-mately improve outcomes for both patients andtheir families. Inclusion of theories about familyadjustment may also be beneficial in identifyinginterventions that would improve outcomes inpatients and their loved ones.
Limitations
This study has several limitations. One limitationis the number of patients who did not complete the12-month interviews due to death or other reasons,although no baseline differences were noted be-tween these two groups. Second, the results maynot be generalizable to all patients with heartfailure because the sample included a large number
680

of minority patients and some were likely indigent;however, they may be generalizable to similar pa-tients in other urban settings. Third, the regressionanalyses to evaluate whether changes in socialsupport predicted changes in quality of life wereconducted as unplanned analyses and need verifi-cation in future studies. The regression analysesfor hospital admissions also require verification infuture studies.
Conclusions
In summary, future studies are warranted to fur-ther evaluate the lower support reported by menunder age 65 in this sample. Studies are indicatedto examine the caregivers’ needs as well as thepatients’ needs. Finally, we need to determine thespecific predictors of changes in social support inthese patients in order to design effective, sup-portive interventions.
Acknowledgements
The authors thank Gertrude Huster, MHS andJarek Harezlak, MSc for statistical assistance andPhyllis Dexter, PhD, for editorial assistance. Thiswork was supported in part by NIH grantsAG07631 and DK 37994 and Boehringer-Mann-heim.
References
1. American Heart Association. 1998 Heart and Stroke Sta-
tistical Update. Dallas, TX: American Heart Association,
1998. www.amhrt.org/1999/stats/OCardDis.html.
2. Croft JB, Giles WH, Pollard RA, et al. Heart failure sur-
vival among older adults in the United States. Arch Intern
Med 1999; 159: 505–510.
3. Dracup K, Walden JA, Stevenson LW, Brecht M. Quality
of life in patients with advanced heart failure. J Heart Lung
Transplant 1992; 11: 273–279.
4. Konstam V, Salem D, Pouleur H, et al. Baseline quality of
life as a predictor of mortality and hospitalization in 5025
patients with congestive heart failure. Am J Cardiol 1996;
78: 890–895.
5. Cohn JN. Physiological variables as markers for symptoms,
risk, and interventions in heart failure. Circulation 1993;
87(Suppl VII): VII-110–VII-114.
6. Wilson IB, Cleary PD. Linking clinical variables with
health-related quality of life. JAMA 1995; 273: 59–65.
7. Bennett SJ, Cordes DK, Westmoreland G, Castro R,
Donnelly E. Self-care strategies for symptom management
in patients with chronic heart failure. Nurs Res 2000; 49:
139–145.
8. Riedinger MS, Dracup KA, Brecht M, Padilla G, Sarna L,
Ganz PA. Quality of life in patients with heart failure: Do
gender differences exist? Heart Lung 2001; 30: 105–116.
9. Chin MH, Goldman L. Gender differences in 1-year sur-
vival and quality of life among patients admitted with
congestive heart failure. Med Care 1998; 36: 1033–1046.
10. Richardson LG. Women and heart failure. Heart Lung
2001; 30: 87–97.
11. Levy D, Larson M, Vasan R. The progression from hy-
pertension to congestive heart failure. JAMA 1996; 275:
1557–1666.
12. Shindler D, Kostis J, Yusuf S, et al. Diabetes mellitus: A
predictor of morbidity and mortality in the studies of left
ventricular dysfunction (SOLVD) trials and registry. Am J
Cardiol 1996; 77: 1017–1020.
13. Cohen S, Mermelstein R, Kamarck T, Hoberman H.
Measure the functional components of social support. In:
Sarason I (ed), Social Support: Theory, Research, and
Applications, Holland: Martines Nijhoff, 1985.
14. Sherbourne CD, Stewart AL. The MOS social support
survey. Soc Sci Med 1991; 32: 705–714.
15. Berkman LF, Vaccarino V, Seeman T. Gender differences
in cardiovascular morbidity and mortality: The contribu-
tion of social networks and support. Ann Behav Med 1993;
15: 112–118.
16. Ornish D. Love and Survival. New York: Harper Collins,
1998.
17. Krumholz H, Butler J, Miller J, et al. Prognostic impor-
tance of emotional support for elderly patients hospitalized
with heart failure. Circulation 1998; 97: 958–964.
18. Friedman M, King KB. The relationship of emotional and
tangible support to psychological well-being among older
women with heart failure. Res Nurs Health 1994; 17: 433–
440.
19. Konstam M, Dracup K, Baker D, et al. Heart Failure:
Evaluation and Care of Patients with Left-ventricular Sys-
tolic Dysfunction. Clinical Practice Guideline No. 11.
AHCPR Publication No. 94-0612. Rockville, MD: Agency
for Health Care Policy and Research, Public Health Ser-
vice, US Department of Health and Human Services, June
1994.
20. Packer M, Cohn JN (eds). Consensus recommendations for
the management of chronic heart failure. Am J Cardiol
1999; 83(Suppl 2A): 18A–20A.
21. Murray MD, Tierney WM, Brater DC. Determining the
effectiveness of torsemide and furosemide in heart failure.
Clin Drug Invest 1998; 16(1): 45–52.
22. Bennett SJ, Baker SL, Huster GA. Quality of life in women
with heart failure. Health Care Women Int 1998; 19: 217–
219.
23. Bennett SJ, Pressler ML, Hays L, Firestine LA, Huster GA.
Psychosocial variables and hospitalization in persons with
chronic heart failure. Prog Cardiovasc Nurs 1997; 12: 4–11.
681

24. Guyatt GH, Nogradi S, Halcrow S, et al. Development and
testing of a new measure of health status for clinical trials in
heart failure. J Gen Intern Med 1989; 4: 101–107.
25. Guyatt GH, Sullivan MJJ, Fallen E, et al. A controlled trial
of digoxin in congestive heart failure. Am J Cardiol 1988;
61: 371–375.
26. Guyatt G, Feeny DH, Patrick DL. Measuring health-re-
lated quality of life. Ann Intern Med 1993; 118: 622–629.
27. Berg RL, Casells JS (eds). The Second Fifty Years: Pro-
moting Health and Preventing Disability. Washington, DC:
National Academy Press, 1990.
28. SAS/STAT User’s Guide, Version 6, 4th ed. Cary, NC: SAS
Institute Inc, 1989; 1–2.
29. Krumholz HM, Chen YT, Wang Y, Vaccarino V, Radford
MJ, Horwitz RI. Predictors of readmission among elderly
survivors of admission with heart failure. Am Heart J 2000;
139: 72–77.
30. Karmilovich SE. Burden and stress associated with spousal
caregiving for individuals with heart failure. Prog in CV
Nurs 1994; 9: 33–38.
31. Bohachick P, Anton BB. Psychosocial adjustment of pa-
tients and spouses to severe cardiomyopathy. Res Nurs
Health 1990; 13: 385–392.
32. Friedman MM. Social support sources among older women
with heart failure: Continuity versus loss over time. Res
Nurs Health 1997; 20: 319–327.
Address for correspondence: Susan J. Bennett, Indiana Univer-
sity School of Nursing, 1111 Middle Drive, Indianapolis, IN
46202, USA
Phone: þ317-274-4432; Fax: þ317-278-1856
E-mail: [email protected]
682