Embed Size (px)
Citation preview
SEVERE DISSEMINATED CUTANEOUS GOUT-CASE REPORT-
Irina Tudose1, Olguta Anca Orzan2, Diana Petrache2, Prof. Dr. Calin Giurcaneanu2
1 Pathology Department, Elias University Emergency Hospital, Bucharest
2 Dermatology Department, Elias University Emergency Hospital, Bucharest
We present the case of a 53-year-old obese caucasian male with a history of severe hyperuricemia and acute gouty arthritis; frequent hunter and consumer of venison
Chief complaints: disseminated yellow skin nodules dating for about five years with an accelerated development of the lesions during the last year.
Histopathological examination (2010): chronic granulomatous inflammatory process, endogenous foreign body, most likely dermal calcinosis

Grade III obesity (BMI = 43 kg/m2)
Joint swelling (right knee joint and bilateral hand interphalangeal joints)
No lung rales, BP = 130/80 mm Hg, AV = 80/min
no bowel obstruction, occasionally rectorhagia
inflammatory syndrome (ESR = 96 mm/h, Fb = 475 mg/dl)
anemia (Hb = 10 g/dl, Ht = 32.2%)
nitrogen retention (creatinine = 1.83 mg/dl)
uric acid = 11.45 mg/dl mild hyperkalemia proteinuria (1.2 g/24 h)
Past medical history (PMH): Gouty arthritis (1996) – inconsistently treatedFocal segmental glomerulosclerosis (renal biopsy, 2003)Chronic renal failureModerate chronic anemiaEssential hypertension (2004)
Medication: Verapamil, FurosemideFamily history (FH): not significant.
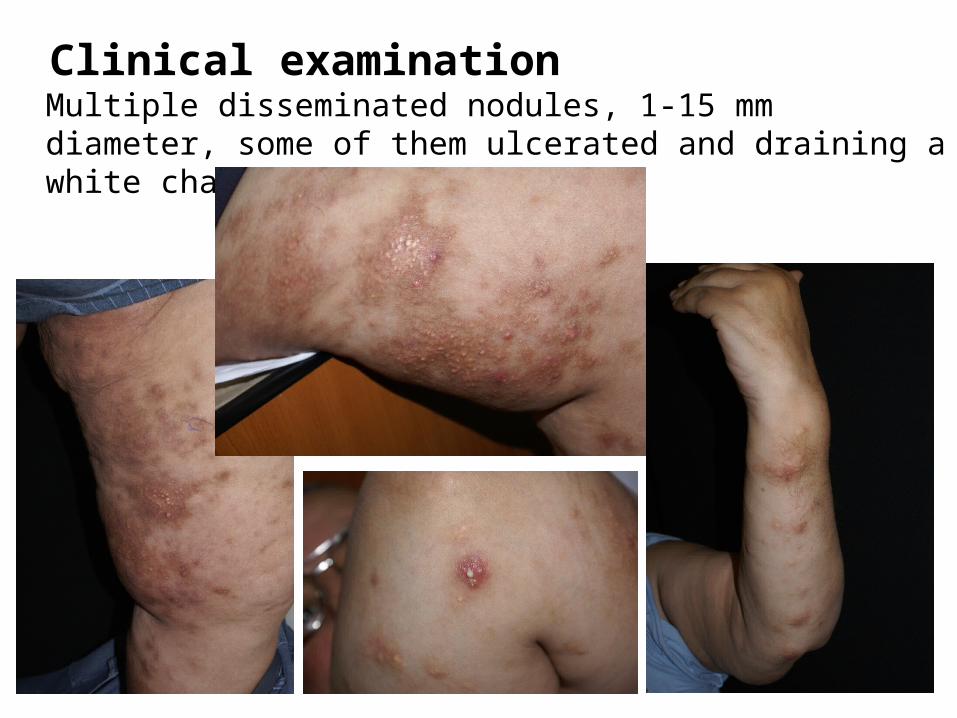
Clinical examination Multiple disseminated nodules, 1-15 mm diameter, some of them ulcerated and draining a white chalky material
Histopathological examination
Usual and special stains: Haematoxilin-eosin Periodic acid Schiff (PAS) Gömöri stain – for reticulin fibers Von Kossa stain – for calcium deposits Red of Congo – for amiloid Elastic Von Gieson – for elastic fibers Polarized light examination
Histopathological description: Two pieces of skin showing dermal granulomatous chronic inflammation with numerous multinucleated giant cells of "foreign body" and foamy macrophages located around focal areas of extensive deposition of amorphous material, acellular, pale-basophilic with focal areas of central suppurative necrosis. After using special stains, it was established that histopathological appearance is compatible with the diagnosis of gout.
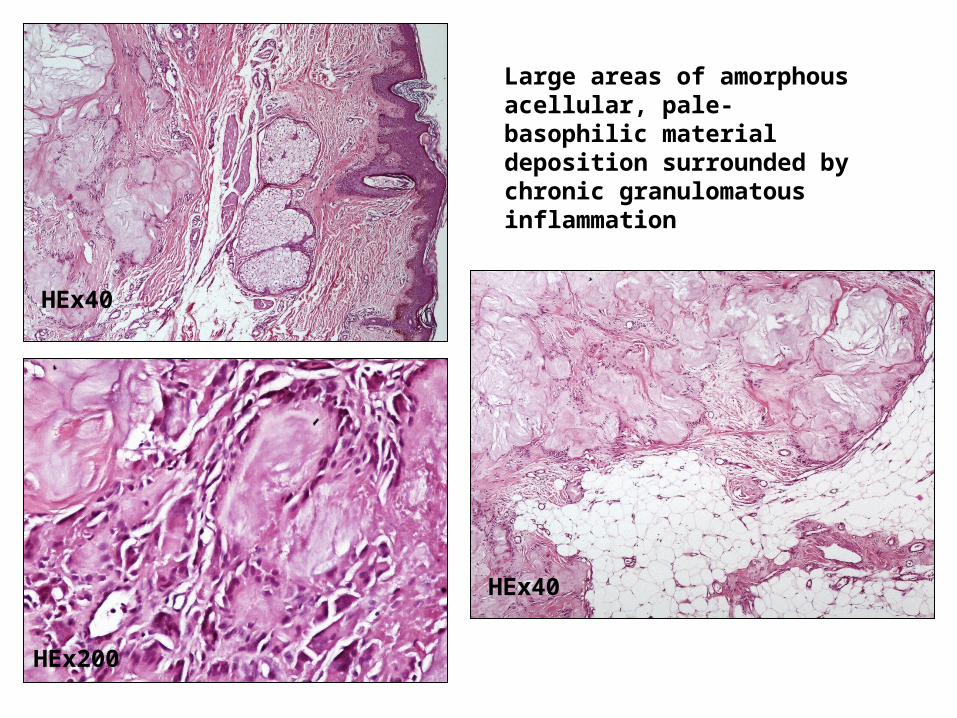
HEx40
HEx40
Large areas of amorphous acellular, pale-basophilic material deposition surrounded by chronic granulomatous inflammation
HEx200
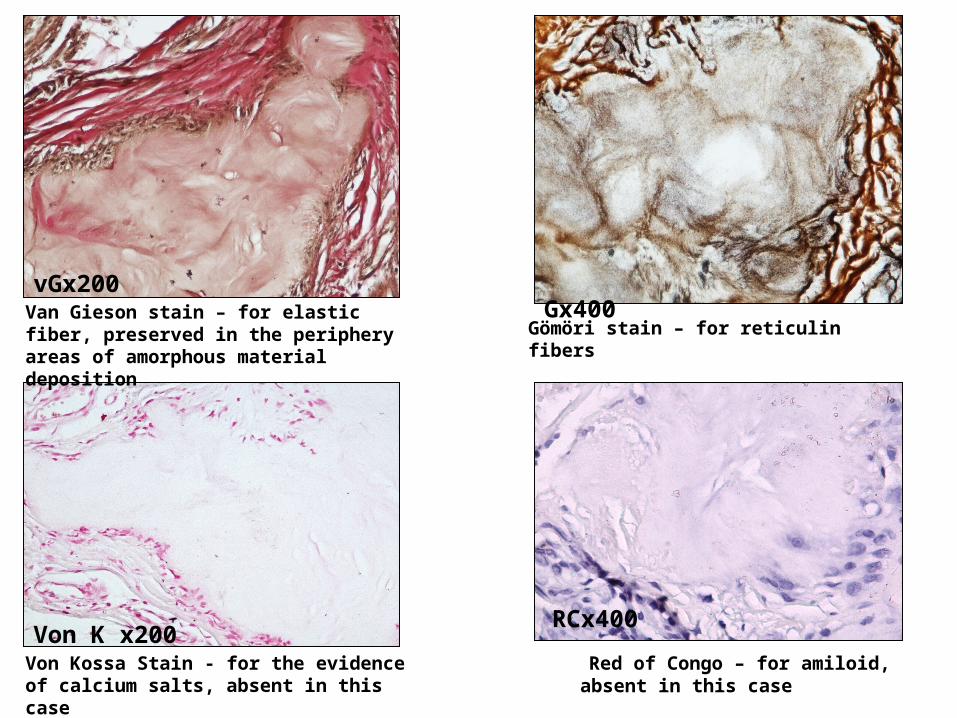
Von K x200Von Kossa Stain - for the evidence of calcium salts, absent in this case
vGx200Van Gieson stain – for elastic fiber, preserved in the periphery areas of amorphous material deposition
Gömöri stain – for reticulin fibers
Gx400
Red of Congo – for amiloid, absent in this case
RCx400

Calcinosis cutis universalis: deposits of calcium phosphate crystals in the tissues
Von Kossa
Rheumatoid nodules:
areas of fibrinoid necrosis board
of chronic granulomatous
inflammation
Differential diagnosis
PAS
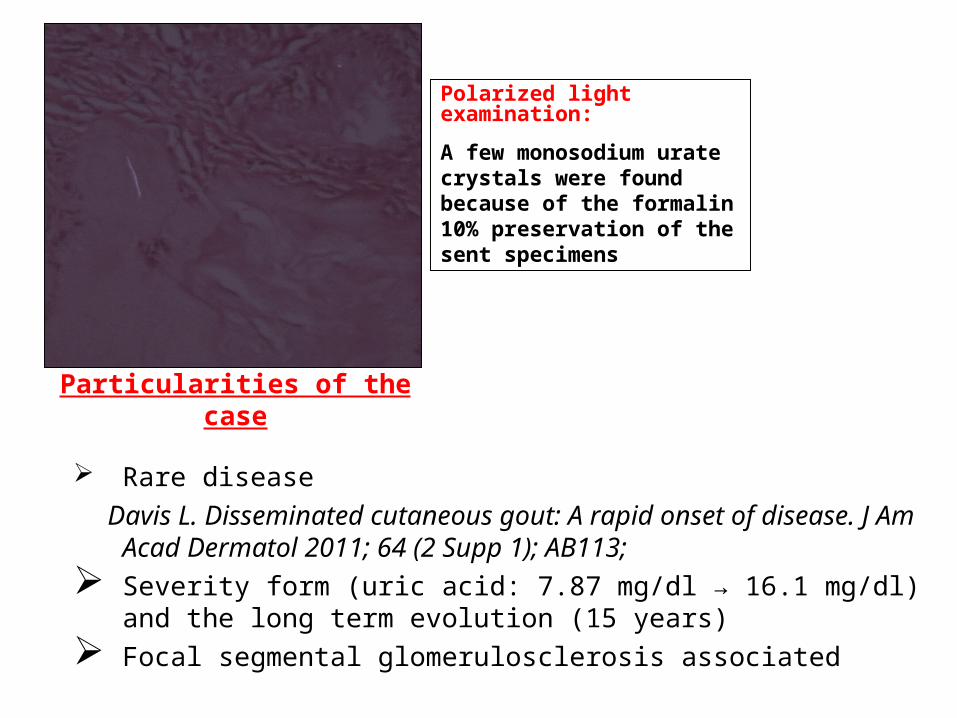
Polarized light examination:
A few monosodium urate crystals were found because of the formalin 10% preservation of the sent specimens
Particularities of the case
Rare disease
Davis L. Disseminated cutaneous gout: A rapid onset of disease. J Am Acad Dermatol 2011; 64 (2 Supp 1); AB113;
Severity form (uric acid: 7.87 mg/dl → 16.1 mg/dl) and the long term evolution (15 years)
Focal segmental glomerulosclerosis associated





























