Embed Size (px)
Citation preview

Acta Neurol. Scandinav. 13, 499-512, 1967.
From the Laboratory of Clinical Neurophysiology, University Hospital, Copenhagen, Denmark.
SENSORY AND MOTOR CONDUCTION IN MOTOR NEURONE DISEASE
CUMHUR ERTEKIN~
In motor neurone disease conduction in motor nerves has been reported to be slightly below normal (Henriksen 1956, Lambert & Mulder 1957, Lambert 1962, Vacek 1965, Kyral 1965) and the distal latency in sen- sory nerve to be normal (Lambert 1962, Fincharti & Van Allen 1964). Conduction in sensory and motor fibres of the same nerve has not been compared nor has the sensory conduction velocity along the extremity been determined.
Sensory findings are scarce in motor neurone disease, but there are a number of neuropathies in which cutaneous sensitivity is normal but abnormalities are found in the conduction rate, the amplitude or the shape of the sensory responses (Gilliaft & Sears 1958, Buchfhal & Rosen- falck 1966). If sensory velocity and the other parameters of the sensory response are normal in motor neurone disease, their measurement may contribute to differential diagnosis.
The aim of this study was therefore to determine in patients with motor neurone disease conduction velocities in motor and sensory fibres of the same nerve and in mixed nerves.
For comparison, the motor conduction velocity of 16 nerves was determined in ten patients with scquelae after acute anterior poliomye- litis. Hodes (1949) found a decreased velocity and attributed it to de- struction of the larger neurones; others (Johnson, Guyton & Olsen 1960, Cerra & Johnson 1961, Herring & Knowlton 1963, Doutlik & Skorpil 1965) found the rate of motor conduction to be normal both in the acute and in later stages of the disease.
PATIENTS
The 15 patients with motor neurone disease were 43-74 years old; 9 were males and 6 females. None complained of paraesthesia, and all showed normal surface sensi-
~
1 On leave from the Aegean University, Medical School, Clinical Neurology, Izmir, Turkey, working under a fellowship from the Danish Secretariat for Technical CO- operation with Developing Countries.
500
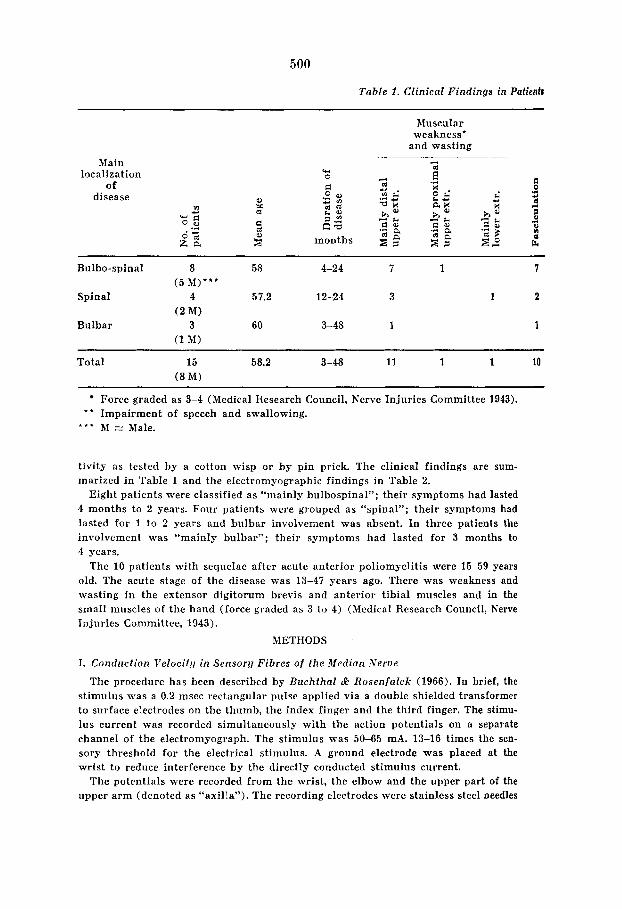
Table I . Clinical Findings in Patienb
Muscular weakness‘
and wasting Main
localization of
disease a ta
u4 0
months
Bulho-spinal 8 58 4-24 7 1 1
Spinal 4 57.2 12-24 3 1 2
Bulbar 3 60 3-48 1 1
( 5 M ) * * *
(2 M)
(1 M)
Total 15 58.2 3-48 11 1 1 10 ( 8 M )
Force graded as 3-4 (Medical Research Council, Nerve Injuries Committee 1943). * * Impairment of speech and swallowing.
* * + M = Male.
tivity as tested by a cotton wisp or by pin prick. The clinical findings are sum- marized in Table 1 and the elcctromyographic findings in Table 2.
Eight patients were classified as “mainly bulbospinal”; their symptoms had lasted 4 months to 2 years. Four patients were grouped as “spinal”; their symptoms had lasted for 1 to 2 years and bnlbar involvement was absent. In three patients the involvement was “mainly bulbar”; their symptoms had lasted for 3 months to 4 years.
The 10 patients with sequelae after acute anterior poliomyelitis were 15-59 years old. The acute stage of the disease was 13-47 years ago. There was weakness and wasting in the extensor digitorum brevis and anterior tibia1 muscles and in the small muscles of the hand (force graded as 3 to 4) (Medical Research Council, Nerve Injuries Committee, 1943).
METHODS
I. Conduction Velocit!i in Sensory Fibres o f the Median Nerve
The procedure has been described by Buchthal & Rosenfalck (1966). In brief, the stimulus was a 0.2 msec rectangular pulse applied via a double shielded transformer to surface electrodes on the thumb, the index finger and the third finger. The stimu- lus current was recorded simultaneously with the action potentials on a separate channel of the electromyograph. The stimulus was 50-65 mA. 13-16 times the sen- sory threshold for the electrical stimulus. A ground electrode was placed at the wrist to reduce interference by the directly conducted stimulus current.
The potentials were recorded from the wrist, the elbow and the upper part of the upper arm (denoted as “axilla”). The recording electrodes were stainless steel needles
501
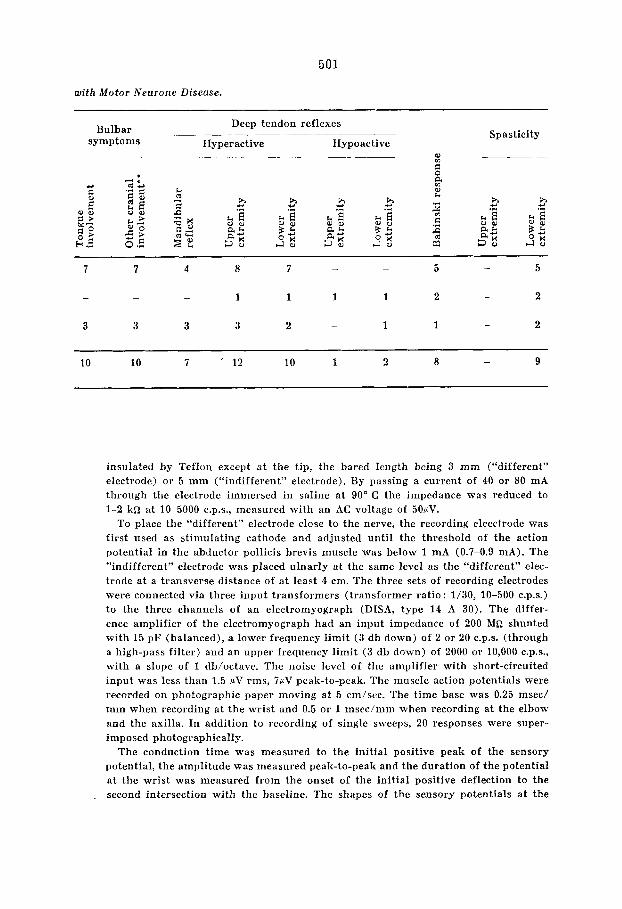
with Motor Neurone Disease.
Deep tendon reflexes Spasticity Bulbar
symptoms Hyperactive Hypoactive
5 - 5 - - 7 7 4 8 7
- 3 3 3 3 2 - 1 1 2
9 - 10 10 7 ’ 12 10 1 2 8
insulated by Teflon except a t the tip, the bared lcngth being 3 mm (“different” electrode) or 5 mm (“indifferent” electrode). By passing a current of 40 or 80 mA through the electrode immersed in saline at 90” C the impedance was reduced to 1-2 k a at 10-5000 c.P.s., measured with an AC voltage of 50fiV.
To place the “different” electrode close to the nerve, the recording eleectrode was first used as stimulating cathode and adjusted until the threshold of the action potential in the abductor pollicis brevis muscle was below 1 mA (0.7-0.9 mA). The ”indifferent” electrode was placed ulnarly a t the same level as the “different” elec- trode at a transverse distance of a t least 4 cm. The three sets of recording electrodes were connected via three input transformers (transformer ratio : 1/30, 10-500 C.P.S.) to the three channels of an electromyograph (DISA, type 14 A 30). The differ- ence amplifier of the electromyograph had an input impedance of 200 M a shunted with 15 pF (balanced), a lower frequency limit (3 db down) of 2 or 20 C.P.S. (through a high-pass filter) and an upper frequency limit (3 db down) of 2000 or 10,000 c.P.s., with a slope of 1 db/octavc. The noise level of the amplifier with short-circuited input was less than 1.5 PV rms, ~ P V peak-to-peak. The muscle action potentials were recorded on photographic paper moving at 5 cm/sec. The time base was 0.25 msec/ mm when recording at the wrist and 0.5 or 1 msec/mm when recording at the elbow and the axilla. In addition to recording of single sweeps, 20 responses were super- imposed photographically.
The conduction time was measured to the initial positive peak of the sensory potential, the amplitude was measured peak-to-peak and the duration of the potential a t the wrist was measured from the onset of the initial positive deflection to the second intersection with the baseline. The shapes of the sensory potentials a t the
502
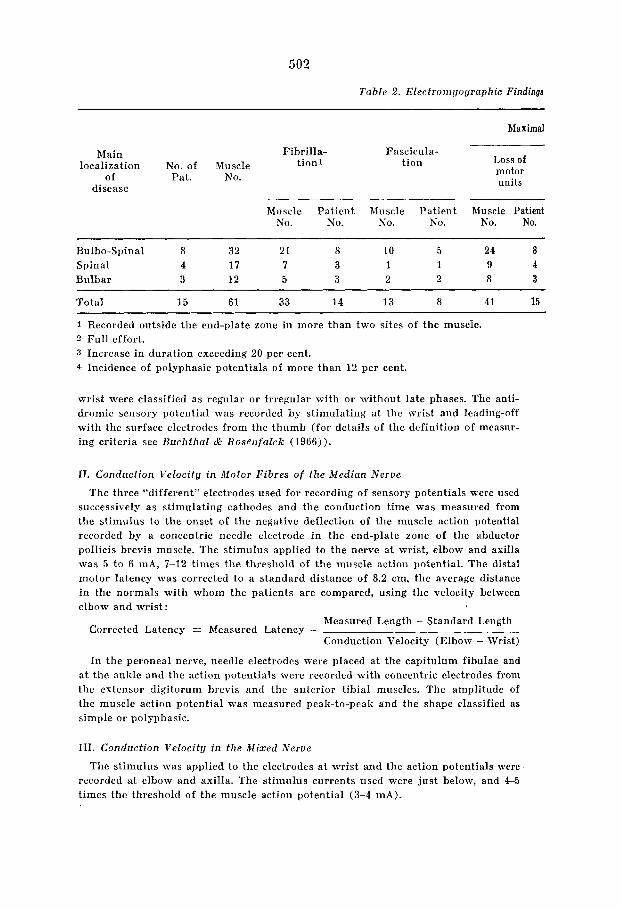
Table 2 . Electroni!jographic Findings
Maximal
Fibrilla- Fascicula- tionl tion Loss of
motor units
Main localization No. of Muscle
of Pat. No. disease
_______ Muscle Patient Muscle Patient hluscle Patient
NO. No. No. No. No. No.
Bulbo-Spinal 8 32 21 8 10 5 24 a Spinal 4 17 7 3 1 1 9 4 Bulbar 3 12 5 3 2 2 8 3
Total 15 61 33 14 13 8 41 15
1 Recorded outside the end-plate zone in more than two sites of the muscle. 2 Full effort. 3 Increase in duration exceeding 20 per cent. 4 Incidence of polyphasic potentials of more than 12 per cent.
wrist were classified as regular or irregular with or withont late phases. The anti- dromic sensory potential was recorded by stimulating at the wrist and leading-off with the surface electrodes from the thnmb (for details of the definition of measur- ing criteria see Bzzchthal & Rosenfalck (1966)).
11. Conduction Velocitg in Motor Fibres of the Median Nerve
The three “different” electrodes used for recording of sensory potentials were used successively as stimulating cathodes and the conduction time was measured from the stimulus to the onset of the negative deflection of the muscle action potential recorded by a concentric needle electrode in the end-plate zone of the abductor pollicis brevis muscle. The stimulus applied to the nerve a t wrist, elbow and axilla was 5 to 6 mA, 7-12 times the threshold of the muscle action potential. The distal motor latency was corrected to a standard distance of 8.2 cm, the average distance in the normals with whom the patients are compared, using the velocity between clbow and wrist:
Xlcasured Length - Standard Length Corrected Latency = Measured Latency -
Conduction Velocity (Elbow - Wrist)
In the peroneal nerve, needle electrodes were placed at the capitulum fibulae and a t the ankle and the action potentials were recorded with concentric electrodes from the extensor digitorurn brevis and the anterior tibia1 muscles. The amplitude of the muscle action potcntial was measured peak-to-peak and the shape classified as simple or polyphasic.
111. Conduction Velocitg in the Mixed Nerve
The stimulus was applied to the electrodes a t wrist and the action potentials were recorded at elbow and axilla. The stimulus currents used were just below, and 4-5 times the threshold of the muscle action potential (3-4 mA).
503
in Patients w i t h nlotor Neurone Disease.
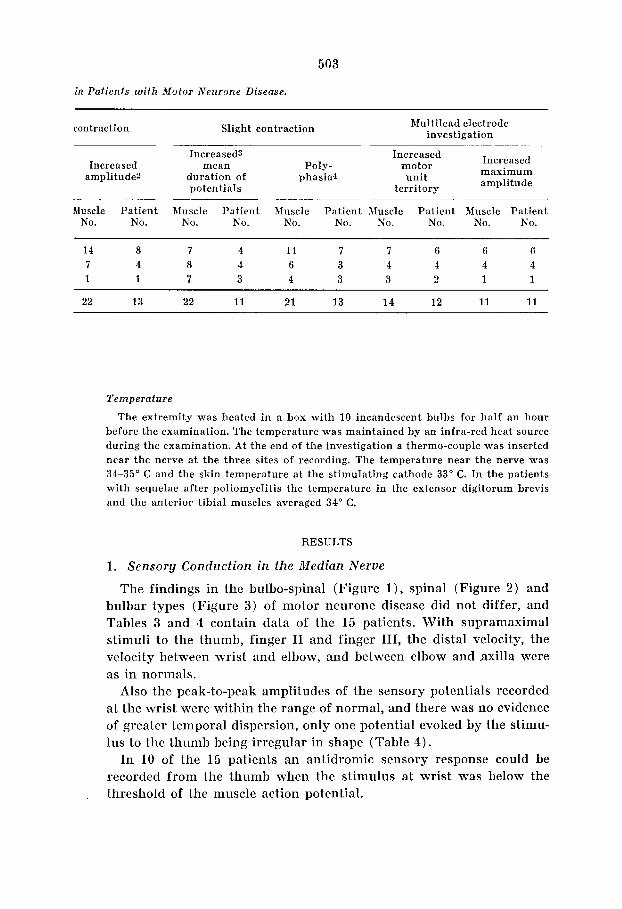
Multilead electrode investigation contraction Slight contraction
Increased maximum amplitude
Increased3 Increased Increased mean Poly- motor
amplitude2 duration of phasia4 unit potentials territory -
Muscle Patient Muscle Patient Muscle Patient Muscle Patient Muscle Patient No. No. No. No. No. No. No. No. No. No.
14 8 7 4 11 7 7 6 6 6 7 4 8 4 6 3 4 4 4 4 1 1 7 3 4 3 3 2 1 1
22 13 22 11 21 13 14 12 11 11
Temperature
The extremity was heated in a box with 10 incandescent bulbs for half an hour before the examination. The temperature was maintained by an infra-red heat source during the examination. At the end of the investigation a thermo-couple was inserted near the nerve at the three sites of recording. The temperature near the nerve was 34-35" C and the skin temperature a t the stimulating cathode 33" C. In the patients with sequelae after poliomyelitis the temperature in the extensor digitorum brevis and the anterior tibia1 muscles averaged 34" C.
RESULTS
1. Sensory Conduction in the Median Nerve
The findings in the bulbo-spinal (Figure l ) , spinal (Figure 2 ) and bulbar types (Figure 3 ) of motor ncurone disease did not differ, and Tables 3 and 4 contain data of the 15 patients. With supramaximal stimuli to the thumb, finger I1 and finger 111, the distal velocity, the velocity between wrist and elbow, and between elbow and .axilla were as in normals.
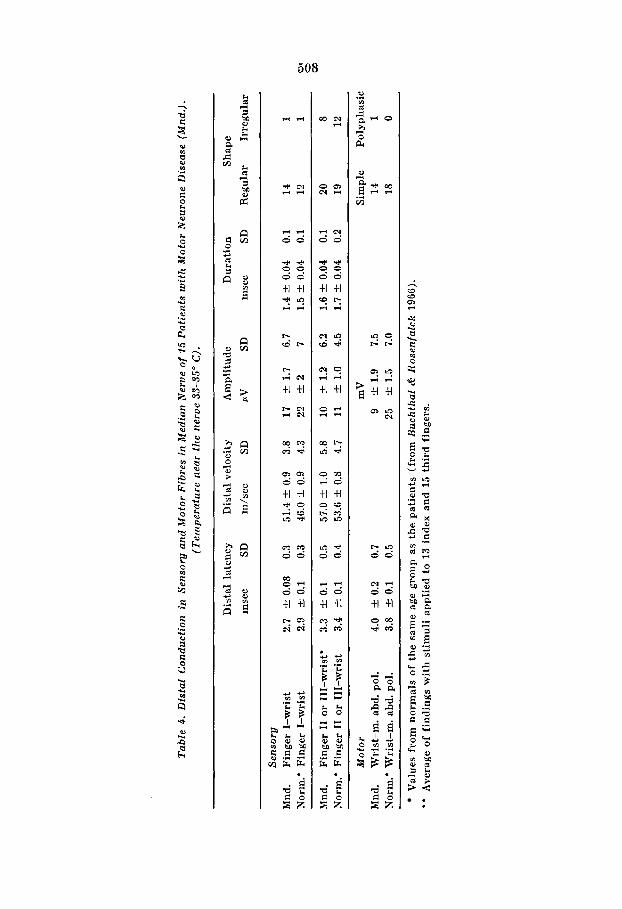
Also the peak-to-peak amplitudes of the sensory potentials recorded at the wrist were within the range of normal, and there was no evidence of greater temporal dispersion, only one potential evoked by the stimu- lus to the thumb being irregular in shape (Table 4 ) .
In 10 of the 15 patients an antidromic scnsory response could be recorded from the thumb when the stimulus at wrist was below the threshold of the muscle action potential. ,
Motor mabd poll.
w n ) 6 ' m 1 l O r n V
u
1 s 1Ornsec
Sensory 5: finger I
-1 + t su
1 O m s e c I S O m A = 1 1 5
5 : iingerl finger11 tingerm
\ ~ O ~ A = I G X T ~ \ S S ~ A = I ~ T~ i 65m1=1SrT5
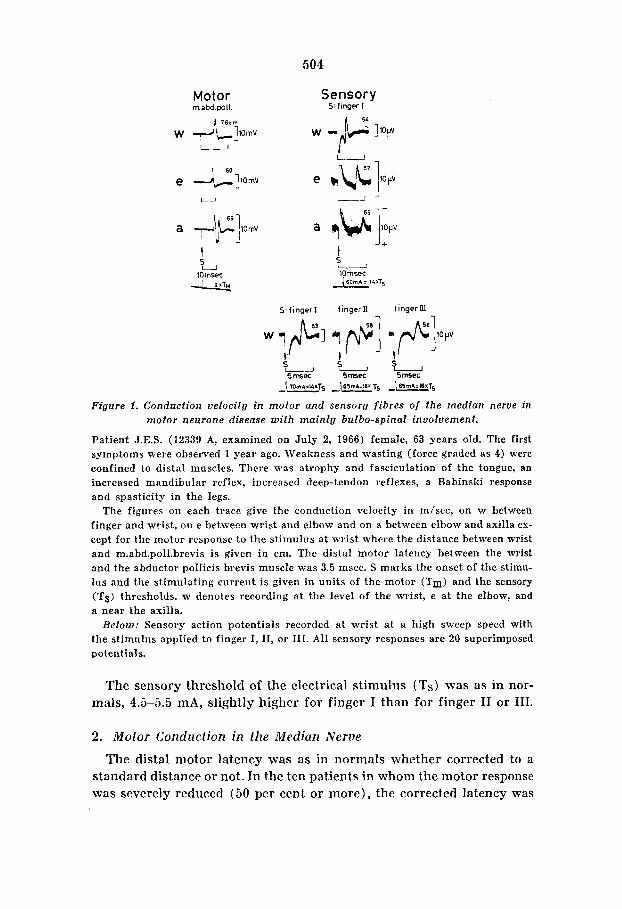
Figure 1. Conduction velocitij in motor and sensory f ibres o f the median nerve in motor neurone disease w i th mainly bulbo-spinal involvement.
Patient J.E.S. (12339 A, examined on July 2, 1966) female, 63 years old. The first symptoms were observed 1 year ago. Weakness and wasting (force graded as 4) were confined to distal muscles. There was atrophy and fasciculation of the tongue, an increased mandibular reflex, increased deep-tendon reflexes, a Babinski response and spasticity in the legs.
The figures on each trace give the conduction velocity in m/sec, on w between finger and wrist, on e between wrist and elbow and on a between elbow and axilla ex- cept for the motor response to the stimulus at wrist where the distance between wrist and m.abd.poll.brevis is given in cm. The distal motor latency between the wrist and the abductor pollicis brevis muscle was 3.5 msec. S marks the onset of the stirnu- lus and the stimulating current is given in units of the motor (Tm) and the sensory (Ts) thresholds. w denotes recording at the level of the wrist, e at the elbow, and a near the axilla.
Below: Sensory action potentials recorded at wrist a t a high sweep speed with the stimulus applied to finger I, 11, or 111. All sensory responses are 20 superimposed potentials.
The sensory threshold of the electrical stimulus (Ts) was as in nor- mals, 4.5-5.5 mA, slightly higher for finger I than for finger I1 or 111.
2 . Motor Conduction in ihe Median Nerve
The distal motor latency was as in normals whether corrected to a standard distance or not. In the ten patients in whom the motor response was severely reduced (50 per cent or more), the corrected latency was

505
Motor rn abd.poU
I
e +]5m~
U
a -+]5mv
1 lOmsec _I,
Sensory ?,:finger 1
Mixed 5: wrist
?,:finger I fingern fingerm -
I I I
Figure 2. Conduction velocity in motor and sensory fibres and o f the mixed nerve in motor neurone disease wi th spinal involvement.
Patient A.K.P. (12299 A, examined on May 21, 1966), female, 74 years old. The first symptoms were observed 2 years ago. Weakness (force graded as 2) and wasting were mainly confined to distal muscles. There were no bulbar signs and symptoms. The deep tendon reflexes were weak in the arms and there was a Babinski response and spasticity in the legs. Fasciculations occurred in the upper extremities.
The figures on each trace give the conduction velocity in m/sec, on w between finger and wrist, on e between wrist and elbow and on a between elhow and axilla ex- cept for the motor response to the stimulus at wrist where the distance between wrist and m.abd.poll.brevis is given in cm. The distal motor latency between the wrist and the abductor pollicis brevis muscle was 3.4 msec. S marks the onset of the stimulus and the stimulating current is given in units of the motor (Tm) and the sensory thresholds (Ts). w denotes recording at the level of the wrist, e a t the elbow, and a near the axilla.
Below: Sensory action potentials recorded at wrist a t a high sweep speed with the stimulus applied to finger I, 11, or 111. A l l sensory responses are 20 superimposed potentials.
normal, whereas the non-corrected latency tended to be slightly longer (O.Ol<p<0.05). The velocity between elbow and wrist was as in nor- mals, irrespective of the reduction in amplitude, and slightly slower than the sensory velocity (O.OOl<p<O.Ol).
The velocity between axilla and elbow was slightly lower than in normals (p<O.OOl) and than the sensory velocity (O.Ol<p<O.O5) re- gardless of the reduction in the motor response.
In patients with mainly bulbo-spinal or spinal involvement the
506
Motor m.abd.poll,
Sensory 5:finger I
5 - lOmsec 10 msec
Mixed 5:wrist
Stinger1 fingern fingerm
Smsec 5msec Smsec I 45d=22qs f i 4om4=\3xT5 I 35d=12xT5
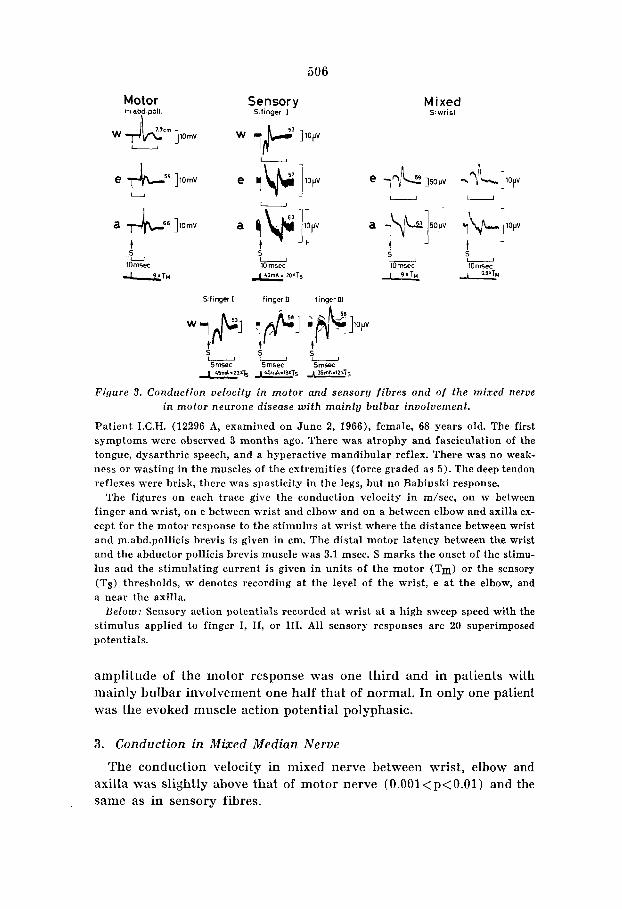
Figure 3. Conducfion velocity in motor and sensory f ibres and o f the mixed nerve in motor neurone disease w i th mainlg bulbar involvement.
Patient I.C.H. (12296 A, examined on June 2, 1966), female, 68 years old. The first symptoms were observed 3 months ago. There was atrophy and fasciculation of the tongue, dysarthric speech, and a hyperactive mandibular reflex. There was no weak- ness or wasting in the muscles of the extremities (force graded as 5 ) . The deep tendon reflexes were brisk, there was spasticity in the legs, but no Babinski response.
The figures on each trace give the conduction velocity in m/sec, on w between finger and wrist, on e between wrist and elbow and on a between elbow and axilla ex- cept for the motor response to the stimulus at wrist where the distance between wrist and m.abd.pollicis brevis is given in cm. The distal motor latency between the wrist and the abductor pollicis brevis muscle was 3.1 msec. S marks the onset of the stimu- lus and the stimulating current is given in units of the motor (Tm) or the sensory (Ts) thresholds, w denotes recording at the level of the wrist, e at the elbow, and a near the axilla.
Below: Sensory action potentials recorded at wrist a t a high sweep speed with the stimulus applied to finger I, 11, or 111. All sensory responses are 20 superimposed potentials.
amplitude of the motor response was one third and in patients with mainly bulbar involvement one half that of normal. In only one patient was the evoked muscle action potential polyphasic.
3 . Conduction in Mixed Median Nerve
The conduction velocity in mixed nerve between wrist, elbow and axilla was slightly above that of motor nerve (O.OOl<p<O.Ol) and the same as in sensory fibres.
507
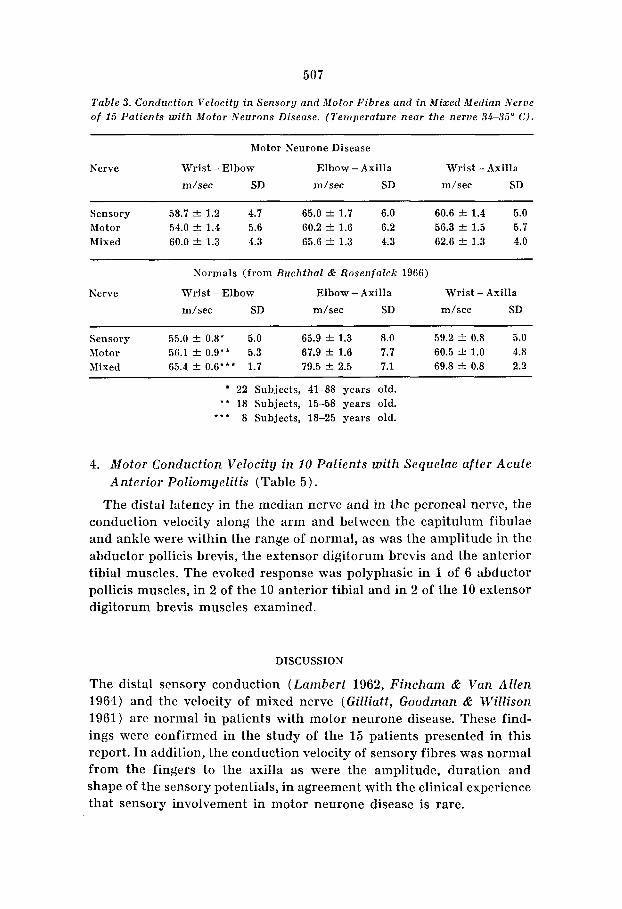
Table 3. Conduction Velocity in Sensory and Motor Fibres and in Mixed Median Nerve of 15 Patients with Motor Neurons Disease. (Temperature near the nerve 34-35" C).
Motor Neurone Disease
Nerve Wrist - Elbow Elbow - Axilla Wrist - Axilla m/sec SD m/sec SD m/sec SD
Sensory 58.7 f 1.2 4.7 65.0 k 1.7 6.0 60.6 f 1.4 5.0 Motor 54.0 f 1.4 5.6 60.2 f 1.6 6.2 56.3 f 1.5 5.7 Mixed 60.0 f 1.3 4.3 65.6 f 1.3 4.3 62.6 f 1.3 4.0
Normals (from Buchthal h Rosenfalclc 1966)
Nerve Wrist - Elbow Elbow - Axilla Wrist - Axilla m/sec SD m/sec SD m/sec SD
Sensory 55.0 f 0.8' 5.0 65.9 f 1.3 8.0 59.2 f 0.8 5.0 Motor 56.1 f 0.9'* 5.3 67.9 f 1.6 7.7 60.5 & 1.0 4.8 Mixed 65.4 f 0.6*** 1.7 79.5 f 2.5 7.1 69.8 f 0.8 2.2
22 Subjects, 41-88 years old. * * 18 Subjects, 15-58 years old.
8 Subjects, 18-25 years old. *.*
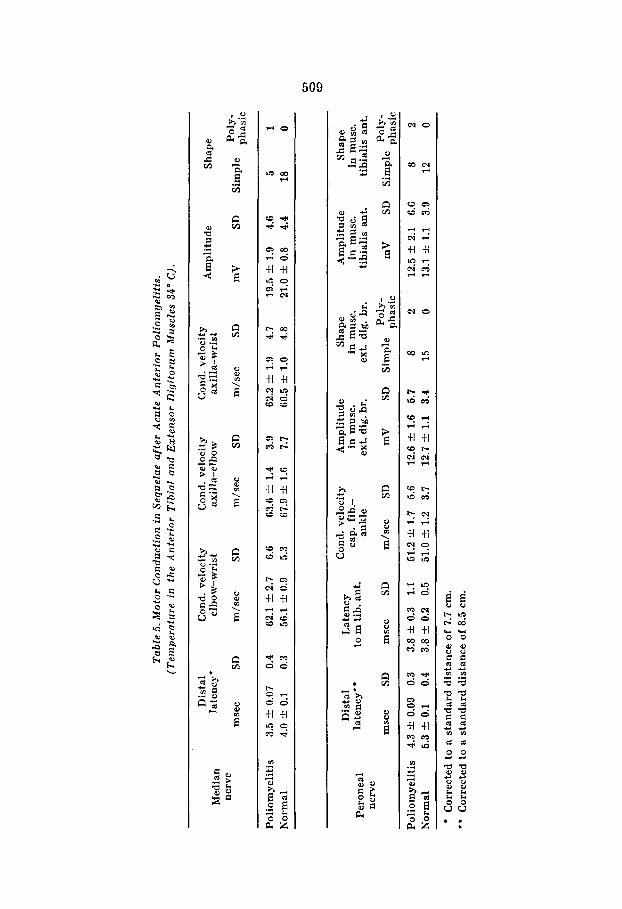
4. Motor Conduction Velocity in 10 Patients with Sequelae after Acute Anterior Poliomyelitis (Table 5 ) .
The distal latency in the median nerve and in the peroneal nerve, the conduction velocity along the arm and between the capitulum fibulae and ankle were within the range of normal, as was the amplitude in the abductor pollicis brevis, the extensor digitorum brevis and the anterior tibial muscles. The evoked response was polyphasic in 1 of 6 abductor pollicis muscles, in 2 of the 10 anterior tibial and in 2 of the 10 extensor digitorum brevis muscles examined.
DISCUSSION
The distal sensory conduction (Lambert 1962, Fincham & V a n Allen 1964) and the velocity of mixed nerve (Gilliatt, Goodman & Willison 1961) are normal in patients with motor neurone disease. These find- ings were confirmed in the study of the 15 patients presented in this report. In addition, the conduction velocity of sensory fibres was normal from the fingers to the axilla as were the amplitude, duration and shape of the sensory potentials, in agreement with the clinical experience that sensory involvement in motor neurone disease is rare.
Tab
le 4.
Dis
tal
Con
duct
ion
in S
enso
ry a
nd M
otor
Fib
res
in M
edia
n N
erve
of
15 P
atie
nts
wit
h M
otor
Neu
rone
Dis
ease
(M
nd.).
(T
empe
ratu
re n
ear
the
nerv
e 33
-35"
C).
Dis
tal
late
ncy
Dis
tal v
eloc
ity
Am
plit
ude
Dur
atio
n S
hape
m
sec
SD
m/s
ec
SD
PV
SD
mse
c SD
R
egul
ar
Irre
gula
r
Sen
sory
M
nd.
Fin
ger
I-w
rist
2.
7 rl:
0.08
0.
3 51
.4 f 0
.9
3.8
17
-+ 1.
7 6.
7 1.
4 f 0
.04
0.1
14
1 N
orm
.' F
inge
r I-
wri
st
2.9
4 0
.1
0.3
46.0
rl:
0.9
4.3
22 3. 2
7
1.5
rl:
0.04
0.
1 12
1
Mnd
. F
inge
r I1
or
111-
wri
st'
3.3
rl:
0.1
0.5
57.0
f 1
.0
5.8
10
+. 1.
2 6.
2 1.
6 f 0
.04
0.1
20
8 N
orm
.' F
inge
r I1
or
111-
wri
st
3.4
4 0
.1
0.4
53.6
f 0
.8
4.7
11
-+ 1
.0
4.5
1.7 f 0
.04
0.2
19
12
Mot
or
Mnd
. W
rist
-m.
abd.
pol
. 4.
0 2 0
.2
0.7
Nor
m.'
Wri
st-m
. ab
d. p
ol.
3.8
+. 0.
1 0.
5
mV
9
4 1
.9
7.5
25
4 1
.5
7.0
Sim
ple
Pol
ypha
sic
14
1 18
0
Val
ues
from
nor
mal
s of
the
sam
e ag
e gr
oup
as t
he p
atie
nts
(fro
m B
ucht
hal
& R
osen
falc
k 19
66).
'*
A
vera
ge o
f fi
ndin
gs w
ith
stim
uli
appl
ied
to 1
3 in
dex
and
15 t
hird
fin
gers
.
Tab
le 5
. Mot
or C
ondu
ctio
n in S
eque
lae
afte
r A
cute
Ant
erio
r P
olio
mge
liti
s.
(Tem
pera
ture
in
the
Ant
erio
r T
ibia
1 an
d E
xten
sor
Dig
itor
um M
uscl
es 3
4" C
).
Am
plit
ude
Shap
e D
ista
l C
ond.
vel
ocit
y C
ond.
vel
ocit
y C
ond.
vel
ocit
y M
edia
n la
tenc
y'
elbo
w-w
ris
t ax
illa-
elbo
w
axil
la-w
ris
t
nerv
e Po
ly-
mse
c SD
m
/sec
SD
m
/sec
SD
m
/sec
SD
m
V
SD
Sim
ple
phas
ic
Pol
iom
yeli
tis
3.5 f 0.07
0.4
62.1 -
F. 2.7
6.6
63.6 ik 1.4
3.9
62.2 f 1.9
4.7
19.5 *
1.9
4.6
5 1
Nor
mal
4.0
-F. 0.1
0.3
56.1 k
0.9
5.3
67.9 -F
. 1.6
7.7
60.5 -
F. 1.0
4.8
21.0 k
0.8
4.4
18
0
cn
0
W
Lat
ency
C
ond.
vel
ocit
y A
mpl
itud
e S
hape
A
mpl
itud
e S
hape
in
mus
c.
in m
usc.
in
mus
c.
in m
usc.
ex
t. di
g. b
r.
ext.
dig.
br.
ti
bial
is a
nt.
tibi
alis
ant
. D
ista
l to
m ti
b. a
nt.
cap.
fib
*-
ankl
e P
eron
eal
late
ncy'
ne
rve ~
mse
c SD
m
sec
SD
m/s
ec
SD
mV
SD
S
impl
e ~~
~~~c
m
V
SD
Sim
ple l$':~~
~~
~ ~~
~ ~
__
__
__
~~
__
__
_
Pol
iom
yeli
tis
4.3
+- 0.09
0.3
3.8
& 0.3
1.1
51.2 k
1.7 5.6
12.6 f 1.6
5.7
8 2
12.5 &
2.1
6.6
8 2
Nor
mal
5.3
0.1
0.4
3.8 k 0.2 0.5
51.0 k
1.2 3.7
12.7 zk
1.1
3.4
15
0 13.1 k
1.1
3.9
12
0
** C
orre
cted
to
a st
anda
rd d
ista
nce
of 7.7
cm.
Cor
rect
ed t
o a
stan
dard
dis
tanc
e of
8.5 c
m.

510
The velocity in the mixed median nerve was the same as that of the sensory fibres and slightly higher than that in motor fibres. In normals of the same age motor conduction was the same in motor and sensory fibres and in mixed nerve (Ruchthal & Rosenfalck 1966). The velocity of the potential of mixed nerve has often been considered to be a suitable measure of velocity in sensory fibres. This was the case in our patients with motor neurone disease; it is by no means always the case in normals (Buchthal c!Z Rosenfalck 1966) and it is never the case when motor conduction velocity is normal and sensory conduction velocity is impaired.
As to motor conduction, statements in the literature differ: Henriksen (1956) reported a small reduction in motor conduction velocity ascribed to the higher age of the patients than of the controls. Lambert & Mulder (1957) found a slight decrease in distal conduction velocity in patients in whom the response amplitude was reduced to less than 20 per cent of normal and Lamberf (1962) did not believe this slowing to be due to low temperature. Hnik et a2. (1962) , Drechsler e f al. (1963), Blom et al. (1964) and Vylclicky (1965) found conduction velocity and distal laten- cy to be the same as in normals, whereas Vacek (1965) found a slight decrease in distal latency. Even in patients in whom the motor response was severely reduced, the distal motor latency corrected to a standard distance was as in normals, as was the velocity between elbow and wrist. Only between axilla and elbow did the motor conduction velocity tend to be slower than in normals, as reported by Lambert (1962) for the distal latency and the velocity between elbow and wrist. In my 15 pa- tients the slowing was not related to the duration of the disease.
The motor conduction velocity in the ten patients with sequelae after acute anterior poliomyelitis was normal, in agreement with findings reported by Henriksen (1956), Johnson et al. (1960), Cerra & Johnson (1961), Herring & Knowl fon (1963), and Doutlik & Skorpil (1965). The low velocities found by Hodes (1949) were probably due to a low tem- perature in the affected extremities.
SUMMARY
Conduction in sensory and motor fibres and in the mixed median nerve was examined in 15 patients with motor neurone disease (8 with mainly bulbo-spinal, 4 with spinal and 3 with mainly bulbar involvement). In addition, motor conduction velocity was determined in 10 patients with scquelae after acute anterior poliomyelitis. The temperature near the nerve was kept at 34-35' C.
1 ) The sensory conduction velocity between fingers and wrist and

between wrist, elbow and axilla was normal as were amplitude, shape and duration of the sensory potentials. The velocity of mixed median nerve between wrist, elbow and axilla was as the velocity of the sensory fibres. The distal motor latency and the motor conduction between elbow and wrist were slightly below the velocity of the sensory fibres but within the range of normal, whether or not the response amplitude was severely reduced. The motor conduction velocity between axilla and elbow was slightly lower than in normals (O.OOl<p<O.Ol).
2 ) In the 10 patients with sequelae after acute anterior poliomyelitis the conduction velocity was normal in the median and peroneal nerves, as were the distal motor latencies, the latency to the anterior tibia1 muscles and the amplitude of the muscle action potentials.
ACKNOWLEDGEMENTS
The work was supported by grants from the Muscular Dystrophy Associations of America and the Danish National Association for Infantile Paralysis (Polio).
My thanks are due to professor F. Buchthal for excellent working conditions and for guidance and encouragement through all phases of the present work.
REFERENCES
Blom, S., E. Hagbarth h P. 0. Lundberg (1964) : Motor conduction velocities in amyo- trophic lateral sclerosis, polyradiculoneuritis and Charcot-Marie-Tooth’s dis- ease. Acta neurol. scand. 40, 6-12.
Buchfhal, F., h A. Rosenfalck (1966) : Evoked action potentials and conduction velo- city in human sensory nerves. Brain Research. 3, pp. 122.
Cerra, D., & E. W. Johnson (1961) : Motor nerve conduction velocity in “idiopathic” polyneuritis. Arch. Phys. hIed. 42, 159-163.
Doutlik, S., & V. Skorpil (1965) : Cit. from Skorpil, V. Conduction velocity of human nerve structures. Nakladatelstvi CeskoslovenskC Akademie Ved. Praha, pp. 58.
Drechsler, B., V. Skorpil & J . Vacek (1963) : Motor nerve conduction in neurology. Abstracts Internat. EMG Meeting, Copenhagen, 74-76.
Fincharn, R. W., & M. W. Van Allen (1964) : Sensory nerve conduction in amyotrophic lateral sclerosis. Neurology 14, 31-33.
Gilliatt, R. W., H. W. Goodman & R. G. Willison (1961) : The recording of lateral popliteal nerve action potentials in man. J. Neurol. Neurosurg. Psychiat. 24,
Gilliatt, R. M., h 2’. A . Sears (1958) : Sensory nerve action potentials in patients with peripheral nerve lesions. J. Neurol. Neurosurg. Psychiat. 21, 109-118.
Henriksen, J. D.: Conduction velocity of motor nerves in normal subjects and in patients with neuromuscular disorders. Thesis, University of Minnesota, Gra- duate School, Minneapolis.
Herring, J., & G. Knowlton (1963) : Motor nerve impulse propagation velocity in poliomyelitis. Arch. Phys. Med. 44, 253-256.
Hnik, P., V. Skorpil h L. VyklickLj (1962) : Diagnosis and therapy of denervation muscle atrophy. Chapter XI1 in Gutmann, E. The Denervated Muscle. Publish- ing House of the Czechoslovak Academy of Sciences. Prague, 433-466.
305-318.
.
33 ACTA NEUROL. SCAND. 43, 4
Hodes, R. (1949) : Selective destruction of large moto-neurons by poliomyelitis virus. I. Conduction velocity of motor nerve fibers of chronic poliomyelitis patients. J. Neurophysiol. 12, 257-266.
Johnson, E. W., J. D. Gugton h K. J. Olsen (1960) : Motor nerve conduction velocity studies in poliomyelitis. Arch. Phys. bled. Of, 185-190.
Kgral , V. (1965) : Cit. from Skorpil, V. Conduction velocity of human nerve structures. Nakladatelstvi Ceskoslovenskb Akademie Ved. Praha, pp. 59.
Lamberf, E. H. (1962) : Diagnostic value of electrical stimulation of motor nerves. Electroenceph. clin. Neurophysiol, Suppl. 22, 9-16.
Lamberf, E. H . , & D. W. fifulder (1957) : Electromyographic studies in amyotrophic lateral sclerosis. Proc. Mayo Clin. 32, 441-446.
Aiedical Research CounciI, Nerve Injuries Committee (1943) : Aids to investigation of peripheral nerve injuries. M.R.C. War Memorandum No. 7, London, H.M. Stationery Office, pp. 48.
Vacek, J. (1965) : Cit. from Skorpil, V. Conduction velocity of human nerve structures. Nakladatelstvi Ceslcoslovenske Akademie Ved. Praha, pp. 59.
I 'gkl ick~, L . (1965) : Cit. from Sliorpil, V. Conduction velocity of human nerve structures. Nakladatelstvi CeskoslovenskC Altademie Ved. Praha, pp. 59.
Received April 15, 1967. Cumhur Eriekin, Laboratory of Clinical Neurophysiology, University Hospital, Tagensvej 18, Copenhagen, Denmark.