Embed Size (px)
DESCRIPTION
Short acting anti-cholinergic Ipratropium. Pharm D student : Eman Youssif Supervised by : prof. Seham Hafez. Ipratropium bromide is a synthetic quaternary ammonium antimuscarinic Chemically related to atropine. Ipratropium use in COPD:. - PowerPoint PPT Presentation
Citation preview

Short acting anti-cholinergic Ipratropium
Pharm D student : Eman YoussifSupervised by : prof. Seham Hafez.

Ipratropium bromide is a synthetic quaternary ammonium antimuscarinicChemically related to atropine.

Ipratropium use in COPD:
• ipratropium is a first-line maintenance bronchodilator for relief of chronic (e.g., daily) symptoms of bronchospasm in patients with mild COPD.
• fixed combination of albuterol and ipratropium results in greater bronchodilation following oral inhalation than either agent given alone in patients with COPD.
• combined therapy with a β2-agonist bronchodilator and ipratropium is useful in patients with acute exacerbations of COPD.

Ipratropium use in COPD:Ipratrpium is not indicated for the initial treatment of acute bronchospasm or acute exacerbation of COPD a β2-adrenergic agonist may be preferred in such cases. Orally inhaled ipratropium produce fewer adverse effects than β2-adrenergic agonist Ipratropium bromide (36 mcg 4 times daily) oral inhalation aerosol with chlorofluorocarbon (CFC) propellants was less effective than tiotropium (18 mcg once daily) in improving lung function (e.g., as determined by changes in FEV1 and peak expiratory flow rate [PEFR]) in patients with COPD.

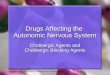
Cholinergic nerve transmission mediated by acetylcholine.

Cholinergic muscarinic receptor subtype M1, showing effectsin the target cell mediated by the stimulatory G protein.PIP2 phosphatidylinositol bisphosphate. DAG diacylglycerol.

Identification and location of muscarinic receptor subtypes M1, M2, and M3 in the vagal nerve, submucosal gland, and bronchial smooth muscle in the airway, showing nonspecific blockade by anticholinergic drugs.

•Administration
Ipratropium bromide is administered by oral inhalation using an oral aerosol inhaler or via nebulization.
Ipratropium bromide is administered in fixed combination with albuterol sulfate via a metered-dose aerosol inhaler or via nebulization.
Patients should be advised that ipratropium must be used consistently throughout the course of therapy for maximum benefit. In addition, patients should be advised that the drug will not provide immediate symptomatic relief and should not be used for the relief of acute bronchospasm .

If the conjunctiva is exposed to aerosolized anticholinergics (from a nebulizer, metered-dose inhaler, or powder inhaler) the patient may develop anisocoria. The left pupil is normal and the right pupil is dilated (mydriatic). To avoid inadvertent contact of the drug with the eyes and subsequent adverse effects, patients should be advised to close their eyes during inhalation of ipratropium aerosol; it also has been suggested that ipratropium aerosol not be administered using the open-mouth technique in patients at high risk for ocular toxicity

Compairing the efficacy and safety of ipratropium bromide/fenoterol hydrobromide (IB/FEN; Berodual) delivered from the novel propellant-free Respimat Soft Mist Inhaler (SMI) with that from a chlorofluorocarbon (CFC) metered-dose inhaler (MDI) plus spacer in children with asthma. IB/FEN delivered via Respimat1SMI is at least as effective as, and is as safe as, when delivered via CFC-MDI plus Aerochamber in children with asthma. Use of Respimat SMI thus enables a 2–4-fold reduction in the nominal dose of IB/FEN, and obviates the need for a spacer

dosageMetred dose aerosol: a dose of 20–21 mcg of ipratropium bromide
per metered spray, this is the amount released from the valve stem during actuation of the inhaler; the dose of ipratropium bromide alone or in fixed combination with albuterol sulfate delivered to the patient through the mouthpiece (actuator) is approximately 17 or 18 mcg, respectively, per metered spray(2 puffs (34 mcg) by inhalation route 4 times per day).
Inhalatin via nebulizer: 250–500 mcg 3 or 4 times daily .

Pharmacokinetics Distribution Quaternary ammonium antimuscarinics are completely ionized and possess poor lipid solubility;
Side effects: because of the drug’s limited systemic absorption, oral inhalation of ipratropium bromide produces anticholinergic adverse effects (e.g., increased intraocular pressure, mydriasis, urinary retention) less frequently than systemically administered antimuscarinic drugs.

•Pregnancy, and Lactation
• There are no adequate and controlled studies to date using orally inhaled ipratropium in pregnant women, and the drug should be used during pregnancy only when clearly needed.
• The manufacturer recommends that orally inhaled ipratropium be used with caution in nursing women.
•

Drug Interactions
Concomitant administration of ipratropium and albuterol via nebulization has been reported to increase intraocular pressure (IOP) and precipitate acute angle-closure glaucoma in susceptible individuals (i.e., individuals with untreated or undiagnosed angle-closure glaucoma),

Stability - Oral inhalation aerosol should be stored at 25 °C.- Exposure to excessive humidity should be avoided - Cooling of the propellants may decrease the internal
pressure of the canister and result in delivery of particles too large to provide full therapeutic effect.
- Inhalation solutions for nebulization should be protected from light
- solutions containing ipratropium bromide stable for 1 hour when mixed in a nebulizer prior to administration.

oxitropium
Oxitropium bromide’s peak bronchodilation may take 60–90 min, and its duration is 5–8 h. It has been available outside the United States as Oxivent, in an MDI that delivers 100 g/puff. Oxitropium’s bronchodilation effect is similar to that of ipratropium bromide, but oxitropium is longer-lasting.The usual dose is 200 g, 2–3 times daily. It is considered to have twice the strength of ipratropium per dose. Although widely used for many years (alone or in combination with short-acting agonists) for both maintenance treatment of stable disease and exacerbation of airway obstruction, Boehringer Ingelheim announced the discontinuation of Oxivent formulations as of May 2004.

Thank you