Embed Size (px)
Citation preview

Archives of Disease in Childhood 1994; 71: 84-89
CURRENT TOPIC
Short term growth: rhythms, chaos, or noise?
J K H Wales, A T Gibson
Non-linear growthIt has been traditional to think ofheight gain ofchildren as a steady process and the term'linear growth' is often used as shorthand forincrease in stature as opposed to weight.' Weare often reminded of this with simple graphicson textbook covers and logos for organisationsand meetings that depict a series of children ofdifferent heights with their heads connectedby a smooth line. It is also easy to believe thatthe beautiful curves on a centile chart2 describethe real progress in height of an individual,without realising that the chart is a statisticalconstruct from population data that often hasbeen 'smoothed' mathematically to producethe finished product.
Paediatricians normally monitor the growthof their patients at relatively infrequentintervals, and for relatively brief periods of thechild's growth span. At this level the healthychild will tend to follow a centile channeldetermined (after the first two years of life)by his or her genetic background. Indeedthe growth of an individual approximates toa series of curves which can be describedmathematically as an exponential (infantilegrowth) plus a second degree polynomial(mid-childhood growth) plus one of a family oflogistic functions (a description of the timingof puberty and then cessation of growth). Thisis the basis ofthe infancy-childhood-puberty orICP model of growth3 4 but it must be remem-bered that this is both a model ofgrowth and anapproximation - not a description of real life.
If we assess the growth of an individualby multiple measurements over a long periodof time then deviations from a smoothcurve become apparent. Montbeillard's son isthe classic example - the Count demonstratingthat there was apparently periodic accelerationand deceleration in the growth rate of his childas early as 1777. Some of these were associatedwith the season of the year, others wereunexplained.5The more closely we look at the growth
process the more non-linear it becomes.Indeed if we think about the process thatleads to an increase in height there is noreason to suppose that linearity is anythingother than a convenient approximation toreality. First picture a single cell in a growthplate: at any time it may be resting, synthesis-ing, or dividing as it passes through the cellcycle. In the simplest possible system of onecell exposed to a single growth factor withfeedback regulation, given a response that
is not instantaneous there would be a simpleoscillation of division and rest with reciprocalpeaks and troughs of the growth factor - thenet result being 'growth' which would bepredictable but non-linear. Then complicatethe system by adding multiple cells, arrangedin thousands of columns per growth plate.Each cell is under the control of multiplehormones and growth factors secreted in anendocrine, paracrine, and autocrine fashion.The endocrine events are modulated them-selves by catabolism, daylight hours, time ofday, and pulse generators in the centralnervous system. Other factors such as temper-ature, nutrient supply, and pressure (in anerect human) also modulate cellular events.The control mechanisms for division andsynthesis are different at each stage of the cells'differentiation in the growth plate. Thenrealise that there are at least 58 epiphysesbetween the heel and the top of the head, notall responding to any of the aforementionedsignals in the same way6 or contributing thesame amount of growth to final height. Themultiple small events throughout the body allsummate, but growth cannot be a linearprocess.We then come to the measurement of
growth itself. All measurements are them-selves approximations and subject to equip-ment and observer error. There have beenmany attempts to refine anthropometricl 7-9or biochemical observations10 to predictsubsequent growth, either natural or as aconsequence of treatment. It may be that thedevelopment of ever more precise measure-ment techniques and devices will merely leadto the observation of more and more detailof the growth process, interesting in itself, butof no help in prediction of later growth.The study of dynamic interacting systems,
of which human growth is but one example,takes us into the realms of chaos theory."IDeterministic chaos is the random lookingand unpredictable output produced by theeffects of different modifiers, any of which canbe described by simple rules, on a singlenon-linear system. It is characterised by'periodicities' and 'intermittencies' wheresmall events summate to produce wild swings(or saltations?) in the observed value. Chaoticsystems are also characterised by 'phase shifts',where there can be sudden changes from onequasistable consequence of summated eventsto another (one could stretch a point andsuggest a parallel with the changes seen at the
Department ofPaediatrics, Universityof Sheffield, Children'sHospital, SheffieldSO 2THJ K H WalesA T Gibson
Correspondence to:Dr Wales.
84

Short term growth: rhythms, chaos, or noise?
interface between infancy and childhoodgrowth and childhood and pubertal growth)and 'sensitivity on starting conditions' wheresmall differences in the initial configurationof the system (child?) may produce extremevariation in the eventual output (height?).To give a familiar example from the litera-
ture of chaos theory, which draws heavily onanalogies with weather forecasting, the 'butter-fly effect' states in simple terms that long termweather prediction is impossible as very smallchanges in the initial conditions can magnify toproduce large variations at another point, or,if a butterfly flaps its wings in a rain forestthis will perturb the 'starting conditions' andcause subtle local changes in air pressure thatproduce larger regional changes the net effectof which may be later storms over England.However, an identical butterfly on the next leafwith the next wing beat may produce noobservable later weather effects, or tornadoesin Arizona. However, although precise predic-tion of next week's weather is not possible, wecan say with virtual certainty that summer willfollow winter. In a similar manner we may notbe able to predict the exact height of a childthree months from now but we can makebroad predictions about a likely final height.As one looks deeper into the processes of the
chaotic system one continues to find apparentdisorder at every level down to the subatomicquantum realm. If the disorder has short,medium, and longer term fluctuations that aresimilar in their appearance, demonstrating'scale invariance', then this is called 'fractal'behaviour. "l 12
Chaotic systems are unpredictable, but thefact that short term unpredictability existsin human growth, and that height gain isnon-linear, does not mean that it is necessarilytruly chaotic. If a large number of independentsources of fluctuations interact on any processthey may produce stochastic (that is, non-deterministic) noise. It may be that growthshould be considered as a single non-linearsystem, when chaos theory might apply,but non-linear time series analysis of a hugenumber of data points (>105), impracticablein longitudinal human studies, is required todifferentiate this from random noise.We will now examine the methodology and
some of the current knowledge of the shortterm growth process to see if any conclusionsmay be reached concerning the 'true' nature ofchildhood growth.
Measurement error(1) HEIGHTHeight is the most reliable of classical anthro-pometric techniques,13 14 but still a source ofartefactual variations in height. This subjecthas recently been explored in detail by theWessex Growth Study15 16 and measurementof height is still often performed very poorly. 17Details of the means of analysing machine,interobserver and intraobserver error can befound in the chapter by Noel Cameron inHuman Growth.'8 It is unfortunately still rarefor researchers to quote these values in relation
to their observations (this is especially true forthat deceptively simple measurement, weight).If one's measurement error exceeds the likelyvalue of the change in the parameter observed,then there is no point in making the measure-ment or drawing conclusions about thechanges you may observe. This should beborne in mind when considering treatmentresponses in height velocity measured overshort periods where these values are notavailable.
Distinctions must be made between com-munity based surveys for short stature andthe more precise growth studies that arepossible using selected subjects in a measuringlaboratory. Voss et al detail error due toequipment malpositioning and child basedfactors,'5 besides observer error that will bemagnified still further if more than onemeasurer is used. One may be reasonablyconfident that a single height observationmay be accurate to ± 2 SD, equivalent to ±0 5cm in many community based studies. Thisis approximately the increment in heightone might observe over 2 months in mid-childhood, and more frequent measurementsare unlikely to be of value.We are lucky in Sheffield to have had
two consecutively employed professionalauxologists who have made observations onhigh quality equipment in a specialisedmeasuring laboratory over the last 20 years. Ithas been their practice to take measurementsof height without knowledge of previousrecords, to avoid bias. Possibly more importantthan the technique are the subjects used in theshort term growth studies quoted below, whoare 'trained' to be 'good' subjects by multipleattendances. The mean SD of measurement ofour current auxologist, performing a series ofcompletely blind replicate measurements onthese individuals is 0 11 cm, equivalent to theincrement of height observed in approximatelyfour weeks.
Postural changes in height through the day,largely due to spinal disc compression, havebeen quantified since the 18th century. TheReverend Wasse demonstrated that height lossthrough the day could be as much as 6/1 Othsof an inch, came from the back not the legs,and was more prominent in younger peopleand heavy labourers.'9 Montbeillard showedthat his son 'shrank' after an all night party.5These postural losses have been quantified as0 55 cm and 1-2 cm by different 20th centuryobservers20 21 and can be minimised, but noteliminated by use of the 'stretch' technique22where the mean morning difference was0-2 cm and 0-46 cm through to the afternoon.It is thus important that short term growthstudies should try to measure children at thesame time of day, wherever possible. The oftenquoted phrase to medical students 'you canlose weight but you can't lose height' is nottrue at this time scale.
(2) HEIGHT VELOCITYIf one considers height velocity the possi-bility that measurement error contributes
85

86Wales, Gibson
significantly to one's observed results increasesdramatically. Meredith estimated the maxi-mum frequency of measurement from the 90thcentile confidence limits of calculation ofvelocity for a number of parameters.14 Heestimated that bimonthly measurements inmid-childhood would yield acceptably accu-rate results given an error of measurementsimilar to that found by Voss et al.15 Themore rigorous 95% confidence limits of avelocity in cm/year calculated from twomeasurements a year apart is ±2 multipliedby the SD of the measurement multipliedby the square root of two. The same limitsfor a velocity calculated over three months is±(2 SDX72-)x4 and at a two months gap± (2 SDxVT2) X 6. Given our observationalaccuracy of 0O11 cm a change in velocity of> ±1I 8 cm/year would have to occur over aneight week period to be reasonably sure that itwas a real event.
Short term growth measurements inchildhood(1) HEIGHTGiven these constraints, what does growth inheight look like when studied at this detail?We have analysed the records of a number ofchildren attending a specialist clinic for cysticfibrosis in whom measuring laboratory heightscollected as detailed above are available, takenat approximately the same time of day, overa long period, at approximately eight weekintervals. It must be stressed that the reason wehave such detailed measurements availableis that these children are not normal healthyindividuals - although in the example citedbelow the health of the child is remarkablygood - but it is still possible to make someinferences about the growth process if oneassumes that catabolic events will be overrepresented.
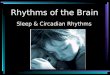
Figure 1 shows the height chart and fig 2 theheight velocity for one such child measured atyearly (two points, one year apart), six monthly(two points, six months apart x 2), threemonthly (two points, three months apart X4),and using all available data (mean intervaleight weeks). One can appreciate an increasingcomplexity of changes in height velocity as themeasuring interval decreases. Even ignoringchanges of less than ± 1-2 cm/year at threemonths, or ±1 8 cm/year at eight weeks aspossibly being artefacts of measurementerror, there are surprising variations in heightvelocity. This pattern would be familiar tostock market analysts, and superficially seemsto demonstrate scale invariance, in other wordsgrowth rate appears to show some attributes offractal behaviour. Superficial analysis of thisdata shows no obvious rhythmicity or seasonalchanges in rate, but mathematic techniquesbeyond the power of these authors, and severalorders of magnitude more data points arerequired to 'prove' chaos.
Larger scale variations in height velocityhave been described with season of the year.These changes are not present in all membersof a population,23 can be in different phase in a
similar population at different times,24 and arereduced in relationship to blindness25 but notreduced daylight hours.26 Seasonal variationsare even said to persist in growth hormonetreated children.27 Careful analysis of heightvelocity in Edinburgh children shows a seriesof growth spurts through childhood,28 some ofwhich may be seasonal and others which mayrepresent the mid-childhood growth spurtsthat have been observed in other studies.29 30Seasonal changes even occur in human hairgrowth, but not in that of fingernails!3'One study that exemplifies all the above
points comes from Japan.32 Two observersmeasured their children daily for a year.Daytime variation in height, due to spinalcompression is clearly seen. The children showsteady growth of subischial leg length at twodifferent rates in the observation period. Theback grows hardly at all for the first part ofobservation, but suddenly grows at a rapid ratein the last two months, resulting in a leap, orsaltation, of height.
(2) ISOLATED AREAS OF SKELETAL GROWTHAND KNEMOMETRYFurther information on the growth process cancome from observations made on single bonesor well defined groups of bones or othertissues. A number of radiographic studies onbone growth have been made in humans.33Over a period of years around puberty,Roche showed that the maximum incrementin length of the radius and tibia had differentrelationships to the peak height spurt.6Measurement of short term growth in stable
aggregates of bones began with ulnar con-dylography7 but evolved into the measurementof the lower leg as knemometry. We have foundknemometry in children to be precise (meancoefficient of variation ofmeasurement 009%)and observer independent.1 The lower legs ofhealthy children appear to grow at a steady ratethen show unexplained leaps in growth. Thereare also clear slowings or shrinkage that can beassociated with even minor catabolic stress,followed by catch-up growth. Shrinkage here ispresumably due to compression of non-growing bone and cartilage and a possible shiftin the balance between bone deposition andresorption with illness that can account for thegrowth arrest or Harris' lines seen on plainradiographs. Hermanussen et al have studiedthe periodic growth in healthy children in mostdetail.34 They describe 'mini-growth spurts'and by analysis of a rolling height velocityascribe a periodicity of 30-55 days to thisphenomenon. The analytical technique usedis, however, prone to a mathematical effectcalled aliasing35 which can produce regularperiodicity where none exists and will maskshort term phenomena.
Radiographic and knemometric observa-tions suffer from the fact that the growthbehaviour of only a single part ofthe skeleton isanalysed. Non-linear behaviour is likely to existin other areas, however, and it is very unlikelythat the periodicities would cancel out toproduce smooth growth in stature.

Short term growth: rhythms, chaos, or noise?
190 97measurement 0 3 mm, but unlike the bigger1--______ knemometer, highly dependent on the use of
180 L Boys ' ° an experienced observer. Soft tissue changes,10Boys 750 using the technique as described have verylittle effect on the observations,8 we have even
170-0 observed leg growth in a hydropic infant who3 lost 30% of his birth weight as fluid in the first
160 - three days of life (unpublished observations).-://///t/t As in older children 'negative' growth, or
150 - shrinkage, may occur, especially at times ofcatabolic stress. Here the bone is not com-
140 pressed, as the infants are nursed supine, butagain presumably reflects a change in the
130 balance of bone resorption over deposition.E ,y// The precision allows for observations of leg
120 growth liable to occur over 2-3 days. We haveused it to explore the effects of chronic lung
I 110 _ ,,%///," disease, nutrition, and steroid treatment in thisgroup of children.39 Long term observations
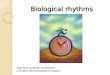
100 _ ,///,on the growth of 'healthy' premature neonatesare, by definition, scarce. We have analysed theleg growth of one 28 week gestation infant whowas free of any complications of prematurityand kept on our unit for 63 days pending adop-tion. Only one change in management wasmade, the institution of low birthweight
70 R formula from day 18 to day 46. Changes in rateof leg growth are shown in fig 3. At 6-7 day
60 increments there was an association betweenchanges in weight and changes in leg length
50 - I I that was less clear when analysed at 2-3 day
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 increments. Most of the changes in leg growthAge (years)
Figure 1 Growth ofsubject plotted on height chart ofUK Tanner and Whitehouse 1975standards; adaptedfrom Castlemead Publications, Weluyn Garden City, 1983 (shading 20indicates limits for single occasions). 2 Yearly
Short term growth measurements in 1infiancy(1) WHOLE BODYPeriodic changes in weight gain have been 20described in neonates.36 The phenomenon of 6 months'fractal' changes in weight gain is clearly seenwith decreasing measurement intervals. 10 _By using a modified length measuring z,A
device, Lampl and colleagues describe growth\in length of the post-term infant as a process of \saltations (leaps) interspersed with long 2periods of stasis.37 Similar data also exists for .5 _ultrasonically estimated leg length of fetuses °(M Lampl, P Jeanty, M L Johnson. Saltatory ?growth patterns infetal tibia; personal communi- 10cation). In these cases data has been analysedby various mathematical models and thesaltatory model provides the 'best fit' through o_l_l_l_l_l_l_lthe data points. Again this does not necessarily 20represent the actual growth of the leg; as we 8 weekshave previously discussed chaotic or complex 10behaviour is prone to show intermittencies.Apparent saltations can also be a consequence Kof growth rate exceeding the measurementerror of an observation. ° --YJ----
o 2 4 6 8 10 12 14 16
(2) KNEMOMETRY Age (years)The neonatal knemometer, first described by Figure2 Heightvelocityofsubjectplottedatyearly,Michaelsen et al 38 has been used by us to
six and three monthly, and at approximately eight weekMichaelsnet al,8 has ben used y us to intervals for 14 years. The total number of observations wasmeasure a large number of premature 89 with a mean (SD) measurement interval of8 (3) weeksneonates. It is also precise, mean SD of (range 2-17 weeks).
87

Wales, Gibson
Beware of drawing too many conclusionsfrom the fit of mathematical models, includingchaos theory, to data. The ICP model has beeninterpreted as showing relative independenceof growth from the influence of growthhormone in infancy,3 4 but real life observa-tions on hypopituitary infants show this not tobe the case.48A single non-linear simple dynamic system
with interacting control mechanisms will tend011101 IIE0 70il to produce a chaotic pattern. A large number
0 10 20 30 40 50 60 70 of independent sources of fluctuation on anyAge in days (midpoint) process will produce unpredictable noise.
3 Two or three day leg length increment measured Differentiation of the two processes withnometry in healthy 28 week gestation infantfrom respect to childhood growth is not currently63 days. Low birthweight formula feeds were possible. We cannot predict an individual'son day 18 and discontinued on day 46. exact height six months from now in the same
way that we cannot predict the weather in aweeks' time. This article has been designed
velocity exceed the error that can be attributedto measurement error and derivation ofvelocity (±O025 mm day) and show non-linearbehaviour with a clear positive effect of theintroduction of low birthweight formula.Bishop et al demonstrated a similar phenom-enon over a much shorter period, after initialweight loss, in a group of 45 term infants.40
Animal modelsUsing tetracycline staining of rabbit bonesexposed to controlled lighting conditionsHansson et al showed that there were distinctperiods of rapid and slow growth throughoutthe day.41 This is in contradistinction toobservations of high accuracy (error ofmeasurement 0-05 mm day) using metalpins inserted into rabbit bones growing at0-27 mm day which failed to show saltation,but revealed a Gaussian distribution of velo-cities around an intermediate value, more
indicative of continuous growth than a
periodic model.42 Individual growth patternswere clearly non-linear, however.
ConclusionsThere is mounting evidence that growth inheight is not a steady process, but made upof intermittent episodes of growth that mayoccur in different parts of the skeleton atdifferent times. Growth rate is determined by a
complex interaction of physical, endocrine,nutritional, and anabolic effects and may be dis-rupted by ill health and psychosocial factors.1 43
Measurement error and postural change ofstanding height may produce apparent changesin growth velocity, but even when these are
accounted for there appears to be evidence ofnon-linearity both at the whole body and singlebone level. It is important to realise that thisnon-linearity defeats any attempts to predictlong term growth from short term observationseither ofone bone or the whole body,23 446 andthis should no longer be attempted.
Short term growth studies may have theirvalue in describing the dynamics of growthand, in well designed research with adequatefollow up, comparing two growth suppressingor promoting treatments.47
to be speculative and thought provokingand to show that growth is complex, at leastin the short term. Possibly by providingmore questions than answers it demonstratesthat much further research remains to beperformed.
Our thanks to Dr Brian Bailey, Faculty of MathematicalStudies, University of Southampton and Dr Peter Dixon,Section of Pure Mathematics, University of Sheffield for theirhelpful comments on the statistics and chaos theory, respec-
tively. Also thanks to Mrs Margaret Pickering, professionalauxologist at Sheffield Children's Hospital for her skill anddedication in measuring children.
1 Wales JKH, Milner RDG. Knemometry in the assessmentof linear growth. Arch Dis Child 1987; 62: 166-71.
2 Tanner JM, Whitehouse RH. Clinical longitudinal stan-dards for height, weight, height velocity, weight velocityand stages of puberty. Arch Dis Child 1976; 51: 170-9.
3 Karlberg J, Fryer JG, Engstrom I, Karlberg P, Fryer JG.Analysis of linear growth using a mathematical model. I.From birth to 3 years. Acta Paediatr Scand 1987; 76:478-88.
4 Karlberg J, Engstrom I, Karlberg P. Analysis oflinear growthusing a mathematical model. II. From 3 to 21 years of age.Acta Paediatr Scand 1987; 337 (suppl): 12-29.
5 Scammon RE. The first seriatim study of human growth.Am JPhysAnthropol 1927; 10: 329-36.
6 Roche AF. Differential timing of maximum length incre-ments among bones within individuals. Hum Biol 1974;46: 145-57.
7 Valk IM, Van den Bosch JSG. Intradaily variation of thehuman ulnar length and short term growth a longitudi-nal study in eleven boys. Growth 1978; 42: 107-11.
8 Gibson AT, Pearse RG, Wales JKH. Knemometry and theassessment of growth in premature babies. Arch Dis Child1993; 69: 498-504.
9 Gregory JW, Greene SA, Jung RT, Scrimgeour M, RennieMJ. Changes in body composition and energy expenditureafter six weeks' growth hormone treatment. Arch Dis Child1991; 66: 598-602.
10 Trivedi P, Hindmarsh P, Risteli J, et al. Growth velocity,growth hormone therapy, and serum concentrations of theamino-terminal propeptide of type III procollagen.Pediatr 1989; 114: 225-30.
11 GleickJ. Chaos. 1st Ed. London: Abacus Books, 1993.12 Sander LM. Fractal growth processes. Nature 1986; 322:
789-93.13 Gavan JA. The consistency of anthropometric measure-
ments.AmJPhysAnthropol 1950; 8: 417-26.14 Meredith HV. The reliability of anthropometric measure-
ments taken on eight- and nine-year-old white males.Child Dev 1936; 7: 262-72.
15 Voss LD, Bailey BJR, Cumming C, Wilkin TJ, Betts PR.The reliability of height measurement. Arch Dis Child1990; 65: 1340-4.
16 Voss LD, Wilkin TJ, Bailey BJR, Betts PR. The reliability ofheight and height velocity in the assessment of growth.(The Wessex growth study.) Arch Dis Child 1991; 66:833-7.
17 Wales JKH. Child health surveillance: illustrations perpetu-ate bad practice. BMJ 1993; 307: 508-9.
18 Cameron N. The methods of auxological anthropometry.In: Falkner F, Tanner JM, eds. Human growth. A compre-hensive treatise. Vol 3. 2nd Ed. New York: Plenum, 1986:30-6.
19 Wasse J. Concerning the differences in the height of thehuman body between the morning and night. PhilosophicalTransactions of the Royal Society ofLondon 1724; 33: 87-8.
20 Baker IA, Hughes J, Jones M. Temporal variation in theheight of children during the day. Lancet 1978; i: 1320.
2
E
Ea,0E
0
-1
Figure:by knenbirth toinstitute
88

Short tern growth: rhythms, chaos, or noise?
21 Strickland AL, Shearin RB. Diurnal height variation inchildren. J Pediatr 1972; 80: 1023-5.
22 Whitehouse RH, Tanner JM, Healy MJR. Diumal variationin stature and sitting height in 12-14-year-old boys.Ann Hum Biol 1974; 1: 103-6.
23 Marshall WA. Evaluation of growth rate in height over peri-ods of less than one year. Arch Dis Child 1971; 46:414-20.
24 De Wijn JF, Postmus S, Dirks C. Seasonal changes in therate of growth. In: Van den Bosch JJ, Haak A, eds.Proceedings of a Boerhaave course for postgraduate medicalteaching. Somatic growth of the child. Leiden, Netherlands:Stenfert Kroese NV, 1966.
25 Marshall WA, Swan AV. Seasonal variation in growth ratesof normal and blind children. Hum Biol 1971; 43: 502-15.
26 Marshall WA. The relationship of variations in children'sgrowth rates to seasonal climatic variations. Ann Hum Biol1975; 2: 243-50.
27 Rudolph MCJ, Zadik Z, Linn S, Hochberg Z. Seasonalvariation in growth during growth hormone therapy.Am _T Dis Child 1991; 145: 769-72.
28 Butler GE, McKie M, Ratcliffe SG. The cyclical nature ofprepubertal growth. Ann Hum Biol 1990; 17: 177-98.
29 Berkey CS, Reed RB, Valadian I. Mid-growth spurt inheight of Boston children. Ann Hum Biol 1983; 10: 25-30.
30 Molinari L, Largo RH, Prader A. Analysis of the growthspurt at age seven (mid-growth spurt). HelveticaPaediatrica Acta 1980; 35: 325-34.
31 Randall VA, Ebling FJ. Seasonal changes in human hairgrowth. BrJ Dermatol 1991; 124: 146-51.
32 Ashizawa K, Kawabata M. Daily measurements of theheights of two children from June 1984 to May 1985.Ann Hum Biol 1990; 17: 437-43.
33 Maresh MM. Measurements from roentgenograms. In:McCammon RW, Thomas CC, eds. Human growth anddevelopment. Springfield, USA: C C Thomas, 1970:157-69.
34 Hermanussen M, Geiger-Benoit K, Burmeister J, SippellWG. Periodical changes of short term growth velocity('mini-growth spurts') in human growth. Ann Hum Biol1988; 15: 103-9.
35 Hermanussen M, Burmeister J. Measuring short-term peri-odicity of pediatric growth. Monatsschr Kinderheilkdunde1989; 137: 403-10.
89
36 Greco L, Capasso A, De Fusco C, Paludetto R. Pulsatileweight increases in very low birthweight babies appro-priate for gestational age. Arch Dis Child 1990; 65:373-6.
37 Lampl M, Veldhuis JD, Johnson ML. Saltation and stasis: amodel of human growth. Science 1992; 258: 801-3.
38 Michaelsen KF, Skov L, Badsberg JH, J0rgensen M. Short-term measurement of linear growth in preterm infants:validation of a hand-held knemometer. Pediatr Res 1991;30: 464-8.
39 Gibson AT, Pearse RG, Wales JKH. Growth retardationafter dexamethasone administration: assessment byknemometry. Arch Dis Child 1993; 69: 505-9.
40 Bishop NJ, King FJ, Lucas A. Linear growth in the earlyneonatal period. Arch Dis Child 1990; 65: 707-8.
41 Hansson LI, Stenstrom A, Thorngren KG. Diurnal varia-tion of longitudinal bone growth in the rabbit. Acta OrthopScand 1974; 45: 499-507.
42 Klein KO, Munson PJ, Bacher JD, Cutler GB, Baron J.Linear growth in the rabbit is continuous not saltatory.Endocrinology 1994; 134: 1317-20.
43 Wales JKH, Taitz LS. Patterns of growth in abused child-ren. In: Hernandez M, Argente J, eds. Human growth:basic and clinical aspects. Amsterdam: Elsevier SciencePublishers, 1992: 151-9.
44 Polychronakos C, Abu-Srair H, Guyda HJ. Transientgrowth deceleration in normal short children. A potentialsource of bias in growth studies. EurJ Pediatr 1988; 147:582-3.
45 Neyzi 0, Bundak R, Molzan J, Gunoz F, Darendeliler F,Saka N. Estimation of annual height velocity based onshort-versus long-term measurements. Acta PaediatrScand 1993; 82: 239-44.
46 Hermanussen M, Burmeister J. Standards for the predictiveaccuracy of short term body height and lower leg lengthmeasurements on half annual growth rates. Arch Dis Child1989; 64: 259-63.
47 Karlberg J, Gelander L, Albertsson-Wikland K.Distinctions between short- and long-term growthstudies. Acta Paediatr Scand 1993; 82: 631-4.
48 Chatelain P. Dramatic early post-natal growth failure inchildren with early onset growth hormone deficiency.Kabi Pharmacia International Growth Study 1991; 7:45-8.