Embed Size (px)
Citation preview

International Medical Corps South Sudan Baseline Mental Health Situational Analysis
March 2015

1
1. Background 2. Methodology
3. Results 3.1 The Environment
3.1.1 Location and physical setting 3.1.2 Socio-economic profile 3.1.3 Socio-political environment 3.1.4 Socio-cultural attitudes towards
people with mental illness
3.2 The Health System 3.2.1 General health services 3.2.2 Mental health services
3.3 Mental Health Needs
3.3.1 Prevalence of mental health problems and psychological distress
3.3.2 Psychosocial issues
3.4 Anticipated challenges in mental health PHC integration
4. Summary and Recommendations Appendices Appendix A: Situational Analysis
Information Framework and Data Sources
Appendix B: IMC MHPSS Situational Analysis Tool
Appendix C: IMC Mental Health Knowledge and Attitudes Questionnaire
Appendix D: IMC PHC MH Integration Checklist
Acknowledgements
The International Medical Corps South Sudan County Team as well as the Mental Health and Psychosocial Support Team have played a pivotal role in bringing this report to light. We especially wish to thank Dr Esubalew Wondimu, Gurusewak Khalsa and Erin Shedd for their invaluable assistance. Agany Majak, the national coordinator of the Global Mental Health PHC Integration Program has contributed substantially in the preparation of this report. We also wish to thank the many key informants who have shared valuable insights with us as well as International Medical Corps’ mental health specialists whose rapid assessment reports conducted earlier have contributed to much of the information included in this report.
Contact
This report was completed by Dr. Neerja Chowdhary, International Medical Corps Global Mental Health PHC Integration Project Coordinator.
For questions regarding this report please contact: Dr. Inka Weissbecker, International Medical Corps Global Mental Health and Psychosocial Advisor ([email protected])
Table of Contents

2
“South Sudan’s political turbulence is akin to the chaotic structure of a stream of water from a tap: unpredictable from moment to moment……”1 This sentence best describes the political chaos and resulting internal conflict in South Sudan since it gained independence in 2011. Fighting in Juba erupted on the December 15, 2013, causing the deaths and displacement of thousands and a wave of insecurity throughout the country, which continues today, particularly in the fragile states of Unity, Jonglei, and Upper Nile. Currently, 2.5 million people face crisis/emergency levels of food insecurity and 1.5 million people are internally displaced by conflict.2
International Medical Corps is currently operating both mobile and static health care units and nutrition interventions to highly vulnerable populations across the three states. In addition, mental health programming is deemed as being essential to address and strengthen the coping mechanisms of the populations in the current crisis, to mitigate the effects of stress and trauma on individuals and to support the social cohesion of society at large. The overall objective of this situational analysis is to review mental health needs and services in South Sudan before International Medical Corps started supporting mental health services in order to have baseline information as a comparison against follow-up and to inform International Medical Corps’ longer term Mental Health and Psychosocial Support (MHPSS) programming in the region. The sites in which this situational analysis has been conducted, therefore, are the sites in which International Medical Corps is currently implementing its MHPSS programs i.e. Juba, Maban, Malakal, Awerial and Akobo.
The situational analysis collated information collected during initial rapid assessments by International Medical Corps’ psychiatrists conducted in April and May 2013, February 2014 and October 2014 and as well as data collected subsequently by the Global and National International Medical Corps program coordinators.
The timelines of the different assessments are presented in the Gantt chart below: Assessment 2013 2014 2015
Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Rapid Mental Health Situational Analysis, International Medical Corps, Maban
Apr
Mental Health in Health Facilities, International Medical Corps South Sudan
May
Rapid Mental Health Siutuational Analysis: Awerial and Malakal
Feb
Rapid Mental health Assessment: International Medical Corps, Akobo and Juba
Aug
Field visit by Global Project Coordinator Feb Data collection methods included desktop reviews as well as semi-structured interviews and focus group discussions with key informants. Appendix A provides the detailed situational analysis information framework and data sources that contributed to this report. The specific tools used for data collection included (Appendices B, C, D): 1 Alex de Waal. When Kleptocracy Becomes Insolvent: Brute Causes Of The Civil War In South Sudan. African Affairs, 2014, 113/452, 347–369. Downloaded from http://afraf.oxfordjournals.org/ 2 The United Nations Office for the Coordination of Humanitarian Affairs (OCHA) South Sudan: Crisis Situation Report No.78 (as of 12 March 2015).
1. Background
2. Methodology

3
1. An adapted version of the WHO/UNHCR (2012) Assessing Mental Health and Psychosocial Needs and Resources - Toolkit for Humanitarian Settings, specifically, the checklist for integrating mental health in primary care in humanitarian settings and the Participatory assessment: perceptions by general community members
2. A Knowledge and Attitudes questionnaire adapted from the following sources: a. US Department of Health and Human Services, Substance Abuse and Mental
Health Services Administration (SAMHSA, 2010). Health Styles Population survey. Conducted annually in the United Stated by Porter Novelli and adapted from British Omnibus National Survey.
b. Scottish Government (2008). Well? What Do You Think?: The Fourth National Scottish Survey of Public Attitudes to Mental Wellbeing and Mental Health Problems.
c. Afghanistan Ministry of Public Health (MOPH). Basic Package of Health Services, Mental health Training attitude survey.
d. IMC Iraq Mental Health Attitudes Survey (described in: Sadik, S., Bradley, M., Al-Hasoon, S., & Jenkins, R. (2010). Public Perception of Mental Health in Iraq. International Journal of Mental Health Systems 2010, 4:26). (adapted from Weller 1998, does contact with people with mental illness affect nurses)
e. Questions suggested for Afghanistan by IMC Afghanistan Technical Team. 3. Field guides for semi- structured interviews prepared based on themes to be explored
for this report.
Informed consent was obtained from all key informants who were interviewed.
Data collected was entered and analyzed using Microsoft Excel software. All qualitative data was analyzed using theme coding analysis.
3.1. The Environment 3.1.1. Location and physical setting South Sudan, officially the Republic of South Sudan, is a landlocked country in northeastern Africa that gained its independence from Sudan in 2011 following a referendum that passed with 98.83% of the vote. South Sudan is divided into ten states, which correspond to three
historical regions: Bahr el Ghazal, Equatoria, and Greater Upper Nile. It is covered in tropical forest, swamps, and grassland. The White Nile passes through the country, passing by Juba. 3.1.2 Socio-economic profile
South Sudan has a population of approximately 8 to 10 million (the exact figure is disputed) and a predominantly rural,
subsistence economy. This region has been negatively affected by war for all but 10 of the years since 1956, resulting in serious neglect, lack of infrastructure development, and major destruction and displacement. The economy of South Sudan is one of the world's most underdeveloped with South Sudan having little existing infrastructure and the highest
3. Results

4
maternal mortality and female illiteracy rates in the world as of 2011. The major ethnic groups present in South Sudan are the Dinka at more than 1 million (approximately 15 percent combined), the Nuer (approximately ten percent), the Bari, and the Azande. While inter-ethnic warfare predates the war of independence, since December 2013 up to 10,000 people are estimated to have been killed in the inter-ethnic Dinka-Nuer fighting.
3.1.3. Socio-political environment
Mental Health Policy and Legislation The policy statement on mental health as part of the South Sudan Health Policy (2006-‐‑2011) asserts that mental health is an integral part of public health and that the Ministry of Health will work with the social and other sectors to develop a flexible integrated system of accountable, accessible, and equitable mental health care and support services particularly at the community level. It states that “a mental health strategy will be developed that will include advocacy, legislation and human rights, planning, financing and organization of services, quality, the use of psychotropic medicines and how to address the mental health of people of all ages including children and adolescents” (Government of South Sudan, 2007). To date, a draft Mental Health Strategy for South Sudan has been developed in a collaboration between WHO and the Ministry of Health (MoH, Dec, 2011) and is currently under review. It outlines six strategic components: 1. Strengthening leadership and political commitment for mental health 2. Scaling up integration of mental health in primary health care2
3. Strengthening secondary and tertiary care mental health services 4. Identifying and prioritizing vulnerable persons 5. Inter-‐‑sectorial coordination and collaboration to promote mental health and prevent mental disorders 6. Promoting operational research. The strategy document also outlines mental health activities and levels of care from the catchment villages to Primary Health Care Units (PHCUs), Primary Health Care Centres (PHCCs) to the County Hospitals that are also specified in the South Sudan Basic Package of Health Services (BPHS) – (Table 1). Table 1: BPHS mental health activities outlined in the South Sudan MoH Strategy, 20113,4 Services and activities Village PHCU PHCC Hospitals Mental health education and awareness ü ü ü ü Case detection ü ü ü ü Anxiety disorders (e.g. post traumatic stress; panic disorder) refer follow up ü ü Depression: identification and biopsychosocial management refer follow up ü ü Epilepsy: identification and treatment refer follow up ü ü Psychotic and psychiatric cases: biopsychosocial management refer follow up ü ü Mental retardation: identification, education to parents ü ü ü ü Community based care and rehabilitation incl. support groups ü ü ü Inpatient treatment ü refer ü+ refer Reporting ü ü ü ü Monitoring and supervision ü ü ü
3 The Basic Package of Health and Nutrition in Primary Care. South Sudan, July 2011 (update) 4 Mental Health in Health Facilities, International Medical Corps South Sudan, May 2013

5
According to the BPHS, service elements for mental health include “(i) awareness creation at community level on mental disorders and their manifestations in local settings (ii) support for parents of infant with mental impairment, (iii) school-‐‑based interventions, such as teacher to pupil counseling, peer to peer counseling, identification and referral of children with poor school progress, counseling and referral of children with “new” onset deterioration in class (iv) workplace and unemployment counseling programs for youths and adults, (v) activity programs for elderly people (vi) abatement of domestic violence and street related aberrant behavior, substance abuse, home and school truancy and gender related violence (vii) interventions to develop assertiveness, self-‐‑reliance and appropriate participation, which are in turn components of mental health e.g, ‘gender equitable rights training” as an integrated component of programs for prevention of HIV infection”. The Government of Southern Sudan (2006) “Prevention and Treatment Guidelines for Primary Health Care Centers and Hospitals Clinical book” contains sections on neurology (including epilepsy) and psychiatry (including psychosis, depression, anxiety disorders, PTSD, alcohol dependence) and it covers psychosocial and pharmacological management. The guidance is only partially consistent with the WHO (2010) mhGAP Intervention Guidelines for mental, neurological and substance use conditions in general health settings and could benefit from updating. Nevertheless, the BPHS mental health component has not been implemented in South Sudan. General health staff has not received training in mental health and psychotropic medication and those is not yet on the list of national essential medicines for PHCCs and PHCUs. In terms of mental health rights and advocacy there is no mental health Act or other mental health related legislation in South Sudan and no informed consent procedures for inpatient admission or mental health treatment. Coordination Several organisations working in South Sudan started implementing psycho-social support programmes, to address the psychological and social effects of the civil war (detailed list in Table 6). This included international and national organisations. The scale and approach to psycho-social programming varied in approach and scale. There is still limited coordination and collaboration of the on-going psycho-social programmes in all sectors, like education, protection and health. This prompted the MoH to establish a MHPSS platform at the national level with the objective of enhancing the coordination and delivery of psychosocial support services and mental health services in South Sudan. Members are drawn from Government Departments, United Nations and Non-governmental Organisations working in health, education, (child) protection and other sectors (nutrition, security etc.) and meet once a month or as and when need arises. International Medical Corps is an active member of this group. The terms of reference of this Platform (drafted in December 2013) has the following specific objectives and activities5: 1. To reinforce the active participation of the members of the Platform while making it an
‘attractive’ platform with an additional value for its members • Visit each potential member of the Platform, assess the motivation, expectations and
expertise • Identify final list of active members of the Platform
5 Terms of reference for psycho-social support and mental health lead organizations in South Sudan. Drafted by the Mental Health Working Group. December 2013

6
• Finalize the mapping of actors for MH and PSS at national and State level as initiated by UNICEF (5Ws format) and translate this in a visual map (who is doing what where)
• Drafting a common and ‘attractive’ agenda in collaboration with Platform members • To conduct monthly platform meetings
2. Contributing to the development of national policies, laws, planning frameworks and
practices that enhance PSS and MH care programming • Support the MoH in its efforts to put MH as a priority on their agenda • Ongoing lobby and Advocacy efforts for PSS and MH within relevant Ministries in
collaboration with the Advocacy Workgroup of DCR • Link the Platform with other different Clusters and Forums ((NGO) Health,
Education) and sub clusters (Child Protection, GBV), Ministries in collaboration with the Advocacy Workgroup of the Dutch Consortium for Rehabilitation (DCR)
• Starting up to link the Platform to similar Regional initiatives (Burundi, Tanzania, Uganda, Congo) in order to exchange best practices
3. Enabling the stakeholders of the Platform to share their knowledge and expertise towards improved capacity and quality delivery of PS and MH interventions • Provide each member of the Platform the opportunity to present, share strategies,
activities, results and training opportunities • Sharing existing Best Practices for PSS and MH care • Compile existing assessments, surveys of the different members of the platform
about PS and MH prevalence rates, priorities to be addressed etc. 4. Ensuring that consultation takes place within the Platform in case of an emergency for the
delivery of quality and cultural appropriate PS/PFA services • Organizing an ad-hoc meeting of the Platform in case of an emergency • Briefing and exchanging about the results of the emergency related actions
3.1.4 Socio-cultural attitudes towards people with mental illness
The lack of a mental health policy and widespread social stigma in South Sudan has meant that mental illness is a hidden issue. People with mental illness are vulnerable to human rights violations, to physical and emotional abuse and from discrimination both from health workers and the wider community6.
Perceptions of general community members
Data in this section has been collated from the earlier rapid assessments (2013, 2014) as well as the recent field assessment done by the Global coordinator (Feb 2015). The sources are detailed in Appendix A. During the 2015 field assessment, community members were asked about their understanding of mental illness using the Participatory Assessment Questionnaire (see Appendix B). This explored how the community recognized someone with a mental illness, the perceived impact of mental illness including how the community treated people with mental illness, coping methods used by the patient and family and the pathways to care. The findings from these interviews are informing the content of International Medical Corps’ awareness raising activities in the community.
6 WHO AIMS report on mental health system in South Sudan. 2009

7
A total of 63 (39 women, 24 men) respondents were interviewed in 4 FGDs. In general, people with mental illness are identified as those who display bizarre appearance and behavior or those with ‘thinking too much’ (Table 2). The former group share common features with psychotic disorders (and called ‘Jin’) as described in Western classification systems. People who had experienced stressful life events were identified as ‘thinking too much’ and having symptoms suggestive of depression/anxiety disorders.
In addition, during the International Medical Corps rapid assessment conducted in Maban (May 2013), key informants reported that non-specific somatic complaints and somatic problems in reaction to stress are common. Depression usually occurs with somatic complaints and people tend to speak about stress in physical ways. Indeed, a local counselor may open a consultation by saying “how is the body”7.
Causes attributed to mental illness were an evil curse, punishment from God due to sins committed by him or his family (including ancestors), stress caused by the conflict, lack of support from family and close ones.
The impact of mental illness is experienced by the individual, the family and the community. The patient’s physical health may be affected, the family may be abandoned or suffer neglect and the community may be exposed to violent acts by the person with mental illness.
Table 2: Summary of mental health problems including symptoms, impact and help-seeking (Source: FGDs with community members, Feb 2013 and International Medical Corps rapid assessment, Maban 2013)
MHPSS Problem
Signs/Symptoms Impact Ways of help-seeking
Jin (possibly psychosis)
Talking alone, saying something that people do not expect them to say, getting worried and almost mad, going and shouting as if something surprised him, person cannot be understood by people, feeling like they need to get something but cannot, fighting, being in the street, not being able to think properly, wandering naked, neglect personal hygiene, isolated, talk to themselves
On the individual: Physical illness, don’t get married. Suicide On the family: abandon the family, including childrenOn the community: may be aggressive and violent with other people
Nothing can be done, some people can recover, some go to the hospital. Those one with severe mental disorders are taken to prison or tied up at home to protect them from making harm to the people. Some families isolate them, don’t take care of them Some take them to the traditional healer/doctor who may advise them to slaughter/sacrifice sheep, chicken
Thinking a lot (possibly depression)
People think about what they had before and what they worked hard for (e.g. land, business, cattle that died or was left behind), they sit with their head down and are worried, they cannot complete daily tasks
There is no help, people do not have a chance to gain anything back.
Alcohol abuse On the individual: neglect of personal health and appearance, may have physical complications such as oedema, anaemia. Neglected by family On the family: These people show lack of responsibility, stress in the family, violence,
7 Rapid Mental Health Situational Analysis, Maban Refugee Camps, South Sudan, International Medical Corps. April 2013

8
Help seeking involves either doing nothing, taking the person to prison or hospital or seeking the help of religious/faith healers. Coping: A literature review article on the mental health of South Sudanese refugees in the Diaspora found that mechanisms of coping with emotional distress, including encouraging connections with others, group social support and sharing experiences, helped to ease emotional difficulties8. Community members in the refugee camps were asked about the ways in which people cope and support each other. The results are summarized below.
Support of people in need • Coming together to help each other • If someone does not have something, neighbors will share
what they have or take up a collection • Giving sick people water and porridge • When someone in the community dies, neighbors cook for
their family
Music and art • Dance, music and drama groups • People coming together and playing guitar
and drums
In addition, people with mental illness are helped by family in fulfilling their practical needs such as nice clothing, good food, Shelter to sleep in and help with bathing and personal hygiene. Perceptions of healthcare providers In order to obtain information about knowledge and attitudes towards people with mental illness among health care providers, a self-report questionnaire was administered to a cohort of 33 respondents whose work experience ranged from 2 weeks to 3.5 years. They were composed of clinical officers (n=7), nurses (n=14), midwives (n= 4), social workers (n= 2) and others (n=6). The questions were rated on a 5-point scale (5=agree, 4=agree somewhat, 3=neutral, 2=disagree somewhat, 1=disagree). Note: While social workers are not directly targeted in the mhGAP training, they have been included here since they support activities in the PHCs. Amongst the causes that health care providers attributed to mental illness, most believed that it was due to trauma/misfortune and almost half believed that mental illness may have spiritual causes or occur as a result of personal weakness. (Figure 1).
Figure 1: Healthcare providers’ perceptions of the causes of mental illness
8 Tempany M. What research tells us about the mental health and psychosocial wellbeing of Sudanese refugees: a literature review. Transcult Psychiatry. 2009; 46(2): 300-‐‑15.
76
45 4236
18
0
20
40
60
80
Mental illness is caused by bad things happening to youI think mental disorders have mainly spiritual causesMental illness is caused by a personal weaknessMost people with convulsions are faking (pretending)Mental illness is God's punishment for having done something wrong
% of respondents who agreed or somewhat agreed
9
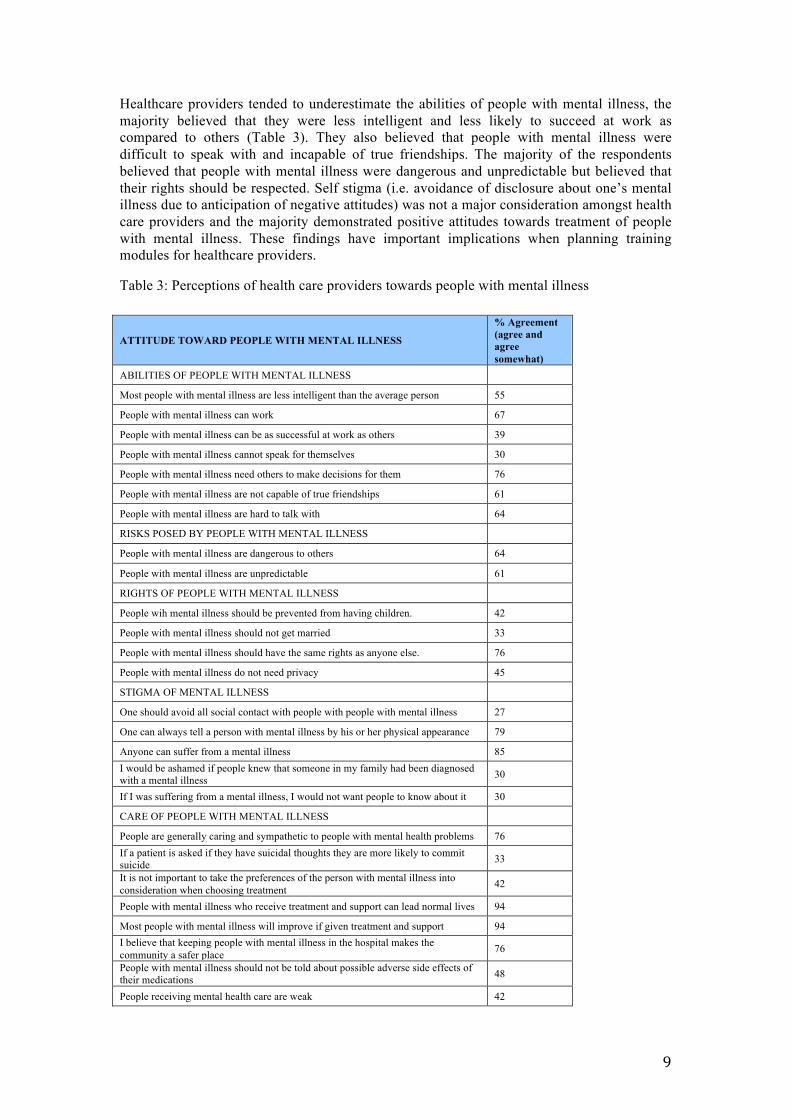
Healthcare providers tended to underestimate the abilities of people with mental illness, the majority believed that they were less intelligent and less likely to succeed at work as compared to others (Table 3). They also believed that people with mental illness were difficult to speak with and incapable of true friendships. The majority of the respondents believed that people with mental illness were dangerous and unpredictable but believed that their rights should be respected. Self stigma (i.e. avoidance of disclosure about one’s mental illness due to anticipation of negative attitudes) was not a major consideration amongst health care providers and the majority demonstrated positive attitudes towards treatment of people with mental illness. These findings have important implications when planning training modules for healthcare providers.
Table 3: Perceptions of health care providers towards people with mental illness
ATTITUDE TOWARD PEOPLE WITH MENTAL ILLNESS
% Agreement (agree and agree somewhat)
ABILITIES OF PEOPLE WITH MENTAL ILLNESS
Most people with mental illness are less intelligent than the average person 55
People with mental illness can work 67
People with mental illness can be as successful at work as others 39
People with mental illness cannot speak for themselves 30
People with mental illness need others to make decisions for them 76
People with mental illness are not capable of true friendships 61
People with mental illness are hard to talk with 64
RISKS POSED BY PEOPLE WITH MENTAL ILLNESS
People with mental illness are dangerous to others 64
People with mental illness are unpredictable 61
RIGHTS OF PEOPLE WITH MENTAL ILLNESS
People wih mental illness should be prevented from having children. 42
People with mental illness should not get married 33
People with mental illness should have the same rights as anyone else. 76
People with mental illness do not need privacy 45
STIGMA OF MENTAL ILLNESS
One should avoid all social contact with people with people with mental illness 27
One can always tell a person with mental illness by his or her physical appearance 79
Anyone can suffer from a mental illness 85 I would be ashamed if people knew that someone in my family had been diagnosed with a mental illness 30
If I was suffering from a mental illness, I would not want people to know about it 30
CARE OF PEOPLE WITH MENTAL ILLNESS
People are generally caring and sympathetic to people with mental health problems 76 If a patient is asked if they have suicidal thoughts they are more likely to commit suicide 33
It is not important to take the preferences of the person with mental illness into consideration when choosing treatment 42
People with mental illness who receive treatment and support can lead normal lives 94
Most people with mental illness will improve if given treatment and support 94 I believe that keeping people with mental illness in the hospital makes the community a safer place 76
People with mental illness should not be told about possible adverse side effects of their medications 48
People receiving mental health care are weak 42

10
People with mental illness can receive good care from a traditional healer 12
3.2 The Health System
3.2.1 General health services
South Sudan is acknowledged to have some of the worst health indicators in the world. The under-five infant mortality rate is 135.3 per 1,000, whilst maternal mortality is the highest in the world at 2,053.9 per 100,000 live births (Table 4). The epidemiology of HIV/AIDS in South Sudan is poorly documented but the prevalence is believed around 3.1%. South Sudan probably has the highest malaria burden in sub-Saharan Africa" and is one of the few countries where dracunculiasis (guinea worm disease) still occurs Table 4: Basic Health Data Health week 10 Cumulative* Number of medical interventions (whole country) 76,780 713,578 Number of people in need (whole country) 6,400,000 Number of people targetted (whole country) 3,400,000 Outpatient consultations conducted 74,018 615,094 Vaccination. Children 0-‐‑5 years protected against polio in round 3 SAID in 3 conflict affected areas
844,483
Reproductive health – women provided ANC services 2,452 27,343 Reproductive health – women with caesarian sections 31 411 People reached with GBV prevention messages Cholera suspected cases 9 52 Leishmaniasis cases 6 1025 Hepatitis E cases 2 6 Health Cluster as of 12th March 2015 *Cumulative figures are of 29 December 2014 South Sudan has 3 teaching hospitals, 7 state hospitals and 27 county hospitals. There are 792 Primary Health Care Units (PHCUs) and 284 Primary Health Care Centres (PHCCs) out of which 20% are not functional because of lack of skilled medical and health personnel. In addition, there are 10 private health facilities, 14 specialised facilities and 10 police/military health facilities International Medical Corps Sit analysis May 2013). On average, in rural areas, there are about 14,000 people per health unit and 75,000 per health center. There are about 400,000 people per hospital; a recent inventory of hospitals in South Sudan describes a heavy, largely derelict infrastructure9. Since the December 2013 conflict, a number of International organisations have begun providing health services to meet the growing need (Figure 2). Figure 2: Health Cluster Mapping in South Sudan (July 2014)
9 The Basic Package of Health and Nutrition in Primary Care. South Sudan, July 2011 (update)

11
3.2.2 Mental health services
In South Sudan, a country of some 11 million people, there are only two trained psychiatrists. "The scale of the problem is huge," says Dr Atong, one of those two, and the new head of mental health care in South Sudan. There is no psychiatric hospital in the country. There is one psychiatric inpatient and one outpatient department as part of the Juba Teaching Hospital. The capacity of the psychiatric department is 12 beds (Table 5). The Military Hospital in Juba provides counselling services to some patients with mental illness. People who suffer from mental illness are also put in in jail. From mid-2011 to mid-2012, 90 South Sudanese were in prison only because they appeared to have mental illness.10 The psychiatrist and psychiatric assistants from Juba teaching hospital conduct regular ‘ward reounds’ in the prison where patients may stay upto one month, ususally 1-2 weeks. This has been cited as a source of concern to human rights organisations.11 Table 5: Mental health facilites and resources in Juba (Source: International Medical Corps MH Situational Analysis May 2013) Staffing Psychiatrist Psychologists Social workers Other Juba Teaching Hospital Psychiatry ward, Juba
2 1 0 3 psychiatry medical assistants 2 counsellors 2 nurses (2 OPD, 6 IPD)
Training Trained in Tanzania and Kenya
Trained in Khartoum (MA in clinical psychology)
Specialist psychiatric medical assistant training in Khartoum. Occassional in-service training
Juba Military Hospital, Juba
0 3 counsellors 0
Training Training in psychology
10 Solomon Ehiemua. Mental Disorder: Mental Health remains an invisible problem in Africa. European Journal of Research and Reflection in Educational Sciences Vol. 2 No. 4, 2014 11 http://www.hrw.org/news/2012/06/21/south-‐‑sudan-‐‑arbitrary-‐‑detentions-‐‑dire-‐‑prison-‐‑conditions

12
While the MoH has begun mapping the mental health service providers in the country since early 2015, this information is not available to date. International Medical Corps mapping conducted during the rapid situational analysis (2013, 2014) and updated during the recent field visit (February 2015) are shown in Table 6, below. Table 6: Select NGOs involved in psychosocial activities in International Medical Corps field sites
Who What Where Handicap International Psychosocial sessions for persons with disability
Juba POC (Persons of Concern camps)
Oxfam Food security and livelihood Juba POCs UNMISS Provides inpatient support and medication for patients referred from
International Medical Corps PHC. Coordinates referral to MoH specialist in Malakal regional hospital
Malakal (Level 2 hospital)
ACTED (Agency for Technical Cooperation and Development)
WASH, SGBV in camps, Food Security and Livelihoods & Camp management
Juba POC Akobo Maban – Kaya, Gendrassa
IOM (International Organisation for Migration)
Registration/Verification of the affected populations; • Stand by teams to register new spontaneous and organized arrivals; • Information sharing
Juba POC Malakal
World Vision General food and blanket distribution & supplementary feeding
Juba POCs Malakal
MSF Inpatient hospital – medical - in Maban. Earlier providing MHPSS services in Gendrassa camp – the patients have now been handed over to International Medical Corps Inpatient hospital in Malakal with 1 psychologist and 2 counsellors – psychosocial activities for women and children admitted in the hospital. Community awareness about mental health
Maban – Batil, Malakal. Earlier, Awerial
Samaritan’s Purse Bunj County Hospital, Inpatient facility. Receives some patients with MI, Epilepsy. Has essential psychotropics
Maban, Bunj
DRC (Dutch Consortium for Rehabilitation)
Psychosocial support including child friendly spaces and women centers Works closely with ACTED. Prepared SOP for SGBV to which IMC will be a signatory
Maban, Malakal
LFW (Lutheran World federation)
Protection (women and children)
Maban
Relief International PHC and mobile units Maban – for the host population
Health Link (S. Sudan NGO)
Runs 2 inpatient health facilities handed over by MSF. Some basic psychosocial services. May have some meds – diazepam, amitriptyline
Awerial
International Red Cross GBV: Case Management and referral • Women and adolescent girls have safe access to psychosocial support activity, women empowerment activities, women’s network built to support each other and access important information and freely voice their concerns through the IRC women’s center. • Protection monitoring – Through out reach activities and risk assessments • Referral – Of people with specific needs (PSNs) to proper agencies • Case Management – Identification, referral/support, follow up • Information sharing - Provision of information about the services available in the camp
Awerial
CCM (Comitao Collaborative Medica)
Runs the PHC with MoH. Offer basic counseling to people in distress Awerial
Save the Children Education, Identification, registration, follow-up and tracing/reunification of separated or unaccompanied children • Child Protection Center (Child Friendly Space)
Akobo Awerial
Plan International (Supported by WFP)
Food distribution Psychosocial support integrated at the child friendly spaces
Akobo Awerial
Psychotropic medication availability: The South Sudan essential medicine list includes drugs for epilepsy and mental illness. However, only a limited number of psychotropic medications are available in the health facilites and their supply is inconsistent. Private pharmacies in Juba stock psychotropic

13
medication but this is expensive and beyond the reach of most people. The MoH too depends on donations from WHO and OVCI (Organismo di Volontariato per la Cooperazione Internazionale) to obtain psychotropics but this is provided only to Juba Teaching hospital and not in other parts of the country. This means that continuation of maintenance medicines is often not possible for patients from outside Juba. Currently, the MoH is trying to negotiate the price of drugs with the private pharmacies by reducing taxes. Specialist training: Opportunities for training in mental health are limited in South Sudan with no specialised training available in psychiatry, psychiatric nursing or psychology. Some health staff such as clinical officers at the Juba Teaching Hospital complete one month placements in the psychiatric department. There are plans to develop new course material in psychiatry to train medical doctors at the Juba Teaching Hospital.
Baseline Mental Health PHC Integration: survey results
A survey was conducted in 11 health facilities to assess mental health capacity and integration using the IMC MH PHC Integration checklist. The survey was conducted prior to the onset of training to reflect baseline information. Table 7 below provides details on the number of health facilities surveyed with the corresponding catchment population per facility type. All of these facilities shown in Figure 3 are supported by International Medical Corps in the current MHPSS program. Figure 3: International Medical Corps supported health facilites in 5 sites in South Sudan (marked with pink arrows)

14
Table 7. Details of health facilities surveyed
Site Health Facility Total Catchment Population
Average No. of Patients
Seen per Day
Staff details
Doctor Clinical
officer Nurse/
Nurse asst Midwife Social
worker/Psy-chologist
CHW Others
Juba POC
Inpatient facility 20,000 150 1 5 10 3 0? 6 4
PHC1 20,000 80 1 2 5 0 29
PHC2 2500 45 0 1 1 0 15
PHC3 20,000 220 1 1 0 2 11
Maban refugee camps
Kaya PHC 21,000 150 1 6 3 2 64
Gendrasa PHC 18,000 250 1 5 3 2
Malakal IDP camp
PHC1 17,000 70 1 2 5 1
PHC2 17,000 150 1 3 4
Awerial IDP camp
PHC1 12,743 80 1 2 3 2 3
PHC2 33,300 70 1 1 3
Akobo County Hospital 185,000 100 3 3 33 5 59 5
The average catchment population of the facilities is 33,322 (range: 2500-185,000) with an average of 124 (range: 45-250) patients visiting the outpatient clinics per day. Staff details: The number of staff in the health facilities varied. Table 7 shows the number of staff per type of health facility. Psychotropic medication availability: Table 8 below illustrates the availability of psychotropic medications Table 8. Availability of psychotropic medication (by site) in 11 International Medical Corps health facilities (10 PHCs and 1 County Hospital).
Basic Pharmacy Data Psychotropic Medications Facilities with available psychotropic medication in the
PHC clinic or nearby pharmacy in the previous week (by site) Juba Maban Malakal Aweria
l Akobo (county hospital)
Generic antidepressant medication (amitriptyline, fluoxetine)
Never Never Never Never Usually
Generic anti-anxiety medication (diazepam) Usually Never Usually Never Usually Generic anti-psychotic medication (haloperidol tab and injection, chlorpromazine, Thioridazine)
Never Never Never Never Usually
Generic anti-epileptic medication (phenobarbital carbamazepine, diazepam inj, valproic acid)
Never Never Usually Never Usually
Generic bipolar disorder medication (valproic acid, carbamazepine)
Never Never Never Never Never

15
Medication as part of substance use programs (nicotine replacement therapy)
Never Never Never Never Never
Generic antiparkinsonian medicine for the management of side effects from antipsychotic medication (biperiden)
Never Never Never Never Usually
Basic laboratory services: Laboratory services to support initiation and monitoring of some psychotropic medications are largely unavailable in the International Medical Corps supported health facilities (Table 9) Table 9: Laboratory services (by site) in 11 International Medical Corps primary health facilities. Laboratory services Juba Maban Malakal* Awerial** Akobo Complete blood count Referred to the Juba
Teaching Hospital or private lab outside the camp
X ✓ ✓ X
Liver Function test Referred to Juba Teaching Hospital
X ✓ X X
Thyroid Function test Referred to Juba Teaching Hospital
X X X X
Rapid blood glucose ✓ ✓ ✓ ✓ ✓ Toxicology screening test (urine) Referred to Juba Teaching
Hospital X ✓ X X
Creatinine clearance test Referred to Juba Teaching Hospital
X ✓ X X
Serum Lithium X X X X X *Laboratory services available at the UN hospital *Laboratory services available at the hospital run by Health Link Staff training and skills: Table 10 shows the number of staff who were provided in-service MH training. No PHC staff received in service mental health training and/or support supervision in all PHCs in Juba and Akobo County Hospital. None of the staff had heard of the mhGAP program and the guidelines. Several Doctors and Clinical Officers in camp clinics had completed their studies in neighboring countries such as Uganda, Ethiopia and Kenya. Several of them had received theoretical training on mental health and some have also completed clinical placements of one to three months in psychiatric facilities (e.g. Butabika mental hospital in Uganda, psychiatric unit at Juba teaching hospital). At the level of community response the community volunteers recruited by various agencies can be an important resource to strengthen the overall coping of the community with mental health issues and to provide assistance and emotional support. Community health workers working in Juba and Akobo did not receive any training related to MHPSS including psychological first aid (PFA). The exceptions to this are two counselors who had been working with MSF-B in Juba PoCs (Persons of Concern camps). The two counselors received training on basics of counseling by MSF?. In Malakal UNHCR and DRC recently began training of community mobilisers. International Medical Corps had trained community members in basic counseling skills and psychosocial support for its Nutrition and GBV program. In Maban, some staff had received prior training from MSF in PFA. Table 10. Staff training (by site) in 11 International Medical Corps health facilities (10 PHCs and 1 county hospital) prior to initiation of the MHPSS program Staff Training Indicators
Staff What % of this staff was trained? How many sessions of on the job supervision were provided?
% of staff trained No. of sites (N=5) % of supervisions No. of sites (N=5)
Doctor ⓪None (0%) ①Some (1-50%) ②Most (>50%)
2 3
⓪None (0) ①Some (1-‐‑2) ②Several(>3)
5

16
Clinical officer ⓪None (0%) ①Some (1-50%) ②Most (>50%)
2 3
⓪None (0) ①Some (1-‐‑2) ②Several(>3)
5
Nurse/nurse asst ⓪None (0%) ①Some (1-50%) ②Most (>50%)
3 2
⓪None (0) ①Some (1-‐‑2) ②Several(>3)
5
Midwife ⓪None (0%) ①Some (1-50%) ②Most (>50%)
5 ⓪None (0) ①Some (1-‐‑2) ②Several(>3)
5
Social Worker/psychologist
(Not applicable)
⓪None (0%) ①Some (1-50%) ②Most (>50%)
⓪None (0) ①Some (1-‐‑2) ②Several(>3)
CHW ⓪None (0%) ①Some (1-50%) ②Most (>50%)
4 1
⓪None (0) ①Some (1-‐‑2) ②Several(>3)
5
During the rapid assessment in Maban (May 2013), a questionnaire was administered on current practices in identifying and addressing priority mental and neurological problems among general health staff in International Medical Corps PHCC/PHCU facilities (5 Clinical Officers, two nurses, one midwife). Data showed that the staff were making efforts to address mental health problems encountered in clinical practice, especially non-specific somatic complaints. General health staff were already identifying and managing some people with mental illness. Staff at general health facilities in the camps and the referral hospital were asked how they identified and managed mental health cases. Their responses are presented in Table 11, below. Table 11: Ways of managing mental health problems at health facilities among general health care providers (PHCU, PHCC, hospital)
Medically unexplained somatic complaints/depression were most common and providers could not distinguish between both. Other mental disorders were detected only rarely and there was a wide variation across camps (which could be due to different diagnostic skills of healthcare providers) and over time. General health staff at PHCU clinics reported that they
Mental health related problem
Reported Signs Psychosocial Intervention Pharmacological Intervention
Unexplained somatic complaints and depression with somatic elements
Somatic complaints such as not being able to sleep, dizziness, headache, general body pain, leg pain, patients say they have fever (but do not), joint pain (many come two days later with another problem)
Giving advice (e.g. explaining that medication is not the solution, that there is no physical problem), talking about stressors (e.g. lost property)
Antihistamine (for sleep/side effect), pain medication (e.g. paracetamol), folic acid (if indicated)
Depression Insomnia, loss of appetite, signs of stress General counseling Treat with diazepam and multi-vitamins
Insomnia Being unable to sleep Asking about current stressors (e.g. problems with husband), providing re-assurance, advising to “take it easy”
None
Psychotic disorders Talking alone, shouting, running off PHCC/PHCU: Talking to them, giving needed items such as mosquito net, piece of clothing (and refer)
Regional hospital: inpatient admission, giving drugs (diazepam) to calm down
Epilepsy Convulsions None Treat with Phenobarbitol (if available)
Inpatient admission and diazepam
Developmental disorders
Slow development Giving nutrition advice N/A

17
do not see people with psychotic disorders at health facilities but that they do see them in the market and around the clinic. Pharmacological management for mental health problems was often not consistent with global guidelines. Some psychosocial management such as addressing current psychosocial stressors is consistent with mhGAP. However, staff could benefit from learning about the range of psychosocial (and pharmacological if appropriate) brief interventions in the mhGAP guide (especially for non-specific somatic complaints, depression and intellectual disabilities). General health staff with previous mental health training reported using their skills when counseling patients but also noted that patients with mental disorders are often not identified or not accessing health facilities. They noted that community awareness raising and a referral system would be needed. In terms of staff roles and team work, in none of the 11 facilities did the staff have defined roles in identification, management and referral of mental disorders nor did discussion of MH cases take place. Referral from general health care to mental health services: General health clinics within the camps in Maban reported referring people with severe mental health problems to the Bunj Hospital where some psychotropic medication is available and patients are kept for a short time as inpatients. In the Juba camps, referrals were made to the Juba teaching hospital and in Malakal to the UN hospital. None of the other sites had referral options for patients with mental illness. Referral from general health care to other services: Referrals are made by general health care providers for GBV, general protection, child protection to International NGOs ie. IRC, DRC, and UNHCR. Only very few health care providers reported having referral links with other agencies. Children with intellectual disabilities and people in need of physical rehabilitation are at times referred to Handicap International. Health Information System (HIS) reporting: HIS reporting to UNHCR occurs at all camp health facilities. UNHCR has one category for mental health and neurological conditions, which is broken down into seven sub-categories and which are used globally by UNHCR and other agencies. Some health facilities including International Medical Corps were reporting under one category of “mental illness or distress” but this was done in an inconsistent manner.
3.3 Mental Health Needs
3.3.1 Prevalence of mental health problems and psychological distress
The World Health Organization estimates that in humanitarian emergencies, the percentage of people with common mental disorders such as depression or anxiety disorders can double from a baseline of 10% to about 20%, while severe mental disorders such as psychotic disorders, which are more rare, can increase by 1% over the baseline of 2–3%.12 In addition, persons who are marginalized and with various disabilities (people with hearing, visual and movement disabilities, with intellectual impairment and with epilepsy) are often neglected or have no caregivers, and/or lack access to services. The Health Cluster Bulletin (December 2014) while identifying the need for mental health services states that 30% to 50% of total outpatient consultations in the Malakal PoC and Mingkaman IDP camp consist of people with mental health problems. There are also concerns that there may be under-reporting of people with mental illness either due to lack of
12 World Health Organization & United Nations High Commissioner for Refugees (2012). Assessing Mental Health and Psychosocial Needs and Resources: Toolkit for Major Humanitarian Settings. Geneva: WHO, 2012.

18
identification by health facility staff or failure to seek help by patients/families13. This is illustrated in the following observation made by one of the International NGO staff in Awerial; “Mental health is the Hippopotamus in the water” - what is seen is only a small part of what is really there. For e.g. one woman committed suicide and only after that did people say she had a mental problem. People don’t recognize that such people need medical attention.
While mental health data from South Sudan is limited, one post-conflict study from Juba found that 36% of the sampled population (n=1242) met criteria for post-traumatic stress disorder (PTSD) and 50% for depression14. The multivariate logistic regression analysis showed strong associations of gender, marital status, forced displacement, and trauma exposure with outcomes of PTSD and depression. Men, IDPs, and refugees and persons displaced more than once were all significantly more likely to have experienced eight or more traumatic events. A study, conducted in northern Uganda and South Sudan, found the prevalence of PTSD was 46% among South Sudanese refugees and 48% among South Sudanese who stayed in the country15. Another study that combined data from rural and urban settings and used diagnostic interviews (rather than only symptom rating scales) PTSD only was found in 331 (28%) and depression only in 75 (6.4%) of the study population. One hundred and twelve (9.5%) of the participants had PTSD-depression comorbid diagnosis. Exposure to traumatic events and socioeconomic disadvantage were significantly associated with having PTSD or PTSD-depression comorbidity but not with depression. Participants with a comorbid condition were more likely to be socioeconomic disadvantaged, have experienced more traumatic events, and showed higher level of psychological distress (PD) than participants with PTSD or depression alone.16 The estimated rates of generalized anxiety disorder (GAD)-only and PD-only (without comorbidity with PTSD) were 5.5% and 3.1%, respectively. Exposure to traumatic events and socio-economic disadvantage were significantly associated with having one or more anxiety diagnoses. After controlling for age, sex, rural/urban setting, and socio-economic disadvantage, exposure to trauma was independently associated with anxiety diagnosis. There were gender differences in the pattern of risk factors for having PTSD, GAD or PD17. Anxiety, substance abuse, and substance abuse-related complications such as alcohol withdrawal are also frequently seen in post-conflict settings18. Alcohol and drug abuse is a growing concern in South Sudan as increasing social freedom and access to alcohol and drugs bring increased risk for excessive use and harmful consequences19. These studies indicate a high prevalence of mental illness in South Sudan as well as the potential for an increase in psychiatric disease as more refugees and internally displaced persons return home20.
3.3.2 Psychosocial issues
13 South Sudan Cluster Bulletin #34. 21st December 2014 14 Roberts B, Damundu EY, Lomoro O, Sondorp E. Post-conflict mental health needs: a cross-sectional survey of trauma, depression and associated factors in Juba, Southern Sudan. BMC Psychiatry. 2009; 9: 7. 15 Karunakara UK, Neuner F, Schauer M, Singh K, Hill K, Elbert T, et al. Traumatic events and symptoms of post-traumatic stress disorder amongst Sudanese nationals, refugees and Ugandans in the West Nile. Afr Health Sci. 2004; 4(2): 83-93. 16 Ayazi et al. What are the risk factors for the comorbidity of posttraumatic stress disorder and depression in a war-affected population? a cross-sectional community study in South Sudan BMC Psychiatry 2012, 12:175 17 Ayazi et al. Association between exposure to traumatic events and anxiety disorders in a post-conflict setting: a cross-sectional community study in South Sudan BMC Psychiatry 2014, 14:6 18 de Jong JT, Komproe IH, Van Ommeren M. Common mental disorders in postconflict settings. Lancet. 2003; 361(9375): 2128-30. 19 King. Alcohol a Growing Problem in South Sudan. Voice of America. 2006. 20 Post-Conflict Mental Health in South Sudan: Overview of Common Psychiatric Disorders. Maithri Ameresekere, MD, MSca and David C. Henderson, Mda. This document was originally published in two parts the South Sudan Medical Journal in volume 5 number 1 and number 2.

19
On collation of information that was reported in the International Medical Corps rapid assessments (Maban, 2013, Awerial and Malakal 2014) and collected during the field visit (February 2015; interviews with 13 PHC staff in Juba, Maban, Malakal, Awerial; 1 FGD with 13 community health workers in Malakal), the following stressful circumstances were cited as most common and can increase the risk of developing mental health problems:
• Loss of loved ones: Having family members killed as a result of the violence or death of family members due to physical illness.
• Conflict and violence: domestic violence, cattle raiding, tribal conflict, past experience of violence or armed conflict, killing or torture of children
• Protection issues: kidnapping of children, orphaned children due to violence, early marriage
• Health/GBV issues: spread of STDs • Environmental issues: Overcrowding, food insecurity, risk of floods
In addition, refugees reported a range of problems in their daily lives that impact their mental health (Table 12): Table 12: Psychosocial problems identified by people residing in the refugee/IDP camps21
• Physical health (e.g. Sickness, Diarrhea, Eye problems, dizziness from heat, back pain from grinding)
• Available Medical treatment (e.g. People at the health center give tablets without examining what the problem is, at home injections and syrup for children were available but not here (children throw up pills))
• Food and Nutrition (e.g. lack of tea, coffee sugar, salt, and milk, green vegetables, only sorghum and lentils available, no balanced diet, supplementary food only available for children under 5, low quality supplementary food)
• Food preparation (e.g. Sorghum available but nothing to grind it (only few grinding machines are available), would need seeds for vegetables (before rainy season), no place to dig and plant)
• Shelter (e.g. tents are hot and wearing out, grass houses would be better but they have to pay to cut the grass or the host community chases them off the land)
• Weather (e.g. heat (different from what they are used to, tents are hot inside), changes in weather)
• Insects (e.g. too many flies, not enough mosquito nets)
• Education (e.g. Education for children is not up to date, both children and adults need education, not enough teachers, teachers are not qualified enough)
• Economic (e.g. no employment available) • WASH (e.g. It takes time to get to water points, water
tables are low, not enough soap available (only 2 pieces per person per month))
• NFIs (e.g. no flashlights (only torch at night, can be dangerous and burn tent), no clothes (some people have to walk around without clothes), no utensils for cooking, no saucepans and cups for tea, lack of clothes (often people can not go out, they have to wait for someone else to come back to wear their clothes), host community does not allow to collect firewood
Psychosocial Related Concerns • Child Development (e.g. Delayed development among
children) • Lack of engagement in meaning ful activties (e.g. many
refugees are skilled and educated but they are idle) • Problems with the host community (e.g. lack of
cooperation with the host community, refugees are blamed for robberies by host community leading to frequent violent confrontations)
Vulnerable groups • People with disabilities (e.g. visually impaired, amputated) • Separated children • People who have no relatives or others to support them. E.g. Women who do not have husbands (they may have died or
have left the family to join the rebellion) 3.4 Anticipated challenges in mental health PHC integration General health care staff at health facilities (n=13) and program managers (n=9) were asked about anticipated needs and challenges for mental health PHC integration during the field visit (February 2015). These results along with data presented in the earlier rapid assessment (Maban 2013) are summarized below. Challenges were mainly in the areas of limited human and material (medication, laboratory facilities, etc) resources, lack of community awareness
21 Rapid Mental Health Situational Analysis, International Medical Corps , Maban, 2013

20
and absence of national legal frameworks. Needs identified were that of comprehensive services including inpatient care and follow up services as well as referral pathways. Psychotropic Medication:
• Availability of psychotropic medication that is affordable and ensuring continued supply
• Availability of better drugs (that are not part of WHO essential drug list)
Laboratory services
• Availability of lab services to monitor psychotropic medication including materials as well as trained personel
Case Finding:
• Increased awareness in the community about mental health
• Stigma prevents help seeking for people with mental illness
Overall system/law
• Need to find out how to work within law of South Sudan (e.g. involuntary admission, protection), no structures in place
• Community beliefs and practices
• People go to traditional healer instead of health facility
• Community believes in injectable drugs (and syrups for children), not in counseling
• Social/community support for people with mental illness very limited
Staff well being
• Staff well being /MHPSS services for staff are needed
Security concerns
• This limits staff and patient mobility
Coordination • Many different organisations involved in
psychosocial services with poor coordination between them
Follow up at community level
• Needed to make sure no danger • Needed to make sure that family and
community accepts them • Stigma attached to mental illness, need to
ensure community acceptance • MH patients need social structure (medication
alone is not enough) • Needed to ensure drug compliance • Need to make sure person comes back
Staff capacity/training
• Limited capacity and large turnover of staff. • No/minimal prior training in mental health • Training of individuals whose contracts are short
Staffing/time
• Staffing might not be enough for the amount of people in the camp
• Community health workers have multiple responsibilities in addition to mental health
Inpatient services
• Patients may need inpatient admission. These resources are limited
Referral
• Referral forms are needed for partners • Need to establish referral mechanism with
community • Need to identify people within community • There could be referral links to schools and
teachers could be trained to identify and refer • Population movement means people need to be
referred to services at their place of return Sustainability of services
• Depends on donor funds and these are mainly given for short periods
• Lack of government health services to sustain programs
This situational analysis provides important guidance for project implementation and expansion including local concepts of mental illness, coping and help seeking behaviors and available mental health services. Based on this, recommendations for International Medical Corps’ MHPSS program which began in August 2014 are outlined below:
Coordination and advocacy
International Medical Corps’ is an active member of the MHPSS platform organized by the MoH to bring together the different organisations involved in MHPSS activities at the national level. Further recommendations:
4. Summary and Recommendations

21
• It is important to explore strategies that can be implemented to strengthen collaboration with MoH and government care providers to build local capacity. This may include application to alternate sources of funding to support collaborative training programs. International Medical Corps will need to also coordinate and communicate with other national and global stakeholders and national authorities in developing the curriculum for training general health workers in mental health and share experiences and results from its own mhGAP training program.
• Continued involvement with the MHPSS cluster to advocate for improving mental health care in the region and strengthen referral mechanisms.
• Support PHC teams to collect and report clinical data in standardized forms including patient outcome data, details of referrals, etc.
• Take steps to identify and overcome the challenges in medication supply. This may include support to PHC teams to record and report psychotropic drug use in order to access medication through international procurement well in advance. Also, close follow up by the IMC Juba team is crucial to ensure medicines are delivered to the field in a timely manner, anticipating the various logistical challenges this may encounter. Explore alternate sources to cover medication supply in the interim such as the MoH and WHO to obtain essential medicines and other partner organisations (for example, the MSF inpatient facility in Malakal has stock of some psychotropic medicines which they do not use. A formal request for donation of this stock could be made to cover any shortfall in International Medical Corps stocks).
Mental health training and supervision
International Medical Corps’ MHPSS program has been providing training in assessment and management of priority mental health conditions to health facility service providers (PHCUs, PHCCs) based on the mhGAP IG adapted to the region. Based on this situational analysis, the following points need emphasis:
• Staff at health facilities are currently able to identify a very small number of people with mental illness. Staff (doctors, clinical officers, nurses, midwifes) could benefit from learning a few basic screening questions for mental health related problems. This would also facilitate better-targeted referrals for mental health problems and more accurate reporting for UNHCR HIS mental health categories. International Medical Corps can focus on health facility staff in International Medical Corps clinics first and could consider expansion to other health facility staff as a second step if resources are available such as health facility staff from the regional hospital (e.g. Bunj).
• In view of the rapid staff turnover, it is important to schedule frequent training workshops in all sites to ensure a critical number of trained staff are present in all the health facilities.
• The unstable security situation may mean that all staff cannot travel to a common training venue. This will require planning for additional resources to support multiple training programs in different sites. Gradually building the capacity of select trained staff who can then facilitate training of other/new staff may be one method of doing this.
• Program trainers will need to ensure close on-the-job supervision of the PHC staff. This is best done in person, however, if this is difficult, they can plan regular supervision of trained PHC teams through mechanisms such as skype/telephone calls. Regular (weekly/fortnightly) case discussions/short online training sessions with PHC staff can also be planned.
• Training of community health workers in conducting awareness programs and providing psychological first aid can be initially done by the program trainers/specialists using the mhGAP material. In due course, the CHWs can be supported by a trained PHC staff.

22
Mental health service provision
International Medical Corps has begun to integrate MHPSS services within its general health care programs in all 5 program sites – Juba POC, Maban, Malakal, Awerial and Akobo. This will be described in the subsequent case study, however, based on this baseline situational analysis, it is recommended that:
• Interventions should address access to other services and supports (e.g. medical, protection), promote social inclusion and facilitate patients taking on daily tasks and family roles as they recover. Patients with acute mental health symptoms (e.g. acute psychosis) should be managed within their family environment and visited by a health service provider on a daily basis for at least the first 1-2 weeks as appropriate.
• Local community mental health workers (from refugee and host communities) have the capacity to play an important role in community outreach, following up with patients (e.g. ensuring medication compliance), psycho-education and mental health promotion and messaging. They can also assist in providing several of the recommended psychosocial interventions in the WHO mhGAP and can engage in basic mental health case management functions such as helping link people to service providers and community supports. A structured plan for involvement of CHWs including awareness activities, group psychosocial activities etc will be useful and ensure uniformity of activities across the different program sites.
Referral
• Build cross referral networks with various other formal and informal service providers. Referral networks for people with mental illness should be broadened from general health facilities and some community leaders to also include a higher number of implementing agencies and facilities and community providers. Community leaders also play important roles in the camps. The community structure among refugees is structured around sheiks who are village leaders and typically responsible for about 500 to 700 people. They can play an especially important role in identifying people with severe mental disorders in their communities. Other agencies and implementing partners in the camps provide important services, which are also relevant for people with mental disorders and their families (e.g. protection, shelter, rehabilitation, etc.) and links to such services should be strengthened. IMC could consider strengthening mental health case coordination by supporting the development and use of common referral forms and the mapping of MHPSS and protection services
• Improve case identification and access for people with severe mental disorders such as psychosis and neurological disorders (epilepsy). Persons with severe or chronic mental illness and their families may seek out traditional healers rather than the health facilities Potentially effective strategies include engaging community leaders such as sheiks, and building links with traditional healers. IMC can work through CHWs and mental health community outreach workers on awareness raising.
Mental health promotion
• Engage people in the camp (especially those experiencing psychological distress and mental health problems) in meaningful structured psychosocial activities. Community discussions showed that loss of resources and belongings are a significant stressor for many refugees, which can increase the risk for common mental disorders such as depression (possibly referring to the local concept of “thinking too much”). IMC can consider structured social, educational and recreational activities for youth and adults in the camp. Other International Medical Corps psychosocial programs for refugees have included activities led by refugee instructors such as cooking together, weaving baskets and mats, sharing daycare responsibilities, sports activities, music and dance. Those

23
activities should include and prioritize people experiencing mental health problems and psychological distress.
• Engage refugees and people from the host community in joint purposeful activities • Tensions with the host community contribute to limited access to resources (e.g. grass,
firewood) and psychological distress. Research suggests that resource conflicts and tensions can be addressed by having people from different groups work on common goals that can benefit all (e.g. building something that benefits both communities). Other International Medical Corps psychosocial programs have engaged refugee and host population youth for example in working together on joint community projects and learning about life skills.
• Development of IEC material that is contextually relevant will be useful in awareness raising as well as self help techniques to deal with stress. This can be adapted from International Medical Corps IEC material being used in other MHPSS programs

24
Appendix A
Situational Analysis Information Framework and Data Sources
1. The
Environment
1.1 Location and
physical setting
Desk top review
• Alex de Waal. When Kleptocracy Becomes Insolvent: Brute Causes Of The Civil War In South Sudan. African Affairs, 2014, 113/452, 347–369. Downloaded from http://afraf.oxfordjournals.org/
• Wikipedia: http://en.wikipedia.org/wiki/South_Sudan • Mental Health in Health Facilities, International Medical Corps
South Sudan, May 2013
1.2
Socioeconomic profile
Desk top review
• The United Nations Office for the Coordination of Humanitarian Affairs (OCHA) South Sudan: Crisis Situation Report No.78 (as of 12 March 2015).
1.3
Socio-Political environment
Desk top review
• The Basic Package of Health and Nutrition in Primary Care. South Sudan, July 2011 (update)
• Mental Health in Health Facilities, International Medical Corps South Sudan, May 2013
• Terms of reference for psycho-social support and mental health lead organizations in South Sudan. Drafted by the Mental Health Working Group. December 2013
1.4 Socio-cultural
attitudes towards
mentally ill
1.41 Perception of community members
• WHO AIMS report on mental health system in South Sudan. 2009 • Four FGDs with 63 respondents in International Medical Corps
field sites • Rapid Mental Health Situational Analysis, Maban Refugee Camps,
South Sudan, International Medical Corps. April 2013 • Tempany M. What research tells us about the mental health and
psychosocial wellbeing of Sudanese refugees: a literature review. Transcult Psychiatry. 2009; 46(2): 300-15.
1.42 Perception of healthcare providers
• Knowledge and Attitude survey with 33 respondents from International Medical Corps supported PHCs
2. The Health System
2.1 General health
services
Desk top review
• Health Cluster report. March 2015 • The Basic Package of Health and Nutrition in Primary Care. South
Sudan, July 2011 (update)
2.2 Mental health
services
Desk top reviews
• Solomon Ehiemua. Mental Disorder: Mental Health remains an invisible problem in Africa. European Journal of Research and Reflection in Educational Sciences Vol. 2 No. 4, 2014
• http://www.hrw.org/news/2012/06/21/south‐sudan‐arbitrary‐detentions‐dire‐prison‐conditions
• International Medical Corps MH Situational Analysis May 2013 • Rapid Mental Health Situational Analysis, Maban Refugee Camps,
South Sudan, International Medical Corps. April 2013 • Rapid Mental health Assessment: Akobo and Juba, International
Medical Corps, August 2014 • Rapid Mental Health Siutuational Analysis: Awerial and Malakal,
Feb 2014
Interviews
• Baseline PHC Integration checklist administered in 11 health facilities
• Interviews with MoH Psychiatrist, program staff in field sites, representatives from partner NGOs
3. Mental
Health Needs
Desk top reviews
• World Health Organization & United Nations High Commissioner for Refugees (2012). Assessing Mental Health and Psychosocial Needs and Resources: Toolkit for Major Humanitarian Settings. Geneva: WHO, 2012.
• South Sudan Cluster Bulletin #34. 21st December 2014 • International Medical Corps MH Situational Analysis May 2013 • Rapid Mental Health Situational Analysis, Maban Refugee Camps,
South Sudan, International Medical Corps. April 2013

25
• Rapid Mental health Assessment: Akobo and Juba, International Medical Corps, August 2014
• Rapid Mental Health Siutuational Analysis: Awerial and Malakal, Feb 2014
• Roberts B, Damundu EY, Lomoro O, Sondorp E. Post-conflict mental health needs: a cross-sectional survey of trauma, depression and associated factors in Juba, Southern Sudan. BMC Psychiatry. 2009; 9: 7.
• Karunakara UK, Neuner F, Schauer M, Singh K, Hill K, Elbert T, et al. Traumatic events and symptoms of post-traumatic stress disorder amongst Sudanese nationals, refugees and Ugandans in the West Nile. Afr Health Sci. 2004; 4(2): 83-93
• Ayazi et al. What are the risk factors for the comorbidity of posttraumatic stress disorder and depression in a war-affected population? a cross-sectional community study in South Sudan BMC Psychiatry 2012, 12:175
• Ayazi et al. Association between exposure to traumatic events and anxiety disorders in a post-conflict setting: a cross-sectional community study in South Sudan BMC Psychiatry 2014, 14:6
• de Jong JT, Komproe IH, Van Ommeren M. Common mental disorders in postconflict settings. Lancet. 2003; 361(9375): 2128-30.
• King. Alcohol a Growing Problem in South Sudan. Voice of America. 2006.
• Post-Conflict Mental Health in South Sudan: Overview of Common Psychiatric Disorders. Maithri Ameresekere, MD, MSca and David C. Henderson, Mda. (This document was originally published in two parts the South Sudan Medical Journal in volume 5 number 1 and number 2).
Interviews • Interviews with program staff, community members,
representatives from MoH and partner NGOs

26
Appendix B
International Medical Corps MHPSS Situational Analysis Tool Informed consent obtained: Yes/No Name of interviewer: Date: Interviewee Name: Interviewee No: Key informant type (e.g. religious leader etc.): Gender of participant: O Male O Female Age: 1) Local concepts of mental health and psychosocial problems 1.1.How would I as an outsider recognize a person with mental health problems?
1.2.How would I as an outsider recognize a person who is emotionally upset?
2. Impact of mental illness Type of mental health or psychosocial problem
Impact
3. Coping and support Type of mental health or psychosocial problem
Coping method Helpful?
Yes/No Yes/No Yes/No Yes/No Yes/No Yes/No Yes/No Yes/No
4. Local attitudes and practices towards people with mental illness 4.1) What do people in the community think about those with mental illness?

27
4.2) How do people in the community treat people with mental illness? 5. Local help seeking behaviours Where do people with mental health problems seek help? 6. Knowledge of referral pathways If you knew someone with mental illness in this community, where will you send them?
28
Appendix C
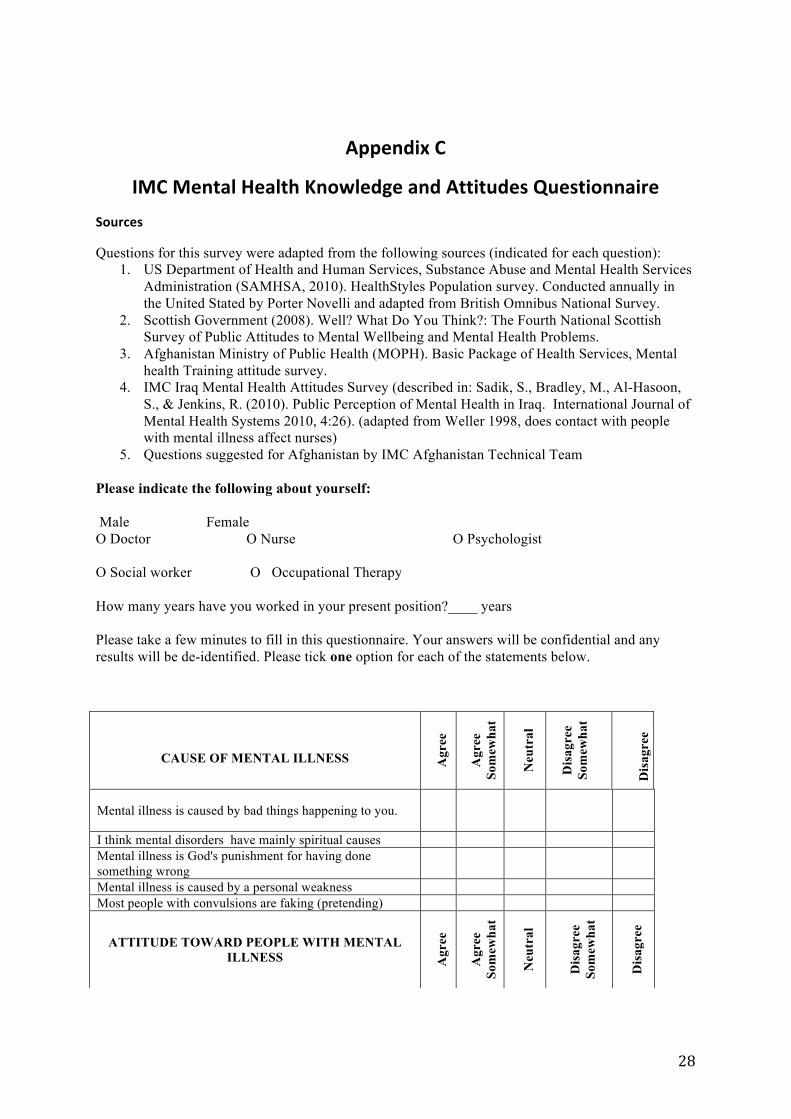
IMC Mental Health Knowledge and Attitudes Questionnaire Sources
Questions for this survey were adapted from the following sources (indicated for each question): 1. US Department of Health and Human Services, Substance Abuse and Mental Health Services
Administration (SAMHSA, 2010). HealthStyles Population survey. Conducted annually in the United Stated by Porter Novelli and adapted from British Omnibus National Survey.
2. Scottish Government (2008). Well? What Do You Think?: The Fourth National Scottish Survey of Public Attitudes to Mental Wellbeing and Mental Health Problems.
3. Afghanistan Ministry of Public Health (MOPH). Basic Package of Health Services, Mental health Training attitude survey.
4. IMC Iraq Mental Health Attitudes Survey (described in: Sadik, S., Bradley, M., Al-Hasoon, S., & Jenkins, R. (2010). Public Perception of Mental Health in Iraq. International Journal of Mental Health Systems 2010, 4:26). (adapted from Weller 1998, does contact with people with mental illness affect nurses)
5. Questions suggested for Afghanistan by IMC Afghanistan Technical Team Please indicate the following about yourself: Male Female O Doctor O Nurse O Psychologist O Social worker O Occupational Therapy How many years have you worked in your present position?____ years Please take a few minutes to fill in this questionnaire. Your answers will be confidential and any results will be de-identified. Please tick one option for each of the statements below.
CAUSE OF MENTAL ILLNESS
Agr
ee
Agr
ee
Som
ewha
t
Neu
tral
Dis
agre
e So
mew
hat
D
isag
ree
Mental illness is caused by bad things happening to you.
I think mental disorders have mainly spiritual causes Mental illness is God's punishment for having done something wrong
Mental illness is caused by a personal weakness Most people with convulsions are faking (pretending)
ATTITUDE TOWARD PEOPLE WITH MENTAL
ILLNESS
Agr
ee
Agr
ee
Som
ewha
t
Neu
tral
Dis
agre
e So
mew
hat
Dis
agre
e

29
People with mental health problems are largely to blame for their own condition.
One can always tell a mentally ill person by his or her physical appearance.
Mentally ill persons are not capable of true friendships.
Most mentally ill persons are less intelligent than the average person.
Mentally ill people do not need privacy.
Mentally ill persons can work.
People with mental illness are dangerous to others
People with mental illness are unpredictable People with mental illness are hard to talk with
Anyone can suffer from a mental illness. People are generally caring and sympathetic to people with mental health problems
Mentally ill persons should be prevented from having children.
Mentally ill persons should not get married.
One should avoid all social contact with people with mental illness persons
Mentally ill people cannot speak for themselves People with mental illness should have the same rights as anyone else
People with mental illness need others to make decisions for them
People with mental illness should not be told about possible adverse side effects of their medications
It is not important to take the preferences of the person with mental disorder into consideration when choosing treatment
If a patient is asked if they have suicidal thoughts they are more likely to commit suicide
I would be ashamed if people knew that someone in my family had been diagnosed with a mental illness.
If I was suffering from a mental illness, I would not want people to know about it.
People with mental illness who receive treatment and support can lead normal lives
People with mental illness be as successful at work as others
Most people with mental illness will improve if given treatment and support.
I believe that keeping people with mental illness in the hospital makes the community a safer place
People receiving mental health care are weak People with mental illness can receive good care from a traditional healer
If I was concerned about a mental health issue with a

30
member of my family I would feel comfortable sending them to _____________________________

31
Appendix D
International Medical Corps PHC MH Integration Checklist Adapted from WHO MHPSS Assessment Toolkit (Draft Feb 2012)
Appendix D. BASELINE DATA collected from PHC Manager of each clinic participating in
training. Name of Interviewer: Date: Duration: Name of PHC clinic: Affiliation (e.g. MoH): Name & Title of Contact: Address: I. Basic Clinic Information Location: □ [Name of Area 1] □ [Name of Area 2] □ [Name of Area 3] □ [Name of Area 4] Catchment Population: Average number of patients visiting per day (past month): Staff Providing initial consultation: O Nurse O GP OOther:______________ II. Clinic Indicators Indicator Scoring: ⓪ Indicator not met ① Indicator partially met ② Indicator met 1. Clinic Staff Number and type of staff
Male Fem Average clinical
hours/day
Average # of patients seen/day
Average time (minutes) spent with patient
GPs ⓪ <5 ② 5-20 ②>20 Nurses ⓪ <5 ② 5-20 ②>20
Midwives ⓪ <5 ② 5-20 ②>20 Social Worker ⓪ <5 ② 5-20 ②>20 Psychologist ⓪ <5 ② 5-20 ②>20 CHWs ⓪ <5 ② 5-20 ②>20 Other (if involved in clinical services:)
⓪ <5 ② 5-20 ②>20
1. Average Score (sum/total # scored) ( )
2. Basic Pharmacy Data

32
Medication (please circle types available) Availability in the PHC clinic or nearby pharmacy in the previous week
Generic antidepressant medication (amitriptyline, fluoxetine)
⓪Never or rarely ①Sometimes ②Usually or always
Generic anti-anxiety medication (diazepam) ⓪Never ①Sometimes ②Usually Generic anti-psychotic medication (haloperidol tab and inj, chlorpromazine, Thioridazine)
⓪Never ①Sometimes ②Usually
Generic anti-epileptic medication (phenobarbital carbamazepine, diazepam inj, valproic acid)
⓪Never ①Sometimes ②Usually
Generic bipolar disorder medication (valproic acid, carbamazepine)
⓪Never ①Sometimes ②Usually
Medication as part of substance use programs (nicotine replacement therapy)
⓪Never ①Sometimes ②Usually
Generic antiparkinsonian medicine for the management of side effects from antipsychotic medication (biperiden)
⓪Never ①Sometimes ②Usually
2. Average Score (sum/total # scored) ( ) 3. Staff Training Indicators Training conducted
Staff
What % of this staff was trained?
How many hours of training was provided?
How many sessions of on the job supervision were provided?
Prior to IMC training, the following staff received in-service mental health training
GPs ⓪None (0%) ①Some (1-50%) ②Most (>50%)
⓪None ①Some (1-2) ②Several (>3)
Nurses ⓪None (0%) ①Some (1-50%) ②Most (>50%)
⓪None ①Some (1-2) ②Several (>3)
Midwife ⓪None (0%) ①Some (1-50%) ②Most (>50%)
⓪None ①Some (1-2) ②Several (>3)
Social Worker
⓪None (0%) ①Some (1-50%) ②Most (>50%)
⓪None ①Some (1-2) ②Several (>3)
Psychologist
⓪None (0%) ①Some (1-50%) ②Most (>50%)
⓪None ①Some (1-2) ②Several (>3)
CHW ⓪None (0%) ①Some (1-50%) ②Most (>50%)
⓪None ①Some (1-2) ②Several (>3)
3. Average Score (sum/total # scored)
3a ( ) 3b ( )
4. Staff Skills Indicators

33
At least one health care provider in the clinic is trained in…
If yes, specify how often trained staff uses skills:
⓪ Rarely/Never ① Sometimes ② Frequently
Assessment and management of mental disorders
Assessment of people with mental health problems ⓪ No
② Yes Clinical history taking Mental Status Exam
⓪ R/N ① S ② F ⓪ R/N ① S ② F
Management of depression ⓪ No ② Yes
Pharmacological Non-pharmacological
⓪ R/N ① S ② F ⓪ R/N ① S ② F
Management of psychosis ⓪ No ② Yes
Pharmacological Non-pharmacological
⓪ R/N ① S ② F ⓪ R/N ① S ② F
Management of bipolar disorder ⓪ No ② Yes
Pharmacological Non-pharmacological
⓪ R/N ① S ② F ⓪ R/N ① S ② F
Management of epilepsy/seizures ⓪ No
② Yes Pharmacological Non-pharmacological
⓪ R/N ① S ② F ⓪ R/N ① S ② F
Management of developmental disorders (intellectual disability) ⓪ No
② Yes Pharmacological Non-pharmacological
⓪ R/N ① S ② F ⓪ R/N ① S ② F
Management of child behavioral disorders (ADHD, conduct)
⓪ No ② Yes
Pharmacological Non-pharmacological
⓪ R/N ① S ② F ⓪ R/N ① S ② F
Management of Dementia ⓪ No ② Yes
Pharmacological Non-pharmacological
⓪ R/N ① S ② F ⓪ R/N ① S ② F
Management of alcohol and drug use disorders ⓪ No
② Yes Pharmacological Non-pharmacological
⓪ R/N ① S ② F ⓪ R/N ① S ② F
Assessment & management of self-harm/suicide ⓪ No
② Yes Risk Assessment Management
⓪ R/N ① S ② F ⓪ R/N ① S ② F
Management of anxiety / stress related disorders (e.g. PTSD) ⓪ No
② Yes Pharmacological Non-pharmacological
⓪ R/N ① S ② F ⓪ R/N ① S ② F
4. Average Score =(sum/total # scored)
4a ( ) 4b ( )

34
Most (50%) health stay are trained in… Communication skills specific to mental illness (e.g. active listening, respectful attitude)
⓪ No ② Yes
Communicating with angry, very anxious, or withdrawn patients ⓪ No ② Yes
The different ways in which people in the area express psychological distress
⓪ No ② Yes
Non-pharmacological management of medically unexplained somatic complaints
⓪ No ② Yes
Giving bad news in a supportive way ⓪ No ② Yes
Responding appropriately to the sharing of extremely private or emotional events (e.g. rape, abuse)
⓪ No ② Yes
Psychological first aid (PFA) ⓪ No ② Yes
Psycho-education (Client and family education about MH) ⓪ No ② Yes
Problem-solving counseling ⓪ No ② Yes
Teaching relaxation techniques ⓪ No ② Yes
Ethics and rights of people with mental illness ⓪ No ② Yes
4. Average Score (sum/total # scored) 4c ( ) 5. Staff roles and team work
Staff Roles Yes/No Specifics Staff have defined roles in identification, management and referral of mental disorders
⓪ No ① Yes, but roles not followed ② Yes and roles are followed
If yes, specify how:
Discussion about MH cases takes place
⓪ No ① Yes, informally ② Yes in regular (weekly or bi-weekly) meetings
If yes, specify who participates:
5. Average Score (sum/total # scored)
( )
6. Service Provision Indicators
Type of Case
# of cases (if known)
In the past month, the following was provided for this diagnostic category…
According to the clinic’s health information system in the last month, service was
provided for:
Identified at the PHC
level
Treated at the PCH level
Referred to specialized care
(MH)
Depression ⓪ No ② Yes
⓪ No ② Yes
⓪ No ② Yes
Psychotic disorder ⓪ No ② Yes
⓪ No ② Yes
⓪ No ② Yes
Epilepsy ⓪ No ② Yes
⓪ No ② Yes
⓪ No ② Yes

35
Bipolar disorder ⓪ No ② Yes
⓪ No ② Yes
⓪ No ② Yes
Developmental disorders (intellectual disability)
⓪ No ② Yes
⓪ No ② Yes
⓪ No ② Yes
Behavioral disorders (ADHD, conduct)
⓪ No ② Yes
⓪ No ② Yes
⓪ No ② Yes
Dementia ⓪ No ② Yes
⓪ No ② Yes
⓪ No ② Yes
Alcohol and drug use disorders
⓪ No ② Yes
⓪ No ② Yes
⓪ No ② Yes
Medically unexplained somatic complaints
⓪ No ② Yes
⓪ No ② Yes
⓪ No ② Yes
Anxiety / stress related disorders (e.g. PTSD)
⓪ No ② Yes
⓪ No ② Yes
⓪ No ② Yes
Other (specify):
⓪ No ② Yes
⓪ No ② Yes
⓪ No ② Yes
6 Average Score (sum/total # scored)
SUM ( )
6a ( ) 6b ( ) 6c ( )
7. Health Information System Indicators Mental disorders are documented in clinical charts ⓪ No
② Yes Mental disorders are documented in weekly or monthly morbidity report
⓪ No ② Yes
If yes, the reports are also separated by gender and age for analysis
⓪ No ② Yes
To Interviewer: If report is available please attach to the checklist
7. Average Score (sum/total # scored) ( )
8. Social Indicators The PHC has the following characteristics: The health care facilities is in safe walking distance of affected/target communities
⓪ No ② Yes
There is at least 1 female health care provider ⓪ No ② Yes
At least 1 staff member per clinic speaks the local dialects
⓪ No ② Yes O N/A
Documented procedures are in place to ensure that patients provide consent before medical procedures
⓪ No ② Yes
Health care provision is organized in a way that respects privacy (e.g. curtain around consultancy area, private room)
⓪ No ② Yes
Information related to the health status of people, especially those related to human rights violations (e.g. rape, torture) is treated confidentially
⓪ No ② Yes
Services are provided: O free of charge $ per consultation:____ What is the percentage of people living in this area who cannot afford services?
②<10 ① 11-50% ⓪ 51-100

36
8. Average Score (sum/total # scored) ( ) 9. Referral indicators Health staff know: Referral options to the mental health system (e.g. staff know the location, contact, costs and referral procedures for nearby mental health services)
⓪ No ② Yes Contacts:
How to link with protection agencies/ social services to address physical and sexual abuse
⓪ No ② Yes Contacts:
How to link with at least 2 social services or support systems in the community ( location, contact -e.g. social worker, social agency, community center, educational/vocational opportunities)
⓪ No ② Yes Contacts:
9. Average Score (sum/total # scored) 9a ( ) In the last 2 weeks mental health-related referrals occurred to PHC from: Mental health specialist care (secondary, tertiary or private care)
②Frequently ① Sometimes ⓪ Rarely/ Never
Community Health Workers (CHWs) ②Frequently ① Sometimes ⓪ Rarely/ Never
Other community workers schools, social services and other community social supports, traditional /religious healers
②Frequently ① Sometimes ⓪ Rarely/ Never
In the last 2 weeks mental health-related referrals occurred from PHC to:
Mental health specialist care (secondary, tertiary or private care)
②Frequently ① Sometimes ⓪ Rarely/ Never
Community Health Workers (CHWs) ②Frequently ① Sometimes ⓪ Rarely/ Never
Other community workers schools, social services and other community social supports, traditional /religious healers
②Frequently ① Sometimes ⓪ Rarely/ Never
9. Average Score (sum/total # scored) 9b ( )
III. Scoring Summary
Please fill scores from above in table below (under matching scoring field and multiplied by 10)

37
Category Actual Score Notes
0-3 4-7 8-11 12-15 16-20
1. Clinic Staff
2. Basic Pharmacy Data
3a. Staff Training Indicators-Theoretical Training
3a. Staff Training Indicators -Supervision
4a. Staff Skills Indicators-management of mental disorders
4b. Staff Skills Indicators-use of management of mental disorders
4c. Staff Skills Indicators-general skills
5. Staff roles and team work
6a. Service Provision Indicators-Identification
6b Service Provision Indicators-Management
6c. Service Provision Indicators-Referral
7. Health Information System Indicators
8. Social Indicators
9a. Referral indicator-knowledge
9b. Referral indicators-to and from PHCs
Total Frequency Scores
Notes:

38