Embed Size (px)
Citation preview
Current Treatment Options in OncologyDOI 10.1007/s11864-014-0296-2
Lower Gastrointestinal Cancers (AB Benson, Section Editor)
Short-Course versusLong-Course Chemoradiationin Rectal Cancer—Timeto Change Strategies?Manisha Palta, M.D*
Christopher G. Willett, M.D.Brian G. Czito, M.D.
Address*Duke University Medical Center DUMC, 3085, Durham, NC 27710, USAEmail: [email protected]
* Springer Science+Business Media New York 2014
Keywords Rectal cancer I Radiotherapy I Short course I Chemoradiation
Opinion statement
There is significant debate regarding the optimal neoadjuvant regimen for resectablerectal cancer patients. Short-course radiotherapy, a standard approach throughoutmost of northern Europe, is generally defined as 25 Gy in 5 fractions over the courseof 1 week without the concurrent administration of chemotherapy. Long-course radio-therapy is typically defined as 45 to 50.4 Gy in 25–28 fractions with the administrationof concurrent 5-fluoropyrimidine-based chemotherapy and is the standard approach inother parts of Europe and the United States. At present, two randomized trials havecompared outcomes for short course radiotherapy with long-course chemoradiationshowing no difference in respective study endpoints. Late toxicity data are lacking giv-en limited follow-up. Although the ideal neoadjuvant regimen is controversial, our cur-rent bias is long-course chemoradiation to treat patients with locally advanced,resectable rectal cancer.
IntroductionThe optimal neoadjuvant regimen for patients withresectable rectal cancer is unclear. In NorthernEuropean countries, the use of short-course preoper-ative radiotherapy (RT) alone (25 Gy in 5 fractions)followed by total mesorectal excision (TME) approx-imately 1 week later has become standard practice.
This approach is supported by multiple randomizedtrials comparing TME alone to preoperative short-course RT and surgery. In the United States and otherparts of Europe, the use of long-course conventional-ly fractionated radiotherapy (45-50.4 Gy in 25-28fractions) with concurrent administration of 5-
fluoropyrimidine (5-FU)-based chemotherapy is fa-vored based on the results of the German rectal can-cer trial. Two published, randomized trials havecompared outcomes of short-course RT to long-course chemoradiation (CRT). The role of neoadju-vant therapy has been questioned in selected pa-tients without threatened circumferential radialmargin (CRM) where local failure is approximately
10 % with TME alone. In addition, an approach ofneoadjuvant chemotherapy, without radiation, of-fers a potential alternative and is an area of activeinvestigation. This review will focus on radiation-based neoadjuvant approaches, short-course RTand long-course CRT, assessing relative strengthsand drawbacks to each approach while presentingavailable data.
Short-course radiotherapy
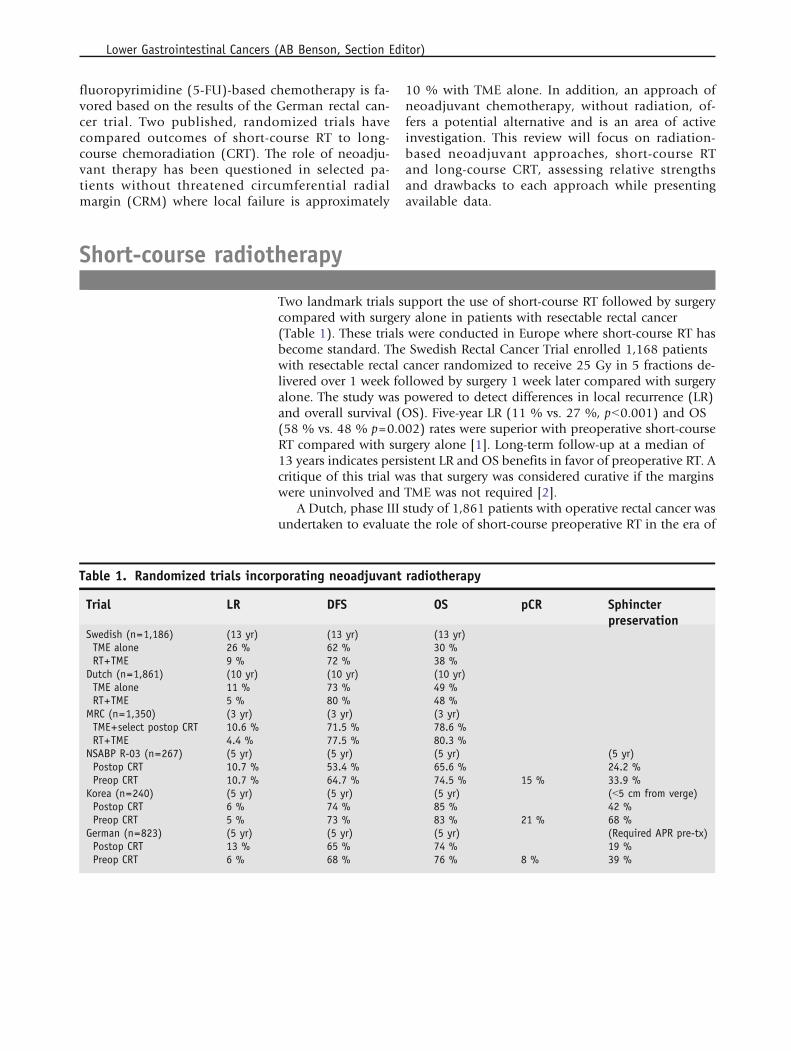
Two landmark trials support the use of short-course RT followed by surgerycompared with surgery alone in patients with resectable rectal cancer(Table 1). These trials were conducted in Europe where short-course RT hasbecome standard. The Swedish Rectal Cancer Trial enrolled 1,168 patientswith resectable rectal cancer randomized to receive 25 Gy in 5 fractions de-livered over 1 week followed by surgery 1 week later compared with surgeryalone. The study was powered to detect differences in local recurrence (LR)and overall survival (OS). Five-year LR (11 % vs. 27 %, pG0.001) and OS(58 % vs. 48 % p=0.002) rates were superior with preoperative short-courseRT compared with surgery alone [1]. Long-term follow-up at a median of13 years indicates persistent LR and OS benefits in favor of preoperative RT. Acritique of this trial was that surgery was considered curative if the marginswere uninvolved and TME was not required [2].
A Dutch, phase III study of 1,861 patients with operative rectal cancer wasundertaken to evaluate the role of short-course preoperative RT in the era of
Table 1. Randomized trials incorporating neoadjuvant radiotherapy
Trial LR DFS OS pCR Sphincterpreservation
Swedish (n=1,186) (13 yr) (13 yr) (13 yr)TME alone 26 % 62 % 30 %RT+TME 9 % 72 % 38 %
Dutch (n=1,861) (10 yr) (10 yr) (10 yr)TME alone 11 % 73 % 49 %RT+TME 5 % 80 % 48 %
MRC (n=1,350) (3 yr) (3 yr) (3 yr)TME+select postop CRT 10.6 % 71.5 % 78.6 %RT+TME 4.4 % 77.5 % 80.3 %
NSABP R-03 (n=267) (5 yr) (5 yr) (5 yr) (5 yr)Postop CRT 10.7 % 53.4 % 65.6 % 24.2 %Preop CRT 10.7 % 64.7 % 74.5 % 15 % 33.9 %
Korea (n=240) (5 yr) (5 yr) (5 yr) (G5 cm from verge)Postop CRT 6 % 74 % 85 % 42 %Preop CRT 5 % 73 % 83 % 21 % 68 %
German (n=823) (5 yr) (5 yr) (5 yr) (Required APR pre-tx)Postop CRT 13 % 65 % 74 % 19 %Preop CRT 6 % 68 % 76 % 8 % 39 %
Lower Gastrointestinal Cancers (AB Benson, Section Editor)

TME. TME is a surgical technique championed by a surgeon, Dr. WilliamHeald, requiring en bloc removal of the tumor with sharp dissection alongthe plane that separates the visceral from the parietal pelvic fascia. Patientswith resectable rectal cancer were randomized to TME alone versus 25 Gy in5 fractions followed by TME. Nearly half of the patients enrolled in this studyhad T1-T2 disease. Despite the preponderance of early-stage tumors, the2 year LR was 8.2 % in the TME arm compared with 2.4 % in the preoper-ative RT arm (pG0.001). There was no difference in 2-year OS. Ten-yearfollow-up indicated persistent benefit in LR of 5 % with RT versus 11 % withTME alone (pG0.0001) [3, 4]. These data highlight the value of preoperativeRT even with the use of TME.
In the era of improved surgical technique, preoperative staging, and rigor-ous histologic assessment, the MRC CR07 trial reevaluated the role of pre-operative RT. A total of 1,350 patients with resectable rectal cancer wererandomized to preoperative RT (25 Gy in 5 fractions) or upfront surgicalresection with selective postoperative CRT (45 Gy in 25 fractions with con-current 5-FU) in patients with a ≤1-mm CRM. All patients underwent rig-orous pathologic evaluation [5••]. At median follow-up of 4 years, LR waslower in the preoperative RT group (4.4 % vs. 10.6 %, hazard ratio (HR)0.39, pG0.001). Although 3-year, disease-free survival (DFS) was improved inthe preoperative RT group (77.5 % vs. 71.5 %, HR 0.76, p=0.013), there wasno difference in OS [6]. This effort to identify patients at high risk of recur-rence after attempted TME resection and administration of selective post-operative CRT based on pathologic review was inferior to nonselectiveupfront preoperative short-course RT.
Long-course radiotherapy
A number of phase III trials have evaluated the role of long course CRT. Inthe 1990s, postoperative CRT was considered standard adjuvant therapy instage II-III rectal cancer with studies demonstrating a 10-15 % survival ad-vantage with the addition of chemotherapy to adjuvant radiotherapy [7, 8].Given the toxicity associated with postoperative therapy, neoadjuvant CRTwas evaluated in a number of phase III, randomized trials (Table 1). TheNational Surgical Adjuvant Breast and Bowel Project (NSABP) R-03 studywas originally designed to accrue 900 patients but was closed prematurelyafter only accruing 267. Patients with clinical T3-T4 and/or node-positiveadenocarcinoma were randomized to surgery followed by one cycle of 5-FU/leucovorin (LV) and then concurrent 5-FU/LV with radiotherapy versus onecycle of 5-FU/LV and concurrent, neoadjuvant CRT followed by surgery. Allpatients received adjuvant 5-FU/LV for four cycles. Although the study wasunderpowered given limited accrual, 5-year DFS was superior in the preop-erative therapy group: 64.7 % versus 53.4 % (p=0.011). There was a trend,although not statistically significant, toward improved 5-year OS with pre-operative therapy: 74.5 % versus 65.6 % (p=0.065) [9].
A Korean randomized trial of 240 patients with locally advanced T3-T4and/or node positive rectal cancer evaluated preoperative or postoperativeCRT. CRT consisted of 50 Gy in 25 fractions with concurrent capecitabine
Short-Course Radiotherapy versus Long-Course Chemoradiation in Rectal Cancer Palta et al.
(1650 mg/m2 per day). The standard surgical procedure was TME and pa-tients received four cycles of adjuvant chemotherapy with either capecitabineor 5-FU. Although there were no differences in 5-year DFS, OS, or LR, pa-tients with low-lying rectal tumors (G5 cm from the anal verge) had higherrates of sphincter preservation in the preoperative CRT group: 68 % versus42 % (p=0.041) [10].
The definitive, phase III study in favor of preoperative CRT conducted bythe German Rectal Cancer Group resulted in a paradigm shift towards neo-adjuvant CRT. A total of 823 patients clinically staged T3-T4 and/or nodepositive rectal cancers were randomized to preoperative CRT followed bysurgery 6 weeks later or surgery followed by postoperative CRT. The radiationdose was 50.4 Gy in 28 fractions in all patients with a 5.4 Gy small-volumeboost in the postoperative arm. Radiation was delivered with concurrent 5-FU, and all patients underwent TME. Before treatment, surgeons evaluatedthe possibility of sphincter preservation, a secondary study endpoint. Five-year results revealed a pelvic recurrence rate of 6 % versus 13 % (p=0.006, HR0.46) in favor of the preoperative CRT arm. Sphincter preservation in 188patients with low-lying tumors declared by the surgeon prior to randomi-zation to require an abdominoperineal resection (APR) revealed that morepatients in the former group (39 % vs. 19 %, p=0.004) underwent sphincter-sparing surgery. In addition, acute and late toxicity rates were lower in thepreoperative arm [11]. Updated results, with a median follow-up of 11 years,indicate consistent benefit in the preoperative arm with a 10-year LR of 7.1 %compared with 10.1 % [12••]. There continues to be no difference in distantmetastases, DFS, or OS.
Comparison of short-course RT and long-course chemoradiation
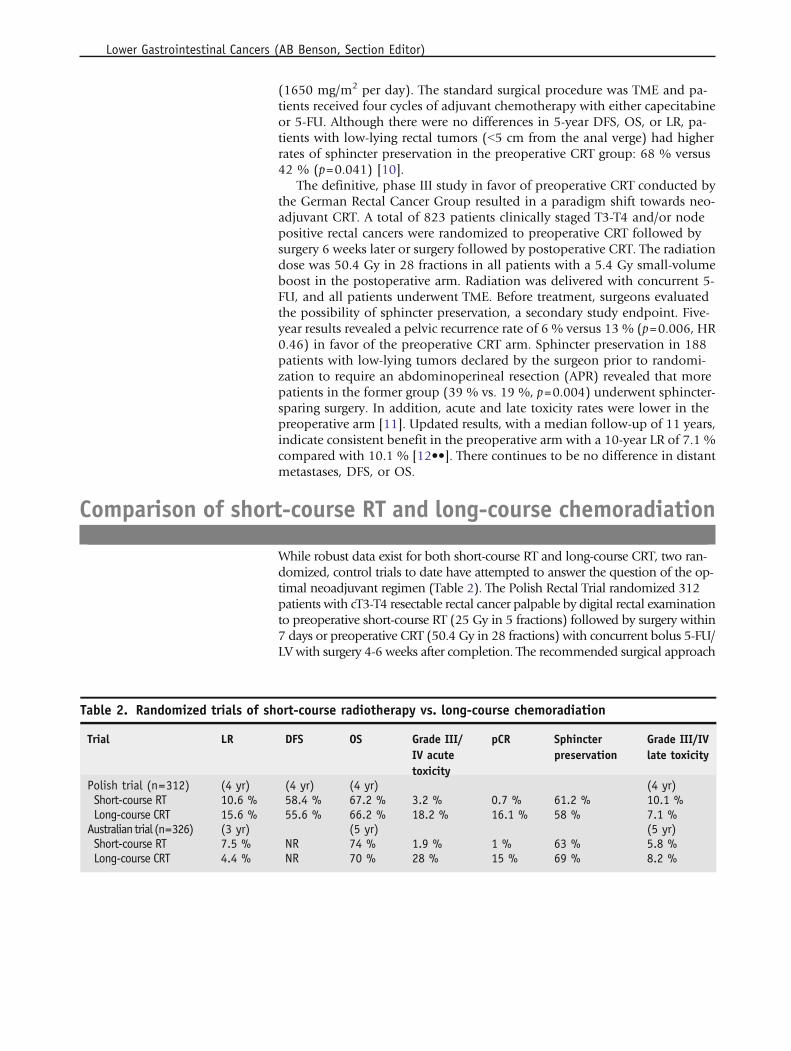
While robust data exist for both short-course RT and long-course CRT, two ran-domized, control trials to date have attempted to answer the question of the op-timal neoadjuvant regimen (Table 2). The Polish Rectal Trial randomized 312patients with cT3-T4 resectable rectal cancer palpable by digital rectal examinationto preoperative short-course RT (25 Gy in 5 fractions) followed by surgery within7 days or preoperative CRT (50.4 Gy in 28 fractions) with concurrent bolus 5-FU/LV with surgery 4-6 weeks after completion. The recommended surgical approach
Table 2. Randomized trials of short-course radiotherapy vs. long-course chemoradiation
Trial LR DFS OS Grade III/IV acutetoxicity
pCR Sphincterpreservation
Grade III/IVlate toxicity
Polish trial (n=312) (4 yr) (4 yr) (4 yr) (4 yr)Short-course RT 10.6 % 58.4 % 67.2 % 3.2 % 0.7 % 61.2 % 10.1 %Long-course CRT 15.6 % 55.6 % 66.2 % 18.2 % 16.1 % 58 % 7.1 %
Australian trial (n=326) (3 yr) (5 yr) (5 yr)Short-course RT 7.5 % NR 74 % 1.9 % 1 % 63 % 5.8 %Long-course CRT 4.4 % NR 70 % 28 % 15 % 69 % 8.2 %
Lower Gastrointestinal Cancers (AB Benson, Section Editor)

was TME, with adjuvant chemotherapy at the discretion of the treatingphysician. The primary study end point was sphincter preservation, andat a median follow-up of 48 months there was no benefit from aprotracted course of CRT with 61 % of patients undergoing sphincter-sparing surgery after short-course RT and 58 % after CRT (p=0.57). Inaddition, there were no differences in DFS or OS and a nonsignificantlower rate of actuarial LR in the short-course RT arm at 10.6 % com-pared with 15.6 % with CRT (p=0.21). Acute Grade 3/4 toxicity washigher in the CRT arm (3.2 % vs. 18.2 %) with no difference in latetoxicity [13].
There are a number of caveats with these data. The study was designedwith power to detect a 15 % difference in sphincter preservation rates, andsmall differences between short- and long-course RT would not be apparentdespite inclusion of patients with T3-T4 disease. Nearly 40 % of the patientsin the short-course arm had pathologic T1-T2 disease and should not havebeen included on study by eligibility criteria. Despite the use of TME, the LRrates in the Polish trial are higher than those reported in other studies (e.g.,the Dutch TME trial) utilizing this surgical technique. There also is somequestion as to surgeon familiarity with CRT downstaging effect and potentialreluctance to alter planned surgery to a sphincter-preserving LAR. In addition,with a median follow-up of 4 years, this time interval may be too short forassessment of late toxicities that may manifest later when larger doses perfraction are administered.
A second, randomized, control trial evaluated long-course CRT comparedwith short-course RT in 326 patients with T3 N0-2 rectal adenocarcinoma.Short-course RT consisted of 25 Gy in 5 fractions with surgery 3-7 days laterversus long-course CRT (50.4 Gy with continuous infusion 5-FU) and surgeryin 4-6 weeks. All patients underwent TME with planned four cycles of ad-juvant chemotherapy. The primary study end point was 3-year LR. Aftermedian follow-up of 5.9 years, the 3-year LR was 7.5 % for short-course RTand 4.4 % for long-course RT (p=0.24). There was no difference in distantmetastases, DFS, or OS. With limited follow-up, late toxicities were notsubstantially different between the two arms [14••].
There are a number of advantages with each respective neoadjuvant RTapproach. Given that surgery typically occurs within 10 days of preopera-tive short-course RT, as well as the absence of concurrent chemotherapy de-livery, rates of Grade 3/4 acute toxicity are typically lower with short-courseRT compared with CRT as demonstrated in both the Polish and Australiantrials. Given the overall shortened course of neoadjuvant therapy, there arehigher rates of compliance with protocol therapy. Compliance in the Polishtrial was 98 %, whereas 100 % completed short-course RT in the Australianstudy. This five-fraction regimen also is lower in cost and more convenientfor patients.
Long-course CRT also has associated advantages. Although both thePolish and Australian trials showed no improvement in sphincter preserva-tion, larger trials, such as the German Rectal Cancer Trial, demonstrated bothtumor downstaging and higher rates of sphincter-sparing surgery in patientswith low-lying rectal malignancies. APR has been associated with highermorbidity and mortality rates compared with a LAR with worse quality of liferelated to changes in body image and depression due to presence of a co-
Short-Course Radiotherapy versus Long-Course Chemoradiation in Rectal Cancer Palta et al.

lostomy [15]. Tumor downstaging is commonly seenwith CRT and pathologiccomplete response rates (pCR) in randomized trials range from approximately10-30 %. Patients achieving a pCR have enhanced long-term outcomes com-pared with nonresponders and, in select situations, may be able to avoidsurgery with rigorous surveillance. Comparison across trials suggest the R0resection rate in the Swedish and Dutch rectal cancer trials was roughly 77 %despite inclusion of patients who had mobile/resectable rectal cancers com-pared with a nearly 85 % rate of R0 resection in trials implementing CRT.Although late toxicity in the Polish and Australian trials was no different withlimited follow-up, basic radiobiologic principles dictate that larger fractionsize has a higher risk of late toxicities, which can manifest in subsequent de-cades. Longer follow-up from the Australian and Polish Rectal Cancer Trials isneeded to adequately assess LR, which increases over time and late toxicitydifferences with short-course RT and long-course CRT.
Future studies
Two additional, randomized trials are evaluating the role of short-course RT andlong-course CRT. The Stockholm III study seeks to answer the question of optimalneoadjuvant fractionation regimen and timing of surgery. This study initiated in1998 and closed in 2009 with a planned 840 patients with resectable rectal cancerrandomized to one of the three following arms: preoperative short-course RT(25 Gy in 5 fractions, with surgery within 1 week); preoperative short-course RT(25 Gy in 5 fractions, with surgery after 4-8 weeks); or preoperative long-course RTalone (50 Gy in 25 fractions) with surgery in 4-8 weeks. The primary study endpoint is LR. Interim analysis showed no difference in Grade 3/4 acute toxicity orpostoperative complication rates. The percentage of patients undergoing APR waslower, although not statistically significant, in the long-course RT arm comparedwith either short-course RT arm. Mature results from this study are awaited [16].
A second study evaluating the question of short course RT versus CRT is theBerlin Rectal Cancer Trial, which commenced in 2004. Patients with T2N+orT3 rectal cancer are randomized to short-course RT (25 Gy in 5 fractions) or CRT(50.4 Gy in 28 fractions with 5-FU). Both groups are scheduled to undergo TMEand 12weeks of adjuvant 5-FU-based chemotherapy. The primary end point is 5-year LR with secondary outcomes of DFS, OS, quality of life, R0 resection rate,sphincter preservation, and acute and late toxicity rates [17]. These trials shouldhelp to clarify the question of the optimal preoperative fractionation regimen andtiming of surgical resection.
Conclusions
For the treatment of locally advanced rectal cancer, neoadjuvant therapy is stan-dard; however, the optimal neoadjuvant approach for resectable rectal cancer isfar from clear. Both short-course RT and long-course CRT represent reasonabletherapeutic options with randomized data supporting either approach. ThePolish and Australian Intergroup trials directly comparing short-course RT andlong-course CRT demonstrated no difference in sphincter-sparing surgery or localrecurrence with limited follow-up. Mature results, including comparative long-term toxicity data, are lacking. As new and long-term data from randomized
Lower Gastrointestinal Cancers (AB Benson, Section Editor)
control trials comparing short- and long-course RT emerge, the optimal neoad-juvant therapy regimen may be more clearly defined.
Compliance with Ethics Guidelines
Conflict of InterestManisha Palta, Christopher G. Willett, and Brian G. Czito declare that they have no conflict of interest.
Human and Animal Rights and Informed ConsentThis article does not contain any studies with human or animal subjects performed by any of the authors.
References and Recommended ReadingPapers of particular interest, published recently, have beenhighlighted as:•• Of major importance
1. Improved survival with preoperative radiotherapy inresectable rectal cancer. Swedish Rectal Cancer Trial.N Engl J Med. 1997; 336(14):980–7.
2. Folkesson J et al. Swedish Rectal Cancer Trial: longlasting benefits from radiotherapy on survival andlocal recurrence rate. J Clin Oncol. 2005;23(24):5644–50.
3. Kapiteijn E et al. Preoperative radiotherapy com-bined with total mesorectal excision for resectablerectal cancer. N Engl J Med. 2001;345(9):638–46.
4. van Gijn W et al. Preoperative radiotherapy com-bined with total mesorectal excision for resectablerectal cancer: 12-year follow-up of the multicentre,randomised controlled TME trial. Lancet Oncol.2011;12(6):575–82.
5.•• Quirke P et al. Effect of the plane of surgery achievedon local recurrence in patients with operable rectalcancer: a prospective study using data from the MRCCR07 and NCIC-CTG CO16 randomised clinical tri-al. Lancet. 2009;373(9666):821–8.
This study incorporated rigorous pathologic evaluation of sur-gical specimens as part of the MRC CR07 randomized trial.Interestingly , although TME was standard, only 50 % of pa-tients had true TME, after pathologic evaluation. In patientsundergoing TME and preoperative RT, local failure was 1 %.6. Sebag-Montefiore D et al. Preoperative radiotherapy
versus selective postoperative chemoradiotherapy inpatients with rectal cancer (MRC CR07 and NCIC-CTG C016): a multicentre, randomised trial. Lancet.2009;373(9666):811–20.
7. Thomas PR, Lindblad AS. Adjuvant postoperativeradiotherapy and chemotherapy in rectal carcinoma:a review of the Gastrointestinal Tumor Study Groupexperience. Radiother Oncol. 1988;13(4):245–52.
8. Krook JE et al. Effective surgical adjuvant therapy forhigh-risk rectal carcinoma. N Engl J Med. 1991;324(11):709–15.
9. Roh MS et al. Preoperative multimodality therapyimproves disease-free survival in patients with carci-noma of the rectum: NSABP R-03. J Clin Oncol.2009;27(31):5124–30.
10. Park JH et al. Randomized phase 3 trial comparingpreoperative and postoperative chemoradiotherapywith capecitabine for locally advanced rectal cancer.Cancer. 2011;117(16):3703–12.
11. Sauer R et al. Preoperative versus postoperative che-moradiotherapy for rectal cancer. N Engl J Med.2004;351(17):1731–40.
12.•• Sauer R et al. Preoperative versus postoperativechemoradiotherapy for locally advanced rectalcancer: results of the German CAO/ARO/AIO-94randomized phase III trial after a median follow-up of 11 years. J Clin Oncol. 2012;30(16):1926–33.
Updated results from the German Rectal Cancer study indi-cating persistent local control benefit assocated with pre-operative chemoradiation.13. Bujko K et al. Long-term results of a randomized trial
comparing preoperative short-course radiotherapywith preoperative conventionally fractionated che-moradiation for rectal cancer. Br J Surg. 2006;93(10):1215–23.
14.•• Ngan SY et al. Randomized trial of short-courseradiotherapy versus long-course chemoradiationcomparing rates of local recurrence in patientswith t3 rectal cancer: trans-tasman radiation on-cology group trial 01.04. J Clin Oncol. 2012;30(31):3827–33.
Short-Course Radiotherapy versus Long-Course Chemoradiation in Rectal Cancer Palta et al.
One of two randomized trials addressing the question of op-timal neoadjuvant regimen: long course chemoradiation orshort course RT befroe surgery. Primary study endpoint was 3-year local control.15. Grumann MM et al. Comparison of quality of life in
patients undergoing abdominoperineal extirpationor anterior resection for rectal cancer. Ann Surg.2001;233(2):149–56.
16. Pettersson D et al. Interim analysis of the StockholmIII trial of preoperative radiotherapy regimens forrectal cancer. Br J Surg. 2010;97(4):580–7.
17. Siegel R et al. Preoperative short-course radiotherapyversus combined radiochemotherapy in locally ad-vanced rectal cancer: a multi-centre prospectivelyrandomised study of the Berlin Cancer Society. BMCCancer. 2009;9:50.
Lower Gastrointestinal Cancers (AB Benson, Section Editor)