Embed Size (px)
Citation preview

Slide 1
Falls and Falls and Stroke Stroke
Central South Regional Stroke Central South Regional Stroke ProgramProgram
September 2007September 2007
Funded by the Ministry of Health and Funded by the Ministry of Health and Long-Term CareLong-Term Care

Slide 2
Session OverviewSession Overview
The types of stroke. The types of stroke. The common changes that result from The common changes that result from
stroke.stroke.The link between stroke and falls.The link between stroke and falls.What factors What factors put a resident at risk of fallingput a resident at risk of falling Strategies to prevent a resident from fallingStrategies to prevent a resident from falling

Slide 3
What is a StrokeWhat is a Stroke
An An interruption of the supply of blood and interruption of the supply of blood and oxygen to an area of the brain.oxygen to an area of the brain.
This causes the brain cells in an area to die, This causes the brain cells in an area to die, and reduces the brain function in that area.and reduces the brain function in that area.
The area of the body controlled by the The area of the body controlled by the damaged area in unable to function properly.damaged area in unable to function properly.
There are two types of stroke.There are two types of stroke.
http://www.hc-sc.gc.ca/iyh-vsv/diseases-maladies/stroke-vasculaire_e.html#efhttp://www.hc-sc.gc.ca/iyh-vsv/diseases-maladies/stroke-vasculaire_e.html#ef

Slide 4
What is a Stroke?What is a Stroke?
A Guide to Understanding Stroke, Heart and Stroke Foundation of Canada, 1996
A stroke can A stroke can happen when a happen when a blood clotblood clot blocks blocks a blood vessel in a blood vessel in the brain.the brain.
80% of strokes are 80% of strokes are this type.this type.

Slide 5
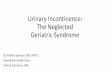
What is a Stroke?What is a Stroke?
A Guide to Understanding Stroke, Heart and Stroke Foundation of Canada, 1996
A stroke can also A stroke can also happen when a happen when a blood vessel blood vessel breaksbreaks and results and results in in bleedingbleeding in the in the brain.brain.
20% of strokes are 20% of strokes are this type.this type.

Slide 6
Risk factors you can do Risk factors you can do something about…something about…
High blood pressureHigh blood pressureHigh blood High blood
cholesterolcholesterolHeart diseaseHeart diseaseDiabetesDiabetes
Being overweightBeing overweightExcessive alcohol Excessive alcohol
useusePhysical inactivityPhysical inactivitySmokingSmokingStressStress
Pearson et.al., (2002) AHA Guidelines for Primary Prevention of Cardiovascular Disease and Stroke: 2002 Update: Consensus Panel Guide to Comprehensive Risk Reduction for Adult Patients Without Coronary or Other Atherosclerotic Vascular Diseases Circulation, 106, 388-391.

Slide 7
What does a What does a resident who has resident who has had a stroke look had a stroke look
like in LTC?like in LTC?

Slide 8
What are some of the losses What are some of the losses due to stroke?due to stroke?
paralysis or weakness on one side of the paralysis or weakness on one side of the body; body;
vision problems (double vision); vision problems (double vision); trouble speaking or understanding language; trouble speaking or understanding language; Difficulty swallowing safely.Difficulty swallowing safely.
http://www.hc-sc.gc.ca/iyh-vsv/diseases-maladies/stroke-vasculaire_e.html#efhttp://www.hc-sc.gc.ca/iyh-vsv/diseases-maladies/stroke-vasculaire_e.html#ef

Slide 9
What are some of the losses What are some of the losses due to stroke?due to stroke?
inability to recognize or use familiar inability to recognize or use familiar objects objects
tiredness; tiredness; depression; depression;
http://www.hc-sc.gc.ca/iyh-vsv/diseases-maladies/stroke-vasculaire_e.html#efhttp://www.hc-sc.gc.ca/iyh-vsv/diseases-maladies/stroke-vasculaire_e.html#ef

Slide 10
What are some of the losses What are some of the losses due to stroke?due to stroke?
exaggerated or inappropriate emotional exaggerated or inappropriate emotional responses; responses;
difficulty learning and remembering new difficulty learning and remembering new information; and information; and
changes in personality. changes in personality.
http://www.hc-sc.gc.ca/iyh-vsv/diseases-maladies/stroke-vasculaire_e.html#efhttp://www.hc-sc.gc.ca/iyh-vsv/diseases-maladies/stroke-vasculaire_e.html#ef

Slide 11
Stroke StatisticsStroke Statistics
There are between 40,000 and 50,000 There are between 40,000 and 50,000 strokes survivors in Canada each year.strokes survivors in Canada each year.
10% (4-5,000) of strokes survivors each year 10% (4-5,000) of strokes survivors each year require long-term care.require long-term care.
40% (16-20,000) of strokes survivors each 40% (16-20,000) of strokes survivors each year are left with a moderate to severe year are left with a moderate to severe impairment.impairment.
http://ww2.heartandstroke.ca/Page.asp?http://ww2.heartandstroke.ca/Page.asp?PageID=33&ArticleID=1078&Src=news&From=SubCategoryPageID=33&ArticleID=1078&Src=news&From=SubCategory

Slide 12
FallsFalls

Slide 13
Falls in CanadaFalls in Canada
In Canada,In Canada, falls are the sixth leading falls are the sixth leading cause of death among older adultscause of death among older adults (RNAO (RNAO Best Practice Guidelines, Falls and Restraints, 2002)Best Practice Guidelines, Falls and Restraints, 2002)
33% of older adults fall each year 33% of older adults fall each year (Campbell, (Campbell, Borrie & Spears, 1989).Borrie & Spears, 1989).
36% of those who fall develop serious 36% of those who fall develop serious injuries injuries (Koski, Luukinen, Laippala & Kiveal, 1998)(Koski, Luukinen, Laippala & Kiveal, 1998)
40% of admissions to nursing homes 40% of admissions to nursing homes are the result of falls are the result of falls (Tinetti, Speechley & Ginter, 1998).(Tinetti, Speechley & Ginter, 1998).

Slide 14
• frail and older • chronic illnesses• difficulty walking• thinking or memory,• independence with activities of daily living,
Increased falls happen in LTCHs Increased falls happen in LTCHs because:because:
People tend to be more:People tend to be more:
(Bedsine et al. (1996) Medical care of the nursing home resident. Philadelphia (PA): American College of Physicians. (Ejaz et al. (1994) Falls among nursing home residents: an examination of incident reports before and after restraint reduction programs. Journal of the American Geriatrics Society, 42, 9:960-4.

Slide 15
Falls related to strokeFalls related to stroke
Poor balancePoor balance– Divided attentionDivided attention– ImpulsivityImpulsivity– Slowed response timesSlowed response times
Inability to walkInability to walk– WeaknessWeakness– Gait problemsGait problems
spatial understanding spatial understanding of the world deficitsof the world deficits
ability to coordinate ability to coordinate body movementbody movement
Mental dysfunctionMental dysfunction
Hyndman et.al., (2004) Stops walking when talking as a predictor of falls in people with stroke living in the community Journal of Neurology Neurosurgery Psychiatry; 75:994-997Ugar et.al., (2000) Characteristics of falling in patients with stroke. Journal of Neurology Neurosurgery Psychiatry. 69, 649-651

Slide 16
Other causes of fallsOther causes of falls
DizzinessDizziness AccidentsAccidents Environment factorsEnvironment factors
– Wet floors Wet floors – Poor lightingPoor lighting– Bed rails and improper bed Bed rails and improper bed
heightheight blood pressureblood pressure Sudden loss of Sudden loss of
consciousnessconsciousness Acute illnessAcute illness Medication side effectsMedication side effects
Rubenstein et.al., (1994) Falls in Nursing Homes Annals of Internal Medicine. 121, 6:442-451.

Slide 17
What is balance?What is balance?
BalanceBalance is is the ability of the ability of a person not a person not
to fall.to fall.
Gustavsen, Marit, Aamodt, Geir and Mengshoel, Anne Marit (2006),'Measuring balance in sub-acute stroke rehabilitation', Advances in Physiotherapy, 8:1, 15 - 22

Slide 18
Balance is important because it Balance is important because it is is involvedinvolved in in day-to-dayday-to-day
activitiesactivities, such as , such as getting up getting up from a chair, walkingfrom a chair, walking and and
bendingbending over to pick up over to pick up something.something.
Gustavsen, Marit, Aamodt, Geir and Mengshoel, Anne Marit (2006) 'Measuring balance in sub-acute stroke rehabilitation', Advances in Physiotherapy,8:1, 15 - 22

Slide 19
Balance can be improved.Balance can be improved.
SSignificant improvement in balance, mobility, and gait
can be made after a stroke.
Garland SJ. Willems DA. Ivanova TD. Miller KJ. Recovery of standing balance and functional mobility after stroke. Archives of Physical Medicine and Rehabilitation. 2003 Dec; 84(12): 1753-9.

Slide 20
Early signs of fatigueEarly signs of fatigue
Foot draggingFoot dragging Increased leaning to Increased leaning to
one sideone side Walking hunched over Walking hunched over
on the walker or on the walker or leaning heavily on the leaning heavily on the walkerwalker
Decreased balance – Decreased balance – wobblywobbly
Michael et.al., (2006) Fatigue After Stroke: Relationship to Mobility, Fitness, Ambulatory Activity,...Rehabilitation Nursing; Sep/Oct 2006; 31, 5; ProQuest Nursing & Allied Health Source pg. 210

Slide 21
StrategiesStrategies
Note on medical chart or resident’s door that Note on medical chart or resident’s door that there is a high risk of fallsthere is a high risk of falls
Move high-risk residents to rooms close to Move high-risk residents to rooms close to the nursing station to increase observationthe nursing station to increase observation
Reassess after new episodes of illness or, Reassess after new episodes of illness or, change in meds. change in meds.
Lower side rails for those that climb out of Lower side rails for those that climb out of bed.bed.
Rubenstein et.al., (1994) Falls in Nursing Homes Annals of Internal Medicine. 121, 6:442-451.

Slide 22
StrategiesStrategies
Increase staff to resident ratio. Increase staff to resident ratio. Attend falls prevention education.Attend falls prevention education.Use alarm systems when residents move Use alarm systems when residents move
unassistedunassistedUse protective hip padsUse protective hip pads
Rubenstein et.al., (1994) Falls in Nursing Homes Annals of Internal Medicine. 121, 6:442-451.

Slide 23
Always remember that you Always remember that you can request an can request an OT/PTOT/PT referral referral
from from CCACCCAC if you need if you need assistance with finding the assistance with finding the
right strategy.right strategy.

Slide 24
Remember to Remember to encourage the encourage the
residents to residents to ask for ask for
assistance.assistance.

Slide 25
CASE STUDYCASE STUDY

Slide 26
SueSue
Sue has just arrived to Cozy Acres long term Sue has just arrived to Cozy Acres long term care home from hospital. Sue was recently care home from hospital. Sue was recently
admitted for management of stroke.admitted for management of stroke.
What are some of the concerns you might What are some of the concerns you might have regarding Sue’s ability to remain safe have regarding Sue’s ability to remain safe upon arrival at the long-term care home?upon arrival at the long-term care home?

Slide 27
SueSue
Later when you are able to review Sue’s transfer Later when you are able to review Sue’s transfer information, you are aware that Sue had fallen 3 information, you are aware that Sue had fallen 3 times prior to her transfer to Cozy Acres. Sue times prior to her transfer to Cozy Acres. Sue walks with a four wheel walker and requires some walks with a four wheel walker and requires some hands on assistance to keep her balance. Sue is hands on assistance to keep her balance. Sue is impulsive and is not aware that her lack of balance impulsive and is not aware that her lack of balance may cause her to fall and possibly hurt herself. may cause her to fall and possibly hurt herself. Sue’s family is very concerned about her falls and Sue’s family is very concerned about her falls and the potential to hurt herself. the potential to hurt herself.
What is your plan to maximize Sue’s safety?What is your plan to maximize Sue’s safety?

Slide 28
Next Steps…Next Steps…
You are the eyes and ears of your facilityYou are the eyes and ears of your facilityBe aware of the diagnosis of your residentsBe aware of the diagnosis of your residentsTake this information and use it with the Take this information and use it with the
residents that you work with.residents that you work with.Share this information with other staff.Share this information with other staff.

Slide 29
More InformationMore Information
Acute Changes and StrokeAcute Changes and Stroke Continence and StrokeContinence and Stroke Dementia and StrokeDementia and Stroke Falls and StrokeFalls and Stroke Pain and StrokePain and Stroke
Please contact: Please contact:
Rebecca Fleck or Kim YoungRebecca Fleck or Kim YoungCommunity and Long Term Care Specialist Community and Long Term Care Specialist Central South Regional Stroke ProgramCentral South Regional Stroke Program905-521-2100 x 44127905-521-2100 x 44127

Slide 30
AcknowledgementsAcknowledgements Best Practices Long-term Care Advisory GroupBest Practices Long-term Care Advisory Group Best Practices Long-term Care Evaluation GroupBest Practices Long-term Care Evaluation Group Best Practice Falls Working Group, Waterloo Best Practice Falls Working Group, Waterloo Mary-Lou van der Horst, Regional Best Practice Coordinator Long-Term Mary-Lou van der Horst, Regional Best Practice Coordinator Long-Term
Care Central South RegionCare Central South Region Wendy MacDougal, Regional Best Practice Coordinator Long-Term Wendy MacDougal, Regional Best Practice Coordinator Long-Term
Care Central West. Care Central West. Beverley Morgan, Beverley Morgan, Project Coordinator, RNAO Best Practice Guidelines, Project Coordinator, RNAO Best Practice Guidelines,
Hamilton Health SciencesHamilton Health Sciences Central South Regional Stroke ProgramCentral South Regional Stroke Program Maryann Watts, Hamilton Health Sciences, Clinical Manager Neuro-Maryann Watts, Hamilton Health Sciences, Clinical Manager Neuro-
ambulatory Centreambulatory Centre Melanie Fall Stratton, Regional Stroke Program, Program Manager,Melanie Fall Stratton, Regional Stroke Program, Program Manager, Kim Young, Regional Stroke Program, Community and Long-term Care Kim Young, Regional Stroke Program, Community and Long-term Care
SpecialistSpecialist Lisa Colizza, Regional Stroke Program, Regional Stroke Development Lisa Colizza, Regional Stroke Program, Regional Stroke Development
SpecialistSpecialist Nancy van Essen, Regional Stroke Program, Stroke Rehabilitation Nancy van Essen, Regional Stroke Program, Stroke Rehabilitation
CoordinatorCoordinator Carol Pereira, Regional Stroke Program, LTC Project CoordinatorCarol Pereira, Regional Stroke Program, LTC Project Coordinator

Slide 31