Embed Size (px)
Citation preview

The Mental Health Context
BC6232
Culture and Mental Health
Rachel Clarke
With thanks to Dr Sarah Coddington-Lawson

Prerequisites for Health (WHO)
The fundamental conditions and resources for
health globally are :
• peace
• shelter
• education
• food
• income
• economic resources (and their distribution)
• sustainable resources and stable ecosystem
• clean water
• social justice, basic human rights and equity
Improvement in health requires a secure foundation in these basic prerequisites
.
Consider also: Love, Communities and Social Connectedness

Determinants of health
The personal, social, economic and
environmental factors which determine
the health status of individuals or
communities (Wilkinson, 2003)
A factor or characteristic that brings
about change in health, either for the
better or for the worse” (Keleher, 2006. P4)

Social determinants of
health
Social gradient (ie “social class” or socio-eco status)
Ethnicity
Stress (effects on health)
Early life
Social exclusion (poverty, discrimination and racism)
Work
Unemployment
Popular culture
Social support
Addiction
Peer pressure
Materialism
Food
Transport
Colonisation
Migration
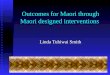
Index : • Life expectancy
• Math & Literacy
• Infant mortality
• Homicides
• Imprisonment
• Teenage births
• Trust
• Obesity
• Mental illness – incl. drug & alcohol addiction
• Social mobility
Health and Social Problems are Worse in More Unequal
Countries
Source: Wilkinson & Pickett, The Spirit Level (2009) www.equalitytrust.org.uk
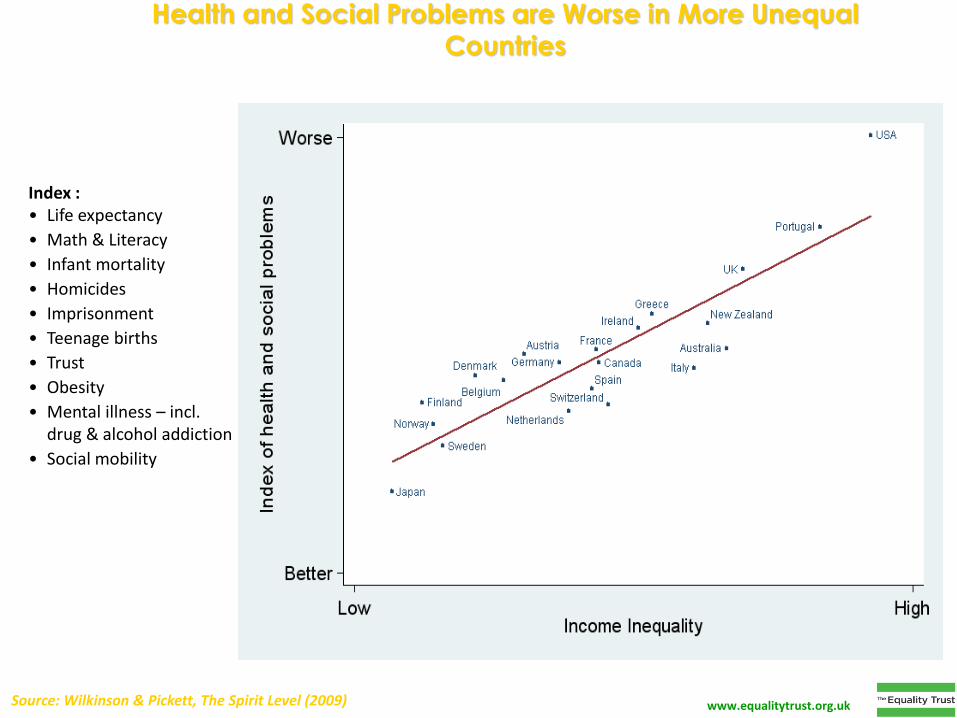
Child Well-being is Better in More Equal Rich Countries
Source: Wilkinson & Pickett, The Spirit Level (2009) www.equalitytrust.org.uk

Drug Use is More Common in More Unequal Countries
Source: Wilkinson & Pickett, The Spirit Level (2009)
Index of use of: opiates, cocaine, cannabis, ecstasy, amphetamines
www.equalitytrust.org.uk
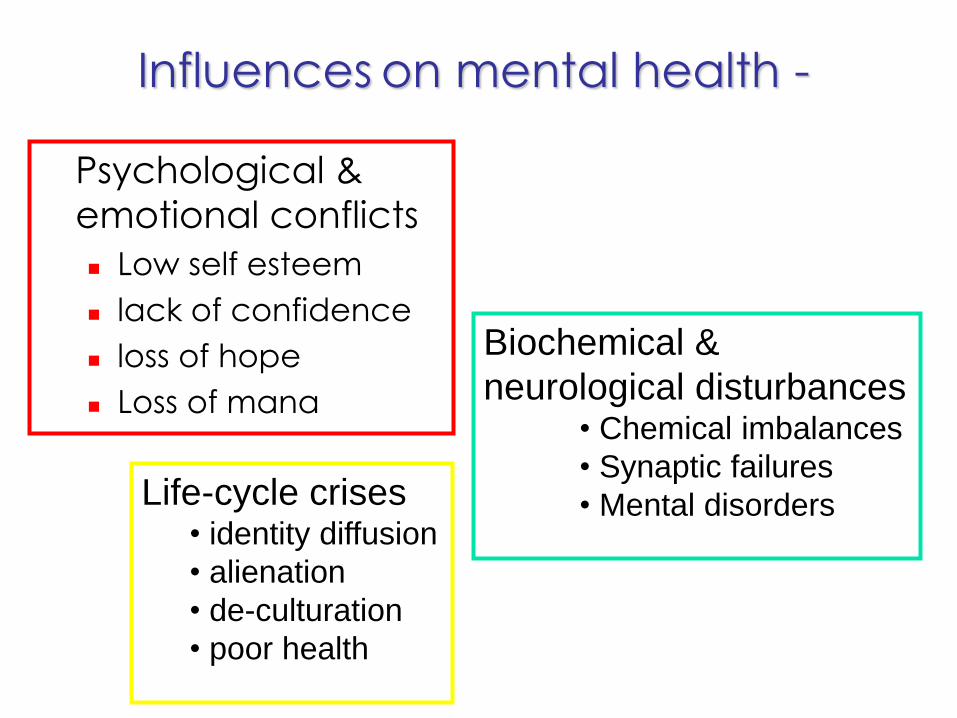
Influences on mental health -
Psychological &
emotional conflicts
Low self esteem
lack of confidence
loss of hope
Loss of mana
Biochemical &
neurological disturbances • Chemical imbalances
• Synaptic failures
• Mental disorders
Life-cycle crises • identity diffusion
• alienation
• de-culturation
• poor health

Interpersonal
relationships Disrupted
Bereavement
Dysfunctional
Threatening
Relationships with family
& community
• Unemployment
• School failure
• Homelessness
• Risk-taking lifestyles
• Bankruptcy
Relationships with society • Loss of usefulness
• Loss of role
• Loss of purpose
• Loss of engagement
Influences on mental health
WHAT IS CULTURE?
In short can be referred to as „a collective sense of identity and belonging‟.

What is Culture?
• Culture refers to the cumulative deposit
of knowledge, experience, beliefs,
values, attitudes, meanings, hierarchies,
religion, notions of time, roles, spatial
relations, concepts of the universe, and
material objects and possessions
acquired by a group of people in the
course of generations through individual
and group striving.

• Culture in its broadest sense is cultivated
behavior; that is the totality of a person's
learned, accumulated experience which
is socially transmitted, or more briefly,
behavior through social learning.
• A culture is a way of life of a group of
people--the behaviors, beliefs, values,
and symbols that they accept, generally
without thinking about them, and that
are passed along by communication and
imitation from one generation to the next.
• Culture is the sum total of the learned
behavior of a group of people that are
generally considered to be the tradition
of that people and are transmitted from
generation to generation.
• Culture is a collective programming of
the mind that distinguishes the members
of one group or category of people from
another

CULTURALLY SANCTIONED ACTS Acts or thoughts that may be considered “abnormal” but
are actually culturally sanctioned
• Talking of “we” not “I” (collective tribal identity): - Maori / Pacific / others
• Hearing voices (Ancestral): - Maori - tupuna / S. America, African nations
• Healing practitioners:- Maori - Tohunga
• Insanity (Incest): - Navaho Indians
• Adoption of female role: - Samoa – Fafafines
• Insanity as Spirit intrusion:- Eskimos
• Arctic Hysteria:- Eskimos
• Terminally Ill (Ritual public suicide):- Eskimos
• Epilepsy (Talking to God):- • Hmong
• Seizures (Powers):- Borneo
• Class (socioeconomic status)
• Gender (Historical context)
• Noble Suicide (Harakiri)/ Japan
Culture Bound syndromes
• DSM-IV: –
• 25 “culture bound syndromes” e.g. • Brain Fags
• Old Hag syndrome
• Amok
• Bouffee delirante
• Wild Man syndrome
• Fan death
• Koro
• …….

Cultural assessment is integral to cultural safety and the development of effective treatment plans. It is widely accepted by practitioners working in mental health services that cultural identity plays a significant part in the wellness of individuals and their communities whatever the culture. Cultural assessment acknowledges the link between identity, wellness, treatment and recovery. Cultural assessment “refers to the process through which the relevance of culture to mental health is ascertained”. Cultural relevance relates to the significance tangata whaiora place on their identity as Māori and how they perceive the role of their cultural heritage in assisting them to achieve wellness. The purpose of cultural assessment is to identify a person‟s cultural needs and any cultural supports or Māori healing practices needed to strengthen identity and enhance wellness.
What is cultural assessment?

The assessment should not only be used to help determine the mental state of tangata whaiora, but also as a tool in planning treatment and rehabilitation programmes. It can determine the significance of cultural factors for the person and enable planning of treatment and rehabilitation processes that address cultural issues. While cultural assessment processes may vary between service providers it is important to remember that they are complementary to clinical assessment and any diagnostic tool, such as DSM IV. Cultural assessment should support service providers to develop and maintain services that are culturally effective and relevant to tangata whaiora and whanau. The outcome of cultural assessment should be a comprehensive treatment and care plan, which includes cultural supports. The information gained from the cultural assessment should fashion the whole clinical care pathway. Mental Health Commission (2004) Delivery of Culturally Appropriate Assessment for Maori. Wellington: Author (pp 3 – 4)

Why Culture Matters in Mental Health
• Striking disparities in mental health care found for
racial and ethnic minorities.
• Less access to and availability of mental health
services
• Less likely to receive needed mental health
services
• Those in treatment often receive a poorer
quality of mental health care
• Barriers to care include mistrust and fear of
treatment, racism and discrimination, and
differences in language and communication.
Murphy and Leighton 1965 recognised that cultural variables on illness existed.
1960‟s
· Community mental health movement
· Greater attention given to ethnic and cultural characteristics of community health
service delivery
1970‟s
· Thomas and Sullen, labelled psychiatry as a „vehicle for covered racism‟
· Indigenous people worldwide voicing concerns
1980‟s
· Maori began presenting an alternative view
· NZ conceding that its attitudes to health and sickness were biased to Western
philosophies and practice
1984
· First major Maori health hui at Hoani Waitititi Marae in Auckland discussed action –
not stats
1986
· Recommendation by Department of Health that the implications of the Treaty of
Waitangi be „seriously considered‟
1988
· Department of Health included statement of corporate intent
· „Accepts‟ biculturalism as a desirable goal
· Te Puawaitanga (2002) – Maori Mental Health National Strategic Framework
1997
· (Durie) rate of mental illness for Maori have increased since 1975, although they
have decreased for a number of primary health problems
Culture and Health – NZ History

http://www.tepou.co.nz/supporting-workforce/lets-get-real




Working with Māori
Essential level learning module
You can access this through Te Pou and use it as a personal resource for developing your learning

Question: What are the fundamental conditions and resources
necessary for health and wellbeing ?
Look in small groups at the policies; organisations and
resources that support mental health in the different
populations
Maori, Pacifica, Asian, Immigrant, Refugee, LGBTT.

Resource Links Look at Te Pou:
http://www.tepou.co.nz/story/2013/11/13/meeting-the-needs-of-gay-
lesbian-bisexual-and-transgender-people---why-it-matters-and-how-to-
do-it
http://www.leva.co.nz/
http://www.matuaraki.org.nz/
http://www.tepou.co.nz/improving-services/asian-refugee-migrant
Look at MOH
http://www.health.govt.nz/our-work/populations
Maori / Pacific / Refugee / Rural / Asian & Migrant
Look at Affinity
http://www.affinityservices.co.nz/resources/
Look at the Australian Clearinghouse
http://203.32.142.106/clearinghouse/
Pacific Information
http://www.networknorth.org.nz/file/Resources/pacific-model-of-care-lo-
res-copy.pdf


http://unitube.otago.ac.nz/file.do?m=5PLC1cYkw6A&name=Kingi_Te_Kani.pdf Click on this link if you wish to view this resource

Emerging approaches to
Diagnosis
Kaupapa Maori Approaches
Pasifika Health and wellbeing
approaches
Positive Psychology (next class)
Underpinned by “Social Determinants” of
health

Kaupapa Maori Assumptions
Foundations Maori knowledge
Maori health perspectives
Engagement with clients
Cultural customs
Whānau sponsorship
Assessment Cultural profile
Relationship map
Cultural interevntion plan
Interventions Rongoa
Cultural therapies
Cultural affirmation
Conventional therapies
Outcomes Wellbeing (spiritual, mental,
physical, family/social)
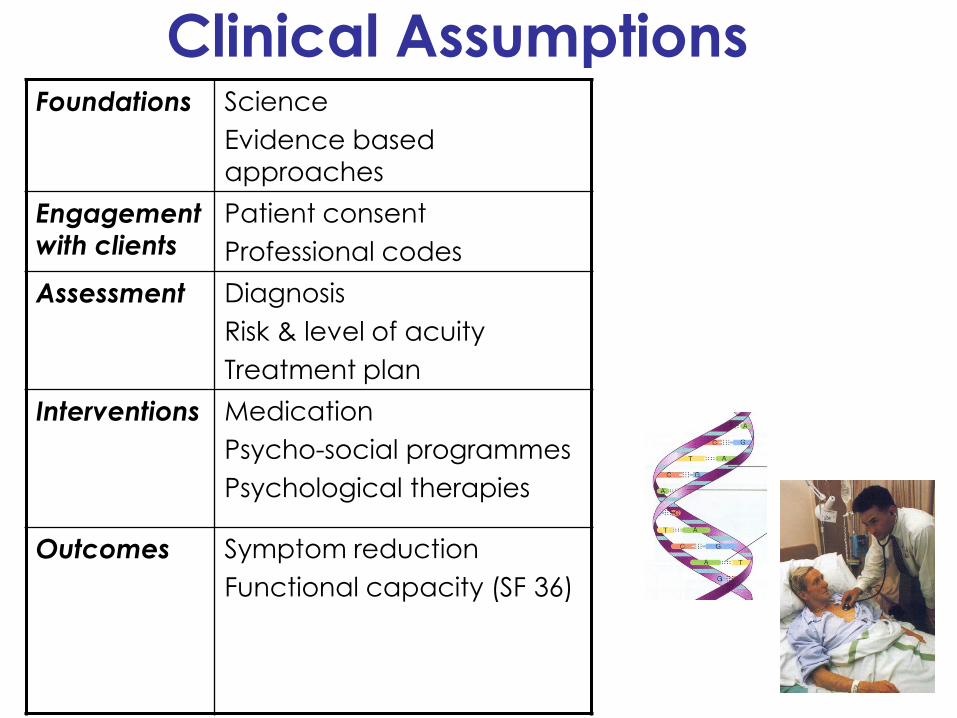
Clinical Assumptions Foundations Science
Evidence based
approaches
Engagement
with clients
Patient consent
Professional codes
Assessment Diagnosis
Risk & level of acuity
Treatment plan
Interventions Medication
Psycho-social programmes
Psychological therapies
Outcomes Symptom reduction
Functional capacity (SF 36)

The Cultural – Clinical Interface
Maori knowledge
Maori health
perspectives
Foundations Science
Evidence based
approaches
Cultural customs
Whānau sponsorship
Engagement with clients
Patient consent
Professional codes
Cultural profile
Relationship map
Cultural intervention plan
Assessment Diagnosis
Risk & level of acuity
Treatment plan
Rongoa
Cultural therapies
Cultural affirmation
Conventional therapies
Interventions Medication
Psycho-social programmes
Psychological therapies
Wellbeing (spiritual,
mental, physical, social) Outcomes Symptom reduction
Functional capacity (SF 36)

THE GOAL
Greater balance
Value of traditional belief systems
+
Incorporation of Western medical
practice

THE MODELS
• Te Whare Tapa Wha
• (Durie 1985)
• All sides are needed to maintain
strength, and ensure shelter
• http://www.health.govt.nz/our-work/populations/maori-health/maori-health-
models/maori-health-models-te-whare-tapa-wha
• Te Wheke
• (Pere 1984)
• Putangitangi
• (Davies, Elkington and Winslade 1993)

TE WHARE TAPA WHA
• Mason Durie
• Maori views on health emphasised aspects different to conservative Western views.
• His model, first presented at hui in Hamilton and Otaki, was received enthusiastically at marae in several parts of the country and was often quoted as the Maori health perspective.
• The model compares health to the four walls of a meeting house
TE WHARE TAPA WHA • Although each wall might be examined separately, all
sides of the house are equally necessary to maintain strength, ensure shelter and give coherence.
• According to Maori tradition, and giving greater meaning to the model proposed by Durie (1985a), a tribal meeting house often represents an ancestor, and within its structure parts of the body are symbolised.
• Each wall was seen to represent a different aspect of health:
• te Taha Wairua, a spiritual component
• te Taha Hinengaro, a psychic component
• te Taha Tinana, a bodily component
• te Taha Whanau, a family component.


Te Taha Wairua
• Whereas there had been an overwhelming Western emphasis on the physical aspects of health and illness (Taha Tinana),
• Maori emphasis had been at a spiritual level (Taha Wairua), sometimes even at the expense of other aspects.
• Good health equated with an appreciation of, and an ability to experience, the unspoken influence: of others, the dead, the environment, and links between them.
• Poor health reflected:
• an absence of a personal or collective spirit and no degree of physical fitness could compensate for an impoverished soul.

Te Taha Tinana • Bodily health, te Taha Tinana. recognised a physical
substrate for health
• though not in quite the same way that anatomists might.
• For one thing, certain parts of the body, and the head in particular, were regarded as special (tapu or sacred).
• Furthermore, bodily functions such as sleeping, eating, drinking and defecating were imbued with their own significance reflecting various levels of importance and requiring quite different rituals. Eating food, for example, was a leveller which removed any vestige of sacredness or distance (as between people).

Te Taha Tinana Maori emphasis on clear separation of Tapu and Noa
Tapu – Head and Genital areas regarded as special of Tapu
Sacred and under restriction, beyond ones power
Head – Housing the brain (hinegaro or think tank)
Genital – Housing Te Whare Tangata or ability to reproduce and there continuation of whakapapa – tribal perpetuation
Noa – Free from Tapu, ordinary, absent from limitation, within ones power
Food removes any vestige of sacredness as does water making one Noa or Whakanoa (to make free from restriction) Thus the need to a group of people to join in a cup of tea immediately after the welcoming ceremony onto a Marae
Also the ritual of washing of throwing water over the body immediately after visiting a deceased body lying in state or a burial

Te Taha Hinengaro • Te Taha Hinengaro, (thoughts and feelings) was seen
as a second fundamental component of health.
• Though similar to 'mental health', it was also different in that Maori views did not regard the separation of thoughts and feelings as valid.
• Equal weight was placed on emotional and verbal communication without an expectation that emotional expression was ultimately only of value if it could be converted into a verbal statement.
• Similarly, Maori placed greater value on thinking which was integrative and holistic, rather than analytical.
• Understanding came from being able to locate an event or comment or situation in a wider context. Microscopic explanations held little sway.

Te Taha Whanau
• Taha Whanau acknowledged that an individual could not exist, healthily, in isolation, particularly from the extended family.
• Independence, to the extent that the group was shunned or even avoided, equated with poor health
• while a close and reciprocal relationship with the whanau (family) was seen as conducive to good health.

TE WHEKE
Pere (1984)
• The octopus, Te Wheke, is used to illustrate the major features of health
• The eight tentacles of the octopus symbolise a particular dimension of health
• The body and head represented the whole family unit.
• The intertwining of the tentacles indicated the close relationships between each dimension.

Te Wheke • Like te Whare Tapa Wha the model
includes:
• wairuatanga (spirituality)
• taha tinana (the physical side)
• hinengaro (the mind)
• whanaungatanga (the extended family, similar to taha whanau).

Pere also promotes the dimensions of:
• mana ake, i.e. the uniqueness of the individual and each family, and the positive identity based on those unique qualities
• mauri, the life-sustaining principle resident in people and objects, including language
• ha a Koro ma a Kui ma, literally the breath of life that comes from forebears, and an acknowledgment that good health is closely linked to a positive awareness of ancestors and their role in shaping the family
• whatumanawa, the open and healthy expression of emotion,necessary for healthy human development
•
• waiora, total wellbeing for the individual and the family, represented in the mode by the eyes of the octopus.


Putangitangi “The Putangitangi is a colourful duck, which is indigenous
to Aoteoroa. Its natural habitat may include four distinct
domains: the sky, the sea, the land and the rivers of
Aoteoroa. At any one time Putangitangi may inhabit any
one of these domains but as a bird it may move with ease
from one habitat to another. Its natural characteristics as
a species grant it the flexibilty to traverse with comfort the
boundaries between sky, sea, land and river. At any one
time we may observe Putangitangi and see it busy living
out its destiny in one habitat, without conceiving of the
whole range of its habitat possiblilites or of how these
might fit together in a life. These characteristics make
Putangitangi useful as a metaphor of our understanding
of Maori worldviews.”
Davies, S., Elkington, A., & Winslade, J. (1993). Putangitangi: A model for understanding
the implications of Maori intra-cultural differences for helping strategies. New Zealand
Association of Counsellors Journal, 15, 2-6.

Sky
Sea
River
Land
Effects of Dominant Culture Str
en
gth
of C
ultu
ral
Ide
ntity
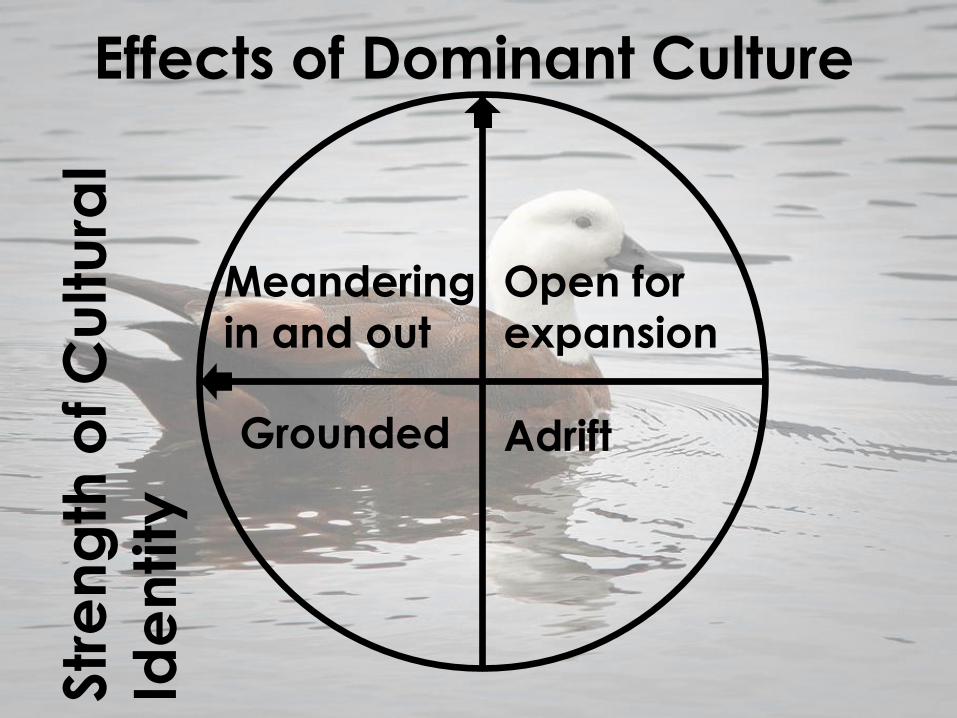
Open for
expansion
Adrift
Meandering
in and out
Grounded
Effects of Dominant Culture Str
en
gth
of C
ultu
ral
Ide
ntity
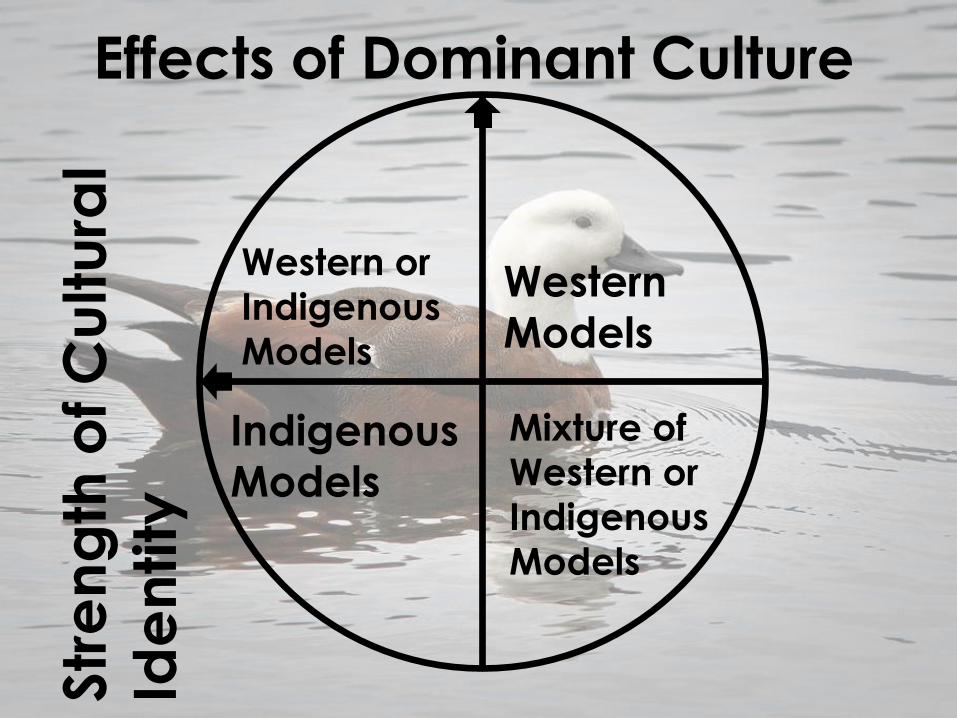
Western
Models
Mixture of
Western or
Indigenous
Models
Western or
Indigenous
Models
Indigenous
Models
Effects of Dominant Culture Str
en
gth
of C
ultu
ral
Ide
ntity

Readings Durie, M. (2009). Maori Knowledge and Medical Science: The
Interface Between Psychiatry and Traditional Healing in New Zealand. In M. Incayawar, R. Wintrob, L. Bouchard & G. Bartocci
(Eds.), Psychiatrists and traditional healers: Unwitting partners in
global mental health (pp. 238-248): John Wiley & Sons.
http://books.google.co.nz/books?id=Su9Zhe3HglsC&pg=PA248&d
q=Durie,+M&hl=en&sa=X&ei=QXGIUsb_AarAiQe99oGAAw&ved=0CDAQ6AEwATgK#v=onepage&q=Durie%2C%20M&f=false
http://www.treasury.govt.nz/publications/media-
speeches/guestlectures/pdfs/tgls-durie.pdf/at_download/file

Pasifika Models


Fonofale model – Samoan holistic model that
recognises that Pacific people’s health is best
nurtured within the social context. Based on Pacific
perspectives it proposes that “the mental
health of Pacific people is intrinsically bound to the
holistic view of health … and … greater
application of Pacific health models is required
including establishing and maintaining links
between mental health primary health and social
services” (Mental Health Commission 2001:6).
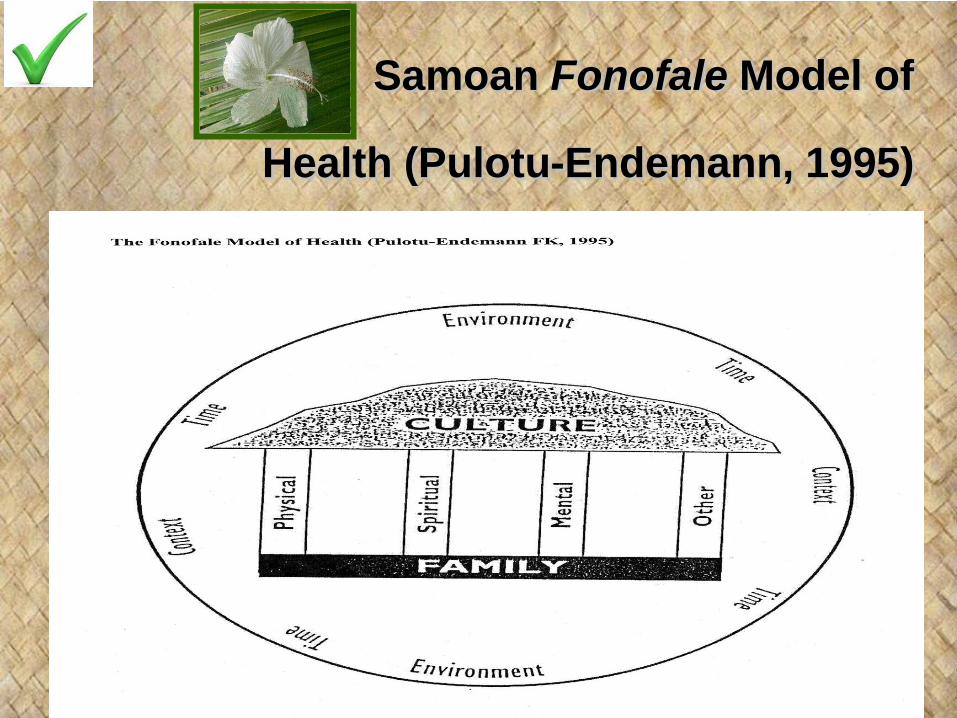
Samoan Fonofale Model of
Health (Pulotu-Endemann, 1995)

FonoFale Model
• Four Pillars of wellbeing supporting Pacific
culture.
• It is set in the wider context of time and the
environment

FonoFale Model
• The Roof-represents pacific peoples
culture – shelter for life
• Culture-incorporates the philosophical
drive and attitudes. It can also include
systems of belief that might be limited to
traditional methods of healing or the use of
Western trained health professionals
FonoFale Model
• The Foundation: is the nucleus and extended family which forms the basis of social organisations for Pacific Peoples. The family provides the base that supports the four posts.
• Spiritual: the sense of wellbeing which stems from a belief system which can include Christianity, traditional spirituality or a combination of both

Four Posts
• Physical: the biological wellbeing of the
body which can be measured by the
absence of illness and pain
• Psychological/mental: the non-physical
aspects of the health of the mind
• Other: this includes things such as gender,
employment, sexuality, age, etc
The cocoon
• Environment: relationship and uniqueness
of Pacific people in relation to their physical
environment (rural or urban).
• Time: Time in history and how this impacts
Pacific people
• Context: influence of Island-reared identity
and NZ-reared identity. Other contexts
include politics and socio-economic

PRESENTATIONS OF MAORI
Later presentation for treatment
Increased acuity levels
Referrals from law enforcement and welfare services (38%)
Early intervention is not accessed
Cultural identity not being recognised, asked about, etc
Shame/Whakama
Te ao Maori – the uniqueness of Maori (As opposed to the socioeconomic disadvantages and disparities
equalled with „being Maori‟)
Possible Cultural Screening
Questions What ethnicities do you identify with?
How willing are they/Do they want to discuss cultural issues with you?
What is their knowledge of whakapapa, reo, tikanga etc
What is their perspective on their presentation/‟Why are you here?‟
What is their perspective on their beliefs, identity, relationships, AOD use, mental health etc?
What is their whanau involvement?
What cultural supports do you have?
What cultural supports do you want?
What do you consider to be treatment options?
What would work/wouldn‟t work for you?

Bridging the
Cultural-Clinical Divide
• Provider experience
Hauora Waikato
• An integrated approach to care and
treatment
• A personalised recovery model

Essentially the “Integrated Personalised Recovery Plan” (IPRP) is a: client centred strengths based recovery focussed model Holistic and culturally focussed model….. That ensures all domains including culture are assessed and integrated treatment plans are developed that support resilience, healing and relevant measurable outcomes.

Towards an
Integrated Personalised Recovery Plan
(IPRP)
• There are limitations in a treatment plan based only on diagnosis
• There are also limitations in a plan for intervention based only on indigenous paradigms
• Limitations can also arise if consumer „autonomy‟ determines the total approach to treatment and care
• What is needed is an integrated recovery plan based on a comprehensive formulation

Integrated
Personalised Recovery Plan A plan for treatment and care that:
• is unified
• is able to respond to all dimensions of
recovery
• incorporates recovery principles
• adopts a positive attitude to long term
outcomes

A Framework for Considering an
IPRP • Aims
• Domains of Recovery
• Recovery principles

IPRP Domains of Recovery • Clinical domains
• Diagnosis & treatment; alleviation of symptoms; syndrome management
• Cultural domains - indigeneity • endorsement of world views, safe engagement with services,
strengthened identity
• Health domains • Improved health status
• (Mental-physical co-morbidities, obesity, heart disease, primary health care)
• Family domains • Family/whānau ongoing care; site for mediation of culture,
relationships
• Societal domains
• greater participation in society – education, employment, housing, income, recreation

IPRP Recovery Principles 1. Personalised recovery
consumer centred, personal values, culture, indigeneity,
the therapeutic relationship
2. Human potential and resilience over time
Adversity should not mask potential; identification of areas
of personal strength and future development
3. Multiple healing pathways
Choice as to intervention, methods of deliver
4. Collaborative leadership Professional e.g. nurse, psychologist, psychiatrist, SW; PHC in future
Consumer e.g. Consumer advocate, consumer advisors
Community leadership e.g. cultural advisors, kaumatua
5. Relevant outcomes
Measurable gains & benefits that are meaningful to
consumers
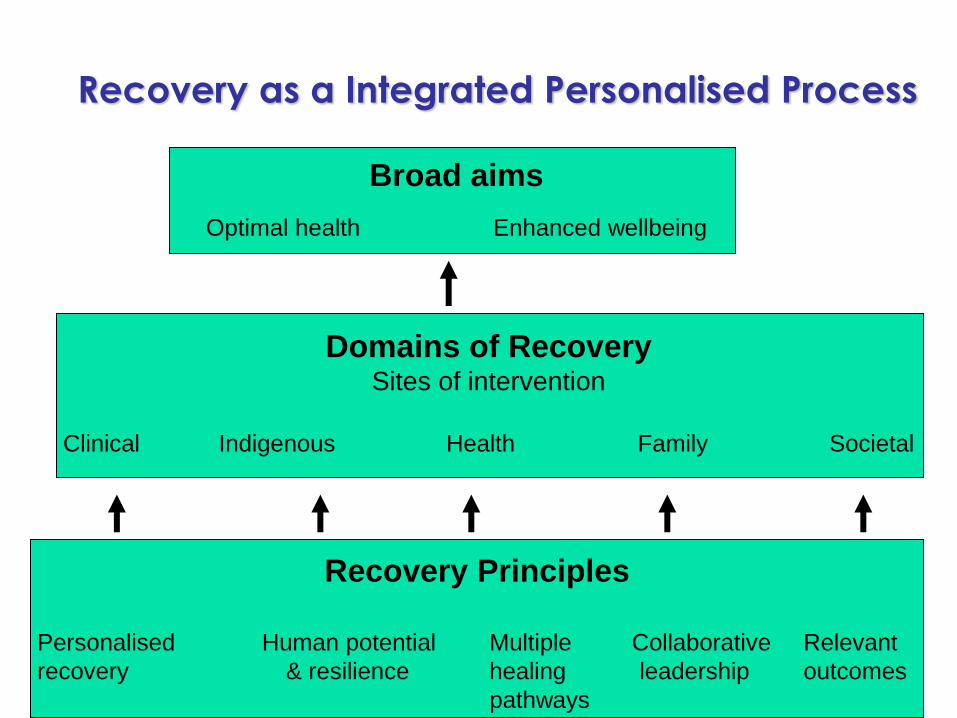
Recovery as a Integrated Personalised Process
Recovery Principles
Personalised Human potential Multiple Collaborative Relevant
recovery & resilience healing leadership outcomes
pathways
Domains of Recovery Sites of intervention
Clinical Indigenous Health Family Societal
Broad aims
Optimal health Enhanced wellbeing

An Integrated Personalised Recovery Plan
Pre-conditions for Change
• A client-centred approach
• A shift from a deficit approach towards a model of potential
• Co-ordination and collaboration across the mental health network of provision (including the primary care sub-sector)
• A „mentor‟ who can work across recovery domains
• (clinical, indigenous, health, family, societal) Durie,M (2007)

CULTURAL INTEGRATION
OVERSEAS
Other Cultures?

Culturally Influenced Perceptions/Barriers
• Associate MHP with other pervasive illnesses
(alcoholism) in their community.
• Believe relapses can occur and a full recovery
to be almost impossible.
• Some distrust of “white” institution.
• View MHP through a narrow lens of
pressure and performance.
• Pride, avoidance of shame, and not losing
face inhibit many from asking for help and
treatment, although many believe that
recovery is possible.
• Perceive MHP as intrinsic to the
acculturation and immigration
process.
• Depression is often seen as a
weakness of character.
Chinese
Native Americans
Hispanics • MHP reflect the inability to cope with life’s
challenges.
• Often too occupied with other priorities,
responsibilities, and challenges to dwell on
mental health.
• Years of discrimination have honed a deep-
rooted pride, that inhibits AAs from
admitting to mental issues, which equate to
weakness.
African Americans

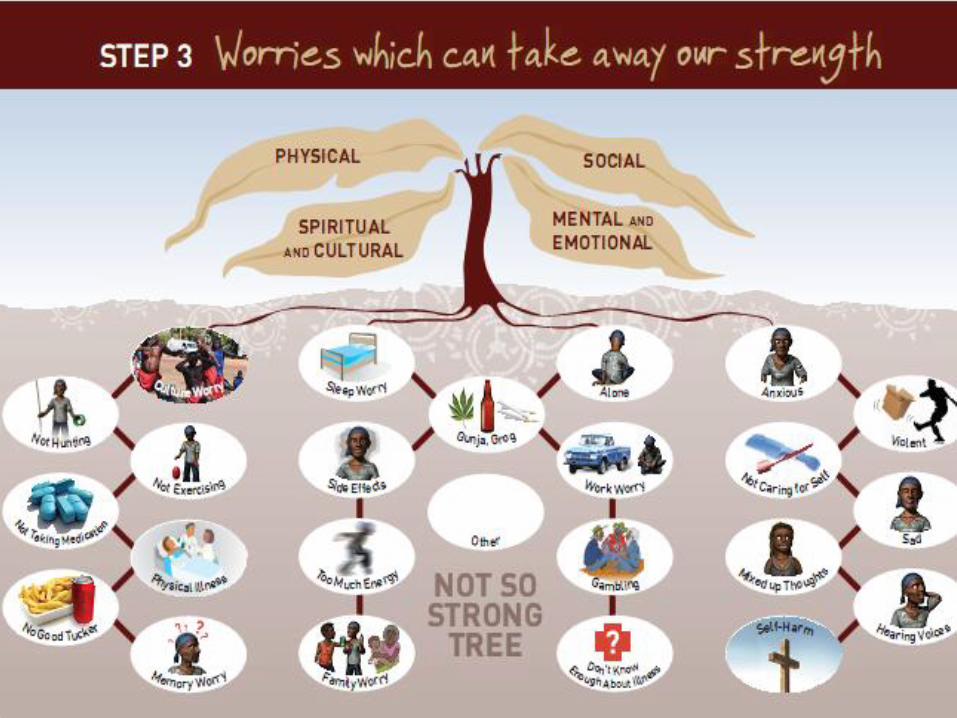
Yarning about Indigenous mental health: Translation of a recovery paradigm to practice.
Abstract of article
Mental health practitioners struggle to translate recovery paradigms into practice. Changing from a
focus on remediation of symptoms to a focus on reclaiming life in the community and enhancing protective factors requires a new approach. One new approach that particularly challenges health providers is the equalising of traditional patient–service provider relationships. Given the additional issues of disempowerment and social disadvantage of Indigenous peoples in Australia, equalising
relationships and embedding recovery values for Indigenous mental health clients especially require urgent attention. There is also a need to learn more about the meaning of recovery in the
Indigenous context and the ways in which it differs from non Indigenous interpretations.
The Aboriginal and Islander Mental health initiative (previously the Australian Integrated Mental health initiative) has developed resources and training which seek to address this gap. The resources support a culturally adapted strengths-based approach to assessment and early
intervention and are increasing popular in mental health, alcohol and other drug and chronic disease settings. Indigenous people with mental illness are subject to additional complex and toxic
combination of social disconnecting factors. Culturally adapted recovery approaches to Indigenous mental illness are thus an important component of closing the gap in Indigenous health.
Citation: Tricia Nagel; Rachael Hinton; Carolyn Griffin (2012). Yarning about Indigenous mental
health: Translation of a recovery paradigm to practice. Advances in Mental Health: Vol. 10, No. 3, pp. 216-223.
doi: 10.5172/jamh.2012.10.3.216
A visually based recovery tool for “The Aboriginal and Islander Mental health initiative” AIMHi (see following slides)



Discussion/Sharing topic
• How can we make our services culturally
safe:
• For clients?
• For clinicians/counsellors?
• What open questions might we ask that
explore how people are connected to or
supported by their whanau or
community?

How can your family or community help you with this problem?
Acknowledgement: Pacific Team, HVDHB. A presentation on Pacific health, 2013