Embed Size (px)
Citation preview

27
Richard L. DotyCharles P. Kimmelman
Ronald P. Lesser
assessment. Emphasis is placed on the sensory eval-uation of olfactory function and on the pathophysi-ology of this system, because olfactory disorders aremuch more common than gustatory ones, and mostcomplaints of taste dysfunction are in fact due toolfactory anomalies.
OLFACTION
Anatomy and Physiology of Olfaction
All environmental nutrients and airborne chemi-cals required for life enter the human body by meansof the nose and the mouth. Olfaction and tastemonitor the intake of such materials and determinethe flavor and palatability of foods and beverages. Inaddition, these primary senses warn of toxins, suchas spoiled food, leaking natural gas, polluted air,and smoke, and serve as diagnostic iJ\dicators for anumber of serious diseases, including Alzheimer'sdisease and some forms of parkinsonism. Despitesuch important functions, however, the chemicalsenses have been generally disregarded from a med-ical perspective and are often not tested. Such neglectdoes not stem from a want of patients experiencingchemosensory problems; for example, data from theNational Ambulatory Medical Care Survey suggestthat, for 1975 and 1976 combined, 435,000 visits tophysicians' offices occurred in which a major pre-senting complaint was chemosensory in nature (Re-port of the Panel on Communicative Disorders to theNational Advisory Neurological and CommunicativeDisorders and Stroke Council, 1979).
This chapter summarizes key aspects of the anat-omy and physiology of the olfactory and gustatorysystems and presents techniques for their clinical
Supported by grant ROl AG 08148 from the National Instituteon Aging and grant POI 00161 from the National Institute onDeafness and Other Communication Disorders.
390
Odorants are detected intranasally by specializedreceptor cells in the olfactory epithelium and, in somecases, by free nerve endings from the ophthalmicand maxillary divisions of the trigeminal nerve withinthe nasal epithelium. In addition, some inhaledchemicals are detected by nerve endings within thepharynx and the oral cavity , such as those associatedwith the glossopharyngeal and vagal nerves. Quali-tative odor sensations are mediated by the cranialnerve I receptors; the sensations mediated by theother nerves are primarily those of the commonchemical sense, such as warmth/coolness, sharpness,and irritation (Doty et aI., 1978; Silver and Moulton,1982).
The human olfactory neuroepithelium is located inthe superior nasal cavity and encompasses a portion

391SMELL AND TASTE AND THEIR DISORDERS
¥
t,, I".
" ,\ ,c "'~\ :.::-- -:~ I
,..:..~:, ,.-,-,.\...~.,~~.~. .J. , p.~~.;. ~,. 0' ~..:\,.
'-~ ...DY ;:t).-'-.. r. ., Q3 " ...,Ao.-y ...':V ;. -.,.,~ .(.\ ; .'., ..~. ..-
{ \.' ""~ .~ ,I..-~ ..~..~.:...: ...
~ m-:.. .-.;.,..., ".
-., ~. , ~\.~ '('., ~ ~.
cp
~
~
nc
$~
.:>
of the superior turbinate, the superior nasal septum,and the region of the cribriform plate. Contrary totextbook descriptions, this 2- to 5-cm2 region is rarelyvisually distinct from the surrounding respiratoryepithelium. At least four main cell types are foundin this region: bipolar olfactory receptor cells, micro-villar cells, sustentacular or supporting cells, andbasal cells (Moran et al., 1982b) (Fig. 27-1).
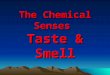
The first of these cell types-the primary olfactoryreceptor cell-numbers approximately 6 million inhumans. Each of these bipolar flask-shaped neuronsbears a slender rod, which enlarges at the surface ofthe epithelium into the olfactory knob or vesicle,from which 10-30 cilia project (Fig. 27-2). Odorantreceptor sites are found on these hair-like processes.The cilia often have the standard 9 + 2 arrangementof micro tubules in their basal segments, althoughvariations occur (e.g., 9 + 3 and 9 + 4). Becausethey generally lack dynein arms, active motility isbelieved to be absent (Moran et al., 1982b).
The second of these cell types-the microvillarcell-contains microvilli that project into the mucus.
,~;. :
~ , ,~ :. ,.., ..." -., , ',~"' .1""'... , , , " .~-t~i
~, , '7'-~ .'.,
Figure 27-2. Longitudinal section through an olfactory vesicle (ov).b ~ basal body; c = olfactory cilium; m = microtubules; nc =nasal cavity. ( x 22,110.) (From Moran D.T., Rowley J.C., JafekB.W.. et al. The fine structure of the olfactory mucosa in man. J.Neurocytol. 11 :721-746. 1982. Published by Chapman & HaJI.)
These rotund cells are located adjacent to the primarybipolar cells in a 1:10 ratio and bear no cilia (Moranet al., 1982a) (see Fig. 27-1). The function of thesecells is unknown, although a study using horseradishperoxidase tracer indicates that they send axons intothe olfactory bulb, suggesting a sensory function(Rowley et al., 1989).
The third of these cell types-the sustentacularcell-is distributed throughout the olfactory regionin contact with the other cell types and with oneanother, forming the matrix of the epithelium. Thesecells contribute to the production of mucus and mayserve pinocytotic uptake and enzymatic degradationfunctions. In addition, they probably insulate theprimary olfactory receptor cells from one another andmay regulate the potassium concentration in theextracellular space near the receptor cells (Walz andHertz, 1983).
The last of these four cell types-the basal cell-serves as -the stem cell- for -the other -cells-in- 1he.olfactory epithelium, including the bipolar receptorcells. These cells are located near the lamina propriaduring their resting stage (see Fig. 27-1) and undergomajor morphologic and functional changes duringdifferentiation. The capacity of the bipolar receptorcell neuron to regenerate continuously from the basalcells or from cells in a compartment immediatelyabove them (e.g., see Yamagishi et al., 1989) is aunique property of the olfactory neuroepithelium
FIgure 27-1. Low-power electron micrograph ( x 670) of a longi-tudinal section through a biopsy specimen of human olfactorymucosa taken from the nasal septum. Four cell Iypes are indicated:ciliated olfactory receptors (c), microvillar cells (m), supporting cells(5). and basal cells (b). The arrows point to ciliated olfactory knobsof the bipolar receptor cells. d = degenerating cells; bs = base ofthe supporting cells; Ip = lamina propria; n = nerve bundle, bg =
Bowman gland. (From Moran D. T ., Rowley J.C., Jafek B. W ..et al.The fine structure of the olfactory mucosa in man. J. Neurocytol.11:721-746.1982. Published by Chapman & Hall.)

392 CRANIAL NERVES AND THEIR DISORDERS
cells and cells within the periglomerular and externalplexiform layer regions. The mitral and tufted cellaxons form the lateral olfactory tract, which projectsto more central brain regions, including the anteriorolfactory nucleus, the prepiriform cortex, the peri-amygdaloid cortex, the olfactory tubercle, the nucleusof the lateral olfactory tract, and the corticomedialnucleus of the amygdala (for details on central pro-jections, see Brodal, 1981; Haberly and Price, 1977;Kretteck and Price, 1977a,b, 1978; MacLeod, 1971;Powell et al., 1965).
The mitral and tufted cells are involved in complexreverberating circuits in which negative feedback andpositive feedback occur. For example, mitral cells canmodulate their own output via the stimulation ofgranule cells (which are inhibitory to them) or viastimulation of excitatory inputs within the externalplexiform layer. Reciprocal inhibition between neigh-boring mitral or tufted cells presumably results insharpening the contrast between adjacent channels,similar to that seen in visual and tactile pathways(MacLeod, 1971).
Although the manner in which specific olfactoryinformation is conveyed via the first-order neuronsis not well understood, the initial component of theolfactory code is mediated by a large ensemble ofsensory cells, each of which conveys a fraction of theinformation that signifies the nature of the odorant(Lancet, 1986). Odorants absorb into the mucus cov-ering the olfactory epithelium and diffuse (alone orin conjunction with carrier proteins) to the cilia andterminal / rocesses of olfactory receptor cells, wherethey bin to proteinaceous receptor sites located onone or both of these structures (Rhein and Cagan,1981). This process leads, at least for some odorants,to the activation of a membrane-bound G protein,which in turn induces an adenylate cyclase-mediatedincrease in intracellular cyclic AMP (cAMP) Oonesand Reed, 1989; Menevse et al., 1977; Pace et al.,1985). As in other senses, intensity is coded, in part,by the relative frequency of firing in the afferentneurons (cf. Drake et al., 1969; Osterhammel et al.,1969). Interestingly, and as would be expected fromthe aforementioned observations, the perceived in-tensity of some odors to humans is correlated withthe degree to which they induce adenylate cyclaseactivity in ciliary preparations (Doty et al., 1990).Odor quality is presumably coded via some type ofa cross-fiber pattern, because individual oliactoryreceptor cells respond to a wide range of odorants,have response spectra that do not completely over-lap, exhibit different types of responses to appliedstimulants (e.g., although most receptor- £ellsevi-dence excitatory responses, some evidence inhibitoryresponses, and others, on-off respons,es), and havehighly overlapping response spectra (Mair andGesteland, 1980; Sicard and Holley, 1984).
(Graziadei, 1973). This property may explain thephenomenon of the delayed return of olfactory func-tion in some persons after viral insult to the olfactoryneuroepithelium. However, some fully differentiatedolfactory receptor cells can be quite long lived, and,under nonpathologic conditions the receptor cellturnover may largely represent newly formed cellsthat fail to establish synapses within the olfactorybulb (Hinds et al., 1984).
The unmyelinated axons of the primary receptorcells traverse the lamina propria, form fine bundlessheathed by Schwann cells (which course throughthe cribriform plate), and enter the olfactory bulb,synapsing in spheric masses of neuropile termedglomeruli (Fig. 27-3). These complex structures con-sist of interwoven processes of the receptor cell axonswith mitral, tufted, and periglomerular cell dendritesor processes. Because many more neurons enterglomeruli than leave them, they are a focus of a highdegree of convergence of information (A.C. Allisonand Warwick, 1949). These spheric structures are akey component of all olfactory systems, being presenteven in insects (MacLeod, 1971; Shepherd, 1972).
As can be seen in Figure 27-3, the mitral andtufted cells are large second-order neurons withprimary dendrites entering the glomeruli and withsecondary dendrites terminating in various regionsof the bulb. These cells give off collaterals along theircentrally directed course that interact with granule
"'--L!.2!:;.l
Figure 27-3. Diagram of major layers and types of olfactory bulbneurons in the mammalian olfactory bulb. as based on stainedGolgi's material. Main layers are indicated on left as follows: ONL= olfactory nerve layer; GL = glomerular layer; EPL = externalplexiform layer; MBL = mitral body layer;IPL= internal plexiformlayer; GAL = granule cell layer. ON = olfactory nerves; PGb =periglomerular cells with biglomerular dendrites; PGm = periglo-merular cell with monoglomerular dendrites; SAe = short-axon cellwith extraglomerular dendrites; M = mitral cell; MfTd = displacedmitral or deep tufted cell; Tm = middle tufted cell; Ts = superficialtufted cell; Gm = granule cell with cell body in mitral body layer;Gd = granule cell with cell body in deep layers; SAc = short-axoncell of Cajal; SAg = short-axon cell of Golgi; C = centrifugal fibers;AON = fibers from anterior olfactory nucleus; AC = fibers fromanterior commissure; LOT = lateral olfactory tract. (From ShepherdG.M. Synaptic organization of the mammalian olfactory bulb. Phys-iol. Rev. 52:864-917.1972.)
Clinical Evaluation of Olfactory Function
Olfactory distortion or loss arises from a numberof causes, including intranasal pathologic conditions

393SMELL AND TASTE AND THEIR DISORDERS
(e.g., sinusitis, rhinitis), mechanical obstruction ofthe nasal airways, environmental or industrial pol-lutants, aging, and various medical and psychologicconditions (e.g., Alzheimer's disease, Parkinson'sdisease, Korsakoff's psychosis, and cystic fibrosis)(Amoore, 1986; 1988a,b; 1989b; Doty, 1979; Doty andFrye, 1989; Doty et al., 1984b; Schiffman, 1983;Schwartz et al., 1989) (Table 27-1). Overall incidenceof smell loss after head injuries is approximately 7%,although this figure is much higher in cases of severeinjury (ranging from 30 to 80% [cf. Sumner, 1976]).In the past, olfactory disorders were rarely examinedquantitatively, largely because of the lack of stan-dardized assessment procedures. Fortunately, signif-icant progress has been made in the area of clinicalmeasurement of olfactory function, permitting moredetailed clinical discription of olfactory disturbances.
Classification of Olfactory Disorders
Both the patient's complaint and the objectivesensory diagnosis can be adequately classified withinthe following schema:
Table 27-1. EXAMPLES OF DISORDERS REPORTEDTO BE ASSOCIATED WITH OLFACTORY
DYSFUNCTION
General (or total) anosmia-inability to detect anyqualitative olfactory sensations
Partial anosmia-ability to detect some, but not all,qualitative olfactory sensations
General (or total) hyposmia-decreased sensitivity toall odorants
Partial hyposmia-decreased sensitivity to some,but not all, odorants
Dysosmia-either a distortion in the perception ofan odor (e.g., the presence of an unpleasantodor when a normally pleasant odor is beingsmelled) or the presence of an odor that occursin the absence of active smelling or sniffingbehavior (sometimes termed an olfactory hallu-cination)
General (or total) hyperosmia-increased sensitivityto all odors
Partial hyperosmia~increased sensitivity to onlysome odors
Agnosia-inability to recognize an odor sensation,even though olfactory sensory processing, lan-guage, and general intellectual functions aresufficiently intact so that the recognition failureis not due to deficits in one or more of thesefunctions
Separate determination of the patient's complaintand the objectively determined sensory disorder isimportant, because the two do not always coincide.Although other classification schemes are utilized inthe literature (e.g., dysosmia is sometimes used as ageneric term under which the other classes fall), theterminology just given suffices to categorize the vastmajority of olfactory complaints and dysfunctions.
Sensory Assessment of Olfactory Function
Quantitative assessment of olfactory function isessential for a number of reasons: first, to establishthe validity of the patient's complaint; second, tocharacterize the exact nature of the problem (whichis critical for establishing a diagnosis); and third, tomonitor objectively the efficacy of any interventionsor treatments. In addition, some tests of smell func-tion provide means for detecting malingering (cf.Doty, 1989; Doty et al., 1984a,b). Such detection isparticularly important in litigation cases, as a numberof courts have awarded sizable sums of money forloss of olfactory function.
Psycho.physical procedures remain the primarymeans by which olfactory function is assessed in theclinic, even though certain electrophysiologic tech-niques offer the theoretic advantage of not beingdependent on a patient's verbal response (e.g., av-eraged evoked potentials) (for review, see Doty ,1991). Controversy surrounds the validity of olfactoryevoked potentials and other odorant-inducedchanges in electrophysiologic measures (e.g., heartrate changes), as they are highly variable and theirneural origin is difficult to determine (cf. I. Allisonand Goff, 1967; Lorig, 1989; Plattig and Kobal, 1979;
EndocrineAdrenocortical insufficiencyCushing's syndromeDiabetes mellitusHypothyroidismKallmann's syndromePrimary amenorrheaPseudoh ypopara thyroidismTurner's syndrome
Local Diseases and MechanicalObstruction of Airways
Adenoid hypertrophyAllergic rhinitisAtrophic rhinitis (ozena)Bronchial asthmaDeformity caused by traumaExposure to toxic chemicalsLeprosyMalignant disease of paranasal
sinuses with extension intonasal cavities
Nasal polyposisSinusitisSjogren's syndromeTumors of nasopharynx with
extension into nasal cavitiesVasomotor rhinitis
NeurologicAlzheimer's diseaseEpilepsyHead traumaHuntington's choreaIntracranial surgeryKorsakoff's psychosisMultiple sclerosisParkinson's disease
Data from Doty R.L. A review of olfactory dysfunctions in man. Am. 1Otolllryngol. 1:57-79. 1979; and Schiffman 5.5. Tast~ and smeU in disease.N. Engl. I. Mtd. 3O8:127S-1279. 1337-1343, 1983.
NutritionalChronic renal failureCyanocobalamin (vitamin B,J
deficiencyKorsakoff's psychosis
Psychi~tricDepressionOlfactory reference syndromeSchizophreniaTumonIntracranial
Aneurysms of the anteriorcommunicating bifurcation
Frontal lobe gliomaHydrocephalusIntemal carotid aneurysms
extending over thepituitary fossa
NeuroblastomaSuprasellar meningiomaSphenoid ridge meningiomaOther meningiomas
IntranasalAdenocarcinomaInverted papillomaMelanomaSquamous cell carcinoma
Vir~1 ~nd infectiousAcute viral hepatitisHerpes simplexInfluenza-like infections

394 CRANIAL NERVES AND THEIR DISORDERS
D.B. Smith et al., 1971). Although psychophysicalresponses can be obtained from subjects injectedintravenously with an odorant (a potentially usefulmeans of assessing the presence of intact cranialnerve I function in persons with nasal diseases thatprevent testing with airborne odorants), the physio-logic basis of this phenomenon is controversial (Ma-runiak et al., 1983), and sound normative data arenot available for the interpretation of such tests.
The first step in assessing olfactory function is todetermine the degree to which qualitative olfactorysensations are present. For this assessment, we rou-tinely use a 4O-item microencapsulated ("scratch 'nsniff") smell test (termed the University of Pennsyl-vania Smell Identification Test; commercially avail-able from Sensonics, Inc., Haddonfield, NJ). Thistest is highly reliable (test-retest reliability is. 95 [cf.Doty et al., 1984a, 1989b», allows the classificationof patients into discrete categories of dysfunction,provides a percentile score of a patient's performancerelative to age- and sex-ffiatched controls, and hasprocedures for detecting malingering. Scores on thistest reflect both gross and subtle olfactory problemsassociated with current and previous smoking be-havior (Frye et al., 1990) and numerous neurologicdiseases (e.g., Alzheimer's disease, Korsakoff's psy-chosis, arid Parkinson's disease [Fig. 27-4) and cor-relate highly with the levels of certain catecholaminemetabolites in the cerebrospinal fluid of some patientgroups (e.g., r == .90 with the lumbar levels of 3-
methoxy-4-hydroxyphenylglycol in patients withKorsakoff's psychosis [cf. Mair et al., 1983». Therelationship between age and the scores on thisstandardized test is presented in Figure 27-5, whichshows the pattern of smell loss in the elderly (Dotyet al., 1984b). It is also apparent from this illustrationthat, on the average, women score higher on thistest than men.
A second step in assessing smell function is todetermine the absolute level of an odorant that thepatient can detect. Although air-dilution olfactometryis the method of choice in presenting stimuli for suchan assessment, it is not practical in the typical clinical
setting. An alternative approach is to present odor-ants diluted in a liquid diluent (e.g., odorless mineraloil) via small vessels held over the nose (i.e., "sniffbottles"). We most commonly use the rose-like odor-ant phenyl ethyl alcohol for such a test, because it ispleasant smelling at higher concentrations, elicitsrelatively little trigeminal activity, and is easily dis-solved in most diluents (Doty et al., 1978; 1984a).Although several psychophysical procedures can beused to establish a threshold estimate, a modifiedascending single staircase procedure is preferable,because higher concentrations are initially avoided(minimizing adaptation effects) and a stable measurecan be established with a minimal number of trials(see Cornsweet, 1962; Doty et al., 1984a; Ghorbanianet al., 1983).
Although detection threshold values typicallyagree with results obtained from smell identificationtests, in some instances patients who fail identifica-tion tests perform normally on detection tests. How-ever, the reverse rarely occurs. Because some patientscan use subtle non-cranial nerve I cues to obtain lowdetection thresholds, the results of the identificationtest are weighted more heavily in ascertaining asensory diagnosis than are those from the thresholdtest. Care must be taken in making this judgment,however, because an odor identification test can besensitive to distortions of smell function that areunaccompanied by changes in the detection thresh-old, including some forms of agnosia. Even thoughsuch conditions are rare compared with uncompli-cated smell losses caused by viruses and nasal ob-struction, they must be kept in mind in cases inwhich central nervous system damage is known orsuspected.
On rare occasion, it is useful to evaluate unilateralolfactory function by occluding each nostril. How-ever, the patency of the nasal airways cyclicallyfluctuates in most persons (the so-called nasal cycle)and the majority of olfactory disorders occur bilater-ally, including the dysfunction associated with Par-kinson's disease (Doty et al., 1991c).
Although a number of other procedures are avail-

395SMELL AND TASTE AND THEIR DISORDERS
-..40...~~
~
'j35~
~T
~ Z:'I-.OT ~-4-1;9ij--- "I j
'1'/,
;ill
Figure 27-5. Scores on the University of ~30Pennsylvania Smell Identification Test as a ~function of age in a large heterogeneous 1:group of subjects. Numbers by data points iindicate sample sizes. (From Doty. R.L., Sha- ---25man P.. Applebaum S.L., et al. Smell identifi- wcation ability: changes with age. Science 3226:1441-1443, 1984. Copyright 1984 by the §AAAS.) 1- 20
<7>Q.:;)
~'5<{Ow~
4C
SMELL IDENTIFICATION TEST SCORES~5e,'i'...'..'.
36 i "'FEMALES (n= 11581
0 0 MALES (n= 7971
TOTAL GROUP ( N = 19551
10-19 20-29 30-39 40-49 50-59 60-69 70-79 80-89 90-99
AGE GROUP (yEARSJ
5-9
able for assessing olfactory function, such as magni-tude estimation and multidimensional scaling, moreresearch is needed to determine whether they con-tribute substantially to the clinical information ob-tained by the aforementioned tests. Procedures suchas magnitude estimation, although quite economicalof time, share with thresholds the problem of markedbetween-subject variability , and-depending on theodorant used-may not be as sensitive to a numberof subject-related variables as detection thresholdmeasures (cf. Berglund et al., 1971; R.L. Doty, un-published observations).
During the physical examination, the physicianshould pay special attention to the nose and theupper respiratory tract. This necessitates endoscopicexamination of the nasal cavity, the meati, the sep-tum, and the sinus ostia. Small polyps may be found,which otherwise would have gone undetected. Anasopharyngeal neoplasm or its metastasis to theneck may be discovered. Neurologic examination ofthe orbital contents and the cranial nerves may directattention to a lesion of the skull base. Although aseverely deviated nasal septum may playa role inolfactory dysfunction (Leopold, 1988), most septaldeviations are unrelated to the ability to smell.
The following laboratory studies are recommendedwhen clinically indicated: complete blood count withwhite blood cell differential count, serum levels ofcalcium and angiotensin-converting enzyme (may beelevated in sarcoidosis), erythrocyte sedimentationrate (may be elevated in inflammatory disorders,such as Wegener's granulomatosis), serologic testsfor syphilis, and serum levels of glucose and creati-nine. Imaging studies of the nose, paranasal sinuses,and cranial contents are critical to the evaluation.This is best done with computed tomography or mag-netic resonance imaging in the axial, coronal and/orsagittal planes. Biopsy of the olfactory neuroepithel-ium has been performed in the research setting butis not done routinely in tb~ ~Iinic (Lovell et al., 1982).
After all information is gathered; -a--dritgnosis -is-reached. Usually, the cause of the olfactory dysfunc-tion is (1) obstruction of odorant access to the neu-roepithelium by inflammation or, rarely, neoplasm;(2) damage to the olfactory neuroepithelium; or (3)damage to the central olfactory pathways. Obstruc-tive problems can result from allergic rhinitis, nasalpolyps, chronic rhinosinusitis, and benign or malig-
Medical Examination and Treatment ofPatients with Olfactory Disorders
The aim of the medical evaluation is to identify thecause of the olfactory dysfunction and to correct theproblem, if possible. The patient's history is ex-tremely important in arriving at a diagnosis. Thephysician needs to assess the pattern of loss (suddenonset, gradual), its duration (days, months, years),preceding events (e.g., head trauma, viral infection),and any accompanying medical disorders (e.g., nu-tritional defect, neurologic conditions [e.g., parkin-sonism)). Specific nasal symptoms, especially epi-staxis, nasal pain, rhinoYrh-ea;-and obstruction,should be elicited; these may direct attention to aninflammatory or neoplastic disorder. A history ofallergy or nasal polyps is important, because thesedisorders can lead to olfactory dysfunction. A familyhistory of other chemosensory or neurologic diseasesshould be sought; environmental exposure to irri-tants and chemicals should be reviewed with the
patient.

396 CRANIAL NERVES AND THEIR DiSORDERS
Howe and Gibson (1982) reviewed 273 patientswith complex partial seizures. Only 22 had olfactoryand 9 had gustatory hallucinations with their sei-zures. Six had both. Three of these were proved tohave gliomas, and one, an arteriovenous malforma-tion. These authors pointed out that, overall, thefrequency of tumors in this group was not higherthan would be expected in patients with temporallobe epilepsy.
Studies of patients undergoing surgical treatmentof intractable psychomotor seizures suggested thatthe amygdala is an essential element for the elabo-ration of olfactory auras and that amygdalotomy caneliminate such hallucinatory phenomena (Andy etal., 1975). For example, Chitanondh (1966) reportedsuccessful treatment of seven patients with seizuredisorders, olfactory hallucinations, and psychiatricproblems by stereotaxically placed amygdalotomiesand that "stereotaxic amygdalotomy has a dramaticeffect upon olfactory seizures, auras and hallucina-tions. It is a safe surgical procedure and can be donewithout neurological deficit."
Although few detailed psychophysical studies ofolfactory function have been performed in patientsreceiving amygdalotomies, there is some indicationthat bilateral amygdaloid lesions have at least someadverse effect on odor differentiation and identifica-tion (Andy et al., 1975). Clearly, unilateral excisionof 5-7 cm of the anterior temporal lobe for intractableepilepsy has detrimental effects on odor quality dis-crimination, immediate and delayed recognitionmemory , ability to match an odor to its visually orhaptically presented source, and the verbal identifi-cation of odors (Eskenazi et al., 1983). However,odor detection ability per se appears to be unim-paired, and the benefits derived from the eliminationof olfactory hallucinations and seizure activity bysuch procedures appear considerable.
It is possible to characterize routinely most olfac-tory problems quantitatively and to use this infor-mation, along with that obtained from the historyand the physical examination, to determine the causeof the dysfunction. Unfortunately, with the exceptionof odorant access problems within the nose and thoserare cases in which dysosmia is associated with clear-cut seizure disorders, meaningful treatments are notavailable for most olfactory problems. Although zincand vitamin therapies have been suggested in theliterature, there is no compelling evidence that thesetherapies are effective, except in cases in which frank.zinc or vitamin deficiences exist. Even though somedysosmias are reportedly cured by periodic anesthe-tization of the olfactory receptor region, most dysos-mias remit spontaneously, and such treatment oftenprovides only temporary relief. Extremely debilitat-ing, long-standing, severe dysosmia may be amena-ble to treatment either by resection of one or botholfactory bulbs (Kaufman et al., 1988) or by operativedestruction of segments of the olfactory neuroepi-thelium (Leopold et al.. 1990).
nant nasal neoplasms. Overuse and abuse of topicalnasal sprays (as in rhinitis medicamentosa) is alsoseen. Direct injury to the neuroepithelium can becaused by nasal or skull base surgery , externaltrauma, topical or systemic effects of drugs (cocaine,aminoglycoside antibiotics), and most commonly,viruses, such as herpes simplex and influenza.
Trauma, although capable of shearing the finenerve fIlaments of cranial nerve I from the olfactorybulb at the cribriform plate, can also have centralcauses (sumner, 1976), and animal research has re-vealed that intracranial hemorrhage can lead to de-generation of the olfactory epithelium without tran-section of the olfactory nerve (Nakashima et al.,1984b). It is generally believed that long-standingcases of anosmia not caused by intranasal disease orblockage are likely permanent and untreatable withcurrent therapies.
Of considerable significance to the neurologist arethe findings that Alzheimer's disease, Korsakoff'spsychosis, Huntington's chorea, idiopathic Parkin-son's disease, and the parkinsonism-dementia com-plex of Guam are accompanied by cIear-cut altera-tions in smell function (Doty et al., 1987, 1988b,1989a, 1991a,b,c; Mair et al., 1983; Moberg et al.,1987; Peabody and Tinklenberg, 1985; Ward et al.,1983). Such alterations are consistent, in several ofthese conditions, with known biochemical and mor-phologic anomalies in brain regions associated witholfaction, including the primary and secondary olfac-tory pathways (Esiri and Wilcock, 1984; Reyes et al.,1986). Indeed, lesions within the olfactory systemappear to be among the first pathologic changes tooccur in Alzheimer's disease (Hyman et al., 1984),and punctate lesions in monoamine-rich regions ofthe brain stem and diencephalon of patients withKorsakoff's psychosis likely relate to the previouslynoted correlation be~'een their smell identificationtest scores and lumbar cerebrospinal fluid levels of3-methoxy-4-hydroxyphenylglycol (Mair et al., 1983).Interestingly, MPTP-induced parkinsonism is unac-companied by major olfactory dysfunction (Doty etal., 1991b).
It is also significant that a variety of intracranialtumors can influence smell function (for review seeDoty, 1979). For example, it has been estimated that20% of the tumors of the temporal lobe or lesions ofthe uncinate convolution produce olfactory distur-bances, usually in the form of unpleasant smellhallucinations (e.g., Furstenberg et al., 1943).
Most authors believe that olfactory auras occur inassociation with temporal lobe seizures (Daly, 1958b;Holmes, 1927; Jackson, 1869, 1880; Penfield and Kris-tiansen, 1951; Weiser et al., 1985). Gloor et al. (1982),elaborating on this, suggested that the mesiotem-porallimbic structures, but not the temporal neocor-tex, were essential for such symptoms. Auras havebeen variously described and include smells resem-bling burning oil (Penfield and Kristiansen, 1951),peaches, lemons (Daly, 1975), blood (Daly, 1958a),and "something to do with animals" (Gloor et al.,1982).

SMELL AND TASTE AND THEIR DISORDERS 397
GUSTATION
Patients commonly fail to distinguish between fla-vor and taste and often report loss of taste sensationin the presence of normal sweet, sour, bitter, andsalty responsiveness. Although true loss of gustatoryfunction exists, it is rare, as taste responsiveness ismediated bilaterally by four nerves within the oralcavity , as indicated in the next section. Thus, anumber of studies report that less than 1% of headinjury patients exhibit true taste loss, as comparedwith more than 7% overall for loss of olfactoryfunction (Sumner, 1976). In our experience, strangetaste sensations (i.e., dysgeusias) are much morecommon than taste losses or decrements per se.
Anatomy and Physiology of Taste
sense, one cannot view this type of stimulation asbeing taste, such stimulation is critical in determiningthe overall gestalt of flavor, such as that experiencedwhen eating spicy foods like chili.
Taste buds are located in the oral cavity on the softpalate and tongue, the pharynx, the larynx, and theesophagus. The largest number are on the surface ofthe tongue, being associated with visible protuber-ances termed papillae. Of the four types of papillae-fungiform, foliate, circumvallate, and filiform-onlythe first three harbor taste buds. The location of thesetypes of papillae varies, with the circumvallate pa-pillae being arranged in an inverted Vat the borderbetween the anterior two-thirds and the posteriorone-third of the tongue. The club-like fungiformpapillae are scattered on the anterior two-thirds ofthe tongue, and the foliate papillae are located onthe lateral border of the posterior middle third of thetongue (Fig. 27-6A).
Up to 200 taste buds are present in each circum-vallate papilla, whereas far fewer buds are presentin each of the other types. The pores of the circum-vallate taste buds open into a furrow or moat, sepa-rating each papilla from the surrounding tissue.Secretions from the glands of von Ebner enter thismoat, which acts as a container for the taste solu-tions. Taste buds associated with the foliate papillaeare similarly positioned within the walls of furrows,unlike the taste buds in the fungiform papillae, whichare positioned within a small opening at their top(Fig. 27-68).
The innervation of the taste buds is complex. Theafferent fibers from the buds within the fungiformpapillae and from trigeminal nerve endings enter thelingual nerve. The taste fibers subsequently join thechorda tympani nerve, which merges with the facialnerve in the temporal bone. These fjbers enter thebrain stem with the nervus intermedius. The tastebuds of the circumvallate and foliate papillae aresubserved by fibers traveling directly to the brainstem with the glossopharyngeal nerve, although theanterior folds of the foliate papillae may be inner-
The peripheral receptors for taste-the tastebuds-are round epithelial structures consisting ofslender cells arranged like the segments of a grape-fruit (Fig. 27-6C). The long axis of the taste bud isperpendicular to the surface of the epithelium. Thesuperficial portion of the bud is marked by an exca-vation, the taste pit, into which the microvilli of thesensory cells project. Several cell types are discerniblewithin the taste bud. Thus, histologic studies reveallight and dark cells that bear microvilli that projectinto the taste pit. There is also a light cell with aclub-like ending, as well as basal cells (Murray, 1973).These different cell types are presumed to representdifferent stages of generation and degeneration ofthe sensory taste cells. Cell turnover is thought tooccur during a 1O-day interval, at least in the rat(BeidJer and Smallman, 1965).
As in the olfactory system, somatosensory sensa-tions (e.g., stinging, burning, cooling, and sharp-ness) can be induced by some oral stimulants viatrigeminal afferents located on the tongue andthroughout the oral cavity .Although, in a strict
FIgure 27-6. (A and B) Distribution oftaste buds on the human tongue. Tastebuds of the fungiform and foliate papillaeare innervated by cranial nerve VII. Thoseof the circumvallate papillae are innervatedby cranial nerve IX. Cranial nerve V carriesnontaste somatosensory sensations. Seetext for details. (C) Fine structure of tastebud. 1 and 2 = presumably suppor1ingcells that secrete materials into the lumenof the bud; 3 = sensory receptor cell; 4= basal cell from which the other cell
types arise. (Modified from Shepherd G.M.Neurobiology. New York, Oxford Univer-sity Press. 1983.)

398 CRANIAL NERVES AND THEIR DISORDERS
As in the case of olfaction, taste intensity in hu-mans has been shown to correlate with the magni-tude of the neural response (as measured electro-physiologically from the chorda tympani nervebundle as it crosses the tympanic membrane) (Oia-mant et al., 1965). The nature of quality coding ismore complex, and there are proponents of bothlabeled line and cross-fiber patterning theories. Otherinvestigators believe that this distinction is artificialand subsume labeled line theory within a cross-fiberpatterning theory .Regardless of such theoretic dis-tinctions, there is evidence at the level of the first-order neuron for reasonably discrete classes of neu-rons (within a broadly tuned population of cel1s) thatcan be identified as responding best to specific tas-tants. For example, there are sweet-sensitive fibersin the hamster chorda tympani nerve that increasetheir fIring rates more vigorously to sucrose than toother tastants (Frank, 1973). Analogous cell types areseen for stimulants representing nonsweet taste cat-egories. However, recordings in taste-related neu-rons in the brain stem suggest that the central fibersare much more broadly tuned than are the first-orderneurons (0. V. Smith et al., 1983). It is noteworthythat substances have been discovered that selectivelyalter taste perceptions. For example, miraculin, aglycoprotein from the berry of the African shrubSyncqJa1um di1cificum, produces an alteration of allsour tastes to a sucrose-Iike sweetness. Gymnemicacid, an extract from the leaves of the Indian plantGymntmQ sy1vestre, can block the perception of sweetsensation (and the corresponding electrophysiologicactivity) without significantly altering the perceptionof the other taste qualities (for review of taste modi-fiers, see I<urihara, 1971).
vated by the chorda tympani nerve in some species.The afferents from taste buds on the palate travelwith the greater superficial petrosal nerve, whichjoins the facial nerve at the geniculate ganglion. Tastebuds of the larynx and the esophagus are subservedprimarily by vagal afferents.
The peripheral gustatory nerve fibers enter thebrain stem and project to the nucleus of the tractussolitarius, which begins in the rosterolateral medullaand extends caudally along the ventral border of thevestibular nuclei. Chorda tympani fibers synapserostral to the glossopharyngeal fibers. The centralrelays for the receptors on the palate probably projectto the region innervated by the chorda tympani, andthose for the receptors subserved by the vagus, to aregion caudal to the projection of the glossopharyn-geal.
The taste fibers subsequently project from thenucleus of the tractus solitarius to the pontine para-brachial nuclei (at least in the rat). From there, twodivergent pathways arise. One synapses in the thal-amus and continues to the cortical gustatory area.There may also be direct connections that by-passthe thalamus. The second pathway from the para-brachial nuclei distributes broadly to the ventralforebrain. Although little is known about these path-ways in the human, there is physiologic evidencethat the primary cortical area for taste in other pri-mates is located deep in the parietal operculum andadjacent parainsular cortex (see Norgren, 1984).
Hausser-Hauw and Bancaud (1987) provided clin-ical evidence that supports this conclusion in a groupof 30 patients who manifested gustatory hallucina-tions during epileptic seizures. Such symptoms couldhave resulted from seizures of parietal or temporalorigin or occur after electrical stimulation of thehippocampus, the amygdala, the rolandic or parietaloperculum, or the first or second temporal convolu-tions. However, whereas they were intermixed withother symptoms in the case of temporal lobe seizures,they occurred as isolated or prominent symptoms inthe case of parietal seizures or parietal or rolandicstimulation. One of their patients and one describedby Penfield and Faulck (1955) reported resolution ofgustatory symptoms after resections of the parietaloperculum. However, Hausser-Hauw and Bancaud(1987) noted that 4% of 305 patients with temporallobe seizures, but only 2% of 309 patients withsuprasylvian seizures and 3% of 102 patients withsuprasylvian and infrasylvian seizures, reported gus-tatory symptoms; they suggested that reorganizationof cortical pathways in patients with temporal lobeepilepsy accounted for the discrepancy .An alterna-tive possibility, suggested by Gloor et al. (1982), isthat activation of mesiotemporal structures is neces-sary before symptoms such as taste achieve experi-ential immediacy .Hausser-Hauw and Bancaud (1987)reviewed the physiologic and anatomic evidence,~hi.ch supports the presence of taste pathway pro-)ections to the amygdala, particularly its central nu-cleus. Such a pathway might provide an additionalexplanation for the observations of Gloor et al. (1982).
Clinical Evaluation of Taste Function
Numerous factors influence normal gustatory func-tion. It should be re-emphasized, however, that mostpatients with the complaint of loss of taste evidence,on psychophysical examination, normal taste func-tion and abnormal smell function. For this reason, itis useful to use the term flavor in describing thecomplex synthesis of gustatory , olfactory , and So-matosensory sensations. Whole-mouth taste deficitsare uncommon.
Many of the same conditions that are assoCiatedwith olfactory disturbances are also reported to influ-ence taste function. For example, taste disorders havebeen reported after head trauma, zinc deficiency ,adrenocortical insufficiency , and viral infections (fa-ble 27-2). In addition, however, taste disturbancesappear to be present much more frequently thanolfactory ones as a result of the use of pharmacologicagents, such as antirheumatic drugs, antiproliferativedrugs, and substances bearing a sulfhydryl group(e.g., penicillamine and captopril). Although the

399SMELl AND TASTE AND THEIR DiSORDERS
ways. Malnutrition associated with these tumors canalso lead to ageusia. Significant increases in recog-nition thresholds for bitter in patients with metastaticcarcinomas and decreases in such thresholds for sourin breast cancer patients were reported (Settle et al.,1979). Radiation therapy alters taste bud cell turnoverand can affect taste function, although return afterradiation treatment has been observed (Conger,1973).
Gustatory symptoms have been reported in asso-ciation with epileptic seizures for more than a century(Daly, 1958a; Gowers, 1909; Holmes, 1927; Jackson,1990; Wieser et al., 1985). Daly (1975) suggested thatsuch sensations reflect those basic to taste (sweet,acid, bitter, and salty), although sweet tastes seemto occur less frequently. Tastes have been describedas peculiar, rotten (Penfield and Kristiansen 1951),sweet-along with a pungent odor (Daly, 1958b), orlike a cigarette, rotten apples, or vomitus (Hausser-Hauw and Bancaud, 1987). However, as noted ear-lier, many of the latter tastes likely represent smellsensations that are miscategorized as tastes by boththe patients and their physicians.
Although taste acuity declines with age, the per-ceptual decrease is not as marked as that seen forolfaction (Cowart, 1981; Weiffenbach, 1984; Weiffen-bach et al., 1982). Nonetheless, in conjunction withthe loss seen in the sense of smell, such decrementsmay lead to anorexia, weight loss, and malnutritionin some of the elderly.
mechanisms responsible for such phenomena arepoorly understood, a number of taste stimuli canelicit taste perceptions when injected into the blood-stream, analogous to the intravascular olfaction phe-nomenon discussed earlier (Bradley, 1973).
Deficiency (as in Sjogren's syndrome) or hypervis-cosity of saliva leads, in time, to lessened taste acuity ,presumably as the result of accompanying decreasesin the number of papillae and taste buds and possiblefunctional alteration in the remaining taste buds(Brightman, 1971). Whether such morphologic alter-ations in humans are due to the elimination oflubricating or trophic activity from the saliva is notknown. In our experience, neither artificial saliva norwater mouthwashes have proved successful in re-storing normal taste function in patients with xero-stomia. However, systematic research is needed toascertain whether such materials can improve tastefunction in certain types of xerostomia.
Post.traumatic ageusia is much less common thanpost-traumatic anosmia. Ageusia to one or more ofthe primary taste modalities is believed to occur inless than 1% of persons with major head injury(Sumner, 1976). Although the literature is scant, theprognosis for post-traumatic ageusia is far better thanfor post-traumatic anosmia. Considerable contro-versy exists regarding the underlying cause of mosthead trauma-related cases of ageusia, because gen-eral ageusia should theoretically be nearly impossibleto induce. Unfortunately, many of the reports ofageusia in the literature are based on the patient'sreport rather than on the results of sound psycho-physical testing, so they may not reflect the trueincidence of this problem and, in some instances,may actually be mislabeled cases of anosmia (Deemset al., 1991).
Complaints of taste loss or distortion are commonlyreported in various carcinomas. For example, squa-mous cell carcinoma of the mucous membranes ofthe upper aerodigestive tract can interfere with tasteby direct destruction of receptors and neural path-
Classification of Taste Disorders
As for olfactory disorders, we classify the patient'scomplaint and the results of sensory tests separately.The terms we use for such classification are as fol-lows:
Total ageusia-Iack of taste sensation to all tastantsPartial ageusia-Iack of taste sensation to some
tastants
Table 27-2. EXAMPLES OF DISORDERS REPORTED TO BE ASSOCIATED WITH GUSTATORY DYSFUNCTION
Nutrition~1CachexiaChronic renal failureCirrhosis of the liverNiacin (vitamin BJ deficiencyZinc deficiency
PsychiatricDepressionSchizophrenia
TumorsOral cavity cancerBase of skull neoplasia
EndocrineAdrenocortical insufficiencyCongenital adrenal hyperplasia
PanhypopituitarismCushing's syndromeCretinism
HypothyroidismDiabetes mellitusTurner's syndromePseudoh ypoparath yroidism
InflammatoryInfections
Candidiasis
GingivitisHerpes simplexPeriodontitisSialadenitis
Autoimmune
PemphigusSjogren's syndrome
local Alterations of Taste Buds or PapillaeChemicals, drugsXerostomia
NeurologicBell's palsy. Epilepsy
Familial dysautonomiaHead traumaMiddle ear operations with manipulation or
damage to chorda tympaniMultiple sclerosisRaeder's paratrigeminal syndrome
Data from Doty R.l. A review of olfactory dysfunctions in man. Am. ,. Oto/4ryngol. 1:57-79, 1979; and Schiffman 5.5. Taste and smeU in disease. N. EnglI M,J ~:I275-l279, 1337-1343, 1983.

400 CRANIAL NERVES AND THEIR DISORDERS
Total hypogt'Usia-lessened sensation to all tastantsPartial hypogeusia-lessened sensation to tastants
representing one to three of the four major taste
qualitiesHypergeusia-heightened smell abilityDysgeusia-the presence of a strange or distorted
taste sensation
If a taste problem is suspected on the basis ofsuprathreshold taste testing, patient report, or ap-parent etiology , we additionally determine singlestaircase gustatory detection thresholds analogous tothose performed in olfaction. For these tests, theaforementioned four tastants are used, and abnor-mality is assumed when a patient's threshold valuefalls beyond two standard deviations from that of ahealthy control group.
Regional (quadrant) taste testing is indicated whendamage to one or more of the individual nervesinnervating the taste buds is suspected. Althoughsuch tests are easy to perform on the front of thetongue, it is sometimes difficult to deposit a tastestimulus accurately on the back of the tongue, givenits depth within the oral cavity and the stimulationof the gag reflex. In most cases, tastants can bemicropipet ted into the region, although stimulusspread can be a problem. Although it is possible toconfine the stimulus spread by using small pieces offilter paper soaked in the taste solution, stimuluscontact is not always adequate and difficulties areencountered in retrieving the small pieces of filterpaper. For such regional testing, it is useful to employan automated micropipette to present supra thresholdconcentrations of the four target tastants in a forced-choice paradigm with deionized water rinsing be-tween trials.
Sensory Assessment of Taste Function
Numerous procedures have been developed forevaluating gustatory function, although few data areavailable concerning their reliability or validity. Wefind that taste tests in \\.hich drops of stimulus areapplied to the tongue are less than satisfactory insome instances, because the area stimulated is diffi-cult to control and often the stimulus volume is notlarge enough to induce a reliable response. Althoughelectrogustometric procedures can be of use in estab-lishing gross neural deficit, they have limited use inthe clinic, as the results obtained are dependent onthe electrodes selected (electrical taste may be aniontophoretic phenomenon) and not all taste qualitiescan be reliably elicited. Furthermore, subtle altera-tions in taste function cannot be measured by thesetechniques. In general, when direct current is used,a sour taste is evoked if the anode is applied to thetongue. Current reversal brings about a less distinctresponse described variously as soap-like, metallic,or bitter. Sweet sensations are rarely, if ever, elicitedusing an electrical stimulus.
The initial test we use for assessing gustatoryfunction incorporates a concentration series of su-prathreshold tastants representing sweet, sour, bit-ter, and salty tastes. In this whole-mouth sip-and-spit test developed by R. Gregg Settle, the patient
1. Swishes 10 mI of solution in his or her mouth2. Indicates the taste quality of each stimulus3. Scales the perceived intensity of each stimulus
using a fully anchored nine-point category scale(1 := no taste; 9 = extremely strong taste)
4. Rates the perceived pleasantness of each stimulanton a similar nine-point scale (1 := dislike ex-tremely; 9 = like extremely)
Five concentrations of sucrose, citric acid, sodiumchloride, and caffeine are presented in counterbal-anced order twice during the test, and deionizedwater rinsings are interspersed between stimuluspresentations. This test reveals gross abnormalitiesof taste function, is easy for the patient to perform,and is reasonably economical of time, in that all fourtaste qualities can be evaluated in half the timerequired to obtain a single taste threshold. The he-donic rating serves both as a measure of perceptualaffect (the chemical senses seem particularly focusedon affect) and as a means of assessing gustatoryfunction in a rare class of patients who deny perceiv-ing taste intensity , yet evidence the ability to tastevia correct quality of classification of stimuli andnormal pleasantness functions.
Medical Examination and Treatment ofPatients with Gustatory Disorders
Dysfunction of the taste system can be due to oneor more causes, including the following:
1. Oral medical problems that release bad-tastingmaterials (e.g., gingivitis and sialadenitis)
2. The use of different types of metals in fillings anddental appliances, which results in intraoral cur-rent gradients sensed by the taste system
3. Transport problems of tastants to the taste buds{e.g., caused by dryness of the oral cavity and bydamage of the taste pores or the papillae)
4. Destruction or loss of the taste buds themselves5. Damage to one or more of the neural pathways
innervating the taste buds6. Central neural factors
In addition to performing the standard history andphysical examination mentioned under Medical Ex-amination and Treatment of Patients with OlfactoryDisorders, we palpate and examine the tongue care-fully to detect signs of scaring, inflammation, atrophyof papillae, or neoplasm. Although not done rou-tinely, biopsy of circumvallate or fungiform papillaefor detailed microscopic examination has proved use-ful in determining whether pathologic changes arepresent in taste bud tissue. In cases of suspectedsalivary gland disease, we obtain a biopsy specimenof minor salivary gland tissue in the lower lip todetermine the presence of Iymphoepithelial lesion{indicative of Sjogren's syndrome). In cases in which

SMELL AND TASTE AND THEIR DISORDERS 401
the basis of the dysfunction cannot be ascribed toperipheral factors, we obtain appropriate radiographsto rule out central nervous system tumors or lesions.
Treatment is straightforward in cases in whichdecreased salivation or local oral pathologic alterationcaused by dental factors is the basis of a dysgeusiaor hypogeusia. Saliva can be supplemented by var-ious salivary substitutes. Nutritional deficiencies canbe corrected. Radiation-induced xerostomia may im-prove with time. In some cases, flavor enhancers canbe of at least some benefit.
CONCLUDING REMARKS
The chemical senses of taste and smell determine,in large part, the flavor of foods and beverages andwarn of fire, dangerous fumes, leaking gas, spoiledfoods, and polluted environments. Disorders of thesesenses often result from accidents, disease states,medical interventions, aging, and exposure to a num-ber of environmental pollutants and can serve asimportant indicators of a number of diseases. Thischapter briefly reviewed the anatomy and physiologyof these senses, some etiologic factors responsiblefor their dysfunction, and information regarding theirevaluation and management. It was specifically notedthat most patients with complaints of taste loss have,in fact, olfactory dysfunction and that true taste lossis relatively rare.
References
ity and preference throughout the life span. P)"ychol. Bull. ~:43-71.1981.
Daly D. Ictal affect. Am. I. Psychiatry 115:97-108. 1958a.Daly D. Uncinate fits. Neurology 8:250-2W. 1958b.Daly D.D. Ictal clinical manifestations of complex partial seizures.
Adv. Neurol. 2:57-83, 1975.~ms D.A., Doty R.L., Settle R.G., et al. Smell and taste
disorders: a study of 750 patients from the University of Penn-sylvania SmeU and Taste Center. Arch. Otolaryngol. Head Neck5urg. 117:519-528, 1991.
Diamant H., Oakley B., Strom L., et al. A comparison of neuraland psychophysical responses to taste stimuli in man. ActaPhysiol. Scand. 64:67-74, 1965.
.Doty R.L. A review of olfactory dysfunctions in man. Am. f.Otolaryngol. 1:57-79, 1979.
Doty R.L. The Smell Identijication Test Administration Manual. 2nded. Haddonfield, NJ, Sensonics, 1989.
Doty R.L. Olfactory pSyChophysics. In Laing D.G., Doty R.L.,Breipol W ., eds. The Human Sense of Smell. New York. Springer-Verlag, in press.
Doty R.L., Frye R. Influence of nasal obstruction on smell function.Otolaryngol. Clin. North Am. 22:398-411, 1989.
Doty R.L., Brugger W.E., Jurs P.C., et al. Intranasal trigeminalstimulation from odorous volatiles: psychometric responsesfrom anosmic and normal humans. Physiol. Behav. 23:373-380,1978.
Doty R.L., Shaman P., Applebaum S.L., et al. Smell identificationability: changes with age. Science 226:1441-1443, 1984a.
Doty R.L., Shaman P., Dann M. Development of the Universityof Pennsylvania Smell Identification Test: a standardized mi-croencapsulated test of olfactory function. Physiol. Behav. (Mon-ograph) 32:489-502, 1984b. .
Doty R.L., Reyes P., Gregor T. Presence of both odor identificationand detection deficits in Alzheimer's disease. Brain Res. Bull.18:597~, 1987.
Doty R.L., Deems D.A., Frye R., et al. Olfactory sensitivity, nasalresistance, and autonomic function in the multiple chemicalsensitivities (MCS) syndrome. Arch. Otolaryngol. Head Neck Surg.114:1422-1427,1988a.
Doty R.L., Deems D., SteUar S. Olfactory dysfunction in Parkin-son's disease: a general deficit unrelated to neurologic signs,disease stage, or disease duration. Neurology 38:1237-1244,1988b.
Doty R.L., Riklan M., Deems D.A., et al. The olfactory andcognitive deficits of Parkinson's disease: evidence for indepen-dence. Ann. Neurol. 25:166-171, 1989a.
Doty R.L., Ugrawal U., Frye R.E. Evaluation of the internalconsistency reliability of the fractionated and whole Universityof Pennsylvania Smell Identification Test (UPSIT). Percept. Psy-chophys. 45:381-384, 1989b.
Doty R.L., Kreiss D., Frye R.E. Odor intensity: correlation withodorant-sensitive adenylate cyclase activity in cilia from frogolfactory receptor cells. Brain RL'S. 527:130-134, 1990.
Doty R.L., Perl D.P., Steele J., et al. Odor identification deficit ofthe parkinsonism-dementia complex of Guam: equivalence tothat of Alzheimer's and idiopathic Parkinson's disease. Neurol-ogy 41(Suppl. 2):77-80, 1991a.
Doty R.L., Singh A., Tetrude J., et al. Lack of olfactory dysfunctionin MPTP-induced parkinsonism. (submitted b).
Doty R.L., Stern M.B., Pfeiffer C.. et al. Bilateral olfactory dys-function in early stage medicated and unmedicated idiopathicParkinson's disease. I. Neurol. Neurosurg. Psychiatry (in press c).
Drake B., Johansson, B., von SydoW E., et al. QuantitativeDSychophysical and electrophysi010gical data on some odorouscompounds. Scand. I. Psychol. 10:89-96, 1969.
Esiri M.M., Wilcock. P.K. The olfactory bulbs in Alzheimer'sdisease. I. Neurol. Neurosurg. Psychiatry 47:56-60, 1984.
Eskenazi B., Cain W.S., NoveUy R.A., et al. Olfactory functioningin temporal lobectomy patients. Neuropsychologia 21:365-374,1983.
Frank M. An analysis of hamster afferent taste nerve responsefunctions. I. Gtn. Physiol. 61:588-618, 1973.
Frye R.E., Schwartz B., Doty R.L. Dose-related effects of cigarettesmoking on olfactory function. I.A.M.A. 263:1233-1236, 1m.
Furstenberg A.C., Crosby E., Farrior B. Neurologic lesions whichinfluence the sense of smell. Arch. Otol. 48:529-530, 1943.
(Key references are designated with an asterisk.)Allison A.C., Warwick R.T.T. Quantitative observations on the
olfactory system of the rabbit. Brain 72:186-197, 1949.Allison T., Goff W.R. Human cerebral evoked responses to odor-
ous stimuli. EI«troencephalogr. Clin. Neurophysiol. 22:558-560,1967.
.Amoore J.E. Effects of chemical exposure on olfaction in humans.In Barrow C.S., ed. Toxicology of the Nasal Passages. Washington,DC. Hemisphere Publishing, pp. 155-1CX). 1986.
Andy O.l., lurko M.F., Hughes l.R. The amygdala in relation toolfaction. Con/in. Neurol. 37:215-222, 1975.
Beidler L.M.. Smallman R.L. Renewal of cells within taste buds.I. Cell Bioi. 27:263-272. 1965.
Berglund B., Berglund U.. Ekman G.. et al. Individual psycho-physical functions for 28 odorants. Percept. Psychophys. 9:379-384. 1971.
Bradley R.M. Electrophysiological investigations of intravasculartaste using perfused rat tongue. Am. 1. Physiol. 224:300-304,1973.
Brightman V.l. Disordered oral sensation and appetite. In KareM.R.. MaIler 0., eds. The Chemical Senses and Nutrition. NewYork. Academic Press, pp. 363-380. 1977.
Brodal A. Neurological Anatomy in Relation to Clinical Medicine. NewYork. Oxford University Press, 1981.
Chitanondh H. Stereotaxic amygdalotomy in the treatment ofolfactory seizures and psychiatric disorders with olfactory hal-lucination. Con/in. Neurol. 27:181-196, 1966.
Conger A.D. Loss and recovery of taste acuity in patients irradi-ated to the oral cavity. Radiat. Res. 53:338-347. 1973.
Corn sweet T.N. The staircase method in psychophysics. Am. 1.Psychol. 75:485-491, 1962.
Cowart B.J. Development of taste perception in humans: sensitiv-

402 CRANIAL NERVES AND THEIR DISORDERS
Ghorbanian S.N., Paradise J.L., Doty R.L. Odor perception inchildren in relation to nasal obstruction. Pediatrics 72:510-516.1983.
Gloor P., Olivier A.. Quesney L.F., et al. The role of the limbicsystem in experiential phenomena of temporal lobe epilepsy.Ann. Nellrol. 12:129-144, 1982.
Gowers W .R. The Hughlings-Jackson lecture on special sensedischarges from organic disease. Brain 32:303-326, 1m.
Graziadei P.P.C. The ultrastructure of vertebrate olfactory mucosa.In Friedmann I.. ed. The Ultrastructure of Sensory Organs. Oxford,Elsevier, pp. 267-305, 1973.
Haberly L.B.. Price J.L. The axonal projection patterns of themitral and tufted cells of the olfactory bulb in the rat. Brain Res.129:152-157, 1977.
Hausser-Hauw C., Bancaud J. Gustatory hallucinations in epilepticseizures. Electrophysiological, clinical and anatomical correlates.Brain 110:339-359. 1987.
.Hinds J.W.. Hinds P.L., McNelly N.A. An autoradiographicstudy of the mouse olfactory epithelium: evidence for long-Iivedreceptors. Anat. Rtr. 210:375-383, 1984.
Holmes G. Local epilepsy. Lancet 1:957-962, 1927.Howe J.C., Gibson J.D. Uncinate seizures and tumors, a myth
reexamined. Ann. Neurol. 12:227, 1982.Hyman B.T.. Van Hoesen G.W., Damasio A.R., et al. Alzheimer's
disease: cell-specific patholog)' isolates the hippocampal forma-tion. Science 225:1168-1170, 1984.
Jackson J.H. (1869) A study of convulsions. In Taylor J., ed.Selected Writings of John Hughlings Jackson. London. Hodder andStoughton, pp. 8-36, 1931.
Jackson J.H. (1880) On right or left-sides spasm at the onset ofepileptic paroxysms, and on crude sensation warnings, andelaborate mental states. In Ta)'ior J., ed. Selected Writings of JohnHughlings lackson. London. Hodder and Stoughton, pp. 308-317, 1936.
Jones D. T.. Reed R.R. GOlf: an olfactory neuron specific-G proteininvolved in odorant signal transduction. Science 244:m-795,1989.
Kaufman M.D.. Lassiter R.R.L., Shenoy B. V. Paroxysmal unilat-eral dysosmia: a cured patient. Ann. Neurol. 24:450-451, 1988.
Krettek J.E.. Price J.L. Projections from the amygdaloid complexand adjacent olfactory structures to the entorhinal cortex and tothe subiculum in the rat and cat. J. Comp. Neurol. 172:723-752,1977a.
Krettek J.E.. Price J.L. The cortical projections of the mediodorsalnucleus and adjacent thalamic nuclei in the rat. J. Comp. Neurol.171:157-191. 1977b.
Krettek J.E., Price J.L. Amygdaloid projections to subcorticalstructures within the basal forebrain and brainstem in the ratand cat. I. Comp. Neurol. 178:225-254, 1978.
Kurihara K. Taste modifiers. In Beidler L.M.. ed. Hand!XJOk ofSensory Physiology. Vol. IV. Chemical Senses. Part 2. Taste. NewYork. Springer-Verlag. pp. 362-378, 1971.
.Lancet D. Vertebrate olfactory reception. Annu. Rev. Neurosci.9:329-355, 1986.
Leopold D.A. The relationship between nasal anatomy and humanolfaction. Laryngoscope 98:1232-1238, 1988.
Leopold D.A.. -Youngentaub S.L., Schwob J.E., et at. Successfultreatment of phantosmia with preservation of olfaction (abstract185). Twelfth Annual Meeting of the Association for Chemo-reception Sciences. Sarasota, FL, April 18-22. 1990.
Lorig T.S. Human EEG and odor response. Prog. Neurobiol. 33:387-398, 1989.
Lovell M.A.. Jafek B.W.. Moran D.T.. et al. Biopsy of humanolfactory mucosa: an instrument and a technique. Arch. Otolar-yngol. 108:247-249, 1982.
.MacLeod P. Structure and function of higher olfactory centers.I~ Beidler L.. ed. Hand~k of Sensory Physiology. Vol. IV. Olfac-t.'n. New York. Springer-Verlag. pp. 182-204, 1971.
.Mair R.B.. Gesteland R.C. Process in olfactory reception. InBreuer M.M.. ed. Cosmetic Science. New York, Academic Press,pp. 83-123, 1980.
Mair R.B.. McEntee W.J., Doty R.L. Olfactory perception inKorsakoff's psychosis: correlation with brain noradrenergic ac-livity. Nellrology 33(Suppl. 2):64-65. 1983.
Maruniak J.A., Silver W.L. Mowton D.G. Olfactory receptorsrespond to bloodbome odorants. Brain Res. 265:312-316, 1983.
Menevse A., Dodd G., Poydner T.M. Evidence for the specificinvolvement of cyclic AMP in the olfactory transduction mech-anism. Biochtm. Biophys. Res. Commun. 77:671-677, 1977.
Moberg P.l.. Pearlson G.D.. Speedie L.J., et al. Olfactory recog-nition: differential impairments in early and late Huntington'sand Alzheimer's disease. I. Clin. Exp. Neuropsychol. 9:650-664.1987.
Moran D.T., Rowley l.C., lafek, B.W. Electron microscopy ofhuman olfactory epithelium reveals a new cell type: the micro-villar cell. Brain Res. 253:39-46, 1982a.
"Moran D.T., Rowley J.C., lafek B.W., et al. The fine structure ofthe olfactory mucosa in man. I. Neurocytol. 11:721-746, 1982b.
Murray R.G. The ultrastructure of taste buds. In Friedman I., ed.The Ultrastructure of Sensory Organs. New York, Elsevier NorthHolland Biomedical Press, pp. 1-81, 1973.
Nakashima T., Kimmelman C.P., Snow J.B. Jr. Effect of olfactorynerve section and hemorrhage on the olfactory neuroepithelium.Surg. Form 35:562-564, 1984a.
Nakashima T., Kimmelman C.P., Snow J.B. Jr. Structure of humanfetal and adult olfactory neuroepithelium. Arch. Otolaryngol.110:641-646, 1984b.
.Norgren R. Central neural mechanisms of taste. In Darien-SmithI., ed. Hand~ of Physiology. Secion 1. The Nem>us Systtm. Vol.3. Sensory Processes. Bethesda, American Physiological Society,1984.
Osterhammel P., Terkildsen K., Zilstorff K. Electro-olfactogramsin man. I. uryngol. Otol. 83:731-733, 1969.
Pace U., Hanski E., Salmon Y. et al. Odorant-sensitive adenyIatecyclase may mediate olfactory reception. Nature 316:255-258,1985.
Peabody C.A., Tinklenberg l.R., Olfactory deficits and primarydegenerative dementia. Am. I. Psychiatry 142:524-;-525, 1985.
Penfield W .G. , Kristiansen K. Epileptic seizure patterns. Spring-field, IL, Thomas, 1951.
Penfield W ., Faulk M.E. The insula: further observations on itsfunction. Brain 78:445-470, 1955.
Plattig K.-H.. Kobal G. Spatial and temporal distribution of olfac-tory evoked potentials and techniques involved in their meas-urement. In Lehmann D., Callaway E., eds. Human EvokEdPotentials. New York, Plenum Publishing, 1979.
Powell T.P.S., Cowan W.M., Raisman G. The central olfactoryconnexions. I. Anat. 99:791-813, 1965.
Report of tht Panel on CommunicatiVt Disorders to the National AdvisoryNeurological and CommunicatiVt Disorders and Stroke Council. June1, 1979. Washington, DC, U.S. Public Health Service, NIHPublication No.81-1914, 1979.
Reyes P.F., Golden G.T., FageI P.L., et al. The prepiriform cortexin dementia of the Alzheimer type. Arch. Neurol. 44:644-645,1987.
Rhein L.D., Cagan R.H. Role of cilia in olfactory recognition. InCagan R.H., Kare M.R., eds. Biochtmistry of Taste and Olfaction.New York, Academic Press, pp. 47-68, 1981.
Rowley J.C. Ill, Moran D.T., Jafek B.W. Peroxidase backfillssuggest the mammalian epithelium contains a second morpho-logically.distinct class of bipolar sensory neuron: the microvillarcen. Brain Res. 502:387-400, 1989.
-Schiffman 5.5. Taste and smell in disease. N. Engl. I. Med.~:127S-1279. 1337-1343, 1983.
-Schwartz B., Doty R.L., Frye R.E., et al. Olfactory function inchemical workers exposed to acrylate and methacrylate vapors.Am. I. Public Health 79:613-618, 1989.
Settle R.G., Quinn M.R., Brand J.G., et aI. Gustatory evaluationof cancer patients; preliminary results. In van Eys J., NicholsB.L., Seeling M.S., eds. Nutrition and Cancer. New York, Spec-trum Publications, 1979.
-Shepherd G.M. Synaptic organization of the mammalian olfactorybulb. Physiol. Rev. 52:864-917, 1972.
Shepherd G.M. NeurOOiology. New York, Oxford University Press,1983.
Sicard G., Honey A. Receptor cell responses to odorants: similarityand differences among odorants. Brain Res. 292:283-2%, 1984.
Silver W .L., Moulton D.G. Chemosensitivity of rat nasal trigeminalreceptors. Physiol. Beha!'. 28:927-931, 1982.
Smith D.B.. Allison T., Golf W.R., et al. Human odorant evokedrespc!nses: effect of trigeminal or olfactory deficit. Electroen-cephalogr. Clin. Neurophysiol. 30:313-317, 1971.

403SMELL AND TASTE AND THEIR DISORDERS
Smith D.V., van Buskirk R.L., Travers l.B., et al. Coding of tastestimuli by hamster brain stem neurons. ,. ,"europhysiol. 50.541-
558, 1983.-Sumner D. Disturbance of the senses of smell and taste after
head injuries. In Vinken P.l., Bruyn G.W., eds. Handbook ofClinical Neurology. Injuries of the Brain and Sku/1. Part II. NewYork, American Elsevier, pp 1-25, 1976.
Walz W., Hertz L. Functional interactions between neurons andastrocytes. II. Potassium homeostasis at the cellular level. Prog.Neurobiol. 20:133-183, 1983.
Ward C.D., Hess W.A., Calne D.B. Olfactory impairment inParkinson's disease. Neurology (N. Y.J 33:943-946, 1983.
Weiffenbach l.M. Taste and smeU perception in aging. Gerontology3.137-146, 1984.
Weiffenbach l.M., Baum B.l., Burghauser R. Taste thresholds:quality specific variations with human aging. /. Gerontol. 32:372-
377, 1982.Weiser H.G., Hailemariam s., Regard M., et al. Unilateral limbic
epileptic status activity: stereo EEG, behavioral and cognitivedata. Epilepsia 26:19-29, 1985.
Yamagishi M., Nakamura H., Takahashi s., et al. Olfactory recep-tor cells: immunocytochemistry for ne~.ous system-specificproteins and re-evaluation of their precursor cells. Arch. Histol.Cytol. 52(suppl.):375-381, 1989.