Embed Size (px)
Citation preview

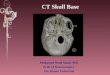
Skull Base Trauma & CSF Leaks
ASHNR 2016
Department of Radiology and Imaging Sciences Division of Neuroradiology
Kristen Lloyd Baugnon, M.D.
Disclosures
No relevant disclosures
Objectives
! Describe patterns of skull base fractures
! Identify complications requiring
multidisciplinary treatment
! Algorithim for CSF Leak Diagnosis and Evaluation
! Develop a checklist
Skull base trauma
! Up to 16% of CHI ! High velocity impact ! Penetrating trauma <10%
! Assoc w complex facial and orbital fractures ! Detection important
! Tx depends on IC injury and complications ! Multidisciplinary care
Detection of skull base fx ! Can be challenging if
nondisplaced ! NCCT Clues:
! Pneumocephalus ! Blood in sinuses/mastoids ! Overlying ST swelling
! Freq missed: Occipital condyle, ACF, tbone
Detection of skull base fx ! Thin section bone
algorithm MDCT with reformats ! Coronal, Sagittal, tbone ! 3D VR reformats ! Curved MIP reformats
! Beware of pseudofractures!
Supraorbital foramen and sphenofrontal suture

Suture diastasis Patterns of SB Fracture ! Patterns seen depend
on direction of impact ! Many different
classification systems ! Location in skull base
(ACF, MCF, tbone, PCF)
! Assoc complications ! Fractures often
complex/mixed
Anterior cranial fossa trauma Anterior skull base fractures ! Direct frontal trauma ! “Frontobasal” fractures
! Frontal (upper 1/3 face) ! Basal (ant skull base)
! Type I-III fractures ! Type I – medial, linear ! Type II – lateral ! Type III – mixed,
comminuted
Type I Frontobasal fracture
Manson et al Plast Recon Surg 2009
Anterior skull base fractures ! Direct frontal trauma ! “Frontobasal” fractures
! Frontal (upper 1/3 face) ! Basal (ant skull base)
! Type I-III fractures ! Type I – medial, linear ! Type II – lateral ! Type III – mixed,
comminuted ! Types II& III more assoc with
complications
Type II Frontobasal fracture
Anterior skull base fractures ! Direct frontal trauma ! “Frontobasal” fractures
! Frontal (upper 1/3 face) ! Basal (ant skull base)
! Type I-III fractures ! Type I – medial, linear ! Type II – lateral ! Type III – mixed,
comminuted ! Types II& III more assoc with
complications
Type III Frontobasal fracture

Middle cranial fossa trauma Central skull base fractures ! Oblique pattern: frontal
impact extending to central skull base ! Facial fxs, type II/III FB
fxs, CSF leak ! Transverse: lat impact
! CN and vascular injury ! Often assoc with tbone
fxs ! Anterior vs posterior Oblique central skull base fracture
Central skull base fractures ! Oblique pattern: frontal
impact extending to central skull base ! Facial fxs, type II/III FB
fxs, CSF leak ! Transverse: lat impact
! CN and vascular injury ! Often assoc with tbone
fxs ! Anterior vs posterior
Anterior Transverse fx
Central skull base fractures ! Oblique pattern: frontal
impact extending to central skull base ! Facial fxs, type II/III FB
fxs, CSF leak ! Transverse: lat impact
! CN and vascular injury ! Often assoc with tbone
fxs ! Anterior vs posterior
Posterior Transverse fx
Posterior skull base trauma Posterior skull base fractures
! Lateral and/or posterior blow to occiput
! Occipital bone, +/-ext to petrous t bone and FM
! No simple classification scheme
! T bone fxs described independently

Clivus fractures
Transverse Clival fx
! Central and posterior skull base fractures
! High mortality ! Brainstem, NV
! Transverse ! Lateral blow ! CN/ICA injury (CN VI)
Clivus fractures
Transverse Clival fx
! Central and posterior skull base fractures
! High mortality ! Brainstem, NV
! Transverse ! Lateral blow ! CN/ICA injury (CN VI)
Clivus fractures
Longitudinal Clival fx
! Central and posterior skull base fractures
! High mortality ! Brainstem, NV
! Transverse ! Lateral blow ! CN/ICA injury (CN VI)
! Longitudinal ! Axial loading ! VB/CC jxn injury, retroclival
hematoma
Clivus fractures
Longitudinal Clival fx
! Central and posterior skull base fractures
! High mortality ! Brainstem, NV
! Transverse ! Lateral blow ! CN/ICA injury (CN VI)
! Longitudinal ! Axial loading ! VB/CC jxn injury, retroclival
hematoma
Complications of SB trauma
! Depend on location ! Intracranial ! Vascular (MCF & PCF) ! CN
! ACF: CN II (Anosmia) ! MCF: CN II, III, IV, V, VI ! Tbone: CN VII, VIII ! PCF: CN IX, X, XI, XII
! CSF leak (ACF, MCF)
Intracranial injury ! IC injuries common – high
velocity impact ! Multicompartmental
hemorrhage, parenchymal contusions, DAI

Intracranial injury: MCF
Venous epidural hematoma
! Anterior MCF epidural hematoma
! Greater wing sphenoid fx ! Benign – venous
(sphenoparietal sinus) ! Self limited
Arterial epidural hematoma
! Anterior MCF epidural hematoma
! Greater wing sphenoid fx ! Benign – venous
(sphenoparietal sinus) ! Self limited
! Lateral MCF epidural – middle meningeal artery
Intracranial injury: MCF
! Posterior Fossa Epidural Hematoma (PFEDH)
! Most common IC comp assoc with posterior skull base fx
! Venous etiology ! Children ! Can expand rapidly ! May require
decompression
Intracranial injury: PCF Vascular Injury: Venous ! Traumatic venous sinus
thrombosis ! 55% of fxs through
jugular bulb/sigmoid sinus
! Transverse and sagittal sinus less common
! ↑ ICP, venous hemorrhage, infarct (7%), dural AVF
Delgado AJE et al. Radiology 2010
! Traumatic venous sinus thrombosis
! 55% of fxs through jugular bulb/sigmoid sinus
! Transverse and sagittal sinus less common
! ↑ ICP, venous hemorrhage, infarct (7%), dural AVF
Non contrast head CT
Delgado AJE et al. Radiology 2010
Vascular Injury: Venous
! Traumatic venous sinus thrombosis
! 55% of fxs through jugular bulb/sigmoid sinus
! Transverse and sagittal sinus less common
! ↑ ICP, venous hemorrhage, infarct (7%), dural AVF
CTA/CTV
Delgado AJE et al. Radiology 2010
Vascular Injury: Venous
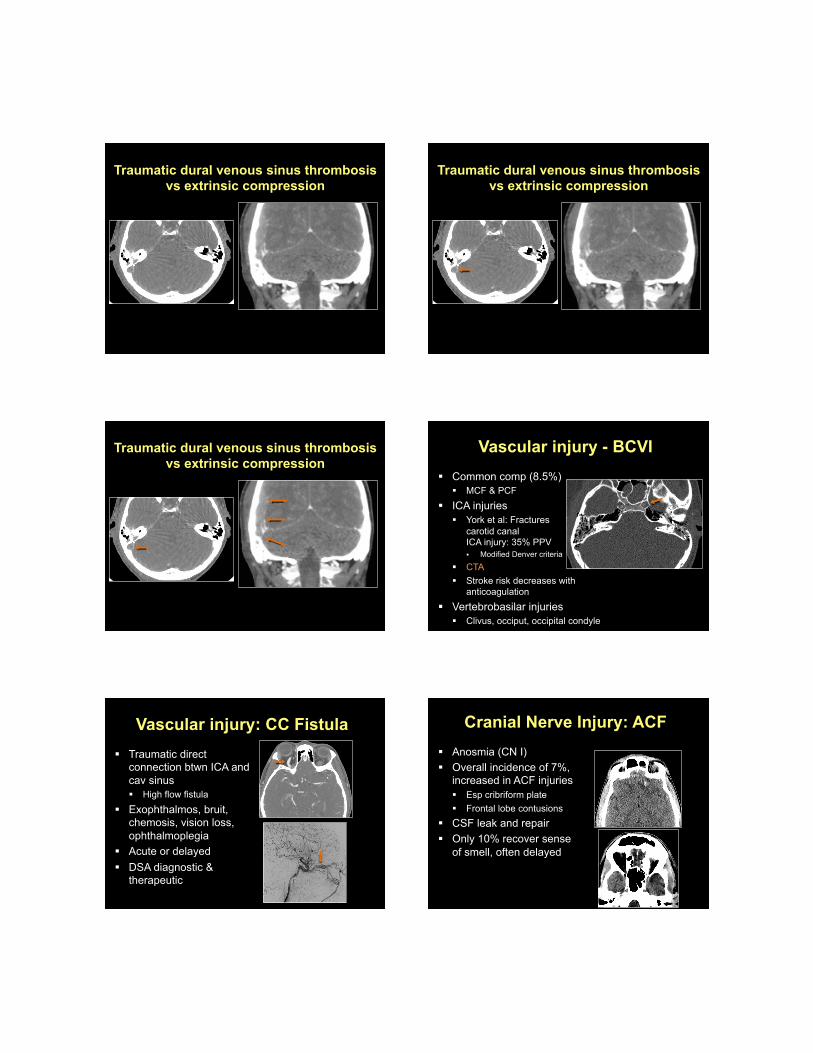
Traumatic dural venous sinus thrombosis vs extrinsic compression
Traumatic dural venous sinus thrombosis vs extrinsic compression
Traumatic dural venous sinus thrombosis vs extrinsic compression
Vascular injury - BCVI ! Common comp (8.5%)
! MCF & PCF
! ICA injuries ! York et al: Fractures through
carotid canal 35% PPV for ICA injury: 35% PPV ! Modified Denver criteria
! CTA ! Stroke risk decreases with
anticoagulation ! Vertebrobasilar injuries
! Clivus, occiput, occipital condyle
Vascular injury: CC Fistula ! Traumatic direct
connection btwn ICA and cav sinus ! High flow fistula
! Exophthalmos, bruit, chemosis, vision loss, ophthalmoplegia
! Acute or delayed ! DSA diagnostic &
therapeutic
Cranial Nerve Injury: ACF ! Anosmia (CN I) ! Overall incidence of 7%,
increased in ACF injuries ! Esp cribriform plate ! Frontal lobe contusions
! CSF leak and repair ! Only 10% recover sense
of smell, often delayed

Cranial nerve injury: MCF ! Acute or delayed presentation
! Delayed: Stretching/edema, better prognosis
! Optic nerve canal: II ! SOF:III, IV, V1, VI
! Orbital apex syndrome
! Sella: bitemporal heminaopsia (chiasm)
! Cav sinus/clivus: III, IV, V1, V2, VI
CN Injury: PCF
! Jugular foramen: IX, X, XI ! Hypoglossal canal
(occipital condyle): XII
CSF Leak
! 10-30% of skull base fxs ! Comminuted fxs
! Type II/III FB fxs, tegmen, sphenoid
! Pneumocephalus ! CSF otorrhea & rhinorrhea
! Often resolves spontaneously ! Surgery for persistent leak
! Delayed presentation
Suspected CSF Leak ! Beta 2 transferrin (beta trace protein) assay
! First screening test “gold standard” ! Protein specific to CSF ! Unequivocal evidence to support use
! High sensitivity and specificity
! Patient collects in testtube ! stores room temp or fridge
! Requires only a few drops (0.5 -1 cc) ! Limitations:
! Intermittent or no leak (unable to collect) ! False postive (rare!) Liver failure
Imaging evaluation ! Goals of imaging:
! LOCALIZE the leak ! Characterize size of defect
! Assess for meningocele ! Confirm diagnosis ! Assess for underlying cause
! No definite imaging gold standard ! Difficult diagnosis ! Lacking randomized controlled trials ! CT/MRI/cisternography (NM, CT, MR)
HRCT ! Standard of care – first line ! Localize osseous defect (s): 95% Sensitivity ! Do not need active leak to see defect ! Images used for intraop guidance ! MDCT : Thin slices (< 1mm) with reformats
! Image sinuses and mastoids ! Manipulate data on workstation, optimize W/L settings ! Measure defect in mutiple planes
! Correlates with size of defect within 2 mm in 75% in one study

HRCT – Imaging findings
Osseous defect with fluid level in sinus or mastoid
Lloyd K, et al Radiology 2008
HRCT – Imaging findings ! Nondependent soft tissue in nasal cavity or ME cavity,
adj to bony defect ! Concerning for cephalocele ! Consider MRI
HRCT ! If only one defect, and positive B2 transferrin
! Surgery
! Limitations: ! Defect does not necessarily = leak ! Multiple osseous defects with adjacent sinus opac
42 yo F w remote h/o trauma
CT - cisternogram ! Pt needs to be actively leaking (or able to elicit) ! Technique:
! Pre-Cisternogram CT: ! Supine MDCT with thin sections (reformats) ! Blood, inspissated secretions, osteogenesis
! LP: 5-7 cc of intrathecal contrast ! Head down and provocative maneuvers
! Post-Cisternogram CT: ! Direct coronal in prone position (elicit leak) ! Supine MDCT with thin section reformats
CT Cg - Findings ! Bony defect ! ↑ density adjacent to
bony defect (measure ROI if no visible change)
! Pooling of high density in adjacent sinuses
Lloyd K, et al Radiology 2008

CT cg findings
• “Souffle” effect • Contrast washout
• Dependent drainage • Mvmt with position
CTcg Findings ROI Measurement
Pre ROI = - 12 Post ROI = 69
CT-Cg Limitations ! Invasive
! Small but inherent risk of infection/lumbar CSF leak ! Intrathecal contrast risk
! Radiation ! Time intensive interpretation ! Limited usefulness in slow flow or intermittent
leaks
MR - Cg ! Noninvasive & nonionizing ! Indicated if suspected encephalocele
! Nondependent soft tissue adjacent to bony defect ! Completely opacified sinus or ME (lobulated) adjacent
to bony defect ! Heavily T2w FS FSE sequences
! High resolution 3D T2 w SSFP (GRE) sequences ! i.e. CISS, FIESTA, SPACE
! Thin (3 mm) T1 axial, sag, coronal
! Sensitivity (85-89%), best combined w HRCT
MR – Cg Imaging Findings ! Continuous column of T2
hyperintense CSF extending from SA space to extracranial soft tissues
! Frank herniation of brain tissue
Lloyd K, et al Radiology 2008
MR – Cg with IT Gad ! Promising studies
! Sensitivity: up to 100% for high flow ! Selculuk et al: 60-70% sens for intermittent or
suspected leaks ! Delayed imaging up to 24 hours later
! No ionizing radiation ! Ease of interpretation ! Improved contrast resolution ! Assess cephaloceles

MR – Cg with IT Gad - Limitations
! Off label use, not FDA approved in US ! Many studies from outside US ! No unexpected adverse effects (HA, meningitis) with
doses and agents used (up to 107 pts in one study) ! No long term safety or large trials yet
! Study in 2016 with Avg 4.2 yr F/u, no long term adverse effects
! Consider carefully, only in pts with nl renal fxn
! Still need HRCT!
Vanhee A, et al. Neurology 86;16 Supplement P4.113, April 2016
MR – Cg with IT Gad ! Technique:
! Mult osseous defects, no/intermittent leaks, postop ! HRCT first ! Off-label use consent ! Pre-gad MR Cg sequences with T1 and T2w images ! LP – 0.5 ml intrathecal gadopentetate dimegulmine in
4 cc sterile, pres free saline, or CSF ! Scan at 1 hour, then again at 4-24 hours, as needed
! Fat sat T1w post in multiple planes
45 yo F w h/o int leak, mult potential osseous defects bilat
Cor T2W MR Cg Cor T1W FS MR Cg w IT Gad
Summary: Algorithm for Work-up of CSF leak
B2-transferrin
Positive HRCT
Multiple osseous defects
CT Cisternogram
Single osseous defect
No further imaging; most
likely site of CSF leak
Suspect Meningo-
encephalocele MR
Cisternogram
Negative
No imaging;
unlikely to be CSF
leak
Unable to collect fluid HRCT
MR Cisternogram, consider Intrathecal
contrast if high suspicion
Summary: SB Trauma
! Complex ! Even linear nondisplaced fractures can be
assoc with complications ! CTA/CTV:
! Carotid canal ! Cavernous sinus ! Jugular foramen/sigmoid sinus ! Clivus ! Occipital condyle
Skull base fractures: Checklist
" Posterior table frontal sinus " Anterior skull base " Skull base foramina (ON, SOF,
FR, FO, IAC, hypoglossal canal) " Carotid canal " Sigmoid sinus/jugular foramen " Clivus " Occipital condyle

References ! Baugnon KL, Hudgins PA. Skull base fractures and their complications. NI Clin N
Am 2014; 24(3):439-465.
! Manson PN, Stanwix MG, Yaremchuk MJ, et al. Frontobasal fractures: anatomical
classification and clinical significance. Plast Reconstr Surg 2009;124:2096-2106.
! Guy WM, Brissett AE. Contemporary management of traumatic fracture of the
frontal sinus. Otolaryngol Clin North Am 2013;46:733-748.
! Gean AD, Fischbein NJ, Purcell DD, et al. Benign anterior temporal epidural
hematoma: indolent lesion with a characteristic CT imaging appearance after blunt
trauma. Radiology 2010;257(1):212-8..
! York G, et al. Assoication of internal carotid artery injury with carotid canal
fractures in patients with head trauma. Am J Roentgenol 2005;184(5):1672-8.
References ! Miller PR, et al. Blunt cerebrovascular injuries: diagnosis and treatment. J Trauma
2001;51:279-85.
! Ochalski PG, et al. Fractures of the clivus: a contemporary series in the computed
tomography era. Neurosurgery 2009;65(6):1063-9.
! Kwong Y, et al. Fracture mimics on temporal bone CT: a guide for the radiologist.
AJR Aug 2012; 199(2):428-34
! Delgado AJE, et al. Prevalence of traumatic dural venous sinus thrombosis in
high-risk acute blunt head trauma patients evaluated with multidetector CT.
Radiology 2010 May;255(2):570-7.
References
• Bleier BS, et al. Preliminary study on the stability of beta-2 Transferrin in extracorporeal CSF. Otolaryngol Head Neck Surg 2011;144:101-3.
• Stone JA, et al. Evaluation of CSF Leaks: High-resolution CT compared with
contrast-enhanced CT and radionuclide cisternography. AJNR 1999;20:706-712 • Shetty PG et al. Evaluation of high-resolution CT and MR cisternography in the
diagnosis of cerebrospinal fluid fistula. Am J Neuroradiol 1998;19:633-639. • El Gammal T, et al. Cerebrospinal fluid fistula: detection with MR cisternography.
Am J Neuroradiol 1998;19:627-631. ! Lloyd MN, et al. Post-traumatic CSF rhinorrhoea: modern HRCT is all that is
required for the effective demonstration of the site of leakage. Clin Radiol 1994;49:100-103.
! Stone JA, et al. Evaluation of CSF Leaks: High-resolution CT compared with
contrast-enhanced CT and radionuclide cisternography. AJNR 1999;20:706-712
References, cont ! Lloyd KM, Delgaudio JH, Hudgins PA Imaging of Skull Base Cerebrospinal Fluid
Leaks in Adults. Radiology 2008;248:725-36. ! Dillon WP. Intrathecal Gadolinium: Its Time has Come? AJNR 2008;29:3-4. ! Manes, RP, Ryan MVV, Marple BF. A novel finding on CT in the diagnosis and
localization of CSF leaks without a clear bony defect. Int Forum Allergy Rhinol 2012;2(5):402-404.
! Sampaio MH, et al. Predictability of quantification of beta-trace protein for diagnosis of cerebrospinal fluid leak: cutoff determination in nasal fluids with two control groups. Am J Rhinol Allergy 2009;23(6):585-90.
! Selcuk H, et al. Intrathecal Gadolinium-Enhanced MR Cisternography in the Evaluation of CSF leakage. AJNR 2010;31:71-75.
! Algin O, et al. The contribution of 3D-CISS and contrast enhanced MR cisternography in detecting cerebrospinal fluid leak in patients with rhinorrhea. British Journal of Radiology 2010;83:225-232.
! LaFata V, et al. CSF leaks: Correlation of High-Resolution CT and Multiplanar reformations with Intraoperative Endoscopic findings. AJNR 2008;29:536-41.
! Vanopdenbosch LJ, et al. MRI with intrathecal Gadolinium to Detect a CSF leak: a prospective open-label cohort study. J Neurol Neursurg Psychiatry 2011;82:456-458.