Embed Size (px)
Citation preview

SEROLOGICALSTUDIES ON INFLUENZA DURINGA NINE-MONTHPERIOD1
By SEYMOURS. KALTERAND ORREND. CHAPMAN(WITH THE TECHNICALASSISTANCE OF CATHERINEBURKHART)
(From the Department of Bacteriology and Parasitology, College of Medicine, Syracuse Uni-versity, and the Virus Laboratory, Bureau of Laboratories, Department of Health,
Syracuse, New York)
(Received for publication November 5, 1946)
The anticipated influenza B epidemic material-ized late in November, 1945 and reached its peakduring the month of December. Sporadic caseswere recognized in the United States (1) for aperiod of some months preceding the actual epi-demic. The importance of recognizing this pre-epidemic period is unquestionably a necessity inorder to avail ourselves of the prepared vaccines.It has been demonstrated (2-12) that immuniza-tion against the influenza viruses elicits an anti-body increase and offers protection to the experi-mental inhalation of the virus strains. Francisand coworkers (13) have demonstrated furtherthat vaccination with inactivated influenza virusesTypes A and B offers protection against influenzaB during an epidemic., That this epidemic wasdue to Type B has also been shown by Dalldorfand Rice (14).
It is recognized that other agents are responsiblefor certain cases of bacteria-free pneumonias.Clinically these various types of virus pneumoniaoften resemble each other. It is essential, there-fore, to determine, if possible, the agent responsiblefor the infection. Their differentiation may bemade by isolation of the virus or by serologicalstudies. In many instances, failure to isolate anorganism does not eliminate its possible role ascausative agent. On the other hand, the develop-ment of specific antibodies in convalescent sera isone criterion that is considered to be conclusiveevidence of contact with the specific antigen. Manyagents have been isolated and serological technicsfor their identification have been developed.
These various viral technics available for labo-ratory diagnosis are now routinely employed inmany laboratories. The examination of serumsamples for the presence of antibodies to viruses,as well as those producing a clinical syndrome
1 Aided by a grant from the Hendricks Research Fund.
similar to that produced by virus agents, may bemade by the Hirst test (15) for influenza; coldagglutination (16) or its modification (17), andthe indifferent Streptococcus MG(18) for atypi-cal pneumonia; and the commercial product Ly-granum CF 2 (19 to 23) for members of thepsittacosis group.
The experiments were designed in order (a) toascertain the approximate time of the epidemics'appearance or an indication of the epidemics' ap-proach by pre-epidemic increases in serum anti-bodies, (b) to determine the nature of the epi-demic in this area, (c) to determine the effect ofvaccination, and (d) to determine what antibodytiters may be expected in a group of presumablynormal individuals.
MATERIALS ANDMETHODS
Sera were derived from 2 sources. One group was ob-tained from 52 medical students who were bled each monthfor a period of 9 months from October, 1945 to June, 1946,inclusive. In this group 3 were females and the remainderwere males. Of these, 15 students were given the con-centrated A and B influenza vaccine prepared from chickembryos. Except for 1 member of this group, all re-ceived their vaccinations after their second blood speci-men had been obtained. The lone student was vaccinatedafter his third blood sample had been taken. The 37 othermembers of this group were either members of the navalunit or civilians and were not required to be vaccinated.
A careful record of each student's health was main-tained with histories obtained before the program wasestablished and at each monthly bleeding. By coincidence,the vaccination program and the influenza epidemic wereconcurrent.
Another group of sera were obtained from the uni-versity student infirmary and consisted of 66 acute phasesera and 25 pairs of acute and convalescent phase sera.The donors of these sera were all university students ad-mitted with upper respiratory infections during the
2 (E. R. Squibb & Sons.) This antigen is used only be-cause of its convenience, rather than its specificity. Theuse of a psittacosis antigen would be preferable, but moredifficult to obtain.
420

SEROLOGICALSTUDIES ON INFLUENZA
epidemic period. In all cases, attempts were made to ob-tain a convalescent phase serum sample. Wherever co-operation was lacking, the acute phase sample was placedin the "single serum group" (these are discussed morefully under results). All acute phase sera were takenupon admission to the infirmary and in most cases wereobtained during the first 2 days of illness. The con-valescent sera were obtained 2 to 6 weeks following in-fection. The clinical diagnosis of this group was varied,but all were considered to be respiratory infections. Thenumber of males and females in this group was approxi-mately equal.
All sera were handled in an identical manner. Theblood samples were obtained under sterile conditions andmaintained in the sterile state. Upon receiving the bloodsample, it was allowed to stand at room temperature forseveral hours, then centrifug~ted, and the serum removed.All sera were frozen and stored at - 70° C. until readyto be tested. Prior to the titration of the serum, it wasthawed and sufficient amounts removed and inactivatedat 560 C. These were to be used in the agglutination-inhibition and complement-fixation tests. The cold ag-glutination and the streptococcus agglutination tests weremade immediately following the thawing of the serumsample. All sera from the same individual were treatedat the same time using the same test preparations.
The sera were stored in sterile vials. All titrationswere completed within 24 hours after removal of thesera from the frozen state and the sera were kept at 4° C.when not in actual use.
Cold agglutination: The procedure was essentially thatrecommended by the Commission on Acute RespiratoryDiseases (17). It consisted of adding 0.5 ml. of a 0.2per cent suspension of fresh type 0 cells, obtained from thesame donor throughout, to 0.5 ml. 2-fold serial serumdilutions starting at 1: 5. The tubes were shaken and keptovernight at 40 C. Readings were made on the followingday before the tubes had any opportunity to become warm.The end point consisted of that dilution giving definiteagglutination of the cells. All titers expressed are re-ciprocals of the final dilutions of the serum.
Streptococcus MGNo. 9: 8 From a culture of this or-ganism bacterial suspensions were made and tested in themanner described by Thomas, et al (18). The organismswere washed 3 times in saline and a suspension corre-sponding approximately to a No. 3 McFarland standardwas made. The streptococci were killed by heating at600 C. for 1 hour. To 0.5 ml. serum dilution starting at1: 5, an equal volume of streptococcus suspensions wasadded. This mixture was placed in a 370 C. water bathfor 2 hours, then overnight at 40 C., and then again at370 C. for 2 hours. Following this, the tubes wereshaken and read. The degree of agglutination used as astandard was that of the original workers. The dilutionof serum giving a 1 plus reaction was used as the titer andis expressed as a final dilution.
Agglutination-inhibition test: The procedure used hereis the same as is described by Hirst (15) except that weemployed a 1 per cent chicken red cell suspension as usedby Henle, et al (12). The virus was obtained from theallantoic fluid of 10- to 11-day-old embryos after numerouspassages. The fluid from the embryos was obtained in theusual manner and then pooled. This pool was then titratedand separated into smaller amounts for storage. All viruspools were stored at - 70° C. until needed. When freshvirus was required, the tube was removed at least 1 dayprior to its use, thawed, and allowed to stand at 40 C. Ahemagglutination titration was again made and exactly 4units antigen were used. The pools maintained the sametiter for the entire test period.
Sera were tested for inhibitory substances to the in-fluenza viruses A, B,4 and Swine.5 The PR 8 and Leestrains of influenza A and B were used respectively.Readings were made after 75 minutes at room temperatureand the titers expressed are those giving a 2 plus or betterinhibition of agglutination. A standard red cell sus-pension as well as the degree of clumping was used forcomparison. All sera from the same individual weretitrated against the influenza strains at the same time.The saline and the red cells were dispensed with an auto-matic pipetting machine. To avoid possible mixing ofinfluenza strains, the same person worked with the samestrains throughout the experiment. Each virus strainhad its own glassware. The expressed titers are finaldilutions.
Henle and coworkers (12) discuss the possibility ofcrossing the strains, which, on the basis of Ziegler's andHorsfall's work on interference (24), appears to pre-clude this possibility. However, titrations in immunizedmice demonstrated that our virus strains were pure.
Complement-fixation: All sera were tested for anti-bodies to members of the psittacosis group of viruseswith Lygranum CF. To 0.2 ml. inactivated serum dilu-tions, 0.2 ml. complement (2 units) was added, followedby 0.2 ml. antigen (1 unit). These were placed in a370 C. water bath for 1%hours and then 0.4 ml. sensitizedcells were added to all tubes. These were then further in-cubated for M hour and reading made. The usual anti-complementary and non-specific controls were included inall tests. The titers of sera giving 50 per cent or betterfixation were considered positive and are expressed asinitial dilutions.
Included with all tests, i.e. cold agglutination, strepto-coccus-agglutination, agglutination-inhibition, and theLygranum complement fixation tests, were positive serumcontrols.
RESULTS
PatientsAn increase in admissions to the student in-
firmary became apparent late in November.
4 These two strains were supplied by Dr. Werner3 A culture of. this organism was received from Dr. Henle.
Frank L. Horsfall, Jr, 5 Dr. Gilbert Dalldorf supplied the Swine strain.
421

SEYMOURS. KALTER AND ORREND. CHAPMAN
TABLE I
Incidence of influenza B among students admitted to thestudent infirmary with upper respiratory infections,
November 1945 to February 1946
Total numberMonth To number of acute and Influenza B Incidenceof admissions convalescent
sera tested
per centNov. 4 1 1 4.0Dec. 48 18 17 68.0Jan. 8 5 2 8.0Feb. 6 1 0 0.0
Total 66 25 20 80.0
These admissions increased rapidly during themonth of December, gradually receding duringthe months of January and February. Table Ishows the total number of students admitted intothe student infirmary during this 4-month period 8for acute upper respiratory infections. Of the 66admissions, 25 pairs of acute and convalescentsera were obtained. The greatest number of ad-missions occurred in December with 48 cases.There were 4 cases late in November, 8 in Janu-ary, and 6 in February. Of the paired sera, weobtained 1 in November, 18 in December, 5 inJanuary, and 1 in February. Upon titration forinfluenza B, these were shown to have an inci-dence of 4.0 per cent, 68.0 per cent, 8.0 per cent,and 0.0 per cent for those months respectively.The total of 80.0 per cent shows a 4-fold or betterincrease in antibodies to influenza B..
The sera were divided into 2 groups for con-venience, one group consisting of the paired sera,the other group composed of a single serum sam-ple. The results obtained from the cold agglutina-tion, indifferent streptococcus No. 9 agglutination,complement-fixation (for members of the psitta-cosis group) and agglutination-inhibition (for in-fluenza A, B, and Swine) tests on the first groupare shown in Table II.
Of the 25 paired sera, 3 showed increases in coldagglutinins, whereas 3 showed cold agglutinins butno increases or a drop in titer during convales-cence. Of the 3 with titer increases, patients Nos.58 and 108 were diagnosed clinically as atypicalpneumonia with characteristic pulmonary involve-
8 Because of facilities at the infirmary, this representsonly a small part of the university students. Many wereentered in other hospitals.
ment. Case 96, although showing a rise in coldagglutinins, demonstrated a more significant in-crease in influenza B antibodies. Clinically, thispatient did not have any extensive pulmonaryinvolvement and was considered to be influenza B.Patients 79, 85, and 86 all showed the presenceof cold agglutinins. These titers, because of theirfailure to increase, were considered to be of littlesignificance, and therefore, non-specific in nature.
TABLE II
Titers of acute and convalescent sera obtained from patientsduring epidemic; winter 1945-1946
Cold Strepto- Psitta- InfluenzaSerum agl- coccus
cos -____sno. tiagglu -MG
grutiain no. 9 gop A B Swine
56 AB
58 AB
59 AB
60 AB
66 AB
67 A'B
74 AB
75 AB
72 AB
76 AB
79 AB
83 AB
84 AB
85 AB
86 AB
87 AB
94 AB
96 AB
100 AB
108 AB
111 AB
110 AB
113 AB
114 AB
121 AB
0
0
2040
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
0
201000
0
0
150
15150
0
0
0
0
200
0
0
300
0
0
0
0
0
0
0
0
0
1015000000
20100000
10102040
00
2020101010201510152040401010204020202040
0000
1020201500
00000000000000000000000000000000000000000000000000
8080
32080
160160160160808080804040
160320320320
808080
1604060
160320160320
8080
640640160160640
1,280320640320640320320320640
80808080
320640
320640
80100
1601,9201,920
320480
402,560
805,120
1602,560
16010,240
3202,560
6402,560
3205,120
32010,240
3202,560
64010,240
64010,240
1,2802,560
3205,1201,2802,560
46032016016040
16080
10,240320320640640
60602040
00
806040402020202040404040
1603206406404040
320320
4040
320640320320160320
80808080
9601,2801,2801,280
640320320
60320320160320
422
SEROLOGICALSTUDIES ON INFLUENZA
Sixteen patients demonstrated antibodies to theindifferent streptococcus MGNo. 9. Their titersranged from 10 to 40 without any showing signifi-cant increases. Of the patients showing increasesin cold agglutinins, patients 96 and 108 gave a2-fold rise in streptococcus antibodies. Patient 58,although diagnosed as atypical pneumonia, did nothave any agglutinins for this indifferent strepto-coccus. Many of the patients with influenza B had-low titers for this organism.
In this group, there were no complement fixingantibodies to the members of the psittacosis group.Several, however, were reactive with the normalchick embryo control.
The titers for influenza A and Swine influenzashowed no significant increase although severalhad high antibody levels. When tested against theLee strain of influenza B, 15 patients showed 4-fold or better increases in their convalescent sera.Five patients showed only 2-fold or even no in-crease over their acute phase titers. However,inasmuch as the acute phase sera were obtainedafter several'days of illness and the titers werequite high, we have considered them to be indica-tive of influenza B.
Of the single serum group, 7 patients demon-strated cold agglutinins in titers ranging from 10to 60. A large number showed agglutinins for thestreptococcus; and, as in the other group, theywere mainly of low titer. One serum however,had a titer of 160. This titer along with a coldagglutinin titer of 60 and low influenza titersmakes one strongly suspect a possible atypicalpneumonia. There seemed to be little correlationbetween the cold agglutinin and the streptococcustiter, as in the other group.
Titrating these sera for antibodies to the psitta-cosis group gave 3 positives. Two of these werequite low, a 1: 5 serum dilution in each case givingbetter than 50 per cent fixation, while one serumtitered to 20.
The influenza results are the usual titers ob-tained when single serum samples are titrated. Awide individual variation was apparent. Severalof the sera did show high titers, one giving a titerof 10,240.
These sera that had high influenza B antibodieswere from students who had been ill several daysbefore entering the infirmary. This would ac-
count for the high titers due to the rapid produc-tion of influenzal antibodies.
Many of the patients from whom only singleserum samples were obtained perhaps would havedemonstrated antibody increases had convalescentserum been received. In some of these, as statedabove, where the acute phase specimen was takenafter a few days of illness, significant titers maybe noted.
Students: The sera obtained from these stu-dents were handled in the same manner as thehospitalized patients. All 9 serum samples fromeach student were titrated at the same time usingthe same test materials. Of the 52 students, 3were unable to continue after their fourth bleeding.Their 4 samples, however, were tested.
The majority of the student serum samples hadtiters of less than 10 for cold agglutinins. Therewere a few that showed a titer of 10 and some atiter of 20. There was only 1 student with a titerof 30 and again only one had a titer of 40. Nogreater titers were obtained. Although there wasa greater number of students with titers for theindifferent streptococcus, here, again, relativelylow titers were obtained throughout. Thereseemed to be little correlation between the presenceof cold agglutinins and streptococcala.ntibodies aswas noted in the hospitalized group. There mayhave been a slight correlation between strepto-coccal antibodies and the presence of upper re-spiratory infections such as colds and sore throats,but the evidence is insufficient to warrant anydefinite conclusion.
With regard to the psittacosis group, there werea few sera that gave positive reactions for thegroup antigen in dilutions of 1: 5. In 1 case, all9 sera, i.e., each monthly sample, were positive atthis dilution. The other sera were positives usu-ally for 1 or 2 months at most. These positivesdid not react with the normal control antigen. Ina few other instances, there were some studentswho had sera that reacted both with the test anti-gen and the control antigen. These apparentlywere non-specific, and so were not included withour positive results.
Table III contains the results of titrating serafor antibodies to influenza A, B, and Swine. Theresults have been summarized on this table andshow the titers of the students for each month.
423

SEYMOURS. KALTER AND ORREND. CHAPMAN
Each number represents the number of studentshaving that titer for the designated antigen ineach represented month. Fifteen students in thisgroup were vaccinated with the army vaccineagainst influenza A and B following their No-vember bleeding. The first two serum sampleswere quite low when tested for influenza A andin the main showed very little variation duringthe course of the winter. It may be seen in TableIII that the majority of students did not demon-strate titers greater than 320. The unvaccinatedgroup maintained a constant titer with some stu-dents showing a 1-tube variation which was con-sidered insignificant. Two members had no dem-onstrable titers for the entire period, while 5 stu-dents, although initially having no titer, developedantibodies during the course of the winter. Thevaccinated group demonstrated, in most instances,at least a 4-fold antibody rise. However, 3 mem-bers of the group gave only a 2-fold rise and 2members showed no antibody increase at all. Ofthose producing increased antibody levels, thelevels resulting were variable with relation to theincrease and duration. Several maintained con-stant titers for the 7 tested months following theirvaccination, whereas others demonstrated antibodydecreases for 1 or more months previous to theirlast sample.
The titers for influenza B were considerablyhigher in the majority of cases. Table III showsthat the majority of students had antibody titersgreater than 320. This was evident before thestart of the vaccination program and was consid-ered to be indicative of subclinical infection priorto the beginning of this study. Several unvac-cinated students demonstrated 4-fold or betterantibody rises to this virus in their December sam-ple. None of these had reported infection or anyillness during the preceding month. This wouldappear to indicate that they had come in contactwith the virus during the epidemic without anyapparent effect other than the stimulation of influ-enza B antibodies. As in influenza A, there areindividual variations in the duration of the anti-body level. Interesting is the fact that the titersof those receiving the vaccine became higher forthis virus than for the Type A strain. The highinitial titer, i.e., the antibody level of October'sserum sample, would seem to indicate that contact
TABLE III
The monthly tigers of the student group,to influenza A, B, and Swine
Following the November bleeding, 15 students received theinfluenza A and B vaccine.
Anti-Influ- body Month (1945-1946)enza titeranti- (finalgen dilu- -
tion) Oct. Nov. Dec. Jan. Feb. Mar. Apr. May June
0 8 7 2 3 3 3 3 3 340 9 9 8 6 5 5 5 5 1680 14 15 12 10 9 6 9 9 14
160 13 13 17 16 18 6 19 19 14320 4 3 5 9 4 21 4 4 3
A 640 3 4 6 '5 5 5 6 6 61,280 1 1 1 1 1 5 2 3 32,560 0 0 1 2 2 3 1 0 05,120 0 0 0 0 0 0 0 0 0
10,240 0 0 0 0 0 0 0 0 0
0 2 2 0 0 0 0 0 0 040 2 3 1 1 1 1 2 1 180 4 2 1 2 2 2 1 2 2
160 4 5 4 1 2 3 4 3 3320 8 6 4 7 8 4 4 7 9
B 640 12 17 14 14 11 16 15 14 121,280 10 7 9 8 8 6 6 6 -62,560 4 5 8 8 9 9 9 9 95,120 6 5 8 7 3 4 5 5 6
10,240 0 0 3 4 5 4* 3 2 1
0 6 5 4 3 3 3 3 3 340 5 5 3 1 2 2 2 2 380 6 7 7 8 8 7 9 10 9
160. 15 17 17 19 17 19 17 15 17320 10 9 12 12 10 9 9 9 9
Swine 640 6 5 4 3 3 3 3 5 31,280 3 4 4 4 3 5 6 5 42,560 1 0 1 2 3 1 0 0 15,120 0 0 0 0 0 0 0 0 0
10,240 0 0 0 0 0 0 0 0 0
to the virus had been made, and makes us feel thatthe virus was present in the community severalmonths prior to the actual outbreak. We wereinterested in observing that the general titers forSwine influenza, although not comparable to thosefor influenza B, were usually higher than those forinfluenza A. There appeared to be little effectresulting from the vaccination; only 3 of the 15had more than a 2-fold antibody increase. Also,the titers of this group appeared to have very littlerelationship to the influenza A titers. Three mem-bers of this group demonstrated no antibody levelduring the entire series.
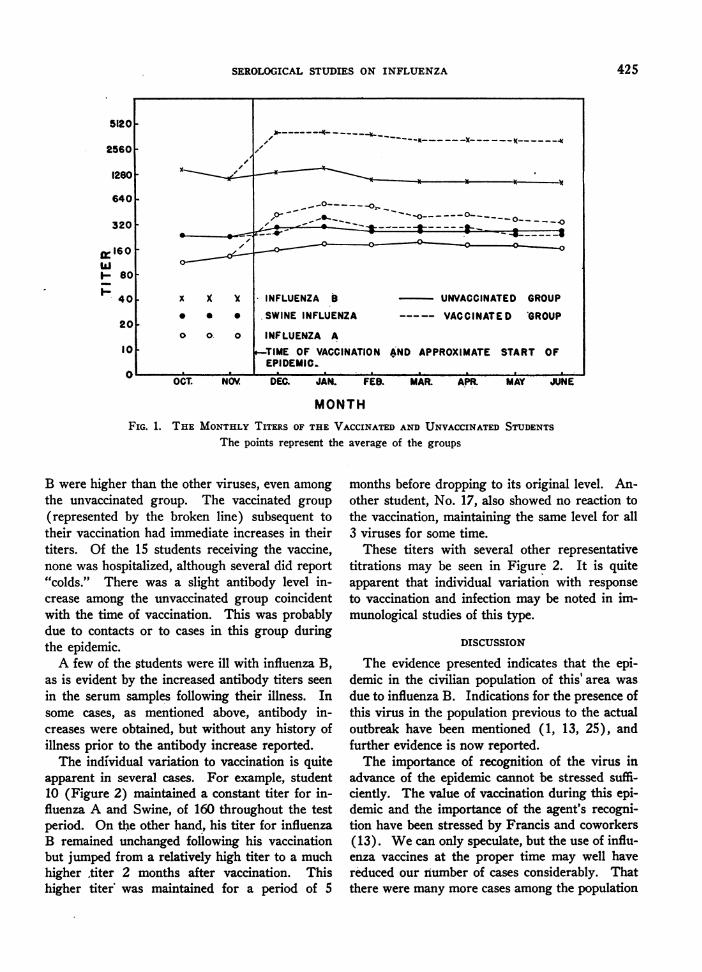
Wehave averaged the titers of the vaccinatedand unvaccinated groups for each month. Theaveraged titers for each group are represented inFigure 1. It is evident that the titers for influenza
424
SEROLOGICALSTUDIES ON INFLUENZA
x,
x X X* * *
o ok 0
-_
0-~~~ . -. . 0 ---
.INFLUENZA B
SWINE INFLUENZA
UNVACCINATED GROUP
VACCINATED GROUP
INFLUENZA A
TIME OF VACCINATION AND APPROXIMATE START OFEPIDEMIC.
FEB. MAR. APR.
MONTHFIG. 1. THE MONTHLYTITERs OF THE VACCINATEDAND UNVACCINATEDSTUDENTS
The points represent the average of the groups
B were higher than the other viruses, even among
the unvaccinated group. The vaccinated group
(represented by the broken line) subsequent totheir vaccination had immediate increases in theirtiters. Of the 15 students receiving the vaccine,none was hospitalized, although several did report"colds." There was a slight antibody level in-crease among the unvaccinated group coincidentwith the time of vaccination. This was probablydue to contacts or to cases in this group duringthe epidemic.
A few of the students were ill with influenza B,as is evident by the increased antibody titers seen
in the serum samples following their illness. Insome cases, as mentioned above, antibody in-creases were obtained, but without any history ofillness prior to the antibody increase reported.
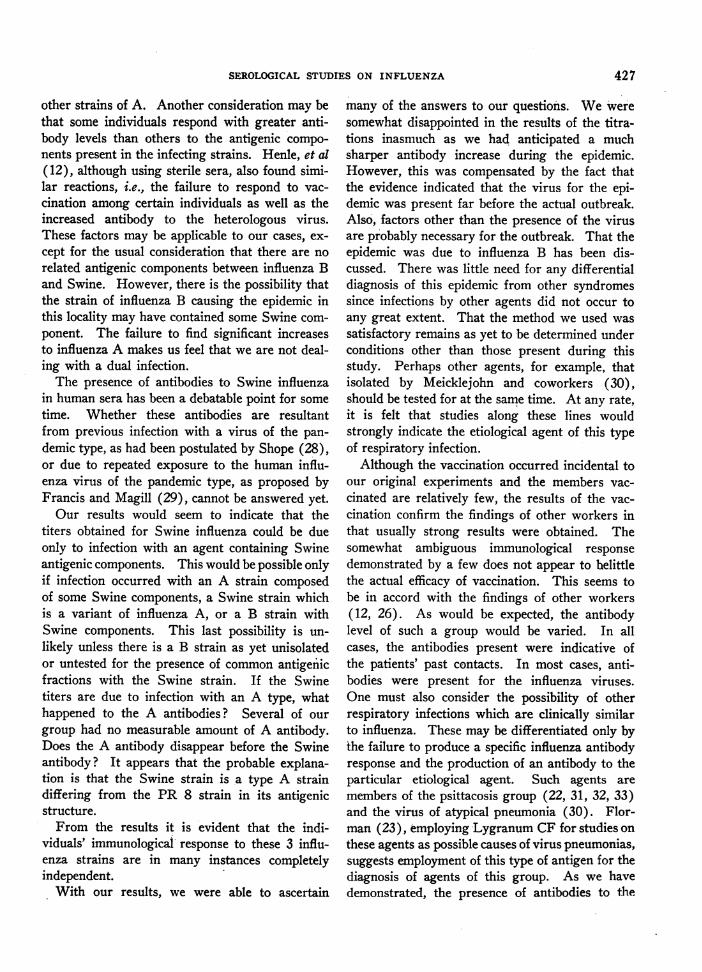
The individual variation to vaccination is quiteapparent in several cases. For example, student10 (Figure 2) maintained a constant titer for in-fluenza A and Swine, of 160 throughout the testperiod. On the other hand, his titer for influenzaB remained unchanged following his vaccinationbut jumped from a relatively high titer to a muchhigher titer 2 months after vaccination. Thishigher titer was maintained for a period of 5
months before dropping to its original level. An-other student, No. 17, also showed no reaction tothe vaccination, maintaining the same level for all3 viruses for some time.
These titers with several other representativetitrations may be seen in Figure 2. It is quiteapparent that individual variation with responseto vaccination and infection may be noted in im-munological studies of this type.
DISCUSSION
The evidence presented indicates that the epi-demic in the civilian population of this' area was
due to influenza B. Indications for the presence ofthis virus in the population previous to the actualoutbreak have been mentioned (1, 13, 25), andfurther evidence is now reported.
The importance of recognition of the virus inadvance of the epidemic cannot be stressed suffi-
ciently. The value of vaccination during this epi-demic and the importance of the agent's recogni-tion have been stressed by Francis and coworkers(13). Wecan only speculate, but the use of influ-enza vaccines at the proper time may well havereduced our number of cases considerably. Thatthere were many more cases among the population
5120
2560 -
1280
640
3201
gI160wI- 80
F 40
20
10
OCT. NOV. DEC. JAN. MAY JUNE
425

SEYMOURS. KALTER AND ORREND. CHAPMAN
10240
5120
2560
1280 -
640 -
320 -
bi'mm
160
80
40
20
10
OCT.
o o 10 *INFLUENZA Bx x x #15.*
_ * * #42-- INFLUENZA A
" " " *rI-*~ - -SWINE INFLUNZ
MAY JUNE
FIG. 2. INDIVIDUAL TITERS OF FIVE STUDENTSOVERTHE NINE MONTHPERIOD FOR INFLUENZA A, B AND
SWINE
* Vaccinated following their November bleeding.
was recognized, since the disease varies among
individuals in its severity and need for hospitaliza-tion. The need for studies along these lines is im-perative for the early recognition of the etiologicagent in order to administer vaccines at the proper
time. The time element for administration of thevaccine is of importance as has been shown byseveral workers (8 to 11). Reinfection, althoughin a milder form, may occur after several monthshave elapsed between vaccination and experi-mental infection. This is apparent in the anti-body decline following vaccination subsequent toits initial increase. The results indicate that theprophylactic administration of the influenza vac-
cine should be given during the month of Sep-tember in order to offer the desired protectionbefore the outbreak of the epidemic.
The significance of antibody levels is still ques-
tionable in resistance to influenza. What may beconsidered a high level apparently is relative tothe individual. Several individuals in our groups
had no initial level. This was evident among the
patients and the students. There were severalwho had no initial titers to one or more of the in-fluenza strains. Then, only because of vaccinationor possibly infection, were titers obtained. Weare still unable to determine what may be con-
sidered as a protective antibody titer to eachindividual.
Usually, the antibody response to infection withinfluenza B resulted in the production of anti-bodies specific for that agent. There were some
individuals who developed a 2-fold antibody in-crease to our PR8 strains and some to our Swinestrain. We feel confident that these slight in-creases are not due to antibody destruction be-cause all materials were handled in such a man-
ner as to avoid bacterial growth. The possibilityof an anamnestic reaction as postulated by Bodilyand Eaton (26) must be considered. These au-
thors also suggest that their high titers to the
Swine strains may be due to the strain responsiblefor their cases which have a greater antigenicfraction in common with the Swine strain than
I DEC. JAN. FEB. MAR. APR.,TIME OF VACCINATION
'AND EPIDEMIC.
426
10
12 C%
46
SEROLOGICAL STUDIES ON INFLUENZA
other strains of A. Another consideration may bethat some individuals respond with greater anti-body levels than others to the antigenic compo-nents present in the infecting strains. Henle, et al(12), although using sterile sera, also found simi-lar reactions, i.e., the failure to respond to vac-cination among certain individuals as well as theincreased antibody to the heterologous virus.These factors may be applicable to our cases, ex-cept for the usual consideration that there are norelated antigenic components between influenza Band Swine. However, there is the possibility thatthe strain of influenza B causing the epidemic inthis locality may have contained some Swine com-ponent. The failure to find significant increasesto influenza A makes us feel that we are not deal-ing with a dual infection.
The presence of antibodies to Swine influenzain human sera has been a debatable point for sometime. Whether these antibodies are resultantfrom previous infection with a virus of the pan-demic type, as had been postulated by Shope (28),or due to repeated exposure to the human influ-enza virus of the pandemic type, as proposed byFrancis and Magill (29), cannot be answered yet.
Our results would seem to indicate that thetiters obtained for Swine influenza could be dueonly to infection with an agent containing Swineantigenic components. This would be possible onlyif infection occurred with an A strain composedof some Swine components, a Swine strain whichis a variant of influenza A, or a B strain withSwine components. This last possibility is un-likely unless there is a B strain as yet unisolatedor untested for the presence of common antigenicfractions with the Swine strain. If the Swinetiters are due to infection with an A type, whathappened to the A antibodies? Several of ourgroup had no measurable amount of A antibody.Does the A antibody disappear before the Swineantibody? It appears that the probable explana-tion is that the Swine strain is a type A straindiffering from the PR 8 strain in its antigenicstructure.
From the results it is evident that the indi-viduals' immunological response to these 3 influ-enza strains are in many instances completelyindependent.
With our results, we were able to ascertain
many of the answers to our questions. Weweresomewhat disappointed in the results of the titra-tions inasmuch as we had anticipated a muchsharper antibody increase during the epidemic.However, this was compensated by the fact thatthe evidence indicated that the virus for the epi-demic was present far before the actual outbreak.Also, factors other than the presence of the virusare probably necessary for the outbreak. That theepidemic was due to influenza B has been dis-cussed. There was little need for any differentialdiagnosis of this epidemic from other syndromessince infections by other agents did not occur toany great extent. That the method we used wassatisfactory remains as yet to be determined underconditions other than those present during thisstudy. Perhaps other agents, for example, thatisolated by Meicklejohn and coworkers (30),should be tested for at the same time. At any rate,it is felt that studies along these lines wouldstrongly indicate the etiological agent of this typeof respiratory infection.
Although the vaccination occurred incidental toour original experiments and the members vac-cinated are relatively few, the results of the vac-cination confirm the findings of other workers inthat usually strong results were obtained. Thesomewhat ambiguous immunological responsedemonstrated by a few does not appear to belittlethe actual efficacy of vaccination. This seems tobe in accord with the findings of other workers(12, 26). As would be expected, the antibodylevel of such a group would be varied. In allcases, the antibodies present were indicative ofthe patients' past contacts. In most cases, anti-bodies were present for the influenza viruses.One must also consider the possibility of otherrespiratory infections which are clinically similarto influenza. These may be differentiated only bythe failure to produce a specific influenza antibodyresponse and the production of an antibody to theparticular etiological agent. Such agents aremembers of the psittacosis group (22, 31, 32, 33)and the virus of atypical pneumonia (30). Flor-man (23), employing Lygranum CF for studies onthese agents as possible causes of virus pneumonias,suggests employment of this type of antigen for thediagnosis of agents of this group. As we havedemonstrated, the presence of antibodies to the
427

SEYMOURS. KALTER AND ORREND. CHAPMAN
psittacosis group were few and the titers obtainedcould easily have been non-specific. Several work-ers have reported that a low percentage of normalsera will give positive reactions with antigens ofthis nature when employed in low dilutions (21,23, 34, 35). None of the students gave historiesto indicate contact with members of this group.The patient who titered to 20, was Frei negativeand unable to give a history of contact with birds.The interpretation of this titer is, therefore, diffi-cult.
The value of cold agglutinins and streptococcalagglutination is still questionable. On the basis ofour results, their value still remains an enigma.However, in agreement with Favour (36) andFinland, et al (37), we feel that our results demon-strate that normal individuals as well as many con-ditions cause type 0 cells to agglutinate in thecold with titers of less than 40. And still moreindividuals cause the agglutination of the indiffer-ent streptococcus in low dilutions, as also ob-served by Finland, et al (38). Webelieve thatthese diagnostic procedures are of aid in atypicalpneumonia only when viewed with other pro-cedures such as x-ray and clinical findings.
It is felt that this group of tests may be of valueto the laboratory in establishing the etiology ofrespiratory infections. Also, because of theirsimplicity, diagnostic laboratories should be ableto employ them as routine group tests in the lab-oratory diagnosis.
CONCLUSIONS
1. The epidemic in this area was due to influ-enza B.
2. This virus was present for several monthsbefore the actual outbreak.
3. Vaccination results in an antibody increaselasting in most cases for at least 5 months. Vac-cines should then be administered in the fall of'the year in order to prevent infection.
4. Serological studies of this nature are of valuein: (a) determining the etiologic agent, (b) as-certaining the duration of antibody titers, and (c)estimating the approximate time for administra-tion of vaccines.
5. These tests may be used as a battery of testsby the laboratory, in order to ascertain the etiologyof this type of respiratory infection.
BIBLIOGRAPHY
1. Reports from the Commission on Influenza to theOffice of the Surgeon General, U. S. Army, Pre-ventive Medicine Service, Washington, D. C.(Cited by Francis, et al, Protective effect of vac-cination against epidemic influenza B. J. A. M. A.,1946, 131, 275).
2. Francis, T., Jr., Intranasal inoculation of human in-dividuals with the virus of epidemic influenza.Proc. Soc. Exper. Biol. & Med., 1940, 43, 337.
3. Burnet, F. M., and Foley, M., The results of intranasalinoculation of modified and unmodified influenzavirus strains in human volunteers. M. J. Australia,1940, 2, 655.
4. Eaton, M. D., and Martin, W. P., Immunization withinactive virus of influenza B: Comparison of anti-body response with that produced by infection.Pub. Health Rep., 1942, 57, 445.
5. Bull, D. R., and Burnet, F. M., Experimental immuni-zation of volunteers against influenza virus B. M.J. Australia, 1943, 1, 389.
6. Henle, W., Henle, G., and Stokes, J., Jr., Demonstra-tion of the efficacy of vaccination against influenzatype A by experimental infection of human beings.J. Immunol., 1943, 46, 163.
7. Francis, T., Jr., Pearson, H. E., Salk, J. E., andBrown, P. N., Immunity in human subjects artifi-cially infected with influenza virus, type B. Am. J.Pub. Health, 1944, 34, 317.
8. Personnel of Naval Laboratory Research Unit No. 1,Experimental human influenza. Am. J. M. Sc.,1944, 207, 306.
9. Hirst, G. K., Rickard, E. R., and Friedewald, W. F.,Studies in human immunization against influenza.Duration of immunity induced by inactive virus.J. Exper. Med., 1944, 80, 265.
10. Francis, T., Jr., Salk, J. E., Pearson, H. E., andBrown, P. N., Protective effect of vaccinationagainst induced influenza A. J. Clin. Invest., 1945,24, 536.
11. Salk, J. E., Pearson, H. E., Brown, P. N., andFrancis, T., Jr., Protective effect of vaccinationagainst induced influenza B. J. Clin. Invest., 1945,24, 547.
12. Henle, W., Henle, G., Stokes, J., Jr., and Maris, E.P., Experimental exposure of human subjects toviruses of influenza. J. Immunol., 1946, 52, 145.
13. Francis, T., Jr., Salk, J. E., and Brace, W. M., Theprotective effect of vaccination against epidemicinfluenza B. J. A. M. A., 1946, 131, 275.
14. Dalldorf, G., and Rice, G. E., A preliminary state wideinfluenza survey using routine blood specimens.(In press.)
15. Hirst, G. K., The quantitative determination of in-fluenza virus and antibodies by means of red cellagglutination. J. Exper. Med., 1942, 75, 49.
16. Peterson, 0. L., Ham, T. H., and Finland, M., Coldagglutinins (antihemagglutinins) in primary atypi-cal pneumonias. Science, 1943, 97, 167.
428

SEROLOGICALSTUDIES ON INFLUENZA
17. Commission on Acute Respiratory Diseases, Coldhemagglutinins in primary atypical pneumonia andother respiratory infections. Am. J. M. Sc., 1944,208, 742.
18. Thomas, L,, Mirick, G. S., Curnen, E. C., Ziegler,J. E., Jr., and Horsfall, F. L., Jr., Studies on pri-mary atypical pneumonia. II. Observations con-cerning the relationship of a non-hemolytic strepto-coccus to the disease. J. Clin. Invest., 1945, 24, 227.
19. Eaton, M. D., and Corey, M., Complement fixationin human pneumonitis with group-reactive virusantigens. Proc. Soc. Exper. Biol. & Med., 1942,51, 165.
20. Smadel, J. E., Wertman, K., and Reagan, R. L.,Yolksac complement fixation antigen for use inpsittacosis-lymphogranuloma venereum group of dis-eases. Proc. Soc. Exper. Biol. & Med., 1943, 54, 70.
21. Rake, G., Shaffer, M. F., Jones, H. P., and McKee,C. M., Lymphogranuloma Venereum. "A mono-graph," E. R. Squibb and Sons, N. Y., 1943.
22. Eaton, M. D., Martin, W. P., and Beck, M. D., Theantigenic relationship of the virus of meningopneu-monitis and lymphogranuloma venereum. J. Exper.Med., 1945, 75, 21.
23. Florman, A. L., The- use of a commercially availablecomplement-fixing antigen for the diagnosis of ele-mentary body types of viral infection. J. Immunol.,1945, S1, 29.
24. Ziegler, J. E., Jr., and Horsfall, F. L., Jr., Interferencebetween the influenza viruses. I. The effect of ac-tive virus upon the multiplication of influenza vi-ruses in the chick embryo. J. Exper. Med., 1944,79, 361.
25. Salk, J. E., Influenza in Europe during the winter of1945-46. J. Bact., 1946, 51, 632.
26. Bodily, H. L., and Eaton, M. D., Specificity of theantibody response of human beings to strains of in-fluenza virus. J. Immunol., 1942, 45, 193.
27. Lennette, E. H., Rickard, E. R., Hirst, G. K., andHorsfall, F. L., Jr., The diverse etiology of epi-demic influenza. Pub. Health Rep., 1941, 56, 1777.
28. Shope, R. E., The incidence of neutralizing antibodies
for swine influenza virus in the sera of human be-ings of different ages. J. Exper. Med., 1936, 63,669.
29. Francis, T., Jr., and Magill, T. P., The incidence ofneutralizing antibodies for human influenza virusin the serum of human individuals of different ages.J. Exper. Med., 1936, 63, 655.
30. Meiklejohn, G., Eaton, M. D., and Van Herick, W.,A clinical report on cases of primary atypicalpneumonia caused by a new virus. J. Clin. Invest.,1945, 24, 241.
31. Smadel, J. E., Atypical pneumonia and psittacosis. J.Chin. Invest., 1943, 22, 57.
32. Eaton, M. D., Beck, M. D., and Pearson, H. E., Avirus from cases of atypical pneumonia. Relationto the virus of meningopneumonitis and psittacosis.J, Exper. Med., 1941, 73, 641.
33. Rake, G., Eaton, M. D., and Shaffer, M. F., Similari-ties and possible relationships among viruses ofpsittacosis, meningopneumonitis, and lymphogranu-loma venereum. Proc. Soc. Exper. Biol. & Med.,1941, 48, 528.
34. Dingle, J. H., Abernethy T. J., Badger, G. F., Bud-dingh, G. J., Feller, A. E., Langmuir, A. D.,Ruegsiggir, J. M., and Wood, B., Jr., Primaryatypical pneumonia, etiology unknown (Part III).Am. J. Hyg., 1944, 39, 269.
35. Blair, J. E., The complement fixation reaction withthe antigen of lymphogranuloma venereum. J. Im-munol., 1944, 49, 63.
36. Favour, C. B., Autohemagglutinins-"cold aggluti-nins." J. Chin. Invest., 1944, 23, 891.
37. Finland, M., Peterson, 0. L., Allen, H. E., Samper,B. A., and Barnes, M. W. (with the technical as-sistance of Muriel B. Stone), Cold agglutinins. I.Occurrence of cold isohemagglutinins in variousconditions. J. Chin. Invest., 1945, 24, 451.
38. Finland, M., Samper, B. A., and Barnes, M. W., Coldagglutinins. VI. Agglutinins for an indifferentstreptococcus in primary atypical pneumonia and inother conditions and their relation to cold iso-hemagglutinins. J. Clin. Invest., 1945, 24, 497.
9:29





























