Embed Size (px)
Citation preview


Short Bowel Syndrome/
High Output Stoma
Professor Simon Lal

Surgical history
Right hemicolectomy
Panproctocolectomy
Small bowel resections x 2
Case History: Background
Medical history
5-ASAs/Recurrent Steroids
Azathioprine: intolerance
Infliximab: anaphylaxis
46 year old female
Crohn’s disease 1996

Surgical history
Right hemicolectomy
Panproctocolectomy
Small bowel resections x 2
Case History: Background
46 year old female
Crohn’s disease 1996

Surgical history
Right hemicolectomy
Panproctocolectomy
Small bowel resections x 2
Case History: Background
46 year old female
Crohn’s disease 1996
November - December 2013
Ileostomy re-fashioned, complicated SI resection
High output stoma
Readmitted dehydrated surgeons advised to drink more

46 year old female, high output stoma
Thirst, lethargy, muscle cramps, dizzy
Dehydrated. BP 85/50.
Stoma output > 2.5 L.
Wt = 43kg BMI = 16
FY2 Plan:
i.v. saline & i.v. magnesium.
Aim for home tomorrow pending repeat bloods.
Senior Review.
Case History: EAU 2014
Na K Urea Creat Alb CCa Phos Mg CRP
129 4.9 12 154 49 1.94 1.3 0.48 5
133-146 3.5-5.3 2.5-7.8 44-97 35-50 2.2-2.6 0.8-1.5 0.7-1.0 <10

SBS
Does she require
admission?
Why is her albumin normal?
How optimise
fluid balance?
How correct
Mg?
Will she need long term HPN?

SBS
Does she require
admission?
SBS
Why is her albumin normal?

46 year old female, high output stoma
Thirst, lethargy, muscle cramps, dizzy
Dehydrated. BP 85/50.
Stoma output > 2.5 L.
Wt = 43kg BMI = 16
Na K Urea Creat Alb CCa Phos Mg CRP
129 4.9 12 154 49 1.94 1.3 0.48 5
133-146 3.5-5.3 2.5-7.8 44-97 35-50 2.2-2.6 0.8-1.5 0.7-1.0 <10
Poor nutritional marker
Negative acute phase protein
Case History: Serum Albumin
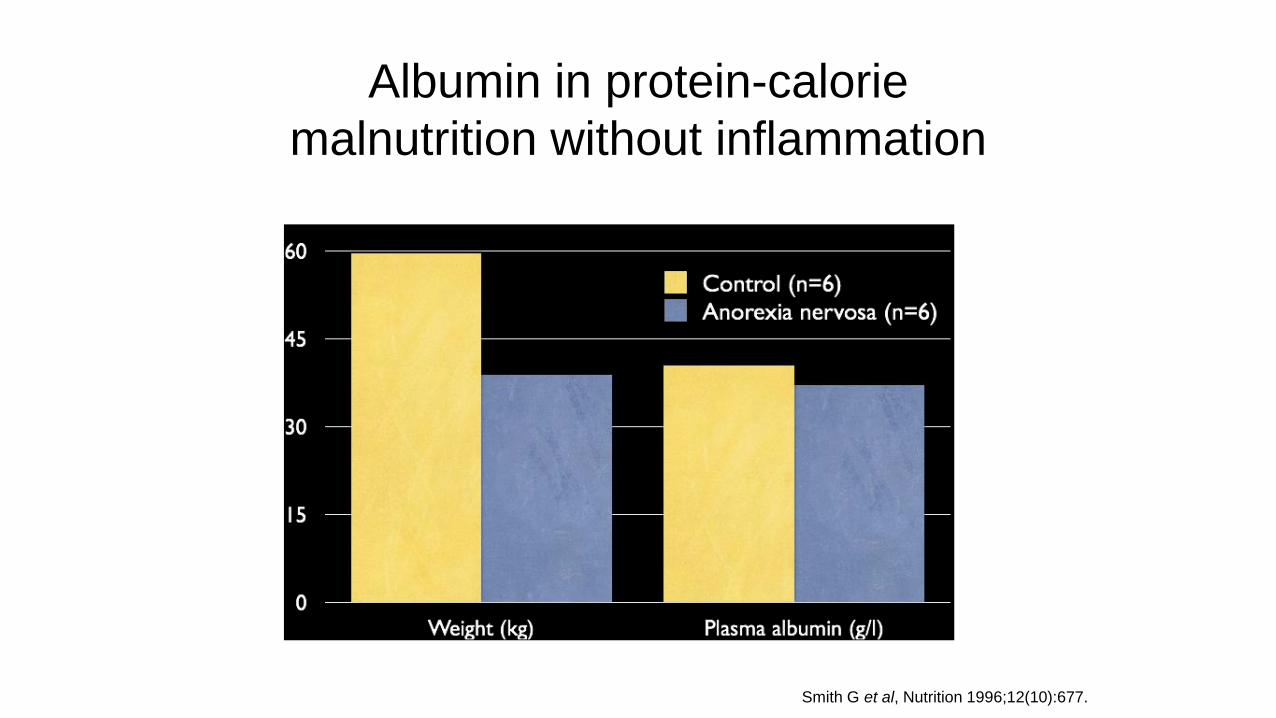
Albumin in protein-calorie
malnutrition without inflammation
**
Smith G et al, Nutrition 1996;12(10):677.

What happened to his albumin?

What happened to his albumin?

SBS
How optimise
fluid balance?

46 year old female, high output stoma
Thirst, lethargy, muscle cramps, dizzy
Dehydrated. BP 85/50.
Stoma output > 2.5 L.
Wt = 43kg BMI = 16
Na K Urea Creat Alb CCa Phos Mg CRP
129 4.9 10 154 49 1.94 1.3 0.48 5
133-146 3.5-5.3 2.5-7.8 44-97 35-50 2.2-2.6 0.8-1.5 0.7-1.0 <10
Dehydration & Renal impairment in SBS
1. Malnourished: Significant renal dysfunction.
2. Recurrent dehydration despite drinking more.
Case History: Renal Function
Why?

A bit of
physiology
(!)….

NORMAL: NET ABSORBER
DRINK MORE ABSORB MORE
SI < ~150cm NET SECRETOR
Normal proximal secretion is not
compensated by distal absorption
DRINK MORE ABSORB LESS
Thirst needs less drinking!

Fluid & Nutritional Assessment
Fluid Nutrition
Accurate fluid balance vital
Intake
Stoma
Urine
48 hours NBM Minimal
stoma loss.
Urine Na best gauge of
hydration status
Urine sodium
< 20mmol
dehydration

Fluid & Nutritional Assessment
Fluid Nutrition
Accurate fluid balance vital
Intake
Stoma
Urine
48 hours NBM Minimal
stoma loss.
Urine Na best gauge of
hydration status
Assessment
Wt, BMI
Anthropometry
Hand-grip strength
Diet history & food charts
Dietitian best gauge of
nutritional status!

BSG Guidelines, Gut, 2006 Lal S Alimen Pharm Ther 2006; 24: 19-31
SBS Treatment
Drug therapyAnti-motility
Loperamide (up to 16mg QDS)
Codeine phosphate (up to 60mg QDS)
Anti-secretoryPPI Stoma pH>5.5
?Octreotide
Restrict hypotonic fluid < 1L/day
Drink glucose-saline solution ~ 1L/day
Nutrition Dietetic Review

BSG Guidelines, Gut, 2006 Lal S Alimen Pharm Ther 2006; 24: 19-31
SBS Treatment
Restrict hypotonic fluid < 1L/day
Drink glucose-saline solution ~ 1L/day
SI < ~150cm NET SECRETOR
Normal proximal secretion is not
compensated by distal absorption

SBS Treatment
Restrict hypotonic fluid < 1L/day
Drink glucose-saline solution ~ 1L/day

SBS Treatment
Restrict hypotonic fluid < 1L/day
Drink glucose-saline solution ~ 1L/day

SBS Treatment
Restrict hypotonic fluid < 1L/day
Drink glucose-saline solution ~ 1L/day
Sodium content must
be > 90mmol/L to
achieve a POSITIVE
sodium balance.
Rodrigues et al. (1988) Clin Sci;74:69P
Nightingale et al (1992) Gut; 33:759-761

Nammol/l
Kmmol/l
Glucosemmol/l
Volumeml
WHO 90 20 111 1000
‘St Mark’s Solution’ 90 0 111 1000
Dioralyte 60 20 90 200
Powerade isotonic 12 4 0 (214) sucrose & maltodextrin
600
Powerade isotonic+ ½teaspoon NaCl
85 4 0 (214) sucrose & maltodextrin
600
Double Strength Dioralyte
Oral Rehydration Solutions

BSG Guidelines, Gut, 2006 Lal S Alimen Pharm Ther 2006; 24: 19-31
SBS Treatment
Drug therapyAnti-motility
Loperamide (up to 16mg QDS)
Codeine phosphate (up to 60mg QDS)
Anti-secretoryPPI Stoma pH>5.5
?Octreotide
Restrict hypotonic fluid < 1L/day
Drink glucose-saline solution ~ 1L/day

-125
-100
-75
-50
-25
0
25
50
Sod
ium
bal
ance
(m
mo
l/d
ay)
control
loperamide
codeineloperamide
& codeine
ranitidine
ORS
loperamide
codeine
ORS
Nightingale JMD et al. Clin Nutr 1992; 11: 101-5
Sodium balancePatient with jejunostomy at 100 cm

Nutrition Dietetic Review
SBS Management
Drug therapyAnti-motility
Loperamide (up to 16mg QDS)
Codeine phosphate (up to 60mg QDS)
Anti-secretoryPPI Stoma pH>5.5
?Octreotide
Restrict hypotonic fluid < 1L/day
Drink glucose-saline solution ~ 1L/day

Jejunostomy: recommended diet
Nutrient group Amount Note
Energy High 30-60 kcal/kg/day
Protein High 0.2-0.25g N2/kg/day (80-100g protein)
Fat High
Fibre Low

BSG Guidelines, Gut, 2006 Lal S Alimen Pharm Ther 2006; 24: 19-31
SBS Treatment
Drug therapyAnti-motility
Loperamide (up to 16mg QDS)
Codeine phosphate (up to 60mg QDS)
Anti-secretoryPPI Stoma pH>5.5
?Octreotide
Restrict hypotonic fluid < 1L/day
Drink glucose-saline solution ~ 1L/day
Nutrition Dietetic Review

SBS
How correct
Mg?

46 year old female, high output stoma
Thirst, lethargy, muscle cramps, dizzy
Dehydrated. BP 85/50.
Stoma output > 2.5 L.
Wt = 43kg BMI = 16
Na K Urea Creat Alb CCa Phos Mg CRP
129 4.9 10 154 49 1.94 1.3 0.48 5
133-146 3.5-5.3 2.5-7.8 44-97 35-50 2.2-2.6 0.8-1.5 0.7-1.0 <10
Magnesium
FY2 Plan:
i.v. saline & i.v. magnesium.
Aim for home tomorrow pending repeat bloods.
Senior Review.

Hypomagnesaemia: Management
Intravenous
MagnesiumNot sustained because rapidly excreted

Hypomagnesaemia: Management
Intravenous
MagnesiumNot sustained because rapidly excreted
Sodium/Water
DepletionCorrect (reduced 20 hyperaldosteronism)
Oral
Magnesium
Vitamin D
PPI Rare with chronic use Don’t forget
Mg Oxide or Aspartate
Mg glycerophosphate X
Dose titration
Vital
Intramuscular or high dose oral

46 year old female, high output stoma
Thirst, lethargy, muscle cramps, dizzy
Dehydrated. BP 85/50.
Stoma output > 2.5 L.
Wt = 43kg BMI = 16
Na K Urea Creat Alb CCa Phos Mg CRP
129 4.9 10 154 49 1.94 1.3 0.48 5
133-146 3.5-5.3 2.5-7.8 44-97 35-50 2.2-2.6 0.8-1.5 0.7-1.0 <10
Calcium & Potassium
Potassium
Hyperaldosteronism in chronic Na deficiency
Negative K+ balance if < 50cm small bowel

SBS
Will she need long term HPN?

Dibb M et al. APT 37(6):587-603
Length matters….
~<100cm Small Bowel
Parenteral Support
Influenced by active disease
Influenced by colon in continuity

Surgical history
Right hemicolectomy
Panproctocolectomy
Small bowel resections x 3
Post-op Small Bowel Length
46 year old female. Crohn’s disease 1996
Adult small bowel 3 - 8.5m
Males > Females
Post-op: How much remaining
not how much removed!

Not enough small bowel =
Home Parenteral Nutrition
Single lumen, PN Dedicated Tunnelled Catheter.
12-14 hours infusion up to 7 nights per week.
Patient or carer: 2-6 weeks training to administer.
Home Care nursing teams: adherence to catheter care protocol.

HPN
COMPLICATIONS
Catheter Infection
Venous Thromboisis
Hepato-biliary
Renal
Metabolic Bone Disease
Psychological
Dibb M, Teubner A, Theiss V, Shaffer J, Lal S APT 2013

CVC Longevity in Intestinal Failure
Repeated catheter loss failed
venous access: indication for a
small bowel transplant.
Ethos of meticulous catheter
care. Only access if trained to protocol
(unless medical emergency).
Dedicated to PN only.
No blood sampling.
Salford IFU: Lowest sustained CVC infection rate.
Longest surviving patient: 34 yrs.
Longest CVC: 16 yrs.
HPN Survival
ITx Survival
Dibb M et al. 2013 APT 37(6):587-603
Dibb M et al 2016 JPEN Epub ahead of print

Case History: Successful Outcome
~150 cm
Op notes (+ contrast study): ~150cm
No sign of active Crohn’s.
Stoma output < 1L, Urine Output >1L
<1L hypotonic fluid restriction
1L D.S. Dioralyte
Loperamide 32mg
Codeine 30mg qds
Omeprazole 20mg b.d.
Mg Aspartate 1 sachet t.d.s.
Vitamin D optimised
GP Blood monitoring.
Dietetic & Gastro Clinic Follow-up
Nutritional progress
Crohn’s prevention vigilance for
recurrence

Case History: Successful Outcome
~150 cm
Op notes (+ contrast study): ~150cm
No sign of active Crohn’s.
Stoma output < 1L, Urine Output >1L
<1L hypotonic fluid restriction
1L D.S. Dioralyte
Loperamide 32mg
Codeine 30mg qds
Omeprazole 20mg b.d.
Mg Aspartate 1 sachet t.d.s.
Vitamin D optimised
GP Blood monitoring.
Dietetic & Gastro Clinic Follow-up
Nutritional progress
Crohn’s prevention vigilance for
recurrence

SBS
Does she require
admission?
Why is her albumin normal?
How optimise
fluid balance?
How correct
Mg?
Will she need long term HPN?

Thank-you





























