Embed Size (px)
Citation preview

1Oncology Nursing Society 39th Annual Congress May 1–4, 2014
Friday, May 2
When it comes to emergency management of hypersen-sitivity infusion reactions, many oncology nurses have a general knowledge but not the ability to apply immediate pharmacologic interventions. Don’t stop at by-the-books knowledge—make sure you’re prepared for the rapid recog-nition, management, and treatment of these complications. In this session, you’ll cover the pathophysiology and etiol-ogy of an infusion reaction, preventive and therapeutic phar-macological management, how to incorporate the CTCEA grading criteria to guide nursing interventions, and how to perform a comprehensive nursing risk assessment. Speak-ers will walk you through an evidence-based, nurse-driven procedure within a large healthcare system, helping you to visualize the outcomes of time-sensitive assessment and management.
Content Area: Clinical Practice
Content Level: Intermediate
Coordinator/Speaker:Mary Brandsema, RN, MSN, OCN®, CHPNOncology Nurse EducatorOcean Medical CenterBrick, [email protected] Disclosure:Nothing to Disclose
Speaker:Seth Eisenberg, RN, ASN, OCN®
Professional Practice Coordinator, Infusion ServicesSeattle Cancer Care AllianceSeattle, [email protected] Disclosure:Nothing to Disclose
Objectives:At the end of this session, participants will be able to:1. Identify pathophysiologic mechanisms responsible for
an infusion reaction.2. Evaluate outcomes of a time-sensitive nurse-driven
protocol for hypersensitivity and anaphylaxis to chemo-therapy/biotherapy.
Content Outline: I. Pathophysiology/etiology of an infusion reaction
A. Hypersensitivity/anaphylaxis immune responsesB. Cytokine release syndrome
1. Chemotherapy/biotherapy associated with high risk for infusion reaction
2. Comprehensive nursing risk assessmenta. Prophylaxis, premedication (anitipyretics,
antihistimines, steroids)b. Therapeutic action of epinephrine in ana-
phylaxis II. Time-sensitive nursing management of infusion reaction
A. Failure mode effect analysisB. The development of an evidence-based nurse-driv-
en policy and procedure1. Inclusion of CTCEA grading criteria to guide
nursing interventions2. Collaboration of pharmacy, physicians, and
nursinga. Implementation of policy and proceduresb. Evaluation of the outcomes
Bibliography:Abraham, S.N., & St. John, A.L. (2010). Mast cell-orchestrated
immunity to pathogens. [Research Support, N.I.H., Extramu-ral, Review]. Nature Reviews. Immunology, 10(6), 440–452. doi:10.1038/nri2782
Baldo, B.A. (2013). Adverse events to monoclonal antibodies used for cancer therapy: Focus on hypersensitivity responses. [Re-view]. Oncoimmunology, 2(10), e26333. doi:10.4161/onci.26333
Cancer Therapy Evaluation Program, Common Terminology Cri-teria for Adverse Events, Version 3.0, DCTD, NCI, NIH, DHHS March 31, 2003 (http://ctep.cancer.gov), Publish Date: August 9, 2006.
Carroll, M.V., & Sim, R.B. (2011). Complement in health and dis-ease. [Review]. Advanced Drug Delivery Reviews, 63(12), 965–975. doi:10.1016/j.addr.2011.06.005
Common Terminology Criteria for Adverse Events, version 4.0, June 2010, National Institutes of Health, National Cancer Institute, http://evs.nci.nih.gov/ftp1/CTCAE/CTCAE_4.03_2010-06-14_QuickReference_5x7.pdf
Eisenberg, S. (2012). Biologic therapy. [Review]. Journal of Infu-sion Nursing: The Official Publication of the Infusion Nurses Soci-ety, 35(5), 301–313. doi:10.1097/NAN.0b013e31826579aa
George, T.J., Jr., Laplant, K.D., Walden, E.O., Davis, A.B., Riggs, C.E., Close, J.L., et al. (2010). Managing cetuximab hyper-sensitivity-infusion reactions: Incidence, risk factors, preven-tion, and retreatment. The Journal of Supportive Oncology, 8(2), 72–77.
Session • 10:15–11:45 am • Room 304 A
Hypersensitivity Infusion Reaction Management: A Time-Sensitive Solution to a Common Problem

2 Oncology Nursing Society 39th Annual Congress May 1–4, 2014
Friday, May 2
_______________________________________________________________________ _______________________________________________________________________ _______________________________________________________________________ _______________________________________________________________________ _______________________________________________________________________ _______________________________________________________________________ _______________________________________________________________________ _______________________________________________________________________ _______________________________________________________________________ _______________________________________________________________________ _______________________________________________________________________ _______________________________________________________________________ _______________________________________________________________________ _______________________________________________________________________ _______________________________________________________________________ _______________________________________________________________________ _______________________________________________________________________
Kanji, S., & Chant, C. (2010). Allergic and hypersensitivity reac-tions in the intensive care unit. [Review]. Critical Care Medicine, 38(6 Suppl), S162–168. doi:10.1097/CCM.0b013e3181de0c99
Kuhrik, N.S., Kuhrik, M., Rimkus, C.F., Tecu, N.J., & Woodhouse, J.A. (2008). Using human simulation in the oncology clinical practice setting. Journal of Continuing Education in Nursing, 39, 345–355.
Lexi-Comp OnlineTM , Lexi-Drugs OnlineTM , Hudson, Ohio: Lexi-Comp, Inc.; February 20, 2011.
Lieberman, P., Nicklas, A.R, et al. (2010). The diagnosis and man-agement of anaphylaxis practice parameter: 2010 update. J Al-lergy Clin Immunol, 126, 477–480
Loos, W.J., Szebeni, J., ten Tije, A.J., Verweij, J., van Zomeren, D.M., Chung, K.N., et al. (2002). Preclinical evaluation of alternative pharmaceutical delivery vehicles for paclitaxel. [In Vitro]. Anti-Cancer Drugs, 13(7), 767–775.
Markman, M., Zanotti, K., Peterson, G., Kulp, B., Webster, K., & Belinson, J. (2003). Expanded experience with an intradermal skin test to predict for the presence or absence of carboplatin hypersensitivity. Journal of Clinical Cncology : Official Journal of the American Society of Clinical Oncology, 21(24), 4611–4614. doi:10.1200/JCO.2003.05.53
Muehlbauer, P.M., Parr, M.B., & Perkins, A.K. (2013). Using sim-ulation to assess chemotherapy competency. Clinical Journal of Oncology Nursing, 17(4), 392–396.
Pichler, W.J. (2006). Adverse side-effects to biological agents. [Research Support, Non-U.S. Gov’t].
Pichler, W.J., Adam, J., Daubner, B., Gentinetta, T., Keller, M., & Yerly, D. (2010). Drug hypersensitivity reactions: Pathomechanism and clinical symptoms. [Review]. The Medi-cal Clinics of North America, 94(4), 645–664, xv. doi:10.1016/j.mcna.2010.04.003
Polovich, M., Whitford, J., & Olsen. (Eds.). (2009). Chemotherapy and biotherapy guidelines and recommendations for practice (3rd ed.). Pittsburgh, PA: Oncology Nursing Society.
Sampson, H.A., Munoz-Furlong, A., Campbell, R.L., et al. (2006). Second symposium on the definition and management of anaphylaxis: Summary report-Second National Institute of Allergy and Infectious Disease/Food Allergy and Anaphylaxis Network symposium. J Allergy Clin Immunol, 117, 391. Copy-right © 2006 The American Academy of Allergy, Asthma, and Immunology.
Simmons, R.E, Ardusso, L.R.F, et al. (2011). World Allergy Orga-nization anaphylaxis guidelines: Summary. World Allergy Orga-nization Journal, 2(3), 13–36
Su, W. M., & Juestel, M.J. (2010). Direct teaching of thinking skills using clinical simulation. Nurse Educator, 35, 197–204.
Szebeni, J. (2005). Complement activation-related pseudoallergy: A new class of drug-induced acute immune toxicity. [Review]. Toxicology, 216(2-3), 106–121. doi:10.1016/j.tox.2005.07.023
Szebeni, J., & Moghimi, S.M. (2009). Liposome triggering of in-nate immune responses: A perspective on benefits and adverse reactions. [Research Support, Non-U.S. Gov’t].
Szebeni, J., Muggia, F., Gabizon, A., & Barenholz, Y. (2011). Acti-vation of complement by therapeutic liposomes and other lipid excipient-based therapeutic products: Prediction and preven-tion. Advanced Drug Delivery Reviews, 63.
Vogel, W.H. (2010). Infusion reactions: Diagnosis, assessment, and management. Clinical Journal of Oncology Nursing, 14(2), E10-E21. doi10.1188//10.CJON.E10-E21
Wang, H., Wang, H.S., & Liu, Z.P. (2011). Agents that induce pseudo-allergic reaction. Drug Discoveries & Therapeutics, 5(5), 211–219.
Weiszhar, Z., Czucz, J., Revesz, C., Rosivall, L., Szebeni, J., & Rozsnyay, Z. (2012). Complement activation by polyethoxyl-ated pharmaceutical surfactants: Cremophor-EL, Tween-80 and Tween-20. [Research Support, Non-U.S. Gov’t]. European Journal of Pharmaceutical Sciences: Official Journal of the Euro-pean Federation for Pharmaceutical Sciences, 45(4), 492–498. doi:10.1016/j.ejps.2011.09.016

3Oncology Nursing Society 39th Annual Congress May 1–4, 2014
Friday, May 24/17/2014
1
1
Non‐Immune(Innate)
Mast Cells
Basophils
Complement
Cytokines
Immune(Adaptive)
T‐Cells
B‐Cells
Antibodies
CARPA Immune MediatedExposure Prior exposure not required Prior exposure usually requiredSubsequent therapy
Reaction decreases or absent with subsequent doses
Reactions worsen withsubsequent doses
Resolution Reactions can resolve with minimal or no treatment
Reactions do not resolve withouttreatment
Re‐challenge Mild reactions can be re‐challenged
Mild reactions should not be re‐challenged
Frequency Relatively common Relatively rare
2Szebeni, J. (2005). Toxocology, 216
•More than 30 proteins that can recognize and bind to foreign molecules
• Complement Activation releases other proteins and enzymes which enhance inflammatory processes
• Once activated, complement proteins coat foreign substances and allows them to be more visible to macrophages and mast cells
• Releases anaphylatoxins which stimulate an inflammatory response
3Carroll, M. & Sim, R. (2011). Advanced Drug Delivery 63; Szebeni, J. (2005), Toxocology.; Moghimi, S. et al. (2011). Advanced Drug Delivery, 65
• Are considered “first responders” to a stimuli • Can live for up to a year• Do not circulate Found throughout the body, (high concentrations in epithelial and mucosal tissues) and are specialized in each location
• Complement (e.g., C3a, C4a, C5a)• Cytokines (IL‐1β, IL‐3, IL‐6, IL‐9, IL‐10, IL‐11, GMCSF)• IgE and IgG• Neuropeptides (e.g., substance P)
4Ibid
Adhesion molecules (allows non‐specific attachment to foreign molecules)
Protease Granules Trypase (Generates complement C3a, enhances respiratory effects of histamine, and recruits inflammatory cells)
Chymase (Converts angiotensin I to angiotensin II, enhances histamine, and stimulates IL‐I β production
Additional granules: Carboxypeptidase Cathepsin G
Heparin
Histamine
5Hogan, A. & Schwartz, L. (1997), METHODS: A Companion to Methods in Enzymology, 13; Abraham, S. & St. John, A. (2010); Welle, M. (1997). Journal of Leukocyte Biology, 61.
Degranulation occurs within seconds to minutes,although not all substances are released at once
•Vasoactive mediators and cytokinesProstaglandins (e.g., PGD2)
Leukotrienes (LTC4, LTD4, LTE4)
Cox2
IL 3, IL‐4, IL‐5, IL6, IL‐8, SCF, TNFα
Lipid‐derived Mediators (from arachidonic acid)
6Abraham, S., & St. John, A. (2010); Hogan, A. & Schwartz, L. (1997); Ono, E., et al (2008). Clinical and Experimental Allergy, 39,
4 Oncology Nursing Society 39th Annual Congress May 1–4, 2014
Friday, May 24/17/2014
2
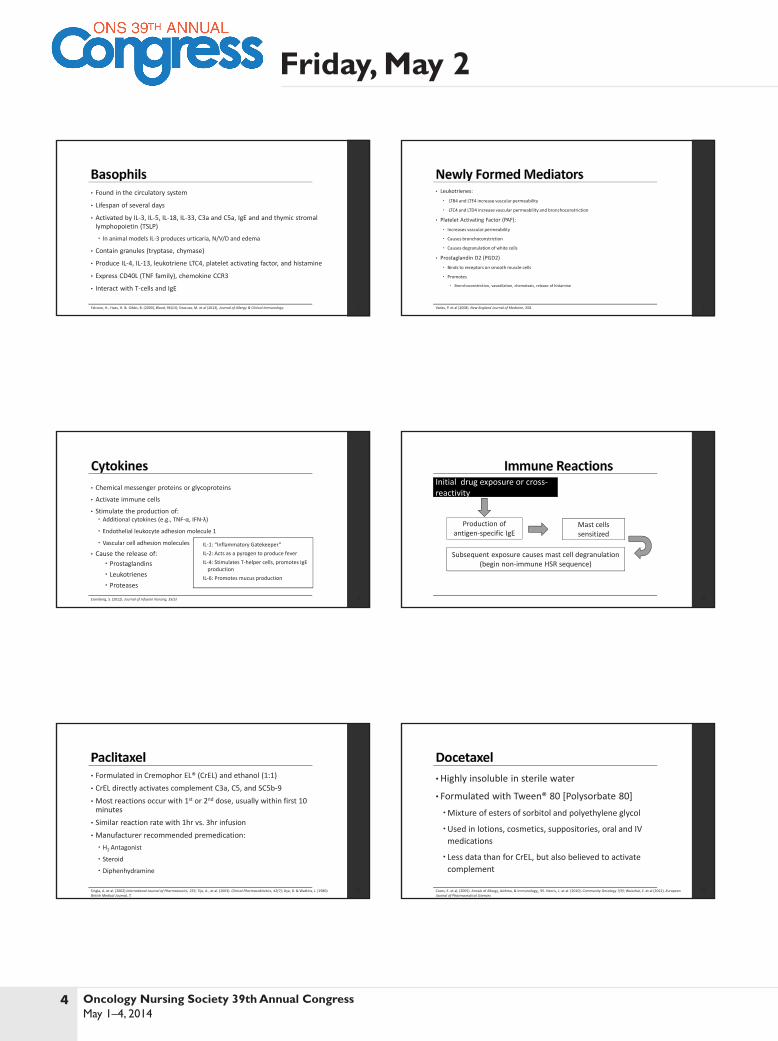
• Found in the circulatory system
• Lifespan of several days
• Activated by IL‐3, IL‐5, IL‐18, IL‐33, C3a and C5a, IgE and and thymic stromal lymphopoietin (TSLP)
In animal models IL‐3 produces urticaria, N/V/D and edema
• Contain granules (tryptase, chymase)
• Produce IL‐4, IL‐13, leukotriene LTC4, platelet activating factor, and histamine
• Express CD40L (TNF family), chemokine CCR3
• Interact with T‐cells and IgE
7Falcone, H., Haas, H. & Gibbs, B. (2000), Blood, 96(13); Siracusa, M. et al (2013), Journal of Allergy & Clinical Immunology.
• Leukotrienes:
LTB4 and LTE4 increase vascular permeability
LTC4 and LTD4 increase vascular permeability and bronchoconstriction
• Platelet Activating Factor (PAF):
Increases vascular permeability
Causes bronchoconstriction
Causes degranulation of white cells
• Prostaglandin D2 (PGD2)
Binds to receptors on smooth muscle cells
Promotes
Bronchoconstriction, vasodilation, chemotaxis, release of histamine
8Vadas, P. et al (2008). New England Journal of Medicine, 358.
• Chemical messenger proteins or glycoproteins
• Activate immune cells
• Stimulate the production of: Additional cytokines (e.g., TNF‐α, IFN‐λ)
Endothelial leukocyte adhesion molecule 1
Vascular cell adhesion molecules
• Cause the release of: Prostaglandins Leukotrienes Proteases
9Eisenberg, S. (2012). Journal of Infusion Nursing, 35(5)
IL‐1: “Inflammatory Gatekeeper”IL‐2: Acts as a pyrogen to produce feverIL‐4: Stimulates T‐helper cells, promotes IgEproduction
IL‐6: Promotes mucus production
10
Initial drug exposure or cross‐reactivity
Mast cells sensitized
Subsequent exposure causes mast cell degranulation (begin non‐immune HSR sequence)
Production of antigen‐specific IgE
• Formulated in Cremophor EL® (CrEL) and ethanol (1:1)• CrEL directly activates complement C3a, C5, and SC5b‐9• Most reactions occur with 1st or 2nd dose, usually within first 10 minutes
• Similar reaction rate with 1hr vs. 3hr infusion• Manufacturer recommended premedication: H2 Antagonist
Steroid
Diphenhydramine
11Singla, A. et al. (2002) International Journal of Pharmaceutics, 235; Tije, A., et al. (2003). Clinical Pharmacokinetics, 42(7); Dye, D. & Watkins, J. (1980). British Medical Journal, 7.
•Highly insoluble in sterile water
• Formulated with Tween® 80 [Polysorbate 80]Mixture of esters of sorbitol and polyethylene glycol
Used in lotions, cosmetics, suppositories, oral and IV medications
Less data than for CrEL, but also believed to activate complement
12Coors, E. et al, (2005). Annals of Allergy, Asthma, & Immunology;, 95. Norris, L. et al. (2010). Community Oncology 7(9); Weiszhár, Z. et al (2012). European Journal of Pharmaceutical Sciences
5Oncology Nursing Society 39th Annual Congress May 1–4, 2014
Friday, May 24/17/2014
3
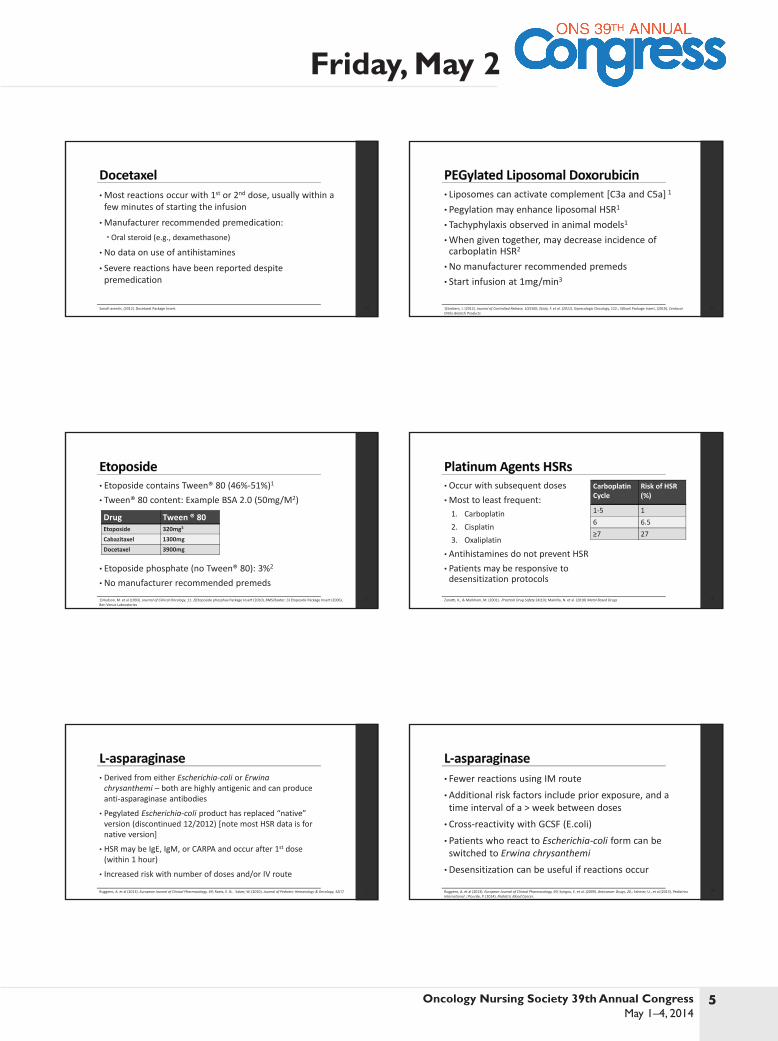
•Most reactions occur with 1st or 2nd dose, usually within a few minutes of starting the infusion
•Manufacturer recommended premedication:Oral steroid (e.g., dexamethasone)
• No data on use of antihistamines
• Severe reactions have been reported despite premedication
13Sanofi‐aventis, (2012). Docetaxel Package Insert.
• Liposomes can activate complement [C3a and C5a] 1
• Pegylation may enhance liposomal HSR1
• Tachyphylaxis observed in animal models1
•When given together, may decrease incidence of carboplatin HSR2
•No manufacturer recommended premeds• Start infusion at 1mg/min3
141)Szebeni, J. (2012). Journal of Controlled Release, 10(160); 2)Joly, F. et al. (2011). Gynecologic Oncology, 122.; 3)Doxil Package Insert, (2010), Centocor Ortho Biotech Products
• Etoposide contains Tween® 80 (46%‐51%)1
• Tween® 80 content: Example BSA 2.0 (50mg/M2)
• Etoposide phosphate (no Tween® 80): 3%2
• No manufacturer recommended premeds151)Hudson, M. et al (1993). Journal of Clinical Oncology, 11. 2)Etoposide phosphae Package Insert (2010), BMS/Baxter; 3) Etoposide Package Insert (2006),
Ben Venue Laboratories
Drug Tween ® 80Etoposide 320mg3
Cabazitaxel 1300mgDocetaxel 3900mg
• Occur with subsequent doses•Most to least frequent:1. Carboplatin2. Cisplatin3. Oxaliplatin
• Antihistamines do not prevent HSR • Patients may be responsive to desensitization protocols
16Zanotti, K., & Markham, M. (2001). Practical Drug Safety 24(10); Makrilla, N. et al. (2010) Metal Based Drugs
Carboplatin Cycle
Risk of HSR (%)
1‐5 16 6.5≥7 27
• Derived from either Escherichia‐coli or Erwina chrysanthemi – both are highly antigenic and can produce anti‐asparaginase antibodies
• Pegylated Escherichia‐coli product has replaced “native” version (discontinued 12/2012) [note most HSR data is for native version]
• HSR may be IgE, IgM, or CARPA and occur after 1st dose (within 1 hour)
• Increased risk with number of doses and/or IV route
17Ruggiero, A. et al (2013). European Journal of Clinical Pharmacology, 69; Raetz, E. & . Salzer, W. (2010). Journal of Pediatric Hematology & Oncology, 32(7)
• Fewer reactions using IM route•Additional risk factors include prior exposure, and a time interval of a > week between doses• Cross‐reactivity with GCSF (E.coli)• Patients who react to Escherichia‐coli form can be switched to Erwina chrysanthemi•Desensitization can be useful if reactions occur
18Ruggiero, A. et al (2013). European Journal of Clinical Pharmacology, 69; Syrigou, E. et al. (2009). Anticancer Drugs, 20.; Sahiner, U., et al (2013). Pediatrics International ; Plourde, P. (2014). Pediatric Blood Cancer.

6 Oncology Nursing Society 39th Annual Congress May 1–4, 2014
Friday, May 24/17/2014
4
• Interaction of Fab portion with the antigen target results in release of TNF‐α and IL‐61
• Sensitization to non‐human proteins can HSR risk2
• Antibody development to murine portion (HAMA) typically results in clearance of the mAb, rendering the therapy ineffective1
• Although less common, fully human mAbs can also elicit antibodies (HAHA)3
• Commonly caused by cytokine mechanisms (non‐immune)• Less commonly caused by Type I‐IV “immune” (pre‐existing or subsequently developed antibodies)
191) Baldo, B. (I2013) Oncoimmunology, 2(10); Chung, C. (2009). Oncology, 23(2S). 2) Calogiuri, G. et al. (2008), Current Pharmaceutical Design, 14; 3) Cheifetz, A. & Mayer, L. (2005), The Mount Sinai Journal of Medicine, 72(4)
• Variable domain targets CD20 antigen on B cells• Constant domain recruits immune cells resulting in complement‐dependent cytotoxicity (CDC) and antibody‐dependent cell mediated cytotoxicity (ADCC)
• Severe reactions common with 1st infusion, occurring 30‐120 minutes after initiating
• Serum IL‐6 and TNF‐α levels peak at 90 minutes1
• HSR severity is related to lymphocyte count1
• Manufacturer recommends premedication with acetaminophen and antihistamine (add steroid for RA)
20Rituxan Package Insert (2013). Genentech, San Francisco, CA.
• 1st dose:
Titrated, starting at 50mg/hr
• Subsequent doses:
Titrated, starting at 100mg/hr OR
Accelerated 90 minute rate for NHL: (20% of dose over 30 minutes, then remainder over 60)
21Rituxan Package Insert (2013). Genentech, San Francisco, CA.; Lang, D., et al. (2011). International Journal of Nursing Practice, 17.
• Chimeric mAb (from mouse plasmacytoma)
• Anti‐epidermal growth factor receptor (EGFR) that mediates antibody‐dependent cellular cytotoxicity (ADCC)
• Reactions can be IgE and/or cytokine mediated
• Manufacturer recommends premedication with H1 antagonist (for first dose)
• 90% of “severe” reactions occur with 1st dose, despite premedication
• Premedication with antihistamines and steroid may not prevent HSR
• Higher percentage of 1st dose HSRs in south and southeastern US
22Erbitux Package Insert (2013), Imclone, Branchburg, NJ.
• Pre‐existing cross‐linked IgE antibodies for galactose‐α‐1,3‐galactose are associated with significantly worse HSRs (particularly 1st dose)
23Chung, C. et al. (2008) New England Journal of Medicine, March 13
Chung et al study (n=75)33% (25) Had HSR92% (17) Antibody positive17% (8) Antibody negative
•HSRs can be non‐immune or immune mediated•Mast cells, complement and cytokines are involved• Reactions can be due to: The diluent (e.g., paclitaxel)Direct antibody formation (e.g., carboplatin) Secondary cytokine release (e.g., rituximab)Components of murine protein (e.g., cetuximab)
• Premedication will not always prevent an HSR
24

7Oncology Nursing Society 39th Annual Congress May 1–4, 2014
Friday, May 24/17/2014
5
Failure Mode Effect Analysis (FMEA)
• Ongoing quality improvement process employed to examine processes to determine points of potential failure and what their effect would be – before any error actually happens.
• A proactive risk management tool used to look more carefully and systematically at vulnerable areas or processes.
• Shared Governance: Chemotherapy Council• Goal to Improve Chemotherapy Administration Safety
– Nurses indicated a learning need for further instruction on how to manage hypersensitivity
– Research was needed to establish the most evidenced based practice for IV and oral chemotherapy administration.
FMEA Prevention Action Plan
• Pharmacy team – Developed medication alerts– Reminded pharmacy and nursing to pre-medicate for hypersensitivity
• Immediate Nursing Education– Underlying pathophysiology of an infusion reaction– Review of anaphylaxis prophylaxis– “Premeds as per protocol” NOT acceptable as an order– Comprehensive Nursing Risk Assessment– Management of Cytokine Release Syndrome (CRS)
Nursing Education
• Assessment of Current Knowledge• Prompted the development of a system-wide educational plan.• During the process of determining which algorithm to employ, we
discovered nurses working in the inpatient and outpatient oncology setting had the general knowledge of emergency management of hypersensitivity infusion reactions, but not the ability to apply immediate pharmacological interventions.
Literature Review: Revealing a Solution
• Early recognition and treatment with Epinephrine to prevent progression to life threatening respiratory and/or cardiovascular event including shock.
• Even mild systemic reactions are best treated immediately with epinephrine, as this appears to prevent progression to more severe symptoms more effectively.
• “There are NO absolute contraindications to epinephrine use in anaphylaxis!• “Reluctance to administer epinephrine due to fear of adverse cardiac effects should be
countered by the awareness that the heart is a target organ in anaphylaxis”.• “The risk of death due to inadequately treated anaphylaxis usually outweighs other
concerns”.
(Simons, Camargo, 2012).
Development of a Nurse Driven Policy
• Analyzed the literature to decide upon the most common criteria for managing adverse effects.
• Planned to implement a nurse-driven protocol which permitted the administration of epinephrine based on clinical judgment and established guidelines using the CTCAE Criteria.
Common Terminology Criteria for Adverse Events (CTCAE)
• Descriptive terminology which can be utilized for adverse Event (AE) reporting• Broken down into categories with a broad classification of AEs based on
anatomy and/or pathophysiology• Within each category, AEs are listed accompanied by their descriptions of
severity (Grade). – Grade 1 Mild AE – Grade 2 Moderate AE – Grade 3 Severe AE – Grade 4 Life-threatening or disabling AE
http://evs.nci.nih.gov/ftp1/CTCAE/CTCAE_4.03_2010-06-14_QuickReference_8.5x11.pdf

8 Oncology Nursing Society 39th Annual Congress May 1–4, 2014
Friday, May 24/17/2014
6
CTCAE Grading to Guide Intervention
Grade 1 Signs and Symptoms• Transient flushing• Rash • Mild itching• Mild anxiety• Mild disorientationInterventions
– Closely monitor patient – No infusion interruption necessary
CTCAE Grading to Guide Intervention
Grade 2 Signs and Symptoms• Fever• Rash• Arthralgia• Noisy breathing, but causing no respiratory distress• Shortness of breath with minimal exertion• Intense itching, or moderate disorientation
Interventions– Stop chemotherapy biotherapy infusion immediately and disconnect chemotherapy/ biotherapy line to
avoid further administration of drug– Call physician and treat as ordered
CTCAE Grading to Guide Intervention
Grade 3 Signs and Symptoms• Severe arthralgia• Extensive rash• Symptomatic bronchospasm with or without urticaria• Hypotension• Angioedema• Shortness of breath with stridor• Decrease in oxygen saturation• Respiratory distress at rest• Rash covering 30% of the body with intense or widespread itching• Severe disorientation, or severe hallucinations
CTCAE Grading to Guide Intervention
• Grade 3 Interventions • Call Rapid Response Team (RRT) • Initiate Hypersensitivity and Anaphylaxis Standing Order for Chemotherapy and
Biotherapy which include administration of IM epinephrine.• Grade 4 Signs and Symptoms• Severe cardiac or respiratory compromise requiring life threatening urgent
intervention such as ventilator support, intubation, tracheostomy or intubation• Interventions• Call Code• Document administration of Epinephrine and ADE in electronic tracking system
Hypersensitivity and Anaphylaxis Standing Orders for Chemotherapy and Biologic Therapy in Oncology:
• Stop chemotherapy/biotherapy infusion immediately.• Disconnect chemotherapy/biotherapy line to avoid further administration of drug.• Assess airway, breathing, circulation, and cognitive function.• For grade 1 or 2 signs or symptoms, call physician and treat as ordered. • For grade 3 or 4 signs and symptoms (bronchospasm, with or without urticaria; allergy-related
edema/angioedema; hypotension, altered mental status):– Call Rapid Response Team.
• Initiate Hypersensitivity and Anaphylaxis Standing Order for Chemotherapy and Biotherapy. FOLLOW ALGORITHM DISPLAYED ON NEXT SLIDE.
Assess Airway
• Not obstructed → Continue close monitoring.• Obstructed → Administer Epinephrine^a
0.3mg IM auto-injector.Establish airway.^Vomiting patients need to be placed on the side.Obtain vital signs every 2-3 min until patient is stable.CPR if pulse is absent
a. IM Epinephrine (1mg/mL 1:1000 preparation): Give epinephrine 0.3 mg intramuscularly, preferably in the mid-anterolateral thigh; can repeat every 5 minutes as needed (may give sooner than 5 min if clinically warranted).
b. B, Oxygen therapy at the first sign of compromise; administer 100% O2 via non-rebreather mask accompanied by continuous oxygen saturation monitoring.
Algorithm adapted with permission from Vogel, W.H. (2010) Infusion reactions: Diagnosis, assessment, and management; Clinical Journal Oncology Nursing; 14 (2), E10–E21
9Oncology Nursing Society 39th Annual Congress May 1–4, 2014
Friday, May 24/17/2014
7
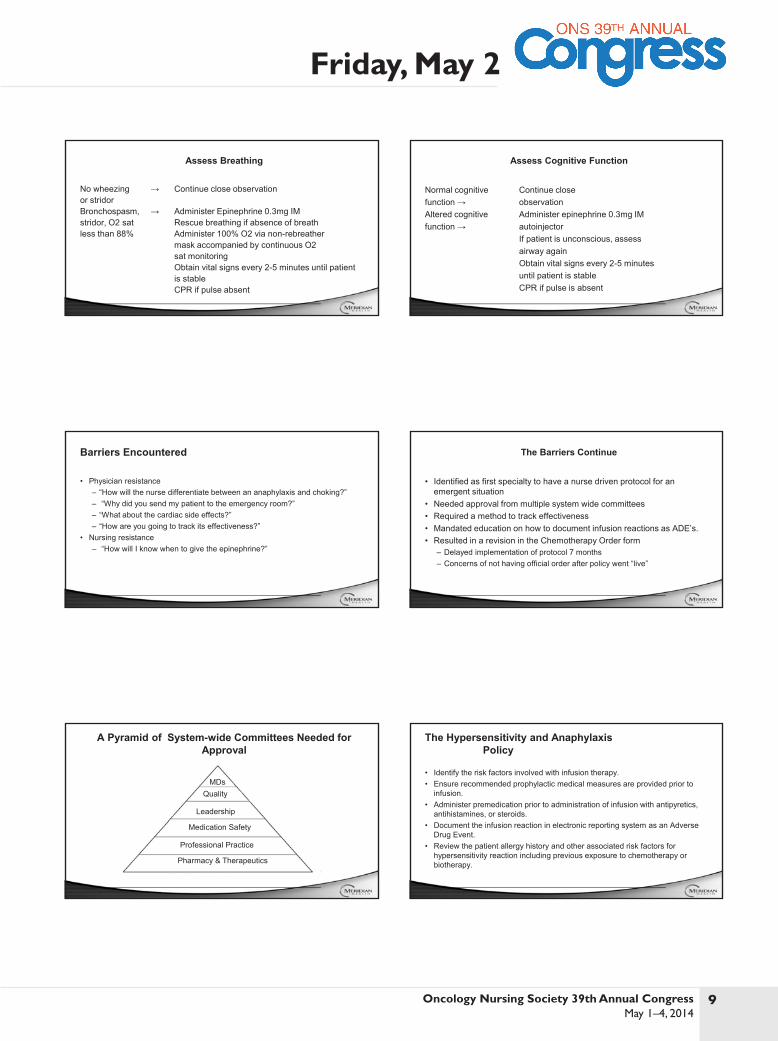
Assess Breathing
No wheezing → Continue close observationor stridorBronchospasm, → Administer Epinephrine 0.3mg IMstridor, O2 sat Rescue breathing if absence of breathless than 88% Administer 100% O2 via non-rebreather
mask accompanied by continuous O2sat monitoringObtain vital signs every 2-5 minutes until patientis stableCPR if pulse absent
Assess Cognitive Function
Normal cognitive Continue closefunction → observationAltered cognitive Administer epinephrine 0.3mg IMfunction → autoinjector
If patient is unconscious, assessairway againObtain vital signs every 2-5 minutesuntil patient is stableCPR if pulse is absent
Barriers Encountered
• Physician resistance – “How will the nurse differentiate between an anaphylaxis and choking?”– “Why did you send my patient to the emergency room?”– “What about the cardiac side effects?”– “How are you going to track its effectiveness?”
• Nursing resistance – “How will I know when to give the epinephrine?”
The Barriers Continue
• Identified as first specialty to have a nurse driven protocol for an emergent situation
• Needed approval from multiple system wide committees• Required a method to track effectiveness• Mandated education on how to document infusion reactions as ADE’s.• Resulted in a revision in the Chemotherapy Order form
– Delayed implementation of protocol 7 months– Concerns of not having official order after policy went “live”
A Pyramid of System-wide Committees Needed for Approval
Professional Practice
Pharmacy & Therapeutics
Medication Safety
Leadership
QualityMDs
The Hypersensitivity and Anaphylaxis Policy
• Identify the risk factors involved with infusion therapy.• Ensure recommended prophylactic medical measures are provided prior to
infusion.• Administer premedication prior to administration of infusion with antipyretics,
antihistamines, or steroids.• Document the infusion reaction in electronic reporting system as an Adverse
Drug Event.• Review the patient allergy history and other associated risk factors for
hypersensitivity reaction including previous exposure to chemotherapy or biotherapy.

10 Oncology Nursing Society 39th Annual Congress May 1–4, 2014
Friday, May 24/17/2014
8
The Hypersensitivity and Anaphylaxis Policy
• Obtain and record baseline vital signs including baseline pulse oximetry.. • Ensure that emergency equipment is readily available at bedside (inpatient
setting) or chair (outpatient setting).• Instruct patient on hypersensitivity symptoms and to report symptom.• Document education in the medical records.
Implementing the Protocol
• System-wide approval for implementation on the oncology units.• Pharmacy consulted about supplying the epinephrine to the medication
dispensing system at each campus.– In the form of a unit dose– Eliminated the potential for an inaccurate amount of drug to be administered during
a time-sensitive situation
Educating the Staff
• Significant change in practice.• Through the use of simulation.• Time sensitive outcomes may be met when all the standard components of
simulation are included, such as preparation, pre-brief, the simulation, and debrief (Muehlbauer, Parr, & Perkins, 2013).
Evaluating Patient Data and Outcomes 2012
• Clinical manifestations of Grade 3 hypersensitivity develops
• Infusion Stopped. Alerted Rapid Response Team.
• Administered diphendramine, corticosteroids
• Patient monitored in the Emergency Room until stable, or admitted for telemetry observation
• ED visit $1300.00• ICU Bed Charge $1200.00
– (Average daily cost $12,000 with care)
• Intubation Charge $3343.00• Average cost of wasting
Chemotherapy drugs $100.00-$30,000
Evaluating Patient Data and Outcomes 2013
• Clinical manifestations of Grade 3 Hypersensitivity develops.• Alert Rapid Response Team, follow protocol• Administer Epinephrine 0.3mg. IM Auto-injector• Cost of Epinephrine Auto-Injector $150.00• 8 patients treated successfully with protocol• 6 of 8 patients able to be discharged after completing chemotherapy• 10 patients eligible for protocol did not receive epinephrine• 2 of 8 patients were admitted for 23 hour observation
The Journey Continues
• Not all RNs comfortable with algorithm• Physician reluctance persists• Developing a Fact Sheet handout for patient education and management of
delayed or recurrent reactions at home• Working with physician colleagues in ordering Epinephrine Auto Injector post
discharge for delayed reaction• Continuing to monitor outcomes and coach and mentor physicians & nurses to
achieve compliance with the algorithm

11Oncology Nursing Society 39th Annual Congress May 1–4, 2014
Friday, May 2
Hypersensitivity and anaphylaxis nursing protocol for chemotherapy and biologics in inpatient and outpatient oncology:
1. Grade 1 Hypersensitivity closely monitor patient.
Signs and Symptoms include: as transient flushing or rash, mild itching, mild anxiety, or mild disorientation. No infusion interruption necessary.
2. Grade 2. Stop chemotherapy/biotherapy infusion immediately and Disconnect chemotherapy /biotherapy line to avoid further administration of drug. Call physician and treat as ordered.
Signs and Symptoms include as fever, rash, arthralgia, noisy breathing but causing no respiratory distress, shortness of breath with minimal exertion, intense itching, or moderate disorientation.
3. Grade 3 signs and symptoms severe arthralgia, extensive rash, symptomatic bronchospasm with or without urticaria, hypotension, allergy related edema (angioedema), shortness of breath with stridor, decrease in oxygen saturation, respiratory distress at rest, rash covering 30% of the body with intense or widespread itching, sever disorientation, or severe hallucinations ;
a. Call Rapid Response Team.
b. Initiate Hypersensitivity and Anaphylaxis Standing Order for Chemotherapy and Biotherapy which include administration of IM epinephrine. ( see protocol)
4. Grade 4 Call Code. Signs and Symptoms include: severe cardiac or respiratory compromise requiring life threatening urgent intervention such as ventilator support, intubation, tracheostomy or intubation.
5. Document Administration of Epinephrine on RRT form and Document ADR in Carelink

12 Oncology Nursing Society 39th Annual Congress May 1–4, 2014
Friday, May 2
a. IM Epinephrine (1 mg/mL 1:1000 preparation): Give epinephrine 0.3 mg intramuscularly, preferably in the mid-anterolateral thigh; can repeat every 5 minutes as needed (may give sooner than 5 min if clinically warranted).
b. Oxygen - therapy at the first sign of compromise; administer 100% O2 via non-rebreather mask accompanied by continuous oxygen saturation monitoring
Note: “Infusion Reactions: Diagnosis, Assessment, and Management” by W. Vogel, 2010, Clinical Journal Oncology Nursing, 14 (2), p. E18. Copyright 2010 by Oncology Nursing Society. Adapted with permission.
If signs and symptoms of a hypersensitivity reaction are present, stop infusion and maintain vascular access.
Assess Airway Assess Breathing Assess Circulation Assess Cognitive Function
Obstructed: -Administer epinephrine^a 0.3mg IM autoinjector -Establish Airway
Not obstructed: -Continue close observation
Tilt head, lift chin to open airway
Vomiting patients may need to beplaced on side
Bronchospasms stridor-oxygen saturation <88%Administerepinephrine^
Rescue breathing if absence of breath occurs
Administer oxygen therapy^b
No wheezing or stridor:-Continue closeobservation
Hypotensive (SBP < 90mmHg or > 30% ↓from baseline) or tachycardic: -Administer epinephrine^a 0.3mg IM autoinjector
Normotensive :-Continue closeobservation
Rapid infusion of 1 L normal saline wide open rate
Place patient in recumbent position and elevate lower extremity
Obtain vital signs every 2-5 minutes until patient is stable
Altered cognitive function: -Administerepinephrine^a 0.3mg IM autoinjector
If patient is unconscious, assess airway again
Normal cognitive function:-Continue closeobservation
Obtain vital signs every 2-5 minutes until patient is stable
Obtain vital signs every 2-5 minutes until patient is stable
Cardiopulmonary resuscitation if pulse is absent
Obtain vital signs every 2-5 minutes until patient is stable
Cardiopulmonary resuscitation if pulse is absent
Cardiopulmonary resuscitation if pulse is absent
Cardiopulmonary resuscitation if pulse is absent
References: Common Terminology Criteria for Adverse Events, version 4.0, June 2010, National Institutes of Health, National Cancer Institute, http://evs.nci.nih.gov/ftp1/CTCAE/CTCAE_4.03_2010-06-14_QuickReference_5x7.pdf. Lexi-Comp OnlineTM , Lexi-Drugs OnlineTM , Hudson, Ohio: Lexi-Comp, Inc.; February 20, 2011. Lieberman, P, Nicklas, A. R, et al. The diagnosis and management of anaphylaxis practice parameter: 2010 Update. J Allergy Clin Immunol. 2010; 126:477-80 Polovich, M, Whitford, J. and Olsen (EDs) (2009). Chemotherapy and biotherapy guidelines and recommendations for practice (3rd Ed). Oncology Nursing Society, Pittsburg, PA, Oncology Publishing Division. Sampson HA, Munoz-Furlong A, Campbell RL, et al. Second symposium on the definition and management of anaphylaxis: summary report-Second National Institute of Allergy and Infectious Disease/Food Allergy and Anaphylaxis Network symposium. J Allergy Clin Immunol 2006; 117:391. Copyright © 2006 The American Academy of Allergy, Asthma, and Immunology. Simmons, R. E, Ardusso, L.R.F, et al. World Allergy Organization anaphylaxis guidelines: Summary. World Allergy Organization Journal 2011; 2(3):13-36 Vogel Wendy. H (2010). Infusion reactions: diagnosis, assessment, and management. Clinical Journal of Oncology Nursing, doi 10.1188//10.CJON.E10-E21





























