Embed Size (px)
Citation preview

P1: GCY
Journal of Genetic Counseling [jgc] ph250-jogc-480246 March 8, 2004 10:23 Style file version Nov 28th, 2002
Journal of Genetic Counseling, Vol. 13, No. 2, April 2004 ( C© 2004)
Short- and Long-Term Impact of Receiving GeneticMutation Results in Women at Increased Risk forHereditary Breast Cancer
Jacqueline Lim,1 Mariette Macluran,1 Melanie Price,1 Barbara Bennett,2
Phyllis Butow,3,5 and the kConFab Psychosocial Group4
Forty-seven unaffected women from high-risk breast cancer families who had re-ceived results for hereditary breast/ovarian predisposition genes between 1 monthand 5 years ago were interviewed regarding their experiences. Women respondedto open-ended questions. The initial emotional turmoil reported by most was gener-ally short lived. However, the impact of genetic testing went beyond the individualto the extended family and social context, particularly in the short-term. A com-mon theme was the difficulty associated with divulging a result to family members,who were also adjusting to their own result. The majority of carriers reportedadvantages that were both physical (options for surveillance programs and pro-phylactic surgery) and emotional (reduced uncertainty, increased awareness ofoptions and knowledge about risk, preparation time). Most carriers reported nochange in lifestyle although some reported discovering their mutation status as apositive life-changing experience. Implications for genetic counseling and furtherresearch are discussed.
KEY WORDS: genetic test results; psychological response; BRCA1 and BRCA2.
1Psychological Medicine, Royal North Shore Hospital, Sydney, Australia.2Department of Medical Oncology, Prince of Wales Hospital, Sydney, Australia.3Medical Psychology Research Unit, University of Sydney, Sydney, Australia.4Kathleen Cuningham National Consortium for Research into Familial Breast Cancer PsychosocialGroup. Members in alphabetical order of group, institute or location: Familial Cancer Centre, PeterMacCallum Cancer Institute (S. A. McLachlan, K. A. Phillips); Department of Medical Oncology,Prince of Wales Hospital (B. Bennett, B. Meiser, K. Tucker); Department of Psychological Medicine,Royal North Shore Hospital (J. Lim, M. Maclurcan, M. Price, C. Tennant); Department of PublicHealth, University of Melbourne (C. Apicella); Department of Psychiatry, University of NSW (I.Hickie); School of Public Health (G. Berry) and Medical Psychology Research Unit (P. Butow),University of Sydney.
5Correspondence should be directed to Phyllis Butow, Medical Psychology Research Unit, BlackburnBuilding (D06), University of Sydney, Sydney, Australia; e-mail: [email protected].
115
1059-7700/04/0400-0115/1 C© 2004 National Society of Genetic Counselors, Inc.

P1: GCY
Journal of Genetic Counseling [jgc] ph250-jogc-480246 March 8, 2004 10:23 Style file version Nov 28th, 2002
116 Lim et al.
INTRODUCTION
There has been exponential growth in our knowledge of the human genomeover the last decade. Predictive testing for familial susceptibility for disorders suchas Huntington’s disease and hereditary breast/ovarian cancer (HBOC) is now pos-sible. The sequencing of breast cancer predisposition genes, BRCA1 and BRCA2,has enabled mutation analysis-based testing to be performed. Having an inheritedgermline mutation (either BRCA1 or BRCA2) in the setting of a strong family his-tory of the disease conveys a 31–78% lifetime risk of breast cancer, and a 2–54%lifetime risk of ovarian cancer (Antoniou et al., 2003).
Information about risk is now readily available to women from high-riskbreast cancer families through genetic counseling services. Ethically, it is impor-tant to ensure that such knowledge creates more benefits than harms. Knowledge ofpositive mutation status potentially provides women with a clearer basis on whichto make decisions regarding options to actively reduce their lifetime risk, (e.g.,active surveillance for early signs of disease, prophylactic surgery), and more re-cently, chemoprevention. Benefits for noncarriers, whose risk of developing breastcancer is similar to that of the general population, potentially includes relief frompersistent worry and the need for heightened surveillance or prophylactic surgery.There are, however, limitations associated with knowledge of genetic mutationstatus. BRCA1/2 mutation carriers do not know when and even if they will getthe disease. Unlike many diseases, inherited cancers have an identified cause andorigin, which can influence self-concept and self-esteem. Knowledge of mutationstatus may also have implications for health insurance or employment. Finally,genetic information carries implications not just for the individual presenting forcounseling, but for the entire family, some of whom may not want such information.
Although the short-term benefits for individual mutation carriers of knowingtheir mutation status have been well established, less is known about the long-termimpact for both the individual and family, although such studies are currently un-derway. To date, studies have followed women for at the most 12 months postresultdisclosure (Butow et al., 2003; Hutson, 2003; Meiser et al., 2002). Furthermore,most of these early studies have been on small samples or clinic populations thatmay not be representative of high-risk women in the community. There is hencea need to examine the long-term impact of women’s knowledge of their carrieror noncarrier status. That is, given the benefit of hindsight, how would they de-scribe their experience of discovering their mutation status and living with thatknowledge for a period of years?
In this study, we sought to discover the emotional and social impact of re-ceiving results of genetic testing for HBOC by documenting the experiences ofwomen participating in a registry of high-risk breast cancer families, and who hadreceived either a positive and negative result for BRCA1, BRCA2, or the ATMgene, as well as those women who declined to know their test result.

P1: GCY
Journal of Genetic Counseling [jgc] ph250-jogc-480246 March 8, 2004 10:23 Style file version Nov 28th, 2002
Impact of Receiving Genetic Test Results for Breast Cancer 117
In Australia, cancer genetic services offer testing through specialized fa-milial cancer clinics which usually include a medically trained person (clinicalgeneticist or oncologist) and a genetic counselor, and are often linked to oncologyservices. The Counselors are genetic counselors, oncology nurses, social work-ers, or psychologists with expertise in oncology or genetics. These clinics providea comprehensive service including risk assessment, genetic testing and adviceregarding early detection and prevention (Kirk and Tucker, 1997). Referral isnecessary, and genetic counseling and testing are currently available in both theState-funded health system and in the private sector. Predictive testing is almostalways restricted to those where a family specific mutation is known, consistentwith overseas guidelines (American Society of Clinical Oncology [ASCO], 2003).Usually the woman is telephoned by the genetic counselor to obtain family historydetails before the appointment, and discusses her risk and management optionsfor 1–2 sessions before genetic testing occurs. Results are given in person andfollow-up appointments are available on demand.
METHODS
Participants
Subjects were unaffected women participating in the Kathleen CuninghamConsortium for Research into Familial Breast Cancer (kConFab) PsychosocialStudy. KConFab is a collaborative research group established in 1996 to coordinatethe collection of genetic, epidemiological, and clinical data in Australian familieswith a dominantly inherited susceptibility to breast cancer. Women are eligiblefor kConFab if they have a family history consistent with a dominantly inheritedsusceptibility to breast cancer, and come from a family that meets the kConFabeligibility criteria summarized in Table I. The exclusion criteria are non-English
Table I. Eligibility Criteria for Recruitment Into the Kathleen Cuningham Consortium for ResearchInto Familial Breast Cancer (kConFab)
Families in which apredisposingmutation has beenidentified
Two or more carriers (or likely carriers amongst first- andsecond-degree relatives from the informative side of the family)
Families in which nopredisposingmutation has beenidentified
All of the following are required:(i) four or more cases of breast or ovarian cancer (on one side of
the family) or two or more cases of breast or ovarian cancer,in same or adjacent generations, if at least one of these cases is“high-risk” (i.e. breast plus ovarian cancer, or onset less than40 years or bilateral breast cancer); and
(ii) two or more living, affected family members; and(iii) four or more living first- or second-degree unaffected female
relatives of affected cases

P1: GCY
Journal of Genetic Counseling [jgc] ph250-jogc-480246 March 8, 2004 10:23 Style file version Nov 28th, 2002
118 Lim et al.
speaking, age less than 18 years and serious mental illness. (For details aboutkConFab and the biological and epidemiological information available, please seewww.kconfab.org.)
All unaffected women enrolled in kConFab are eligible for participation inthe ongoing kConFab Psychosocial Study. Women are recruited either on entryinto the main kConFab study or at approximately 3 years follow-up when theirclinical information is being updated. Invitations to participate in the study aremailed from the coordinating research center, along with a detailed informationand consent form, a questionnaire booklet, and reply paid envelope. Women areprovided with a “free-call” number if they wished to obtain further informationabout the study. Participation in the kConFab Psychosocial Study entails complet-ing a set of questionnaires measuring a range of psychological factors thought tobe associated with the development of cancer (such as emotional repression anddepression) and a telephone interview eliciting stressful life events (Life Eventsand Difficulties Schedule [LEDS]; Brown and Harris, 1978). Women are given theoption to complete either the questionnaire or the interview component only, orboth. Participants are recruited through 11 study sites across Australia. The studywas approved by each of the institutional ethics committees.
The current report focuses on a subsample of the kConFab PsychosocialStudy, namely those unaffected women for whom mutation results were available,recruited between August 2001 and July 2002. All such women had received apredictive test where a family specific mutation had already been delineated inanother family member.
Procedures
This study reports on responses to five open-ended questions raised only withwomen who had received a genetic mutation test result.
Measures
Sociodemographic variables: age, marital status, number of children, andeducational level were obtained during the telephone interview.
Interview questions: The following questions were raised during the life eventstress interview. As the LEDS interviews are not recorded, interviewers madecontemporaneous written records of verbatim responses.
• How did you feel about the result of your genetic testing?• Has it affected your relationships with immediate family members?• How have other members of the family responded?• What are some advantages and disadvantages of receiving a result?• Has it changed your life/activities in anyway?

P1: GCY
Journal of Genetic Counseling [jgc] ph250-jogc-480246 March 8, 2004 10:23 Style file version Nov 28th, 2002
Impact of Receiving Genetic Test Results for Breast Cancer 119
Ten women who declined knowledge of their test result were also identified.These women were simply asked the rationale for their decision.
Data Analysis
A qualitative methodology was selected as most appropriate (Inu, 1996; Popeand Mays, 1995) as little is known about the longer-term impact of knowing one’sgenetic predisposition for breast or ovarian cancer.
To aid data analysis, the detailed written records of the respondents’ replieswere imported into the computer program NUD.IST (Richards and Richards,1994). This software program facilitates organizing, managing, and analysesof qualitative data. Initially each woman’s responses were scanned, phrase byphrase and sentence by sentence, by two of the authors (JL, BB) to identifycontent and emergent themes. Themes were placed with higher order cate-gories that were reviewed and revised by all authors until consensus wasachieved.
Subgroup differences in themes were assessed according to: (a) genetic muta-tion test result (positive or negative), (b) time since result (less than/more than themedian of 13 months), and (c) age (less than/more than the median of 48 years).Subgroup differences identified are noted in the text.
RESULTS
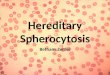
Of unaffected women participating in the main kConFab study, 80% agreeto participate in the kConFab Psychosocial study. All participants who had re-ceived a genetic test result (n = 47) completed the five questions reported here.Twenty-three women were mutation-positive and 24 were mutation-negative. Thesociodemographic and family history variables of the sample are shown in Table II.The women ranged in age between 24 and 76 with a median of 48 years. Fifty-seven percent of women had no postsecondary school qualifications. The majoritywere married and had one or more children. The median time since receiving re-sults was 13 months, ranging from 1 month to over 5 years. Themes identified aresummarized in Table III according to mutation status, age at the time results werereceived and time since result.
Initial Impact of Receiving a Genetic Mutation Test Result
Women reported the impact of receiving a genetic mutation result for them-selves, and the impact on their relationships with their partner and widerfamily.

P1: GCY
Journal of Genetic Counseling [jgc] ph250-jogc-480246 March 8, 2004 10:23 Style file version Nov 28th, 2002
120 Lim et al.
Table II. Sociodemographic and Family History Variables (n = 47)
Variable Category N %
Age <30 years 4 8.530–39 years 13 27.740–49 years 11 23.450+ years 19 40.4
Education Postschool qualifications 19 43.2No postschool qualifications 25 56.8
Marital status Married 37 78.7Not married 10 21.3
Number of children No children 10 21.31–2 children 22 46.8Three or more 15 31.9
Mutation status Positive 23 49Negative 24 51
Time since result 1–6 months 11 23.47–12 months 11 23.413–36 months 12 25.537–70 months 13 27.7
Self
Women described a range of responses upon receiving the results of ge-netic mutation status, with many acknowledging conflicting emotions. Feelingsof shock, relief, and acceptance were reported in both mutation-positive and neg-ative groups. Not surprisingly, many mutation-positive women reported feelinghigh levels of distress, while mutation-negative women more commonly reportedfeeling good, normal but also guilty (Fig. 1).
The majority of women reporting initial shock were mutation-positive, al-though some were mutation-negative. Comments included feeling flat and dazed.Approximately one third of women mentioned relief, although the form of reliefvaried according to mutation status. For mutation-positive women, the relief wasin the validation of their own beliefs and relief from uncertainty. There was alsorelief from guilt.
Thank God I’ve got it as I would have felt guilty if I didn’t. All my brothers and sisters haveit.
For mutation-negative women, relief came in the form of peace of mind anda decrease in worry, fear and uncertainty regarding their own risk and that of theirchildren. For some, the relief was more physical in nature.
I feel better physically, less tense.
Nine women reported a neutral or accepting response, even amongst mutation-negative women where a stronger response may have been expected. The themeamong five mutation-positive women was that living with cancer was a fact of life.
P1: GCY
Journal of Genetic Counseling [jgc] ph250-jogc-480246 March 8, 2004 10:23 Style file version Nov 28th, 2002
Impact of Receiving Genetic Test Results for Breast Cancer 121
Table III. Themes of Impact of Genetic Testing by Result, Age and Time Since Result
Mutation status Age in years Time since result
Positive Negative <48 >48 <13 months >13 monthsTheme (N ) (n = 23) (n = 24) (n = 23) (n = 24) (n = 23) (n = 24)
Initial impact: SelfShock (8) 6 2 2 6 3 5Relief (18) 7 11 8 10 8 10Neutral/Accepting (9) 5 4 6 3 3 6Distress (8) 7 1 6 2 4 4Guilt (5) 0 5 1 4 2 3Normal (3) 0 3 2 1 3 0
Initial impact: PartnerNo impact (23) 10 13 12 11 12 11Supportive (7) 6 1 4 3 5 2
Initial impact: Wider familySupportive (25) 12 13 9 16 14 11Difficulty breaking news (6) 4 2 3 3 4 2No impact (13) 6 7 5 8 5 8Unsupportive (4) 3 1 4 0 3 1Dealing with others (5) 4 1 1 4 3 2Didn’t tell (8) 5 3 3 5 5 3
AdvantagesKnowledge (20) 17 3 10 10 10 10Screening/Surgery (13) 13 0 6 7 7 6Peace of mind (8) 0 8 4 4 3 5Feeling normal (6) 0 4 4 0 2 2None (3) 2 1 3 0 2 1
DisadvantagesNone (26) 10 16 13 13 9 17Loss of innocence (4) 4 0 4 0 4 0Complacency (1) 0 1 1 0 1 0
Life changeNone (18) 6 12 6 12 10 8Change in priorities (4) 3 1 4 0 2 2
Change over timeSelf (9) 7 2 4 5 4 5Family (2) 1 1 2 0 1 1
Note. Not all women responded in every category; some categories may add to more than total asmultiple responses apply
I wasn’t bothered by having the gene as I’d seen my mum get through it.
However, many women with a mutation-positive result reported feeling dis-tressed, upset, rotten, or anxious. A typical response was:
I was more upset than I expected . . . I thought the odds would come out in my favour.
More graphic was this woman’s response.
I thought I’d had time to prepare and that I had not much of a chance of being positive. Icheated myself. I felt like I was smashed in the chest.

P1: GCY
Journal of Genetic Counseling [jgc] ph250-jogc-480246 March 8, 2004 10:23 Style file version Nov 28th, 2002
122 Lim et al.
Fig
.1.
Initi
alim
pact
onse
lfby
mut
atio
nst
atus
.

P1: GCY
Journal of Genetic Counseling [jgc] ph250-jogc-480246 March 8, 2004 10:23 Style file version Nov 28th, 2002
Impact of Receiving Genetic Test Results for Breast Cancer 123
Five mutation-negative women reported feelings of guilt.
I would have preferred to get the gene because I have no children and my sister does.
Three mutation-negative women described feeling normal for the first time.
Partner
Most women reported no significant impact on their relationship within theirpartner. Seven women specified the benefits of a supportive partner during thetesting process. Only one woman reported an unsupportive partner, indicating thiswas characteristic of their relationship—they have since separated.
Wider Family
The responses of the wider family relationships varied from supportive, neu-tral, or unsupportive. A few women were selective in who they told, while forothers the focus was on the difficulty of dealing with the emotional reactions ofother family members to their results (Fig. 2).
More than half the women reported supportive responses from wider familymembers. Thirteen mutation-negative women reported positive responses such asdelight, happiness, and relief on sharing the news. At the same time women alsodescribed the difficulty of breaking the news, including those with positive andnegative results. A mutation-negative woman said:
I found it difficult to tell my sister who was positive, but she asked and was fine about it.
There was also a sense of support in being able to talk about the result with otherfamily members, particularly among mutation-positive women.
I was able to talk about it with my sister. We came to the same decision . . . my cousins madedifferent decisions . . . it was good to get another view.
Six mutation-positive and seven mutation-negative women cited no impact onfamily relationships, the common theme again was that they were used to livingwith cancer.
We have already been touched by cancer.
Three mutation-positive women found their family unsupportive. One family wasshocked and upset at her decision to have a bilateral prophylactic mastectomy.
Both mutation-positive and mutation-negative women spoke of the difficultyof dealing with other family members’ results and emotions at the same time. Amutation-positive woman reported:
My youngest brother felt better as he wasn’t the only one, but he felt angry about getting it.

P1: GCY
Journal of Genetic Counseling [jgc] ph250-jogc-480246 March 8, 2004 10:23 Style file version Nov 28th, 2002
124 Lim et al.
Fig
.2.
Impa
cton
wid
erfa
mily
bym
utat
ion
stat
us.

P1: GCY
Journal of Genetic Counseling [jgc] ph250-jogc-480246 March 8, 2004 10:23 Style file version Nov 28th, 2002
Impact of Receiving Genetic Test Results for Breast Cancer 125
Five mutation-positive and three mutation-negative women didn’t tell their familiesor were selective in who they told about their result.
Advantages and Disadvantages
The majority of women thought there were advantages in knowing their mu-tation status. The themes arising in this section did vary considerably according tothe mutation result (Fig. 3).
Advantages (Mutation-positive)
Knowledge Is Powerful. Most mutation-positive women reported that simplyknowing their mutation status was an advantage. Concern about being at high-riskhad been validated and the removal of uncertainty about their risk produced a senseof control.
I can do something about it and have more control. I also think about it more often whendealing with other issues like the contraceptive pill.
There was also a sense that the knowledge provided the opportunity to prepareemotionally and mentally.
It reinforced my need to research the area and sort out what I need to do for the future.
Increased education rather than having a big shock when I do get cancer. I can be moreprepared by knowing about treatment options.
Several mutation-positive women saw the advantage for future generations.
The grandchildren can do something about it.
More practically, the advantages of increased access to screening programs and sur-gical options were readily acknowledged. A more positive attitude towards screen-ing was also common. Others spoke about the options of prophylactic surgery andhad a clear knowledge of the options available to them, although choices varied.
I was offered bilateral mastectomy but I said no, but if by chance I do get cancer, I will getboth of them off.
I have had a mastectomy. I know I have a decreased chance of dying of breast cancer. I havealso had a hysterectomy as my sister had ovarian cancer.
The ovaries can be removed when you are finished with them. I know I will have a betterquality of life mentally because I don’t have to worry about ovarian cancer which is hardto detect.
Advantages (Mutation-Negative)
Advantages from among the mutation-negative women included peace ofmind, relief for their children, and a reduction in anxiety.

P1: GCY
Journal of Genetic Counseling [jgc] ph250-jogc-480246 March 8, 2004 10:23 Style file version Nov 28th, 2002
126 Lim et al.
Fig
.3.
Adv
anta
ges
and
disa
dvan
tage
sby
mut
atio
nst
atus
.

P1: GCY
Journal of Genetic Counseling [jgc] ph250-jogc-480246 March 8, 2004 10:23 Style file version Nov 28th, 2002
Impact of Receiving Genetic Test Results for Breast Cancer 127
It removes the uncertainty and I feel I don’t need to be as vigilant.
Eight specifically named:
Peace of mind that I haven’t passed it on to my children.
Four mutation-negative women used the phrase being or feeling normal.
No Advantages
Two mutation-positive and one mutation-negative women said there were noadvantages in knowing their genetic mutation status. All these women were lessthan 48 years of age.
I have always been careful and will continue with monitoring.
Disadvantages
The majority of women reported no disadvantages. However, there were fourmutation-positive women who mentioned intrusive thoughts about being at riskmore often or lamented their loss of innocence. Of note, all of these women wereless than 48 years of age and had received their result less than 13 months ago.
One woman who subsequently had a prophylactic mastectomy, although notregretting the decision, said she wished she didn’t know her result saying ignoranceis bliss, while another worries for her children all the time. Others said:
If I think about it too much I can get depressed.
It would have been better to find out later in life.
Only one mutation-negative woman noted a disadvantage, concerned she maybecome too complacent.
Life Style Changes or Life Changing Experience
The majority of women cited no changes or impact on their lifestyle sincereceiving their result. No change was more common in older women and womenwith no mutation. However, among a few of the younger women, were descriptionsof a life changing experience, a reassessment of priorities and a renewed apprecia-tion for life. Remarkably the themes were apparent in both mutation-positive andnegative women. One mutation-positive woman said:
My perspective has changed. I used to think that success was to do with money and materialthings. Now I focus more on family and friends.

P1: GCY
Journal of Genetic Counseling [jgc] ph250-jogc-480246 March 8, 2004 10:23 Style file version Nov 28th, 2002
128 Lim et al.
Other mutation-positive women mentioned taking better care of their generalhealth, such as with weight, diet, fitness and stress.
I’ve changed my attitude. I don’t take myself as seriously any more, I find it unnecessaryto stress over things that used to be important to me.
Among the mutation-negative women the comments were similar.
I am more positive and relaxed about everything now.
It probably influenced my decision to move to the country. It made me think about life. . . working long hours. . . life doesn’t need to be like this. It makes you step back and lookat what you are doing.
Change Over Time
A number of women commented about the change over time in their own feel-ings and thinking reflecting their adjustment. Comments from mutation-positivewomen included:
For the first three months I used to think about it every day, but since then it has been easier.
I can’t live my life thinking I may get it tomorrow. I go to my doctor twice a year for abreast examination.
From a mutation-negative woman:
I initially felt invincible, but over time this has become more balanced.
There were also some comments about the changes in the thinking of other familymembers over time. One mutation-positive woman described her family:
Initially they were shocked and upset by my double mastectomy. Now they are more sym-pathetic and realise that my sister with breast cancer would have been better with surgery.
A mutation-negative woman reported:
Before I was tested my father said he didn’t think I should have. . . children. When I waspregnant, he said I should terminate it. When he found out I was negative, he was relieved.
Note, no other differences were found between those women who receivedtheir mutation status result less than 13 months ago and those women who receivedtheir mutation status result more than 13 months ago.
Decliners
In addition to the 47 women who had received genetic mutation testing results,10 women were identified who declined to receive the results of genetic testing(which were available) or had requested not to be informed of the result when itbecame available. These women were aged 19–54 years, with a median age of

P1: GCY
Journal of Genetic Counseling [jgc] ph250-jogc-480246 March 8, 2004 10:23 Style file version Nov 28th, 2002
Impact of Receiving Genetic Test Results for Breast Cancer 129
39.5 years. Three women reported that they did not want to become stressed outby the constant thought of getting cancer, should they be identified as carriers, sothey do not dwell on their elevated risk and try to live life as it comes. A numberof these said that they would not change their current regular screening and ahealthy lifestyle, so knowledge of test results was superfluous. Younger womenoverrepresented in this group. One woman said: I am too young for them to doanything, for example, yearly mammogram, and I don’t want to have mastectomies.Two women who were below 35 years of age cited insurance implications asanother reason for declining to receive knowledge of their result. Three womenacknowledged that they might change their mind, as they get older.
DISCUSSION
The aim of the study was to document the qualitative experience of unaffectedwomen who have received a genetic mutation result for hereditary breast/ovariancancer predisposition genes. We were interested in the emotional and social im-pact of women’s knowledge of their mutation status (positive/negative), and theinfluence of time since result disclosure (less than/greater than 13 months) and age(less than/greater than 48 years) on these outcomes. In addition, unaffected womenwho were able to undergo HBOC mutation testing but declined knowledge of theresults provided some insight into their reasoning.
Women’s reports of the initial emotional impact of receiving their result weresurprisingly similar, whether it was positive or negative, although their rationalefor the response was different. For example, relief for women with a mutation-negative result was for themselves and their children; whereas relief for womenwith a mutation-positive result related to the removal of uncertainty, having theirown self-image of being at risk validated and feeling a greater sense of control.
Women’s responses ranged from feelings of shock, distress, and guilt, to reliefand acceptance and this high level of negative response is consistent with previousfindings (Lynch et al., 1993, 1997). However, some women within both groupsexpressed even initially, a strong sense of acceptance, based on having seen otherfamily members coping with cancer. Thus, any test result (positive or negative)resulted in a short period of emotional turmoil for most but not all women.
Although many women reported an initial negative response to discover-ing their mutation status, for most individuals this negative response was shortlived. The majority of women confirmed long-term advantages and cited no disad-vantages to knowing their mutation status. Those with a mutation-positive resultwere reassured that they could take decisive steps to reduce their risk (i.e., screen-ing/surgical options). In the long-term, knowledge of mutation status was describedas empowering, providing an opportunity to prepare emotionally and mentally fora potential cancer diagnosis. Indeed, some women, particularly those who wereyounger, reported that the mutation testing experience had generated important and

P1: GCY
Journal of Genetic Counseling [jgc] ph250-jogc-480246 March 8, 2004 10:23 Style file version Nov 28th, 2002
130 Lim et al.
positive life changes. Moreover, they felt future generations could benefit from thisknowledge. These findings reinforce previous studies which show that individualswith positive mutation result seem to benefit psychologically from knowing theirstatus because of uncertainty reduction (Lynch and Lynch, 1996; Wiggins et al.,1992), which promotes active coping, thus buffering the impact of their risk status.These results also underscore the importance of long-term follow-up of people re-ceiving mutation test results, as reliance on short-term follow-up may exaggerateits negative impact.
However, some women in our study who were mutation-negative said thatthe results had not changed their sense of being at risk and one reported that shehad gone ahead with prophylactic mastectomy regardless. Other women reportedthey felt a need for continuing careful screening. This supports previous studiesthat indicated that in a subgroup of women, genetic counseling is not successful inreducing an inflated perception of personal risk (Cull et al., 1998, 1999; Watsonet al., 1999) and does not alter intention to undertake prophylactic surgery (Meiseret al., 2000). Perhaps the women understand their risks but really cannot toleratethem or they might have other psychological needs to remove body parts that theyconsider risky (Hallowell et al., 2001). In any case, this raises important clinicalissues in term of how such information is relayed and whether interventions areneeded to shift inflated risk perception in other ways.
Our findings also confirmed other researchers’ observations that the impactof genetic testing extends beyond the individual to their family and social context(Appleton et al., 2000; Smith et al., 1999). The women described both supportiveand unsupportive responses from extended family members to their own test resultand subsequent decisions about their risk management. They also reported a com-plex interplay of interreactions as test results for different family members werereceived. Family members who were mutation-negative responded differently tothose who were mutation-positive. This lends support to Smith et al. (1999) whoreport that emotional responses differ according to the mutation status of other fam-ily members and to the order in which results are received. There is also evidencesuggesting that the uptake of genetic testing is moderated by complex family dy-namics (Broadstock et al., 2000). Our findings reinforce the importance of a familysystems approach to the understanding of psychological responses to genetic test-ing. Most previous studies have focused on individual psychological outcomes ofreceiving a test result without reference to family context. The next generation ofstudies should adopt a more complex model exploring family dynamics in relationto the genetic status of all family members.
We also interviewed women who had declined their test result regarding theirmotivation for doing so. Rationales varied widely, and included those with elementsof avoidance and fear, and those involving realistic assessments of potential dis-advantages of testing. The latter included concerns about insurance and awarenessof the limitations of screening, particularly for younger women. Several younger

P1: GCY
Journal of Genetic Counseling [jgc] ph250-jogc-480246 March 8, 2004 10:23 Style file version Nov 28th, 2002
Impact of Receiving Genetic Test Results for Breast Cancer 131
women noted that they might choose to be informed of their results when theyare older, when prophylactic surgery would be a more acceptable option. It wouldseem that the rationale for declining test results might have important implicationsfor subsequent emotional adjustment. Indeed Lerman et al. (1995) reported thatonly decliners who were initially depressed were at greater risk of psychologicalmorbidity, supporting the notion that declining per se may not be problematical.This issue deserves more attention. Future research should explore the way inwhich a woman’s rationale for declining influences psychological outcome, andthe influence of age at the time of testing.
CONCLUSIONS
These findings have several implications for clinical practice. First, as initialturmoil was a common response to both positive and negative test results, it may beuseful to warn and prepare women for this likely emotional response, emphasizingthat it is likely to be short-lived, while also acknowledging potential long-termoutcomes. Telling women how other women have responded would be a usefulstrategy in this process, so that she knows what to expect, and that her responsesare not uncommon. Normalizing responses to health threats is an important wayof promoting good coping.
Second, many women described difficulties or concerns about communicat-ing with their family about genetic test results and subsequent decisions. Preparingwomen for such difficulties, and the rippling effects within the family of obtain-ing test results, may allow them to better negotiate communication around thisissue. Family interventions may also be useful for some, an option currently un-available within most hereditary cancer clinics. Specialist staff with expertise infamily dynamics may be required for such interventions. Future research is neededto expand our understanding of the ways in which families negotiate and blockcommunication about their genetic status.
Third, the reasons why women decline test results needs carefully exploration,as declining testing or receipt of a test result may be an indicator of significant psy-chological distress; however for others it may reflect only a mature understandingof the current limitations of testing and management.
This study was qualitative in design with a limited sample size, and therefore itwas not possible to determine the generalizability of the results to other women, andto those in other cultures. However, this study had several advantages over previousstudies. The women involved were from the community, and are thus likely to bemore representative of high-risk women as a whole, than those attending hereditarycancer clinics, many of whom are self-selecting. All women in this sample wereunaffected, preventing confounding by breast cancer status. Finally, we were ableto explore the impact of time since receiving the test result, since some womenhad received the test result many years ago. As far as we are aware, this is the first

P1: GCY
Journal of Genetic Counseling [jgc] ph250-jogc-480246 March 8, 2004 10:23 Style file version Nov 28th, 2002
132 Lim et al.
study that has explored the impact of receiving a test result beyond a 12-monthfollow-up.
ACKNOWLEDGMENTS
We thank the kConFab nurses for recruitment of participants: Meryl Altree,Helen Conlon, Vicky Fennelly, Janine Furmedge, Marianne Griffin, MargaretGleeson, Vivianne Geldard, Anna Nash, Karen Robinson, Susan Schulz, KlausSommer, Margaret Tanner, and Jane Wylie. This research was supported by ProjectGrants No. 153824 of the National Health and Medical Research Council of Aus-tralia and a grant from the Breast Cancer Association of Queensland. KConFabhas been funded by the Kathleen Cuningham Foundation, National Breast CancerFoundation, National Health and Medical Research Council, Anti Cancer Coun-cil of Victoria, Anti Cancer Foundation of South Australia, Cancer Foundationof Western Australia, Queensland Cancer Fund, and NSW Cancer Council. Fur-ther details and updates can be found on http://www.kconfab.org/organisation/funding.asp. Bettina Meiser is supported by Public Health Australia FellowshipNo. 007079 from the National Health and Medical Research Council of Australia(NHMRC), and Phyllis Butow by a Senior Research Fellowship (Level B) fromthe NHMRC. We are most grateful for the valuable contribution of all the womenwho participated in this study.
REFERENCES
American Society of Clinical Oncology. (2003). American Society of Clinical Oncology policy state-ment update: Genetic testing for cancer susceptibility. JCO, 21(12), 2397–2406.
Antoniou, A., Pharoah, P. D., Narod, S., Risch, H. A., Eyfjord, J. E., Hopper, J. L., et al. (2003). Averagerisks of breast and ovarian cancer associated with BRCA1 or BRCA2 mutations detected in caseSeries unselected for family history: A combined analysis of 22 studies. Am J Hum Genet, 72(5),1117–1130.
Appleton, S., Fry, A., Rees, G., Rush, R., & Cull, A. (2000). Psychosocial effects of living with an in-creased risk of breast cancer: An exploratory study using telephone focus groups. Psychooncology,9(6), 511–521.
Broadstock, M., Michie, S., Gray, J., Mackay, J., & Marteau, T. M. (2000). The psychological con-sequences of offering mutation searching in the family for those at risk of hereditary breast andovarian cancer—a pilot study. Psychooncology, 9(6), 537–548.
Brown, G. W., & Harris, T. O. (1978). Social origins of depression: A study of psychiatric disorder inwomen. London: Tavistock.
Butow, P. N., Lobb, E. A., Meiser, B., Barratt, A., & Tucker, K. M. (2003). Psychological outcomesand risk perception after genetic testing and counselling in breast cancer: A systematic review.MJA, 178(2), 77–81.
Cull, A., Anderson, E. D., Campbell, S., Mackay, J., Smyth, E., & Steel, M. (1999). The impact ofgenetic counselling about breast cancer risk on women’s risk perceptions and levels of distress.Br J Cancer, 79(3/4), 501–508.
Cull, A., Miller, H., Porterfield, T., Mackay, J., Anderson, E. D., Steel, C. M., et al. (1998). The useof videotaped information in cancer genetic counselling: A randomized evaluation study. Br JCancer, 77(5), 830–837.

P1: GCY
Journal of Genetic Counseling [jgc] ph250-jogc-480246 March 8, 2004 10:23 Style file version Nov 28th, 2002
Impact of Receiving Genetic Test Results for Breast Cancer 133
Hallowell, N., Jacobs, I., Richards, M., Mackay, J., & Gore, M. (2001). Surveillance or surgery?A description of the factors that influence high risk premenopausal women’s decisions aboutprophylactic oophorectomy. J Med Genet, 38(10), 683–691.
Hutson, S. P. (2003). Attitudes and psychological impact of genetic testing, genetic counseling, andbreast cancer risk assessment among women at increased risk. Oncol Nurs Forum, 30(2), 241–246.
Inu, T. (1996). The virtue of qualitative and quantitative research. Ann Intern Med, 125(9), 770–771.Kirk, J., & Tucker, K. (1997). National best practical guidelines for familial cancer clinics. Sydney:
National Health & Medical Research Council of Australia’s National Breast Cancer center.Lerman, C., Seay, J., Balshem, A., & Audrain, J. (1995). Interest in genetic testing among first-degree
relatives of breast cancer patients. Am J Med Genet, 57(3), 385–392.Lynch, H., Lemon, S. J., Durham, C., Tinley, S. T., Connolly, C., Lynch, J. F., et al. (1997). A descriptive
study of BRCA1 testing and reactions to disclosure of test results. Cancer, 79(11), 2219–2228.Lynch, H. T., & Lynch, J. F. (1996). Breast cancer genetics: Family history, heterogeneity, molecular
genetic diagnosis, and genetic counselling. Curr Probl Cancer, 20(6), 332–365.Lynch, H. T., Watson, P., Conway, T. A., Lynch, J. F., Slominski-Caster, S. M., Narod, S. A., et al.
(1993). DNA screening for breast/ovarian cancer susceptibility based on linked markers: A familystudy. Arch Intern Med, 153, 1979–1987.
Meiser, B., Butow, P., Friedlander, M., Barratt, A., Schnieden, V., Watson, M., et al. (2002). Psycho-logical impact of genetic testing in women from high-risk breast cancer families. Eur J Cancer,38(15), 2025–2031.
Meiser, B., Butow, P., Friedlander, M., Schnieden, V., Gattas, M., Kirk, J., et al. (2000). Intention toundergo prophylactic bilateral mastectomy in women at increased risk of developing hereditarybreast cancer. J Clin Oncol, 18(11), 2250–2257.
Pope, C., & Mays, N. (1995). Reaching the parts other methods cannot reach: An introduction toqualitative methods in health and health services research. BMJ, 311(6996), 42–45.
Richards, T. J., & Richards, T. (1994). NUD.IST Users manual. La Trobe University: QualitativeSolutions and Research (QSR).
Smith, K., West, J. A., Croyle, R. T., & Botkin, J. R. (1999). Familial context of genetic testing forcancer susceptibility: Moderating effect of siblings’ test results on psychological distress oneto two weeks after BRCA1 mutation testing. Cancer Epidemiol Biomarkers Prev, 8(4, Pt 2),385–392.
Watson, M., Lloyd, S., Davidson, J., Meyer, L., Eeles, R., Ebbs, S., et al. (1999). The impact of geneticcounselling on risk perception and mental health in women with a family history of breast cancer.Br J Cancer, 79(5/6), 868–874.
Wiggins, S., Whyte, P., Huggins, M., Adam, S., Theilmann, J., Bloch, M., et al. (1992). The psycho-logical consequences of predictive testing for Huntington’s disease. Canadian collaborative studyof predictive testing. N Engl J Med, 327(20), 1401–1405.