Embed Size (px)
Citation preview

Injury Extra (2007) 38, 78—80
www.elsevier.com/locate/inext
CASE REPORT
Simultaneous gluteal and forearm compartmentsyndrome: An unusual case
Ashok Rampurada *, Sanjeev Sharma, Akingboye A. Akingfemi,Trinath Kumar
Doncaster Royal Infirmary, Armthorpe Road, Doncaster DN2 5LT, United Kingdom
Accepted 20 July 2006
Acute compartment syndrome is an orthopaedicemergency common in lower limb, less common inupper limb and gluteal compartment syndrome israre. We describe a patient with simultaneous fore-arm and contralateral gluteal compartment syn-drome. The forearm compartment syndrome wasdiagnosed clinically and confirmed with intraopera-tive findings. The gluteal compartment syndromewas diagnosed clinically, confirmed with invasivecompartment pressure measurement and intrao-perative findings.
This case report is intended to highlight the factthat compartment syndrome in one compartmentcan be followed by compartment syndrome inanother region in the body. A high index of suspicionis required. Early recognition and treatment is thekey to prevent complications.
Case report
A 13-year-old boy presented to the accident andemergency department in our hospital with com-plaints of a sudden onset swelling and blistering in
* Corresponding author. Present address: 35, Bruce Crescent,Doncaster DN2 5JL, South Yorkshire, United Kingdom.Tel.: +44 779 321 4615.
E-mail address: [email protected] (A. Rampurada).
1572-3461/$ — see front matter # 2006 Elsevier Ltd. All rights resedoi:10.1016/j.injury.2006.07.051
the right forearm and hand. There was a history ofalcohol consumption the night before and sleeping inan awkward position with the right forearm possiblytrapped beneath his back. There was no significantpast medical history.
The boy was systemically well but had a tenseswelling in his right forearm and hand with asso-ciated blistering and erythema (Figs. 1 and 2).Passive dorsi/volar flexion was very painful with aweak radial pulse and hypoesthesia in both medianand ulnar nerve distribution. He also had erythema-tous patches over his left gluteal region, both anklesand left shoulder. His haematological investigationsrevealed an elevated, creatine kinase of 79,692 IU/L, white cell count of 26.8 � 109/L, alkaline phos-phatase 813 IU/L and an increased aspartate trans-aminase of 1646 IU/L. C-reactive protein was10 mg/ml. The alcohol levels were not measured.
A provisional diagnosis of acute compartmentsyndrome of forearm and hand was made and anemergency fasciotomy was performed for the rightforearm and hand. This revealed some darkening ofthe flexor digitorum profundus belly but the musclewas contracting and bleeding and therefore was notdebrided.Dorsal compartmentwasnot involved.Dueto thepresenceof generalisederythematous patchesand unhealthy looking deep fascia a differentialdiagnosis of an early necrotising fascitis was alsoconsidered and therefore tissue and fluid samples
rved.

Simultaneous gluteal and forearm compartment syndrome 79
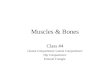
Figure 1 Note the blistering and erythema over forearmand hand.
were sent for culture and sensitivity and histopathol-ogy. Serum ASO titres were within normal limits. Thepatient was managed on intravenous flucloxacillin,benzylpenicillin and high dose clindamycin as per theadvice of microbiologist.
On the first post-operative day, he started com-plaining of severe left gluteal pain and invasivecompartment pressure measurement revealed anabsolute pressure of 69 mmHg in the gluteal musclesand 21 mmHg in the thigh. An emergency fasciotomy
Figure 2 Note the flexed position of fingers and swellingof fingers, thenar and hypothenar area.
was performed for the left gluteal and thigh areawhich revealed discoloured, non-contracting glu-teus maximus and minimus. Tissue and fluid culturesfrom both these sites failed to grow any organism.Histopathology revealed no signs of atrophy/necro-sis with areas of haemorrhage between the musclefibres. The patient started improving clinically aswell as on haematological parameters on the thirdpost-operative day. Creatinine kinase came down to25,442 IU/L and white cell count to 14.8 � 109/Lalthough C-reactive protein showed a minor rise to33 mg/ml.
On the nineth post-operative day the plasticsurgeons closed the gluteal wound secondarily andthe forearm wound was managed by vacuumassisted closure. There were no signs of infection.Finally split skin grafting was performed at 2 weekspost-operatively. The patient suffered no morbidityfrom the gluteal site but had a minor degree ofVolkmann’s ischaemic contracture of the right forearm which improved after intensive physiotherapy.He has finally regained good function in his rightforearm.
Discussion
Compartment syndrome (CS) is a condition in whichincreased tissue pressure within a closed osteofas-cial compartment compromises blood flow to mus-cles and nerves within that compartment, whichresults in tissue and nerve damage. We are notaware of any previously reported case of acute CSin forearm followed with gluteal CS or CS elsewhere.
There is an exhaustive list of possible etiologies.Although trauma is the most common etiologicalfactor, CS has been shown to occur following minortrauma, strangulation of the extremity, crush inju-ries and drug and alcohol abuse.2,4,9 You need to havea low threshold to diagnose1,6 and treat with fasciot-omy.3,5 The functional outcome is far better if fas-ciotomy is doneearlier, i.e.<12 h.10Muscles tolerate4 h of ischaemiawell, but by 6 h results are uncertainand after 8 h, the damage is irreversible.12 If diag-nosed late, fasciotomy is less beneficial and there is arisk of infection in the necrotic muscle.
Gluteal compartment syndrome is rare, oftenmissed or diagnosed late because of its rarity andanatomical location.7 If left untreated, it can leadto rhabdomyolysis, renal failure and sepsis earlierbecause of large muscle group and delay in diag-nosis.7,9 CS in gluteal region commonly occurs inpeople who lie in one position as a result of alcoholor due to drugs7,9 and can involve the sciatic nerve.8
The clinical picture sometimes can be confusedwith necrotising fascitis [type 2] as was seen in this

80 A. Rampurada et al.
case. The boy was systemically well. ASO titres werewithin normal range and cultures were negative.Early fasciotomy is advised if CS is suspected.1,11
The purpose of this case report is to highlight theoccasional unusual presentation of compartmentsyndrome at two sites in the body which can confusethe clinician as it did in this case. A high index ofsuspicion is required to diagnose such a situation andenable prompt surgical decompression in order tominimise complications.
References
1. Assenza M, Borromeo C, Moschella CM, Romagnoli F, ClementiI, Portieri M, et al. Compartment syndrome or gas gangrene? Acase report. G Chir 2001;22(10):345—7.
2. Beall S, Garner J, Oxley D. Anterolateral compartment syn-drome related to drug-induced bleeding. A case report. Am JSports Med 1983;11(6):454—5.
3. Botte MJ. Gelberman RH acute compartment syndrome of theforearm. Hand Clin 1998;14(3):391—403.
4. Gal P, Melichar I. The compartment syndrome in injuriesof the upper extremity in children. Rozhl Chir 1999;78(1):40—4.
5. Gelberman RH, Garfin SR, Hergenroeder PT, Mubarak SJ,Menon J. Compartment syndromes of the forearm: diagnosisand treatment. Clin Orthop Relat Res 1981;161:252—61.
6. Halpern AA. Nagel DA compartment syndromes of the fore-arm: early recognition using tissue pressure measurements. JHand Surg (Am) 1979;4(3):258—63.
7. Hill SL, Bianchi J. The gluteal compartment syndrome. AmSurg 1997;63(9):823—6.
8. Prynn WL, Kates DE, Pollack Jr CV. Gluteal compartmentsyndrome. Ann Emerg Med 1994;24(6):1180—3.
9. Schmalzried TP, Neal WC, Eckardt JJ. Gluteal compartmentand crush syndromes. Report of three cases and review of theliterature. Clin Orthop Relat Res 1992;277:161—5.
10. Sheridan GW, Matsen 3rd FA. Fasciotomy in the treatment ofthe acute compartment syndrome. J Bone Joint Surg Am1976;58(1):112—5.
11. Swaringen JC, Seiler III JG, Bruce Jr RW. Influenza A inducedrhabdomyolysis resulting in extensive compartment syn-drome. Clin Orthop June 2000;(375):243—49.
12. Whitesides TE, Heckman MM. Acute compartment syndrome:update on diagnosis and treatment. J Am Acad Orthop Surg1996;4:209—18.