Embed Size (px)
Citation preview

Short-term Loss of Consciousness:
New European and American syncope guidelines
from the perspective of Emergency Room
Artur Fedorowski
MD, PhD, Assoc. Prof., FESC
Dept. of Cardiology, Skåne University Hospital & Dept of Clinical Sciences, Lund University,
Malmö, Sweden
November 15, 2019 Lodz (Poland)

ARTUR FEDOROWSKI Department of Clinical Sciences, Malmö, Lund University and Skåne University Hospital, Malmö, Sweden
Should I be worried?

ARTUR FEDOROWSKI Department of Clinical Sciences, Malmö, Lund University and Skåne University Hospital, Malmö, Sweden
Syncope - A Difficult Problem
• Find the cause
• Determine the risk
• Streamline the evaluation
• Prevent recurrence and debilitation
• Reduce hospitalization and mortality
Management - Complex, Confusing, Challenging
Brian Olshansky, 2019
Lifetime prevalence 40%
1-3% ED visits
6% Hospitalizations

Ricci F, De Caterina R, Fedorowski A. JACC 2015; 66(7): 846-60.
Autonomic failure
(Orthostatic hypotension)
Reflex syncope
(vasovagal)
Cardiac arrhythmias
Structural heart and
great vessels diseases
Baroreceptor
dysfunction
(CSS)

ARTUR FEDOROWSKI Department of Clinical Sciences, Malmö, Lund University and Skåne University Hospital, Malmö, Sweden
American and European Syncope Guidelines

ARTUR FEDOROWSKI Department of Clinical Sciences, Malmö, Lund University and Skåne University Hospital, Malmö, Sweden
SYNCOPE
Classification & Pathophysiology

www.escardio.org/guidelines
Definition
Syncope is a transient loss of consciousness (TLOC), due to
transient global cerebral hypoperfusion, characterized by
rapid onset, short duration and spontaneous complete
recovery.
72018 ESC Guidelines on Syncope – Michele Brignole & Angel MoyaEuropean Heart Journal (2018) 39, 1883–1948

www.escardio.org/guidelines
Classification of TLOC
8
Epileptic seizuresSyncope Psychogenic Rare causes
TLOC
TLOC due to head traumaNontraumatic TLOC
Reflex syncope
Orthostatic hypotension
Cardiac
Tonic-clonic seizures Psychogenicpseudosyncope
Subclavian steal syndrome
Vertebrobasilar TIA
Subarachnoid haemorrhage
Cyanotic breath holding spell
2018 ESC Guidelines on Syncope – Michele Brignole & Angel MoyaEuropean Heart Journal (2018) 39, 1883–1948
35-40%* 0.6-0.9%*
* Lifetime prevalence Neurology 2017;88:296–303

www.escardio.org/guidelines
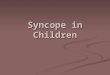
Epidemiology Frequency of the causes of syncope according to age
Age Source Reflex
(%)
Orthostatic hypotension
(%)
Cardiac
(%)
Non syncopal T-LOCs
(%)
Un-explained
(%)
<40 years OldeNordkamp
51 2.5 1.1 18 27
40-60 years
OldeNordkamp
37 6 3 19 34
<65 years Del Rosso 68.5 0.5 12 - 19
>60/65years
Del Rosso 52 3 34 - 11
Ungar 62 8 11 - 14
OldeNordkamp
25 8.5 13 12.5 41
>75 years Ungar 36 30 16 - 9
2018 ESC Guidelines on Syncope – Michele Brignole & Angel MoyaEuropean Heart Journal (2018) 39, 1883–1948

ARTUR FEDOROWSKI Department of Clinical Sciences, Malmö, Lund University and Skåne University Hospital, Malmö, Sweden
SYNCOPE
Initial Evaluation & Risk Stratification

www.escardio.org/guidelines
Initial presentation & evaluation of syncopeTLOC present?
(history)
No TLOC Syncope TLOC - non syncopal
Act as needed
Treat appropriately
• Epileptic seizure• Psychogenic TLOC• TLOC, rare cause
Initial syncope evaluation(H&P exam, ECG, supine
and standing BP)
Risk stratification
Uncertain diagnosisCertain or highly likely diagnosis
Start treatment
High-risk ofshort-term
serious events
Early evaluation& treatment
Low-risk but recurrentsyncopes
Ancillary testsfollowed by treatment
Low-risk,single or rarerecurrences
Explanation,no further evaluation
• High-risk !
• Age>65/75 y
• ECG changes
• Heart disease
• No prodrome
• Trauma
• Supine/during
exercise
2018 ESC Guidelines on Syncope – Michele Brignole & Angel MoyaEuropean Heart Journal (2018) 39, 1883–1948

Transient loss of consciousness*
Suspected
syncope
Yes
Evaluation as clinically
indicatedNo
Risk assessmentCause of syncope
certain
Cause of syncope
uncertain
Further evaluationTreatment
Initial evaluation:
history, physical examination,
and ECG
(Class I)
2017 ACC/AHA Syncope Guideline
ESC and ACC/AHA/HRS AGREE

Initial Evaluation
• Initial evaluation: history, physical
exam (standardized orthostatic
vitals) and 12-lead ECG.
• Additional tests based on
differential diagnosis.
Sheldon et al. CJC. 2011;27:246-253.

Risk Stratification Low-Risk Features High-Risk Features
History • Reflex syncope: prodrome, triggers, situations
• Positional• No cardiovascular disease
• Syncope during exertion or supine or without prodrome
• History of cardiovascular disease • Concomitant trauma• Family history of sudden cardiac death
(age < 50 years)
Physical exam • Normal • Abnormal vitals, cardiac exam
12-lead ECG • Normal • Abnormal brady/tachy arrhythmia• Conduction disease
Labs • Normal • Elevated biomarkers or abnormal tests with a suspected related diagnosis
Sheldon et al. CJC. 2011;27:246-253.

Syncope Risk Scores
• Numerous syncope risk scores
• Aid in triage decisions
• Do not reduce unnecessary admissions and costs.
• Do not perform better than clinical judgment.
COR LOE
IIb B
Use of risk stratification tools in the ED may be considered in the management of syncope.
ACC/AHA/HRS &
ESC Guidelines
Sheldon et al. CJC. 2011;27:246-253.

ARTUR FEDOROWSKI, Department of Clinical Sciences, Malmö, Lund University and Skåne University Hospital, Malmö, Sweden
UNEXPLAINED SYNCOPE
Further evaluation

www.escardio.org/guidelines
Should not be dischargedfrom the ED
Any high-riskfeatures require intensive
diagnostic approachShould not be discharged
from the ED
Low-riskfeatures only
Can be dischargeddirectly from the ED
Neitherhigh nor low-risk
Syncope out-patientclinic (SU) (if available)
ED or Hospital SyncopeObservational Unit
(if available)
Any high-riskFeature
Admission for diagnosisor treatment
Syncope Management(after initial evaluation in ED)
Likely reflex,situational or orthostatic
Ifrecurrent
172018 ESC Guidelines on Syncope – Michele Brignole & Angel MoyaEuropean Heart Journal (2018) 39, 1883–1948
ESC emphasizes the role of “syncope units”

www.escardio.org/guidelines
Staffing of an SU is composed of:1. One or more physicians who are syncope specialists.2. A support team comprised of trained professionals.
Equipment:
1. Essential Equipment/tests:
– 12-lead ECG and 3-lead ECG monitoring,
– non-invasive beat-to-beat blood pressure monitor,
– tilt-table,
– Holter monitors,
– external loop recorders,
– follow-up of implantable loop recorders (*),
– 24-hour blood pressure monitoring,
– Basic autonomic function tests.
Organizational aspects: Structure of the SU
2. Established procedures for:
– Echocardiography
– Electrophysiological studies
– Stress test
– Neuroimaging tests
3. Specialists’ consultancies (cardiology, neurology, internal medicine, geriatric,psychology), when needed
2018 ESC Guidelines on Syncope – Michele Brignole & Angel MoyaEuropean Heart Journal (2018) 39, 1883–1948

www.escardio.org/guidelines
Certain or highly likely diagnosis
Uncertain diagnosis
Initial syncope evaluation
Start treatment
Cardiac unlikely &recurrent episodes
EchocardiographyECG monitoring
(external or implantable)EP study
Stress testCoronary angiography
No further evaluation
Cardiaclikely
CV autonomic tests&
ECG monitoring(external or
implantable)
Cardiac unlikely &rare episodes
The diagnostic strategy for unexplained syncope
2018 ESC Guidelines on Syncope – Michele Brignole & Angel MoyaEuropean Heart Journal (2018) 39, 1883–1948
☞ 10-15% ☞ 70-75%
Cardiac pathway Autonomic pathway

Evaluation
2017 ACC/AHA Syncope Guideline
ESC and ACC/AHA/HRS AGREE
Cardiac pathwayAutonomic pathway

www.escardio.org/guidelines
ECG monitoring: indications
Low risk, arrhythmia likely
& recurrent episodes
Not indicated
If negative
Syncope T-LOCnon-syncopal
Unconfirmedepilepsy
Unexplained falls
Low risk &rare episodes
High risk, arrhythmia
likely
In-hospitalmonitoring
(Class I)
ILR(Class I)
Low risk, reflex likely & need for specific
therapy
ELR(Class IIa)
Holter(Class IIa)
ILR(Class I)
ILR(Class IIa)
ILR(Class IIb)
Certain diagnosis/mechanism
Treat appropriately
T-LOC suspected syncope
Uncertain diagnosis/mechanism
2018 ESC Guidelines on Syncope – Michele Brignole & Angel MoyaEuropean Heart Journal (2018) 39, 1883–1948
ESC emphasizes more ILR

www.escardio.org/guidelines
Pacing for reflex syncope: decision pathway
Clinical features
Perform CV autonomic tests
Implant ILR
Severe, reccurentunpredictable syncopes,
age >40 years ?no Pacing not indicated
CI-CSS?
Yes
No
No
No
Asystolictilt test?
Asystole?
Pacing not indicated
Yes & Tilt negative
Yes & Tilt positive
Implant a DDD PM
Implant a DDD PM & counteracthypotensive susceptibility
Yes Implant a DDD PM & counteract hypotensive susceptibility
Implant a DDD PM
Implant a DDD PM & counteracthypotensive susceptibility
Yes & Tilt negative
Yes & Tilt positive
2018 ESC Guidelines on Syncope – Michele Brignole & Angel MoyaEuropean Heart Journal (2018) 39, 1883–1948
Arrhythmia
Normal
Artefacts
CSS/VVS/OH
ESC emphasizes Aut-ILR algorithm

ARTUR FEDOROWSKI Department of Clinical Sciences, Malmö, Lund University and Skåne University Hospital, Malmö, Sweden
Take-home message
✓ Reflex syncope (vasovagal and carotid sinus reflex), orthostatic intolerance and cardiac
arrhythmias are the most common syncope diagnoses. Treatment is highly dependent on the
correct diagnosis.
✓ History → Examination (ECG/BP supine/standing/ telemetry) → Risk Stratification →
Admission/Observation/Discharge are the way to go …
✓ Identify syncope experts/units if uncertain and refer the patient (do not let them go home with a
message – “it is benign” – it may be the last time you see the patient alive).

ARTUR FEDOROWSKI Department of Clinical Sciences, Malmö, Lund University and Skåne University Hospital, Malmö, Sweden
… and remember ...
• Guidelines are a tool to help you make the most optimal decision in specific
circumstances in regard to specific patient (”guidelines patients” do not exist in the real
world).
• Use your best clinical judgment and common sense, and ask the senior doctor when in
doubt. Guidelines are not a law book!
• Guidelines change as our knowledge and experience develop. Make sure you are
updated!

ARTUR FEDOROWSKI Department of Clinical Sciences, Malmö, Lund University and Skåne University Hospital, Malmö, Sweden
Thank you for your attention!
Special thanks to Bob Sheldon, Win-Kuang Shen and Brian Olshansky for sharing their material.