Embed Size (px)
Citation preview

Should we Screen for Celiac Disease in IBS?
Brennan Spiegel, MD, MSHS
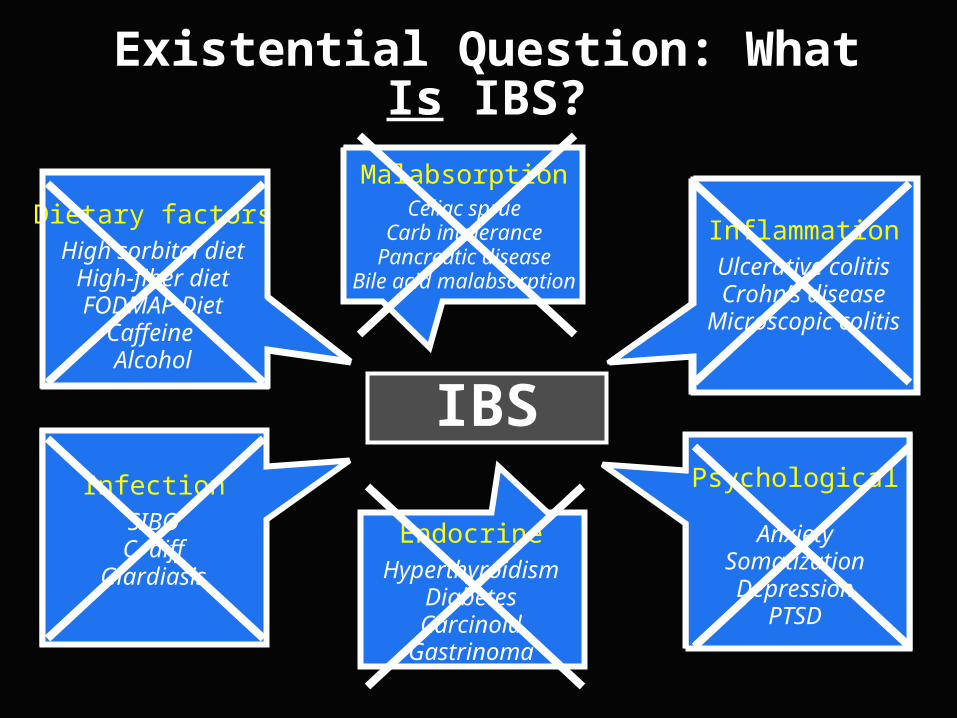
Dietary factorsHigh sorbitol diet
High-fiber dietFODMAP Diet
Caffeine Alcohol
InflammationUlcerative colitisCrohn’s disease
Microscopic colitis
EndocrineHyperthyroidism
DiabetesCarcinoid
Gastrinoma
Psychological
AnxietySomatizationDepression
PTSD
InfectionSIBOC. diff
Giardiasis
MalabsorptionCeliac sprue
Carb intolerancePancreatic disease
Bile acid malabsorption
Existential Question: What Is IBS?
IBS

Is IBS an absence of other things?
Or is it some thing… unto itself?
IBS

InflammationAltered brain–
gut interactions
Visceral hypersensitivity
Geneticfactors
Psychosocialfactors
Bacterial-Host Interactions
IBSIBS
Proposed Pathophysiological Mechanisms Involved in IBS

IBS Celiac
How often is overlap?When to screen?
How to screen?

Patient C.M. Case History
• 34 year old woman with 10-years of loose stools
• 4-6 bowel movements per day
• LLQ crampy pain that improves with stool passage
• Always feels “bloated”
• No weight loss, nighttime symptoms, incontinence, fevers, vomiting, or rectal bleeding
• No dairy intolerance, unusual travel, acute GI illnesses, recent antibiotics or other relevant meds
• No alarm features on physical examination
Patient C.M. – Laboratories
• Normal studies included:
– Complete blood count
– Serum electrolytes
– Stool cultures, sensitivity, and leukocytes
– Stool occult blood
– Erythrocyte sedimentation rate
– C Reactive Protein

Patient C.M. – Treatment Course
• Treated with antispasmodics
No improvement, felt sleepy
• Treated with rifaximin
“Little better at first, then worse again”
• Treated with loperamide
Diarrhea improved, but still had abdominal pain


“My IBS went away once I started the gluten free diet. And then, soon after trying bread again, it all came back.”
Clinical Questions
• Does she have celiac disease (CD), gluten sensitivity, or both?
• Does gluten exposure explain her symptoms?
• Could she still have IBS in addition to CD?
• Is a gluten-free diet appropriate at this point?
• What about gluten challenge, then re-biopsy?
• Need to check HLA-DQ2 or HLA-DQ8?

IBS Celiac
100% have symptoms consistent with celiac
20-75% have symptoms consistent with IBS
Zipser RD, et al. Dig Dis Sci 2003;48:761O’Leary C, et al. Am J Gastro 2002;97:1463

InflammationSIBO
IBS
66% have SIBO15-80% have SIBO
Tursi A, et al. Am J Gastro 2003;98:839
O’Leary C, Quigley E. Am J Gastro 2003;98:720
Verdu E, et al. Am J Gastro 2009
Celiac

Is this just a case of “true, true, and
unrelated?”
Is this just a case of “true, true, and
unrelated?”
Clinical Spectrum – Definitions
Overt celiac: Positive serology with Marsh III lesion.
Latent celiac: Normal serology and mucosa despite gluten, but genetic predisposition for sprue, persistent underlying immunologic abnormalities, with potential to express overt celiac with gluten challenge.
Gluten sensitivity: Minimal enteropathy (Marsh I-II) that improves histologically and symptomatically to gluten withdrawal in a patient with HLA DQ positivity
Wahnschaffe U, et al. Gastro 2001;1329Weinstein W. Gastro 1972;66:489
Verdu E, et al. Am J Gastro, 2009
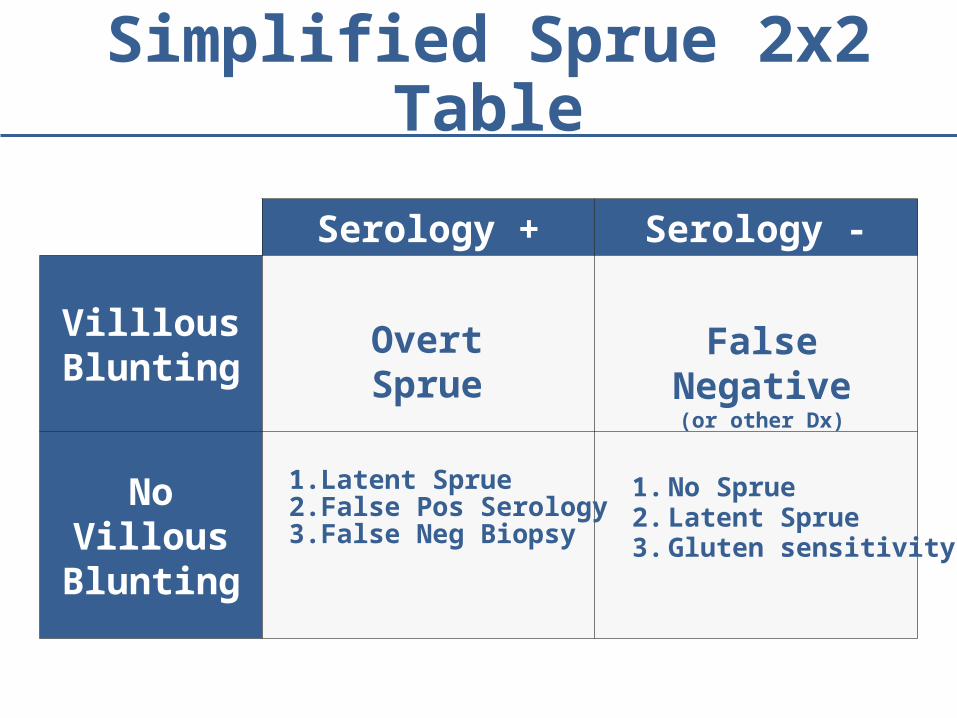
Serology + Serology -
Villlous Blunting
No Villous Blunting
Simplified Sprue 2x2 Table
Overt Sprue
1. Latent Sprue2. False Pos Serology3. False Neg Biopsy
False Negative(or other Dx)
1. No Sprue2. Latent Sprue3. Gluten sensitivity

More Realistic Sprue Table
TTG –AGA -
TTG –AGA +
TTG +AGA -
TTG +AGA +
Marsh0
Marsh I-II
Marsh III
1. No Sprue2. Latent Sprue
1. Gluten sens.2. False Pos AGA
Overt Sprue
1. Latent Sprue2. False Pos AGA
& TTG
1. Latent Sprue2. False Pos
Gluten sens.1. Gluten sens.2. False Neg
1. Other Dx2. False Neg
1. Overt Sprue2. Other Dx with FP
AGA
1. Gluten sens.2. False Pos TTG
Overt Sprue
1. No Sprue2. Latent Sprue
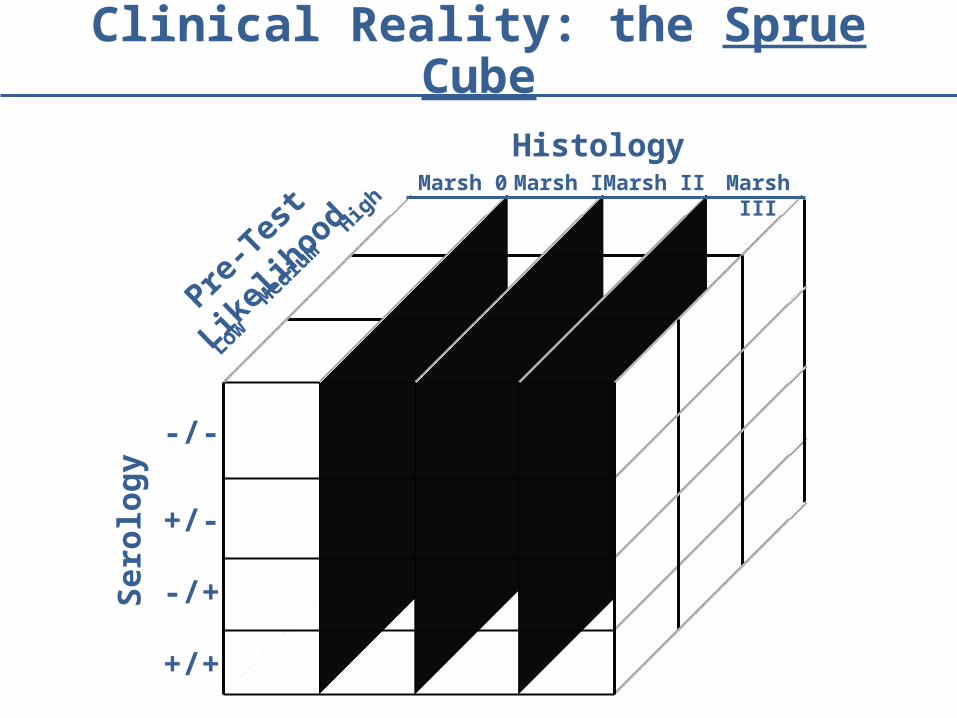
Pre-T
est L
ikel
ihood
Low
Med
ium
High
HistologyMarsh 0 Marsh IIMarsh I Marsh III
Ser
olo
gy
-/-
+/-
-/+
+/+
Clinical Reality: the Sprue Cube

Biopsy-Proven Celiac Disease in IBS: Results of Meta-Analysis
Ford A, Chey W, Talley N, Malhotra A, Spiegel B, Moayyedi P. Arch Int Med 2009;13:169
It is cost-effective to screen for celiac sprue in IBS if pre-test likelihood exceeds 1%
Spiegel et al. Gastroenterology 2004;126:1721
It is cost-effective to screen for celiac sprue in IBS if pre-test likelihood exceeds 1%
Spiegel et al. Gastroenterology 2004;126:1721

Data from U.S. – Link is Weaker
Cash et al. Gastroenterol 2011;141:1178
Biopsy proven sprue in IBS: 0.41%
Patient C.M. – Continued
• Reluctant to diagnose celiac disease
– Only Marsh I lesion
– Anti-TTG negative 98% NPV
– Anti-GA equivocal
– Lifetime diagnosis has significant implications
• Opted for gluten challenge with re-biopsy with HLA testing
– Cannot yet rule-out gluten sensitivity

Patient C.M. – Continued
• Enteroscopy with duodenal and jejunal biopsies normal after 2 month gluten challenge
• Follow-up labs
– ESR / CRP normal
– CBC normal
– IBD Panel negative
– HLA-DQ2 positive, HLA-DQ8 negative

Prometheus Sprue Panel
Does she have gluten sensitivity?
Latent Sprue and Gluten Sensitivity in IBS
• Wahnschaffe et al. studied 102 IBS patients:
– 0% had positive antibodies in serum– 35% were HLA-DQ2 +– 23% had elevated IELs (Marsh I), none Marsh II+– 30% had positive anti-TTG IgA in duodenal aspirate
• Treated sub-set with gluten-free diet
– Compared to controls, GFD improved stool frequency in HLA+ and duodenal anti-TTG+ patients
– Elevated IELs did not predict symptom response
Wahnschaffe U, et al. Gastro 2001;1329

D-IBS Patients: Predicting Response to Gluten-Free diet
Wahnschaffe U, et al. CGH 2007;5:844
Profile PPV NPV
DQ2 + 44% 94%
Antibody + (AGA/TTG)
45% 86%
DQ2+ and Ab+ 56% 88%
Impact of Gluten on EMA Positive Patients with Marsh I-II Lesions
Kurppa K, et al. Gastroentrol 2009;136:816-823

Impact of Gluten on Symptoms
Kurppa K, et al. Gastroentrol 2009;136:816-823
• Patients with mild enteropathy and positive serologies may benefit from early treatment with a gluten free diet even if they don’t meet strict criteria for celiac disease
• Current diagnostic criteria for celiac disease may need to be expanded to include patients with mild enteropathy (Marsh I-II)
• Patients with mild enteropathy and positive serologies may benefit from early treatment with a gluten free diet even if they don’t meet strict criteria for celiac disease
• Current diagnostic criteria for celiac disease may need to be expanded to include patients with mild enteropathy (Marsh I-II)

What About if Negative Serologies?

Vazquez-Roque, et al. Gastroentrol 2013;144:903-911

Patient C.M. – Continued
• Has been on strict gluten-free diet for 6 years, and has remained considerably better but still has some “IBS symptoms with stress.”

Take Home Messages
• Non-U.S. IBS patients around 4x more likely to harbor underlying biopsy-proven celiac disease
• Testing for celiac cost-effective if pre-test likelihood exceeds 1% – but probably lower in U.S.
• Even if no celiac disease, may still harbor latent celiac disease or gluten sensitivity
• If borderline, consider checking HLA DQ2 – if negative, probably no celiac; if positive, consider GFD





























