Embed Size (px)
Citation preview

Discharge planning from hospital to home (Review)
Shepperd S, Parkes J, McClaran J, Phillips C
This is a reprint of a Cochrane review, prepared and maintained by The Cochrane Collaboration and published in The Cochrane Library
2008, Issue 3
http://www.thecochranelibrary.com
1Discharge planning from hospital to home (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

T A B L E O F C O N T E N T S
1ABSTRACT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2PLAIN LANGUAGE SUMMARY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2BACKGROUND . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2OBJECTIVES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
3CRITERIA FOR CONSIDERING STUDIES FOR THIS REVIEW . . . . . . . . . . . . . . . . . .
3SEARCH METHODS FOR IDENTIFICATION OF STUDIES . . . . . . . . . . . . . . . . . . .
4METHODS OF THE REVIEW . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
4DESCRIPTION OF STUDIES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
5METHODOLOGICAL QUALITY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
5RESULTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
6DISCUSSION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
7AUTHORS’ CONCLUSIONS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
8FEEDBACK . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
8POTENTIAL CONFLICT OF INTEREST . . . . . . . . . . . . . . . . . . . . . . . . . . .
8ACKNOWLEDGEMENTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
8SOURCES OF SUPPORT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
8REFERENCES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
11TABLES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
11Characteristics of included studies . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
15Characteristics of excluded studies . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
17ANALYSES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
17Comparison 01. Hospital length of stay . . . . . . . . . . . . . . . . . . . . . . . . . . .
17Comparison 02. Effect of discharge planning on unscheduled readmission rates . . . . . . . . . . . . .
17Comparison 03. Effect of discharge planning on days in hospital due to unscheduled readmission . . . . . . .
17Comparison 04. Mortality . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
18Comparison 05. Effect of discharge planning on patient health outcomes . . . . . . . . . . . . . . .
18Comparison 06. Effect of discharge planning on health care costs . . . . . . . . . . . . . . . . . .
18Comparison 07. Effect of discharge planning on use of primary care services . . . . . . . . . . . . . .
18Comparison 08. Effect of discharge planning on patients’ place of discharge . . . . . . . . . . . . . .
18Comparison 09. Outpatient attendance . . . . . . . . . . . . . . . . . . . . . . . . . . .
19Comparison 10. Medication . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
19INDEX TERMS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
19COVER SHEET . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
21GRAPHS AND OTHER TABLES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
21Analysis 01.01. Comparison 01 Hospital length of stay, Outcome 01 hospital length of stay elderly medical patients .
21Analysis 01.02. Comparison 01 Hospital length of stay, Outcome 02 hospital length of stay - elderly medical and surgical
patients . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
22Analysis 01.03. Comparison 01 Hospital length of stay, Outcome 03 hospital length of stay - elderly surgical patients
22Analysis 02.01. Comparison 02 Effect of discharge planning on unscheduled readmission rates, Outcome 01 Patients
with a medical condition . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
23Analysis 02.02. Comparison 02 Effect of discharge planning on unscheduled readmission rates, Outcome 02 Patients
who have had surgery . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
23Analysis 02.03. Comparison 02 Effect of discharge planning on unscheduled readmission rates, Outcome 03 Patients
with medical or surgical condition . . . . . . . . . . . . . . . . . . . . . . . . . . .
24Analysis 02.04. Comparison 02 Effect of discharge planning on unscheduled readmission rates, Outcome 04 unscheduled
readmission within 3 months of discharge from hospital . . . . . . . . . . . . . . . . . . .
24Analysis 03.01. Comparison 03 Effect of discharge planning on days in hospital due to unscheduled readmission,
Outcome 01 Patients with a medical or surgical condition . . . . . . . . . . . . . . . . . .
24Analysis 03.02. Comparison 03 Effect of discharge planning on days in hospital due to unscheduled readmission,
Outcome 02 Patients with a medical condition . . . . . . . . . . . . . . . . . . . . . .
iDischarge planning from hospital to home (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd
25Analysis 03.03. Comparison 03 Effect of discharge planning on days in hospital due to unscheduled readmission,
Outcome 03 Patients with a surgical condition . . . . . . . . . . . . . . . . . . . . . .
25Analysis 04.01. Comparison 04 Mortality, Outcome 01 Mortality at 6 to 9 months . . . . . . . . . . . .
25Analysis 04.04. Comparison 04 Mortality, Outcome 04 Mortality for trials recruiting both patients with a medical
condition and those recovering from surgery . . . . . . . . . . . . . . . . . . . . . . .
26Analysis 05.01. Comparison 05 Effect of discharge planning on patient health outcomes, Outcome 01 Patients with a
medical condition . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
30Analysis 05.02. Comparison 05 Effect of discharge planning on patient health outcomes, Outcome 02 Patients with a
surgical condition . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
30Analysis 05.03. Comparison 05 Effect of discharge planning on patient health outcomes, Outcome 03 Patients with a
medical or surgical condition . . . . . . . . . . . . . . . . . . . . . . . . . . . .
30Analysis 05.04. Comparison 05 Effect of discharge planning on patient health outcomes, Outcome 04 Effect of discharge
planning on patients’ and carers’ satisfaction . . . . . . . . . . . . . . . . . . . . . . .
31Analysis 06.01. Comparison 06 Effect of discharge planning on health care costs, Outcome 01 Patients with a medical
condition . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
31Analysis 06.02. Comparison 06 Effect of discharge planning on health care costs, Outcome 02 Patients with a surgical
condition . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
32Analysis 07.01. Comparison 07 Effect of discharge planning on use of primary care services, Outcome 01 Patients with a
medical condition . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
32Analysis 08.01. Comparison 08 Effect of discharge planning on patients’ place of discharge, Outcome 01 Patients with a
medical condition . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
33Analysis 08.02. Comparison 08 Effect of discharge planning on patients’ place of discharge, Outcome 02 Patients with a
medical or surgical condition . . . . . . . . . . . . . . . . . . . . . . . . . . . .
33Analysis 08.03. Comparison 08 Effect of discharge planning on patients’ place of discharge, Outcome 03 Patients
discharged from hospital to home . . . . . . . . . . . . . . . . . . . . . . . . . . .
34Analysis 09.01. Comparison 09 Outpatient attendance, Outcome 01 Elderly medical patients at 6 months . . . .
34Analysis 10.01. Comparison 10 Medication, Outcome 01 Medication problems after being discharged from hospital
34Analysis 10.02. Comparison 10 Medication, Outcome 02 Adherence to medicines . . . . . . . . . . . .
34Analysis 10.03. Comparison 10 Medication, Outcome 03 Knowledge about medicines . . . . . . . . . . .
35Analysis 10.04. Comparison 10 Medication, Outcome 04 Hoarding of medicines . . . . . . . . . . . .
iiDischarge planning from hospital to home (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Discharge planning from hospital to home (Review)
Shepperd S, Parkes J, McClaran J, Phillips C
This record should be cited as:
Shepperd S, Parkes J, McClaran J, Phillips C. Discharge planning from hospital to home. Cochrane Database of Systematic Reviews
2004, Issue 1. Art. No.: CD000313. DOI: 10.1002/14651858.CD000313.pub2.
This version first published online: 26 January 2004 in Issue 1, 2004.
Date of most recent substantive amendment: 25 September 2003
A B S T R A C T
Background
Discharge planning is a routine feature of health systems in many countries. The aim is to reduce hospital length of stay and unplanned
readmission to hospital, and improve the co ordination of services following discharge from hospital thereby bridging the gap between
hospital and place of discharge. Sometimes discharge planning is offered as part of an integrated package of care, which may cover both
the hospital and community. The focus of this review is discharge planning that occurs while a patient is in hospital; we exclude studies
that evaluate dischage planning with follow up care.
Objectives
To determine the effectiveness of planning the discharge of patients moving from hospital.
Search strategy
Relevant studies were identified using Medline, Embase, SIGLE database for grey literature, Bioethics database, Health Plan, Psych.
Lit, Sociofile, CINAHL, Cochrane Library, Econ Lit, Social Science Citation Index, EPOC register. The review was updated using the
EPOC trials register in August 2002.
Selection criteria
Study design: randomised controlled trials (RCTs) that compare discharge planning (the development of an individualised discharge
plan) with routine discharge care. Participants: all patients in hospital. Intervention: the development of an individualised discharge
plan.
Data collection and analysis
Data analysis and quality assessment was undertaken independently by two reviewers using a data checklist. Studies are grouped
according to patient group (elderly medical patients, surgical patients, and those with a mix of conditions), and by outcome.
Main results
Three new studies were included in this update. In total we included eleven RCTS: 6 trials recruited patients with a medical condition
(2,368 patients), and four recruited patients with a mix of medical and surgical conditions (2,983 patients), one of these four recruited
medical and surgical patients as separate groups, and the final trial recruited 97 patients in a psychiatric hospital and from a general
hospital. We failed to detect a difference between groups in mortality for elderly patients with a medical condition (OR 1.44 95% CI
0.82 to 2.51), hospital length of stay (weighted mean difference -0.86, 95% CI -1.9 to 0.18), readmission rates (OR 0.91 95% CI
0.67 to 1.23) and being discharged from hospital to home (OR 1.15 95% CI 0.72 to 1.82). This was also the case for trials recruiting
patients recovering from surgery and those recruiting patients with a mix of medical and surgical conditions. One trial comparing a
structured care pathway for patients recovering from a stroke with multidisciplinary care reported a significant rate of improvement
in functional ability and quality of life for the control group (median change in Barthel score between 4 to 12 weeks of 2 points for
the treatment group, versus 6 for the control group, p<0.01); (Euroqol scores at 6 months 63 for the treatment group, vs. 72 for the
control group, p<0.005). Two trials reported that patients with medical conditions allocated to discharge planning reported increased
satisfaction compared with those who received routine discharge. No statistically significant differences were reported for overall health
care costs.
1Discharge planning from hospital to home (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Authors’ conclusions
The impact of discharge planning on readmission rates, hospital length of stay, health outcomes and cost is uncertain. This reflects a
lack of power as the degree to which we could pool data was restricted by the different reported measures of outcome. It is possible
that even a small reduction in length of stay, or readmission rate, could have an impact on the timeliness of subsequent admissions in
a system where there is an shortage of acute hospital beds.
P L A I N L A N G U A G E S U M M A R Y
The impact of discharge planning on readmission rates, hospital length of stay, health outcomes, and cost to patients and health care
providers is uncertain.
Discharge planning is the development of a discharge plan for the patient prior to leaving hospital, with the aim of containing costs
and improving patient outcomes. The development of a discharge plan is increasingly becoming part of an integrated package of care,
making it difficult to study the effects of discharge planning alone. Although the impact of discharge planning may be small, it is
possible that even a small reduction in length of stay or readmission rate could free up capacity for subsequent admissions in a health
care system where there is a shortage of acute hospital beds.
B A C K G R O U N D
Cost containment is a feature of all health care systems, espe-
cially for acute hospital services (Schwartz 1991). Recent trends
include decreasing the lengths of stay for inpatient care; reducing
the number of long stay beds; moving care into the community;
an increased use of day surgery; providing increased levels of acute
care at home (“hospital at home”), and policies such as discharge
planning. The aim of these policies has been to contain costs, and
improve patient outcomes. For example discharge planning may
influence both the length of hospital stay and the pattern of care
within the community by bridging the gap between hospital and
home (Townsend 1988). Medical or non medical reasons may de-
lay a patient’s discharge from hospital. It has been estimated that
30% of all hospital discharges are delayed for non-medical reasons
(Selker 1989). Despite recent advances in electronic records, pa-
tient pathways and technology assisted decision support, the fol-
lowing factors identified nearly 20 years ago (Barker 1985) remain
causes of delayed discharge from hospital (Dept of Health 2003):
1. Inadequate assessment of the patient by health care professionals
resulting in, for example, a poor knowledge of the patient’s social
circumstances.
2. Poor organisation, for example late booking of transport pre-
venting timely discharge from hospital.
3. Poor communication between the hospital and providers of
services in the community.
It has been suggested that discharge planning can reduce un-
planned readmission to hospital. Formal assessment of patients
prior to discharge and adequate provision of care following dis-
charge may reduce the likelihood of referral back to hospital with
preventable problems (Williams 1988). A reduction in readmis-
sions will decrease inpatient costs; however, this reduction in costs
may be offset by an increase in the provision of community services
as a result of planning. In the USA 42% of the national health care
budget is spent on in-patient care, and readmissions account for
one quarter of Medicare inpatient expenditure (Anderson 1984).
Even a small reduction in readmission rates could have a substan-
tial financial impact (Anderson 1985).
The emphasis placed on discharge planning varies between coun-
tries. In the United States discharge planning is mandatory for hos-
pitals participating in the Medicare and Medicaid programmes.
In the UK the Department of Health has published guidance
on discharge practice for health and social care (Dept of Health
2003). However, procedures may vary between specialities in the
same hospital (Brent Soc Ser 1991; Young 1991; Victor 1988),
and sometimes may be embedded in another intervention, such
as a specialised assessment unit (Rubenstein) or home follow-up
(Parker 2002). These disparities make it difficult to interpret data
on the effectiveness of discharge planning. We have conducted a
systematic review of discharge planning to categorise the different
types of interventions and study populations, and to assess the
effectiveness of organising services in this way.
We have excluded interventions that provide care after discharge
from hospital, and those in which discharge planning is part of a
larger package of care but is poorly described.
O B J E C T I V E S
To determine the effectiveness of planning the discharge of patients
from hospital to home. The following questions were addressed:
Does discharge planning improve the process of patient care?
1. Effect of discharge planning on length of stay in hospital com-
pared to usual care.
2Discharge planning from hospital to home (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd
2. Effect of discharge planning on unscheduled readmission rates
compared to usual care.
3. Effect of discharge planning on the incidence of complications
related to the initial admission compared to usual care.
4. Effect of discharge planning on other process variables: patients’
place of discarge
Does discharge planning improve or (at least) have no adverse
effect on patient outcome?
5. Effect of discharge planning on mortality rate compared to usual
care.
6. Effect of discharge planning on patient health outcomes com-
pared to usual care.
7. Effect of discharge planning on patients’ and carers’ satisfaction
compared to usual care.
Does discharge planning reduce overall costs of health care?
8. Effect of discharge planning on hospital care costs compared to
usual care.
9. Effect of discharge planning on community care costs compared
to usual care.
10. Effect of discharge planning on overall costs of health care
compared to usual care.
11. Effect of discharge planning on the use of medication
C R I T E R I A F O R C O N S I D E R I N G
S T U D I E S F O R T H I S R E V I E W
Types of studies
1. Randomised controlled trials
2. Controlled trials
Types of participants
All patients in hospital (acute, rehabilitation or community) irre-
spective of age, gender or condition.
Types of intervention
Discharge planning is defined as the development of an individu-
alised discharge plan for the patient prior to them leaving hospital
for home. Where possible the process of discharge planning will be
divided according to the steps identified by Marks (Marks 1994):
a) Pre-admission assessment (where possible).
b) Case finding on admission.
c) In-patient assessment and preparation of a discharge plan based
on individual patient needs.
d) Implementation of the discharge plan.
e) Monitoring.
Studies that did not include an assessment and implementation
phase, those where it was not possible to separate the effects of dis-
charge planning from the other components of the intervention,
and those that provided care after discharge from hospital were
excluded from the review.
Types of outcome measures
We included studies that reported any clinically important out-
comes, these cover:
1) Length of stay in hospital.
2) Readmission rate to hospital.
3) Complication rate.
4) Place of discharge.
5) Mortality rate.
6) Patient health status.
7) Patient satisfaction.
8) Carer satisfaction- professional and non-professional.
9) Psychological health of patient.
10) Psychological health of carers.
11) Cost of discharge planning to the hospital and to the commu-
nity.
12) The use of medication for trials evaluating a pharmacy dis-
charge plan was included in the update to reflect the focus of the
intervention for two trials.
S E A R C H M E T H O D S F O R
I D E N T I F I C A T I O N O F S T U D I E S
See: Cochrane Effective Practice and Organisation of Care Group
methods used in reviews.
Relevant studies as described were identified in the following
way:
1.MEDLINE search of years 1966-1996, using patient
discharge(tw), hospital discharge(tw),discharg* plan*(tw),
hospital near discharge(tw), readmissions (tw), length of stay (tw),
patient discharge (mh), patient readmission (mh) in combination
with the optimally sensitive search strategy (OSS) developed by
the UKCC (Dickersin 1994) to identify randomised controlled
trials.
2. Embase database search of years 1980-1996 using the
following terms, patient discharg*, discharge plan*, hospital
discharg*, readmission will be added to an optimally sensitive
search strategy to identify randomised controlled trials.
3. SIGLE database search for grey literature 1980-1996, using
search terms discharg* plan, patient discharge, hospital discharge.
4. Bioethics database 1985-1996, using search terms discharg*
plan*.
5. Health Plan database search for all available years, using search
terms discharge plan*, patient discharge, hospital discharge,
readmission.
6. ASSIA database search for all available years, using search
terms discharge plan*, patient discharg*, hospital discharg*.
7. Psych.Lit database search 1974-1996. The search terms will be
discharge plan, hospital discharge.
8. Sociofile database search using discharge plan*.
3Discharge planning from hospital to home (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

9. CINAHL nursing database search of years 1982-1996, using
search terms discharge plan*. patient discharge, length of stay
hospital discharg*.
10 Cochrane Library using search terms discharg* plan*, hospital
discharge, patient discharge for all available years.
11. Econ Lit 1969-1996, using search terms discharge plan*.
12. Personal liaison with interested colleagues.
13. EPOC register using relevant terms from EPOC taxonomy.
14. Searching reference lists of review articles and trials.
15. Contact with individual trialists whose trials are included in
the review, to clarify issues, to identify unpublished data, and
to establish awareness of work published and unpublished in
discharge planning.
Additional search terms were added as identified from relevant
articles.
The review was updated using the EPOC trials register in August
2002.
M E T H O D S O F T H E R E V I E W
Three reviewers (SS and JP, or SS and DH) independently selected
the studies to be included in the primary review, and two reviewers
independently selected studies for the update (SS and JM). Any
disagreement was settled by discussion. The quality of the selected
trials was assessed using the criteria described by the EPOC group
(see methods used in reviews under editorial information in group
details). SS and JP, and SS and JM independently assessed the
methodological quality and undertook data extraction using a
checklist developed by EPOC, modified and amended for the
purposes of this review. JP and SS contacted all investigators for
missing data; however, none provided unpublished data.
The primary analysis was a comparison of discharge planning
versus routine discharge care for each of the review questions. The
intention was to group the studies and undertake an exploratory
analysis of the standardised mean differences. We undertook meta
analysis for the effects of discharge planning on mortality, length of
hosptial stay, unscheduled readmission to hospital, and discharge
destination using the fixed effects model to calcuate the Peto odds
ratio. However combining the studies was judged inappropriate
for the other outcomes due to the different methods of measuring
and reporting the remaining outcome variables. We grouped trial
results by participants (patients with a medical condition, a surgical
condition, or patients recruited to a trial with a mix of conditions)
as the discharge planning needs for patients admitted to hospital
for elective surgery could differ from those who are elderly and
are admitted with an acute medical condition, or with multiple
medical conditions. Confidence intervals were calculated when
the authors did not report these.
Methods used to exclude trials from the review:
The decision to exclude trials where discharge planning was part
of a broader package of inpatient care was dependent on the detail
provided by the authors. We also excluded any studies that had
major methodological weaknesses despite fulfilling our criteria for
inclusion; details of why studies were excluded are reported in the
excluded studies section.
D E S C R I P T I O N O F S T U D I E S
Electronic searching yielded a total of 3112 citations. From these
abstracts 55 studies appeared to meet the entry criteria and were
retrieved for further assessment. Eleven trials [Kennedy; Hen-
driksen; Moher; Evans; Naughton; Naylor; Parfrey; Weinberger;
Nazareth; Shaw; Sulch] met all the review criteria and the re-
maining 44 were excluded (see excluded trials table). One of the
trials included in the review was translated from Danish to En-
glish [Hendriksen] the remaining trials were published in English.
Three of these trials [Sulch; Nazareth; Shaw] were identifed for
the recent update of the review. Two of the trials in the update
assessed the effectiveness of a pharmacy discharge plan, one for
elderly patients with a medical condition and the other recruited
both elderly patients and those admitted to a psychiatric hospital
and reported results across both conditions. The third trial in the
update evaluated an integrated care pathway which consisted of
rehabiliation and discharge planning for patients recovering from
a stroke.
Follow-up times varied from 2 weeks to 9 months. The trials in-
cluded in the review evaluated a broadly similar intervention of
discharge planning which included an assessment, planning, im-
plementation and monitoring phase, although two trials did not
describe a monitoring phase (see Characteristics of included stud-
ies). However, the intervention was implemented at varying times
during a patient’s stay in hospital, from admission to 3 days prior
to discharge. The study population differed between the trials. Six
trials recruited patients with a medical condition; one of these trials
included a group of patients with a surgical condition, three trials
recruited patients with a mix of medical and surgical conditions.
Two trials used a questionnaire designed to identify patients likely
to require discharge planning [Evans; Parfrey]. Patients recruited
to nine of the trials were elderly. One trial recruited patients across
two hospitals and reported data separately for the each of the hos-
pitals. For hospital A the average age was 53 years, and for hospital
B 56 years [Parfrey]. Another trial evaluating a pharmacy discharge
plan recruited patients aged from 23 to 86 years [Shaw].
The description of the type of care the control group received var-
ied. One trial did not describe the care received by the control
group [Kennedy]. Six trials described the control group as receiv-
ing usual care with some discharge planning but without a formal
link through a co ordinator to other departments and services,
although other services were available on request from nursing
or medical staff [Hendriksen; Moher; Naylor; Naughton; Parfrey;
Weinberger]. One trial explictly stated that the control group did
not receive discharge planning [Evans]. The control groups in two
4Discharge planning from hospital to home (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

of the trials included in the update that evaluated the effective-
ness of a pharmacy discharge plan did not have access to a review
and discharge plan by a pharmacist [Nazareth; Shaw]. In the third
trial included in the update the control group received multidisci-
plinary care which was not defined in advance but was determined
by the patients’ progress [Sulch].
M E T H O D O L O G I C A L Q U A L I T Y
Seven criteria are recommended by EPOC to judge the quality
of randomised studies, these are described elsewhere (see METH-
ODS USED IN REVIEWS under EDITORIAL INFORMA-
TION in GROUP DETAILS). One of the criteria, follow-up of
professionals, was not relevant to the trials included in this review.
The remaining six criteria were used, and showed that the quality
of the trials was variable, only 5 trials reported full concealment of
allocation, there was insufficient information to determine if this
was attained in the remaining 6 trials. Only four trials reported
blinded assessment of outcomes, and two trials reported no base-
line measurements.
R E S U L T S
Does discharge planning improve the process of patient care?
Comparison 1. Effect of discharge planning on length of stay in
hospital compared to usual care.
We failed to detect a statistically significant difference between
groups from a pooled analysis for hospital length of stay of elderly
patients with a medical condition (weighted mean difference -
0.86, 95% CI -1.9 to 0.18) [Kennedy; Moher; Naughton; Naylor;
Sulch]. Trials not included in the pooled analysis did not report a
significant difference in length of stay for surgical patients (differ-
ence +1.0 day, 95% CI -2.0 to 4.0) [Naylor], or for a mixed group
of patients recovering from surgery or with a medical condition
(difference -3.3 days, p>0.05 [Hendriksen]; difference -0.6, 95%
CI -2.38 to 1.18 [Evans]). Only one trial [Parfrey], recruiting from
two hospitals, reported a small significant reduction in length of
stay for patients receiving discharge planning in one hospital only
(median difference - 0.8 days, p<0.03).
Comparison 2. Effect of discharge planning on unscheduled read-
mission rates compared to usual care.
Seven trials measured readmission to hospital, results were reported
as rates of readmission to hospital or days spent in hospital as
a result of readmission. We pooled readmission data for the tri-
als recruiting elderly patients with a medical condition reporting
readmission rates at up to 3 months of discharge from hospital
[Kennedy; Moher; Naylor; Shaw; Nazareth]. We failed to detect a
difference between those allocated to discharge planning and those
in the control group (OR 0.91, 95% CI 0.67 to 1.23). One trial
not included in the pooled analysis presented readmission data
in a number of different ways [Weinberger]. Although a statisti-
cally significant increase in mean monthly readmission rate was
observed at six months follow-up for patients receiving discharge
planning (intervention group = 0.19 (sd+0.4) control group = 0.14
(sd+ 0.2) p= 0.005), and for the mean number of readmission days
(intervention 10.2 (19.8), control 8.8 (19.7) p<0.04), no statisti-
cally significant difference was detected at 6 months follow-up for
the proportions of patients readmitted to hospital (intervention =
49% control = 44% p = 0.06) [Weinberger]. One trial reported
a significant reduction in readmission days for patients allocated
to discharge planning (mean difference -33 days at 2 to 6 weeks
follow-up, 95% CI -53 to -13) [Naylor]; however, this difference
was not detected at longer term follow-up. These findings were
not replicated in another trial measuring readmission days at 1
year follow-up (difference +2 days, p >0.05 [Hendriksen].
No significant reduction in readmission rates (difference +3%,
95% CI-7% to 13%), or days in hospital due to readmission (dif-
ference +26 days, 95% CI -8 to +60 at 6 - 12 weeks) were reported
for patients recovering from surgery [Naylor].
Only one trial recruiting a mix of patients reported data on read-
mission [Evans]. A statistically significant decrease in readmissions
was observed for those receiving discharge planning (difference -
11%, 95% CI -17% to -4%) at 4 weeks follow-up; however, this
difference was not detected at 9 months follow-up (difference -
6%, 95% CI -12.5% to 0.84%; p>0.08). There was a significant
reduction in the days in hospital due to readmission (difference -
2.0, 95% CI -3.18 to -0.82).
Comparison 3. Effect of discharge planning on the incidence of
complications related to the initial admission compared to usual
care.
No studies provided data for this comparison.
Comparison 4. Effects of discharge planning on other process
variables: patients’ place of discharge.
Five trials provided data on patients’ place of discharge. A meta
analysis looking at the proportion of patients being discharged
home failed to detect a statistical difference between groups (OR
1.15, 95% CI 0.72 to 1.82) [Moher; Sulch]. One trial [Evans] re-
cruiting both medical and surgical patients reported that a greater
proportion of patients allocated to discharge planning were dis-
charged home compared with those receiving no formal discharge
planning (difference 6% 95% CI 0.4% to 12%), this difference
increased at 9 months follow up (difference 8.3% 95% CI 1.6% to
15%). Two trials failed to detect a difference in the proportion of
patients discharged to a nursing home [Naughton; Hendriksen].
Does discharge planning improve or (at least) have no adverse
effect on patient outcome?
Comparison 5. Effect of discharge planning on mortality rate com-
pared to usual care.
A meta analysis of 2 trials failed to detect a statistically significant
difference in mortality at 9 months (OR 1.44, 95% CI 0.82 to
5Discharge planning from hospital to home (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

2.51) [Nazareth; Sulch]. The two trials recruited different pop-
ulations, one recruited elderly patients with a range of medical
conditions and the other patients recovering from a stroke. One
study [Evans] recruiting a mix of surgical and medical patients
failed to detect a difference between groups at 9 months follow up
(treatment group 66/417 (16%), compared with 67/418 (16%)
in the control group).
Comparison 6. Effect of discharge planning on patient health out-
comes compared to usual care.
Six trials measured patient outcomes including functional status,
mental well-being, perception of health, self-esteem and affect.
Three of these trials did not publish follow up data [Kennedy;
Naylor; Weinberger]. One trial recruiting patients with medical
conditions reported no differences between groups for functional
status (mean difference on the Barthel Index -1.2, 95% CI -4.05
to 1.65, [Evans]), whereas another trial recruiting patients recov-
ering from a stroke reported a significant improvement from 4 to
12 weeks for those allocated to the control group, who received
conventional multidisciplinary care, on the Barthel score (median
change: control group 6 versus treatment group 2, p<0.01), and
for a change in the Euroqol score at 26 weeks (control group 72
versus treatment group 63 p<0.005), but failed to detect a dif-
ference for the Rankin score and the hospital anxiety and depres-
sion scale [Sulch]. A trial evaluating a pharmacy discharge plan
for elderly medical patients failed to detect a difference with the
General Well Being questionnaire (mean difference 0.1, 95% CI
-0.14 to 0.34) at 6 months [Nazareth].
Comparison 7. Effect of discharge planning on patients’ and carers’
satisfaction compared to usual care.
One trial recruiting patients with a medical condition reported
increased patient satisfaction for those allocated to discharge plan-
ning at one and six months follow up, with the greatest differences
reported for patients’ perceptions of continuity of care and non fi-
nancial access to medical care [Weinberger]. Another trial recruit-
ing fewer patients failed to detect a difference between groups for
patient satisfaction at three and six months follow up [Nazareth].
In the study by Moher a subgroup of 40 patients, who were asked
to complete a satisfaction questionnaire, reported increased sat-
isfaction with discharge planning (difference 27%, p<0.05, 95%
CI 2% to 52%) [Moher].
Does discharge planning reduce overall costs of health care?
Comparison 8. Effect of discharge planning on hospital care costs
compared to usual care.
In the study by Naylor [Naylor] involving patients with a med-
ical condition no significant differences for costs between the
two groups for their initial hospital stay were observed. However,
a significant difference for hospital costs was detected for total
charges including readmission costs at 2 weeks follow-up (dif-
ference-$170,247, 95%CI -$253,000 to -$87,000) and at 2 to
6 weeks follow-up (difference -$137,508, 95%CI -$210,000 to
-$67,000) with patients receiving discharge planning incurring
lower costs. No significant difference in costs was detected for pa-
tients with surgical conditions in the same study [Naylor].
The study by Naughton [Naughton] observed lower costs for lab-
oratory services for patients receiving discharge planning (mean
difference per patient -£295, 95% CI -£564 to -£26).
Comparison 9. Effect of discharge planning on community care
costs compared to usual care.
No studies provided cost data for this comparison. Weinberger
[Weinberger] measured the use of primary care and reported a
significant increase in the use of primary care by those allocated to
discharge planning (median time from hospital discharge to first
primary care consultation t=7 days, c=13 days, p<0.001; mean
number of visits to general medical clinic t=3.7 days, c=2.2 days
p<0.001). One trial provided data on general practitioner con-
sultations and failed to detect a difference between groups at 3
months (mean difference 2.7%, 95% CI -7.4% to 12.7%) and
at 6 months (mean difference 0.3% 95% CI -11.6% to 12.3%)
[Nazareth].
Comparison 10. Effect of discharge planning on overall costs of
health care compared to usual care.
One trial [Naughton] reported no significant difference between
the groups for overall health service costs.
Comparison 11. Effect of a pharmacy discharge plan on the use
of medication.
Both trials evaluating the effectiveness of a pharmacy discharge
plan measured different outcomes related to medication. Shaw
[Shaw] failed to detect a difference in the mean number of prob-
lems with medication reported (at 12 weeks T=1.4 (SD 1.2) n=21,
C=2.4 (SD 1.6) n=14). Problems included difficulty obtaining
a prescription from the general practicioner (GP), insufficient
knowledge about the medication and non compliance. Nazareth
also failed to detect a difference between groups for adherence to
medicines, knowledge about medicines and hoarding of medicines
[Nazareth].
D I S C U S S I O N
This review assessed the effectiveness of discharge planning in hos-
pital. Eleven randomised controlled trials met the pre-set criteria
for inclusion, three of these were included in this update. Meta-
analysis of 5 trials recruiting elderly medical patients failed to de-
tect a difference for the primary measures of outcome of length
of stay and readmission to hospital within 3 months of discharge.
However, it could be argued that even a small reduction in length
of stay or readmission to hospital may have an impact on the
timeliness of subsequent admissions in a system where there is a
shortage of acute hospital beds. A pooled analysis of two trials, one
recruiting patients recovering from a stroke [Sulch] and the other
elderly patients with a mix of conditions [Nazareth], suggests a
non significant increase in the odds of death of 44%, with 95%
6Discharge planning from hospital to home (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

CI of 0.82 to 2.51 at 6 to 9 months follow up. If true this result
is potentially important; however, interpretation is limited by the
small number of trials (2 trials with 152 [Sulch] and 362 patients
[Nazareth]), and the different patient populations and interven-
tions. Participants in the Sulch trial were recovering from a stroke
requiring inpatient hospital rehabilitation and had an average age
of 74 to 75 years. Most of the deaths occured after discharge from
hospital. Interestingly Sulch reported a quicker improvement in
quality of life and activities of daily living for the control group,
the authors speculate that this surprise finding may be due to a
less structured, more flexible approach to continuing patient as-
sessment. The mean age of participants in the trial evaluating a
pharmacy discharge plan was 84 years, and participants had an av-
erage of three chronic conitions. Mortality should be measured in
future trials to explore this finding. No differences in other health
outcomes were reported, and there is some evidence to suggest that
patients receiving discharge planning experience increased levels
of satisfaction with their care [Moher; Weinberger].
Two trials examining cost to the health service of implementing
discharge planning failed to detect a difference in health service
costs between those receiving discharge planning and those receiv-
ing standard care [Naughton; Naylor]. In one trial [Naylor] costs
to the health service were calculated using hospital charges, not
on the basis of resources used. The method of costing was not
described in the second trial [Naughton]. Although the costs re-
ported by the two trials differ, the variation in charges between dif-
ferent provider units makes it difficult to comment on the mean-
ing of these differences.
A key issue in interpreting the evidence is the definition of the in-
tervention and the subsequent understanding of the relative con-
tribution of each element. Authors of all of the trials provided
some description of the intervention, however it was not possi-
ble to assess how some components of the process compared be-
tween trials. For example the trial conducted by Naylor [Naylor]
formalised the inclusion of the patient’s caregiver into the assess-
ment process, and included the caregiver in the development of
the discharge plan. Although inclusion of the caregiver or fam-
ily was mentioned by the majority of the other trials [Kennedy;
Hendriksen; Evans; Naughton] the degree to which this was done
was not always apparent. Two of the trials [Evans; Parfrey] used
an assessment tool to find cases eligible for discharge planning.
The monitoring of discharge planning also differed. In one trial
this was done primarily by telephone [Naylor]; and in another
trial patients were given appointments to attend a primary care
clinic [Weinberger]. The context in which an intervention such
as discharge planning is delivered may also play a role, not only
in the way the intervention is delivered but in the way services
are configured for the control group. Five of the trials included
in this review were based in the USA, three in the UK, two in
Canada and one in Denmark. In each country the orientation
of primary care services differs, which may affect communication
between services. Different perceptions of care by professionals of
alternative care settings, and funding arrangements, may also in-
fluence timely discharge. The point in a patient’s hospital admis-
sion when discharge planning was implemented also varied across
studies. Two trials reported discharge planning commencing from
the time a patient was admitted to hospital [Parfrey; Sulch] and
another that discharge planning was implemented three days prior
to discharge [Weinberger]. The timing of an intervention such as
discharge planning, which depends on organising other services,
will have some bearing on how quickly these services can begin
delivering care. The patient population may also impact on out-
come; for example, patients recruited to the trial by Weinberger
were experiencing major complications from their chronic disease,
and this combined with an intervention designed to increase the
intensity of primary care services may explain the observed in-
crease in readmission days for those receiving the intervention.
Interestingly in the update of this review we only identified three
trials that met our inclusion criteria [Nazareth; Shaw; Sulch]. Two
trials focused on specific interventions examining the impact of
a pharmacy discharge plan on readmission rates, and other out-
comes such as knowledge of medication and health status. The
third trial evaluated the effectiveness of an integrated care pathway
that focused on rehabiliation and used a structured approach to
discharge planning for patients recovering from a stroke. With the
move towards care pathways it is possible that discharge planning
will be less frequently implemented as an intervention in isolation,
but will be part of an integrated package of care. This will present
further challenges in interpreting the evidence as it will become
more difficult to understand the relative contribution of each as-
pect of health care.
A U T H O R S ’ C O N C L U S I O N S
Implications for practice
This review indicates that the impact of discharge planning that
occurs while a patient is in hospital is uncertain on readmission
rates, hospital length of stay and health outcomes. However, it is
possible that even a small reduction in length of stay or readmission
rate could free up capacity for subsequent admissions in a system
where there is a shortage of acute hospital beds. It is not clear if
costs are reduced or shifted from secondary to primary care as a
result of discharge planning. Interestingly there is no evidence that
health care services outside a secondary care setting have adopted
discharge planning, despite patients’ requirements, and hence the
appropriateness of a place of care, changing over time; and waiting
lists for placement in a nursing home or for home care services.
Systematic reviews have been published in related areas; for ex-
ample, geriatric assessment which includes discharge planning as
part of a broader package of care (Stuck, 1993), and integrated
care pathways for stroke. This latter review concluded that this
type of care may be associated with both positive and negative ef-
7Discharge planning from hospital to home (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

fects on the process of care and clinical outcomes (Kwan 2003). A
recently published review by Parker included discharge planning
interventions that were in a hospital setting, comprehensive geri-
atric assessment, discharge support arrangements and educational
interventions, and concluded that interventions providing an ed-
ucational component had an effect on reducing readmission rates
(Parker 2002).
Implications for research
Surprisingly some of the stated policy aims of discharge planning
(bridging the gap between hospital and home) were not reflected
in the trials included in this review. An important element of dis-
charge planning is the effectiveness of communication between
hospital and community, yet this was not reported in any of the
trials included in this review. The expectation is that discharge
planning will ensure that patients are discharged from hospital
at an appropriate time in their care, and with adequate notice,
to organise the provision of other services. A high level of com-
munication between the discharge planner and the providers of
services outside the hospital setting is clearly important. Future
well conducted studies should collect mortality data to provide a
more robust estimate of this important outcome, and ensure the
generalisability of results by providing details of the intervention
and the context in which it was delivered. Safeguards should be
developed against contamination of the control group, for exam-
ple through the design of trials employing cluster randomisation.
Methods should be developed to measure the impact of a delayed
or inappropriate discharge on overall bed utilisation.
F E E D B A C K
Cochrane Highly Sensitive Search Strategy
Summary
The Cochrane Highly Sensitive Search Strategy should BE REF-
ERENCED ’Dickersin K, Scherer R, Lefebvre C. Identifying rel-
evant studies for systematic reviews. BMJ 1994;309:1286-91’ in-
stead of ’Anonymous. Medline optimally sensitive search strategy
(OSS) for SilverPlatter. Workshop on Identifying and Registering
Trials. UK Cochrane Centre, 1996’.
Author’s reply
This change has now been made.
Contributors
Mike Clarke
P O T E N T I A L C O N F L I C T O F
I N T E R E S T
None
A C K N O W L E D G E M E N T S
Diana Harwood for assisting in scanning abstracts retrieved from
electronic searches, NHS R&D Anglia and Oxford for contribut-
ing to the funding of the original review Jeremy Grimshaw, Andy
Oxman and Daryl Wieland for helpful comments on earlier drafts.
S O U R C E S O F S U P P O R T
External sources of support
• Imperial College School of Medicine UK
Internal sources of support
• Anglia and Oxford Regional Research and Development Pro-
gramme. UK
R E F E R E N C E S
References to studies included in this review
Evans {published data only}
Evans, R. L, Hendricks, R. D. Evaluating Hospital Discharge Plan-
ning: a Randomised Controlled Trial. Medical Care 1993;31(4):358–
370.
Hendriksen {published data only}
Hendriksen, C, Stromgard, E, Sorensen, K. [Current cooperation
concerning admission to and discharge from geriatric hospitals].
[Danish] [Current cooperation concerning admission to and dis-
charge from geriatric hospitals]. [Danish] [Nyt samarbejde om gamle
menneskers syehusindlaeggelse og - udskrivelse]. Nordisk Medicin
1990;105:58–60.
Kennedy {published data only}
Kennedy, L, Neidlinger, S, Scroggins, K. Effective comprehensive
discharge planning. The Gerontologist 1987;27(5):577–580.
Moher {published data only}
Moher, D, Weinberg, A, Hanlon, R, Runnalls, K. Effects of a medical
team coordinator on length of hospital stay. Can Med Assoc J 1992;
146(4):511–515.
Naughton {published data only}
Naughton, B, Moran, M, Feinglass, J, Falconer, J. Reducing hospital
costs for the geriatric patient admitted from the emergency depart-
ment: a randomised trial. J Am Geriatr. Soc 1994;42:1045–1049.
Naylor {published data only}
Naylor, M, Brooten, D, Jones, R, Lavizzo, M.R, Mezey, M, Pauly,
8Discharge planning from hospital to home (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

M. Comprehensive discharge planning for the hospitalised elderly: a
randomized clinical trial. Ann. Intern. Med 1994;120:999–1006.
Nazareth {published data only}
Nazareth, I, Burton, A, Shulman, S, Smith, P, Haines, A. A phar-
macy discharge plan for hospitalized elderly patients - a randomized
controlled trial. Age and Ageing 2001;30:33–40.
Parfrey {published data only}
Parfrey, P. S, Gardner, E, Vavasour, H, et al.The feasibility and efficacy
of early discharge planning initiated by the admitting department in
two acute care hospitals. Clin. Invest. Med 1994;17:88–96.
Shaw {published data only}
Shaw, H, Mackie, C A, Sharkie, I. Evaluation of effect of phar-
macy discharge planning on medication problems experienced by
discharged actue admission mental health patients. The International
Journal of Pharmacy Practice 2000;8:144–153.
Sulch {published data only}
Sulch, D, Perez, I, Melbourn, A, Kalra, L. Randomized controlled
trial of integrated (managed) care pathway for stroke rehabilitation.
Stroke 2000;31(8):1929–1934.
Weinberger {published data only}
Weinberger, M, Oddone, E. Z, Henderson, W. G. Does increased
access to primary care reduce hospital admissions? Veterans Affairs
Cooperative Study Group on Primary Care and Hospital Readmis-
sions. N. Engl. J Med 1996;334:1441–1447.
References to studies excluded from this reviewApplegate
Applegate, W. B, Miller, S. T, Graney, M. J, Elam, J. T, Akins, D.
E. A randomized controlled trial of a geriatric assessment unit in a
community rehabilitation hospital. N. Engl. J. Med 1990;322:1572–
1578.
Brooten
Brooten, D, Kumar, S, Brown, L. P, et al.A randomized clinical trial
of early hospital discharge and home follow-up of very-low-birth-
weight infants. NLN Publications 1987;21-2194:95–106.
Brooten D
Brooten, D, Roncoli, M, Finkler, S, Arnold, L, Cohen, A, Mennuti,
M. A randomized trial of early hospital discharge and home follow-
up of women having cesarean birth. Obstet. Gynecol 1994;84:832–
838.
Carty
Carty, E. M, Bradley, C. F. A randomized, controlled evaluation of
early postpartum hospital discharge. Birth 1990;17:199–204.
Casiro
Casiro, O. G, McKenzie, M. E, McFadyen, L, et al.Earlier discharge
with community-based intervention for low birth weight infants: a
randomized trial. Pediatrics 1993;92:128–134.
Choong
Choong, PFM, Langford, AK, Dowsey, MM, Santamaria, NM. Clin-
ical pathway for fractured neck of femur: a prospective controlled
study. Medical Journal of Australia 2000;172:423–426.
Donahue
Donahue, D, Brooten, D, Roncoli, M, et al.Acute care visits and re-
hospitalization in women and infants after cesarean birth. J. Perinatol
1994;14:36–40.
Dudas
Dudas, V, Bookwalter, T, Kerr, KM, Pantilat, SZ. The impact of fol-
low up telephone calls to patients after hospitalization. The American
Journal of Medicine 2001;111(9b):26s–30s.
Epstein
Epstein, A. M, Hall, J. A, Fretwell, M, et al.Consultative geriatric
assessment for ambulatory patients. A randomized trial in a health
maintenance organization. JAMA 1990;263:538–544.
Fretwell
Fretwell, M. D, Raymond, P. M, McGarvey, S. T, et al.The Senior
Care Study. A controlled trial of a consultative/unit-based geriatric
assessment program in acute care. J Am Geriatr. Soc 1990;38:1073–
1081.
Gayton
Gayton, D, Wood, D. S, de-Lorimer, M, Tousignant P, Hanley, J.
Trial of a geriatric consultation team in an acute care hospital. J Am
Geriatr. Soc 1987;35:726–736.
Germain
Germain, M, Knoeffel, F, Wieland, D, Rubenstein, L. Z. A geriatric
assessment and intervention team for hospital inpatients awaiting
transfer to a geriatric unit: a randomized trial. Aging Milano 1995;7:
55–60.
Gillette
Gillette, Y, Hansen, N. B, Robinson, J. L, Kirkpatrick, K, Grywalski,
R. Hospital-based case management for medically fragile infants:
results of a randomized trial. Patient. Educ. Couns 1991;17:59–70.
Haggmark
Haggmark, C, Nilsson, B. Effects of an intervention programme for
improved discharge planning. Vard I Norden 1997;2:4–8.
Hansen
Hansen, F. R, Spedtsberg, K, Schroll, M. Geriatric follow-up by home
visits after discharge from hospital: a randomized controlled trial.
Age. Ageing 1992;21:445–450.
Hendriksen cooperati
Hendriksen, C, Stromgard, E, Sorensen, K. H. Cooperation concern-
ing admission to and discharge of elderly people from the hospital.
1. The coordinated contributions of home care personnel [Samar-
bejde om gamle menneskers sygehusindlaeggelse og - udskrivelse. 1.
Hjemmesygeplejerskens koordinerende indsats pa sygehuset]. Ugeskr.
Laeger 1989;151:1531–1534.
Hogan
Hogan, D. B, Fox, R. A. A prospective controlled trial of a geriatric
consultation team in an acute-care hospital. Age. Ageing 1990;19:
107–113.
Jenkins
Jenkins, H. M, Blank, V, Miller, K, Turner, J, Stanwick, R. S. A
randomized single-blind evaluation of a discharge teaching book for
pediatric patients with burns. J Burn. Care Rehabil 1996;17:49–61.
Karppi
Karppi, P, Tilvis, R. Effectiveness of a Finnish geriatric inpatient
assessment. Two-year follow up of a randomized clinical trial on
community-dwelling patients. Scand. J. Prim. Health Care 1995;13:
93–98.
9Discharge planning from hospital to home (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Kravitz
Kravitz, R. L, Reuben, D. B, Davis, J. W, et al.Geriatric home as-
sessment after hospital discharge. J. Am. Geriatr. Soc 1994;42:1229–
1234.
Landefield
Landefield, C. S, Palmer, R. M, Kresevic, D. M, Fortinsky, R. H,
Kowal, J. A randomized controlled trial of care in a hospital medical
unit especially designed to improve functional outcomes of acutely
ill older patients. N Engl J Med 1995;332:1338–1344.
Martin
Martin, F, Oyewole, A, Moloney, A. A randomized controlled trial
of a high support hospital discharge team for elderly people. Age and
Ageing 1994;23:228–234.
McGrory
McGrory, A, Assmann, S. A study investigating primary nursing,
discharge teaching, and patient satisfaction of ambulatory cataract
patients. Insight 1994;19 (2):8-13, 29.
Melin
Melin, A. L. A randomized trial of multidisciplinary in-home care for
frail elderly patients awaiting hospital discharge. Aging Milano 1995;
7:247–250.
Melin health
Melin, A. L, Wieland, D, Harker, J. O, Bygren, L. O. Health out-
comes of a post-hospital in-home team care: secondary analysis of a
Swedish trial. J. Am. Geriatr. Soc 1995;43:301–307.
Melin re-hab
Melin, A. L, Hakansson, S, Bygren, L. O. The cost-effectiveness of
rehabilitation in the home: A study of Swedish elderly. American
Journal of Public Health 1993;83:356–362.
Murray
Murray, S. K, Garraway, W. M, Akhtar, A. J, Prescott, R. J. Com-
munication between home and hospital in the management of acute
stroke in the elderly: results from a controlled trial. Health Bulletin
1995;40/5:214–219.
Naylor comp
Naylor, M. D, Brooten, D, Campbell. R, et al.Comprehensive dis-
charge planning and home follow-up of hospitalized elders: a ran-
domized controlled trial. JAMA 1999;281:613–620.
Nikolaus
Nikolaus, T, Specht Leible, N, Bach, M, Wittmann Jennewein, C,
et al.Effectiveness of hospital-based geriatric evaluation and manage-
ment and home intervention team (GEM-HIT): Rationale and de-
sign of a 5-year randomized trial. Z. Gerontol. Geriatr 1995;28:47–
53.
Reuben
Reuben, D. B, Borok, G. M, Wolde, T. G, et al.A randomized trial
of comprehensive geriatric assessment in the care of hospitalized pa-
tients. N. Engl. J Med 1995;332:1345–1350.
Rich
Rich, M. W, Beckham, V, Wittenberg, C, Leven, C. L, Freedland,
K. E, Carney, R. M. A multidisciplinary intervention to prevent the
readmission of elderly patients with congestive heart failure. N. Engl.
J. Med 1995;333:1190–1195.
Rich prevention
Rich, M. W, Vinson, J. M, Sperry, J. C, et al.Prevention of read-
mission in elderly patients with congestive heart failure: results of
a prospective, randomized pilot study. J. Gen. Intern. Med 1993;8:
585–590.
Rubenstein
Rubenstein, L. Z, Josephson, K. R, Wieland, G. D, English, P. A,
Sayre, J. A, Kane, R. L. Effectiveness of a geriatric evaluation unit.
N. Engl. J. Med 1984;311:1664–1670.
Saltz
Saltz, C. C, McVey, L. J, Becker, P. M, Feussner, J. R, Cohen, H. J.
Impact of a geriatric consultation team on discharge placement and
repeat hospitalization. The Gerontologist 1988;28:344–350.
Siu
Siu, A. L, Kravitz, R. L, Keeler, E, et al.Postdischarge geriatric assess-
ment of hospitalized frail elderly patients. Arch. Intern. Med 1996;
156:76–81.
Smith
Smith, D. M, Weinberger, M, Katz, B. P, Moore, P. S. Postdischarge
care and readmissions. Med. Care 1988;26:699–708.
Thomas
Thomas, D. R, Brahan, R, Haywood, B. P. Inpatient community-
based geriatric assessment reduces subsequent mortality. J. Am. Geri-
atr. Soc 1993;41:101–104.
Townsend
Townsend, J, Piper, M, Frank, A. O, Dyer, S, North, W. R, Meade,
T. W. Reduction in hospital readmission stay of elderly patients by
a community based hospital discharge scheme: a randomized con-
trolled trial. BMJ 1988;297:544–547.
Victor
Victor, C. R, Vetter, N. J. Rearranging the deckchairs on the Titanic:
failure of an augmented home help scheme after discharge to reduce
the length of stay in hospital. Arch. Gerontol. Geriatr 1988;7(1):83–
91.
Winograd
Winograd, C. H, Gerety, M. B, Lai, N. A. A negative trial of inpa-
tient geriatric consultation. Lessons learned and recommendations
for future research. Arch. Intern. Med 1993;153 (17):2017–2023.
Additional referencesAnderson 1984
Anderson GF, Steinberg EP. Hospital readmissions in the Medicare
population. N Engl J Med 1984;311:1349–53.
Anderson 1985
Anderson GF, Steinberg EP. Predicting hospital readmissions in the
Medicare population. Inquiry 1985;22:251–8.
Barker 1985
Barker WH, Williams TF, Zimmer JG, Van Buren C, Vincent SJ,
Pickrel SG. Geriatric consultation teams in acute hospitals: impact
on back-up of elderly patients. J Am Geriatr Soc 1985;33:422–8.
Brent Soc Ser 1991
Brent Social Services Dept. Hospital disharge and continuing care in
Brent, London. London: Brent Social Services Dept, 1991.
Dept of Health 2003
Department of Health. Discharge from hospital: pathway, process
and practice [A manual of discharge practice for health and social care
10Discharge planning from hospital to home (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

commissioners, managers and practitioners]. Department of Health;
www.doh.gov.uk/changeagentteam/discharge_getri.pdf 2003.
Dickersin 1994
Dickersin K, Scherer R, Lefebvre C. Identifying relevant studies for
systematic reviews. BMJ 1994;309:1286–91.
Kwan 2003
Kwan, J, Sandercock. P. In hospital care pathways for stroke. Cochrane
Library 2003, Issue 2.
Marks 1994
Marks L. Seamless care or patchwork quilt? Discharging patients from
acute hospital care. London: Kings Fund, 1994.
Parker 2002
Parker, SG, Peet, SM, McPherson< A, Cannaby, AM, Abrams, K,
Baker, R, Wilson, A, . Lindesay, J, Parker, G, Jones, DR. A systematic
review of discharge arrangements for older people. Health Technol
Assess 2002;6(4):1–183.
Schwartz 1991
Schwartz WB, Mendelson DN. Hospital cost containment in the
1980s. Hard lessons learned and prospects for the 1990s. N Engl J
Med 1991;324:1037–42.
Selker 1989
Selker HP, Beshansky JR, Pauker SG, Kassirer JP. The epidemiology
of delays in a teaching hospital. Med Care 1989;27:112.
Stuck, 1993
Stuck, AE, Sui AL, Wieland, GD, Adams, J, Rubenstein, LS. Com-
prehensive geriatric assessment: a meta analysis of controlled trials.
Lancet 1993;342:1032–1036.
Townsend 1988
Townsend J, Piper M, Frank AO, Dyer S, North WR, Meade TW.
Reduction in hospital readmission stay of elderly patients by a com-
munity based hospital discharge scheme: a randomised controlled
trial. BMJ 1988;297:544–7.
Victor 1988
Victor CR, Vetter NJ. Preparing the elderly for discharge from hospi-
tal: a neglected aspect of patient care?. Age Ageing 1988;17:155–63.
Williams 1988
Williams EI, Fitton F. Factors affecting early unplanned readmission
of elderly patients to hospital. BMJ 1988;297:784–7.
Young 1991
Young E, et al.Older people at the interface. A study of the provision of
services within Parkside Health Authority [occasional paper]. London:
Dept Gen Practice St Mary’s Hospital, 1991.
T A B L E S
Characteristics of included studies
Study Evans
Methods RCT
Participants Elderly medical, neurological, surgical
average age
T=66.6
C=67.9
Number recruited:
T=417
C=418
Interventions Discharge planning by physician and research assistant. Questionnaire to identify eligible patients followed
by assessment, planning, implementation, monitoring
Setting: V A Hospital, Seattle
Outcomes Hospital length of stay, re admission to hospital, discharge destination, health status
Notes Also validated an instrument to assess high risk patients
Intervention implemented on day 3 of hospital admission
Allocation concealment B – Unclear
Study Hendriksen
Methods RCT
11Discharge planning from hospital to home (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Characteristics of included studies (Continued )
Participants Elderly patients admitted to 4 wards, including surgical
median age
T=76.5
C=76.6
Number recruited:
T=135
C=138
Interventions Discharge planning by co ordinator, a project /community nurse (assessment, planning, implementation,
monitoring)
Setting: Hospital in suburb of Copenhagen
Outcomes Hospital length of stay, re admission to hospital, discharge destination
Notes Details of measures of outcome not provided. Translated from Danish.
Intervention implemented at time of admission
Allocation concealment B – Unclear
Study Kennedy
Methods RCT
Participants Elderly acute care medical patients
average age
T=80.1
C=80.5
Number recruited:
T=39
C=41
Interventions Discharge planning protocol by geriatric nurse, and research assistant (assessment, planning, implementation,
monitoring)
Setting: Setting: 500 bed non-profit acute care teaching hospital, Texas
Outcomes Hospital length of stay, re admission to hospital, discharge destination, health status
Notes Not clear when intervention implemented
Allocation concealment A – Adequate
Study Moher
Methods RCT
Participants Elderly medical patients
average age
T=66.3
C=64.3
Number recruited:
T=136
C=131
Interventions Discharge planning - medical team co ordinator (nurse) (assessment, planning, implementation)
Setting: 2 clinical teaching units,
Ottawa
Outcomes Hospital length of stay, re admission to hospital, discharge destination, patient satisfaction
12Discharge planning from hospital to home (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd
Characteristics of included studies (Continued )
Notes Baseline data recorded only on age, sex, diagnosis
Not clear when intervention implemented
Allocation concealment B – Unclear
Study Naughton
Methods RCT
Participants Elderly medical patients admitted from emergency department
Average age
80 yrs
Number recruited:
T=51
C=60
Interventions Discharge planning- geriatrician and social worker: assessment, planning, intervention and monitoring
Setting: Private, non-profit, academic medical centre,
Chicago
Outcomes Hospital length of stay, discharge destination, health service costs
Notes Intervention implemented at time of admission
Allocation concealment B – Unclear
Study Naylor
Methods RCT
Participants Elderly medical and cardiac surgery patients
Average
76 years
Number recruited:
T=140
C=136
Interventions Discharge planning by geriatric nurse specialist (assessment, planning, implementation and monitoring
Setting: Hospital of the University of Pennsylvania
Outcomes Hospital length of stay, re admission to hospital, health status, health service costs
Notes Intervention implemented at time of admission
Allocation concealment B – Unclear
Study Nazareth
Methods RCT
Participants Elderly patients, aged 75 years and over, on 4 or more medicines who were discharged from 3 acute wards
and one long stay ward. Each patient had a mean of 3 chronic medical conditions, and was on a mean of 3
drugs (SD 2) at discharge. Mean age of participants 84 years (SD 5.2)
Interventions Hospital pharmacist assessed patients medication, rationalized the drug treatment, provided information and
liaised with carer and community professionals. An aim was to optimize communication between secondary
and primary care professionals Copy of the discharge plan were given to the patient, carer, community
pharmacist and GP.
Follow up visit by community hospital at 7 to 14 days after discharge to check medication and intervene if
necessary. Subsequent visits arranged if appropriate.
13Discharge planning from hospital to home (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Characteristics of included studies (Continued )
Includes an assessment, planning, implementation and monitoring phase.
Outcomes Hospital re admission; mortality; quality of life; client satisfaction; knowledge and adherence to prescribed
drugs; consultation with GP.
Notes
Allocation concealment A – Adequate
Study Parfrey
Methods RCT
Participants Medical and surgical patients
Average
Hospital A
53 yrs
Number recruited:
Hospital A
T=421
C=420
Interventions Discharge planning - admitting department personnel referred to nursing, social work, physiotherapy, oc-
cupational therapy, or dietary services for possible discharge planning (questionnaire to identify eligible pa-
tients): assessment, planning, implementation.
Setting: Newfoundland
Outcomes Hospital length of stay
Notes Also validated an instrument to assess high risk patients.
Intervention implemented at time of admission
Allocation concealment A – Adequate
Study Shaw
Methods RCT
Participants Patients discharged from a psychiatric hospital or care of the elderly ward with a mean age of 47 (SD 17)
years. 82% in the intervention group were diagnosed with an affective disorder, and 57% in the control
group. 43% in the intervention group were diagnosed with a psychotic disorder, and 16% in the control
group. Number of drugs on admission ranged from 1 to 10.
Interventions A pharmacy discharge checklist to identify particular problems, such as therapeutic drug monitoring, com-
pliance aid requirements, and side effects. Patients’ knowledge, obtained from a questionnaire up to 7 days
prior to discharge, was completed by all recruited patients, was incorporated into the checklist and specific
information provided to patients prior to discharge. A pharmacy discharge plan was supplied to the patients’
community pharmacist for the intervention group. Includes an assessment, planning, implementation and
monitoring phase.
Outcomes Re admission to hospital, re admission due to non compliance, medication problems after being discharged
from hospital
Notes
Allocation concealment B – Unclear
Study Sulch
Methods RCT
Participants Patients with a mean age (SD)
14Discharge planning from hospital to home (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd
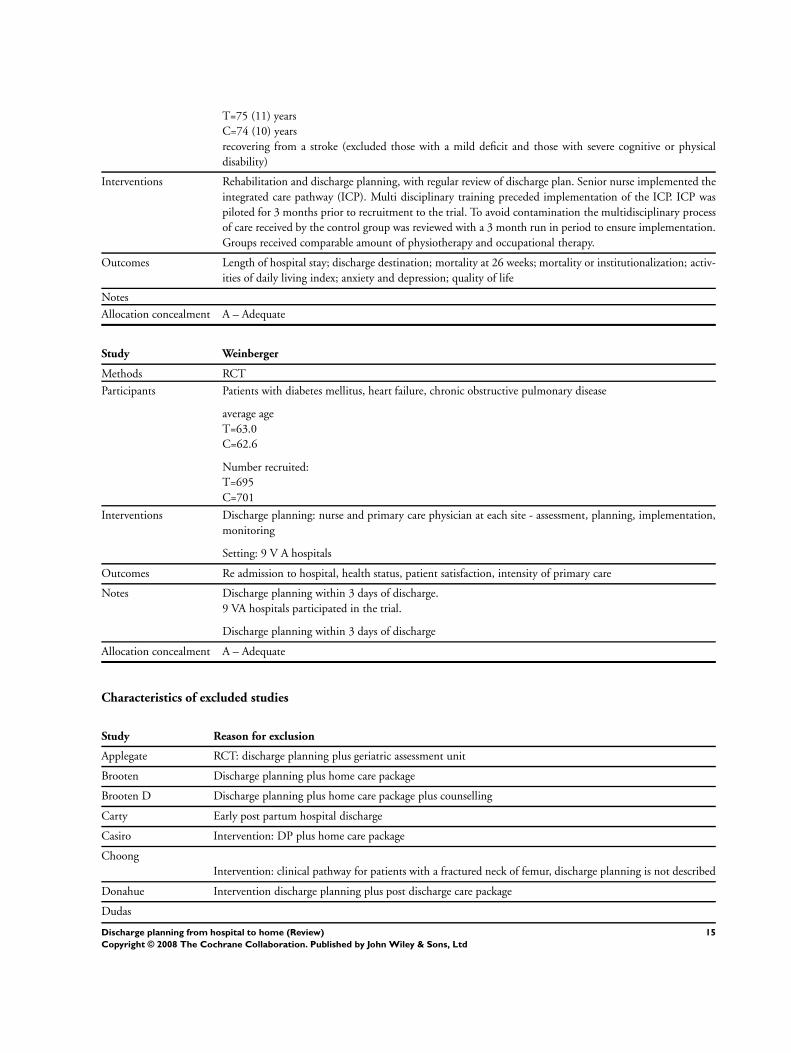
T=75 (11) years
C=74 (10) years
recovering from a stroke (excluded those with a mild deficit and those with severe cognitive or physical
disability)
Interventions Rehabilitation and discharge planning, with regular review of discharge plan. Senior nurse implemented the
integrated care pathway (ICP). Multi disciplinary training preceded implementation of the ICP. ICP was
piloted for 3 months prior to recruitment to the trial. To avoid contamination the multidisciplinary process
of care received by the control group was reviewed with a 3 month run in period to ensure implementation.
Groups received comparable amount of physiotherapy and occupational therapy.
Outcomes Length of hospital stay; discharge destination; mortality at 26 weeks; mortality or institutionalization; activ-
ities of daily living index; anxiety and depression; quality of life
Notes
Allocation concealment A – Adequate
Study Weinberger
Methods RCT
Participants Patients with diabetes mellitus, heart failure, chronic obstructive pulmonary disease
average age
T=63.0
C=62.6
Number recruited:
T=695
C=701
Interventions Discharge planning: nurse and primary care physician at each site - assessment, planning, implementation,
monitoring
Setting: 9 V A hospitals
Outcomes Re admission to hospital, health status, patient satisfaction, intensity of primary care
Notes Discharge planning within 3 days of discharge.
9 VA hospitals participated in the trial.
Discharge planning within 3 days of discharge
Allocation concealment A – Adequate
Characteristics of excluded studies
Study Reason for exclusion
Applegate RCT: discharge planning plus geriatric assessment unit
Brooten Discharge planning plus home care package
Brooten D Discharge planning plus home care package plus counselling
Carty Early post partum hospital discharge
Casiro Intervention: DP plus home care package
Choong
Intervention: clinical pathway for patients with a fractured neck of femur, discharge planning is not described
Donahue Intervention discharge planning plus post discharge care package
Dudas
15Discharge planning from hospital to home (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd
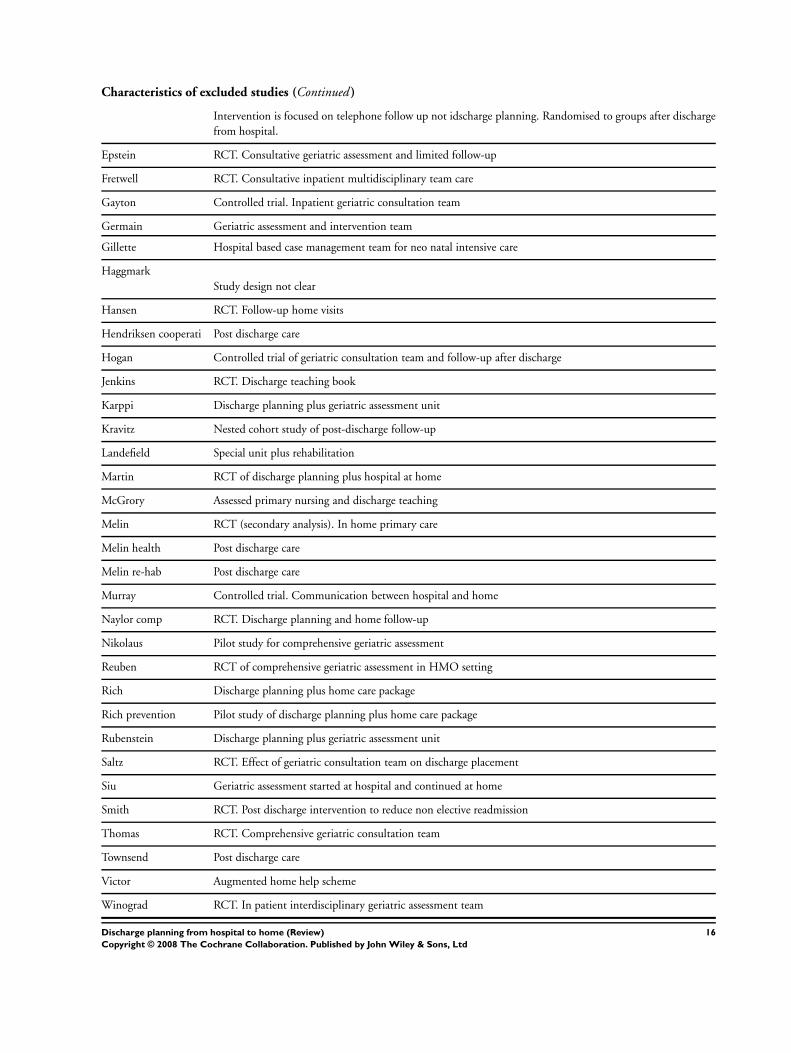
Characteristics of excluded studies (Continued )
Intervention is focused on telephone follow up not idscharge planning. Randomised to groups after discharge
from hospital.
Epstein RCT. Consultative geriatric assessment and limited follow-up
Fretwell RCT. Consultative inpatient multidisciplinary team care
Gayton Controlled trial. Inpatient geriatric consultation team
Germain Geriatric assessment and intervention team
Gillette Hospital based case management team for neo natal intensive care
Haggmark
Study design not clear
Hansen RCT. Follow-up home visits
Hendriksen cooperati Post discharge care
Hogan Controlled trial of geriatric consultation team and follow-up after discharge
Jenkins RCT. Discharge teaching book
Karppi Discharge planning plus geriatric assessment unit
Kravitz Nested cohort study of post-discharge follow-up
Landefield Special unit plus rehabilitation
Martin RCT of discharge planning plus hospital at home
McGrory Assessed primary nursing and discharge teaching
Melin RCT (secondary analysis). In home primary care
Melin health Post discharge care
Melin re-hab Post discharge care
Murray Controlled trial. Communication between hospital and home
Naylor comp RCT. Discharge planning and home follow-up
Nikolaus Pilot study for comprehensive geriatric assessment
Reuben RCT of comprehensive geriatric assessment in HMO setting
Rich Discharge planning plus home care package
Rich prevention Pilot study of discharge planning plus home care package
Rubenstein Discharge planning plus geriatric assessment unit
Saltz RCT. Effect of geriatric consultation team on discharge placement
Siu Geriatric assessment started at hospital and continued at home
Smith RCT. Post discharge intervention to reduce non elective readmission
Thomas RCT. Comprehensive geriatric consultation team
Townsend Post discharge care
Victor Augmented home help scheme
Winograd RCT. In patient interdisciplinary geriatric assessment team
16Discharge planning from hospital to home (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd
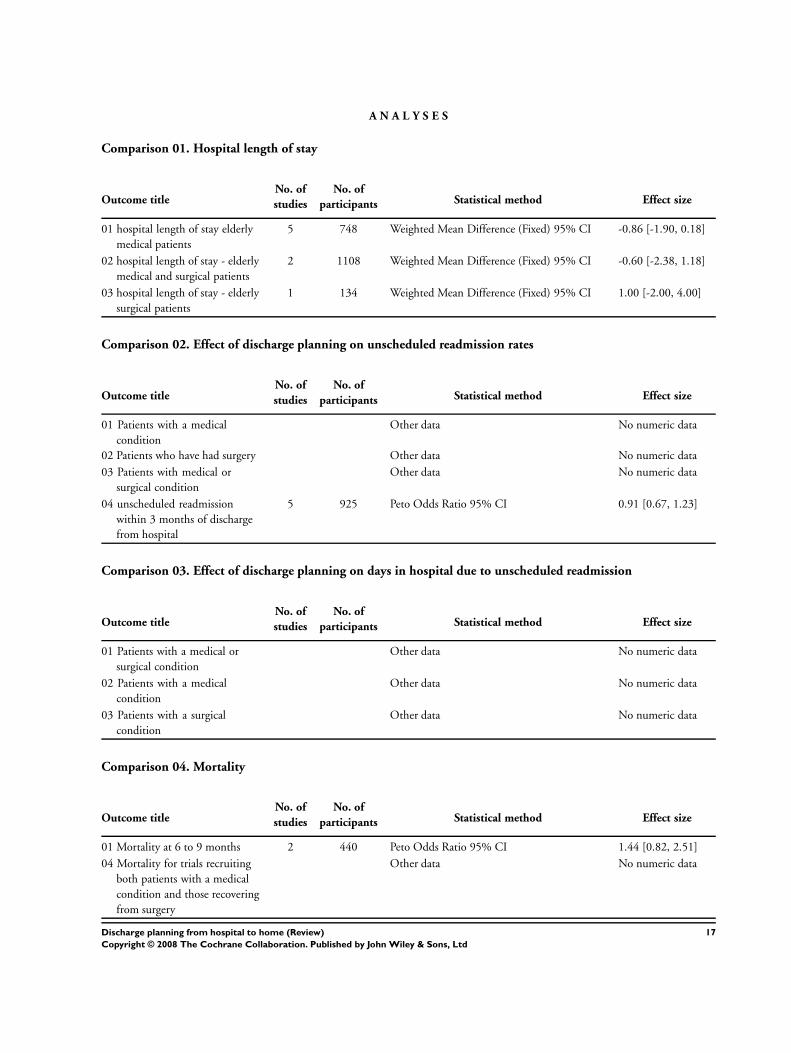
A N A L Y S E S
Comparison 01. Hospital length of stay
Outcome titleNo. of
studies
No. of
participants Statistical method Effect size
01 hospital length of stay elderly
medical patients
5 748 Weighted Mean Difference (Fixed) 95% CI -0.86 [-1.90, 0.18]
02 hospital length of stay - elderly
medical and surgical patients
2 1108 Weighted Mean Difference (Fixed) 95% CI -0.60 [-2.38, 1.18]
03 hospital length of stay - elderly
surgical patients
1 134 Weighted Mean Difference (Fixed) 95% CI 1.00 [-2.00, 4.00]
Comparison 02. Effect of discharge planning on unscheduled readmission rates
Outcome titleNo. of
studies
No. of
participants Statistical method Effect size
01 Patients with a medical
condition
Other data No numeric data
02 Patients who have had surgery Other data No numeric data
03 Patients with medical or
surgical condition
Other data No numeric data
04 unscheduled readmission
within 3 months of discharge
from hospital
5 925 Peto Odds Ratio 95% CI 0.91 [0.67, 1.23]
Comparison 03. Effect of discharge planning on days in hospital due to unscheduled readmission
Outcome titleNo. of
studies
No. of
participants Statistical method Effect size
01 Patients with a medical or
surgical condition
Other data No numeric data
02 Patients with a medical
condition
Other data No numeric data
03 Patients with a surgical
condition
Other data No numeric data
Comparison 04. Mortality
Outcome titleNo. of
studies
No. of
participants Statistical method Effect size
01 Mortality at 6 to 9 months 2 440 Peto Odds Ratio 95% CI 1.44 [0.82, 2.51]
04 Mortality for trials recruiting
both patients with a medical
condition and those recovering
from surgery
Other data No numeric data
17Discharge planning from hospital to home (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd
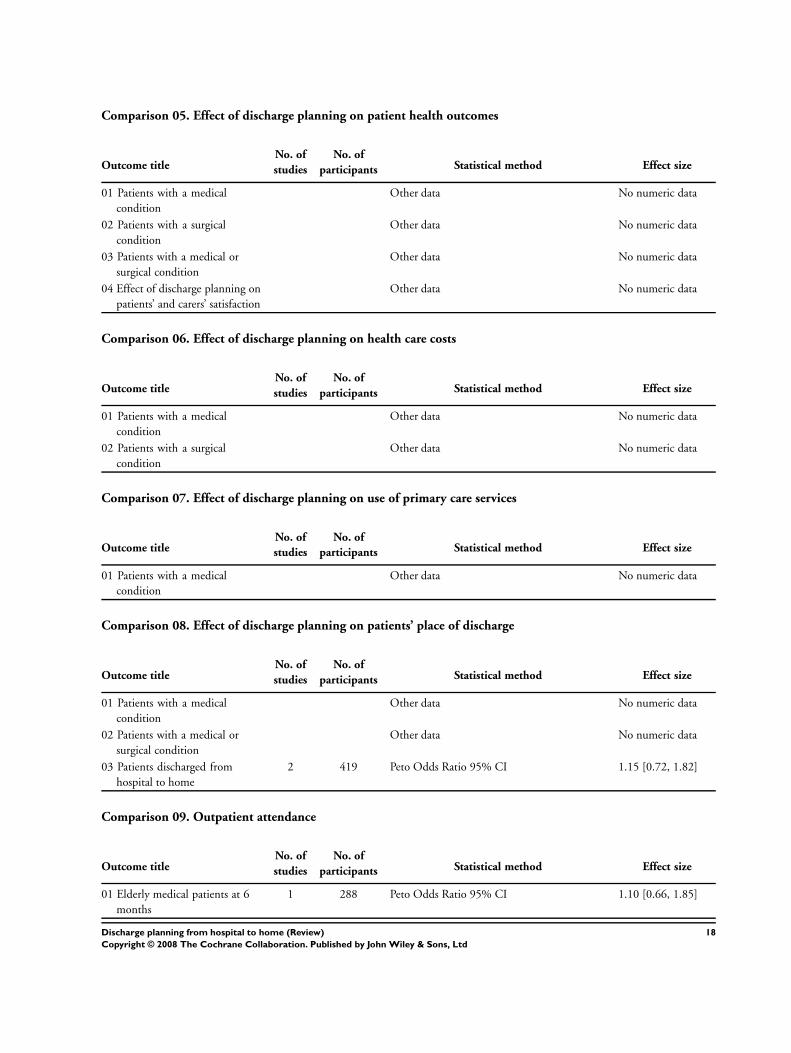
Comparison 05. Effect of discharge planning on patient health outcomes
Outcome titleNo. of
studies
No. of
participants Statistical method Effect size
01 Patients with a medical
condition
Other data No numeric data
02 Patients with a surgical
condition
Other data No numeric data
03 Patients with a medical or
surgical condition
Other data No numeric data
04 Effect of discharge planning on
patients’ and carers’ satisfaction
Other data No numeric data
Comparison 06. Effect of discharge planning on health care costs
Outcome titleNo. of
studies
No. of
participants Statistical method Effect size
01 Patients with a medical
condition
Other data No numeric data
02 Patients with a surgical
condition
Other data No numeric data
Comparison 07. Effect of discharge planning on use of primary care services
Outcome titleNo. of
studies
No. of
participants Statistical method Effect size
01 Patients with a medical
condition
Other data No numeric data
Comparison 08. Effect of discharge planning on patients’ place of discharge
Outcome titleNo. of
studies
No. of
participants Statistical method Effect size
01 Patients with a medical
condition
Other data No numeric data
02 Patients with a medical or
surgical condition
Other data No numeric data
03 Patients discharged from
hospital to home
2 419 Peto Odds Ratio 95% CI 1.15 [0.72, 1.82]
Comparison 09. Outpatient attendance
Outcome titleNo. of
studies
No. of
participants Statistical method Effect size
01 Elderly medical patients at 6
months
1 288 Peto Odds Ratio 95% CI 1.10 [0.66, 1.85]
18Discharge planning from hospital to home (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Comparison 10. Medication
Outcome titleNo. of
studies
No. of
participants Statistical method Effect size
01 Medication problems after
being discharged from hospital
Other data No numeric data
02 Adherence to medicines Other data No numeric data
03 Knowledge about medicines Other data No numeric data
04 Hoarding of medicines Other data No numeric data
I N D E X T E R M S
Medical Subject Headings (MeSH)
Controlled Clinical Trials as Topic; Health Care Costs; Length of Stay; Outcome Assessment (Health Care); ∗Patient Discharge; Patient
Readmission; Randomized Controlled Trials as Topic
MeSH check words
Humans
C O V E R S H E E T
Title Discharge planning from hospital to home
Authors Shepperd S, Parkes J, McClaran J, Phillips C
Contribution of author(s) Sasha Shepperd (SS) co authored the protocol for the review with JP, obtained funding for
the review, helped JP develop the search strategy, scan abstracts, and data extraction. SS
took the lead in writing the review, did the data analysis, constructed the results tables, and
responded to refereess comments. SS updated the review.
Julie Parkes (JP) co authored the protocol, performed the electronic and non-electronic
searches, retrieved relevant articles and did the initial sifting of these articles using the
exclusion and inclusion criteria to produce the included studies for the review, assisted
with data extraction, contacted authors of the included studies and relevant experts, and
produced the first draft of the review.
Jacqueline McClaren assisted with data extraction for the update of the review, interpretation
of the studies and commented on drafts of the update.
Chris Phillips assisted with the identification of studies for the update of the review and
commented on a draft of the update.
Diana Harwood (DH) assisted with scanning abstracts retrieved from electronic searches.
Issue protocol first published /
Review first published 2000/4
Date of most recent amendment 02 March 2004
Date of most recent
SUBSTANTIVE amendment
25 September 2003
What’s New Three studies were included in the update, taking the total number of trials included in the
review to 11. The inclusion of these three trials has had little effect on the overall results of
the review. The impact of discharge planning on readmission rates, hospital length of stay,
health outcomes (including mortality) and cost remains uncertain. This reflects a lack of
power as the degree to which we could pool data was restricted by the different reported
measures of outcome. However, it is possible that even a small reduction in length of stay,
19Discharge planning from hospital to home (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd
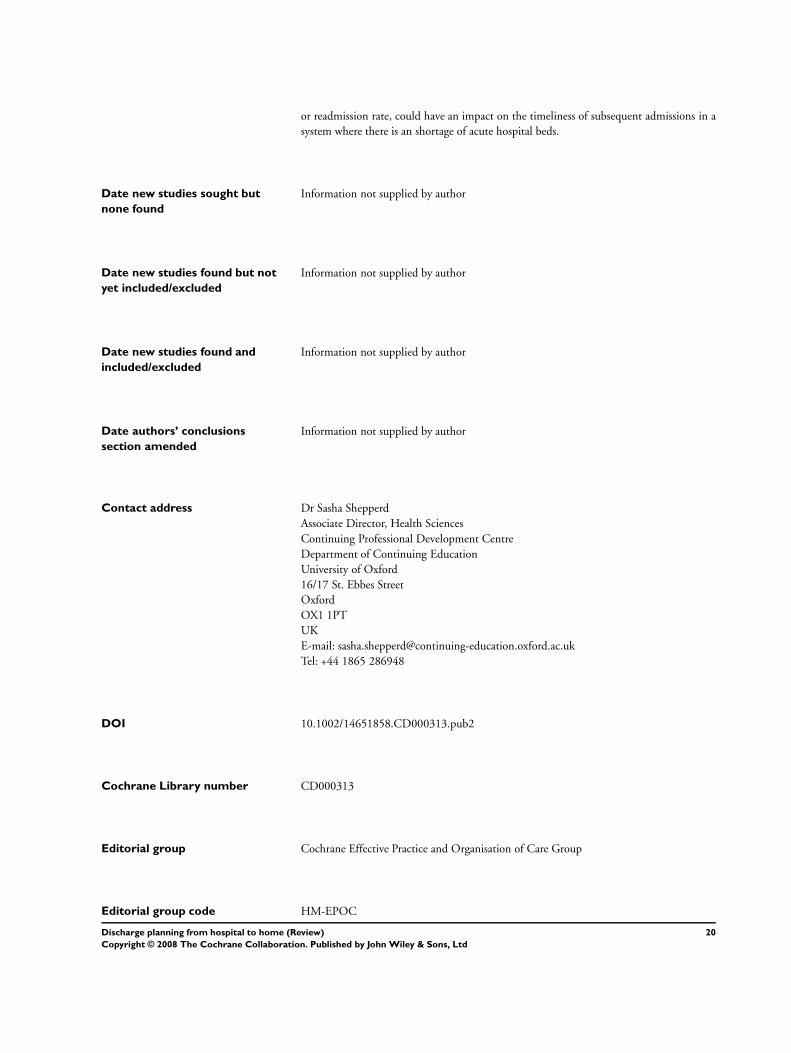
or readmission rate, could have an impact on the timeliness of subsequent admissions in a
system where there is an shortage of acute hospital beds.
Date new studies sought but
none found
Information not supplied by author
Date new studies found but not
yet included/excluded
Information not supplied by author
Date new studies found and
included/excluded
Information not supplied by author
Date authors’ conclusions
section amended
Information not supplied by author
Contact address Dr Sasha Shepperd
Associate Director, Health Sciences
Continuing Professional Development Centre
Department of Continuing Education
University of Oxford
16/17 St. Ebbes Street
Oxford
OX1 1PT
UK
E-mail: [email protected]
Tel: +44 1865 286948
DOI 10.1002/14651858.CD000313.pub2
Cochrane Library number CD000313
Editorial group Cochrane Effective Practice and Organisation of Care Group
Editorial group code HM-EPOC
20Discharge planning from hospital to home (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

G R A P H S A N D O T H E R T A B L E S
Analysis 01.01. Comparison 01 Hospital length of stay, Outcome 01 hospital length of stay elderly medical
patients
Review: Discharge planning from hospital to home
Comparison: 01 Hospital length of stay
Outcome: 01 hospital length of stay elderly medical patients
Study discharge planning control Weighted Mean Difference (Fixed) Weight Weighted Mean Difference (Fixed)
N Mean(SD) N Mean(SD) 95% CI (%) 95% CI
Kennedy 39 7.80 (0.0) 41 9.70 (0.0) 0.0 Not estimable
Moher 136 7.43 (6.33) 131 9.40 (8.97) 31.1 -1.97 [ -3.84, -0.10 ]
Naughton 51 5.40 (5.50) 60 7.00 (7.00) 20.1 -1.60 [ -3.93, 0.73 ]
Naylor 72 7.40 (3.80) 66 7.50 (5.20) 46.4 -0.10 [ -1.63, 1.43 ]
Sulch 76 50.00 (19.00) 76 45.00 (23.00) 2.4 5.00 [ -1.71, 11.71 ]
Total (95% CI) 374 374 100.0 -0.86 [ -1.90, 0.18 ]
Test for heterogeneity chi-square=5.62 df=3 p=0.13 I2 =46.6%
Test for overall effect z=1.62 p=0.1
-10 -5 0 5 10
Favours treatment Favours control
Analysis 01.02. Comparison 01 Hospital length of stay, Outcome 02 hospital length of stay - elderly medical
and surgical patients
Review: Discharge planning from hospital to home
Comparison: 01 Hospital length of stay
Outcome: 02 hospital length of stay - elderly medical and surgical patients
Study discharge planning Control Weighted Mean Difference (Fixed) Weight Weighted Mean Difference (Fixed)
N Mean(SD) N Mean(SD) 95% CI (%) 95% CI
Evans 417 11.90 (12.70) 418 12.50 (13.50) 100.0 -0.60 [ -2.38, 1.18 ]
Hendriksen 135 11.00 (0.0) 138 14.30 (0.0) 0.0 Not estimable
Total (95% CI) 552 556 100.0 -0.60 [ -2.38, 1.18 ]
Test for heterogeneity: not applicable
Test for overall effect z=0.66 p=0.5
-10 -5 0 5 10
Favours treatment Favours control
21Discharge planning from hospital to home (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd
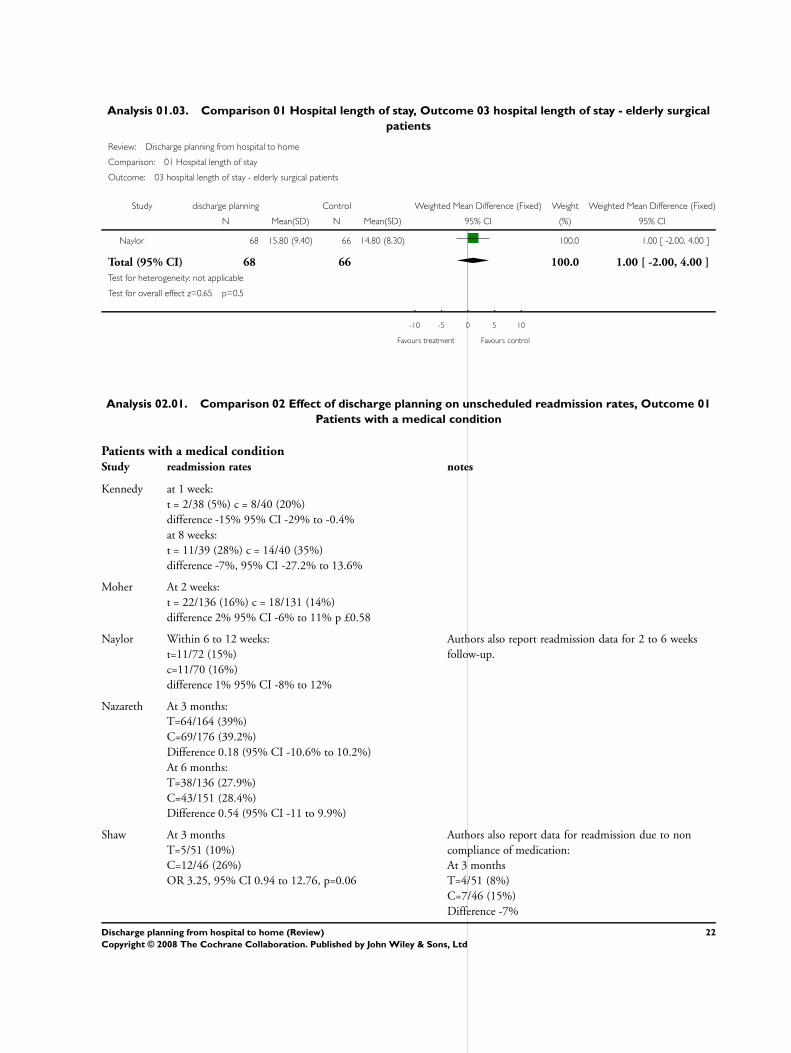
Analysis 01.03. Comparison 01 Hospital length of stay, Outcome 03 hospital length of stay - elderly surgical
patients
Review: Discharge planning from hospital to home
Comparison: 01 Hospital length of stay
Outcome: 03 hospital length of stay - elderly surgical patients
Study discharge planning Control Weighted Mean Difference (Fixed) Weight Weighted Mean Difference (Fixed)
N Mean(SD) N Mean(SD) 95% CI (%) 95% CI
Naylor 68 15.80 (9.40) 66 14.80 (8.30) 100.0 1.00 [ -2.00, 4.00 ]
Total (95% CI) 68 66 100.0 1.00 [ -2.00, 4.00 ]
Test for heterogeneity: not applicable
Test for overall effect z=0.65 p=0.5
-10 -5 0 5 10
Favours treatment Favours control
Analysis 02.01. Comparison 02 Effect of discharge planning on unscheduled readmission rates, Outcome 01
Patients with a medical condition
Patients with a medical conditionStudy readmission rates notes
Kennedy at 1 week:
t = 2/38 (5%) c = 8/40 (20%)
difference -15% 95% CI -29% to -0.4%
at 8 weeks:
t = 11/39 (28%) c = 14/40 (35%)
difference -7%, 95% CI -27.2% to 13.6%
Moher At 2 weeks:
t = 22/136 (16%) c = 18/131 (14%)
difference 2% 95% CI -6% to 11% p £0.58
Naylor Within 6 to 12 weeks:
t=11/72 (15%)
c=11/70 (16%)
difference 1% 95% CI -8% to 12%
Authors also report readmission data for 2 to 6 weeks
follow-up.
Nazareth At 3 months:
T=64/164 (39%)
C=69/176 (39.2%)
Difference 0.18 (95% CI -10.6% to 10.2%)
At 6 months:
T=38/136 (27.9%)
C=43/151 (28.4%)
Difference 0.54 (95% CI -11 to 9.9%)
Shaw At 3 months
T=5/51 (10%)
C=12/46 (26%)
OR 3.25, 95% CI 0.94 to 12.76, p=0.06
Authors also report data for readmission due to non
compliance of medication:
At 3 months
T=4/51 (8%)
C=7/46 (15%)
Difference -7%
22Discharge planning from hospital to home (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd
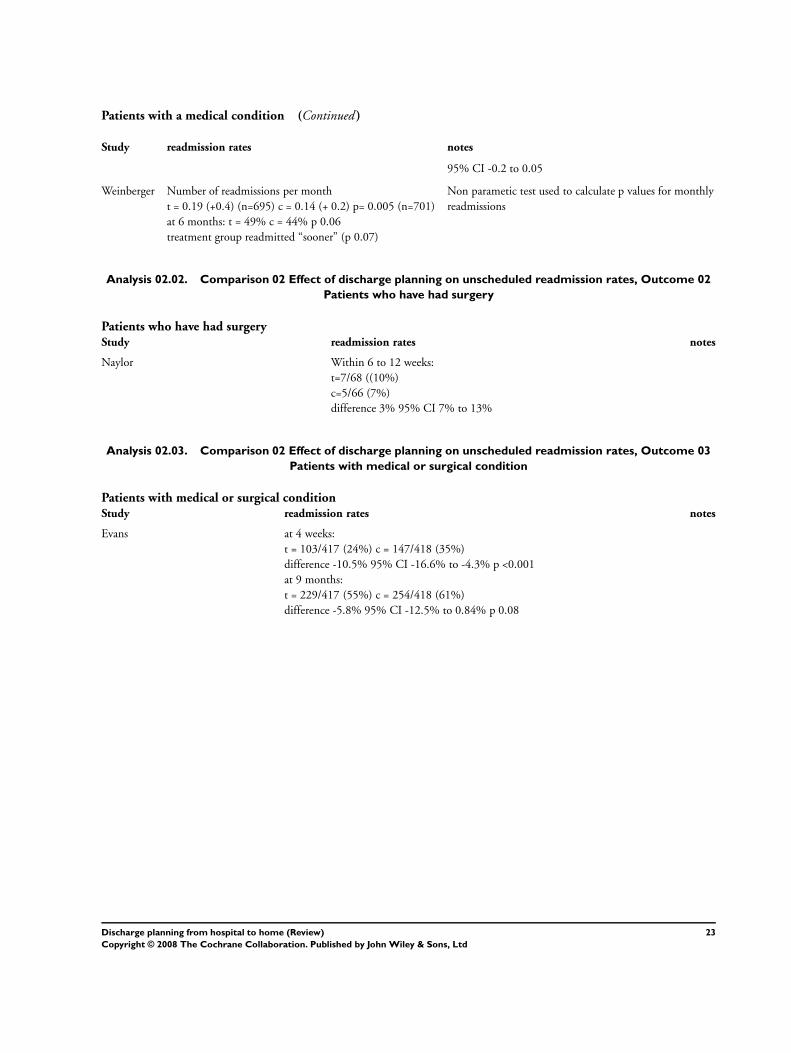
Patients with a medical condition (Continued )
Study readmission rates notes
95% CI -0.2 to 0.05
Weinberger Number of readmissions per month
t = 0.19 (+0.4) (n=695) c = 0.14 (+ 0.2) p= 0.005 (n=701)
at 6 months: t = 49% c = 44% p 0.06
treatment group readmitted “sooner” (p 0.07)
Non parametic test used to calculate p values for monthly
readmissions
Analysis 02.02. Comparison 02 Effect of discharge planning on unscheduled readmission rates, Outcome 02
Patients who have had surgery
Patients who have had surgeryStudy readmission rates notes
Naylor Within 6 to 12 weeks:
t=7/68 ((10%)
c=5/66 (7%)
difference 3% 95% CI 7% to 13%
Analysis 02.03. Comparison 02 Effect of discharge planning on unscheduled readmission rates, Outcome 03
Patients with medical or surgical condition
Patients with medical or surgical conditionStudy readmission rates notes
Evans at 4 weeks:
t = 103/417 (24%) c = 147/418 (35%)
difference -10.5% 95% CI -16.6% to -4.3% p <0.001
at 9 months:
t = 229/417 (55%) c = 254/418 (61%)
difference -5.8% 95% CI -12.5% to 0.84% p 0.08
23Discharge planning from hospital to home (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd
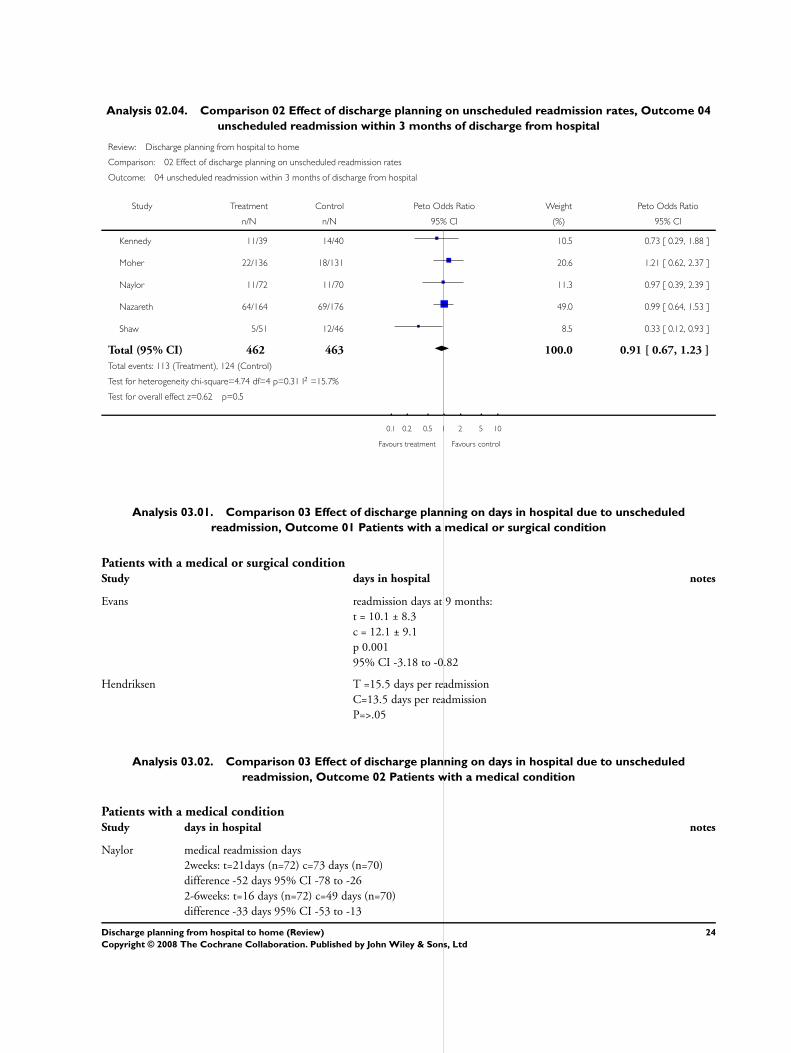
Analysis 02.04. Comparison 02 Effect of discharge planning on unscheduled readmission rates, Outcome 04
unscheduled readmission within 3 months of discharge from hospital
Review: Discharge planning from hospital to home
Comparison: 02 Effect of discharge planning on unscheduled readmission rates
Outcome: 04 unscheduled readmission within 3 months of discharge from hospital
Study Treatment Control Peto Odds Ratio Weight Peto Odds Ratio
n/N n/N 95% CI (%) 95% CI
Kennedy 11/39 14/40 10.5 0.73 [ 0.29, 1.88 ]
Moher 22/136 18/131 20.6 1.21 [ 0.62, 2.37 ]
Naylor 11/72 11/70 11.3 0.97 [ 0.39, 2.39 ]
Nazareth 64/164 69/176 49.0 0.99 [ 0.64, 1.53 ]
Shaw 5/51 12/46 8.5 0.33 [ 0.12, 0.93 ]
Total (95% CI) 462 463 100.0 0.91 [ 0.67, 1.23 ]
Total events: 113 (Treatment), 124 (Control)
Test for heterogeneity chi-square=4.74 df=4 p=0.31 I2 =15.7%
Test for overall effect z=0.62 p=0.5
0.1 0.2 0.5 1 2 5 10
Favours treatment Favours control
Analysis 03.01. Comparison 03 Effect of discharge planning on days in hospital due to unscheduled
readmission, Outcome 01 Patients with a medical or surgical condition
Patients with a medical or surgical conditionStudy days in hospital notes
Evans readmission days at 9 months:
t = 10.1 ± 8.3
c = 12.1 ± 9.1
p 0.001
95% CI -3.18 to -0.82
Hendriksen T =15.5 days per readmission
C=13.5 days per readmission
P=>.05
Analysis 03.02. Comparison 03 Effect of discharge planning on days in hospital due to unscheduled
readmission, Outcome 02 Patients with a medical condition
Patients with a medical conditionStudy days in hospital notes
Naylor medical readmission days
2weeks: t=21days (n=72) c=73 days (n=70)
difference -52 days 95% CI -78 to -26
2-6weeks: t=16 days (n=72) c=49 days (n=70)
difference -33 days 95% CI -53 to -13
24Discharge planning from hospital to home (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Patients with a medical condition (Continued )
Study days in hospital notes
6-12 weeks: t=94 days (n=72) c=100 days (n=70)
difference -6 days 95% CI -83 to 71
Weinberger medical readmission days at 6 months follow up: t=10.2 (19.8) c=8.8 (19.7) difference 1.4 days p<0.04
Analysis 03.03. Comparison 03 Effect of discharge planning on days in hospital due to unscheduled
readmission, Outcome 03 Patients with a surgical condition
Patients with a surgical conditionStudy days in hospital notes
Naylor surgical readmission days
2 weeks: t=34 days (n=68) c=32 days (n=66)
difference 2 days 95% CI -13 to 17
2-6 weeks: t=63 (n=68) c=52 (n=66)
difference 11 days 95% CI -20 to 52
6-12 weeks: t=52 (n=68) c=26 (n=66) difference 26 days 95% CI -8 to 60
Analysis 04.01. Comparison 04 Mortality, Outcome 01 Mortality at 6 to 9 months
Review: Discharge planning from hospital to home
Comparison: 04 Mortality
Outcome: 01 Mortality at 6 to 9 months
Study Treatment Control Peto Odds Ratio Weight Peto Odds Ratio
n/N n/N 95% CI (%) 95% CI
Nazareth 22/137 19/151 71.0 1.33 [ 0.69, 2.57 ]
Sulch 10/76 6/76 29.0 1.74 [ 0.62, 4.89 ]
Total (95% CI) 213 227 100.0 1.44 [ 0.82, 2.51 ]
Total events: 32 (Treatment), 25 (Control)
Test for heterogeneity chi-square=0.19 df=1 p=0.66 I2 =0.0%
Test for overall effect z=1.28 p=0.2
0.001 0.01 0.1 1 10 100 1000
Favours treatment Favours control
Analysis 04.04. Comparison 04 Mortality, Outcome 04 Mortality for trials recruiting both patients with a
medical condition and those recovering from surgery
Mortality for trials recruiting both patients with a medical condition and those recovering from surgeryStudy Mortality @ 9 months notes
Evans t=66/417 (16%)
c=67/418 (16%)
25Discharge planning from hospital to home (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Analysis 05.01. Comparison 05 Effect of discharge planning on patient health outcomes, Outcome 01
Patients with a medical condition
26Discharge planning from hospital to home (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Patients with a medical conditionStudy pt health outcomes notes
Kennedy Long Term Care Information System (LTCIS)
Health and functional status
(also measures services required)
No data reported
Naylor Data aggregated for both groups. Mean Enforced Social Dependency Scale
increased from 19.6 to 26.3 p<0.01
No data reported for each group. Decline in functional status reported for all
patients.
Functional status. Scale measured:
Mental status
Perception of health
Self esteem
Affect
Nazareth General well being questionnaire 1=ill health
5=good health
At 3 months:
T=76, mean 2.4 (SD 0.7)
C=73 mean 2.4 (SD 0.6)
At 6 months
T=62, mean 2.5 (SD 0.6)
C=61 mean 2.4 (SD 0.7)
Mean difference 0.1 (95% CI -0.14 to 0.34)
Sulch Barthel activities of daily living
Median scores
At 4 weeks
T=13
C=11
At 12 weeks
T=15
C=17
At 26 weeks
T=17
C=17
median change from 4 to 12 weeks
P<0.01
Rankin score
Median score
At 4 weeks
T=1
27
Disc
harg
ep
lan
nin
gfro
mh
osp
italto
ho
me
(Revie
w)
Co
pyrig
ht
©2008
Th
eC
och
ran
eC
olla
bo
ratio
n.P
ub
lished
by
Joh
nW
iley
&S
on
s,L
td

Patients with a medical condition (Continued )
Study pt health outcomes notes
C=1
At 12 weeks
T=3
C=3
At 26 weeks
T=3
C=3
Hospital anxiety and depression scale
Anxiety:
Median scores
At 4 weeks
T=5
C=5
At 12 weeks
T=4
C=4
At 26 weeks
T=4
C=4
Depression
Median scores
At 4 weeks
T=6
C=5
At 12 weeks
T=5
C=5
At 26 weeks
T=5
C=5
Euroqol
At 4 weeks
T=41
C=44
Median scores
At 4 weeks
28
Disc
harg
ep
lan
nin
gfro
mh
osp
italto
ho
me
(Revie
w)
Co
pyrig
ht
©2008
Th
eC
och
ran
eC
olla
bo
ratio
n.P
ub
lished
by
Joh
nW
iley
&S
on
s,L
td

Patients with a medical condition (Continued )
Study pt health outcomes notes
T=41
C=44
P=0.1
At 12 weeks
T=59
C=65
P=0.07
At 26 weeks
T=63
C=72
P<0.005
Weinberger at 1 month: no significant differences
p 0.99
at 3 months: no significant differences
p 0.53
SF 36
No data shown
29
Disc
harg
ep
lan
nin
gfro
mh
osp
italto
ho
me
(Revie
w)
Co
pyrig
ht
©2008
Th
eC
och
ran
eC
olla
bo
ratio
n.P
ub
lished
by
Joh
nW
iley
&S
on
s,L
td
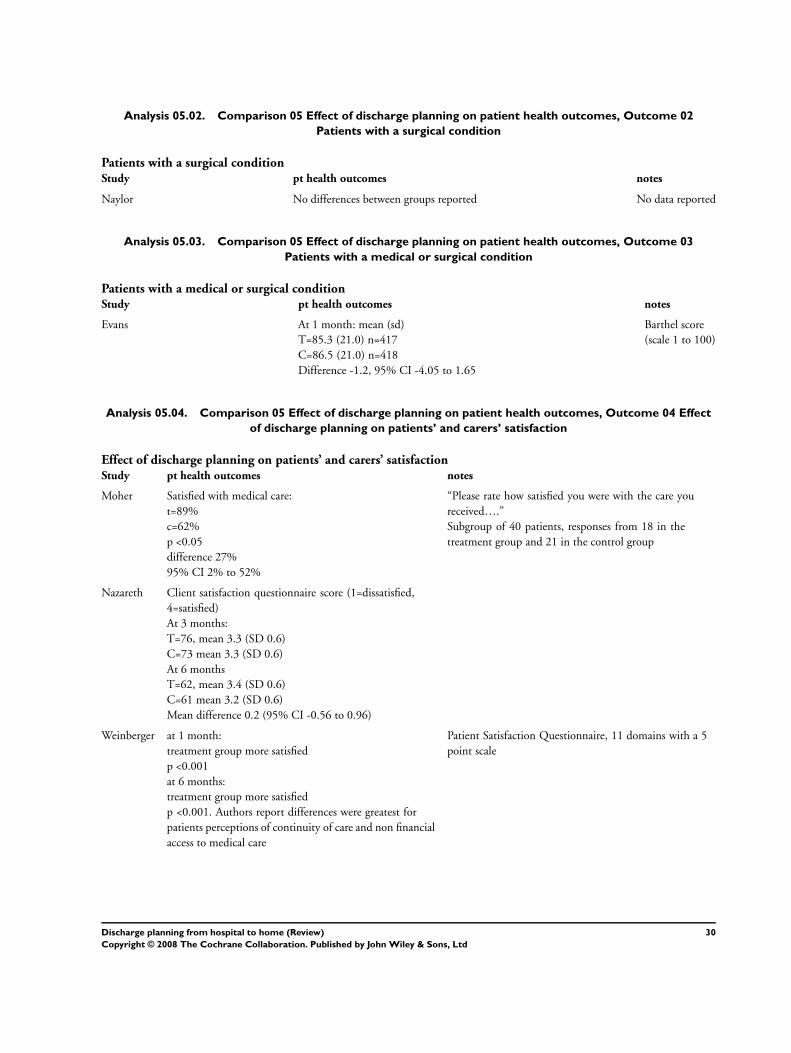
Analysis 05.02. Comparison 05 Effect of discharge planning on patient health outcomes, Outcome 02
Patients with a surgical condition
Patients with a surgical conditionStudy pt health outcomes notes
Naylor No differences between groups reported No data reported
Analysis 05.03. Comparison 05 Effect of discharge planning on patient health outcomes, Outcome 03
Patients with a medical or surgical condition
Patients with a medical or surgical conditionStudy pt health outcomes notes
Evans At 1 month: mean (sd)
T=85.3 (21.0) n=417
C=86.5 (21.0) n=418
Difference -1.2, 95% CI -4.05 to 1.65
Barthel score
(scale 1 to 100)
Analysis 05.04. Comparison 05 Effect of discharge planning on patient health outcomes, Outcome 04 Effect
of discharge planning on patients’ and carers’ satisfaction
Effect of discharge planning on patients’ and carers’ satisfactionStudy pt health outcomes notes
Moher Satisfied with medical care:
t=89%
c=62%
p <0.05
difference 27%
95% CI 2% to 52%
“Please rate how satisfied you were with the care you
received….”
Subgroup of 40 patients, responses from 18 in the
treatment group and 21 in the control group
Nazareth Client satisfaction questionnaire score (1=dissatisfied,
4=satisfied)
At 3 months:
T=76, mean 3.3 (SD 0.6)
C=73 mean 3.3 (SD 0.6)
At 6 months
T=62, mean 3.4 (SD 0.6)
C=61 mean 3.2 (SD 0.6)
Mean difference 0.2 (95% CI -0.56 to 0.96)
Weinberger at 1 month:
treatment group more satisfied
p <0.001
at 6 months:
treatment group more satisfied
p <0.001. Authors report differences were greatest for
patients perceptions of continuity of care and non financial
access to medical care
Patient Satisfaction Questionnaire, 11 domains with a 5
point scale
30Discharge planning from hospital to home (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd
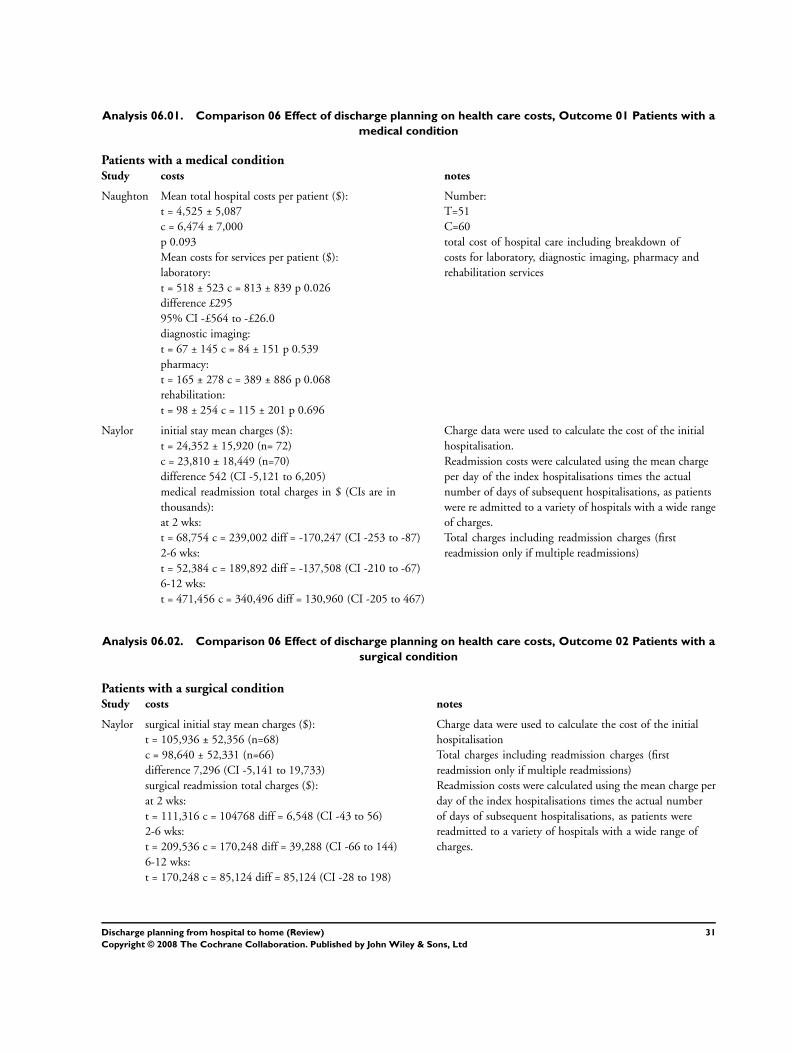
Analysis 06.01. Comparison 06 Effect of discharge planning on health care costs, Outcome 01 Patients with a
medical condition
Patients with a medical conditionStudy costs notes
Naughton Mean total hospital costs per patient ($):
t = 4,525 ± 5,087
c = 6,474 ± 7,000
p 0.093
Mean costs for services per patient ($):
laboratory:
t = 518 ± 523 c = 813 ± 839 p 0.026
difference £295
95% CI -£564 to -£26.0
diagnostic imaging:
t = 67 ± 145 c = 84 ± 151 p 0.539
pharmacy:
t = 165 ± 278 c = 389 ± 886 p 0.068
rehabilitation:
t = 98 ± 254 c = 115 ± 201 p 0.696
Number:
T=51
C=60
total cost of hospital care including breakdown of
costs for laboratory, diagnostic imaging, pharmacy and
rehabilitation services
Naylor initial stay mean charges ($):
t = 24,352 ± 15,920 (n= 72)
c = 23,810 ± 18,449 (n=70)
difference 542 (CI -5,121 to 6,205)
medical readmission total charges in $ (CIs are in
thousands):
at 2 wks:
t = 68,754 c = 239,002 diff = -170,247 (CI -253 to -87)
2-6 wks:
t = 52,384 c = 189,892 diff = -137,508 (CI -210 to -67)
6-12 wks:
t = 471,456 c = 340,496 diff = 130,960 (CI -205 to 467)
Charge data were used to calculate the cost of the initial
hospitalisation.
Readmission costs were calculated using the mean charge
per day of the index hospitalisations times the actual
number of days of subsequent hospitalisations, as patients
were re admitted to a variety of hospitals with a wide range
of charges.
Total charges including readmission charges (first
readmission only if multiple readmissions)
Analysis 06.02. Comparison 06 Effect of discharge planning on health care costs, Outcome 02 Patients with a
surgical condition
Patients with a surgical conditionStudy costs notes
Naylor surgical initial stay mean charges ($):
t = 105,936 ± 52,356 (n=68)
c = 98,640 ± 52,331 (n=66)
difference 7,296 (CI -5,141 to 19,733)
surgical readmission total charges ($):
at 2 wks:
t = 111,316 c = 104768 diff = 6,548 (CI -43 to 56)
2-6 wks:
t = 209,536 c = 170,248 diff = 39,288 (CI -66 to 144)
6-12 wks:
t = 170,248 c = 85,124 diff = 85,124 (CI -28 to 198)
Charge data were used to calculate the cost of the initial
hospitalisation
Total charges including readmission charges (first
readmission only if multiple readmissions)
Readmission costs were calculated using the mean charge per
day of the index hospitalisations times the actual number
of days of subsequent hospitalisations, as patients were
readmitted to a variety of hospitals with a wide range of
charges.
31Discharge planning from hospital to home (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd
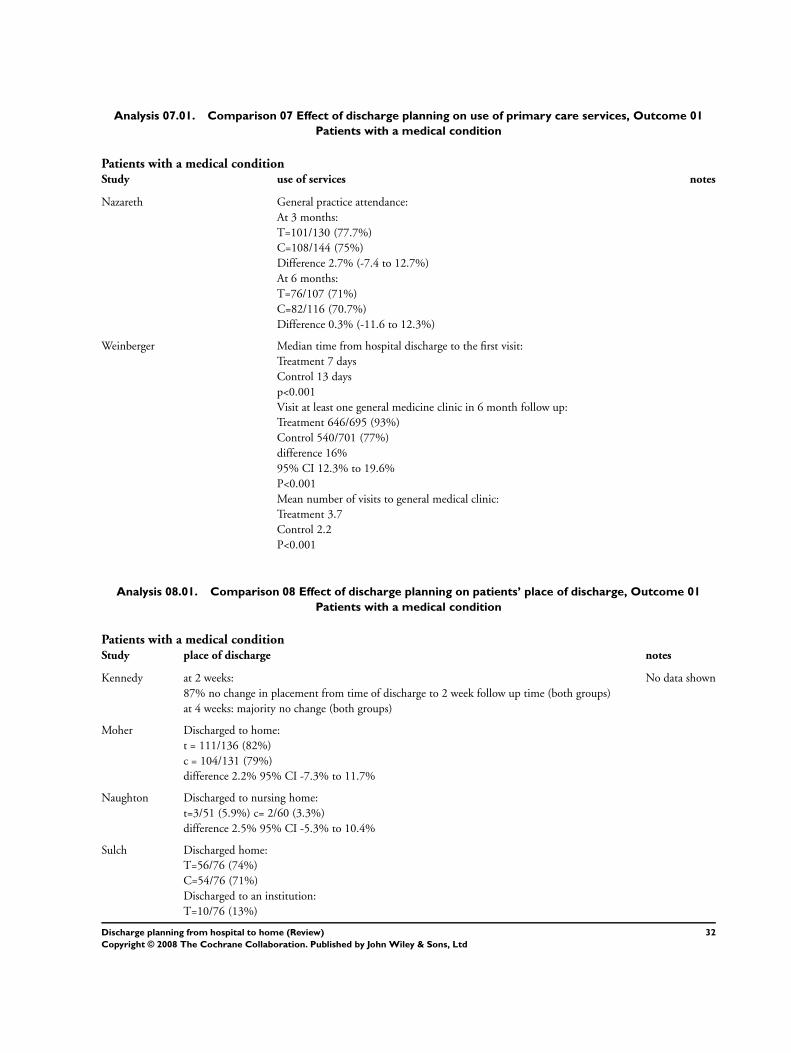
Analysis 07.01. Comparison 07 Effect of discharge planning on use of primary care services, Outcome 01
Patients with a medical condition
Patients with a medical conditionStudy use of services notes
Nazareth General practice attendance:
At 3 months:
T=101/130 (77.7%)
C=108/144 (75%)
Difference 2.7% (-7.4 to 12.7%)
At 6 months:
T=76/107 (71%)
C=82/116 (70.7%)
Difference 0.3% (-11.6 to 12.3%)
Weinberger Median time from hospital discharge to the first visit:
Treatment 7 days
Control 13 days
p<0.001
Visit at least one general medicine clinic in 6 month follow up:
Treatment 646/695 (93%)
Control 540/701 (77%)
difference 16%
95% CI 12.3% to 19.6%
P<0.001
Mean number of visits to general medical clinic:
Treatment 3.7
Control 2.2
P<0.001
Analysis 08.01. Comparison 08 Effect of discharge planning on patients’ place of discharge, Outcome 01
Patients with a medical condition
Patients with a medical conditionStudy place of discharge notes
Kennedy at 2 weeks:
87% no change in placement from time of discharge to 2 week follow up time (both groups)
at 4 weeks: majority no change (both groups)
No data shown
Moher Discharged to home:
t = 111/136 (82%)
c = 104/131 (79%)
difference 2.2% 95% CI -7.3% to 11.7%
Naughton Discharged to nursing home:
t=3/51 (5.9%) c= 2/60 (3.3%)
difference 2.5% 95% CI -5.3% to 10.4%
Sulch Discharged home:
T=56/76 (74%)
C=54/76 (71%)
Discharged to an institution:
T=10/76 (13%)
32Discharge planning from hospital to home (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Patients with a medical condition (Continued )
Study place of discharge notes
C=16/76 (21%)
OR 1.5 95% CI 0.5 to 2.8
Analysis 08.02. Comparison 08 Effect of discharge planning on patients’ place of discharge, Outcome 02
Patients with a medical or surgical condition
Patients with a medical or surgical conditionStudy place of discharge notes
Evans Discharged to home:
t = 330/417 (79%)
c = 305/418 (73%)
p 0.05 difference 6% 95% CI 0.39% to 12%
home at 9 months:
t = 259/417 (62%)
c = 225/418 (54%)
p 0.05 difference 8.3% 95% CI 1.6% to 15%
Hendriksen Discharged to nursing home:
t=0/135 (0%) c=3/138 (2%)
Difference -2% 95% CI -4.6% to 0.26%
At 6 months: admitted to another institution
t=3/135 (2%) c=14/138 (10%)
difference -8% 95% CI -13.5% to -2.3%
Analysis 08.03. Comparison 08 Effect of discharge planning on patients’ place of discharge, Outcome 03
Patients discharged from hospital to home
Review: Discharge planning from hospital to home
Comparison: 08 Effect of discharge planning on patients’ place of discharge
Outcome: 03 Patients discharged from hospital to home
Study intervention control group Peto Odds Ratio Weight Peto Odds Ratio
n/N n/N 95% CI (%) 95% CI
Moher 111/136 104/131 57.9 1.15 [ 0.63, 2.11 ]
Sulch 56/76 54/76 42.1 1.14 [ 0.56, 2.31 ]
Total (95% CI) 212 207 100.0 1.15 [ 0.72, 1.82 ]
Total events: 167 (intervention), 158 (control group)
Test for heterogeneity chi-square=0.00 df=1 p=0.98 I2 =0.0%
Test for overall effect z=0.58 p=0.6
0.1 0.2 0.5 1 2 5 10
Favours treatment Favours control
33Discharge planning from hospital to home (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Analysis 09.01. Comparison 09 Outpatient attendance, Outcome 01 Elderly medical patients at 6 months
Review: Discharge planning from hospital to home
Comparison: 09 Outpatient attendance
Outcome: 01 Elderly medical patients at 6 months
Study Treatment Control Peto Odds Ratio Weight Peto Odds Ratio
n/N n/N 95% CI (%) 95% CI
Nazareth 39/137 40/151 100.0 1.10 [ 0.66, 1.85 ]
Total (95% CI) 137 151 100.0 1.10 [ 0.66, 1.85 ]
Total events: 39 (Treatment), 40 (Control)
Test for heterogeneity: not applicable
Test for overall effect z=0.37 p=0.7
0.1 0.2 0.5 1 2 5 10
Favours treatment Favours control
Analysis 10.01. Comparison 10 Medication, Outcome 01 Medication problems after being discharged from
hospital
Medication problems after being discharged from hospitalStudy number of problems notes
Shaw Mean number of problems (SD)
At 1 week
T=2.0 (1.3)
C=2.5 (1.6)
At 4 weeks
T=1.9 (1.5)
C=2.9 (1.8)
At 12 weeks
T=1.4 (1.2)
C=2.4 (1.6)
Problems included difficulty obtaining a prescription from the GP; insufficient knowledge
about medication; non compliance
Analysis 10.02. Comparison 10 Medication, Outcome 02 Adherence to medicines
Adherence to medicinesStudy adherence to meds notes
Nazareth At 3 months:
T=79, mean 0.75 (SD 0.3)
C=72 mean 0.75 (SD 0.28)
At 6 months
T=60, mean 0.78 (SD 0.3)
C=58 mean 0.78 (SD 0.3)
0=none
1=total/highes level
Analysis 10.03. Comparison 10 Medication, Outcome 03 Knowledge about medicines
34Discharge planning from hospital to home (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Knowledge about medicinesStudy knowledge notes
Nazareth At 3 months:
T=86, mean 0.69 (SD 0.33)
C=83 mean 0.62 (SD 0.34)
At 6 months
T=65, mean 0.69 (SD 0.35)
C=68 mean 0.68 (SD 0.3)
Mean difference 0.01 (95% CI -0.12 to 0.13)
0=none
1=total/highes level
Analysis 10.04. Comparison 10 Medication, Outcome 04 Hoarding of medicines
Hoarding of medicinesStudy hoarding notes
Nazareth At 3 months:
T=87, mean 0.006 (SD 0.04)
C=82 mean 0.005 (SD 0.03)
Mean difference 0.001 (95% CI -0.01 to 0.012)
At 6 months
T=70, mean 0.02 (SD 0.13)
C=69 mean 0.013 (SD 0.06)
Mean difference 0.007 (95% CI -0.013 to 0.27)
0=none
1=total/highes level
35Discharge planning from hospital to home (Review)
Copyright © 2008 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd