Embed Size (px)
Citation preview

[CANCER RESEARCH 50. 5904-5910. September 15. 1990]
Serum Tumor Marker Half-Life during Chemotherapy Allows Early Prediction ofComplete Response and Survival in Nonseminomatous Germ Cell Tumors'
Guy C. Toner, Nancy L. Geller, Claire Tan, Jerome Nisselbaum, and George J. Bosl2
Genitourinary Oncology Sen'ice [C. C. T., G. J. B.], Division of Soliti Tumor Oncology, Department of Medicine, Division of Biostalistics [N. L. G., C. T.], Departmentoj Epidemiology and Biostatistics, and Department of Clinical Chemistry ¡J.N.], Memorial Sloan-Keltering Cancer Center, New York, New York 10021 and Departmentof Medicine ¡G.C. T., G. J. B.¡,Cornell University Medical College, Ithaca, New York 14850
ABSTRACr
The prognostic value and therapeutic utility of monitoring the decayof a-fetoprotein (AFP) and human chorionic gonadotropin (HCG) afterchemotherapy for nonseminomatous germ cell tumors was assessed.Patients treated on successive front line chemotherapy protocols atMemorial Hospital between 1979 and 1988 were studied. Marker valuestaken within the first 90 days of treatment were reviewed for the 198patients who had initially abnormal values and serial measurements atMemorial Hospital. Since markers frequently increased in an unpredictable fashion in the first week after chemotherapy, prechemotherapyvalues would be inaccurate for assessment of subsequent half-life. Therefore, the first two values measured >7 days after the start of treatmentwere used for all calculations of half-life. Among 38 patients who hadthe two successive AFP measurements elevated, those who later achieveda complete response (CR) had a median AFP half-life of 6.1 days (n =20), whereas those not achieving CR had a median AFP half-life of 13.3days (P = 0.02). Among 37 patients with the two successive HCG valueselevated, those who later achieved CR had a median HCG half-life of 4.2days (n = 10), whereas those not achieving CR had a median HCG half-life of 18.4 days (P = 0.04). Forty-two patients who had an AFP half-life >7 days or an HCG half-life >3 days had significantly shorter overallsurvival (median, 8 months) than the other 156 patients (median notreached) (P < 0.0001). These 42 patients also achieved CR in lowerproportion (29%) than the other 156 patients (89%) (P < 0.0001). Coxregression identified prolonged marker half-life as the most significantindependent predictor of survival. Lack of appropriate decay of serumtumor markers can identify patients unlikely to achieve CR or prolongedsurvival and thus can be used to select patients during treatment whomay benefit from an early change to more aggressive therapy.
INTRODUCTION
Identification of the 20-30% of patients with advancedNSGCT' who are destined to fail conventional therapy (and
ultimately die from malignancy) remains an important objectiveof clinical research. Most studies have concentrated on pretreatment clinical characteristics as prognostic variables. Pretreatment features have been used to predict the probability ofattaining CR (1) and relapsing after CR (2), demonstrate potential prognostic features within risk strata (3), and provideevidence of stage migration (4). Despite their use, as many as10% of "good risk" patients fail to achieve CR in current trials
(5, 6). Almost all patients with refractory disease subsequentlydie (7). A proportion of "poor risk" patients will achieve long-
term survival with conventional therapy (3, 8, 9), making theuse of very intensive initial therapy inappropriate. Clarificationof new clinical characteristics permitting more accurate recognition of patients likely to fail therapy is therefore valuable.
Received 3/19/90: accepted 6/14/90.The costs of publication of this article were defrayed in pan by the payment
of page charges. This article must therefore be hereby marked advertisement inaccordance with 18 U.S.C. Section 1734 solely to indicate this fact.
1Supported in part by N1H Grants CA 05826 and CM 57732 and the BrianPiccolo Cancer Research Fund.
! To whom requests for reprints should be addressed, at Memorial Sloan-Kettering Cancer Center. 1275 York Avenue, New York, NY 10021.
3The abbreviations used are: NSGCT. nonseminomatous germ cell tumor;AFP. u-fetoprotcin: CR, complete response; d.f., degrees of freedom; HCG.human chorionic gonadotropin; LDH. láclatedchydrogenase.
The introduction of novel treatment strategies may allow animprovement in survival for patients with a poor prognosis,particularly if introduced early during management.
The management of NSGCT has been distinguished not onlyby the frequency with which patients can be cured but also bythe availability of accurate serum tumor markers. AFP andHCG are glycoproteins that are present at elevated levels in theserum of most patients with metastatic NSGCT (10, 11). Thesemarkers aid in management by reducing errors in diagnosis andstaging, providing prognostic information at the time of presentation of patients with metastatic disease and furnishing anaccurate and objective means of monitoring response to therapyand detecting recurrent disease (10, 12-14).
Each marker is elevated in approximately 50-70% of patientsand 70-85% of patients with disseminated disease will haveone or both markers elevated at presentation (10, 11). Thekinetics of both markers have been studied after completesurgical resection of disease and the biological half-life was 5-7 days for AFP and 18-48 h for HCG (15). This is the same asthe half-life in normal subjects (16, 17). While clearance fromthe serum after chemotherapy has been less well studied, onegroup reported mean half-lives of 5.7 days for AFP and 3.1days for HCG (18).
In the setting of advanced disease, elevated pretreatmentmarker values have been associated with a worse prognosis (1,19). Therefore, a higher proportion of patients likely to failconventional therapy will have elevated marker levels prior tothe commencement of chemotherapy. Studies of markers afterchemotherapy have identified an increase immediately afterinitiation of treatment in some patients (18, 20). This has beenpostulated to be due to release of these substances after tumorcell death.
The aim of this study was to analyze the prognostic value ofmonitoring the decay of AFP and HCG after the commencement of chemotherapy. Prior studies of prognostic featureshave emphasized pretreatment clinical characteristics. Markerregression is a posttreatment characteristic which may be ableto identify early treatment failure (21) regardless of pretreatment risk stratification.
PATIENTS AND METHODS
All patients with NSGCT treated on Memorial Hospital front-linechemotherapy protocols designed for good risk and poor risk patientsbetween 1979 and 1988 who had elevated AFP or HCG levels wereconsidered. To assure comparability of laboratory measurements, patients who did not have an adequate number of serial measurements atMemorial Hospital were excluded. The numbers of patients studiedand inclusion criteria are detailed in Table 1. All patients receivedchemotherapy regimens containing high doses of cisplatin (>100 mg/nr/cycle) or carboplatin. The details of treatment and response havebeen described previously (5. 8, 22. 23).
Complete resolution of all biochemical and radiographie abnormalities or the resection of only teratoma or necrotic debris after chemotherapy was classified as CR to chemotherapy. Complete resection ofresidual malignancy after chemotherapy was classified as CR to chemo-
5904
Research. on September 26, 2020. © 1990 American Association for Cancercancerres.aacrjournals.org Downloaded from

HALF-LIFE OF SERUM TUMOR MARKER DECLINE IN NSGCT
Table 1 Criteria for inclusion in the analysis
Patients Criteria
341
266
231
198°
176'
Evaluable patients with NSGCT entered inprospective clinical trials 1979-1988
AFP > 15 ng/ml or HCG > 2 ng/ml (i.e.,75 patients had normal pretreatmentAFP and HCG)
Marker levels monitored at MemorialHospital
>2 marker values assayed between days 7and 90 of treatment
orInitial marker value after day 7 was normal
>2 marker values assayed between days 7and 90 of treatment
" Patients included in analysis.* Patients included in Cox regression analysis.
therapy plus surgery. Any response less than CR was considered to bean incomplete response. Patients were classified as good or poor riskaccording to their predicted probability of achieving CR calculated bya logistic regression model using pretreatment HCG, LDH, and numberof metastatic sites (1). Patients with an NSGCT and either a predictedprobability of CR <0.50 or an extragonadal primary site were considered poor risk. Patients with an NSGCT arising in the testis and apredicted probability of CR >0.50 were considered good risk.
HCG was assayed using a modification of the highly sensitive andspecific double antibody radioimmunoassay procedure of Vaitukaitis etal. (24). The standard HCG for this assay was obtained from NationalInstitute of Arthritis, Metabolism and Digestive Diseases (standardCRII7). The antiserum against the purified /i subunit of HCG wasprepared in rabbits. A value of <2 ng/ml was considered normal. Twoassays were used to quantitate serum AFP. Prior to June 1984, aradioimmunoassay was used with reagents kindly provided by WampoleLaboratories, a division of Carter Wallace. A specific antiserum topurified AFP from pooled human fetal serum was prepared in rabbits.After June 1984, a sandwich enzyme immunoassay method from Hy-britech (San Diego, CA) was used. Both the capture and signal antibodies were monoclonal. Both methods provide equivalent quantitativeresults, but the enzyme immunoassay has an improved sensitivity of 15ng/ml. All values for AFP >15 ng/ml were considered abnormal.
The first 10 values for HCG and AFP recorded in the clinicalchemistry department at Memorial Hospital were collected for 231patients. Marker values were plotted semilogarithmically, and the half-life of marker decline was calculated between each point using acomputer spreadsheet program. Marker values frequently increased inan unpredictable manner during the first 7 days after the initiation ofchemotherapy. This is consistent with release from treated, dying tumor(18). Therefore, no pretreatment values or values measured during thefirst week of therapy were used for assessment of marker half-life. Thefirst two values measured more than 7 days after the start of treatmentwere used for all calculations of the half-life of marker decline. In orderto limit the time span under study, only values measured in the first 90days after the start of chemotherapy were considered.
Patients were classified as having prolonged marker half-life if thefirst 2 values after the seventh day of treatment were abnormal and thehalf-life for AFP was >7 days or for HCG was >3 days. Marker declinewas deemed to be satisfactory if the half-life of AFP was <7 days orHCG was <3 days or if either of the first 2 values after day 7 wasnormal. Patients who had elevations of both markers were consideredto have prolonged marker half-life if either HCG or AFP half-life wasprolonged.
Hypotheses concerning differences in proportions were tested usingx2 and Fisher's exact tests and those concerning differences in medians
of continuous data using the Wilcoxon test (25). Survival distributionswere estimated by the method of Kaplan and Meier (26), and univariatecomparisons were made using the log rank test (27).
Two analyses were performed. In the first analysis of 198 patients,survival was calculated from the time the patient was deemed to havesatisfactory markers or a prolonged half-life. This was at the date ofthe first marker value after day 7 if this value was normal or at the dateof the second marker value otherwise. Comparisons of survival in this
analysis were made with the log rank test (27). In the second analysisutilizing Cox regression (28), survival was always calculated from thedate of the second marker value after day 7. This analysis included 176patients, since the remaining 22 patients did not have a second markervalue prior to day 90. If both AFP and HCG were elevated, survivalwas calculated from the latter of the 2 dates. Survival was alwayscalculated from a date within 90 days from the start of chemotherapy.
Cox regression analysis (28) was used to assess whether prolongedmarker half-life was a prognostic factor for survival. A variable, NORMALIZE, was defined to indicate whether markers were decaying atthe proper rate or not. NORMALIZE took the value 1 if marker half-life was prolonged and 0 if markers were decreasing satisfactorily, asdefined above. Along with known prognostic variables (see below), weconsidered whether NORMALIZE was an independent prognosticvariable for survival.
Cox regression considers the logarithm (base e) of the relative riskof death, log [\(t)/\0(t)}, to be a linear function of A-prognostic variablesZ¡,where i = 1,2 k:
AO(')(A)
In Equation A, \(t) is the hazard function (relative rate of death) attime t, A0(f)is a baseline hazard function (corresponding to Z, = Z2 =. . . = Zk = 0), Z, is a value of the /th prognostic variable, and thecoefficients a¡are estimated from the data. The variables considered aspotential prognostic factors were NORMALIZE and the known prognostic factors (1, 19, 29): pretreatment HCG [or log (HCG + 1)],pretreatment LDH [or log (LDH + 1)], the total number of metastaticsites (coded as 0 for elevated markers only, 1 for one site of metastasis,or 2 for two or more sites of metastasis), AFP [or log (AFP + I)], siteof primary tumor, and a variable termed RISK (coded as 0 for goodrisk patients and 1 for poor risk patients). RISK took the value 1 if theprobability of CR (1) was calculated to be <0.5 or the primary site wasextragonadal. Otherwise, RISK took the value 0. Procedures of theStatistical Analysis System were used for all computation (30).
RESULTS
Patient Characteristics. AFP baseline values were elevated in151 patients, HCG values in 134 patients, and both markers in87 patients. Patient characteristics for the 198 patients studiedare shown in Table 2.
Since marker values increased unpredictably in the first 7days after the initiation of chemotherapy, only values measuredafter the seventh day of treatment were used to calculate thehalf-life of marker decay. For patients with 2 elevated markervalues after the seventh day, the half-life between the first 2values was calculated and results are shown in Table 3. BothAFP and HCG half-lives were significantly prolonged in thosepatients not achieving a CR.
Half-life values were calculated in this way; patients whoseAFP half-life was >7 days or whose HCG half-life was >3 dayshad significantly shorter survival and achieved CR less frequently. The cutoff values of 7 days and 3 days were chosenprospectively, based on the expected biological half-lives. Eventhough the median half-life of HCG decline in patients achieving CR with chemotherapy was 3.5 days, a cutoff of 3 days wasused, because only 2 patients had a half-life for HCG between3 and 4 days and neither achieved a prolonged CR.
Response Proportions and Relapse. Proportions of CR according to prolonged or satisfactory decline of serum markersare shown in Table 4. If prolonged half-life of either AFP orHCG were considered separately, each was capable of identifying a group of patients less likely to achieve CR. If patientswith a prolonged half-life of either marker were included in asingle group, a larger, more clinically useful group of 42 patientswas identified. Only 12 of these 42 patients (29%) achieved a
5905
Research. on September 26, 2020. © 1990 American Association for Cancercancerres.aacrjournals.org Downloaded from

HALF-LIFE OF SERUM TUMOR MARKER DECLINE IN NSGCT
Table 2 Characteristics of 198 patients with elevated AFP or HCG
PatientsAge
(yr)MedianRangePrimary
siteTestisMediastinumRetroperitoneumNo.
of metastaticsites0Markers
elevatedonly1>2Chemotherapy
regimenVAB-6*-rVAB-6
vi.EPfVAB-6+EP*CBE'AFPElevatedMedian
elevated value(ng/ml)Range(ng/ml)HCGElevatedMedian
elevated value(ng/ml)Range(ng/ml)LDH°ElevatedMedian
elevated value(units/liter)Range(units/liter)All2613-54173(87%)14
(7%)11(6%)18(9%)61
(31%)117(60%)75642930151
(76%)25616-139.600134(68%)642.2-44.500141
(72%)493239-16.629Good
risk2813-54118(100%)0018(16%)51
(44%)47(40%)54640091
(77%)16518-10.40071
(60%)192.5-3.80063
(54%)347239-1.440Poor
risk2615-5155
(69%)14(17%)11
(14%)0
(0%)10(12%)70
(88%)210293060
(75%)45316-139.60063
(79%)1.4922.2-44.50078
(98%)771240-16.629
°Adequale data available in 196 patients.* Ref. 22.' Ref. 5." Ref. 23.' Ref. 8.' VAB-6. cyclophosphamide + vinslastine + bleomycin + dactinomycin + cisplatin: EP. etoposide + cisplatin; CBE. carboplatin + bleomycin + etoposide.
Table 3 Correlation of response and marker half-life calculated between the first
and second marker values measured after day 7 of chemotherapy, for 66 patientsin whom both the first and second values were abnormal
Table 4 Correlation of response with prolonged marker half-life
ResponseAFP
half-lifeNo.ofpatientsMedian
(davs)Range(days)HCG
half-lifeNo.ofpatientsMedian
(days)Range(days)CR-chemo"175.93.3-35.783.52.5-62.4AIICR206.13.3-Inc104.22.5-62.4IR1813.33.2-Inc2718.30.9-lncP
value*0.0170.037
°CR-chemo. complete response to chemotherapy alone: All CR, all completeresponses, including CR-chemo; IR. incomplete response: Inc. increasing markervalue, half-life not valid.
* Wilcoxon test comparing all CR with incomplete responses.
CR, compared with 139 of 156 patients (89%) with satisfactorymarker values (x2 = 63.67, l d.f., P < 0.0001).
Twelve patients who had prolonged marker half-life achieveda CR. Residual viable malignancy was resected after chemotherapy more frequently in this group of patients. Four of the12 patients (33%) had residual malignancy resected comparedto 13 of 139 patients (9%) who were found to have satisfactorymarker decay (Fisher's exact test, P = 0.03). Relapse also
occurred much more frequently; 8 of the 12 patients (67%) withabnormal marker half-life relapsed after CR compared to 18 of139 patients (13%) with satisfactory markers (Fisher's exact
test, P = 0.0001). The 13% relapse rate is slightly higher thanexpected for an overall group of patients with germ cell tumors,but this was probably due to the worse prognosis of patientswho were selected for this analysis because they had an NSGCTand elevated markers.
Proportions of CR are shown in Table 4 for MemorialHospital good and poor risk patient groups (1). Prolongedmarker half-life identified patients within each group whoachieved a CR less frequently.
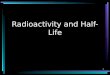
Survival Analysis. Survival for all patients is shown in Fig. 1.
CR-chemo . All CR IR
Response N % N % N % P value*
All patientsAFP or HCG half-life prolonged (N = 42) 819 12293071Satisfactory AFP and HCG (A/= 156) 126 81 139 89 17 11 <0.0001
AFP half-life >7 days (N = 16)Satisfactory AFP (N = 129)HCG half-life >3 days (N = 29)Satisfactory HCG (A"= 102)
Good risk patientsAFP or HCG half-life prolonged (N = 9)Satisfactory AFP and HCG (N = 109)
3 19 5 31 11 6999 77 111 86 18 14 <0.0001
5 17 7 24 22 7682 80 91 89 11 11 <0.0001
111 4 44 5 5697 89 106 97 3 3 <0.0001
Poor risk patientsAFP or HCG half-life prolonged (N =Satisfactory AFP and HCG (N = 47)
33) 7 2129 62
8 24 25 7633 70 14 30 0.0001
Cox regression patientsAFP or HCG half-life prolonged (N = 42)Satisfactory AFP and HCG (N = 134)
8 19 12 29 30 71105 78 118 88 16 12 <0.0001
°CR-chemo, complete response to chemotherapy alone; All CR. all completeresponses, including CR-chemo: IR, incomplete response.
X2test.
Patients with prolonged marker half-life had dramaticallyshorter survival compared to the other patients (log rank x2 =
66.4, l d.f., P < 0.0001). Only 6 patients with prolonged markerhalf-life were alive >24 months from the start of treatment.Three of these 6 patients had viable malignancy resected afterchemotherapy; 1 additional patient relapsed 13 months afterstarting chemotherapy and has remained alive with disease at35+ months. Only 2 patients with prolonged marker half-lifeachieved a CR with chemotherapy alone and remained aliveand free of disease >24 months (32+ and 69+ months) afterstarting treatment.
Prolonged half-life of both AFP and HCG could be usedindividually to identify a group of patients with shorter survival
5906
Research. on September 26, 2020. © 1990 American Association for Cancercancerres.aacrjournals.org Downloaded from

100*
80%
60«
oo.oi
40*
20*
0%
HALF-LIFE OF SERUM Tl'MOR MARKIÕR!>!•:<LINK IN NSGCT
A 100*
Satisfactory Markers(156 pts, 129 olive)
Prolonged Marker Half-Life
(42 pts, 12 alive)
Years
Fig. 1. Survival for 198 patients according to abnormal or satisfactory decayof AFP and HCG after initiation of chemotherapy (log rank test, x2 = 66.37, 1d.f.,/>< 0.0001).
/\ 100* r
en 80*
coco
60*
40*
20*
0%
Satisfactory AFP(129 pts, 103 alive)
Prolonged AFP Half-Life
(16 pts, 5 alive)
246
Years
8 10
100* -
80*
60*
•f 40*
oo¿ 20*
O*
Satisfactory HCG(102 pts, 85 alive)
I Prolonged HCG Half-Life'"•"' j (29 pts, 7 alive)
10
Years
Fig. 2. A. survival for 145 patients with initially elevated AFP according toabnormal or satisfactory decayof AFP after initiation of chemotherapy (log ranktest, x! = 21.74, l d.f., P < 0.0001). fi, survival for 131 patients with initiallyelevatedHCG according lo abnormal or satisfactory decayof HCG after initiationof chemotherapy (log rank test. x2 = 64.02.1 d.f.. P < 0.0001).
(Fig. 2). Fourteen patients had prolonged half-life of one markerbut satisfactory values for the other. Seven of these 14 patients(50%) achieved a CR, but only 4 remained continuously aliveand free of disease after therapy. Thus, patients who had onlyone abnormal marker, while the other was satisfactory, had apoor prognosis. Therefore, analyses of marker half-lives of bothHCG and AFP should be considered complementary. In addition, prolonged marker half-life identified a group of patientswith shorter survival within both the good risk and poor risk(Fig. 3) patient subgroups.
Seventy-five patients with NSGCT, who were otherwise ex-
80*
n 60*(/I
oà 20*
Satisfactory Markers
(109 pts. 100 alive)
Prolonged Marker Half-Life
(9 pts, 3 alive)
2 4 6
Years
8 10
B 100* r
80* -
60*
oa.o
Q_
40*
20*
Satisfactory Markers(47 pts, 29 alive)
Prolonged Marker Half —Life
(33 pts, 9 alive)
4 6
Years
10
Fig. 3. A. survival for 118 good risk patients according to abnormal orsatisfactory decayof AFP and HCG after initiation of chemotherapy (log ranktest, x2= 31.67, l d.f., P < 0.000 1). B, survival for 80 poor risk patients accordingto abnormal or satisfactory decay of AFP and HCG after initiation of chemotherapy (log rank test, x2 = 10.57. I d.f.. P = 0.0012).
eluded from this analysis because they had normal pretreatmentAFP and HCG values (Table 1), had longer survival comparedto all of the 266 patients (Table 1) with initial marker elevation(log rank x2 —4.5, P = 0.03). This supports the notion that
patients selected for inclusion in the analysis because they hadinitially elevated AFP or HCG values had a worse prognosis.
Cox regression analysis was used to derive independent prognostic variables for survival. In this analysis, survival was alwaysmeasured from the date of the second marker value after theseventh day of treatment. Twenty-two of the 198 patientsstudied were excluded from the Cox regression. All of thesepatients had a normal value for the first marker assay after theseventh day but did not have a second marker assay before the90th day. CR proportions for the 176 patients included in theCox regression are shown in Table 4.
The Cox model yielded NORMALIZE as the most significant prognostic factor among the variables considered andRISK as a second independent prognostic factor. None of theother variables entered the Cox model, and these 2 prognosticvariables did not have a significant interaction. The final modelwas
logMt) = 1.29 NORMALIZE + 1.41 RISK (B)
This model has an overall x2 (score statistic) of 76.15, 2 d.f.,
and a P< 0.0001.The model yields four prognostic groups of patients. Kaplan-Meier plots of survival for these groups are displayed in Fig. 4.The survival curves are very similar to those for the original
5907
Research. on September 26, 2020. © 1990 American Association for Cancercancerres.aacrjournals.org Downloaded from

HALF-LIFE OF SERUM TUMOR MARKER DECLINE IN NSGCT
100%
80*
n 6056c/1
~ 40*oo.oCL 20*
Good Markers & Risk
Good Markers, Poor Risk
Bad Markers, Good Risk
Bad Markers, Poor Risk
4 6
Years
10
Fig. 4. Survival for 176 patients included in the Cox regression analysisaccording to abnormal or satisfactory decay of AFP and HCG and good or poorrisk patient group. Includes 92 good risk patients with satisfactory markers (85alive). 42 poor risk patients with satisfactory markers (25 alive), 9 good riskpatients with prolonged AFP or HCG half-lives (3 alive), and 33 poor risk patientswith prolonged AFP or HCG half-lives (9 alive).
198 patients as shown in Fig. 3. For patients in the same RISKgroup (good or poor risk), the relative risk of dying for thosewith prolonged marker half-life compared to those with satisfactory markers was 3.63. This means that there was >3-fold
risk of death for those whose elevated markers did not declineappropriately. For patients in the same NORMALIZE group,the risk of dying for poor risk patients relative to good riskpatients was 4.10. This implies approximately a 4-fold risk ofdeath for poor risk patients compared to good risk patients.
After inspection of the coefficients in Equation B, the hypothesis that the two coefficients were equal was generated.This hypothesis was tested and confirmed. This meant that aCox model could be generated with a single independent variable taking the value 0 for good risk patients with markersnormalizing appropriately, the value 1 for good risk patientswith markers not normalizing appropriately or poor risk patients with markers normalizing appropriately, and the value 2for poor risk patients whose markers were not normalizingappropriately. There was then a relative risk of dying of 3.82for one of these groups relative to the adjacent better one. Thismodel is not reported in more detail because it was suggestedonly by the results of the first Cox regression analysis and lacksclinical applicability.
Similar results were found when Cox regression was undertaken separately in the good and poor risk patient subgroups.These analyses were limited by small numbers of patients.NORMALIZE was the only variable to enter the model forpoor risk patients and NORMALIZE and LDH were the onlyvariables for good risk patients.
DISCUSSION
This study shows that assessment of the decline of serumtumor markers after the initiation of chemotherapy is a powerful prognostic tool. The identification and utilization of prognostic factors has made possible the rational development oftreatment programs for germ cell tumors. Clinical trials forpatients with a good prognosis have demonstrated that fewercycles of treatment (6, 31) and fewer cytotoxic agents (5) canbe used without jeopardizing response proportions and survivaloutlook. The aims of trials for patients with a poor prognosishave been to increase the frequency of CR without intolerabletoxicity (23, 32). Although disagreement exists over the weight
of individual prognostic variables, decision algorithms usedinternationally to classify good and poor risk patients havegenerally recognized baseline tumor marker levels and bulk ofdisease as the most important predictive factors for response(19). These pretreatment prognostic factors have been used todecide what treatment program should be recommended for anindividual patient.
Exploration of possible prognostic features evident only afterthe initiation of chemotherapy has been limited. Almost allcurrent treatment programs await assessment of response afterthe completion of 3 or 4 cycles of chemotherapy before decisions regarding further treatment are considered. Assessmentof response frequently involves surgical exploration and resection of residual disease in the retroperitoneum and chest.
Several studies of fewer patients have suggested that a prolonged half-life of marker decline may have prognostic implications (15, 18, 21, 33). The therapeutic usefulness of thisinformation has, however, remained ill defined. The data in thisreport demonstrate that prolonged decay of markers comparedto expected biological half-life is a powerful predictor of failureto respond and poor survival. Patients in whom a prolongedmarker half-life was identified had a CR proportion of 31% andmost patients achieving CR subsequently relapsed. Only 5 of42 patients (12%) remained alive and free of disease >24months from the start of treatment. It is possible that some ofthe long-term survivors were salvaged from chemotherapy-resistant malignancy by complete resection of residual malignancy after chemotherapy. Abnormal marker decline identifieda poor prognosis subset of patients within both good and poorrisk patient groups.
Cox regression analysis selected prolonged marker decay asthe most significant predictor of limited survival. The onlyother independent prognostic factor for survival was good orpoor risk patient category. The risk categorization was in turnderived from the primary site (all extragonadal tumors considered poor risk) and a mathematical formula which uses pretreatment HCG, LDH, and the number of sites of metastatic diseaseto predict the chance of achieving a CR. No other potentialprognostic factor entered the model. This result indicates theimportance of prolonged marker half-life as a predictor of poorsurvival. It also confirms that our existing risk stratification,which was derived from a logistic regression analysis of response, also predicts survival more powerfully than individualpretreatment variables and independently of the analysis ofmarker half-life. This substantiates the hypothesis that post-treatment clinical variables can complement pretreatment riskstratification.
Can the prognostic implications of marker half-life analysisbe used to the patients' advantage? Once a treatment program
has been initiated, why not wait until response is assessed atthe completion of therapy? While these questions require evaluation in prospective studies, there are strong theoretical reasons to suggest that an early change of chemotherapy regimenmay be of benefit to those patients identified with a poorprognosis. The median time to classification of patients according to marker half-life in this study was 33 days after the startof treatment. This is much briefer than the 3-6 months usuallyrequired to assess response. An early change to a more intensiveregimen may avoid the problem of cumulative toxicities fromchemotherapy and the potential development of chemotherapyresistance. For example, good risk patients may benefit from achange to a more intensive chemotherapy combination containing ifosfamide. Poor risk patients with abnormal marker half-life may benefit from a change to therapy such as high dose
5908
Research. on September 26, 2020. © 1990 American Association for Cancercancerres.aacrjournals.org Downloaded from

HALF-LIFE OF SERIAI TIMOR MARKER DECLINE IN NS(.< I
chemotherapy with autologous stem cell support. The latteroption is currently the subject of prospective evaluation in aclinical trial at Memorial Hospital.
Previous reports have suggested the value of monitoringtumor marker half-life (15, 18, 21, 33-35). The majority ofthese studies have compared the marker levels prior to chemotherapy with the level at the time of the second cycle oftreatment. Some studies have found this to be useful (21). whileothers have not (34). The likely reason for this discrepancy, andthe potential flaw in this methodology, is that such an analysisfails to consider an initial increase in serum tumor markerlevels which may occur at the initiation of chemotherapy. Thisphenomenon has been well described and is unpredictable, inthat some patients have no increase while others may haveelevations up to 600% of baseline (18, 20). This elevation makescomparisons of half-lives calculated from marker values measured prior to and immediately after treatment unreliable. Inthis study, the first marker value considered was always takenafter the seventh day of treatment. In our experience, the peakin marker levels occurred prior to this time. In addition, somepublished reports have monitored only HCG (21 ). This analysisdemonstrates that both HCG and AFP can be useful individually and when used together provide increased accuracy.
Two criticisms of this study are that all data were collectedretrospectively and that marker values were often measuredinfrequently during initial treatment. Patients treated in thelast 10 years were included and markers were less regularlymeasured a decade ago. We were unable to measure markerhalf-life for each patient using many data points but, instead,restricted the analysis to the potentially less accurate methodof measuring it from 2 points only. Of the 156 patients with"satisfactory markers," 132 were classified by the fact that their
markers had returned to normal values rather than by measurement of the half-life of marker decay. Nonetheless, it is clearthat analysis of marker values after initiation of chemotherapyprovides powerful prognostic information. It is likely that themost accurate method of assessing marker decline would be bymeasurement of multiple elevated values after the first week oftreatment, with measurement of a best fit half-life applied tothe data. This does not require excessively complicated analysis,because the calculations can be easily performed in a numberof currently available personal computer programs. These results have led us to consider the more complex decline in LDH.It is possible that further prognostic information may be discerned from the decline in LDH, particularly in patients withinitially normal AFP and HCG values.
This study demonstrates that prolonged decay of AFP orHCG after chemotherapy identifies patients unlikely to achieveCR or long-term survival. These patients may benefit from anearly change in treatment. We recommend that all patients withNSGCT receiving chemotherapy be monitored with weeklyassays for AFP and HCG until these markers have normalized.Patients enrolled in clinical trials should be prospectively monitored to confirm the significance of prolonged marker half-life.Patients who are not receiving treatment in a clinical trial andwho are found to have an abnormal decay of markers should bereferred to a major treatment center so that a change to moreintensive therapy can be considered.
REFERENCES
1. Bosl. G. J.. Geller. N. L., Cirrincione, C.. Vogelzang, N. J.. Kennedy. B. J..Whitmore. W. F.. Jr., Vugrin. D.. Scher, H.. Nisselbaum. J.. and Golbcy. R.B. Multivariatc analysis of prognostic variables in patients with metastatictesticular cancer. Cancer Res., 43: 3403-3407. 1983.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
Geller, N. L., Bosl. G. J., and Chan, E. Y. Prognostic factors for relapseafter complete response in patients with metastatic germ cell tumors. Cancer(Phila.). 63: 440-445, 1989.Toner, G. C., Lin, S-Y.. Geller. N. L.. Ochoa, M., and Bosl. G. J. Survivaland prognostic features of extragonadal and poor risk nonscminomatousgerm cell tumors. Proc. Am. Assoc. Cancer Res.. 30: 259. 1989.Bosl. G. J., Geller. N. L., and Chan, E. Y. W. Stage migration and theincreasing proportions of complete responders in patients with advancedgerm cell tumors. Cancer Res.. 48: 3524-3527. 1988.Bosl, G. J.. Geller. N. L., Bajorin. D.. Leitner, S. P., Yagoda. A.. Golbcy. R.B.. Scher. H.. Vogelzang. N. J.. Auman, J.. Carey, R., et al. A randomizedtrial of etoposide -t- cisplatin versus vinblastine + bleomycin + cisplatin +cyclophosphamide + dactinomycin in patients with good-prognosis germ celltumors. J. Clin. Oncol.. 6: 1231-1238, 1988.Einhorn, L. H., Williams, S. D.. Loehrer, P. J., Birch, R.. Drasga, R., Omura,G., and Greco, F. A. Evaluation of optimal duration of chemotherapy infavorable-prognosis disseminated germ cell tumors: a Southeastern CancerStudy Group protocol. J. Clin. Oncol., 7: 387-391, 1989.Motzer. R.. Geller. N., Bajorin. D.. Scher. H.. Tan. C.. Hen. H.. Sogani. P..Fair. W.. Morse. M.. Russo. P.. and Bosl, G. Salvage chemotherapy for germcell tumor patients: prior complete response as an important prognosticvariable (Abstract). Proc. Am. Soc. Clin. Oncol.. 9: 141, 1990.Motzer, R. J.. Cooper, K.. Geller, N. L., Pfister, D. G.. Lin, S-Y., Bajorin.D.. Scher. H. !.. Herr. H.. Fair. W.. Morse. M., Sogani. P.. Whitmore. W.,and Bosl. G. J. Carboplatin + etoposide + bleomycin for patients with poorrisk germ cell tumors. Cancer (Phila.). 65: 2465-2470. 1990.Bajorin. D.. Katz. A.. Chan. F.. Geller. N.. Vogelzang. N., and Bosl, G. J.Comparison of criteria for assigning germ cell tumor patients to "good risk"and "poor risk" studies. J. Clin. Oncol.. 6: 786-792. 1988.
Bosl. G. J., Geller, N. L., Cirrincione, C., Nisselbaum, J., Vugrin. D.,Whitmore. W. F.. Jr.. and Golbey. R. B. Serum tumor markers in patientswith metastatic germ cell tumors of the testis: a ten year experience. Am. J.Med.. 75: 29-35. 1983.Lange. P. H.. and Fraley. E. E. Serum alpha-fetoprotein and human chorionicgonadotropin in the treatment of patients with testicular tumors. L'rol. Clin.North. Am.. 4: 393-406. 1977.Bosl. G. J., Lange. P. H.. Fraley. E. E., Goldman. A., Nochomovitz, L. E.,Rosai, J., Waldmann. T. A.. Johnson. K.. and Kennedy. B. J. Humanchorionic gonadotropin and alphafetoprotein in the staging of nonsemino-matous testicular cancer. Cancer (Phila.). 47: 328-332. 1981.Bosl. G. J.. Lange. P. H.. Nochomovitz, L. E., Goldman, A.. Fraley. E. E.,Rosai. J.. Johnson. K.. and Kennedy. B. J. Tumor markers in advancednonseminomatous testicular cancer. Cancer (Phila.). 47: 572-576, 1981.Loehrer. P. J., Sr.. Williams. S. D.. and Einhorn, L. H. Tcsticular cancer:the quest continues. J. Nati. Cancer. Inst., 80: 1373-1382. 1988.Lange. P. H.. Vogelzang. N. J., Goldman. A.. Kennedy. B. J.. and Fraley, E.E. Marker half-life analysis as a prognostic tool in testicular cancer. J. Imi.128: 708-711. 1981.Gillin. D.. and Boesman. M. Serum »-fetoprotein. albumin and vglobulinin the human conceptus. J. Clin. Invest.. 45: 1826-1838. 1966.Wehmann. R. E., and Nisula. B. C. Metabolic and renal clearance rates ofpurified human chorionic gonadotropin. J. C'lin. Invest.. 68: 184-194. 1981.
Vogelzang, N. J.. Lange. P. H.. Goldman. A.. Vessela. R. H.. Fraley. E. E.,and Kennedy. B. J. Acute changes of »-fetoprotein and human chorionicgonadotropin during induction chemotherapy of germ cell tumors. CancerRes.. «.-4855-4861. 1982.Vogelzang, N. J. Prognostic factors in metastatic testicular cancer. Int. J.Andrò!.. IO: 225-237. 1987.Horwich, A., and Peckham, M. J. Transient tumor marker elevation following chemotherapy for germ cell tumors of the testis. Cancer Treat. Rep.. 70:1329-1331, 1986.Picozzi. V. J., Freiha, F. S.. Hannigan, J. F., and Torti, F. M. Prognosticsignificance of a decline in serum human chorionic gonadotropin levels afterinitial chemotherapy for advanced germ-cell carcinoma. Ann. Intern. Med..100: 183-186.1984.Bosl. G. J.. Gluckman. R.. Geller, N. L.. Golbey. R. B.. Whitmore. W. F..Jr.. Herr. H.. Sogani, P., Morse. M., Martini. N., Bains. M.. and Mc-Cormack. P. V'AB-6: an effective chemotherapy regimen for patients withgerm cell tumors. J. Clin. Oncol.. 4: 1493-1499. 1986.Bosl. G. J., Geller, N. L.. Vogelzang, N. J.. Carey. R.. Auman. J.. Whitmore.W. F., Herr, H.. Morse. M., Sogani, P., and Chan, E. Alternating cycles ofetoposide plus cisplatin and VAB-6 in the treatment of poor-risk patientswith germ cell tumors. J. Clin. Oncol., 5: 436-440. 1987.Vaitukaitis. J. L.. Braunstein. G. D., and Ross, G. T. A radioimmunoassaywhich specifically measures human chorionic gonadotropin in the presenceof human leutinizing hormone. Am. J. Obstet. Gynecol.. 113: 751-758,1972.Zar. J. H. Biostatistical Analysis. Englewood Cliffs. NJ: Prentice Hall Inc..1974.Kaplan. E. L.. and Meier. P. Nonparametric estimation from incompleteobservations. J. Am. Slat. Assoc., 53:457-481. 1958.Mantel. N. Evaluation of survival data and two new rank order statisticsarising in its consideration. Cancer Chemother. Rep.. 50: 163-170, 1966.Kalbfleisch. J. D.. and Prentice. R. L. The Statistical Analysis of FailureTime Data. New York: John Wiley & Sons, 1980.Droz, J. P., Kramar. A.. Ghosn. M., Piot, G., Rey, A., Theodore. C., Wibault,P.. Court. B. H.. Perrin. J. L.. Travagli. J. P.. Bellet. D., Caillaud. J. M.,Pico. J. L.. and Hayal. M. Prognostic factors in advanced nonscminomalous
5909
Research. on September 26, 2020. © 1990 American Association for Cancercancerres.aacrjournals.org Downloaded from

HALF-LIFE OF SERUM TUMOR MARKER DECLINE IN NSGCT
lesticular cancer. A multivarialc logistic regression analysis. Cancer (Phila.). chemotherapy regimen in the treatment of poor prognosis nonseminomatous62- 564-568 1988 germ-cell tumors. J. Clin. Oncol., 6: 10.11-1040, 1988.
30. SUGI Supplemental Library User's Guide. 1987 ed.. pp. 269-293. 437-466. -"•Thompson. D. K.. and Haddow. J. E. Serial monitoring of serum alpha-f Mf~. CAS i« i»i„„lasi fetoprotem and chononic gonadotropm in males with germ cell tumors.vary,iNi..jv\.>insiiiuii.ini.., ITO/. .-, /ph'i.\^?.iii^nift'^Qio"7Q
31. Einhorn. L. H.. Williams. S. D.. Trôner. M.. Birch. R., and Greco. F. A. The ,4 Horwjch A' and Peckham. M. J. Serum tumor regression rate following
role of maintenance therapy in disseminated tcsticular cancer. N. Engl. J. chemotherapy for malignant teratoma. Eur. J. Cancer. Clin. Oncol.. 20:Med..J05: 727-731. 1981. 1463-1470. 1984.
32. Ozols. R. F.. Ihde. D. C.. Lineham. W. M.. Jacob. J.. Ostchega. Y.. and 35. Carl. J. Drug-resistance patterns assessed from tumor marker analysis. J.Young. R. C. A randomized trial of standard chemotherapy r a high-dose Nail. Cancer. Ina., SI: 1631-1639. 1989.
5910
Research. on September 26, 2020. © 1990 American Association for Cancercancerres.aacrjournals.org Downloaded from

1990;50:5904-5910. Cancer Res Guy C. Toner, Nancy L. Geller, Claire Tan, et al. Nonseminomatous Germ Cell TumorsEarly Prediction of Complete Response and Survival in Serum Tumor Marker Half-Life during Chemotherapy Allows
Updated version
http://cancerres.aacrjournals.org/content/50/18/5904
Access the most recent version of this article at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cancerres.aacrjournals.org/content/50/18/5904To request permission to re-use all or part of this article, use this link
Research. on September 26, 2020. © 1990 American Association for Cancercancerres.aacrjournals.org Downloaded from