Embed Size (px)
Citation preview

Session 88 PD, Drug Claim Management
Presenters: Daniel Berty
Suzanne Lepage
SOA Antitrust Disclaimer SOA Presentation Disclaimer

Industry pooling solution –Outcomes and opportunities
Dan Berty, Executive Director Canadian Drug Insurance Corporation (CDIPC)June 13, 2017
SOA – Health Meeting – Session 88: Drug Claim Management
(C) Canadian Drug Insurance Pooling Corporation - June 2017 1

Agenda
• Fully insured plan drug pooling in Canada• The story so far• Tends and results• What CDIPC it is and isn’t
• Observations• The eco system’s players and awareness• Industry challenges
• Crystal ball
(C) Canadian Drug Insurance Pooling Corporation - June 2017 2

Who’s in the room?
(C) Canadian Drug Insurance Pooling Corporation - June 2017 3
Who’s heard me speak on drug pooling before?
HEALTH INSURER RE-INSURER
ADVISER, BROKER, CONSULTANT
PHARMA

Time for some exercise in our people pool…..
(C) Canadian Drug Insurance Pooling Corporation - June 2017 4
1) Everyone please stand
up
4) Those standing, with your hand up, grab the flag
and hold it up if the person has
had 2 consecutive
years of drugs costing more than $65,000
2) Sit down if you don’t
personally knowsomeone who is
taking drugs that cost more than $10K per
year
3) Those standing, raise
your hand if you think one of the
person take drugs costing
more than $32,500 per
year

Start with:History / perspective
(C) Canadian Drug Insurance Pooling Corporation - June 2017 5
Source: Shoppers Drug Mart

Extended health insurance – the recent past (through 2005’ish)
• Largest recurrent claims were typically hospital or nursing.
• Often with annual or lifetime caps to limit risk exposure.• Frequency: Low• Annual cost $10-25K
• Drugs have crept up• Annual inflation outpacing CPI at double or triple – largely
driven by new drugs & patent protection.• Largest drug cost approx. $10K per patient per annum.
(C) Canadian Drug Insurance Pooling Corporation - June 2017 6

Incidence rate
(C) Canadian Drug Insurance Pooling Corporation - June 2017 7
Source: Express Scripts Canada Drug Trend Report 2016

High cost drug trend ($10K-30K / certificate estimated by CDIPC)
(C) Canadian Drug Insurance Pooling Corporation - June 2017 8
Estimate:Likely looks
something like…. EP3 / pooling
charge impact

CDIPC claims paid by drug trend 2012-2015
(C) Canadian Drug Insurance Pooling Corporation - June 2017 9

Risk driven by drug coverage
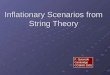
Worst case risk – extended health insurance (excl. travel health insurance risks)
(C) Canadian Drug Insurance Pooling Corporation - June 2017 10
$15,000 $30,000 $100,000
$1,200,000
$2,000,000
$2,500,000
0
1
2
3
4
5
6
$0
$500,000
$1,000,000
$1,500,000
$2,000,000
$2,500,000
$3,000,000
1995 - 2000 2000 - 2005 2005 - 2010 2010 - 2015 2015 - 2020 2020 - 2025
Largest annual EHC expense by certificate Recurrency risk impact index (1-5)

Ergo – need for fully insured drug claim pooling in Canada
• Orphan, biologic, and other drug advances at very high cost for specialized treatments.
• Advances in science = growing pipeline• Sustainability & viability in the face of high cost recurrent drug claims.• Public relation concerns.
• Canadians / plan members and dependents• Plan sponsors• Insurers – 24 member companies
• All fully insured drug plans (not ASO, not refund)• 2 tier pooling structure breaking out LAP risks at a) Insurer and b) Industry levels• Not for profit industry created and owned. CDIPC administers and oversees
adherence to CDIP framework• Not government mandated.
• First year of industry pooling was 2013
(C) Canadian Drug Insurance Pooling Corporation - June 2017 11
Why
Who
What
When

Landing place: Fully insured drug pooling regime or CDIPC framework
(C) Canadian Drug Insurance Pooling Corporation - June 2017 12
Insu
rer
Indu
stry
Proprietary Extended drug Policy Protection Plan Pool or Pools(formerly referred to as Large Amount Pooling / LAP)
Industry pool sharing costs between insurance company members for certificates with recurrent high cost drugs.
In a rapidly evolving Rx drug world, CDIPC is
intended to be a “short term” (10-15 year)
solution, buying time to protect the availability and solvency of small /
mid-size plans.

CDIPC regime components –deeper dive
• Pooling of high costs across employers in designated EP3 pool• Pool entry point defined by insurer - typically between $10K and $15K per
certificate.• Pool up to “CDIPC initial threshold” - $32.5K in 2017.• Can be multiple EP3 pools within an insurer’s offering.• Plans that move between insurers have pooling certificates tracked and pooling
continues. • EP3 pools are prohibited from experience rating customers. Each customer
rated the same way in the pool.• Pools can not be anti-selective (ex: no good, bad, ugly).
• CDIPC or industry pooling• To share recurrent drug costs by certificate from year 2 of occurrence and
beyond.• Pool entry point is CDIPC “Ongoing threshold” ($32.5K in 2017) after 2 years of
drugs at $65K or more.• Pooling at 85% in industry pool up to $500K per certificate.• Allows movement of plans with certificates who have repeating high drug costs
by continuing industry pooling if employer plan moves to new insurer.
(C) Canadian Drug Insurance Pooling Corporation - June 2017 13

CDIPC framework risk design
InsurerEP3 pool(s)
EP3 pooling threshold ($7,500-$15,000 is often typical)
Industry/CDIPC pool threshold ($32,500 in 2017)
Industry/CDIPC pooling maximum ($500K in 2017)
CDIPC Industry pool
Insured plan
sponsor
Claims exceeding CDIPCpooling maximum CDIPC pooling structure:
Shown:• Amounts of claims below
EP3 threshold• EP3 pooling• 15% of claims qualifying
for CDIPC pool• Insurer’s share of CDIPC
pool• 100% of claims exceeding
CDIPC pool maximumNot shown:• Claims that don’t qualify
for CDIPC pooling• 1st year of claims that do
qualify for CDIPC pooling but not pooled till 2nd year it occurs
Insurer risks components:

Industry pool allocationA. % paid drug market share per CDIPC insurer is
determinedB. “A” is multiplied against total of industry pool
for each CDIPC insurer to establish “its share” by paid claim weight.
C. CDIPC tallies the amount pooled in the industry pool by establishing the certificates that qualify for pooling.
D. C is subtracted from B• If negative, this amount is the member pays into the
pool.• If positive, this is the amount the member receives
once all members who pay into the pool have contributed their share.
(C) Canadian Drug Insurance Pooling Corporation - June 2017 15
Example: Canprotect Life Co
A. 15.6% of paid fully insured drug claims in Canada.
B. Industry pool total is $14.2M * 15.6% = $2.21M ins Canprotect’s share of pool.
C. Canprotect’s qualified claims for pooling is $1.9M
D. $1.9M – $2.21 = -$0.31 that Canprotect pays into industry pool.

EP3 and CDIPC successes CDIPC is now in its 5th operating year of pooling.
For insured plans, the program is helping insurers and employers manage catastrophic drug costs and maintain plan affordability as evidenced by:
(C) Canadian Drug Insurance Pooling Corporation - June 2017 16
Measure 2013 2014 2015
Total paid drug claims from fully insured plans $1,327.9M $1,379.9M $1,463.3MClaims where certificate's drugs exceed initial threshold of $25K in 2013, $27.5K in 2014, and $30K in 2015
$170.3M $189.0M $288.7M
Eligible amounts of claims that qualify for pooling(2 or more yrs greater initial threshold –or- 2 yrs greater than initial threshold and subsequent yrs greater than initial threshold)
$16.3M $24.5M $31.6M
CDIPC pool shared by insurers from qualified claims $8.9M $13.0M $16.7M
# of certificates exceeding initial threshold 4,205 4,018 4,093
# of certificates in pool 190 262 395
# of by duration of pooling 1 yr = 144 1 or 2 yrs = 144
2 yrs = 893 yrs = 306
# of “leading” drugs in the pool 42 51 63
# “leading” drugs not pooled in prior year - 17 15
Direct impact of risk averted: EP3 level pooling that might not have existed for many small/mid size employers.
Catastrophic plan risk averted and plan viability
maintainedDrug plan viability maintained despite material risk exposure increase from
new drugs.

and CDIPC drug pooling:What it is and isn’t
(C) Canadian Drug Insurance Pooling Corporation - June 2017 17
Is Is notEP3: Standardized risk sharing approach within the insurer's book of business of high cost drugs (typically greater than $10K per year per certificate).
A means to mute inflationary pressures on drug plans. Like all pooling programs, it spreads the risk to a wider “pool” and shares the impact when realized.
EP3: Ensures experience rating does not occur and ensures bad risks are not selected against by the insurer.
An industry vehicle to provide alternatives to ASO and Refund plans with recurrent large drug claims. When ASO or refund moves to CDIPC, those plan members are excluded from CDIPC coverage.
CDIPC: Standardized approach to share costs for paid drug claims over $32.5K from year two onward, up to $500K annually.
A means to reduce the cost of drugs or address inherent “challenges” in the pharma / pricing system.
A means to ensure the extended health care private insurance market remains competitive.
A vehicle to advance socio/political agendas in drug spending and health care.

Observations after 3 years of pooling
(C) Canadian Drug Insurance Pooling Corporation - June 2017 18

Paid claims
Stop loss impact
Stop loss %
increase over
prior year
Paid claims
Stop loss impact
Stop loss %
increase over
prior year
Paid claims
Stop loss impact
Stop loss %
increase over
prior year
Paid claims
Stop loss impact
Stop loss %
increase over
prior year
Net value over stop
loss threshold
Net inflation above stop
loss threshold over prior
year
Net cumulative
inflation above stop
loss threshold
2013 $10,000 4.2% $11,000 $1,000 N/A $13,500 $3,500 N/A $375 $0 N/A $4,500 N/A N/A2014 $10,000 3.9% $12,100 $2,100 110% $16,500 $6,500 86% $25,000 $15,000 N/A $264 $0 $23,600 424% 424%2015 $10,000 6.0% $12,500 $2,500 19% $16,750 $6,750 4% $27,500 $17,500 17% $30,000 $27,900 N/A $54,650 132% 1114%2016 $10,000 6.6% $12,850 $2,850 14% $16,600 $6,600 -2% $27,900 $17,900 2% $31,250 $28,750 3% $56,100 3% 1147%
YearStop loss /
LAP threshold
Annual total drug
inflation on plan
Howard Sheila Rubby Godfrey Total impact above stop loss threshold
The leveraged effect of high cost drug inflation on pooling
(C) Canadian Drug Insurance Pooling Corporation - June 2017 19
Capital sewage
and drainage
Keeping the nation’s capital blockage free since
confederation
- 46 employees- 6 locations in Ottawa- $7.8M in annual revenue
Fictitious company but this kind of situation occurs with regularity.

Observation: Consequence of pooling & leverage effect
Marketplace:A. Perception that extended health insurance, especially drug, is very
profitable for insurers.B. Pooling not well understood outside of actuarial community
including brokers, insurer account execs, and some marketing team members.• There hasn’t really been a need in a material way to explain pooling until high
cost drugs. • Situation is compounded by lack of transparency to a degree.• Explaining pooling is reasonably complicated and could compromise (to a
degree) an insurer’s competitiveness.C. “Leverage effect” largely not understood.
(C) Canadian Drug Insurance Pooling Corporation - June 2017 20

Observation: Insurer organizational design can cause gaps in market messaging around pricing focus.
(C) Canadian Drug Insurance Pooling Corporation - June 2017 21
Group benefits
Finance & actuarial
FinanceActuarial
(prime focus is LTD and Life)
Business Development
Underwriting Marketing Sales
Operations
Claiims
Who tells the story?What is the story?

(C) Canadian Drug Insurance Pooling Corporation - June 2017 22
Snapshot of drug trend:“Leading” drugs pooled by CDIPC
Observations:• This is only drugs pooled at industry level. What about those
that pool only in EP3?• New drugs (even factoring in recurrent nature – 1 yr lag)• Predicting risk of occurrence: To a degree / unluckiness factor underwriting / pricing?

Drug pooling future / rapidly shifting (by insurance standards) landscape
• Environment continues to get more complex with many moving elements impacting both public and private payors.
(C) Canadian Drug Insurance Pooling Corporation - June 2017 23
Issue Public payor significance
Private payor significance
Pharma strategies High High
Pharmacy strategies N/A Medium
Patent medicines pricing review board (PMPRB) direction High High
Risk tolerance of underwriter Medium High
Specialty drug pipeline Medium High
Pharmacare directions or not High High
Drug cost management strategies High High
Drug prior authorization strategies N/A Medium
Drug eligibility / coverage strategies High High

Crystal ball
(C) Canadian Drug Insurance Pooling Corporation - June 2017 24

Fearless predictions• Many more biologics and orphan drugs coming• More approved uses of “newer” high cost drugs• Greater emphasis on drug risk analysis
• Pipeline and likeliness of occurrence• Potentially new drug pooling innovations for ASO and possibly Refund lines
• Considerably more drug risk management approach innovation coming
• PBM based (and possibly shared amoungst PBM users)• Insurer based – likely competitive differentiator• Mobile devices will somehow play a role
• It’s a matter of time before the “big one” hits the press and in a slow news cycle.
(C) Canadian Drug Insurance Pooling Corporation - June 2017 25

(C) Canadian Drug Insurance Pooling Corporation - June 2017 26

REPRODUCTION REQUIRES PERMISSION OF SUZANNE LEPAGE CONSULTING INC.
Canadian Drug TrendsExamining drug costs
and levers that influence them
Health Meeting of the Society of Actuaries (SOA)
Diplomat Resort, Hollywood, FL
June 13, 2017
Presented by: Suzanne Lepage, Private Health Plan Strategist

REPRODUCTION REQUIRES PERMISSION OF SUZANNE LEPAGE CONSULTING INC.
Overview1. Drug cost components2. Patented Medicine Price Review Board (PMPRB)3. Pan Canadian Pharmaceutical Alliance (pCPA)4. Drug Mix – new vs old drugs5. Drug Choice - influencers6. Drug Acquisition Cost - Pharmacy Agreements and Preferred
Networks7. Cost Shifting

REPRODUCTION REQUIRES PERMISSION OF SUZANNE LEPAGE CONSULTING INC.
Drug Price
Mark-up
Dispensing Fee
Drug Cost Claims Volume
• Age • Health• Industry• Location• Gender

REPRODUCTION REQUIRES PERMISSION OF SUZANNE LEPAGE CONSULTING INC.
Savings can be generated by Reducing purchase price of prescribed drugCost shifting to patient or governmentReducing or eliminating claimsChanging prescription to lower cost medication
Drug Plan Savings

REPRODUCTION REQUIRES PERMISSION OF SUZANNE LEPAGE CONSULTING INC.
Patented Medicine Price Review Board (PMPRB)

REPRODUCTION REQUIRES PERMISSION OF SUZANNE LEPAGE CONSULTING INC.
Patented Medicine Price Review Board (PMPRB)
Regulatory mandate : To ensure that prices at which patentees sell their medicines in Canada are not excessive • Regulates pharma list prices for Brand Name Drugs ONLY (NOT
markup or dispensing fee or generic drugs)• Determines maximum price at which a drug can be sold in
Canada• Key factors:
a. Therapeutic improvement relative to standard of careb. Therapeutic class comparatorsc. Canadian prices of comparatorsd. International prices
• Drug prices cannot increase by more than the Consumer Price Index (CPI)
• Price can never be higher than highest international price of: France, Germany, Italy, Sweden, Switzerland, UK and USA
Drug Price
Mark-up
Dispensing Fee
PMPRB

REPRODUCTION REQUIRES PERMISSION OF SUZANNE LEPAGE CONSULTING INC.
Pricing – International comparisons• Many countries reference other countries’ prices• Complex and constantly changing• Requires active monitoring and management• Significant financial implications • May delay or forego product launch in a country if
international impact determined to be net negative• Canadian pricing teams must consider impact of
Canadian prices on other countries• Price often a global head office decision

REPRODUCTION REQUIRES PERMISSION OF SUZANNE LEPAGE CONSULTING INC.
PMPRB Reform
• PMPRB consultation on guidelines reform• Discussion Paper and public submissions (2016)
Objectives:• informed discussion on changes that have taken place in the operating environment• identify areas of the guidelines that may be particularly in need of reform • encourage public participation to obtain a diverse array of viewpoints
“Recent and significant changes in the Patented Medicine Prices Review Board’s (PMPRB) operating environment necessitate corresponding changes to modernize and simplify its regulatory framework.”
67 Submissions as of deadline (October 31, 2016)
PMPRB Guidelines Modernization – Discussion Paper – June 2016

REPRODUCTION REQUIRES PERMISSION OF SUZANNE LEPAGE CONSULTING INC.
May 16, 2017 – Federal Health Minister Addressed Economic Club to discuss proposed changes to drive down ‘unacceptably high drug costs’

REPRODUCTION REQUIRES PERMISSION OF SUZANNE LEPAGE CONSULTING INC.
Proposed Amendments to PMPRB Regulations Highlights:
Introduce three new factors to determine excessive drug price:• Pharmacoeconomic evaluation for the medicine and others in the same therapeutic class in and
outside of Canada • Size of the market for the medicine in Canada and other countries (estimated uptake of by approved
indication)• Gross Domestic Product in Canada
Require drug companies to report to the PMPRB all indirect price reductions (rebates, discounts, free goods)

REPRODUCTION REQUIRES PERMISSION OF SUZANNE LEPAGE CONSULTING INC.
Change Comparator CountriesCurrent Proposed
No Change
FranceGermanyItalySwedenSwitzerlandUnited Kingdom
FranceGermanyItalySwedenSwitzerlandUnited Kingdom
New
AustraliaBelgiumJapanNetherlandsNorwaySouth KoreaSpain
Removed United States United States
Additional potential changes noted:
• Increase capacity of pCPA• Align Health Canada and CADTH review process to run concurrently
to provide faster access to new medications • Expand Priority Review process for new drugs that meet special
needs• Common National Formulary• Improved data analysis via CIHI• Improve monitoring and analysis of real world evidence during
drug life cycle• Canada Health Infoway – introduce national electronic prescribing
Proposed Amendments to PMPRB Regulations
Health Canada is currently seeking input from stakeholders and the public on these proposed amendments. The online consultation runs through June 28, 2017
https://www.canada.ca/en/health-canada/programs/consultation-regulations-patented-medicine.html

REPRODUCTION REQUIRES PERMISSION OF SUZANNE LEPAGE CONSULTING INC.
Pan Canadian Pharmaceutical Alliance pCPA

REPRODUCTION REQUIRES PERMISSION OF SUZANNE LEPAGE CONSULTING INC.
Pan Canadian Pharmaceutical Alliance (pCPA)
• Joint confidential negotiations for brand name drugs for publicly funded drug programs ONLY
• Generic Value Price Initiative and Biosimilars First Principles lowered prices for all Canadians
• CLHIA lobbying for private payers to be included in negotiations
Drug Price
Mark-up
Dispensing Fee
PCPA

REPRODUCTION REQUIRES PERMISSION OF SUZANNE LEPAGE CONSULTING INC.
Did you say lower drug prices?
Why not have private plans be part of pCPA?

REPRODUCTION REQUIRES PERMISSION OF SUZANNE LEPAGE CONSULTING INC.
Considerations - Private Plans joining pCPAPrivate plans may • be required to harmonize drug plan designs• be limited by government listing recommendations • cover fewer drugs• face listing delays
pCPA negotiations –Listing Delays 1
• 40% of drugs remain at six months
• 25% remain at nine months
• Two drugs beyond one year
1 - Research conducted by Roubaix Strategies Inc (as of December 31, 2016)

REPRODUCTION REQUIRES PERMISSION OF SUZANNE LEPAGE CONSULTING INC.
Skinner et al. Pharmacare: what are the costs for patients and taxpayers? (2015)
Considerations - Private Plans joining pCPA

REPRODUCTION REQUIRES PERMISSION OF SUZANNE LEPAGE CONSULTING INC.
Considerations - Private Plans joining pCPAPrivate plans may • be required to harmonize drug plan designs• be limited by government listing recommendations • cover fewer drugs• face listing delays• have different objectives than government plans • be first and only payer (in pCPA for certain drug and competitor(s) or province(s) that are not)• lose competitive advantage • may get less savings than individual negotiations• potential to dilute overall potential savings due to consensus based negotiating• require additional resources to manage pCPA participation

REPRODUCTION REQUIRES PERMISSION OF SUZANNE LEPAGE CONSULTING INC.
Potential Impacts of Private Plans joining pCPA?
• Would private plans be better served by negotiating their own agreements with pharmaceutical manufacturers?
• Individually (e.g. Remicade)
• Collectively (buying group)
Potential Challenges
• Competition Law
• Harmonization of plan designs
• Reduced competitive advantage
• Resourcing and expertise

REPRODUCTION REQUIRES PERMISSION OF SUZANNE LEPAGE CONSULTING INC.
Drug Mix

REPRODUCTION REQUIRES PERMISSION OF SUZANNE LEPAGE CONSULTING INC.
Drug Mix
• New drugs enter the market at higher cost than existing treatments
• Shifts use from lower to higher cost drugs• Why do we need new treatments?
• Incremental innovation• Improved outcomes• Scientific advancements• Unmet need
Impact1
• increased costs by 5.6% in 2015• up from approx. 3% per year in 2008 to 2011
1 - Private Drug Plans in Canada: Cost Drivers, 2008 to 2015, National Prescription Drug Utilization Information System (NPDUIS), (Partnership between the PMPRB and the Canadian Institute for Health Information (CIHI)) http://www.pmprb-cepmb.gc.ca/view.asp?ccid=1245&lang=en
Drug Price
Mark-up
Dispensing Fee
Drug Mix

REPRODUCTION REQUIRES PERMISSION OF SUZANNE LEPAGE CONSULTING INC.
Drug Choice

REPRODUCTION REQUIRES PERMISSION OF SUZANNE LEPAGE CONSULTING INC.
Drug Price
Mark-up
Dispensing Fee
Drug Choice

REPRODUCTION REQUIRES PERMISSION OF SUZANNE LEPAGE CONSULTING INC.
Drug Price
Mark-up
Dispensing Fee
Drug Choice
• Physicians are the gatekeepers for prescriptions
• Most physicians have limited knowledge of relative drug pricing
• Pharmacists can have a role to influence drug choice
• Expanding scope of practice -may be able to adapt Rx
• Contact Dr to change Rx
• 72% of Drs say a patient having private prescription drug coverage has an impact on their approach to patient care and prescribing prescription drug
• 52% more likely to prescribe brand name drugsThe Group Benefits Prescription Drug Outlook (2014)
Unfortunately, current pharmacy systems and physician EMR provide limited or no information about private
coverage, plan designs and lower cost alternatives

REPRODUCTION REQUIRES PERMISSION OF SUZANNE LEPAGE CONSULTING INC.
Generic Substitution Vs SwitchingGeneric substitution
• Health Canada determines generic and brand are interchangeable• Pharmacist can switch to generic drug without notifying doctor
Switching (Therapeutic Substitution)• pharmacist dispenses different drug than prescribed by doctor
• Why? – Medical: tolerability, adverse event– Non Medical: plan design, affordability
• consult with doctor and patient to dispense a different drug• some provinces now allow pharmacists to substitute different medication without
consulting doctor

REPRODUCTION REQUIRES PERMISSION OF SUZANNE LEPAGE CONSULTING INC.
Drug Price
Mark-up
Dispensing Fee
Drug Choice
Plan Designs influence drug choice
• Managed Formularies• Tiered Formularies• Provincial Mimic Plans• Prior Authorization• Step Therapy• MAC /Reference Pricing• Case Management• Preferred Pharmacy Network

REPRODUCTION REQUIRES PERMISSION OF SUZANNE LEPAGE CONSULTING INC.
Deciding which drugs to cover
• Why are certain therapies covered versus others?• Why do different payers come to different coverage decisions
about the same drug?

REPRODUCTION REQUIRES PERMISSION OF SUZANNE LEPAGE CONSULTING INC.
Determining value depends on:• perspective of the evaluator• what is included in benefit and cost
Deciding which drugs to cover

REPRODUCTION REQUIRES PERMISSION OF SUZANNE LEPAGE CONSULTING INC.
CADTH - CDR“Through the CDR process, CADTH conducts thorough and objective evaluations of the clinical, economic, and patient evidence on drugs, and uses this evaluation to provide reimbursement recommendations and advice to Canada’s federal, provincial, and territorial public drug plans, with the exception of Quebec.”
“The perspective chosen for the evaluation should fit the needs of the target audience. The perspective in the Reference Case should be that of the publicly funded health care system.”

REPRODUCTION REQUIRES PERMISSION OF SUZANNE LEPAGE CONSULTING INC.
Improved health
outcomes
Reduce Dr Visits
Reduce hospital
stays
Reduce tests required
Reduce health care staff
costs
Societal Benefits
Population Health
Improved productivity
Reduce absenteeism
Prevent long term disability
Public Plan QC
Private Drug Plan
?
Patient
Value is in the eye of the beholder

REPRODUCTION REQUIRES PERMISSION OF SUZANNE LEPAGE CONSULTING INC.
Preferred Pharmacy Network (PPN)

REPRODUCTION REQUIRES PERMISSION OF SUZANNE LEPAGE CONSULTING INC.
Drug Price
Mark-up
Dispensing Fee
Pharmacy Agreements
Plan Sponsors
~400-600K
PlanAdvisors~3,000
Insurers~15
Pharmacies~9K
PBM~3
Plan Members~ 19M
Pharmacy Agreement Terms1. Drug Price Source2. Allowable Markup3. Allowable Dispensing Fee

REPRODUCTION REQUIRES PERMISSION OF SUZANNE LEPAGE CONSULTING INC.
Drug Price
Mark-up
Dispensing Fee Preferred
Pharmacy Network
PPN
Preferred Pharmacy Network (PPN)
A network of pharmacies that agree to provide guaranteed levels of service, competitive dispensing fees and markups for the plans that participate in the network.
Potential Savings MoreLess
OptionalUse of PPN is optional for
member
MandatoryRequire
members to use the PPN to be reimbursed
IncentiveProvide a
higher reimbursement
% for members who
choose PPN

REPRODUCTION REQUIRES PERMISSION OF SUZANNE LEPAGE CONSULTING INC.
Cost Shifting

REPRODUCTION REQUIRES PERMISSION OF SUZANNE LEPAGE CONSULTING INC.
Cost Shifting
Plan Pays
Plan Member Copayment
Plan Designs that shift cost
• Coinsurance• Dispensing fee caps• Maximums• Tiered Formularies
Potential Challenges• Member/patient affordability• Poor adherence• Impact on health outcomes

REPRODUCTION REQUIRES PERMISSION OF SUZANNE LEPAGE CONSULTING INC.
Prov
inci
al D
rug
Plan
Inte
grat
ion Cost
Shifting Government Cost Shifting Challenges
• Lack of alignment between Private vs Public• Provincial plans cover less drugs• Different clinical criteria• Satisfying deductibles

REPRODUCTION REQUIRES PERMISSION OF SUZANNE LEPAGE CONSULTING INC.
Provincial Drug Plan Integration ChallengesExample ON Trillium Drug Program• To satisfy deductible ONLY out-of-pocket
expenses borne strictly by the plan member (no COB or pharma PSP)
• Deductible ~4% of household income• Median income of $78,790 = ~$3,000
per year deductiblePotentially only 9% of plan members
would be eligible for Trillium1
1 - De-mystifying the Trillium Drug Program (TDP)http://assets.greenshield.ca/greenshield/GSC%20Stories%20(BLOG)/Follow%20the%20Script/2017/english/Follow%20the%20Script_Spring%202017.pdf
• Two application processes1. Trillium – Financial Eligibility2. Exceptional Access Program (EAP)
– Clinical eligibility• Not all private plan drugs covered by
ODB• ODB EAP criteria may be different that
private plan criteria

REPRODUCTION REQUIRES PERMISSION OF SUZANNE LEPAGE CONSULTING INC.
Plan objectives should drive decisions

REPRODUCTION REQUIRES PERMISSION OF SUZANNE LEPAGE CONSULTING INC.
Plan objectives should drive decisions
• Insurance protection for employee’s unexpected serious illness? (risk management)
• Tax effective compensation? • Health care costs - cash flow / expense management?• Line item expense to be budgeted and managed?

REPRODUCTION REQUIRES PERMISSION OF SUZANNE LEPAGE CONSULTING INC.
Summary1. Drug cost components2. Patented Medicine Price Review Board (PMPRB)3. Pan Canadian Pharmaceutical Alliance (pCPA)4. Drug Mix – new vs old drugs5. Drug Choice - influencers6. Drug Acquisition Cost - Pharmacy Agreements and Preferred
Networks7. Cost Shifting

REPRODUCTION REQUIRES PERMISSION OF SUZANNE LEPAGE CONSULTING INC.
Questions and Discussion
[email protected]@suzannelepage.ca
519-954-8873 (B)519-635-5175 (M)
@suzannelepage