Embed Size (px)
Citation preview

Nonalcoholic Fatty Liver Disease
s_khalilzadeh

A NovelCardiometabolic Risk Factor for Type 2 Diabetes
NAFLD and T2DMNAFLD is closely associated with features of the metabolic
syndrome and is regarded as the hepatic manifestationof the syndrome .The amount of intrahepatic
fat closely correlates with serum liver enzyme levels andthe number of metabolic syndrome features Patients
with T2DM have approximately 80% more intrahepaticfat content than age-, sex-, and body weight-matched
nondiabetic
Controls, and their serum liver enzymes are lessrepresentative of the severity of intrahepatic fat
accumulation

NAFLD AND T2DM
patients with NAFLD and T2DM arealso more likely to develop the more
advanced forms ofNAFLD, such as NASH, advanced fibrosis,
cirrhosis, andin some cases hepatocellular carcinoma

Poor glycemic controlBecause NAFLD is strongly associated
with IR, patients With T2DM and NAFLD often have poor
glycemic controlcompared to their counterparts without
NAFLD The presence of NAFLD in people with
T2DM oftenmakes it difficult to obtain good glycemic
control
stable glycemic control with in insulin treated T2DM patient it has
been demonstrated that the intrahepatic triglyceride content
was more closely correlated with the daily insulin dose
and the ability of insulin to suppress hepatic glucose production
and better explained the interindividual variation
in insulin requirements

In addition, when the relationship between NAFLD
and peripheral glucose metabolism was explored in
healthy individuals, the association between the intrahepatic
triglyceride content and systemic IR was stronger
than the association with intramyocellular lipid content,
visceral fat content, or sc fat content

NAFLD and risk of chronic diabetic complicationsand mortality among T2DM patients
The presence of NAFLD among patients with T2DMappears to be an important risk factor for all-cause mortality.
A community-based study of T2DM individualsreported that those with NAFLD had a 2.2-fold increased
risk of all-cause mortality compared with thosewithout NAFLD; the most common causes of death
were malignancy, CVD, and liver-related complicationsEvidence is mounting that NAFLD is associated
with the presence of vascular disease, ie, the most commoncause of death in people with T2DM

Evidence Linking NAFLD With Risk ofDeveloping T2DM
modestly increased serum GGT and ALT levels were independent,
long-term predictors of incident T2DM in
both sexes


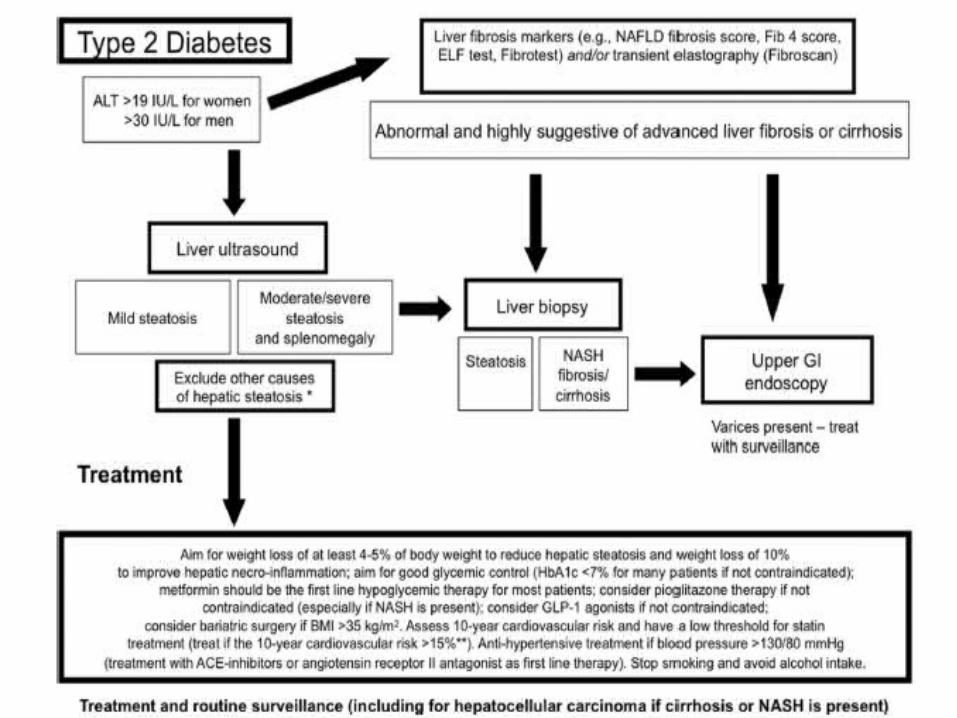
Treatment Options for NAFLD
Presently, there is no licensed treatment for human NAFLD
Most interventions evaluated for the treatmentof NAFLD are those commonly used for the
treatment ofT2DMand exert a rather indirect effect through
improvementin IR and glycemia

Statinsstatins can be used in dyslipidemic
individuals with increasedbaseline liver enzymes and may even
produceSome histological benefit in NASH

Lifestyle modificationsgradual weight reduction,
achieved either by hypocaloric diet alone or in combination
with increased physical exercise, can be effective indecreasing hepatic steatosis and
necroinflammation (thereduction of hepatic steatosis and necroinflammation
isproportional to the intensity of the lifestyle
interventionand generally requires a weight loss between 5 and
10%)
Insulin-sensitizing agentsMetformin, the first-line choice in oral
therapy forT2DM, has beneficial effects on serum
aminotransferasesand IR but has no significant effect on
liver histology andis not recommended as a specific
treatment for liver disease in patients with NAFLD/NASH

Insulin-sensitizing agents Pioglitazone can
be used to treat steatohepatitis in patients with biopsyproven NASH;
there are no randomized clinical trials withhistological endpoints that investigated
pioglitazone tospecifically t reat patients with NAFLD. A recent
metaanalysisreported that pioglitazone improved steatosis
andnecroinflammation, but not fibrosis

Omega-3 polyunsaturated fatty acid (PUFA)supplementation
supplementationHigh doses of omega-3 PUFAs are effective
in treatinghypertriglyceridemia that is often a feature
of NAFLD andT2DM.

Glucagon-like peptide agonist (GLP-1 analog)
GLP-1 agonists have proved to be effective therapies to
improve glycemic control in people with T2DM; and interesting
additional effects of treatment are weight loss,
decreased appetite, and improved IR, which can prove
helpful in people with NAFLD

Vitamin EIt is known that increased oxidative stress occurs in
Both NAFLD and T2DM .Consequently, besides targetingIR or lipid synthesis mechanisms per se, another
therapeuticoption for NAFLD treatment may be to decrease
oxidative stress by administration of an antioxidant suchas vitamin E. Vitamin E therapy, as compared with placebo,
was associated with significant improvements in liver enzymes
and some histological features of NASH such assteatosis and necroinflammation

Vitamin DPreliminary experimental evidence
suggests that via effects in both adipose tissue and liver,
low serum vitaminD levels may predispose to intrahepatic
lipid accumulation and hepatic inflammation, contributing
to the development and progression of NAFLD .However, whether vitamin D supplementation
amelioratesNAFLD is uncertain, and randomized clinical
trials are needed in man.
Vitamin D





![Beneficial Effects of Thymoquinone on Metabolic Function ... · impacts the liver [4]. Recent data suggest that nonalcoholic fatty liver disease (NAFLD), considered the hepatic manifestation](https://img.dokumen.tips/doc/110x75/5f2e6e1bcadd385cc567ce93/beneficial-effects-of-thymoquinone-on-metabolic-function-impacts-the-liver-4.jpg)