Embed Size (px)
Citation preview

JOURNAL OF PATHOLOGY, VOL. 145: 1-25 ( 1 985)
SMALL CELL TUMOURS IN CHILDHOOD: A REVIEW
S. VARIEND
Department of Histoputhology , Children’s Hospital, Shefield, U.K.
Received 20 July 1984 Accepted 24 July 1984
SUMMARY The past decade has seen significant advances in the treatment of childhood malignancies accompanied by appreci-
able improvement in survival rates. Treatment programmes have been largely formulated to meet the specific characteristics of individual tumours, as well as being based on the extent ofdisease presented at diagnosis. In selecting the most appropriate treatment protocol, accurate histological categorization of resected or biopsied tumour is thus of paramount importance. In the pacdiatric age range in which so many tumours lack differentiation as to present as, or mimic, other small cell tumours, routine methods are often insufficient to resolve problematic histology. A wide range of special techniques is now at hand to assist the pathologist with this problem and this review is an attempt partly to rationalize the application of available methodology. Of considerable importance also is a knowledge of the behavioural characteristics of this group of tumours, their prototypic histology, as well as the range of morpho- logical variability. KEY WORDS- Childhood tumours, neuroblastoma, Ewing’s sarcoma, rhabdomyosarcoma.
INTRODUCTION
The recent substantial improvement in survival among children with malignant disease may be attributed largely to the introduction of multi- modality treatment and aggressive clinical staging of Histological diagnosis and extent of disease determine the choice of therapy protocol which, in turn, has increased the requirement for accurate pathological reporting. Consequently, imprecise diagnoses such as ‘small cell tumour’, otherwise unspecified, are unhelpful and should be strongly discouraged.
The new challenge for the histopathologist who is involved with childhood neoplasms is related par- ticularly to neuroblastoma and rhabdomyo- sarcoma ; they commonly are poorly differentiated and may be easily confused histologically with other small cell neoplasms, notably Ewing’s sarcoma and non-Hodgkin’s lymphoma. To facilitate their dis- tinction, there now exists a large battery of special diagnostic procedures that should be applied to their full advantage.
So that therapy may be instituted with the minimum of delay, speedy histological reporting is commendable, but the current practice of submit- ting smaller samples of tissue for histological assess-
c’ 1985 by John Wilcy & Sons, Ltd. 0022-341 7/85/0 1000 l-25$02.50
ment, especially since the advent of needle aspiration as a biopsy t e~hn ique ,~ has not particu- larly eased the situation. Over the past few years, however, the histopathologist has considerably widened his diagnostic armamentarium beyond that which rests on the assessment of simple two- dimensional morphology. Apart from the appreci- able progress that has already been achieved with non-Hodgkin’s lymphoma, mainly through the harnessing of the well-known biological function of the lymphoid system, the list of tumour markers relating to other small cell tumours has also expanded rapidly. Such sophisticated methods should not, however, substitute for, but should serve rather to reinforce, conventional light microscopy. A sound basic understanding of the biological behaviour and nature of these neoplasm is, of course, also important as this undoubtedly contributes significantly towards their accurate evaluation.
NEUROBLASTOMA
Neuroblastoma is the third commonest solid malignant tumour of infancy and childhood, being superseded only by lymphoid neoplasms and

2 S. VARIEND
cerebral tumours4~ Ninety per cent of tumours occur in patients less than 10 years of age,6although birth to 5 years represents the usual age range. There is a slight male preponderance. The tumour arises from neuroblasts, the undifferentiated pre- cursor cells of the sympathetic nervous system. The adrenal is the seat of primary growth in about a quarter of cases ;6 elsewhere, the neoplasm occurs mainly along the sympathetic chain. Consistent with this derivation from the sympathetic nervous system, neuroblastoma and its variants occur typi- cally in a variety of paraspinal locations including the retroperitoneum, posterior mediastinum7 and cervical area,8 in order of decreasing frequency. Paralysis from tumours insinuating through inter- vertebral foramina causing spinal cord compression may O C C U ~ . ~ It is possible, however, that such dumb- bell neoplasms originate directly from the posterior root ganglia which are also of neural crest origin.’O Primary tumours occur exceptionally in the kid- ney’l and arise apparently from neural crest cells that have undergone aberrant migration.12 A stag- ing system currently widely employed is that of Evans et d . 1 3 (Table I).
Of the common childhood tumours, neuro- blastoma shows the most unpredictable clinical behaviour with a tendency to spontaneous ‘matura- tion’ or regression. l4 Patients with adrenal neuroblastoma generally have a poor outcome, related possibly to the high incidence of poorly dif- ferentiated growth at that site.1°
There is some evidence that patients with dif- ferentiating tumours fare better than those with undifferentiated neuroblastoma10 although general agreement concerning this association is still lack- ing.15 The greater proportion of favourably staged cases at a younger age is thought to account for the more favourable outcome among those under one year.16 The generally better prognosis among girls may be related to a greater capacity in that gender for the tumour to mature.6
Whilst bone marrow, liver and lymph nodal metastases are common, isolated pulmonary secondaries do occur but they are usually part of more widespread dissemination that constitutes a grave prognostic sign.I7 The outlook for ‘metastatic’ growth in the first year is not necessarily gloomy as many of these cases frequently undergo spontaneous resolution of their disease, an outcome which is particularly associated with Stage IV-S cases.12 Compared with conventional Stage VI, patients with Stage IV-S disease have an excellent prognosis even without treatment although it may
Table I-Neuroblastoma staging
I Tumour confined to structure of origin I1 Tumour extends beyond structure of origin but in
continuity and not crossing the midline. (Regional lymph nodes on the same side may be involved)
111 Tumour extends in continuity beyond midline. (Lymph nodes may be involved on both sides)
IV Distant disease I or I1 and distant disease, e.g. liver, skin or bone marrow (but without x-ray evidence of bone involvement)
IV-S
take some time for hepatic enlargement and skin nodules to regress. The occurrence of Stage IV-S disease in the neonate, however, seems to be an exception to this excellent prospect for survival.18
Clusters of neuroblasts may persist in the adrenal medulla after birth and be found incidentally at autopsy, usually in infants less than three months of age.19,20 These lesions are referred to as neuro- blastoma-in-situ, the incidence of which has been calculated to be about 40 times greater than clini- cally overt neuroblastoma, suggesting that many such lesions involute with time. According to Knudson’s two-hit theory of oncogenesis,2’ neuroblastoma-in-situ may be considered an expression of the first hit with a second hit manifest- ing as overt neuroblastoma. Stage IV-S disease, with its high incidence of spontaneous regression, has been considered in a similar contextZ2 and the possibility that it represents a multifocal lesion related to abnormally placed neural crest cells has been considered. lo
Histologically, the tumour seems committed to a programme of continuous differentiation with progressive neurogenesis giving rise to a histological spectrum that includes neuroblastoma, ganglio- neuroblastoma and ganglioneuroma. Undifferenti- ated neuroblastoma presents a structureless array of small, round to ovoid cells (Fig. I ) , frequently divided into lobules by delicate, vascular connective tissue septiae. Nuclei are hyperchromatic but mitoses are not particularly common. Pseudo- rosettes and patches of pink fibrillary material are useful histological markers of early differentiation (Figs 2a, b) while early neuronal development is characterized by increasing nuclear vesiculation, prominent nucleoli and more voluminous cyto- plasm (Fig. 2b). Necrosis and focal calcification are common.
The boundary between neuroblastoma and gang- lioneuroblastoma is ill-defined’ with no general agreement on the degree of neural differentiation

SMALL CELL TUMOURS IN CHILDHOOD 3
Fig. I - Sheets of small cells with scant cytoplasm and hyperchromatic nuclei with no tendency towards organoid differentiation are the usual features of poorly differentiated neuroblastoma. H & E, x 314
that separates these two groups. A composite pat- tern, characterized by one or more discrete nodules of pure neuroblastoma occurring in a ganglioneuro- blastoma, and a diffuse pattern which shows a mix- ture of primitive and differentiating neuroblasts, further categorize ganglioneuroblast~rna.~~~~ The importance of this distinction lies in the better outlook for patients with the diffuse pattern.
Ganglioneuromas are benign, often encap- sulated, generally circumscribed tumours that may attain an enormous size.7 They have an anatomical distribution similar to that of neuroblastomas. Foci of cystic degeneration, haemorrhage and calcifica- tion are seen occasionally. Microscopically, rela- tively mature ganglion cells occur singly or in groups set in an abundant neurocollagenous matrix (Fig. 3). Satellite cells may or may not be present. Ganglion cells may retain a degree of multi- nuclearity but mitoses are always absent. Multiple sections should be examined in order to exclude residual neuroblasts which, however, should not be mistaken for lymphocytic foci that are fairly common.
Biochemical aspects Many of these tumours are biologically active
and capable of elaborating a variety of
catecholamine precursors and their metabolite^.^^ Vanilylmandelic acid (VMA), homovanillic acid (HVA), or both, are secreted in 80 per cent of patients with neuroblastoma.16 Noradrenaline and adrenalin, as such, are rarely secreted and urinary VMA and HVA are usually measured as biochemi- cal markers to aid diagnosis and monitor therapy. Hypertension may occur, probably related to the secretion of these compoundszs although, with retroperitoneal tumours, renal pedicle compression as a mechanism should also be c o n ~ i d e r e d . ’ ~ ~ ~ ~ The ratio of VMAIHVA is also regarded a useful prog- nostic index, higher values being associated with a more favourable outcome.z6 Some tumours, par- ticularly those with advanced differentiation, pro- duce and secrete VIP with intractable diarrhoea as the main clinical presentation.z7
Ancillary diagnostic methods
Touch-imprints of tumour stained with haematoxylin and eosin show characteristic small groups of tumour cells with tapering cytoplasmic extensions directed radially or linking individual cells, and may be present even when differentiation is lacking in routine preparations (Fig. 4). Glyoxylic acid-induced fluorescence of tumour cells has been reported to occur in over 80 per cent of cases.z8

4 S. VARIEND
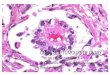
Fig. 2-(a) Neuroblastoma with well developed rosettes containing central neurofbrillary cores. H & E, x 502. (b) On the right side of the field there is poorly nucleated neurofibrillary material; the left shows a mixturc of neuroblasts and larger cells with features of early neurogenesis. H & E, x 314

SMALL CELL TUMOURS IN CHlLDHOOD 5
Fig. 3-GanghOneUrOmd showing clusters of ganglion cells set in a stroma of neurocollagenous tissue. H & E, x 125
Other diagnostic aids include the utilization of monoclonal antibodiesz9 and immunochemical markers such as neurone-specific enolase30 which is not specific, however, as a similar reaction may occur in other tumours such as melanoma.
The unique property of tumour cells to form neurite processes and cell clumping in tissue cul- ture has been exploited as a diagnostic
method.28 Neuroblastoma has recognized status among the neuroendocrine tumours3 and, apart from its ability to produce catecholamine, is also known to elaborate acetylch~linesterase.~~ The presence of this enzyme has been demonstrated by histochemistry in human neurob la~ toma~~ (Fig. 5 ) . Such reactivity for acetylcholinesterase does not appear to occur in Ewing’s sarcoma or lympho-
Fig. 4 Touch-imprint of poorly differentiated neuroblastoma Fig. 5-Poorly differentiated neuroblastoma with strong showing frequent cytoplasmic extensions, sometimes bridging cytoplasmic positivity for acetykholinesterase. Acetyl- individual tumour cells. H & E, x 1056 cholinesterdse, x 264

6 S. VARIEND
blastic lymphoma although, with rhabdomyo- sarcoma, focal positivity may be demonstrated. Glycogen, as demonstrated by diastase-sensitive PAS-positivity, is present in a large proportion of n e u r o b l a s t ~ m a s ~ " ~ ~ but the en bloc positivity encountered in rhabdomyosarcoma and Ewing's sarcoma has not been reported.26
Ultrastructure
Catecholamine granules measuring 50-200 nm in diameter are usually regarded as fundamental to ultrastructural d i a g n ~ s i s . ' ~ ~ ~ ~ - ~ ~ The granules, which should be distinguished from lysosomes, are present in the cell body but are generally more frequent in the cytoplasmic extensions3' (Fig. 6). A correlation between the level of urinary catecholamine products and the frequency of occur- rence of catecholamine granules has been reported.3s Increasing tumour differentiation also appears to be associated with greater numbers of catecholamine granules.38 A compact meshwork of interdigitating neurites containing longitudinally orientated neurofilaments and neurotubules (approximately 20 nm in diameter (Fig. 7)) is com- mon and useful in d i a g n o s i ~ , ~ ~ ~ ~ ~ and their number and length increase proportionately with degree of
tumour differentiation, being particularly pro- nounced in gang l ione~roma .~~ Clear vesicles, about half the size of catecholamine granules, probably representing acetylcholine activity, may be p r e ~ e n t . ~ ~ , ~ ~ Cell-cell attachments and glycogen may be seen.ls Mitochondria, granular and smooth endoplasmic reticulum, free ribosomes and Golgi complexes are other features whose numbers appear to increase in accordance with the degree of neurogenic differentiation.
Related neoplasms
Neuroblastoma containing neuromelanin has been reported.40 A special variant of neuro- blastoma derived from the olfactory apparatus, so- called olfactory neuroblastoma (esthesioneuro- blastoma), resembles conventional neuroblastoma both histologically and ultrastructurally.41~4z Although the majority of these tumours has been reported in adults, a modest number occur in children.
Neuroblastoma also occurs as a component of progonomas (melanotic neuroectodermal tumour of infancy)43 where it forms part of a biphasic pat- tern in conjunction with melanin-containing cuboidal cells. Generally, patients are under 1 year
Fig. 6-Two transversely sectioned neurites reveal dense, cored, neurosecretory granules (arrow). Uranyl acetate & lead citrate, x 68 400

SMALL CELL TUMOURS IN CHILDHOOD 7
Fig. 7-Neuroblastoma showing intertwining, closely apposed dendrite processes. Uranyl acetate & lead citrate, x 6840
of age and, although the great majority of cases affect the maxilla, they have been described occas- ionally in the mediastinum, epididymis and long bones. Rarely, the neuroblastomatous component may predominate and mask the underlying pattern.
N e ~ r o e p i t h e l i o m a ~ ~ ~ is a rare malignant tumour with microscopic and ultrastructural fea- tures resembling neuroblastoma. These include the presence of pseudo-rosettes (Fig. S), and an ability in some to elaborate catecholamine metabolite^.^^ It is probable that such tumours represent neuro- blastoma arising in peripheral nerves. Neuro- epitheliomas are more commonly reported in adults but their relation to the small cell tumours of the chest wall in children and adolescents, as described by Barson et d 4 I and Askin et U I . ~ ~ remains ill- defined. So-called Askin tumours have been shown recently to immunoreact for neurone-specific e n ~ l a s e , ~ ~ as have similar tumours affecting
RHABDOMYOSARCOMA
one year of age observed in other small cell tumours is a feature not shared by rhabdomyosarcoma. 5 1 9 5 2
The extent of disease and degree of resectability determine the stage of diseases3 (Table 11).
Microscopic diagnosis depends on pattern recog- nition and evidence of skeletal muscle differenti- ation, notably the presence of rhabdomyoblasts and the demonstration of cytoplasmic cross-striations.
Rhabdomyosarcoma is the commonest soft tis-
group is generally associated with better Survival, the particularly excellent outcome of children under
sue Sarcoma in the younger age Fig. 8-Neuroepithelioma from the chest wall of a 12 year-old boy showing pseudo-rosettes reminiscent of neuroblastoma. H & E, x 256

8 S. VARIEND
Table I 1 - Rhabdomyosarcoma staninn
I Disease localized- completely resected I 1 Regional disease, resected I11 Localized disease not completely resected IV Metastatic disease presenting at diagnosis
Cross-striations, now generally regarded as not essential for diagnosis, are recognized to occur in less than 50 per cent of turn our^.^^^^^ Rhab- domyoblasts exhibit abundant pink-staining, slightly granular cytoplasm that may assume a variety of shapes; strap, tadpole, oval, spindle and racquet; the cytoplasm stains deep red with Mas- son’s trichrome and deep blue with PTAH.55 Cross- striations, when present, are found within the cytoplasm of the rhabdomyoblast. The histological categories of rhabdomyosarcoma include the embryonal, alveolar and pleomorphic patterns.56
Embryonal tumours predominate in the head, neck and genitourinary tract, including the epi- didymis; other well recognized, but less common sites are the thorax, biliary tree, retroperitoneum and perineum. Males are affected more commonly and the average age of presentation is 3 4 years. Congenital tumours have been described. 5 7 , 5 8
Embryonal rhabdomyosarcoma tends to arise
where striated muscle does not normally occur and origin from uncommitted multipotent primitive mesenchyme seems probable.59
Neoplasms of the head and neck are generally associated with poor survival compared with those arising in the genito-urinary tract. This less favour- able outlook for the head tumours, in particular those arising in the nasopharynx, paranasal sinuses and middle ear, has been ascribed to their parameningeal location and, consequently, early infiltration of the central nervous system.60
The embryonal sub-group may be further cate- gorized into those showing predominantly a myx- oid pattern, spindle-cell pattern or a round-cell pattern.61 The myxoid pattern is comprised of stel- late and spindle cells arranged in a loose syncytium and set in a mucoid matrix (Fig. 9); nuclei are hyperchromatic and mitoses are generally frequent.
Although essentially an embryonal tumour, the botryoid rhabdomyosarcoma, which grows as a grape-like cluster beneath the mucous membrane of hollow viscera (Fig. lo), has been regarded as a special group.62 This form of the tumour predom- inates in the genito-urinary tract where it involves the trigone of the bladder, the anterior vaginal wall in females and the prostate in males, but may also arise in the middle ear, maxillary sinus,
Fig. 9 - Myxoid type of embryonal rhabdomyosarcoma showing small, dark, stellate cells set in a loose mucoid background H & E , x314

SMALL CELL TUMOURS IN CHILDHOOD 9
Fig. 10- Botryoid-embryonal rhabdornyosarcoma from the middle ear of a 4 year-old boy showing typical, grape-like, polypoid appearance. x 2.8
nasopharynx and soft palate.56 It is the usual type seen in association with the biliary tract.50 Histolo- gically, it is characterized by a dense zone of sub- epithelial neoplastic cells, the so-called cambium layer, which frequently reveals rhabdomyoblasts while the deeper portions are more vascular, myx-
oid and relatively acellular (Fig. 1 I).,, The round cell pattern (Fig. 122) may be easily
confused with a variety of other small cell tumours, although early rhabdomyoblasts are revealed frequently after diligent searching. The spindle-cell pattern of rhabdomyosarcoma (Fig. 13) resembles fibrosarcoma, fibrous histiocytoma or leiomyo- sarcoma while myxoid liposarcoma and chondro- sarcoma should be considered when the myxoid pattern prevails.63 On the other hand, many of these tumours are unusual in childhood and need not be considered ordinarily in the differential diagnosis of rhabdomyosarcoma in this age group.
Benign vaginal polyps with features similar to the botryoid pattern of rhabdomyosarcoma have been reported and, although the majority occur in older subjects, infants are not exempt.64 Fetal rhab- d o m y ~ m a ~ ~ v ~ ~ a benign tumour usually located in the subcutaneous soft tissue, has a similar age dis- tribution to that of embryonal rhabdomyosarcoma and presents a potential source of diagnostic con- fusion. The head and neck are usually affected with predilection for the posterior auricular area. A marked male predominance exists. These lesions are generally circumscribed and histologically feature a mixture of rhabdomyoblasts and primitive mesenchymal cells ; rhabdomyoblasts occur com-
Fig. 11 -Microscopic view of a botryoid tumour showing condensation of tumour cells beneath attenuated epithelium (cambium layer). The deeper part is less cellular and more myxoid in appearance. H & E, x 216

10 S . VARIEND
Fig. 12-A round cell variant of embwonal rhabdomyosarcoma. Biopsy of orbital tumour from a 10 month-old female. H & E, x415
monly at the tumour periphery. Compared with rhabdomyosarcoma, the cell population is more uniform, hyperchromatic cells are lacking and mitoses are rare or absent.
Alveolar rhabdomyosarcoma is usually recog- nized by a pattern of irregular spaces or ‘alveoli’ separated by vascular fibrous septa of variable thickness.ss~58~66 The spaces are lined by a layer of tumour cells that impart an epithelial appearance and may show degrees of myoblastic differ- entiation. The spaces contain dehiscent or ‘floating’ cells that are frequently pyknotic and karyhorrectic (Figs 14a, b). Characteristic multinucleated tumour giant cells with a wreath of marginally placed nuclei are fairly (Fig. 15). Mitotic figures may be sparse. The alveolar pattern may be lacking, however, and coexist with extensive areas in which the cells are closely packed. The alveolar spaces develop probably as a degenerative feature and, consequently, are found more often in the centre of the tumour where vascularization is likely to be most precarious. Multiple sections may be necess- ary therefore to disclose this characteristic.
Compared with the embryonal sub-group, alveolar rhabdomyosarcoma is generally associated with a less favourable The incidence of alveolar rhabdomyosarcoma increases with age and
there is a predilection for the soft tissues of the e x t r e m i t i e ~ . ~ ~ This pattern of the tumour is not limited to skeletal muscle, however, and there is some overlap with the usual anatomical distribu- tion of embryonal tumours with periorbital, perianal and perineal soft tissues being other recognized primary sites. 54 Alveolar rhab- domyosarcoma tends to metastasize to lymph nodes, lungs, pleura, pancreas and boness and dif- fuse lymph nodal and bone marrow metastases with a leucoerythroblastic blood picture, which may stimulate a haemopoietic malignancy, is a recognized clinical presentation.68 In such cases, the primary tumour may not be discovered even after exhaustive searching. That embryonal and alveolar patterns may co-exist in the same tumour is well recognized ;51, 57 ,69 this pattern has been referred to as mixed rhabdomyosarcoma. s8
The embryonal and alveolar patterns resemble developing muscle during early gestation.69 The pleomorphic pattern, on the other hand, which pre- dominates in adults does not seem to recapitulate any recognizable stage of muscle development and probably represents dedifferentiation in mature stri- ated muscle.69 The pleomorphic pattern seems to be rare in childhood with a reported frequency of 0.7 per cent and 5 per cents7 However, many of the

SMALL CELL TUMOURS IN CHILDHOOD 1 1
Fig. 13-Spindle-cell variant of embryonal rhdbdomyosarcoma with focal rhabdomyoblastic differentiation. H & E, x 195
documented large series have not included its occur- r e n ~ e , ~ l , 5 8 and such disparity is possibly related to the application of different diagnostic criteria.
Soft tissue tumours lacking sufficient cellular dif- ferentiation to allow an unequivocal histological diagnosis of rhabdomyosarcoma have been vari- ably referred to as ‘sarcoma of undetermined histo- genesis’,58 ‘undifferentiated mesenchymal sarcoma’55 and ‘mesenchymal sarcoma, probably rhabdomyosarcoma’. 5 7 In practice, the clinical response of these neoplasms to the usual therapeutic regime advocated for proven rhab- domyosarcoma has been similar.70 However, there now exists a wide range of special techniques that may aid substantially in resolving the histology of tumours presenting diagnostic difficulty by routine methods.
Histochemistry and immunochemistry
Positive staining for glycogen is common in rhab- domyosarcoma and its successful demonstration is enhanced in frozen sections (Fig. 16), or by prior fixation in absolute alcohol. PTAH staining is use- ful and serves to emphasize cytoplasmic cross- striations frequently already apparent on conven- tional staining.
Myosin may be demonstrated histochemically in tumour cells using the myofibrillar (calcium- activated) adenosine triphosphatase technique (Fig. 17).71972 An advantage of this method is that it can be carried out rapidly and the reagents used are generally inexpensive. Both early and advanced rhabdomyoblasts are accentuated with the method carried out following acid pre-incubation. At this pH, the small undifferentiated cell of alveolar rhab- domyosarcomas also reacts with a degree of positivity that easily distinguishes the cell type from other small celled tumours likely to be encountered in the paediatric age range.59
Myophosphorylase, a glycolytic enzyme present normally in striated and smooth m ~ c l e , ~ ~ may also be demonstrated histochemically in rhabdomyo- ~ a r c o m a , ~ ’ . ~ ~ but a positive reaction is probably limited by the degree of cyto-differentiation. Rhab- domyoblasts also reveal focal acetylcholinesterase activity (Fig. IS), a feature that is probably related to the early development of acetylcholine neuro- transmitter activity.
Immunochemical diagnosis of rhabdomyo- sarcoma has utilized antisera directed against a variety of muscle proteins including myosin,74 a ~ t i n , ~ ~ d e ~ m i n ’ ~ and my~globin.~’ 8o However, only myoglobin appears to be specific for skeletal

12 S. VARIEND
(h)
Fig. 14--(a) Rhabdomyosarcoma showing a well defined ‘alveolar’ pattern. The spaces are separated by thick fibrous bands and lined by tumour cells; they contain degenerate, ‘free-floating’ cells. (b) The ‘alveolar’ pattern is less developed in this tumour. H & E. x 314

SMALL CELL TUMOURS IN CHILDHOOD 13
Fig. 15--Alveolar rhabdomyosarcoma containing several tumour giant cells with peripherally marginated nuclei. H & E, x 125
Fig. 16- Embryonal tumour metastic to lymph node showing strong, frequently clumped, PAS cytoplasmic positivity. PAS, x 314

14 S. VARIEND
Fig. 17-Small and large rhabdomyoblasts are heavily accentu- ated by the ATP-ase reaction in an embryonal tumour. ATP-ase with acid pre-incubation, x 205
muscle as the remainder occur in other tissues, most notably smooth muscle. Thus, the demonstration only of immunoreactive myoglobin indicates that the tumour is truly rhabdomyoblastic in nature (Fig. 19); yet studies on its diagnostic effectiveness have, so far, fallen far short of 100 per ~ent , ’~-~O regardless of histological type, although a positive reaction is more frequent with alveolar rhab- do rnyosa r~oma .~~ Failure of tumour cells to react positively may be due to lack of differentiation of the tumour, or result from sub-optimal fixation of tissue.
Caution in interpretation is necessary when undifferentiated tumour occurs in or near normal striated muscle as deeply entrapped non-neoplastic myofibres are likely to immunoreact for myoglobin and lead to erroneous diagnosis. Cells of non- rhabdomyosarcomatous tumours metastic to skeletal muscle as well as local reactive histiocytes may react positively for myoglobin, apparently due to the ‘uptake’ of myoglobin released from dam- aged skeletal muscle.s1 p-Enolase, a dimeric gly- colytic enzyme found normally in striated muscle, has also been shown recently to have a high degree of specificity as an immunomarker of rhabdomyosarcoma.82
Ultrastructure
The value of electron microscopy lies mainly in its potential to confirm the presence of rhab- domyoblastic differentiation.8s86 Rhab- domyoblasts are likely to be confused at the light microscopy level with the cells of malignant
Fig. 18 --Strong, patchy, acetylcholinesterase cytoplasmic reac- tivity in embryonal rhabdomyosarcoma. Acetylcholinesterase, x 264
melanoma or epithelioid sarcoma and, arguably, electron microscopy has greater applicability in an older age group where such tumours are much more common. The minimal ultrastructural criteria advocated for confirmation of rhabdomyoblasts are the presence of alternating thick (myosin) filaments and thin (actin) filaments arranged in b ~ n d l e s . ~ ~ . s ~ Intermittent formation of attentuated Z-band material, occurring as rectangular densities with their long axes perpendicular to the alignment of filaments is an additional helpful featureE7 (Fig. 20). Such appearances are an attempt at sarcomere organization, the fundamental contractile unit of normal skeletal muscle. The small primitive cell of rhabdomyosarcoma, on the other hands, shows
Fig. 19-Turnour cells of embryonal rhabdomyosarcoma show focal reaction for myoglobin. Imrnunoperoxidase, x 422

SMALL CELL TUMOURS IN CHILDHOOD 15
Fig. 20-Cytoplasm of tumour cell in an alveolar rhabdomyosarcoma showing bundles of alternating thick and thin filaments with occasional rectangular densities (arrow). Uranyl acetate and lead citrate. x 40 850
monoparticulate glycogen, pinocytotic vesicles, cell junctions and basement membrane which, essen- tially, are non-specific and, not unexpectedly, may accompany sarcomeric organization in the better differentiated tumour. Thus, when rhab- domyosarcoma is completely undifferentiated by light microscopy, the value of electron microscopy with respect to yield of confirmatory evidence, is arguable, a problem undoubtedly exacerbated by the inherent problem of sample limitation.
Compared with the embryonal tumours, tumour cell junctions in alveolar rhabdomyosarcoma are common while myofilament formation in such tumours is relatively less advanced.84 At certain sites, rhabdomyosarcomas may incorporate adja- cent normal muscle fibres and particular caution is necessary at the ultrastructural level to distinguish these from neoplastic cells. Such entrapped, non- neoplastic muscle fibres are, however, generally recognized by a degree of myofilamental organiza- tion comparable to that found in normal muscle.
NON-HODGKIN’S LYMPHOMA AND LEUKAEMIA
Non-Hodgkin’s lymphoma (NHL) and leukaemia account for a significant proportion of
malignant tumours among children under the age of fifteen In children, NHL differs from that occurring in adults insofar as they are predominantly extranodal, rarely nodular, often leukaemic, rapidly proliferative and they rarely secrete para protein^.^^,^^ Also, there is usually an association between the different histological types and anatomical site and the clinical response rate to therapy is e n c o ~ r a g i n g . ~ ~ The majority of child- hood NHL fall into four major histological cate- gories : lymphoblastic lymphoma, Burkitt’s lymphoma, undifferentiated lymphoma and large- cell (‘histiocytic’) type.88,89 In view of the predominance of extranodal disease, non- contiguous involvement and frequent progression to leukaemia, the Ann-Arbor staging system is diffi- cult to apply and other systems have been pro-
Spread to the central nervous system is common and represents a poor prognostic fea- t ~ r e . ~ ~ The great majority of childhood NHL is committed to T- or B-cell differentiation, contrast- ing with the usual phenotype of most childhood lymphoblastic l e ~ k a e m i a s . ~ ~
Lymphoblastic lymphoma accounts for approx- imately 3 5 4 0 per cent of childhood NHL, tends to predominate in the supra-diaphragmatic region and presents commonly as a mediastinal mass (Fig. 21)88,89 Males are affected more commonly

16 S. VARIEND
than females and the peak age incidence is about 1 I years. Morphologically, lymphoblastic lym- phoma and acute leukaemia (ALL) are indis- tinguishableg3 and, though certain differences exist in their clinical behaviour, i t is increasingly evident that they express stages of the same neoplastic process.94
Histologically, lymphoblastic lymphoma is characterized by a diffuse, monomorphous, small cell pattern with round to ovoid nuclei, and a rim of barely discernible cytoplasm (Fig. 22).95 Chromatin is finely dispersed and two to several nucleoli are present. Nuclear convolutions may be numerous, sparse or absentg6s9’ and the mitotic count is usually high. The presence of macrophages containing ingested cellular debris frequently imparts a ‘starry sky’ pattern, although this feature is not usually as pronounced as in Burkitt’s lym- phoma or undifferentiated lymphoma. Diastase- digestible PAS-positive staining for cytoplasmic glycogen is sometimes present but the clumped positivity seen in Ewing’s sarcoma and rhab- domyosarcoma has, so far, not be described.26 Methyl green pyronine staining is minimal and Fig. 21-Chest radiograph showing a mediastinal mass in a 12
year-old boy with lymphoblastic lymphoma (courtesy of Dr R. K . Levick) chloroacetate esterase.
turnour cells are negative for
Over a wide age range the majority of lym-
Fig. 22-Lymphoblastic lymphoma showing monomorphic appearance of tumour cells and vigorous mitotic activity. Several macrophages are also present and impart a ‘starry sky’ effect. H & E, x 523

SMALL CELL TUMOURS IN CHILDHOOD 17
phoblastic lymphoma are of T-cell origin98 and are also positive for terminal deoxynucleotidyl transferase (TdT).97 A modest number belong to the non-B, non-T group or are of B-cell lineage.93 Punctate paranuclear positivity with the acid phos- phatase reaction is a useful histochemical marker (Fig. 23).
Sporadic non-African Burkitt’s lymphoma (small, non-cleaved cell malignant lymphoma) is morphologically indistinguishable from endemic African Burkitt’s lymphoma99 and has a notable predilection for the abdominal viscera.96 The tumour is composed of cells that are of uniform size with a thin rim of basophilic cytoplasm and round- to-ovoid nuclei containing coarse chromatin.94 Nuclear convolutions are absent and 2-5 eosinophilic nucleoli are fairly conspicuous. Mitotic activity is pronounced and a ‘starry sky’ pattern, due to the presence of macrophages frequently con- taining ingested cell debris, is usually appreciable. Fine cytoplasmic vacuoles which stain positively for neutral fat can be discerned with high magnification in thin sections or imprint preparations. Cytoplasm is strongly pyroninophilic. PAS staining is con- sistently negative and there is no naphthol-ASD chloroacetate esterase activity. Burkitt’s lymphoma has surface immunoglobulin and other character- istics of a B-cell neoplasm. loo
Undifferentiated lymphoma, also a B-cell tumour, occurs predominantly in adultsIo’ but a limited number of cases have been reported in chil- dren.Io2 The anatomical distribution is similar to that of Burkitt’s lymphoma. The cells are larger and more pleomorphic, nucleoli are fewer but more dis- tinct. Nuclear chromatin is coarse. The histochemi- cal features, however, are similar to those of Burkitt’s lymphoma and cytoplasmic vacuoles may be also demonstrated. lo’ The value of distinguish- ing undifferentiated lymphoma from Burkitt’s lym- phoma lies in the poorer prognosis of the former.’02
Large cell lymphoma (LCL), an immunologically heterogeneous group, is now recognized to arise mainly from transformed lymphocyte^.'^^ A num- ber of reports have documented their occurrence in children.93- lo2> Io4 Compared with the preceding groups, the anatomical distribution of LCL is much more random. Presentation as a mediastinal mass is rare while central nervous system, hepatic and bone marrow involvement is unusual at the time of diagnosis.88 More than 50 per cent of such tumours are derived from B-cells and 5-10 per cent have T- cell markers ; a small proportion are truly histiocytic or have no detectable markers.Io3 Histologically,
Fig. 23-Dot-like paranuclear positivity with acid phosphatase reaction in lymphoblastic lymphoma. H & E, x 1056
true histiocytic tumours are recognized by cells with large irregular vesicular nuclei, prominent nucleoli and abundant, weakly eosinophilic cytoplasm. Their histiocytic derivation may be confirmed by positive staining for lysozyme, a-antichymotrypsin, non-specific esterase or acid phosphatase.Io5
Granulocytic sarcoma (chloroma) This uncommon tumour, composed of granulo-
cyte precursors,lo6, lo’ is associated with and frequently precedes the onset of leukaemia, usually of the acute myeloid type. Bone, orbit, soft tissue, lymph node and skin are common sites and there is a predilection for the tumour to occur in child- hood. Well-differentiated tumours contain eosinophil precursors that are an important clue to diagnosis, and when poorly differentiated, the tumour is most commonly misdiagnosed as lym- phoma. Naphthol-ASD chloroacetate esterase and antilysozyme immunoperoxidase staining are posi- tive in the majority of cases and are an important aid to diagnosis.
EWING’S SARCOMA
In 1921 James Ewinglo8 described a primary malignant tumour of bone in which he emphasized the perivascular arrangement of the tumour cells and suggested a derivation from vascular endo- thelium. Any age or bone may be affected but the neoplasm predominates in the second decade of life and the pelvis and femur are the most common sites.

18 S. VARIEND
In one large study, 2 per cent of tumours occurred in babies and toddlers.'09 Pain and swelling are common symptoms and there is a modest male preponderance. Compared with distal lesions, tumours arising in the pelvis and proximal extremi- ties tend to be associated with a lower survival
The histogenesis is still a matter of controversy and, apart From the suggested endothelial cell origin, Ewing's sarcoma has been also considered to be derived from the primitive mesenchymes4 or myelogenous tissue.112 The rare co-existence of Ewing's sarcoma and myeloid leukaemia has been used as argument against the latter thesis,lI3 while the occasional location of histologically similar tumour in soft tissue114 may be viewed as support- ing a derivation from mesenchyme.
Ewing's sarcoma has a strong propensity to penetrate cortical bone and develop an extra- osseous mass, often far removed from the epicentre of the tumour, which is commonly the metaphysi~."~ Resected tumour is white and soft, presumably due to lack of appreciable stroma, or may be yellow and friable with advanced degenera- tion. Metastases to lung, bone and regional lymph nodes are common but, with longer survival from
rate. 1 10,111
more effective therapy, cerebral metastasis is recognized increasingly.
The tumour is extremely friable and frequently shows necrosis and degeneration.111.113g 116 In the better preserved areas the cells are moderate in size with generally round to oval and vesicular nuclei. Nuclear membranes are distinct and nucleoli are inconspicuous. Mitoses are present in most tumours but are not usually abundant. Cytoplasm is finely granular, but may be clear or vesicular, reflecting presumably the presence of intracellular glycogen. Cell boundaries are typically ill-defined. A propor- tion of tumours show cells with small, dark, elongated nuclei and scalloped cytoplasmic borders. These cells occur singly or in groups (Fig. 24) and are commonly referred to as 'second- ary cells'. Although their nature is still controver- sial, a degenerative origin is favoured by most.117-119 Aggregation of cells around necrotic foci is the explanation advanced for the rosettes encountered occasionally in Ewing's sarcoma;1'6compared with neuroblastoma, the rosettes of Ewing's sarcoma are more irregular in outline and lack a distinct neuro- fibrillary core. A range of histological patterns including diffuse, lobular, filigree and trabecular arrangements are recognized." Those tumours
Fig. 24- Ewing's sarcoma showing a dimorphic pattern. The principal cells have vesicular nuclei with well-defined nuclear membranes and poorly delimited cytoplasmic boundaries. The nuclei of the secondary cells are, by contrast, small, dark and angulated. The tumour is divided irregularly into lobules by delicate vascular connective tissue septa. H & E, x 201

SMALL CELL TUMOURS IN CHILDHOOD 19
showing a filigree pattern are reported to be associ- ated with the least favourable outcome. A propen- sity for some tumours to invade the sarcoplasm of skeletal myofibres has been also viewed as a poor prognostic sign. lZo
Diatase labile PAS-positive staining for glycogen in tumour cell cytoplasm is common, the positivity occurring en bloc or finely dispersed (Fig. 25). The glycogen content of the ‘secondary cell’ is sparse by comparison, or may be absent. The demonstration of glycogen is influenced by the type of fixation, and optimal results are usually obtained with prior fixa- tion in absolute alcohol or in frozen sections. Characteristically, staining for reticulin shows fibres related to connective tissue or vascular walls with little tendency to encompass individual tumour cells (Fig. 26).115,116 Cell membrane-bound alkaline phosphatase activity has been demonstrated.
Ewing’s sarcoma may mimic osteomyelitis clini- cally, radiologically and even on histology. IZ1, 122
Histologically, the tumour should be distinguished from the round cell variant of o ~ t e o s a r c o m a ~ ~ ~ and mesenchymal chondrosarcoma (poly- h i s t i ~ m a ) . ’ ~ ~ ~ ~ ~ ~ The latter neoplasm may display cytoplasmic glycogen but, on careful searching, foci of chondroblastic differentiation are frequently revealed. Mesenchymal chondrosarcoma spans a
wide age range with the highest incidence in the second and third decades ; occasionally, younger patients are affected. The primary tumour may involve bone or soft tissue. In the small cell variant of osteosarcoma, reticulin staining shows fibres encompassing individual tumour cells.
Soft tissue Ewing’s sarcoma
Several reports have documented the existence of a soft tissue or extra-skeletal variant of Ewing’s
I Z 6 Usually deep-seated, the tumour is often attached to underlying periosteum. Glycogen may be present but tends to be sparse and secondary cells are usually lacking. There is no distinct male predilection as in conventional Ewing’s sarcoma and patients tend to be older, with a median age of twenty years. Common sites include the chest wall, paravertebral regions and lower extremities and lung and bone are the usual metastatic sites. Preliminary data suggest that there is a favourable response to treatment.lZ6 The paravertebral ‘round- cell’ tumours in children reported by Tefft et ~ 1 . ’ ~ ~ are now known to belong to this group. The possi- bility that this form of Ewing’s sarcoma is a manifestation of an underlying undetected primary osseous Ewing’s sarcoma has been raised. 128
Fig. 25 -Frozen scction preparation of Ewing’s sarcoma showing pronounced clumped cytoplasmic positivity with PAS reaction. PAS. x 502

20 S. VARIEND
Fig. 26-Ewing’s sarcoma showing reticulin fibres limited to connective tissue and vessels. with little tendency for fibres to encompass individual tumour cells. Gomori’s reticulin, x 502
Large cell variant of Ewing’s sarcoma
The existence of an uncommon atypical or large cell variant of Ewing’s sarcoma is also recognized.’29. 130 Compared with conventional Ewing’s sarcoma, there is no difference in anatom- ical location or age distribution and the male preponderance is retained. Apart from the increased nuclear size (being about twice that of conventional Ewing’s sarcoma), the cells also show a greater degree of nuclear irregularity as well as increased mitotic activity. Cytoplasmic glycogen and small, dark, secondary cells are seen and nucleoli are often conspicuous. This variant of Ewing’s sarcoma, in particular, may be confused with large-cell lymphoma or the small cell type of osteosarcoma. It is claimed that similar histology may be induced in conventional Ewing’s sarcoma by radiotherapy or ~hemothe rapy . ’~~ A large cell variant is also recognized to occur in association with the soft tissue form of Ewing’s sarcoma.Iz6
Ultrastructure
Electron microscopy has proved useful in diagnosis and also in characterizing the nature of Ewing’s sarcoma.117 ‘ *c) ,131 Cells appear ovoid to polygonal in shape and the nuclear outlines are usu-
ally smooth with one or two conspicuous nucleoli. Chromatin is generally finely dispersed but margin- ated along the nuclear membrane. The paucity of cytoplasm is confirmed, with organelles represented by only a few mitochondria and profiles of rough endoplasmic reticulum. By contrast, free ribosomes and polyribosomes are fairly numerous.
Diagnostically, the presence of aggregated glyco- gen is almost certainly the most important fea- ture.117*”8 Material prepared from paraffin blocks due to prior dissolution in formalin may not, how- ever, reveal glycogen. Junction complexes are sparse but occur in a large proportion of tumours while intracytoplasmic microfilaments and Golgi apparatus are sometimes seen. The occasional presence of dense bodies (probably lysosomes) and lipid droplets raises the possibility that the tumour is of histiocytic lineage.54 Attention has been drawn to similarities in the ultrastructure between alveolar rhabdomyosarcoma and Ewing’s sarcoma.84 Con- densed chromatin with inconspicuous nucleoli and vacuolated cytoplasmic processes extending between other (principal) cells characterize the secondary cell. The ultrastructure of the soft tissue variant of Ewing’s sarcoma and conventional osseous Ewing’s sarcoma has been reported as being similar.132-134

SMALL CELL TUMOURS IN CHILDHOOD 21
CONCLUSION
Microscopic assessment of small cell tumours must take account of a full clinical history, results of special investigations such as x-rays, and the measurement of biochemical markers, all of which require a close collaboration with the clinical oncologist. Problematic histology, as determined by routine methods, should be always anticipated and measures taken so that tissue samples are set aside provisionally for special procedures. Those involved in the removal of surgical material from children with suspected neoplasms must ensure that samples reach the laboratory in a fresh condition to permit appropriate sampling and preparation for enzyme histochemistry, immunochemistry, electron microscopy and suitable imprints.
Awareness of the prototypic histology, the spec- trum of variability and the usual biological behaviour of a given tumour adds significantly towards its accurate histological classification that helps, subsequently, to ensure that the most appropriate treatment programme is instituted. Conversely, the continued appraisal of therapy pro- tocols is dependent t o a great extent on accurate diagnosis.
In view of the inevitable impingement on the paediatric age range of some undifferentiated tumours commonly encountered in adults, this review cannot claim to be entirely comprehensive. Those tumours commonly encountered in children, however, have been discussed. There will remain, nevertheless, a minority of tumours with a small cell pattern that, despite the full application of current methodology, will defy diagnostic classification. Their histogenetic categorization will have to await further progrcss.
REFERENCES
Ghavimi F, Exelby PR, Lieberman PH, e ta l . Multidisciplinary treatment of embryonal rhab- domyosdrcoma in children: a progress report. Nut1 Cancer lnst Monogr 1981 ; 56: I 11-120. Rosen G, Juergens H, Caparros B, et al. Combina- tion chemotherapy (T-6) in the multidisciplinary treatment of Ewing’s sarcoma. Nut1 Cancer Inst Monogr 1981 ; 56: 289-299. Schaller RT, Schaller JF, Buschmann, G, Kiviat N. The usefulness of percutaneous fine needle aspira- tion biopsy in infants and children. J PedSurg 1983 ; 18: 398405.
4. Marsden HB, Steward JB (eds). Tumours in Chil- dren. Berlin, Heidelberg, New York : Springer. 1976; I .
5. Young JL, Miller RW. Incidence of malignant tumors in children. J Pediatr 1975; 86: 254258.
6. Kinnier Wilson LM, Draper GJ. Neuroblastoma, its natural history and prognosis: a study of 487 cases. Br M e d J 1974; 3: 301-307.
7. Adam A, Hochholzer L. Ganglioneuroblastoma of the posterior mediastinurn : a clinicopathologic review of 80 cases. Cancer I98 I ; 47: 373-38 1 .
8. Brown RJ, Szymula NJ, Lore JM. Neuroblastoma of the head and neck. Arch Otoluryngol 1978: 104:
9. Punt J, Pritchard J, Pincott JR, e t a / . Neuroblastoma: a review of 21 cases presenting with spinal cord compression. Cancer 1980; 45: 3095-3 10 1 .
10. Beckwith JB, Martin RF. Observations on the histopathology of neuroblastoma. J PedSurg 1968 ;
1 1. Beckwith JB. Wilms’ tumor and other renal tumors of childhood. A selective review from the National Wilms’ Tumor Study Pathology Centre. Hum Pathol1982; 14:481492.
12. D’Angio GJ, Evans AE, Koop CE. Special pattern of widespread neuroblastoma with a favourable prognosis. Lancet 1971 ; i: 1046-1049.
13. Evans AE, D’Angio GJ, Randolph J. A proposed staging for children with neuroblastoma. Cancer 1971 ; 27: 314318.
14. Bill AH. Thc regression of neuroblastoma. J Ped Surg 1968; 3: 103-106.
15. Triche TJ, Askin FB. Neuroblastoma and the dif- ferential diagnosis of small-, round-, blue-cell tumors. Hum Patholl983; 14: 569-595.
16. Evans AE. Staging and treatment of neuroblastoma. Cancer 1980; 45: 1799-1802.
17. Tobin R, Grippo RA. Pulmonary metastases in neuroblastoma. AJR 1982; 138: 75-78.
18. Gale GB, D’Angio GJ, Uri A, Chatten J, Koop CE. Cancer in neonates: the experience at the Children’s Hospital of Philadelphia. Pediatrics 1982; 70: 409413.
19. Beckwith JB, Perrin EW. In situ neuroblastoma. Am
20. Bolande RP. Benignity of neonatal tumors and con- cept of cancer repression in early life. Am J Dis Child
21. Knudson AG, Meadows AT. Regression of neuroblastoma TV-S; a genetic hypothesis. New Engl J Med I980 ; 302: 1254-1 255.
22. Boland RP, Vekemans MJ-J. Genetic models of car- cinogenesis. Hum Patholl983; 14: 658-662.
23. Stout AP. Ganglioneuroma of the sympathetic nervous system. Surg Gynecol Obstet 1947; 84:
24. Schweisguth 0. Excretion of catecholamine metab-
395-398.
3: 106-1 10.
J Path01 I963 ; 43 : 1089- 1099.
1971 ; 122: 12-14.
I0 1- 109.

22 S . VAP !IEND
olites in urine of neuroblastoma patients. J Ped Surg 1968;3: 118-120.
25. Kogut MD, Kaplan SA. Systemic manifestations of neurogenic tumors. J Pediatr 1962; 60: 694-704.
26. Triche TJ. Round cell tumors in childhood: the application of newer techniques to the differential diagnosis. Perspect Pediatr Pathol I982 ; 7:
27. Mendelsohn G, Eggleston JC, Olson JL, Said SI, Baylin SB. Vasoactive intestinal peptide and its rela- tion to ganglion cell differentiation in neuroblastic tumors. Lab Invest 1979; 41 : 144-149.
28. Reynolds CP, Smith RG, Frenkel EP. The diagnostic dilemma of the ‘small round cell neoplasm’. Cancer 1981 ; 48: 2088-2094.
29. Kemshead JT, Goldman A, Fritschy J, Malpas JS, Pritchard J. Use of panels of monoclonal antibodies in the differential diagnosis of neuroblastoma and lymphoblastic disorders. Lancet 1983; i: 12-14.
30. Dhillon AP, Rode J, Leathern A. Neurone specific enolase: an aid to diagnosis of melanoma and neuroblastoma. Histopathology 1982; 6: 81-92.
3 1. Bolande RP. The neurocristopathies : a unifying concept of disease arising in neural crest develop- ment. Hum Pathol1974; 5: 409-429.
32. Blume A, Gilbert F, Wilson S, Farber J, Rosenberg R, Niremberg M. Regulation of acetyl- cholinesterase in neuroblastoma cells. Proc Natl Acad Sci USA 1970; 67: 786-792.
33. Variend S, Loughlin MA. Histochcmical dem- onstration of acetylcholinesterase in neuro- blastoma. J Clin Patholl984; 37: 288-292.
34. Triche TJ, Ross WE. Glycogen containing neuroblastoma with clinical and pathological fea- tures of Ewing’s sarcoma. Cancer 1978; 41:
35. Yunis EJ, Walpusk JA, Agonstini RMJr, Hubbard JD. Glycogen in neuroblastomas. Amer J Surg Pathol1979; 3: 313-323.
36. Coppersmith DL, Powers JM, Hennigar GR. Angiomatoid neuroblastoma with cytoplasmic gly- cogen. A case report with histogenetic considera- tions. Cancer 1980; 45: 553-560.
37. Misugi K, Misugi N, Newton WA. Fine structural study of neuroblastoma, ganglioneuroblastoma and pheochromocytoma. Arch Pathol Lab Med 1968; 86: 160-169.
38. Yokoyama M, Okada K, Tolue A, Takayasu H, Yamada R. Ultrastructural and biochemical study of neuroblastoma and ganglioneuroblastoma. Invest Urol1971; 9: 156163.
39. Mackay B, Maasse SR, King OY, Butler JJ. Diagnosis of neuroblastoma by electron microscopy of bone marrow aspirates. Pediatrics
40. Mullins JD. A pigmented differentiating
41. Wilander E, Nordlinder H, Grimelius L, Larsson
279-322.
1425-1432.
1975; 56: 1045-1049.
neuroblastoma. Cancer 1980; 46: 522-528.
L-I, Angelborg C. Esthesioneuroblastoma. Virch- ows Arch (PatholAnat) 1977; 375: 123-128.
42. Elkon D, Hightower SI, Lim ML, Cantrell RW, Constable WC. Esthesioneuroblastoma. Cancer
43. Johnson RE, Scheithauer BW, Dahlin DC. Melanotic neuroectodermal tumor of infancy. A review of seven cases. Cancer 1983; 52: 661-666.
44. Bolen JW, Thorning D. Peripheral neuro- epithelioma : a light and electron microscopic study. Cancer 1980; 46: 2456-2462.
45. Harper PG, Pringle J, Souhami RL. Neuro- epithelioma-a rare malignant peripheral nerve tumor of primitive origin. Cancer 1981; 48: 2282-2287.
46. Hashimoto H, Enjoji M, Nakajima T, Kiryn H , Daimarn Y. Malignant neuroepitheliorna (periph- eral neuroblastoma). Amer J Surg Pathol 1983; 7:
47. Barson AJ, Ahmed A, Gibson AAM, MacDonald AM. Chest wall sarcoma of childhood with a good prognosis. Arch Dis Child 1978; 53: 882-889.
48. Askin FB, Rosai J, Sibley RK, Dehner LP, McAlis- ter WH. Malignant small cell tumor of the thora- copulmonary region in childhood. Cancer 1979; 43:
49. Linnoila RI, Tsokos M, Triche TJ, Chandra R. Evi- dence of neural origin and periodic acid-Schiff- positive variants of malignant small cell tumor of thoracopulmonary region (‘Askin tumour’). (Abstract) Lab Invest 1983; 48: 52A.
50. Soule EH, Mahour GH, Mills SD, Lynn HB. Soft tissue sarcomas of infants and children: a clini- copathological study of 135 cases. May Clin Proc
51. Weichert KA, Bove KC, Aron BS, Lampkin B. Rhabdomyosarcoma in children. A clinicopatho- logical study of 35 patients. Amer J Clin Pathol
52. Bale PM, Parsons RE, Stevens MM. Diagnosis and behaviour of juvenile rhabdomyosarcoma. Hum PathoZ1983; 14: 596-611.
53. Maurer HM. The Intergroup Rhabdomyosarcoma Study (NIH) : objectives and clinical staging classi- fication. J PedSurg 1975; 10: 977-978.
54. Dehner LP. Soft tissue sarcomas of childhood: the differential diagnostic dilemma of the small blue cell. Natl Cancer Inst Monogr No. 56. 1981 ; 43-59.
55. Enzinger FM, Shiraki M. Alveolar rhab- domyosarcoma. An analysis of 110 cases, Cancer
56. Horn RC, Enterline HT. Rhabdomyosarcoma; a clinicopathological study and classification of 39 cases. Cancer 1958; 11: 181-199.
57. Bale PM, Reye RDK. Rhabdomyosarcorna in childhood. Pathology 1975; 7: 101-1 1 1 .
58. Gonzales-Crussi F, Black-Shaffer S. Rhab- domyosarcoma of infancy and childhood. Amer J
1979; 44: 1087-1094.
309-3 1 8.
2438-245 1.
1968 ; 43: 3 13-326.
1976;66:692-701.
1969; 24: 18-31.

SMALL CELL TUMOURS IN CHILDHOOD 23
Surg Pathol1979; 3: 157-171. 59. Davis GL, Kissale JM, Ishak KG. Embryonal rhab-
domyosarcoma (sarcoma botryoides) of the biliary tree. Cancer 1969; 24: 333-342.
60. Tefft M, Fernandez C, Donaldson M, Newton W, Moon TE. Incidence of meningeal involvement by rhabdomyosarcoma of the head and neck in chil- dren. Cancer 1978; 42: 253-258.
61. Van Unnik AJM. Muscle tumours. In: Mastaglia FL, Walton J, eds. Skeletal Muscle Pathology. Edinburgh, London, Melbourne, New York: Churchill Livingstone, 1982; 561-574.
62. Canale VC, Volpe R, Carbone A, Grigoletto E. Botryoid rhabdomyosarcoma of the nasopharynx. J Laryngol Otol1983; 97: 553-556.
63. Enjoji M, Hashimoto H. Diagnosis of soft tissue sarcomas. Pathol Res Pract 1984; 178: 215-226.
64. Norris HJ, Taylor HB. Polyps of the vagina. A benign lesion resembling sarcoma botryoides. Can- cer 1966; 19: 227-232.
65. Dehner LP, Enzinger FM, Font RL. Fetal rhab- domyoma : an analysis of nine cases. Cancer 1972 ; 30: 160-166.
66. Enterline HG, Horn RC. Alveolar rhab- domyosarcoma : a distinctive tumor type. Cancer
67. Hays DM, Newton W J., Soule EH, et a/. Mortality among children with rhabdomyosarcomas of the alveolar histologic subtype. J Pediatr Surg 1983; 18: 412417.
68. Nuncz C, Abboud SL, Lemon NC, Kemp JA. Ovarian rhabdomyosarcoma presenting as Icukemia. Case report. Cancer 1983; 52: 297-300.
69. Patton RB, Horn RC Jr. Rhabdomyosarcoma: clinical and pathological features and comparison with human fetal and embryonal skeletal muscle. Surgery 1962; 52: 572-584.
70. Maurer HM, Moon T, Donaldson M, etal. Thc lntergroup Rhabdomyosarcoma Study : a prelimi- nary rcport. Cancer 1977; 40: 2015-2026.
71. Sarnat HV, DeMello DE, Siddiqui SY. Diagnostic value of histochemistry in embryonal rhab- domyosarcoma. Amer J Surg Pathol 1979; 3:
72. Variend S, Loughlin MA. An evaluation of enzyme histochemistry in the diagnosis of rhab- domyosarcoma in childhood. Histopathology in prccs.
73. Ciodlcwski HG. Are active and inactive phos- phorylase histochemically distinguishable? J Histochem Cytochem 1963; 11: 108-112.
74. Koh SJ, Johnson WW. Antimyosin and anti- rhabdomyoblast sera. Their use in the diagnosis of childhood rhabdomyosarcoma. Arch Pathol Lab Med 1980; 104: 118-122.
75. Mukai K, Schollmeyer JV, Rosai J. Immuno- histochemical localisation of actin : applications in surgical pathology. Amer J Surg Pathol 198 1 ; 5:
1958; 29: 356-366.
177-1 83.
91-97. 76. Miettinen M, Lehto VP, Badley RA, Virtanen I .
Alveolar rhabdomyosarcoma: demonstration of the muscle type of intermediate filament protein, Desmin, as a diagnostic aid. A m J Patholl982; 108: 24625 1.
77. Mukai K, Rosai J , Hallaway BE. Localisation of myoglobin in normal and neoplastic human skeletal muscle cells using an immunoperoxidase method. Amer J Surg Patholl979; 3: 373-376.
78. Corson JM, Pinkus GS. lntracellular myoglobin. A specific marker for skeletal muscle differentiation in soft tissue sarcoma. Am J Pathol 1981; 103: 384-389.
79. Brooks JJ. Immunohistochemistry of soft tissue tumors. Cancer 1982; 50: 1757-1763.
80. Kahn HJ, Yeger H, Kassim 0, etal. Immuno- histochemical and electron microscopic assessment of childhood rhabdomyosarcoma. Cancer 1983 ; 51 :
81. Eusebi V, Bondi A, Rosai J. Immunohistochemical localisation of myoglobin in non-muscular cells. Amer JSurg Pathol1984; 8: 51-55.
82. Royds JA, Variend S, Timperley WR, Taylor CB. An investigation of p-enolase as a histological marker of rhabdomyosarcoma. J Clin Pathol1984;
83. Morales AR, Fine G, Horn RC. Rhabdomyo- sarcoma; an ultrastructural appraisal. Path Annu
84. Churg A, Ringus J. Ultrastructural observations on the histogenesis of alveolar rhabdomyosarcoma. Cancer 1978;41: 1355-1361.
85. Mierau GW, Favara BE. Rhabdomyosarcoma in children: ultrastructural study of 31 cases. Cancer
86. LaValle Bundtzen J , Norback DH. The ultrastruc- turc of poorly differentiated rhabdomyosarcoma. Hum Patholl982; 13: 301-313.
87. Ghadially FN. Diagnostic Electron Microscopy of Tumours. London: Butterworths, 1980; 123.
88. Callihan TR, Coston WB. Childhood non- Hodgkin’s lymphomas in current histological perspectives. Perspect Pediatr Pathol 1982; 7:
89. Kjeldsberg CR, Wilson JF, Berard CW. Non- Hodgkin’s lymphoma in children. Hum Pathol
90. Murphy SB. Childhood non-Hodgkin’s lymphoma. N Engl J Med 1978; 299: 146-1449.
91. Wollner N. Non-Hodgkin’s lymphoma in children. Pediatric Clinics 1976; 23: 371-378.
92. Bernard A, Murphy SB, Melvin S, et al. Non-T, non-B lymphomas are rare in childhood and associ- ated with cutaneous tumor. Blood 1982; 59: 549-554.
93. Pinkel D, Johnson W, Aur RJA. Non-Hodgkin’s lymphoma in children. Br J Cancer 1975; 31 (Suppl
1897- 1903.
37: 905-910.
1972; 7: 81-106.
1980; 46: 2035-2040.
259-277.
1983; 14: 612-627.

24 S. VARJEND
2): 298-323. 94. Crist WM, Kelly DR, Ragab AH, et a/. Predictive
ability of Lukes-Collins classification for immunologic phenotypes of childhood non- Hodgkin’s lymphoma : an institutional serics and literature rcview. Cancer 1981 ; 48: 2070-2075.
95. Wright DH, Isaacson PG. Biopsy Pathology of the Lymphoreticular System. London : Chapman & Hall, 1983; 230.
96. Nathwani BN, Diamond LW, Winberg CD, et ul. Lymphoblastic lymphoma: a clinicopathologic study of 95 patients. Cancer 1981 ; 48: 2347-2357.
97. Long JC, McCaffrey RP, Aisenberg AC, Marks SM, K ung PC. Terminal deoxynucleotidyl transferase positive lymphoblastic lymphoma. Can- cer 1979; 44: 2127-2139.
98. Cossman J, Jaffe ES, Fisher RI. Diversity of immunologic phenotypes of T-cell lymphoma. Amer J Surg Patho11982 ; 6: 72.
99. Wright DH, Isaacson PG. Biopsy Pathology of the Lymphoreticular System. London: Chapman & Hall, 1983; 190.
100. Mann RB, Jaffe ES, Braylan RC, rt ul. Non- endemic Burkitt’s lymphoma: a B-cell tumor related to germinal centers. N Engl .I Mcd 1976;
101. Grogan TM, Warnke RA, Kaplan HS. A compara- tive study of Burkitts’ and non-Burkitt’s ‘undif- ferentiated’ malignant lymphoma. Cancer 1982; 49:
102. Hausner RJ, Rosas-Uribe A, Wickstrum DA, Smith PC. Non-Hodgkin’s lymphoma in the tirst two decades of life. A pathological study of 30 cases. Cancer 1977; 30: 1533-1547.
103. Berard CW, Jaffe ES, Braylan PC, Mann RB, Nanba K. Immunological aspects and pathology of the malignant lymphoma. Cancer 1978; 42:
104. Koh SJ, Vargas GF, Caces JN, Johnson WW. Malignant ‘histiocytic’ lymphoma in childhood. Am JClin Pathol1980; 74: 417-426.
105. Azar HA, Jaffc ES, Berard CW, et al. Diffuse large cell lymphomas (reticulum cell sarcomas, histiocytic lymphomas) : correlation of morphological features with functional markers. Cancer 1980; 46: 1428-1441.
106. Brooks HW, Evans AE, Glass RM, Pang EM. Chloromas of the head and neck in childhood. Arch Otolaryngull974; 100: 306-308.
107. Neiman RS, Barcos M, Bcrard C, et al. Granulo- cytic sarcoma: a clinicopathological study of 61 biopsied cases. Cancer 1981 ; 48: 1426-1437.
108. Ewing J. Diffuse endothelioma of bone. Pror New York Path Soc 1921 ; 21 : 17-24.
109. Siegal GP, Schoppe J, Foulkes M, Kissane JM, Askin FB. Ewing’s sarcoma in babies and toddlers; a clinicopathological report from the Intergroup Ewing’s Sarcoma Study Group. (Abstract.) Lab
295 : 685-69 I .
18 17-1 828.
91 1-921.
Invest 1983 ; 48: 13P. 110. Phillips RF, Higginbotham NL. The curability of
Ewing’s cndothelioma of bone in children. J Pediatr
I 1 1. Kissane JM, Askin FB, Foulkes M, Stratton LB, Shirlcy SF. Ewing’s sarcoma of bone: c h i - copathologic aspects of 303 C ~ S C S from the Inter- group Ewing’s Sarcoma Study. Hum Parhol 1983;
112. Kadin ME, Bensch KG. On the origin of Ewing’s tumor. Cancer 1971 ; 27: 257-273.
113. Kissane JM, Askin FB, Nesbit ME Jr., e t a / . Sarcomas of bone in childhood : pathologic aspects. Cancer Inst Monogr No. 56 1981 ; 29-41.
114. Angervall L, Enzinger FM. Extraskeletal neoplasm resembling Ewing’s sarcoma. Cancer 1975; 36:
115. Dahlin DC, Coventry MB, Scanlon PW. Ewing’s sarcoma: a critical analysis of 165 cases. J Bone Joint Surg 1961 ; 43-A: 185-192.
1 16. Lichtenstein L, Jaffe HL. Ewing’s sarcoma of bone. Am J Pathol1947; 23: 43-71.
I 17. Povysil C, Matejovsky A. Ultrastructure of Ewing’s tumour. Virchows Arch (Pathol Anat) 1977; 374:
118. Llombart-Bosch A, Blache R, Peydro-Olaya A. Ultrastructural study of 28 cases of Ewing’s sarcoma: typical and atypical forms. Cancer 1978;
119. Mahoncy JP, Alexander RW. Ewing’s sarcoma. A light- and electron-microscopic study of 21 cases. Amer J Surg Pathof 1978; 2: 283-298.
120. Stratton B, Askin FB, Kissane JM. Intramyofibcr skeletal muscle invasion in Ewing’s sarcoma 01‘ bone: clinicopathological observations from the lntcrgroup Ewing’s Sarcoma Study. Am J Pcdiu[r Hematol Oncol1982; 4: 231-235.
121. Nance CL, Roberts WM, Miller GR. Ewing’s sarcoma mimicking osteomyelitis. South Med J 1967;60: 10441050.
122. Cabanela ME, Franklin HS, Beabout, JW, Dahlin DS. Osteomyelitis appearing as neoplasms: a diagnostic problem. Arch Surg 1974; 109: 68-72.
123. Sim FH, Unni KK, Beabout JW, Dahlin DC. Ostcosarcoma with small cells simulating Ewing’s tumour. JBnneJoirrt Surg 1979; 61-A: 207-215.
124. Salvador AH, Beabout JW, Dahlin DC. Mesen- chymal chondrosarcoma-observation in 30 new cases. Cancer 1971 ; 28: 605-615.
125. Jacobson SA. Polyhistioma: a malignant tumor of bone and extraskeletal tissue. Cancer 1977; 40:
126. Soule EH, Newton W Jr., Moon TE, Tefft M. Extra- skeletal Ewing’s sarcoma. Cancer 1978; 42:
127. Tcfft M, Vawter GF, Mitus S. Paravertebral ‘round- cell’ tumours in children. Radiology 1969; 92:
1967; 70: 391L397.
14: 713-779.
240-25 1.
303-3 16.
41: 1362-1373.
2116-2130.
259-264.
1501-1 509.

SMALL CELL TUMOURS IN CHILDHOOD 25
128. Bignold LP. So-called ‘extraskeletal’ Ewing’s sarcoma. Am JClin Pathol1980;73: 132-143.
129. Nascimento AG, Unni KK, Pritchard DJ, Cooper KL, Dahlin DC. A clinicopathological study of 20 cases of large-cell (atypical) Ewing’s sarcoma of bone. Am J Clin Patholl980; 4: 29-36.
130. Llombart-Bosch A, Blache R, Peydro-Olaya A. Round cell sarcomas of bone and their differential diagnosis (with particular emphasis on Ewing’s sarcoma and reticulosarcoma). Hum Pathol 1982 ;
13 1. Hou-Jensen K, Priori E, Dmochowski L. Studies on 17: 113-145.
ultrastructure of Ewing’s sarcoma of bone. Cuncer 19 72 ; 29 : 280-286.
132. Wigger HJ, Salazar GH, Blane WA. Extraskeletal Ewing’s sarcoma. An ultrastructural study. Arch Pathol Lab Med 1977 ; 101 : 44-9.
133. Meister P, Gokel JM. Extraskeletal Ewing’s sarcoma. Virchows Arch (Pathol Anat) 1978; 378: 173- 179.
134. Navas-Palacios JJ, Aparicio-Duque R, Valdes MD. On thc histogenesis of Ewing’s sarcoma. An ultrastructural, immunohistochemical and cytochemical study. Cancer 1984; 53: 1882-1901.