Embed Size (px)
Citation preview

SELF STUDY DOCUMENT FOR ACCREDITATION REVIEW BY
THE COUNCIL ON EDUCATION FOR PUBLIC HEALTH (CEPH)
University of Utah Department of Family and Preventive Medicine
Division of Public Health 375 Chipeta Way, STE A Salt Lake City, UT 84108
801-587-3315
CONTACT: Stephen C. Alder, PhD Chief, Division of Public Health
Phone: 801-587-3315 Email: [email protected]
2
Table of Contents Executive Summary ............................................................................................ 10
1.0 The Public Health Program ........................................................................ 11
1.1 Mission. .................................................................................................................................... 11
1.2 Evaluation. ................................................................................................................................ 17
1.3 Institutional Environment. ......................................................................................................... 28
1.4 Organization and Administration. ............................................................................................. 36
1.5 Governance. ............................................................................................................................. 43
1.6 Fiscal Resources. ..................................................................................................................... 49
1.7 Faculty and Other Resources. .................................................................................................. 55
1.8 Diversity. ................................................................................................................................... 60
2.0 Instructional Programs ................................................................................ 70
2.1 Degree Offerings. ..................................................................................................................... 70
2.2 Program Length. ....................................................................................................................... 72
2.3 Public Health Core Knowledge. ................................................................................................ 73
2.4 Practical Skills. .......................................................................................................................... 74
2.5 Culminating Experience. ........................................................................................................... 79
2.6 Required Competencies. .......................................................................................................... 82
2.7 Assessment Procedures. .......................................................................................................... 92
2.8 Bachelor’s Degrees in Public Health. ....................................................................................... 98
2.9 Academic Degrees. .................................................................................................................. 99
2.10 Doctoral Degrees.................................................................................................................... 103
2.11 Joint Degrees. ........................................................................................................................ 106
2.12 Distance Education or Executive Degree Programs. ............................................................. 111
3.0 Creation, Application and Advancement of Knowledge ............................ 112
3.1 Research. ............................................................................................................................... 112
3.2 Service. ................................................................................................................................... 123
3.3 Workforce Development. ........................................................................................................ 133
4.0 Faculty, Staff and Students ...................................................................... 146
4.1 Faculty Qualifications. ............................................................................................................. 146
4.2 Faculty Policies and Procedures. ............................................................................................ 154
4.3 Student Recruitment and Admissions. ................................................................................... 158
4.4 Advising and Career Counseling. ........................................................................................... 164
3
List of Tables
Table 1.2.1 Measureable Objectives ...................................................................................................... 21
Table 1.5.1 Functions addressed by the Division committees ................................................................ 45
Table 1.6.1 Sources of Funds and Expenditures by Major Category, 2009 to 2014 .............................. 52
Table 1.6.2 Outcome Measures for 2010/2011, 2011/2012, and 2012/2013 ......................................... 53
Table 1.7.1 Headcount of Primary Faculty .............................................................................................. 55
Table 1.7.2 Faculty (Fac), Students and Student/Faculty Ratios by Department or Specialty Area 2011-2014 ............................................................................................................................................... 56
Table 1.7.3 Outcome Measures for 2011-2014 ...................................................................................... 59
Table 1.8.1 Diversity of Core Faculty (source Mission Base Management – MBM) ............................... 65
Table 1.8.2 Diversity of full-time staff (source self-reported) .................................................................. 65
Table 1.8.3 Diversity of Students (source self-reported, applications) .................................................... 66
Table 1.8.4 Summary Data for Faculty, Students and/or Staff ............................................................... 68
Table 2.1.1 Instructional Matrix – Degrees ............................................................................................. 70
Table 2.3.1 Required Courses Addressing Public Health Core Knowledge Areas for MPH ................... 73
Table 2.4.1 CEPH Practicum 2012 and 2013 ......................................................................................... 76
Table 2.6.1 Courses and other learning experiences by which the competencies are met for all masters ................................................................................................................................................... 84
Table 2.6.2 Secondary Courses ............................................................................................................. 86
Table 2.6.3 Courses and other learning experiences by which the MSPH specific Competencies are met .......................................................................................................................................................... 88
Table 2.6.4 PhD Competencies and other learning experiences ............................................................ 89
Table 2.7.1 Outcome Measures for 2013-2014 ...................................................................................... 93
Table 2.7.2 Students in MPH Degree, By Cohorts Entering Between 2010-2011 .................................. 94
Table 2.7.3 Students in PhD Degree, By Cohorts Entering Between 2007-2008 and 2013-2014 .......... 95
Table 2.7.4 Destination of MPH Graduates by Employment Type ......................................................... 96
Table 2.7.5 Destination of MSPH Graduates by Employment Type ....................................................... 96
Table 2.7.6 Destination of PhD Graduates by Employment Type .......................................................... 96
4
Table 2.10.1 Required Courses Addressing Public Health Core Knowledge Areas for PhD Degree .................................................................................................................................................. 103
Table 2.10.2 Doctoral Student Data for year 2013-2014 ...................................................................... 104
Table 2.11.1 Electives for the MD/MPH students ................................................................................. 106
Table 2.11.2 Difference DNP/MPH students ........................................................................................ 107
Table 2.11.3 MPH Coursework for DNP/MPH ...................................................................................... 107
Table 2.11.4 Electives for the DNP/MPH students ............................................................................... 107
Table 2.11.5 Electives for the MHA/MPH students ............................................................................... 108
Table 2.11.6 Electives for the MPA/MPH students ............................................................................... 109
Table 2.11.7 Electives for the MPP/MPH students ............................................................................... 109
Table 2.11.8 Electives for the MSW/MPH students .............................................................................. 110
Table 3.1.1 Research Activity from 2011-2013 ..................................................................................... 115
Table 3.1.2 Outcome Measures for Research activities ....................................................................... 120
Table 3.2.1 Faculty Service from 2011 to 2014 .................................................................................... 124
Table 3.2.2 Service Activity from 2011-2013 ........................................................................................ 129
Table 3.2.3 Outcome Measure for Service activities ............................................................................ 131
Table 3.3.1 Emerging Leader Workshop Series ................................................................................... 136
Table 3.3.2 Public Health Grand Rounds ............................................................................................. 137
Table 3.3.3 Global Public Health Grand Rounds .................................................................................. 138
Table 3.3.4 Learning Management System (LEARN) ........................................................................... 139
Table 3.3.5 Rapidly Conducting Community Health Needs Assessments ........................................... 140
Table 3.3.6 Utah Public Health Association Pre-conference 2012 ....................................................... 140
Table 3.3.7 Utah Public Health Performance Improvement Boot Camp ............................................... 140
Table 3.3.8 Knowledge Café................................................................................................................. 140
Table 3.3.9 Emerging Leader Workshop Series ................................................................................... 140
Table 3.3.10 Funded Training/Continuing Education Activity from 2011 to 2013 ................................. 141
Table 3.3.11 Certificate Data from 2011 to 2014 .................................................................................. 143
Table 4.1.1 Current Primary Faculty Supporting Degree Offerings of General Program ...................... 147

5
Table 4.1.2 Other Faculty Used to Support Teaching Programs (adjunct, part-time, secondary appointments, etc.) ............................................................................................................................... 150
Table 4.1.3 Outcome Measures for faculty members qualifications ..................................................... 151
Table 4.3.1 Quantitative Information on Applicants, Acceptances, and Enrollments, 2011 to 2014 ..... 161
Table 4.3.2 Student Enrollment Data from 2011-2014 ......................................................................... 162
Table 4.3.3 Outcome Measures for Enrollment of Qualified Student Body .......................................... 162
6
List of Figures
Figure 1.3.1 The University of Utah Orgnaizational Chart ...................................................................... 29
Figure 1.3.2 Senior Vice President for Health Sciences Orgnaizational Chart ....................................... 30
Figure 1.3.3 Deparmtnet of Family and Preventive Medicine Orgnaizational Chart ............................... 31
Figure 1.4.1 Divisoin of Public Health Orgnaizational Chart ................................................................... 40
Figure 1.4.2 Division of Public Health Leadership Team Orgnaizational Chart ...................................... 41
7
List of Appendices
Appendix 1.2A End of Semester Survey Overview
Appendix 1.2B Focus Group April 30 13
Appendix 1.3A University of Utah Specialized Accreditation Schedule
Appendix 1.5A Division Committees
Appendix 1.5B Scholarship Criteria
Appendix 1.5C Scholarship Applications
Appendix 2.2A MPH Degree Faculty/ Student Work Sheet
Appendix 2.5A Student Contribution
Appendix 2.5B MPH/MSPH Comprehensive Examination Team Member Evaluation Form
Appendix 2.6A Alumni Survey
Appendix 2.7A 2013 Survey Results
Appendix 2.9A MSPH Worksheet
Appendix 2.10A PhD Worksheet
Appendix 2.11A MD/MPH Worksheet
Appendix 3.3A An Assessment of Utah’s Local Health Departments Training Needs
Appendix 4.2A Guidelines for Faculty Annual Reviews
Appendix 4.3A Summer 2013 Newsletter
Appendix 4.3B FAQ Answers to inquiries and worksheet
8
List of Abbreviations ACCME Accreditation Council for Continuing Medical Education APHA America Public Health Association ADA Americans with Disabilities Act AHEC Area Health Education Centers BPCCDP Bassi Pathana Community Collaborative Development Project BYU Brigham Young University BPC Budget Planning Consolidation CPHAWE California Public Health Alliance for Workforce Excellence CIS Campus Information System CCTS Center for Clinical and Translational Science CDS Center for Disability Services CDC Center for Disease Control and Prevention CESA Center for Ethnic Student Affairs CMMI Center for Medicare and Medicaid Innovation CTLE Center for Teaching and Learning Excellence CIGH Certificate in Global Health CRMS Clinical Research Management System CFU Community Faces of Utah DHHS Department of Health and Human Services DNP Doctor of Nurse Practitioner F&A Facilities and Administrative FES Fertility Experiences Study FAQ frequently asked questions GHI Global Health Initiative GRE Graduate Record Examination HRSA Health Resources and Services Administration HOPE Home Observation of Periconceptional Exposures HCI Huntsman Cancer Institute IRB Institutional Review Board IPA Interagency Personnel Agreement ILLiad Interlibrary Loan and Document Delivery INHANCE International Head and Neck Cancer Epidemiology Consortium iNEST International NaProTechnology Evaluation and Surveillance of Treatment IRC International Rescue Center LEARN Learning Management System MHA Master of Healthcare Administration MPA Master of Public Administration MPP Master of Public Policy MSW Master of Social Work MACPAC Medicaid and CHIP Payment and Access Commission MBM Mission Based Management MBMAC Mission-Based Management Advisory Committee MTDC Modified Total Indirect Cost Rate NIEHS National Institute of Environmental Health Sciences NWCCU Northwest Commission on Colleges and Universities SED Office for Student Equity and Diversity OEO/AA Office of Equal Opportunity and Affirmative Action OPHP Office of Public Health Practice OSP Office of Sponsored Projects
9
List of Abbreviations (continued) ONES Outstanding New Environmental Scientist PIM Performance Improvement and Management RPT retention, promotion and tenure SLCHD Salt Lake County Health Department SRPHTC Southwest Regional Public Health Training Center SAC Student Advisory Committee SPRINT Systolic Pressure Intervention Trial TLT Teaching and Learning Technologies NPH The New Public Health TDC Total Direct Costs TFFA Total Federal Funds Awarded T-Cer Translational Comparative Effectiveness Research UCLA University of California Los Angeles, Fielding School of Public Health uTRAC University Tracking of Clinical Research APCD Utah All Payer Claims Database UDOH Utah Department of Health UPHW Utah Partnership for Healthy Weight PANO Utah Physical Activity, Nutrition, and Obesity UPDB Utah Population Database UPHA Utah Public Health Association UROP Utah Rural Outreach Program USIIS Utah Statewide Immunization System UWAG Utah Women and Girls WRAPS Wireless Remote Abdominal Pressure Sensor WIMS Women in Medicine and Science
10
Executive Summary The Division of Public Health is one of four Divisions within the Department of Family and Preventive Medicine, at the University of Utah. The Division of Public Health has played a major role in research, education, and service within the School of Medicine for the past 35 years. Since our last review, we have expanded in terms of the number of faculty, our research portfolio, diversity of fiscal resources, and diversity in the learning environment with our global public health programming. By introducing differential tuition, expanding our gifts and development funds, and growing our extramural funding, we have been able to offset a decline in state support. Our faculty members are increasingly active in research, with a growing portfolio of funded projects. The research expertise of our faculty members is both diverse and complementary, allowing for focused and collaborative, multi-disciplinary projects. Students are more involved in faculty-led scholarship as research assistants and as part of their academic coursework. This general trend of expanded student involvement in research activities is expected to continue consistently as we increase the competitiveness of our extramurally funded research program. We have also expanded our role in workforce development through our Office of Public Health Practice (OPHP). As a partner in the Southwest Regional Public Health Training Center, we have successfully engaged with health departments and public health-related organizations throughout Utah, Nevada, and Southern California in advancing public health workforce capacity. Our degree programs are well established for both professional (MPH) and academic (MSPH and PhD) education. We have added Graduate Certificates in Public Health and Global Health. These certificates are designed to allow graduate students outside of the Public Health degree programs to gain foundational education in these areas. Although we have not had any major changes in courses offered since the last review we have updated our core curriculum to include coursework in research design as well as program planning and evaluation. Global Health has evolved a great deal since our last self-study accreditation. We have gone from offering one community-engaged scholarship-based learning abroad summer program to four per year. We have also coordinated the coursework in global health under the Global Health Certificate. As well as expanded our global health scholarship through growth in extramurally funded research. Through the self-study process, we received guidance regarding opportunities to update the competencies for our degree programs. We initiated a process by which we developed an updated set of competencies which we are now implementing. We also have reoriented our diversity framework, focusing on gender, urban versus rural origins, and race/ethnicity reflective of our region. Through this process, we recognized that while we are attracting a breadth of students, we have failed to effectively connect with the Hispanic/Latino community as evidenced by underrepresentation among our students, faculty, and staff. We have since designated a Diversity Committee with an initial charge to develop a strategic plan for better inclusion of this community. We are also working towards a revised degree strategy that will enhance the distinction between professional and academic degrees, formal assessment of service activities in the Division, expanding our resource streams with a more aggressive donor plan, and prioritizing individual career development needs to ensure appropriate advancement and retention of the junior faculty. We are pleased that with a growing core faculty and administrative staff, we are able to distribute responsibilities across the Division of Public Health so that effective progress occurs across these initiatives simultaneously.

11
1.0 The Public Health Program 1.1 Mission. The program shall have clearly formulated and publicly stated mission with supporting goals, objectives, and values a. A clear and concise mission statement for the program as a whole.
The Mission of the Division of Public Health is to protect and promote the health of people in communities in Utah and around the globe through high quality scholarship. We research (Knowledge Production through use-inspired research and innovation)…
• Causes and risk factors of disease
• Effective methods of prevention
• Health services
• Advances in public health and health service delivery
We educate (Knowledge Sharing through education and other learner-oriented activities)…
• Dedicated individuals who serve the public's health in government, non-profit and private organizations, and academia
• Current and future health professionals
• Community members to make informed health decisions
We serve (Knowledge Implementation through engaged scholarship)…
• Community members striving to improve health
• Health professionals engaged in research and care
• The global community of science
Vision:
The Division of Public Health serves as a premier academic unit that is advancing the discipline of public health through exemplary scholarship and training of academicians, professionals and leaders to
perform at the highest standards of competence. Mission Integration: The Division of Public Health mission is vertically integrated with the mission of the Department of Family and Preventive Medicine by addressing healthcare needs by educating healthcare professionals, conducting applied research, and implementing interventions in clinical or community-based settings. Our mission is also aligned with the School of Medicine mission through service to the people of Utah and beyond, and through focusing on research and education to improve community health. With respect to the University of Utah mission, we are also aligned through engaged service to the people of Utah and the world, as well as discovery, application and dissemination of knowledge.
12
b. A statement of values that guides the program. We Value Intellectual Curiosity, Scholarship, and Innovation
We pursue the truth We examine and communicate ideas We celebrate academic freedom We are committed to life-long learning and career-long scholarship We provide faculty with the tools and educational opportunities required to perform programmatic
duties and to develop new skills necessary for a successful academic career We Value Collaboration
We encourage teamwork in the pursuit of excellence across all Divisions We pursue synergy by working with university and community partners to meet our mission We work within our campus community to improve our academic quality
We Value a Positive and Respectful Working Environment
We create a climate suitable for effective teaching and learning We respect the personal, physical, and psychological space of others We respect faculty time and strive to be punctual for appointments and meetings We respect the inherent worth of all individuals We celebrate diversity in all its dimensions
We Value Integrity
We teach our students the importance of maintaining confidentiality of privileged information by our example
We treat our colleagues and students with courtesy, respect, dignity, and fairness We Value Accountability and Self Reflection
We hold ourselves and our departmental leadership accountable to our mission, vision, and core values
We reevaluate the departmental mission and vision on a recurring basis We conduct fair, equitable, and timely assessments and evaluations We seek feedback from faculty on departmental leadership responsibilities We communicate regularly and openly about departmental priorities, opportunities, and
challenges We maintain departmental policies and programs that support every faculty member We conduct periodic and continuous Departmental and individual self-evaluation
We Value Excellence.
13
c. One or more goal statements for each major function through which the program intends to attain its mission, including at a minimum, instruction, research, and service. Our goal statements are: Research (Knowledge Production through use-inspired research and innovation)
1. Goal: The Division of Public Health will be productive in population-based research, community focused interventions, health system transformation, and community-engaged participatory research.
2. Goal: Maintain partnerships within and outside of the University of Utah as a foundation for serving as an assembler of disciplines to drive an interdisciplinary scholarly agenda focused on advancing public health.
3. Goal: Increase research opportunities for student and trainee involvement at multiple levels of training.
Education (Knowledge Sharing through education and other learner-oriented activities) 4. Goal: Actively recruit and admit a diverse and qualified student body. 5. Goal: Provide an academically rigorous and relevant educational experience. 6. Goal: Increase public health workforce productivity by training and graduating students that meet
all program competencies. Service (Knowledge Implementation through engaged scholarship)
7. Goal: Encourage student participation in service. 8. Goal: All faculty members at associate professor and professor ranks to have at least one major
university or department level service appointment.
d. A set of measurable objectives with quantifiable indicators related to each goal statement as provided in Criterion 1.1.c. In some cases, qualitative indicators may be used as appropriate. Our goal statements and corresponding measurable objectives are: Research (Knowledge Production through use-inspired research and innovation)
1. Goal: The Division of Public Health will be productive in population-based research, community focused interventions, health system transformation, and community-engaged participatory research.
Objective 1.a: Increase extramural research funding, per tenure-line or research track faculty, to $400,000. Objective 1.b: Publishing at a rate of four peer-reviewed publications per faculty member, per year.
2. Goal: Maintain partnerships within and outside of the University of Utah as a foundation for serving as an assembler of disciplines to drive an interdisciplinary scholarly agenda focused on advancing public health.
Objective 2.a: Faculty members will attend and present at least one national meeting each year that aligns with their academic focus. Objective 2.b: Tenure-line and Research track faculty members will engage in at least one inter-disciplinary research collaboration. Objective 2.c. Faculty members will participate and present research in at least one University of Utah forum each year to ensure intra-institutional networking. Objective 2.d. Maintain scholarly-productive community collaboration to ensure emphasis in community-engaged scholarship.
14
3. Goal: Increase research opportunities for student and trainee involvement at multiple levels of training.
Objective 3.a: Each faculty member will involve at least one doctoral or master level student in scholarship for at least one project annually. Objective 3.b: 1/4 doctoral students and 1/10 master students will be involved in faculty driven research. Objective 3.c: Tenure-line or research track faculty members for research will on average be engaged with one clinical learner (clinical student, medical student, nursing students, pharmacy student, residents and fellows etc.).
Education (Knowledge Sharing through education and other learner-oriented activities) 4. Goal: Actively recruit and admit a diverse and qualified student body.
Objective 4.a: Student body reflects the gender, racial/ethnic, and urban and rural/ frontier distribution of the community. Objective 4.b: Admit academically qualified students with 95% of accepted students above a specified GRE score and GPA.
5. Goal: Provide an academically rigorous and relevant educational experience.
Objective 5.a. All courses will be taught by faculty members with specific content expertise. Objective 5.b: The 17 core master and doctoral courses and distance-based delivery of the five basic MPH/MSPH courses will be offered annually. Objective 5.c: Extracurricular applied research/engaged scholarship presentations will be held at least monthly. Objective 5.d: Student will have overall satisfaction with courses.
6. Goal: Increase public health workforce productivity by training and graduating students that meet
all program competencies. Objective 6.a: Meet an 80% 4 year graduation rate for master students and a 60% 7 year graduation rate for doctoral students. Objective 6.b: Assure the Curriculum Committee reviews all course syllabi annually, with a focus on identifying and ensuring appropriate competencies are included in required coursework, and reflected in course descriptions. Objective 6.c: Maintain an active presence in workforce development including providing average monthly workshops, and linking the public health workforce to online training resources and public health agencies to help develop workforce strategies.
Service (Knowledge Implementation through engaged scholarship) 7. Goal: Encourage student participation in service.
Objective 7.a: Support annual community-engaged scholarship opportunities for all graduate students in public health. Objective 7.b: Maintain at least 4 community-engaged scholarship-based learning abroad summer programs available to all University of Utah students. Objective 7.c: Work with the student advisory committee (SAC) to conduct major community service projects semi-annually.
8. Goal: All faculty members at associate professor and professor ranks to have at least one major university or department level service appointment.
Objective 8.a: All faculty members will have at least one major Division level service appointment. Objective 8.b: On average, all faculty members will have at least one community public health service appointment.

15
e. Description of the manner through which the mission, values, goals and objectives were developed, including a description of how various specific stakeholder groups were involved in their development. In 2008, the Division of Public Health underwent its five-year University of Utah Graduate Council Review. One of the comments in the final report was that the Division’s Mission Statement needed to be updated so that it would be aligned with the Mission of the Department, School of Medicine and the University. In response to that recommendation a Mission Statement Committee was formed, consisting of three full-time faculty members. Mission Committee Chair, Dr. VanDerslice, discussed the different mission statements that are found throughout the University of Utah. (i.e. University of Utah, School of Medicine, Department of Family and Preventive Medicine, and the Division of Public Health), asking faculty to keep these in mind as they reviewed the proposed changes. The final wording of the Mission Statement was generated by the committee with input from the Division Chief and approved by the Division of Public Health faculty. It was then taken to the External Advisory Board for input prior to final adoption. Since then, the missions, value, goals and objectives are reviewed and updated during the Division of Public Health annual retreat. The 2011, Division of Public Health Faculty retreat, which included faculty, staff, Advisory Board members, and SAC representatives, focused on the role of the Division of Public Health as one of the four main components of the Department of Family and Preventive Medicine, the School of Medicine and the University of Utah as a whole. We assessed our opportunities, strengths, weaknesses, challenges, and institutional identity as a foundation for a strategic development plan. This process has continued through faculty and leadership meetings, with participation by our Public Health Student Advisory Community, our External Advisory Board and the Department of Family and Preventive Medicine Executive Committee. This process has provided the basis for a formal strategic planning process that has included better connection with employers of graduates, stabilization of course offerings including scheduling, expanding extramurally funded research and training, increasing cross-institutional partnerships, increasing the number of core Division of Public Health faculty members, and stabilizing educational funding through the adoption of differential tuition. From this process, the objectives listed in table 1.2 were generated to more clearly align our priorities with our Mission. This strategic planning was again revisited during the Division of Public Health September 2012 retreat. New challenges posed by then newly appointed Senior Vice President for Health Sciences, Dr. Vivian Lee, were presented to the Division of Public Health faculty, with a focus on expanding extramural funding and participation on healthcare transformation activities related to the Patient Protection and Affordable Care Act, especially in relation to managing the health of populations and expanding wellness and health promotion activities. This has also involved providing ongoing participation in helping to expand the opportunities for patients to be served by medical homes and supporting University of Utah Hospitals and Clinics efforts to contain costs and improve the quality of care. In this process, more emphasis is being placed on preventive medicine, health promotion, patient self-management education, and measurable improvements in population health [see https://www.youtube.com/user/UofUHealthCare for an illustration of these efforts]. This has provided opportunities for an expanded role for the Division of Public Health based on institutional priorities, including advancing the scholarship of integrating public health and clinical care, especially primary care.
16
f. Description of how the mission, values, goals, and objectives are made available to the program’s constituent groups, including the general public, and how they are routinely reviewed and revised to ensure relevance. The mission, values, goals, and objectives, are available to the general public on the Division of Public Health webpage (currently being updated as part of a University wide webpage update), clearly described on our conference displays posted at Utah Public Health Association (UPHA), America Public Health Association (APHA), and Utah Graduate School Fair. For incoming students, the mission is presented and discussed at the orientation meeting before they start the program. They are also presented periodically in the Division of Public Health bi-annual newsletter. As previously noted, these are reviewed at least annually by faculty, staff, our Student Advisory Committee and community members, especially through our External Advisory Board (with representation from state and local health departments, employer groups, community service providers and major health networks). Further, the mission, values, goals, and objectives are reviewed at the annual Division of Public Health retreat, with recommendations incorporated where appropriate with formal faculty approval. g. Assessment of the extent to which this criterion is met and an analysis of the program’s strengths, weaknesses, and plans relating to this criterion. This criterion is met. Strengths: We have a clear mission statement with obtainable goals, objectives, and values. Our mission reflects the recognition of the interactions and relationships among multiple determinants of health, and that improving heath requires effort from a consortium of disciplines. Our Division is active in instruction, research, and community service. Our graduates become public health academicians and practitioners who have a prevention orientation and are able to assess population needs, implement programs, promote the health of populations, and advance the science of public health. Weaknesses: We have a good Mission Statement, but as we look at what is being defined as the new public health there is a misalignment with our mission statement. It is more linked to the classic public health idea. Plans: We will modify our mission statement to be in line with the new public health definition per “The New Public Health (NPH) is an integrative approach to protecting and promoting the health status of both the individual and the society. The dimensions of the NPH include conceptual, methodological, scientific, political, and moral factors recognizing the interdependency and interrelationship of the health of people, communities, and nations” We will think more about how we address what’s included in this description by Tulchinsky TH, Varavikova EA. What is the “New Public Health”? Public Health Reviews 2010;32:25-53.
17
1.2 Evaluation. The program shall have an explicit process for monitoring and evaluating its overall efforts against its mission, goal and objectives; for assessing the program’s effectiveness in serving its various constituencies; and for using evaluation results in ongoing planning and decision making to achieve its mission. As part of the evaluation proves, the program must conduct an analytical self-study that analyzes performance against the accreditation criteria defined in this document. a. Description of the evaluation processes used to monitor progress against objectives defined in Criterion 1.1.d, including identification of the data systems and responsible parties associated with each objective and with the evaluation process as a whole. If these are common across all objectives, they need be described only once. If systems and responsible parties vary by objective or topic area, sufficient information must be provided to identify the systems and responsible party for each. The Division of Public Health continues to take steps to clarify and implement goals, objectives and measurable targets for the program. Measurable targets associated with each program objectives are summarized in Table 1.2.1, along with an assessment of whether each objective has been ‘Met’ based on the identified outcome measure. These are presented for the 2011-12, 2012-13 and 2013-14 academic years. The leadership of the Division of Public Health has used the results of these assessments to identify areas where improvements can be made. Data to evaluate processes used to monitor progress against objectives are collected by the following responsible parties:
Division Chief Evaluates faculty progress through the annual faculty review meetings and ongoing mentoring of
junior faculty members. The faculty members summarize and discuss their academic focus, resumes (including grants, publications and service), course evaluations, list of advisees, annual and long-term goals, and grant funding plans. Future decisions about faculty hires, courses, and budget issues, take into account the data gathered in these reviews.
Meets with the Chair of the Department of Family and Preventive Medicine at least monthly to assess goals, problem solve, and address anything in need of attention either immediate or for the future for the Division.
Meets with the Division Program Manager for ongoing operational and budgetary review at least monthly.
Meets monthly with the Student Advisory Committee leadership to get a student perspective on Division objectives.
Meets quarterly with the External Advisory Board to provide updates on Division activities and seek guidance in achieving and further developing objects.
Reviews all course evaluations each semester.
Faculty At the monthly faculty meeting, all research projects are reviewed including pilot, collaboration
and consulting, major projects (including in development, submitted, and funded). The information reviewed includes the PI, co-investigators, funding agency, title of the grant, funding amount, and updated status (in review, scored, resubmission). Faculty members inform each other of the type of multidisciplinary collaborations that are in place or are being developed for research projects.
18
CVs are continually updated using the online University of Utah Mission-Based Management system allowing for ongoing review of publications, service, meeting participation, student mentoring, and teaching information.
Participate in various Division committees (described in section 1.5) that evaluate the curriculum, admissions process, student learning (comprehensive and general exams), global health programs, and Division policy.
Participate in research development meetings organized by the Office of Public Health Research.
Are responsible for bringing up any serious issues with students in terms of academic conduct, to the Division Chief or at the faculty meetings for discussion.
Review the status of the PhD students each semester. The Academic Advisor provides a list for the faculty to review with completed requirements. The PhD faculty advisor reports on the status of the student.
Students
During Breakfast with the Chief (a forum for informal student – Division Chief communication) students are invited to prepare questions or state concerns/recommendations that are discussed in the context of the Division’s vision, mission, values, goals, and objectives.
Evaluate content and instructors for all courses completed. Students log into their account on the Campus Information System (CIS), select the Student Course Feedback, and complete the course evaluation up to two weeks after the course has been completed. The student’s identity remains anonymous.
Are given an opportunity to provide feedback through alumni surveys that are distributed annually in fall. This survey was first launched in 2007. This survey is sent to all graduates of the Division of Public Health.
Participate in the Student Advisory Committee, which provides requested and self-generated feedback reflecting student views on programmatic issues including academic and administrative aspects of the Division of Public Health. A SAC representative also participates in Division-wide and faculty meetings to provide feedback regarding recommendations and issues that have an impact on students.
Academic advisor
Collects and tracks on a regular basis, student numbers, enrollment in courses, graduation rates, faculty to student ratios, faculty advisory committees, GPA, and diversity information on all applications that were completed on the online Graduate School Application. Reports are generated every semester, with tailored reports provided as needed.
Monitors student performance so that appropriate actions can be initiated when a student does not get an adequate grade or does not meet standards for non-course degree requirements.
Oversees the alumni survey sent out to graduates for evaluation of the educational program and job placement.
Provides administrative support for the comprehensive and general exams and gives input on student performance to the faculty.
Gives individual counseling to students in coordination with their faculty advisor and graduate committee to guide course selection, degree progress, and steps for addressing any other issues that may be of importance to their academic performance.
Maintains a listing of research opportunities available to students as well as links to relevant faculty members.
19
Administrative Staff Attend Division and faculty meetings, and provide their input on issues as appropriate. Meet with the Division Chief and Associate Division Chief each week as part of the
Administrative Committee to provide feedback on administrative support for all the functions of the Division.
Oversees the research practicum and collects the evaluation forms from the supervisor and the faculty advisor.
Community organizations
Starting spring 2013 the Division has held focus groups to solicit feedback from community partners who are also frequent employers of our graduates. The Division also maintains ties to a variety of community organizations that link our academic activities through engaged-scholarship to issues of importance in the community. These links range from working with the Community Faces of Utah (a multi-cultural consortium that includes leadership from the African, African American, American Indian, Hispanic and Pacific Islander communities as well as the University of Utah and Utah Department of Health) to the Mothers’ Milk Donation Center. Other ongoing partnering includes bi-directional interactions that help shape the activities of the Division of Public Health.
External Advisory Board
This group consists of representation from health departments, community organizations, employer groups, and healthcare systems to provide an external perspective on the performance of the Division of Public Health. This group meets quarterly and has subcommittee meetings on an as needed basis. By-laws are in place to guide the functions of this board. Members of this board are also invited to participate in monthly Division meetings and Division annual retreat.
Multiple responsible parties The Division meetings include; faculty, staff, adjuncts, department heads, SAC members and
advisory committee members. This meeting is held to review progress of the Division, competencies, address any concerns, SAC updates, Grand Rounds announcements in additional to gathering informal feedback, and development updates.
The Global Health working group comprised of Study Abroad Directors and staff support meet monthly to review deadlines for student applications, and study abroad program policies.
Division retreats include faculty, staff, students, and advisory committee members. A theme is selected each year and the Division focuses on evaluating the current status.
b. Description of how the results of the evaluation processes described in Criterion 1.1.a are monitored, analyzed, communicated, and regularly used by managers responsible for enhancing the quality of programs and activities. The results of the evaluation processes that are monitored, analyzed, communicated, and used to enhance the quality of the programs and activities are described below by cross-cutting evaluation processes and in the three core areas of research, education, and service. Cross-cutting evaluation processes The Division Chief and Administrative Program Manager monitor, analyze, and direct communication on the Division budget at least twice a year at the faculty meetings, provide an overview of the Division status at the annual Division retreat, present this information to the External Advisory Board and coordinate budgetary issues with the Department of Family and Preventive Medicine Executive Committee. Any policy change proposals are brought to the relevant committee for discussion and refinement, with final adoption occurring at faculty meetings based on faculty approval.

20
Research Research is largely evaluated by the research projects inventory that is reviewed each month at the faculty meeting and through faculty resumes that include grants and publications. It is also discussed with the Division Chief at the faculty annual review meetings. Increasing the research focus of the Division has been a discussion topic in various faculty meetings and research development meetings. Ideas on how to increase research are brought to the Division Chief who would oversee implementation. Education Any major issues in the educational program that require change in policy or programs, which are raised by any of the responsible parties, would be considered by the relevant committee (curriculum, global health program, comprehensive exam, general exam, policy, admissions) for discussion. A proposal would then be brought to the faculty meeting for discussion and voting. Service Service by students is monitored by the respective programs (global health, UROP, SAC, practicum). A review of the public health and global health grand rounds topics allows us to assess the exposure students have for service opportunities. Service by faculty are monitored within the faculty CVs.
21
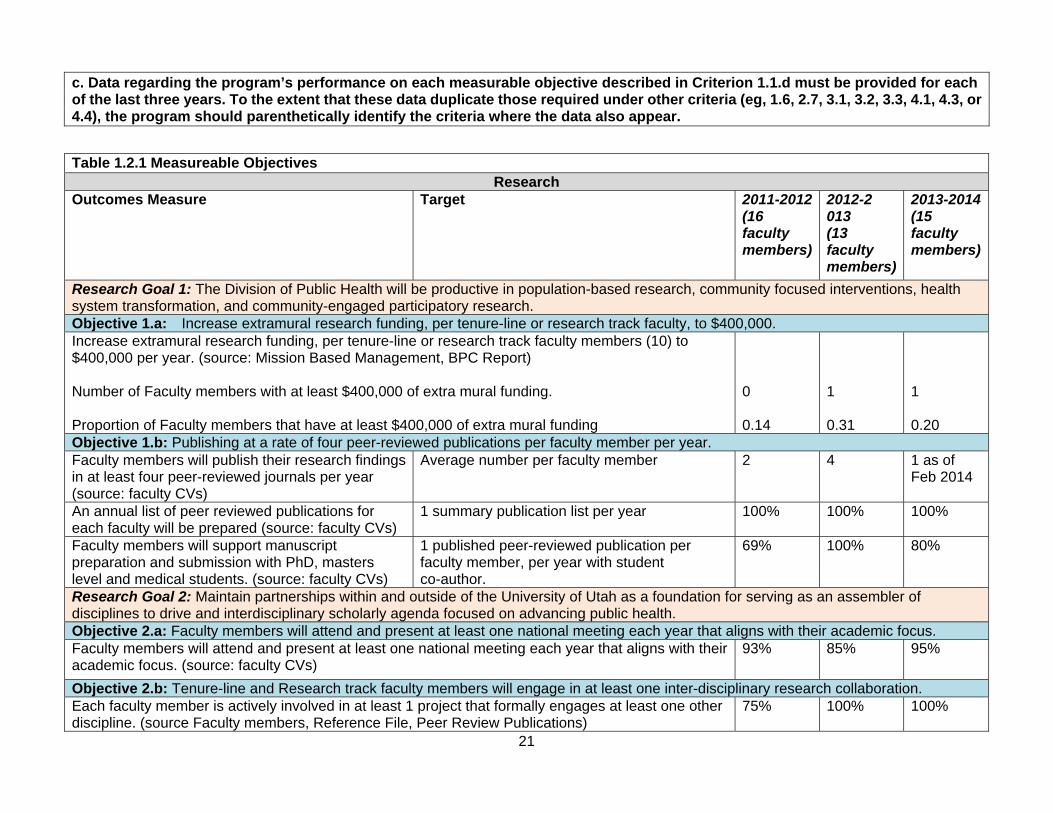
c. Data regarding the program’s performance on each measurable objective described in Criterion 1.1.d must be provided for each of the last three years. To the extent that these data duplicate those required under other criteria (eg, 1.6, 2.7, 3.1, 3.2, 3.3, 4.1, 4.3, or 4.4), the program should parenthetically identify the criteria where the data also appear.
Table 1.2.1 Measureable Objectives Research
Outcomes Measure Target 2011-2012(16 faculty members)
2012-2 013 (13 faculty members)
2013-2014 (15 faculty members)
Research Goal 1: The Division of Public Health will be productive in population-based research, community focused interventions, health system transformation, and community-engaged participatory research. Objective 1.a: Increase extramural research funding, per tenure-line or research track faculty, to $400,000. Increase extramural research funding, per tenure-line or research track faculty members (10) to $400,000 per year. (source: Mission Based Management, BPC Report) Number of Faculty members with at least $400,000 of extra mural funding. Proportion of Faculty members that have at least $400,000 of extra mural funding
0 0.14
1 0.31
1 0.20
Objective 1.b: Publishing at a rate of four peer-reviewed publications per faculty member per year. Faculty members will publish their research findings in at least four peer-reviewed journals per year (source: faculty CVs)
Average number per faculty member 2 4 1 as of Feb 2014
An annual list of peer reviewed publications for each faculty will be prepared (source: faculty CVs)
1 summary publication list per year 100% 100% 100%
Faculty members will support manuscript preparation and submission with PhD, masters level and medical students. (source: faculty CVs)
1 published peer-reviewed publication per faculty member, per year with student co-author.
69% 100% 80%
Research Goal 2: Maintain partnerships within and outside of the University of Utah as a foundation for serving as an assembler of disciplines to drive and interdisciplinary scholarly agenda focused on advancing public health. Objective 2.a: Faculty members will attend and present at least one national meeting each year that aligns with their academic focus. Faculty members will attend and present at least one national meeting each year that aligns with their academic focus. (source: faculty CVs)
93% 85% 95%
Objective 2.b: Tenure-line and Research track faculty members will engage in at least one inter-disciplinary research collaboration. Each faculty member is actively involved in at least 1 project that formally engages at least one other discipline. (source Faculty members, Reference File, Peer Review Publications)
75% 100% 100%
22
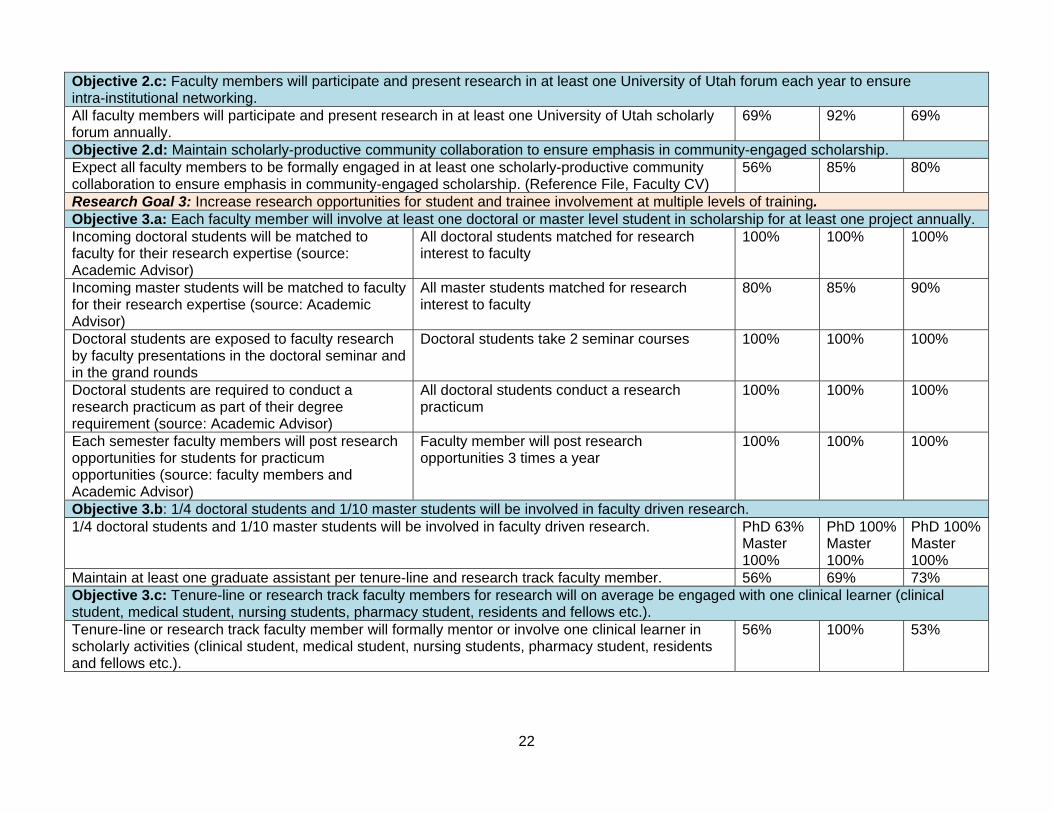
Objective 2.c: Faculty members will participate and present research in at least one University of Utah forum each year to ensure intra-institutional networking. All faculty members will participate and present research in at least one University of Utah scholarly forum annually.
69% 92% 69%
Objective 2.d: Maintain scholarly-productive community collaboration to ensure emphasis in community-engaged scholarship. Expect all faculty members to be formally engaged in at least one scholarly-productive community collaboration to ensure emphasis in community-engaged scholarship. (Reference File, Faculty CV)
56% 85% 80%
Research Goal 3: Increase research opportunities for student and trainee involvement at multiple levels of training. Objective 3.a: Each faculty member will involve at least one doctoral or master level student in scholarship for at least one project annually. Incoming doctoral students will be matched to faculty for their research expertise (source: Academic Advisor)
All doctoral students matched for research interest to faculty
100% 100% 100%
Incoming master students will be matched to faculty for their research expertise (source: Academic Advisor)
All master students matched for research interest to faculty
80% 85% 90%
Doctoral students are exposed to faculty research by faculty presentations in the doctoral seminar and in the grand rounds
Doctoral students take 2 seminar courses 100% 100% 100%
Doctoral students are required to conduct a research practicum as part of their degree requirement (source: Academic Advisor)
All doctoral students conduct a research practicum
100% 100% 100%
Each semester faculty members will post research opportunities for students for practicum opportunities (source: faculty members and Academic Advisor)
Faculty member will post research opportunities 3 times a year
100% 100% 100%
Objective 3.b: 1/4 doctoral students and 1/10 master students will be involved in faculty driven research. 1/4 doctoral students and 1/10 master students will be involved in faculty driven research. PhD 63%
Master 100%
PhD 100%Master 100%
PhD 100% Master 100%
Maintain at least one graduate assistant per tenure-line and research track faculty member. 56% 69% 73% Objective 3.c: Tenure-line or research track faculty members for research will on average be engaged with one clinical learner (clinical student, medical student, nursing students, pharmacy student, residents and fellows etc.). Tenure-line or research track faculty member will formally mentor or involve one clinical learner in scholarly activities (clinical student, medical student, nursing students, pharmacy student, residents and fellows etc.).
56% 100% 53%
23
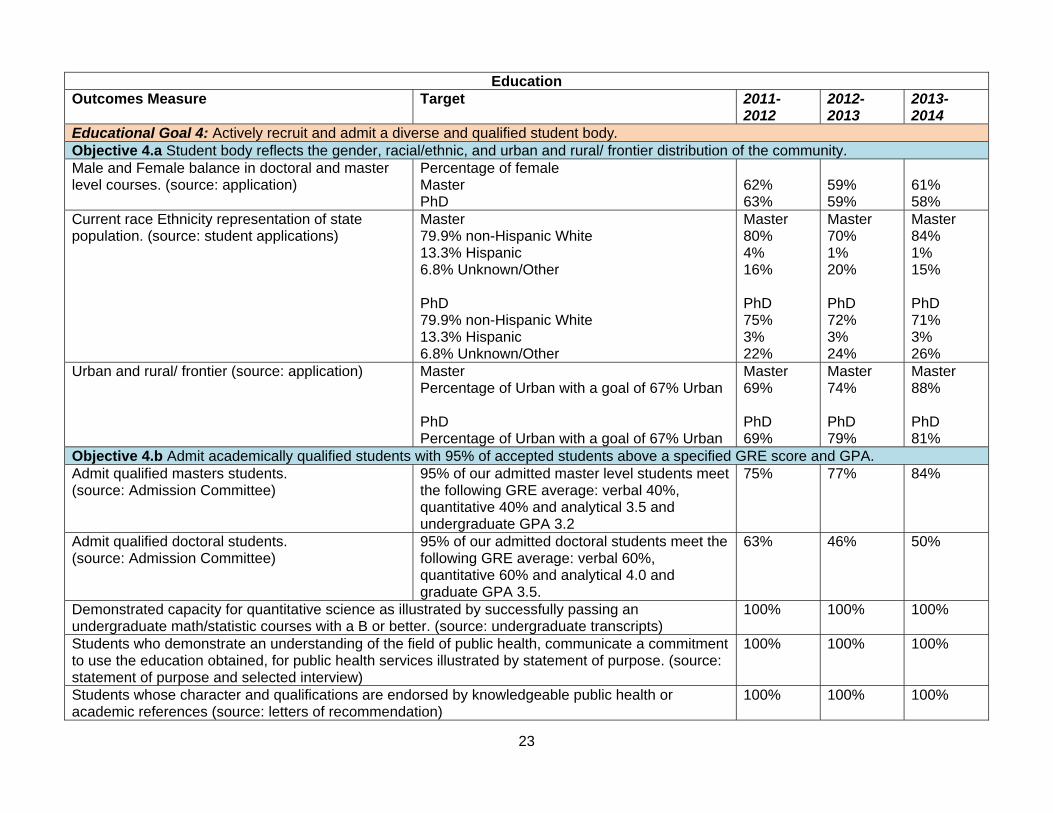
Education Outcomes Measure Target 2011-
2012 2012- 2013
2013- 2014
Educational Goal 4: Actively recruit and admit a diverse and qualified student body. Objective 4.a Student body reflects the gender, racial/ethnic, and urban and rural/ frontier distribution of the community. Male and Female balance in doctoral and master level courses. (source: application)
Percentage of female Master PhD
62% 63%
59% 59%
61% 58%
Current race Ethnicity representation of state population. (source: student applications)
Master 79.9% non-Hispanic White 13.3% Hispanic 6.8% Unknown/Other PhD 79.9% non-Hispanic White 13.3% Hispanic 6.8% Unknown/Other
Master 80% 4% 16% PhD 75% 3% 22%
Master 70% 1% 20% PhD 72% 3% 24%
Master 84% 1% 15% PhD 71% 3% 26%
Urban and rural/ frontier (source: application) Master Percentage of Urban with a goal of 67% Urban PhD Percentage of Urban with a goal of 67% Urban
Master 69% PhD 69%
Master 74% PhD 79%
Master 88% PhD 81%
Objective 4.b Admit academically qualified students with 95% of accepted students above a specified GRE score and GPA. Admit qualified masters students. (source: Admission Committee)
95% of our admitted master level students meet the following GRE average: verbal 40%, quantitative 40% and analytical 3.5 and undergraduate GPA 3.2
75% 77% 84%
Admit qualified doctoral students. (source: Admission Committee)
95% of our admitted doctoral students meet the following GRE average: verbal 60%, quantitative 60% and analytical 4.0 and graduate GPA 3.5.
63% 46% 50%
Demonstrated capacity for quantitative science as illustrated by successfully passing an undergraduate math/statistic courses with a B or better. (source: undergraduate transcripts)
100% 100% 100%
Students who demonstrate an understanding of the field of public health, communicate a commitment to use the education obtained, for public health services illustrated by statement of purpose. (source: statement of purpose and selected interview)
100% 100% 100%
Students whose character and qualifications are endorsed by knowledgeable public health or academic references (source: letters of recommendation)
100% 100% 100%
24
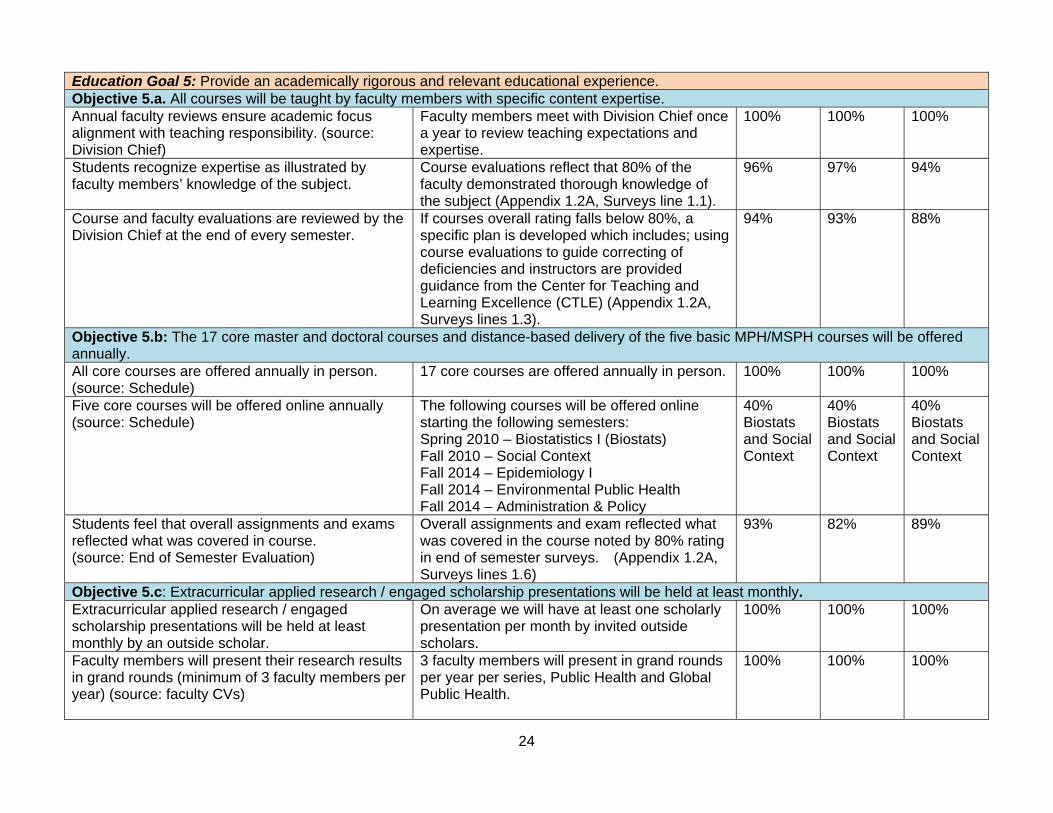
Education Goal 5: Provide an academically rigorous and relevant educational experience. Objective 5.a. All courses will be taught by faculty members with specific content expertise. Annual faculty reviews ensure academic focus alignment with teaching responsibility. (source: Division Chief)
Faculty members meet with Division Chief once a year to review teaching expectations and expertise.
100% 100% 100%
Students recognize expertise as illustrated by faculty members’ knowledge of the subject.
Course evaluations reflect that 80% of the faculty demonstrated thorough knowledge of the subject (Appendix 1.2A, Surveys line 1.1).
96% 97% 94%
Course and faculty evaluations are reviewed by the Division Chief at the end of every semester.
If courses overall rating falls below 80%, a specific plan is developed which includes; using course evaluations to guide correcting of deficiencies and instructors are provided guidance from the Center for Teaching and Learning Excellence (CTLE) (Appendix 1.2A, Surveys lines 1.3).
94% 93% 88%
Objective 5.b: The 17 core master and doctoral courses and distance-based delivery of the five basic MPH/MSPH courses will be offered annually. All core courses are offered annually in person. (source: Schedule)
17 core courses are offered annually in person. 100% 100% 100%
Five core courses will be offered online annually (source: Schedule)
The following courses will be offered online starting the following semesters: Spring 2010 – Biostatistics I (Biostats) Fall 2010 – Social Context Fall 2014 – Epidemiology I Fall 2014 – Environmental Public Health Fall 2014 – Administration & Policy
40% Biostats and Social Context
40% Biostats and Social Context
40% Biostats and Social Context
Students feel that overall assignments and exams reflected what was covered in course. (source: End of Semester Evaluation)
Overall assignments and exam reflected what was covered in the course noted by 80% rating in end of semester surveys. (Appendix 1.2A, Surveys lines 1.6)
93% 82% 89%
Objective 5.c: Extracurricular applied research / engaged scholarship presentations will be held at least monthly. Extracurricular applied research / engaged scholarship presentations will be held at least monthly by an outside scholar.
On average we will have at least one scholarly presentation per month by invited outside scholars.
100% 100% 100%
Faculty members will present their research results in grand rounds (minimum of 3 faculty members per year) (source: faculty CVs)
3 faculty members will present in grand rounds per year per series, Public Health and Global Public Health.
100% 100% 100%
25
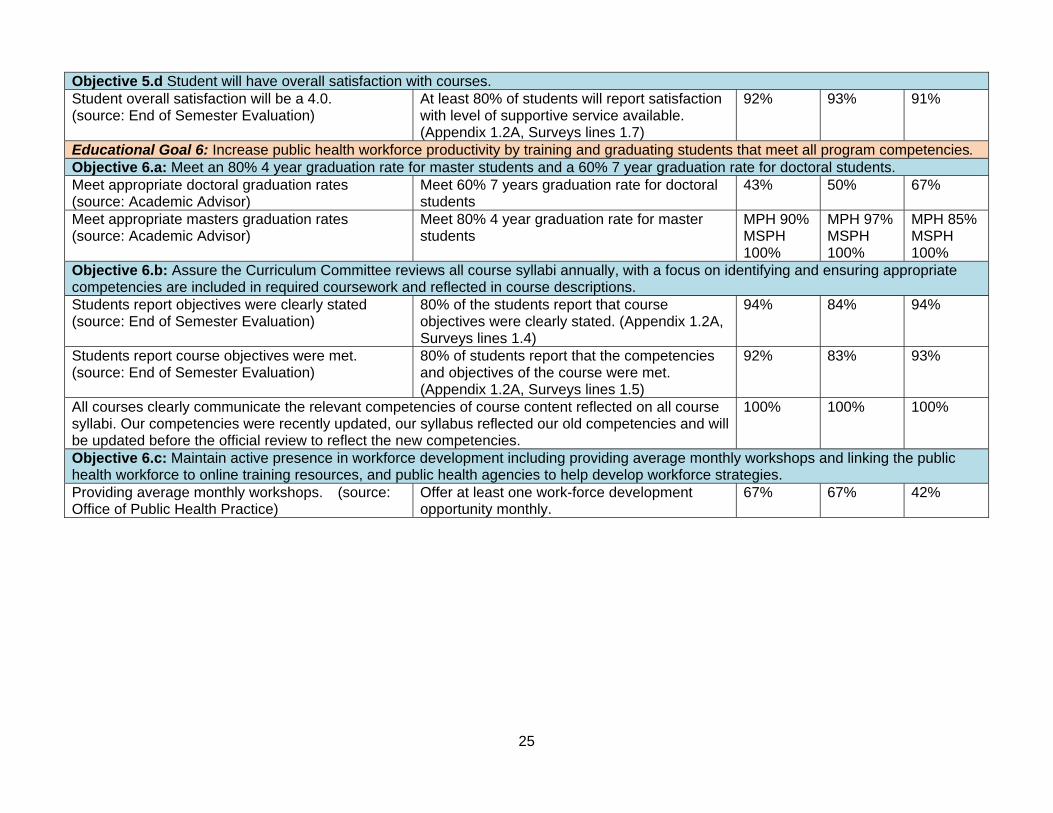
Objective 5.d Student will have overall satisfaction with courses. Student overall satisfaction will be a 4.0. (source: End of Semester Evaluation)
At least 80% of students will report satisfaction with level of supportive service available. (Appendix 1.2A, Surveys lines 1.7)
92% 93% 91%
Educational Goal 6: Increase public health workforce productivity by training and graduating students that meet all program competencies. Objective 6.a: Meet an 80% 4 year graduation rate for master students and a 60% 7 year graduation rate for doctoral students. Meet appropriate doctoral graduation rates (source: Academic Advisor)
Meet 60% 7 years graduation rate for doctoral students
43% 50% 67%
Meet appropriate masters graduation rates (source: Academic Advisor)
Meet 80% 4 year graduation rate for master students
MPH 90% MSPH 100%
MPH 97% MSPH 100%
MPH 85% MSPH 100%
Objective 6.b: Assure the Curriculum Committee reviews all course syllabi annually, with a focus on identifying and ensuring appropriate competencies are included in required coursework and reflected in course descriptions. Students report objectives were clearly stated (source: End of Semester Evaluation)
80% of the students report that course objectives were clearly stated. (Appendix 1.2A, Surveys lines 1.4)
94% 84% 94%
Students report course objectives were met. (source: End of Semester Evaluation)
80% of students report that the competencies and objectives of the course were met. (Appendix 1.2A, Surveys lines 1.5)
92% 83% 93%
All courses clearly communicate the relevant competencies of course content reflected on all course syllabi. Our competencies were recently updated, our syllabus reflected our old competencies and will be updated before the official review to reflect the new competencies.
100% 100% 100%
Objective 6.c: Maintain active presence in workforce development including providing average monthly workshops and linking the public health workforce to online training resources, and public health agencies to help develop workforce strategies. Providing average monthly workshops. (source: Office of Public Health Practice)
Offer at least one work-force development opportunity monthly.
67% 67% 42%
26
Service Outcomes Measure Target 2011-
2012 2012- 2013
2013- 2014
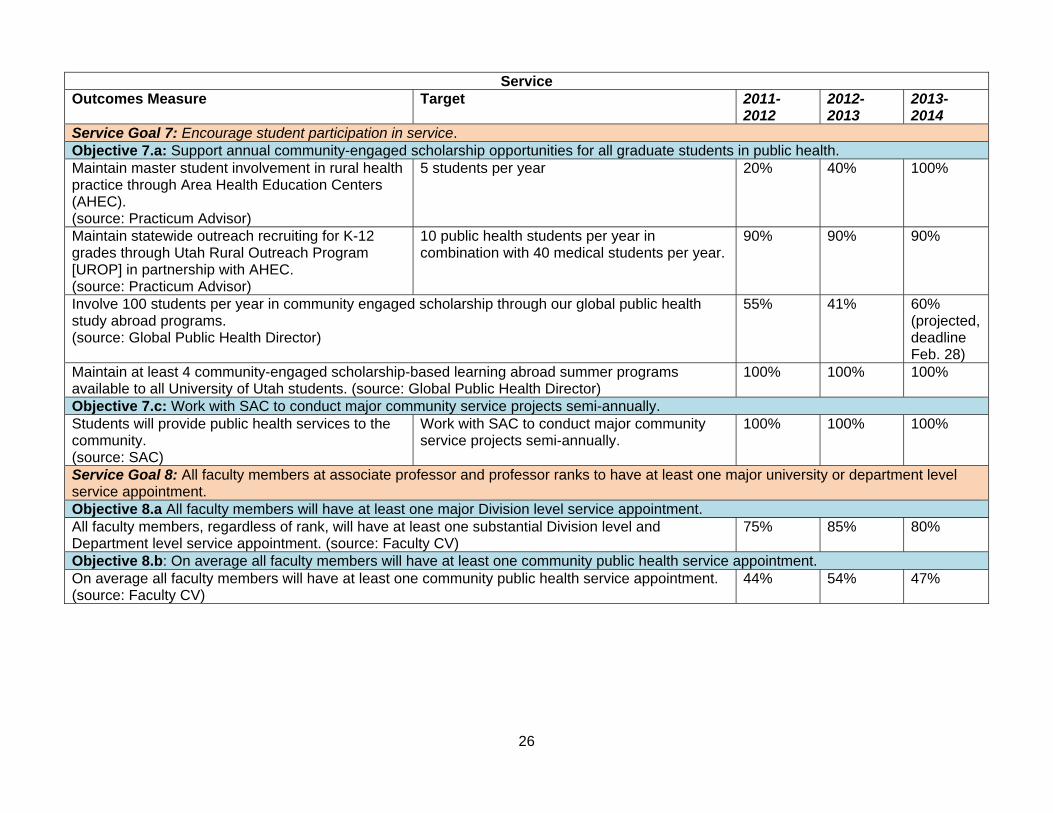
Service Goal 7: Encourage student participation in service. Objective 7.a: Support annual community-engaged scholarship opportunities for all graduate students in public health. Maintain master student involvement in rural health practice through Area Health Education Centers (AHEC). (source: Practicum Advisor)
5 students per year 20% 40% 100%
Maintain statewide outreach recruiting for K-12 grades through Utah Rural Outreach Program [UROP] in partnership with AHEC. (source: Practicum Advisor)
10 public health students per year in combination with 40 medical students per year.
90% 90% 90%
Involve 100 students per year in community engaged scholarship through our global public health study abroad programs. (source: Global Public Health Director)
55% 41% 60% (projected, deadline Feb. 28)
Maintain at least 4 community-engaged scholarship-based learning abroad summer programs available to all University of Utah students. (source: Global Public Health Director)
100% 100% 100%
Objective 7.c: Work with SAC to conduct major community service projects semi-annually. Students will provide public health services to the community. (source: SAC)
Work with SAC to conduct major community service projects semi-annually.
100% 100% 100%
Service Goal 8: All faculty members at associate professor and professor ranks to have at least one major university or department level service appointment. Objective 8.a All faculty members will have at least one major Division level service appointment. All faculty members, regardless of rank, will have at least one substantial Division level and Department level service appointment. (source: Faculty CV)
75% 85% 80%
Objective 8.b: On average all faculty members will have at least one community public health service appointment. On average all faculty members will have at least one community public health service appointment. (source: Faculty CV)
44% 54% 47%

27
d. Description of the manner in which the self-study document was developed, including effective opportunities for input by important program constituents, including institutional officers, administrative staff, faculty, students, alumni, and representatives of the public health community. The self-study document was developed by the CEPH accreditation committee (Courtney DeMond, David Sundwall and Mia Hashibe). The committee has been meeting weekly since mid-October 2012. The committee members consulted with: • Faculty - through email surveys, discussion at the monthly faculty meetings, and in depth discussions
at the annual Division retreat. Faculty members were contacted by email for detailed information that was required for the self-study. In the annual Division retreat (May 2013), the faculty discussed the targets of the objectives and targets for research, education and service.
• Students - in person, with a survey, in focus group meetings. The survey gathers information on what type of employment the graduates find after completing their degree program.
• Administrative staff - in person, in focus group meetings and at the annual Division retreat. Administrative staff contributed greatly in gathering information on the faculty and the program from previous documents and online CVs. They also contributed to the discussion of the objectives and targets for research, education, and service at the annual retreat.
• Alumni and representatives of the public health community – through online surveys, in person and at a focus group lunch meeting held in April 2013 (Appendix 1.2B). The focus group lunch meeting for employers of public health graduates was held to discuss the competencies observed by the employers, and to discuss what areas of knowledge and skills could be improved to better serve the major employers of public health graduates.
e. Assessment of the extent to which this criterion is met, and an analysis of the program’s strengths, weaknesses, and plans relating to this criterion. This criterion is met. Strengths: The strengths of our evaluation process are that it is diverse in the responsible parties including: the Division Chief, faculty, students, the Academic Advisor, staff, community organizations, and external advisory board. We have many important faculty committees that oversee various aspects of our program including admissions, administration, curriculum, and policy. The Office of Public Health Research is responsible for evaluating and increasing the research activities within the Division. Changes to policy are discussed at the faculty meetings and voted on, assuring a transparent process that provides for opportunity for input from both faculty and staff. The annual Division retreat is also an important opportunity for the Division to review the program and discuss new ideas for improving the program. Weaknesses: Though service by students and faculty are evaluated by the respective programs or on faculty CVs, an overall Division process to enhance the quality of programs and activities is not available. Plans: We would like to evaluate how many students took our undergraduate Global Health course, applied, and were accepted into the Masters of public health program. We will also evaluate how many Honors College Students (undergraduates) apply and are accepted into the Master of public health program. We will also develop a plan to review and oversee the service in the Division overall.
28
1.3 Institutional Environment. The program shall be an integral part of an institution of higher education. a. A brief description of the institution in which the program is located, and the names of accrediting bodies (other than CEPH) to which the institution responds. The University of Utah, located in Salt Lake City in the foothills of the Wasatch Mountains, is the flagship institution of higher learning in Utah. Founded in 1850, it serves over 31,000 students from across the U.S. and the world. There are over 72 major subjects at the undergraduate level and more than 90 major fields of study at the graduate level, including law and medicine. The University of Utah School of Medicine combines teaching, research, and clinical expertise to train tomorrow's physicians for the rapidly changing world of medicine. With a faculty of more than 1,000 physicians and researchers and 22 clinical and basic-science departments, the School of Medicine trains the majority of Utah physicians, whether it is to receive an M.D. degree, residency or fellowship specialty training. The School of Medicine is also widely recognized for interdisciplinary research in the genetics of disease, cancer, biomedical informatics, infectious diseases, and other areas of medicine, including public health. The University of Utah is accredited by the Northwest Commission on Colleges and Universities (NWCCU). The University was last evaluated in fall 2012, and their next evaluation will be fall 2015.
The School of Medicine, medical degree is accredited by Accreditation Council for Continuing Medical Education (ACCME). They were last accredited in 2012 and their next accreditation will be 2020.
The Division of Public Health is one of the four primary organizational entities within the Department of Family and Preventive Medicine, the other three Divisions include Occupational and Environmental Health, Physician Assistant Studies, and Family Medicine. The Division of Public Health has played a major role in research, education, and service within the School of Medicine for the past 35 years.
For a list of all Colleges/Department or Programs at the University (Appendix 1.3A.)
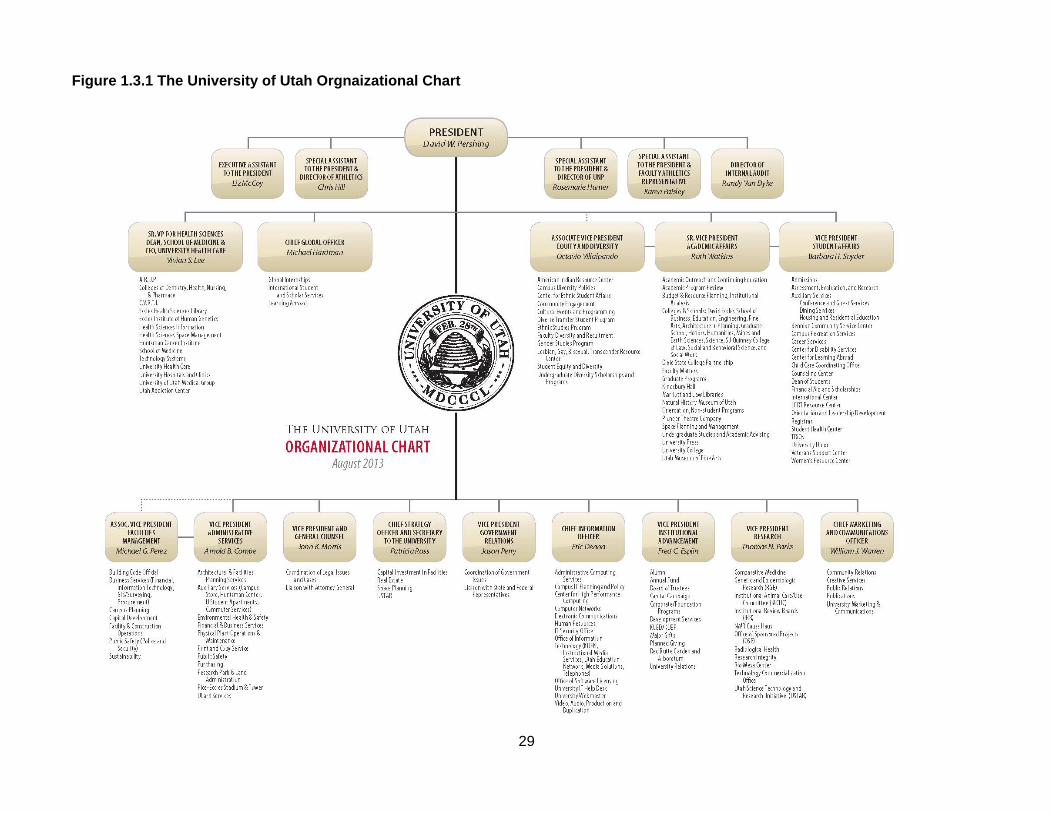
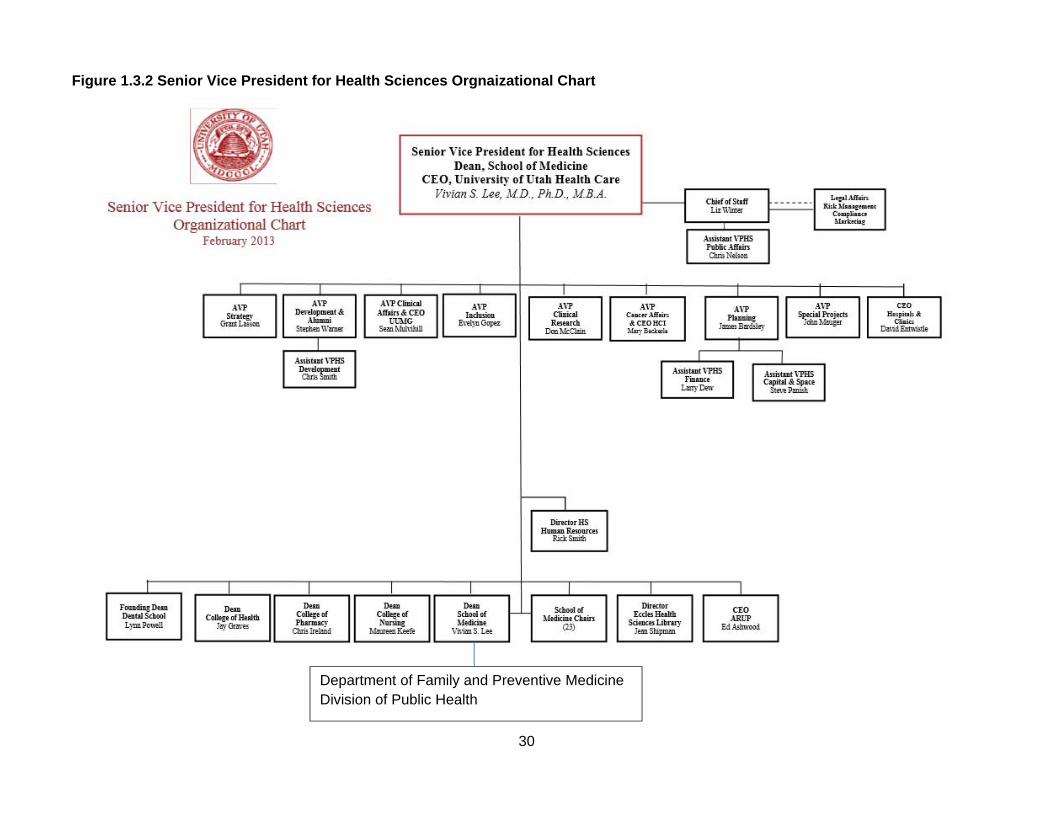
b. One or more organizational charts of the university indicating the program’s relationship to the other components of the institution, including reporting lines and clearly depicting how the program reports to or is supervised by other components of the institution. As indicated in the introduction of this self-study document, the Division of Public Health is a part of the University of Utah School of Medicine, which is under the umbrella of Health Sciences within the University of Utah as shown in the figures on the following pages.
29
Figure 1.3.1 The University of Utah Orgnaizational Chart
30
Figure 1.3.2 Senior Vice President for Health Sciences Orgnaizational Chart
Department of Family and Preventive Medicine Division of Public Health
31
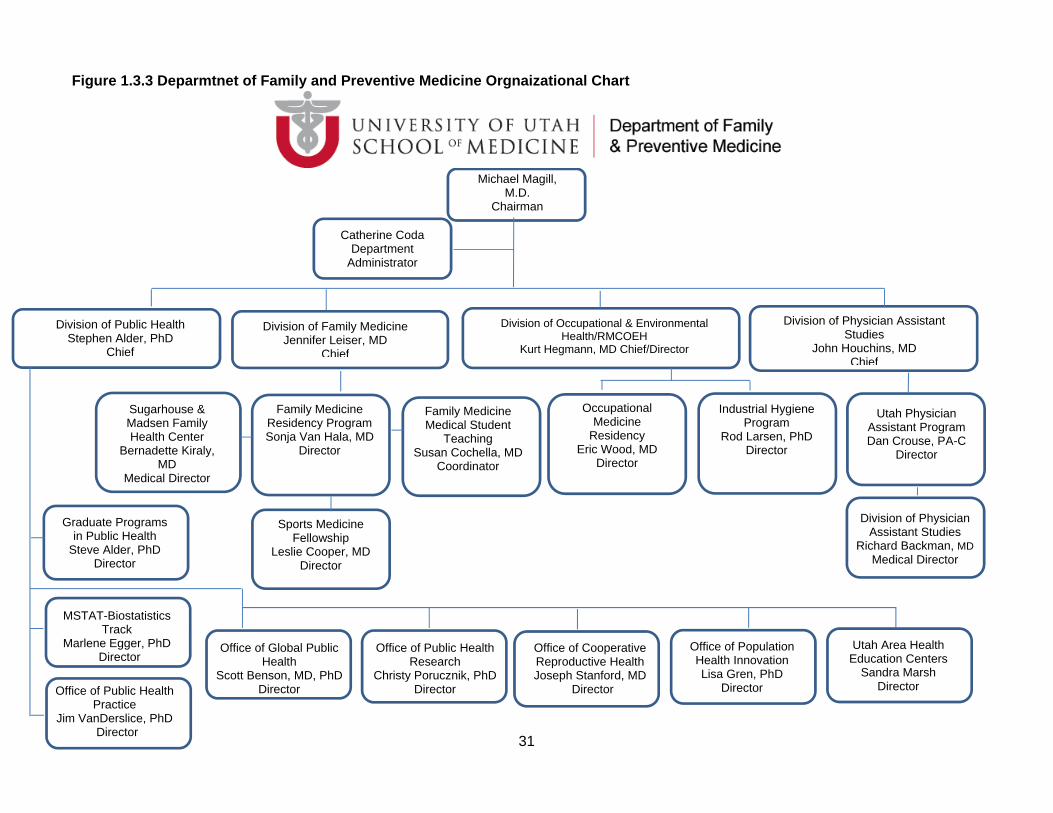
Figure 1.3.3 Deparmtnet of Family and Preventive Medicine Orgnaizational Chart
Michael Magill, M.D.
Chairman
Sugarhouse & Madsen Family Health Center
Bernadette Kiraly, MD
Medical Director
Division of Public Health Stephen Alder, PhD
Chief
Division of Family Medicine Jennifer Leiser, MD
Chief
Division of Occupational & Environmental Health/RMCOEH
Kurt Hegmann, MD Chief/Director
Catherine Coda Department
Administrator
Division of Physician Assistant Studies
John Houchins, MD Chief
Occupational Medicine
Residency Eric Wood, MD
Director
Family Medicine Medical Student
Teaching Susan Cochella, MD
Coordinator
Family Medicine Residency Program Sonja Van Hala, MD
Director
Utah Physician Assistant Program Dan Crouse, PA-C
Director
Industrial Hygiene Program
Rod Larsen, PhD Director
Sports Medicine Fellowship
Leslie Cooper, MD Director
Division of Physician Assistant Studies
Richard Backman, MD Medical Director
Graduate Programs in Public Health
Steve Alder, PhD Director
Office of Global Public Health
Scott Benson, MD, PhD Director Office of Public Health
Practice Jim VanDerslice, PhD
Director
MSTAT-Biostatistics Track
Marlene Egger, PhD Director
Office of Public Health Research
Christy Porucznik, PhD Director
Office of Cooperative Reproductive Health Joseph Stanford, MD
Director
Utah Area Health Education Centers
Sandra Marsh Director
Office of Population Health Innovation Lisa Gren, PhD
Director
32
c. Description of the program’s involvement and role in the following: Budgeting and resource allocation, including budget negotiations, indirect cost recoveries, Distribution of tuition and fees, and support for fund-raising Each department within the School of Medicine submits an annual budget for the fiscal year which starts on July 1st and ends June 30th. In addition to the tuition funds that our organization receives, in the form of state appropriated funds, we instituted a tuition differential in 2008 to secure additional resources to sustain our organization and programs.
An annual budget is submitted each spring with estimates of financial needs during the following fiscal year. The University of Utah’s fiscal year is July 1st through June 30th. The budget is submitted in accordance with the University of Utah’s School of Medicine budget guidelines which follow University policies and procedures. The funds allocated to the university by legislative appropriation are budgeted in accordance with legislative intent and approved by the State Board of Regents. University departments follow the budget guidelines issued from the Office of Budget and Institutional Analysis. The School of Medicine Dean’s office provides departments with state appropriated budget figures in early spring. Budgets are submitted to the School of Medicine Dean’s Office in accordance with the annual budget timeline. The entire budget package including the budget narrative, goals for upcoming year, faculty composition, gender analysis, research portfolio, and faculty salary allocation report must be submitted together on the due date specified. The University of Utah, School of Medicine has recently been using Budget Planning Consolidation (BPC) System software to prepare the budget. The BPC system incorporates historical data to make multiple years of information easily accessible. The Dean’s office reviews budgets for accuracy and completeness and works with the departments to correct any problems and clarify questions. The budgets are then forwarded to the Senior Vice President and the Mission-Based Management Advisory Committee (MBMAC) for review. Each department is responsible to present their budget to the MBMAC on a specified date. Upon review and after any corrections, the Vice President will notify each department in writing that their budget has been approved. During the fiscal year, each department will continue to submit reports explaining any major variances between budget and actual operating results. After proposed budgets are approved, departments are notified before July 1st of the amount allocated for its use during the ensuing fiscal year.
http://healthsciences.utah.edu/mbm/internal/budgetProcess/ http://regulations.utah.edu/administration/3-002.php Personnel recruitment, selection, and advancement, including faculty and staff - The faculty hiring process at the University of Utah is supervised by different offices to ensure compliance with federal and state regulations and recruit a diverse pool of candidates. The Office for Equal Opportunity and Affirmative Action ensures that federal and state reporting requirements are met. For the Health Sciences Colleges and other health science academic departments and programs, oversight is provided by The Office of Faculty Affairs in the Vice President for Health Sciences Office.
The Office of HSC Faculty Affairs strives to meet three goals in faculty recruitment:
Provide information to help departments recruit a diverse pool of candidates. Ensure that federal, state, and University regulations are followed in recruitment and job offers. Provide information and resources to assist departments in attracting and securing outstanding
candidates.
We have contracted with PeopleAdmin, a vendor who specializes in higher education. All faculty, staff, and student job postings and applications have been processed using PeopleAdmin since fall 2011. PeopleAdmin is accessed through the University's Campus Information System. Reference: http://medicine.utah.edu/facultyadmin/policy/recruitment/index.htm
33
The University of Utah complies with all state and federal laws regulating equal opportunity, nondiscrimination, and affirmative action in employment. As an institution we believe in the educational value of a diverse student body, staff, and faculty population as essential for the future growth and success of the University of Utah as well as the state of Utah. A campus population that reflects all aspects of diversity (experience, skills, socioeconomic background, race/ethnicity, gender, sexual orientation, gender identity/expression, disability, military service, color, religion, national origin, etc.) broadens and strengthens the university’s instructional and research programs. The University of Utah is making strides to achieve many aspects of diversity in our student population. However, we have not been as successful in attaining racial, ethnic and gender diversity within our faculty. Institutional leadership, as well as national research, indicates extensive research universities must develop a greater awareness and outreach in order to fully diversify their faculty. The University of Utah leadership is committed to improving the diversity of the campus and therefore, diversity and retention of faculty are valued.
Advertising -- Language, placement, and requirements Reference: http://medicine.utah.edu/facultyadmin/policy/recruitment/index.htm
A faculty search provides Divisions with the opportunity to assess current strengths and needs, and to create a search process accordingly. Position descriptions should be flexible documents that seek to strengthen the Division’s research, teaching, and service missions. New descriptions for each search are created to reflect the needs of the unit at the time of the search. In order to attract the widest range of qualified candidates, it is recommended that descriptions be as broad as possible while still consistent with the needs of the Division. Search committees and Division hiring authorities should thoroughly consider the qualifications that are necessary to the position and carefully distinguish between minimum qualifications and preferences. Language in the job description or advertisement that may have the effect of excluding applicants from underrepresented communities, women or disabled applicants are avoided. The Division of Public Health follows the usual and customary procedures outlined by the University of Utah School of Medicine for faculty advertising search and candidate selection. Postings for the position are through mechanisms that are connected with a diverse potential applicant pool to reach a diverse audience (including but not limited to the American Public Health Association Career Mart, the Insight Into Diversity Journal, and the Chronicle of Higher Education.) Further, we adhere to University of Utah Equal Opportunity guidelines to protect against discrimination in the hiring process. A diverse search committee of five members (3 Division faculty members and 2 external faculty members) is assembled to bring together a balanced array of perspectives when reviewing applicants and making hiring recommendations. After reviewing the applicants the search committee will submit their recommendations to the Division Chief for his review and approval. The Division Chief will then present the search committees recommendations to the faculty for their review and approval. Candidates are then contacted to arrange travel (if necessary) to our facility for in-person interviews and a lunchtime presentation. Promotion in rank is the acknowledgment by the University of continuing and increasing professional competence and responsibility in teaching, research and creative work, and University and public service. In each department all tenure-line faculty members of equal or higher rank than that proposed for the candidate for promotion are eligible to participate in the consideration of and to vote on recommendations in individual cases on matters of promotion. Other faculty members may participate in the consideration of candidates for promotion if allowed by department rules, but may not vote.
34
Regarding Tenure-Line Faculty - Tenure-line faculty in the Department of Family and Preventive Medicine undergo mid-probationary reviews in the 3rd and 5th years. Promotion, to Associate Professor or “full” Professor, and the awarding of tenure occurs in the 7th year. Tenured faculty members are formally reviewed every 5 years thereafter. Each candidate for retention, promotion, or tenure shall be given at least 30 days advance notice of the department RPT advisory committee meeting and an opportunity to submit any information the candidate desires the committee to consider. Regarding Career-Line Faculty (Clinical, Research, & Lecturer Tracks) - Full time career-line faculty in the Department of Family and Preventive Medicine undergo formal reviews in the 3rd and 6th years of appointment to promote the professional development of the faculty member and to ensure continued quality performance, and every 5 years thereafter. Promotions (reappointment at a higher rank) may occur when a faculty member, in consultation with their Division Chief, determines that criteria at rank have been met. Academic standards and policies, including establishment and oversight of curricula - Academic standards and policies are established from the University of Utah Academic Standard as well as the program's policies and guidelines, which can all be found at (http://medicine.utah.edu/dfpm/divisionph/current/Policies_Guidelines.pdf). For establishment and oversight of curricula, there is a committee (Jim VanDerslice, Courtney DeMond, and Staci Wallace). d. If a collaborative program, descriptions of all participating institutions and delineation of their relationships to the program. The University of Utah is not a collaborative program. e. If a collaborative program, a copy of the formal written agreement that establishes the rights and obligations of the participating universities in regard to the program’s operation. The University of Utah is not a collaborative program. f. Assessment of the extent to which this criterion is met and an analysis of the program’s strengths, weaknesses and plans relating to this criterion. This criterion is met. Strengths: Our program is an integral part of an accredited institution of higher education, the University of Utah. The faculty, staff, and students maintain important relationships within the department, across the School of Medicine, and throughout the University. We have a high degree of discretion in our budgeting and resource allocation, and have been active in fund-raising. Weaknesses: As we continue to grow our education, research, and service mission, we are consistently reviewing our budget to strategically plan for growth of staffing and faculty to support our endeavors. State financial support has continued to decline over the years and we have had to plan for other financial resources such as research grants, consulting, and development/donor funds. We receive 7.5% of returned overhead from our overall research indirect costs, which is primarily used to support infrastructure such as phones, building maintenance, and lighting. Our challenge is to strategically access and utilize other resource sources to support the needed increases in our research infrastructure and to find investment resources to support our competitiveness in accessing extramural funding.

35
We acknowledge the need to work on our diversity. We have not been as successful in attaining racial, ethnic and gender diversity within our faculty. Plans: We are working to grow our extramurally funded research while also bringing in more contracts and consultation work which provide more flexible resources. We are also working to access more in the way of planning grants and intramural funding that supports the type of infrastructure development we need to facilitate our targeted growth in research. We are also working with our department leadership to access resources for the startup funding for strategic faculty hires. We have also initiated a Diversity Committee with the specific charge for developing a strategic plan to insure that we achieve appropriate representation across students, staff and faculty, with the initial priority to develop a plan for improving Hispanic representation.
36
1.4 Organization and Administration. The program shall provide an organizational setting conducive to public health learning, research, and service. The organizational setting shall facilitate interdisciplinary communication, cooperation, and collaboration that contribute to achieving the program’s public health mission. The organizational structure shall effectively support the work of the program’s constituents. a. One or more organizational charts delineating the administrative organization of the program, indicating relationships among its internal components. Please see Figure 1.4.1 & 1.4.2 on the next page for the Division of Public Health Organizational Chart and the Offices within the Division. b. Description of the manner in which interdisciplinary coordination, cooperation and collaboration occur and support public health learning, research and service. The Division of Public Health enjoys a high degree of collaboration within its programs. Communication and coordination is supported through a series of meetings, including: Division-wide meetings each semester, monthly faculty and key staff meetings, weekly meetings of faculty directing our specific Offices/activities, and weekly administrative meetings. The monthly faculty meetings provide a venue for initiating collaboration on new projects, research opportunities, and service efforts. Any faculty member can add items to the agenda. Admissions, PhD student progress reviews, PhD concept proposal reviews, curriculum issues, and reports on the Comprehensive and General exams are discussed in the faculty meetings. We also conduct a formal review of all research development efforts as well as progress on on-going research at the faculty meetings. A yearly day-long Division Retreat provides an opportunity to reflect on the progress made during the previous year and develop a strategic plan for the coming year. These discussions include faculty from all disciplines. In addition, we hold weekly informal research meetings, where faculty members present research ideas for peer-review and discussion. This has led to new research collaborations between investigators both within and outside the Division. Cross-disciplinary collaboration is one of our Measureable Objectives (Objective 2b.) Internal Division committees (e.g., admissions, curriculum, general exam, comprehensive exam) include faculty with diverse backgrounds and at all levels of appointment. This fosters interdisciplinary coordination and cooperation in our educational program. The Division also takes a proactive role to foster cooperation and collaboration with partners of academia.
Utah Rural Outreach Program (UROP) is an ongoing student lead program currently in its tenth year. This is a program initiated and operated primarily by volunteer students between the University of Utah, School of Medicine and Division of Public Health. This outreach program directly addresses the issue of disproportionately low numbers of health care providers in rural and frontier Utah through the promotion of health care educational programs to rural high school students. Through this program, volunteer students travel to rural high schools and give presentations to educate high school students, teachers, and counselors about careers in health care, requirements for admission into different health care educational programs, and the need for different health professions in rural communities.

37
Utah’s Area Health Education Centers (AHEC) consists of three regional centers in Utah, where students can be placed in practica or internships with local health departments, and supported with funds for expenses by the AHEC. AHEC’s mission is to improve access to health care through education. It fulfills its mission through programs developed to enhance the diversity of Utah’s health care work force and improve access to care for urban and rural medically underserved populations through appropriate distribution of health care providers. Its programs are developed under three main focal areas:
1. Recruit youth from Utah’s minority and disadvantaged populations into health-related careers.
2. Provide educational opportunities for students in health professions training programs in community-based clinical settings largely serving Utah’s medically underserved residents.
3. Retain health professionals practicing in Utah’s medically underserved communities through convenient professional development opportunities and health-related community advocacy and leadership.
Southwest Regional Public Health Training Center (SRPHTC) In August 2010, we joined with
the University of California Los Angeles, Fielding School of Public Health (UCLA) to form the Southwest Regional Public Health Training Center (SRPHTC). This collaboration enhanced our ability to systematically assess training needs and to develop additional competency sets by which to assess needs in various specialty areas (Health education, environmental health, and epidemiology). All assessment activities were based on the Council on Linkages Core Public Health Competencies.
Huntsman Cancer Institute (HCI) is a National Cancer Institute-Designated Cancer Center, which means it meets the highest national standards for cancer care and research and receives support for its scientific endeavors. The Division works with the HCI through joint appointments of faculty (Dr. Hashibe, Dr. Wu), hosting conferences together (Hope, Healing and Health – May 7-9, 2013), and collaborating on projects (Native Americans cancer screening projects).
International Head and Neck Cancer Epidemiology (INHANCE) consortium was established in 2004, based on the collaboration of research groups leading large molecular epidemiology studies of head & neck cancer that are on-going or have been recently completed. When taken collectively, questionnaire data on over 26,000 cases & 34,000 controls, and biological samples from a majority of the study population would be available. Two faculty members from the Division (Drs. Hashibe and Lee) coordinate the consortium by managing the pooled data, organizing the annual meetings and maintaining the member area webpage.
Utah Population Database (UPDB) is one of the world’s richest sources of in-depth information that supports research on genetics, epidemiology, demography, and public health. For more than 30 years, researchers at the University of Utah and other institutions have used UPDB to identify and study individuals and families that have higher than normal incidence of cancer or other diseases, to analyze patterns of genetic inheritance, and to identify specific genetic mutations. The Division has multiple projects based on UPDB, including topics such as reproductive and cancer epidemiology. Dr. VanDerslice serves on the committee that reviews and approves data requests.
Utah Partnership for Healthy Weight (UPHW) – Collaboration with the Utah Partnership for Healthy Weight (UPHW) – a non-for-profit collaborative of almost 50 organizations committed to addressing the obesity epidemic. Public health students have worked with the Executive Director to sponsor educational events and community activities. This organization has also provided opportunities for collaboration with public health students at Brigham Young University on “healthy weight” initiatives.
38
Learning Abroad Partner collaboration - We implement a unique model that we have created
over the last decade that is based upon a long-term partnership with in-country government representatives, university and hospital faculty, and local village elders and residents. We provide student, professor, and doctor exchanges with partner universities and hospitals worldwide while providing all participants a deeper understanding of each other’s areas of expertise. In collaboration with our partners, we assess and prioritize local needs, evaluate potential solutions, prioritize projects and create sustainable programs that we extend into local communities in cooperation with partner universities, hospitals, local governments and civic leaders. We evaluate success, relevance and worthiness of each program for replication in other parts of the country and in other countries around the world where similar need exists.
All Payers Claim Database – Utah All Payer Claims Database (APCD) is a compilation of health care claims records of non-elderly (<65 years old) patients in Utah, publicly administered through the Utah Department of Health, which incorporates a comprehensive profile of healthcare utilization, regardless of source of payment (including Medicaid). This database has the capacity to construct an accurate and comprehensive longitudinal profile of cost of health care for any cohort of patients in Utah. Dr. Kim sits on the Utah Health Data Committee that has oversight over the use of this data resource, and this has allowed us to develop a close collaboration with the administrators of this database.
Utah Statewide Immunization System (USIIS) - The Utah Statewide Immunization Information System (USIIS) is a free, confidential, web-based information system that contains immunization histories for Utah residents of all ages. USIIS is designed to help health care providers track immunization information for patient care. It consolidates immunizations from all providers into one centralized record. Only authorized users, such as health care providers, schools, and public programs have access to USIIS. USIIS is populated with birth records of infants (through a link with electronic birth records) and immunization records from public and private healthcare providers.
Community Faces of Utah (CFU) - The Community Faces of Utah believes it is important to make informed, preventive healthcare decisions for ourselves, our children, our families, and our friends. By increasing our knowledge we become empowered to improve health for our families and our community. CFU interfaces for diverse community organizations and institutions to fruitfully dialogue and collaborate to build trust, learn from each other, and work together to enhance our communities' health.
Utah public health agencies- We have strong relationships with public health practice agencies in Utah, both at the state and local levels. We have worked on collaborate projects including trainings, assessment of workforce competency and training needs, development of training workshops and videos, and training needs assessments. We have also provided technical assistance on an ad hoc basis in areas of environmental epidemiology, maternal and child health, and mapping health data.
o Utah Department of Health (UDOH) (state health department), o Local health districts: Bear River Health Department, Weber-Morgan Health Department,
Davis County Health Department, Summit County Health Department, Salt Lake County Health Department, Wasatch County Health Department, Tricounty Health Department, Tooele County Health Department, Utah County Health Department, Central Utah Public Health Department, Southeastern Utah District Health Department, Southwest Utah Public Health Department,
o Utah Association of Local Health Departments, Utah Area Health Education Centers. A description of our involvement can be found in 3.3 Workforce Development.

39
Nevada public health agencies - Over the last two years we have developed strong ties with
several public health agencies in Nevada. We have been active participants in the Nevada Public Health Association, and have convened the Utah-Nevada Public Health Workforce Alliance, a group of public health practitioners and academics working together to identify key issues in the public health workforce and develop strategies for addressing these needs. Nevada Division of Public and Behavioral Health (state health department), Washoe County Health District (local health district), Southern Nevada Health District (local health district), Carson City Health and Human Services (local health district).

40
Figure 1.4.1 Divisoin of Public Health Orgnaizational Chart
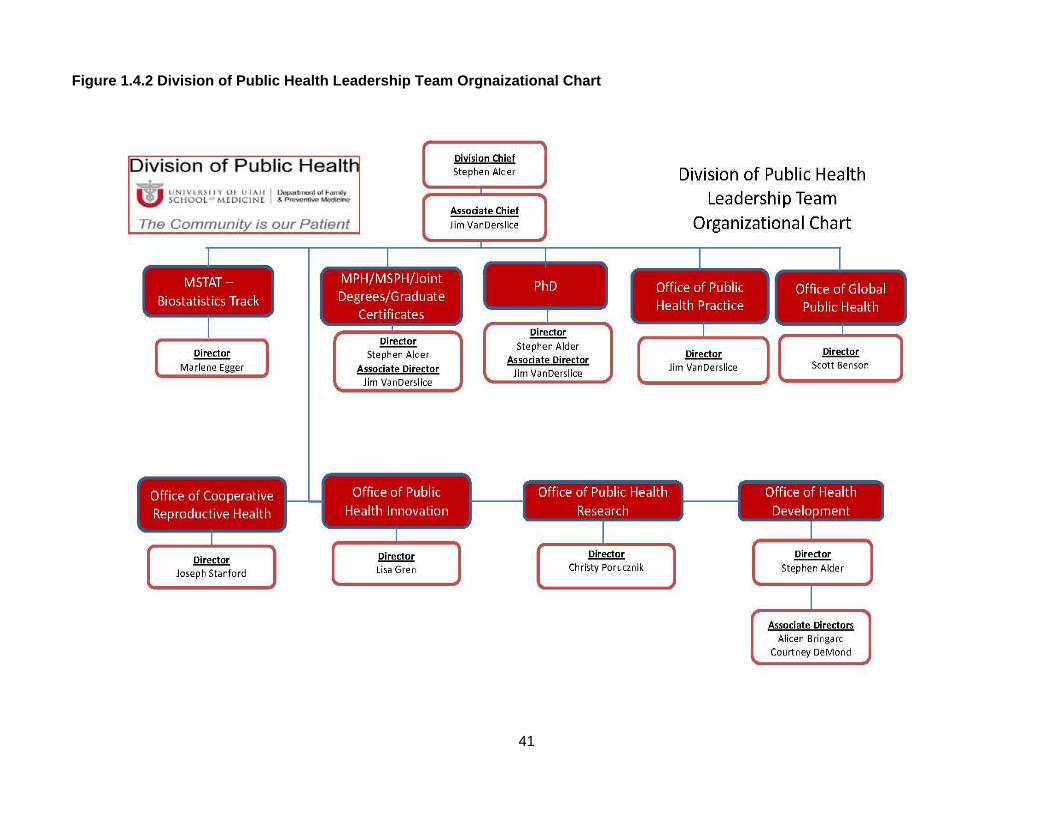
41
Figure 1.4.2 Division of Public Health Leadership Team Orgnaizational Chart
42
c. Assessment of the extent to which this criterion is met and an analysis of the program’s strengths, weaknesses and plans relating to this criterion. This criterion is met. Strengths: Our administrative structure has effectively grown as the Division of Public Health has expanded. The current organization serves current efforts well and offers a good foundation for our intended mid- and long-term growth. Growing leadership capacity among faculty and staff has provided an essential resource to make this possible. The administrative structure is also aligned with our mission, vision, and goals. Weaknesses: A major challenge in advancing our administrative structure is that even with our growth in leadership capacity, we still have a high proportion of faculty members at the instructor or assistant professor level, which means that individual career development needs to remain a priority to ensure appropriate advancement and retention. Plans: Continue to project our programmatic functional needs and priority thematic areas to insure that we are developing our administrative structure appropriately. Work to provide the needed support and protection to junior faculty members so that they can advance in their careers and academic ranks and assume more administrative leadership. Continue to make mid-level faculty recruitment a hiring priority.
43
1.5 Governance. The program administration and faculty shall have clearly defined rights and responsibilities concerning program governance and academic policies. Students shall, where appropriate, have participatory roles in the conduct of program evaluation procedures, policy setting, and decision making.
a. A list of standing and important ad hoc committees, with a statement of charge, composition, and current membership for each. The committees within the Division of Public Health consist of at least two faculty members, two staff members and in some cases, a student. The student committee member is the SAC President. The membership is summarized in Table 1.5.1. A brief description of the charge for each of the committees is described below. The current membership for each committee can be found in Appendix 1.5A.
Administration Committee (Standing) The Administration committee meets weekly to review the operational aspects of the Division including budget, program oversight, facilities, student issues, personnel issues, and planning strategic development. Admissions Committee (Standing) The admissions committee reviews completed student applications immediately following the application deadline. Prior to application review, the admissions committee will decide in conjunction with the Administrative Faculty how many students at each level will be admitted. Each application is evaluated for meeting the minimal admission criteria. Any applications that are incomplete do not go on for review. Applicants meeting minimum criteria may be invited for an interview over the phone. Applicants will be interviewed by at least two faculty members. The Admissions Committee meets to discuss the applicants and generates a list for recommended admissions. The Chair of the Admissions Committee presents the recommendation list at the Faculty Meeting held at the beginning of each month. CEPH (Council on Education for Public Health) Accreditation Committee (Ad hoc) The CEPH committee is responsible for preparing the accreditation report for the public health program. They are tasked with providing all required information and assessing the program. They meet weekly to compile and gather the relevant information and discuss the progress of the report. This committee is most active leading up to accreditation. This committee will continue after the reaccreditation with an annual review and update of the self-study. Comprehensive Exam Committee (Standing) The comprehensive exam committee is responsible for preparing and administering the comprehensive exam to MPH students three times a year. The examination consists of complex questions based on a real-life public health issue. Groups of qualifying students are divided into small groups and assigned separate questions. The group must develop an in-depth report and presentation for the public health issue which includes literature review, and development of a public health project to address the issue. Curriculum Committee (Standing) This committee is responsible for reviewing current course offering, and ensuring that all coursework content is appropriate and beneficial to the students. The committee coordinates class offerings with joint degree programs. The committee also reviews all waiver requests and syllabi. Development committee (Standing) The development committee, which meets weekly, focuses on strategic development and resource generation with a focus on donor and endowment support.
44
Leadership Committee (Standing) The leadership committee, which meets monthly, includes the directors of each of the offices, and meets to coordinate the activities of the offices. The offices were shown in the organizational charts in the previous section and include the offices of the MSTAT program, Public Health Practice, Global Public Health, MPH/MSPH/Joint Degrees/Graduates certificates, PhD program, AHEC, Public Health Innovation, Public Health Research, and Health Development. General Exam Committee (Standing) The General Exam committee is responsible for preparing and administering the general exam to PhD students, two times per year. The exam consists of a brief literature review on a specified topic, analysis of a dataset to answer specific research questions, preparation of a short manuscript and a short presentation to the faculty. The committee thus selects the research topic and prepares the data to be used in the exam. The committee reviews the report submitted by the student and is present to assess the presentation given by the student. Certificate in Global Health Committee (Standing) The Certificate in Global Health (CIGH) Committee is responsible for overseeing the administration of the CIGH. The committee reviews all applications from students for admission and reviews progress made by students in the program. Certificate in Public Health Committee (Standing) The Certificate in Public Health (CIPH) Committee is responsible for overseeing the administration of the CIPH. The committee reviews all applications from students for admission and reviews progress made by students in the program. Scholarship Committee (Standing) The Scholarship committee is responsible for reviewing scholarship applications (Appendix 1.5B & 1.5C). The Scholarship Committee announces the “Call for Application” when scholarships are made available. The committee then reviews all applications and discusses the criteria and applicants. Specific scholarships may require donor participation in the final decision-making process (i.e. James C. Reading Scholarship and Utah Public Health Association Scholarship). Currently the Division of Public Health provides two scholarships and on average six scholarships from endowments. Policy Committee (Standing) The Policy Committee is responsible for maintaining an up-to-date record of current policies and making these policies available to faculty, staff, and students. It is also the Policy Committee’s responsibility to present recommended policy changes to the Faculty members during Faculty meetings for final approval.
Website Reconstruction Committee (Ad hoc) Currently the website committee meets once a week to develop the webpages for the new updated public health site. The University of Utah is under-going an update to the webpage. The Division is using the update opportunity to further enhance the Division webpage for the various user groups such as new and continuing students, faculty, staff, external research and service collaborators, and donors. After the completion of the website we will form a new committee for maintenance of the website.

45
b. Identification of how the following functions are addressed within the program’s committees and organizational structure
Table 1.5.1 Functions addressed by the Division committees Functions
Committee:
General program
policy developm
ent P
lanning and evaluation
Budget and resource allocation
Student recruitm
ent, adm
ission, and award of
degrees
Faculty recruitm
ent, retention, prom
otion, and tenure
Academ
ic standards and policies, including curriculum
developm
ent
Research and service
expectations and policies
Administration X X X X X X X Admissions X X X CEPH Accreditation X X Comprehensive Exam X X Curriculum X X X Development X X X Leadership X X X X X General Exam X X Certificate in Global Health Committee
X x
Certificate in Public Health X Scholarship X X Policy X X X X X Website reconstruction X X X The listed functions above are addressed by the various committees generally by meetings for discussion. We have not experienced large overlaps in the responsibilities of the committees. The mechanism for processing committee recommendations is for the committee to bring the issue to the monthly faculty meetings. The issue is discussed and voted upon when action is necessary. Thus any overlaps in responsibilities are not a problem since major decisions are brought to the entire faculty and there is a transparent process for the decision making. c. A copy of the bylaws or other policy document that determines the rights and obligations of administrators, faculty, and students in governance of the program, if applicable. Policy documents for each of the following are available at the following website links:
Faculty handbook - http://admin.utah.edu/faculty-handbook Student handbook –http://medicine.utah.edu/dfpm/divisionph/current/Policies_Guidelines.pdf Student code - http://regulations.utah.edu/academics/6-400.php Staff Handbook - https://www.hr.utah.edu/ethicalstandards/ Human resources regulations - http://regulations.utah.edu/human-resources/5-102.php
46
d. Identification of program faculty who hold membership on university committees, through which faculty contribute to the activities of the university. Steve Alder, PhD 2013 - 2016 Member, University Faculty IT Committee 2013 - 2016 President, Commission on Status of Women 2013 - 2016 President Elect (2013-14), President (2014-15) and Past President (2015-16),
Academic Senate 2013 - Present Department of Population Sciences, Working Group 2013 - Present Member, Health System Innovation and Research Program, Steering Committee 2013 – Present Member, Managing the Health of Populations sub-committee – University of Utah Hospitals and Clinics Healthcare Transformation Working Group Director of Scientific Affairs, Institute for Healthcare Transformation, Development 2007 - Present Affiliated Faculty Member, University of Utah, Global Health Scholars, Honors
College, 2010 - 2013 Member, Academic Senate 2010 - 2013 Member, Academic Senate Executive Committee
Scott Benson, MD, PhD, MPH 2011 - Present Assistant Director, University Travel Clinic
Marlene Egger, PhD 2011 - Present Member, Center for Clinical Translational Science, CCTS Study Design and
Biostatistics Center 2009 - 2010 Executive Committee Member, Academic Senate 2009 - 2010 Member, University Statistics Committee 2007 - 2010 Senator, Academic Senate 2006 - 2010 Member, University of Utah Medical Group, UUMG Process Improvement and
Quality Group
Jessica Greenwood, MD, MSPH 2011 - Present Co-Founder & Co-Director, Redwood Health Center, Mothers Milk Donation
Center 2006 - Present Initiator & Member, University Hospital, Madsen Family Health Center, Reach out
and Read Steering Committee - Assisted with initiating children's reading program. 2012 Guest Panelist, University of Utah, Japanese Health Policy Workshops;
Healthcare for non-Japanese residents: beyond the barriers of language and culture
Lisa Gren, PhD, MSPH 2012 - Present Member, Family and Preventive Medicine, Search Committee, 4 clinical faculty
positions. 2011 Committee Member, Family and Preventive Medicine, Plan annual Department Retreat.
Mia Hashibe, PhD, MPH 2013 - Present Member, University of Utah, Faculty search committee for Director of
Evidence-based Nursing Practice, College of Nursing and Huntsman Cancer Institute
2011 - Present Member, Huntsman Cancer Institute, Seminar Committee 2010 - Present Committee Member, Huntsman Cancer Institute, Survey Methods Data Collection
Shared Resource Oversight Committee
47
Jaewhan Kim, PhD 2009 – Present Member, University of Utah, Biostatistics Track Representative in Master of
Statistics program 2011 - 2012 Representative, University of Utah, Biostatistics Track Representative in Master of
Statistics program
Christy Porucznik, PhD, MSPH 2013 - Present Faculty Senator, Academic Senate, University of Utah 2011 - Present Co-Founder & Co-Director, Salt Lake Mothers' Milk Donation Center 2013 Chair, Graduate School Internal Review Committee, Review of the Department of
Health Promotion and Education 2012 Candidate, Academic Senate, Nominated to run for Senate but was not elected.
Sara Simonsen, PhD, CMN, MSPH 2000 - 2001 Member, Health Sciences Center, Senior Vice Presidents' Health Sciences
Leadership Forum 2000 – 2001 Member, College of Nursing, Helene Fuld Leadership Forum 1999 - 2001 Mentor, College of Nursing, Mentor Program 1999 - 2000 Member, College of Nursing Baccalaureate Admissions and Advancement
Committee Joe Stanford, MD, MSPH 2001 - Present Team Leader, Primary Care Research Center 2006 - 2008 Member, Primary Care Research Center, Steering Committee 2005 - 2008 Member, Primary Care Research Center, Review Committee
David Sundwall, MD 2012-2014 President, School of Medicine Alumni Association 2010-Present Member, School of Medicine Alumni Association 1988 - Present Member, University of Utah, The Governor Scott M. Matheson Center for Health
Care Studies Advisory Council Jim VanDerslice, PhD 2011 - Present Member & Reviewer, Utah Resource for Genetic and Epidemiological Research 2011 - Present Member of the RGE Review Committee responsible for reviewing and approving
proposals that use Utah Population Database resources. 2012 Chair & Reviewer, The Graduate School, Graduate Council Review Committee for
the Department of Sociology
e. Description of student roles in governance, including any formal student organizations. Students from SAC serve on 4 of 12 Division committees, and also have a Student Advisory Committee (SAC). On average SAC has between 10-20 students participating each year. They have five officers, Chair, Vice-Chair, Secretary, Treasurer and Public Relations. The SAC president or designee sits on the following four standing committees; CEPH self-study (later in the process), curriculum, Certificate in Global Health and the Certificate in Public Health. The Division of Public Health SAC purposes are:
To promote and organize student departmental activities, promote communication between the student body and faculty; coordinate with and promote other public health student organizations;
To make recommendations for faculty retention, promotion and tenure (at the request of the Department Chair); and play an active role in community outreach.
48
To encourage student participation in SAC and department activities, develop activities in which students can participate and assist with organizing and facilitating programs which foster student interaction within the department.
To serve as liaison between various groups within the department and students. The SAC should notify students of departmental information through newsletters, classroom announcements, e-mails, and social media, including the SAC web page as part of the Division of Public Health website.
To interact and collaborate with other University of Utah organizations and community organizations as deemed appropriate.
To actively work to stay well informed about opportunities to enhance education and to communicate those opportunities to the students.
Encourage students to apply their academic knowledge through service to the community and work to make such opportunities available.
SAC helps support Breakfast and Lunch with the Chief, where the students are able to interact with the Division Chief directly, although specific topic areas may be covered in an open forum. The Division also asks SAC to help promote Grand Rounds, as well as other community service activities such as Coalition of a Healthier Community for Utah Women and Girls (UWAG) Health Fair, International Rescue Center (IRC) Coat Drive and 4th Street Triathlon. The Department of Family and Preventive Medicine, Division of Public Health, Student Advisory Committee bylaws can be found: http://medicine.utah.edu/dfpm/divisionph/current/SAC/SAC_By_Laws.pdf. f. Assessment of the extent to which this criterion is met and an analysis of the program’s strengths, weaknesses, and plans relating to this criterion. This criterion is met. Strengths: Faculty and administration have full rights to assure integrity of the program and to allow accomplishment of the program’s stated mission, goals, and objectives. Faculty members have formal opportunities for input through membership on the committees described above and in the areas of admissions and progress, resource allocation, faculty recruitment and promotion, curriculum design and evaluation, research and service activities, and degree requirements. Division faculty members also participate in university level committees such as the faculty senate. Students also have formal methods through the SAC structure to participate in policy making and decision making, with participation on appropriate committees. The rights and obligations of faculty, students, and staff are available publicly. The current governance structure allows for faculty and students to participate in policy making and decision making. Weaknesses: None noted. Plans: Future plans are to assure that the membership by faculty in various committees will be balanced, especially as new faculty members are hired into the Division.
49
1.6 Fiscal Resources. The program shall have financial resources adequate to fulfill its stated mission and goals, and its instructional, research, and service objectives. a. Description of the budgetary and allocation processes, including all sources of funding supportive of the instruction, research and service activities. This description should include, as appropriate, discussion about legislative appropriations, formula for funds distribution, tuition generation and retention, gifts, grants and contracts, indirect cost recovery, taxes or levies imposed by the university or other entities within the university, and other policies that impact the fiscal resources available to the program. Each department within the School of Medicine is required to complete an annual budget in accordance with the School of Medicine budget guidelines. The University of Utah’s fiscal year is July 1st through June 30th. The Department of Family and Preventive Medicine’s Administrative Director oversees the budget process. The Director has established a budget committee consisting of the department administrators and managers from each Division. The budget committee meets regularly to review, collect, and prepare data for the annual budget and budget narrative. The finalized budget is then submitted to the School of Medicine Dean’s Office. The Dean’s office will review budgets for accuracy and completeness and will work with departments on any questions or corrections that are needed. The Department of Family and Preventive Medicine Chairman and Administrative Director will then present the budget to the School of Medicine’s Mission Based Management Advisory Committee. After review and any other necessary corrections, the Sr. Vice President of Health Sciences and Dean of the School of Medicine will notify the department that their budget has been approved. Throughout the year, the Dean’s office will monitor financial reports and may ask for justification explaining any major financial variances between budget and actual operating results.
Relative to other faculty in the School of Medicine, we are not well supported financially by the University. Additionally, in contrast to other doctoral degree granting departments, the students in our Division are for the most part responsible for their own tuition.
The Division of Public Health budgeting and resource allocation includes state appropriated funds, faculty development funds (consulting, honorariums, etc.), gift funds (which may be restricted depending on donor request), endowment funds, indirect costs, and grants and contracts. Division of Public Health fiscal resources mainly include state appropriated funds including tuition and tuition differential, grants and contracts, gifts, and faculty development and consulting funds.
The Mission Based Management (MBM) state fund allocation model for FY14 utilizes separate pools for Basic Science Units and Clinical Departments. Within each group, funds are allocated to departments based on proportional activity in both teaching and research areas. A tuition differential was instituted starting fall 2008. These funds have increased from $150,000 in FY09 to a projected amount of $600,000 in FY14. With the impact of other state budget cuts, these funds have been instrumental in keeping our Division functioning. State and education funds make up about 25% of our current annual budget.
The Division of Public Health continues to grow in research endeavors as this is a high priority area for the Division as well as the School of Medicine. About 30% of the current annual budget consists of grants and contracts. The University of Utah’s Dean’s office returns 7.5% from the total indirect cost recovery or Facilities and Administrative (F&A) costs on grants and contracts to the department. The 7.5 % is based off the total F&A generated. Some projects will actually generate no F&A and thus receive no funding returned from them to the department. Implications of this are that we have be very thoughtful because so little of that returned amount is under our discretion. We need to consider target investments and how we can focus on activities that align with multiple elements of our mission and resource streams that support that.
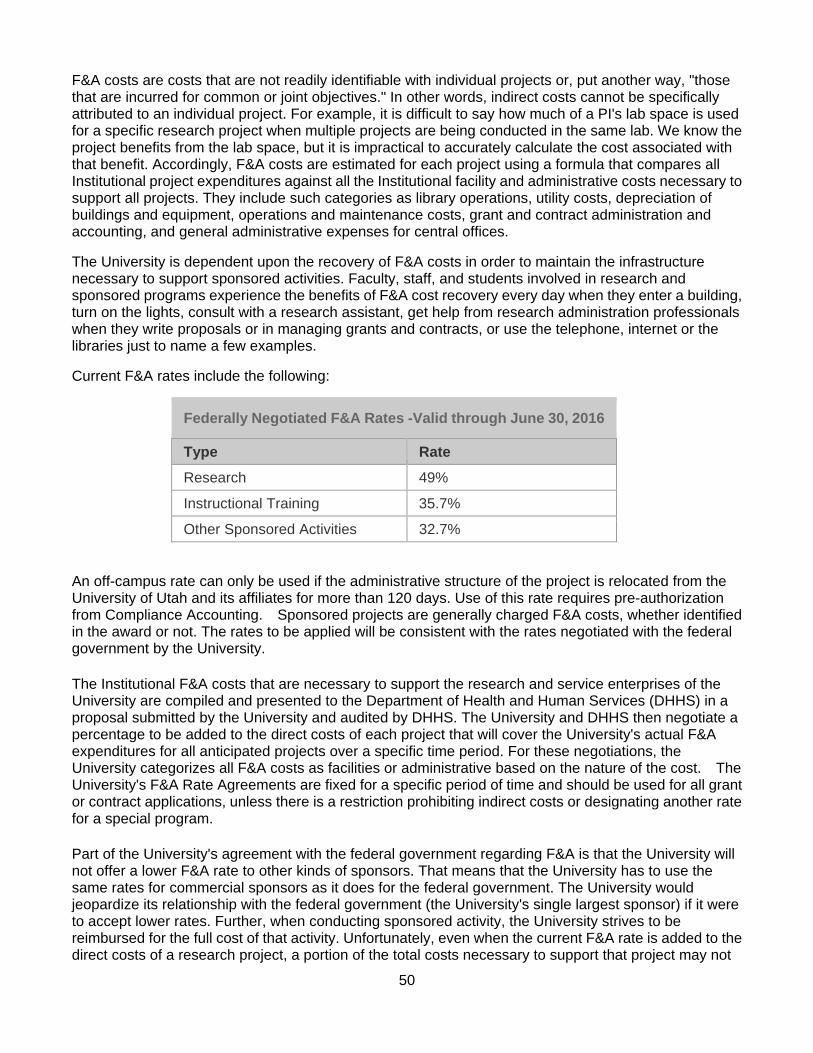
50
F&A costs are costs that are not readily identifiable with individual projects or, put another way, "those that are incurred for common or joint objectives." In other words, indirect costs cannot be specifically attributed to an individual project. For example, it is difficult to say how much of a PI's lab space is used for a specific research project when multiple projects are being conducted in the same lab. We know the project benefits from the lab space, but it is impractical to accurately calculate the cost associated with that benefit. Accordingly, F&A costs are estimated for each project using a formula that compares all Institutional project expenditures against all the Institutional facility and administrative costs necessary to support all projects. They include such categories as library operations, utility costs, depreciation of buildings and equipment, operations and maintenance costs, grant and contract administration and accounting, and general administrative expenses for central offices.
The University is dependent upon the recovery of F&A costs in order to maintain the infrastructure necessary to support sponsored activities. Faculty, staff, and students involved in research and sponsored programs experience the benefits of F&A cost recovery every day when they enter a building, turn on the lights, consult with a research assistant, get help from research administration professionals when they write proposals or in managing grants and contracts, or use the telephone, internet or the libraries just to name a few examples.
Current F&A rates include the following:
Federally Negotiated F&A Rates -Valid through June 30, 2016
Type Rate
Research 49%
Instructional Training 35.7%
Other Sponsored Activities 32.7%
An off-campus rate can only be used if the administrative structure of the project is relocated from the University of Utah and its affiliates for more than 120 days. Use of this rate requires pre-authorization from Compliance Accounting. Sponsored projects are generally charged F&A costs, whether identified in the award or not. The rates to be applied will be consistent with the rates negotiated with the federal government by the University.
The Institutional F&A costs that are necessary to support the research and service enterprises of the University are compiled and presented to the Department of Health and Human Services (DHHS) in a proposal submitted by the University and audited by DHHS. The University and DHHS then negotiate a percentage to be added to the direct costs of each project that will cover the University's actual F&A expenditures for all anticipated projects over a specific time period. For these negotiations, the University categorizes all F&A costs as facilities or administrative based on the nature of the cost. The University's F&A Rate Agreements are fixed for a specific period of time and should be used for all grant or contract applications, unless there is a restriction prohibiting indirect costs or designating another rate for a special program.
Part of the University's agreement with the federal government regarding F&A is that the University will not offer a lower F&A rate to other kinds of sponsors. That means that the University has to use the same rates for commercial sponsors as it does for the federal government. The University would jeopardize its relationship with the federal government (the University's single largest sponsor) if it were to accept lower rates. Further, when conducting sponsored activity, the University strives to be reimbursed for the full cost of that activity. Unfortunately, even when the current F&A rate is added to the direct costs of a research project, a portion of the total costs necessary to support that project may not
51
be recovered by the University because of limitations created by federal allowable cost principles. The University would in effect be subsidizing the actual costs of a sponsored activity when nonstandard F&A rates are applied. While some may perceive that F&A is discretionary, the University could not maintain sponsored activity on campus for long without reimbursement for the costs required to support the research and service enterprise. Even at the current rate the University ultimately only collects a little less than 50 cents on every dollar spent by the University to support sponsored activities infrastructure.
Indirect costs are charged to a project by applying a percentage to the total direct costs (TDC) of the project. In some instances the TDC may be modified to exclude capital equipment, participant support, patient care, and subcontract expenditures in excess of $25,000. This rate is known as the modified total indirect cost rate (MTDC).
Note: The University charges F&A on the first $25,000 of each sub-agreement for a project period. Any amount above $25,000 for each sub-agreement is not subject to F&A for the remainder of the project period. However, the University as the award recipient or sub-recipient will defer to the written, universal F&A policy of the awarding sponsor, if different from above. The sponsor's policy will also be flowed to the University sub-recipients.
If a sponsor limits F&A to less than the University's federally negotiated rate, the F&A rate base should be calculated by adding all direct costs (TDC) with no exclusions or exceptions. If you are calculating TDC using the 22% on total federal funds awarded (TFFA) as required by the USDA, add direct costs with no exclusions or exceptions to TDC. 28.20513% of the TDC would be used to arrive at 22% TFFA.
The F&A being requested cannot exceed what would be allowable using the University's negotiated rates and exclusions. Therefore, we calculate the F&A using both the sponsor's F&A rate as well as our negotiated rate to ensure we are not requesting excessive F&A. If the indirect costs are excessive, modify the percentage being applied to the TDC until you arrive at indirect costs that are equal to, but not more or less than, what would normally be requested using our negotiated rate. Reference: http://osp.utah.edu/policies/handbook/budget-development/indirect-costs.php
The Division of Public Health has partnered with a major donor over the past two years. We are currently working with this specific donor on building the first accredited School of Public Health in Ghana which may become the West African Regional Hub for the University of Utah. This partnership, along with other donations, has made a significant impact on our gift revenue. About 35% of our current annual budget consists of gifts.
The remaining 10% of our current annual budget consists of faculty development and consulting. We hope to continue collaboration with other faculty outside our department as well as partnering with other businesses.
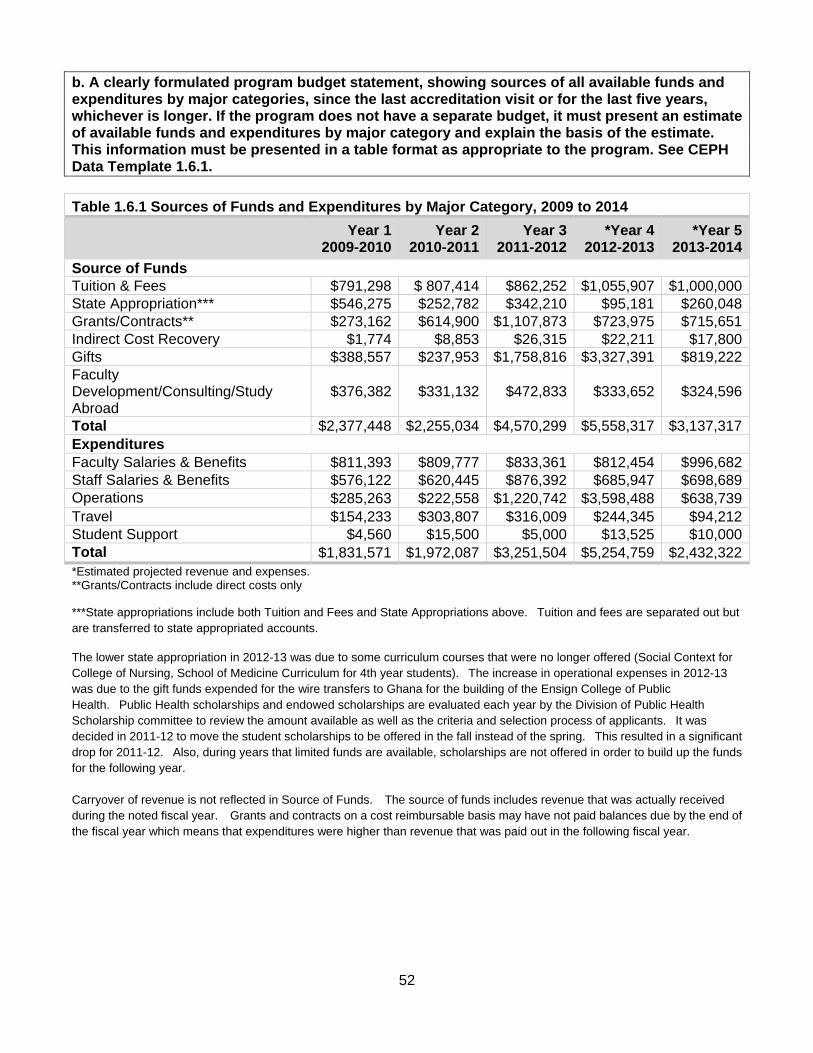
52
b. A clearly formulated program budget statement, showing sources of all available funds and expenditures by major categories, since the last accreditation visit or for the last five years, whichever is longer. If the program does not have a separate budget, it must present an estimate of available funds and expenditures by major category and explain the basis of the estimate. This information must be presented in a table format as appropriate to the program. See CEPH Data Template 1.6.1.
Table 1.6.1 Sources of Funds and Expenditures by Major Category, 2009 to 2014 Year 1
2009-2010Year 2
2010-2011Year 3
2011-2012*Year 4
2012-2013*Year 5
2013-2014
Source of Funds Tuition & Fees $791,298 $ 807,414 $862,252 $1,055,907 $1,000,000State Appropriation*** $546,275 $252,782 $342,210 $95,181 $260,048Grants/Contracts** $273,162 $614,900 $1,107,873 $723,975 $715,651Indirect Cost Recovery $1,774 $8,853 $26,315 $22,211 $17,800Gifts $388,557 $237,953 $1,758,816 $3,327,391 $819,222Faculty Development/Consulting/Study Abroad
$376,382 $331,132 $472,833 $333,652 $324,596
Total $2,377,448 $2,255,034 $4,570,299 $5,558,317 $3,137,317Expenditures Faculty Salaries & Benefits $811,393 $809,777 $833,361 $812,454 $996,682Staff Salaries & Benefits $576,122 $620,445 $876,392 $685,947 $698,689Operations $285,263 $222,558 $1,220,742 $3,598,488 $638,739Travel $154,233 $303,807 $316,009 $244,345 $94,212Student Support $4,560 $15,500 $5,000 $13,525 $10,000Total $1,831,571 $1,972,087 $3,251,504 $5,254,759 $2,432,322*Estimated projected revenue and expenses. **Grants/Contracts include direct costs only
***State appropriations include both Tuition and Fees and State Appropriations above. Tuition and fees are separated out but are transferred to state appropriated accounts.
The lower state appropriation in 2012-13 was due to some curriculum courses that were no longer offered (Social Context for College of Nursing, School of Medicine Curriculum for 4th year students). The increase in operational expenses in 2012-13 was due to the gift funds expended for the wire transfers to Ghana for the building of the Ensign College of Public Health. Public Health scholarships and endowed scholarships are evaluated each year by the Division of Public Health Scholarship committee to review the amount available as well as the criteria and selection process of applicants. It was decided in 2011-12 to move the student scholarships to be offered in the fall instead of the spring. This resulted in a significant drop for 2011-12. Also, during years that limited funds are available, scholarships are not offered in order to build up the funds for the following year. Carryover of revenue is not reflected in Source of Funds. The source of funds includes revenue that was actually received during the noted fiscal year. Grants and contracts on a cost reimbursable basis may have not paid balances due by the end of the fiscal year which means that expenditures were higher than revenue that was paid out in the following fiscal year.
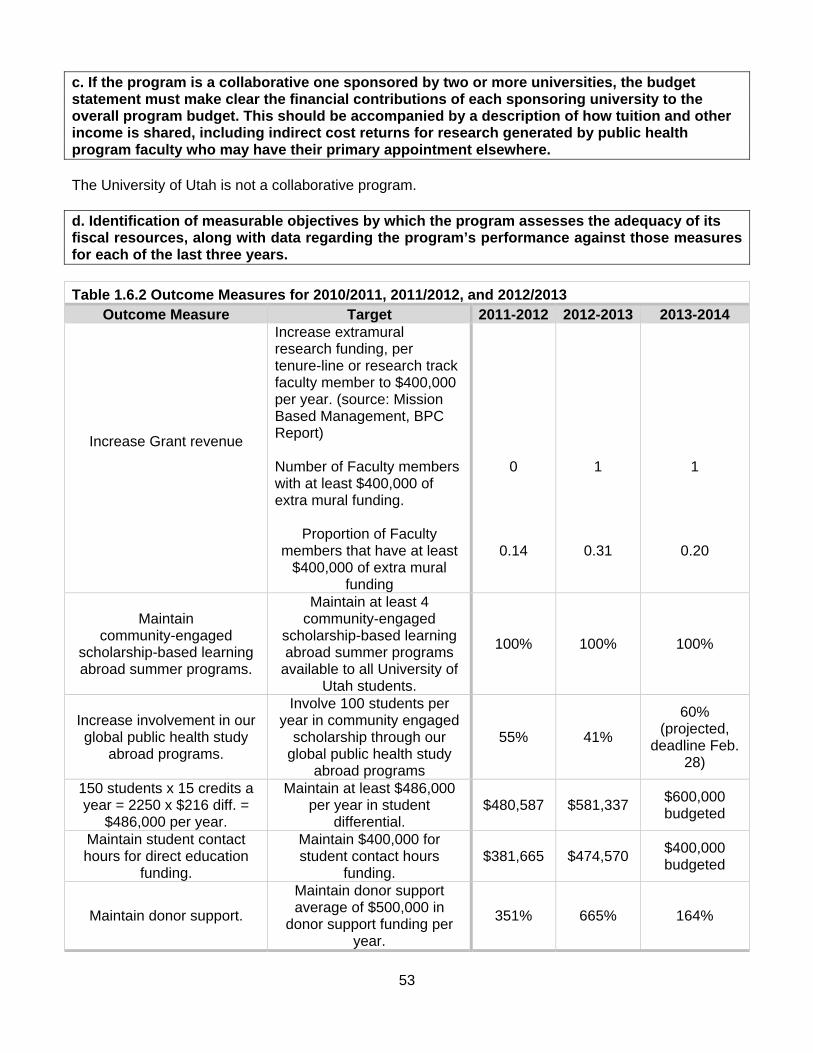
53
c. If the program is a collaborative one sponsored by two or more universities, the budget statement must make clear the financial contributions of each sponsoring university to the overall program budget. This should be accompanied by a description of how tuition and other income is shared, including indirect cost returns for research generated by public health program faculty who may have their primary appointment elsewhere. The University of Utah is not a collaborative program. d. Identification of measurable objectives by which the program assesses the adequacy of its fiscal resources, along with data regarding the program’s performance against those measures for each of the last three years.
Table 1.6.2 Outcome Measures for 2010/2011, 2011/2012, and 2012/2013 Outcome Measure Target 2011-2012 2012-2013 2013-2014
Increase Grant revenue
Increase extramural research funding, per tenure-line or research track faculty member to $400,000 per year. (source: Mission Based Management, BPC Report) Number of Faculty members with at least $400,000 of extra mural funding.
Proportion of Faculty members that have at least
$400,000 of extra mural funding
0
0.14
1
0.31
1
0.20
Maintain community-engaged
scholarship-based learning abroad summer programs.
Maintain at least 4 community-engaged
scholarship-based learning abroad summer programs
available to all University of Utah students.
100% 100% 100%
Increase involvement in our global public health study
abroad programs.
Involve 100 students per year in community engaged
scholarship through our global public health study
abroad programs
55% 41%
60% (projected,
deadline Feb. 28)
150 students x 15 credits a year = 2250 x $216 diff. =
$486,000 per year.
Maintain at least $486,000 per year in student
differential. $480,587 $581,337
$600,000 budgeted
Maintain student contact hours for direct education
funding.
Maintain $400,000 for student contact hours
funding. $381,665 $474,570
$400,000 budgeted
Maintain donor support.
Maintain donor support average of $500,000 in
donor support funding per year.
351% 665% 164%

54
e. Assessment of the extent to which this criterion is met and an analysis of the program’s strengths, weaknesses and plans relating to this criterion. This criterion is met.
Strengths: Since our last review, we have successfully diversified our funding to allow more financial stability. This has provided a foundation upon which our growth during that time has been supported. By introducing differential tuition, expanding our gifts and development funds, and growing our extramural funding, we have been able to offset the decline in state support. This has also facilitated our improvements in balancing our efforts to more closely align with our three missions of education, research, and service. Improved financial stability has allowed us to expand faculty resources, ensure an effective administrative, education and research staff, and provides more funding support for students through graduate assistantships and scholarship support. This support is also helping us to position for marked growth in the future as we work towards meaningful roles with the developing campuses at the Songdo Global University in Korea and the Ensign College of Public Health in Ghana.
Weaknesses: While our financial stability has improved, it remains one of our top challenges. Major shifts in funding from the state, federal sources and donors continue to occur, and often are unpredictable. Other institutional priorities, such as expanding the medical student class size, take priority over the funding needs for graduate programs like public health. Further, our institution also requires state support and base tuition resources to be spent down annually, thereby creating a challenge for developing reserve funds. Our growth in funded student assistantships, with the accompanying tuition waivers, is still insufficient to meet the demand from qualified students.
Plans: We continue to manage our resources carefully to try to be as efficient as possible while still working to support educational excellence, growth in our research and innovation activities, and service to our identified constituents and partners. We are working to expand our resource streams with a more aggressive donor plan, supported by our development committee and institutional development expertise, strategic growth in our extramural research and training funding, and through contract and consultative work that aligns with our mission. We have been generally successful in growth across these resource categories and will continue to emphasize this as a priority.

55
1.7 Faculty and Other Resources. The program shall have personnel and other resources adequate to fulfill its stated mission and goals, and its instructional, research and service objectives. a. A concise statement or chart defining the number (headcount) of primary faculty employed by the program for each of the last three years, organized by concentration. Table 1.7.1 Headcount of Primary Faculty 2011-2012 2012-2013 2013-2014 Generalist 16 13 15 Two of our faculty retired effective 6/30/12 and were transitioned to Emeritus faculty. They have both stayed involved in teaching for this current fiscal year (2012-13). One of them will continue teaching in a support role in the upcoming fiscal year. We recently hired two new faculty members including a joint hire with the Huntsman Cancer Institute at the University of Utah for a tenure track position and Public Health tenure track faculty position with a focus on Public Health Workforce Development. We anticipated that these two hires will replace faculty that have recently retired. We also plan to hire additional Visiting Professors in the upcoming fiscal year. A faculty member may hold the rank of Visiting Instructor up to three years. If the Visiting Instructor is appointed to a tenure generating rank, the time spent, or yearly portions thereof, may be counted toward the pre-tenure probationary period unless stated otherwise in writing by the candidate or in the Department Chair's Offer Letter. Faculty members in this rank have a yearly contract. No advertising or search is required. These are temporary positions with the University renewable at the end of the academic year (up to three years.) Recruitment procedures must be followed if the individual is recommended for appointment as an Instructor or Assistant Professor in any of the other tracks. The basic requirements of this rank may be awarded to individuals who have met the minimal requirements for faculty membership. It is intended for individuals who are completing their training or acquiring essential experience while simultaneously serving a faculty role. Visiting faculty members are evaluated the same way as all of our other faculty members within the Division as described in 4.2.d. They do not however undergo RPT procedures since they are not formally on a track (lecturer, clinical, research, scientist scholar or clinician scholar).
EDUCATION: A doctoral degree (MD, PhD, or other terminal professional degree) from an accredited institution of higher learning. IN CLINICAL DEPARTMENTS: completion of the residency training normally required for board certification, or for non-M.D.'s, a minimum of two years of post-doctoral training and/or experience.
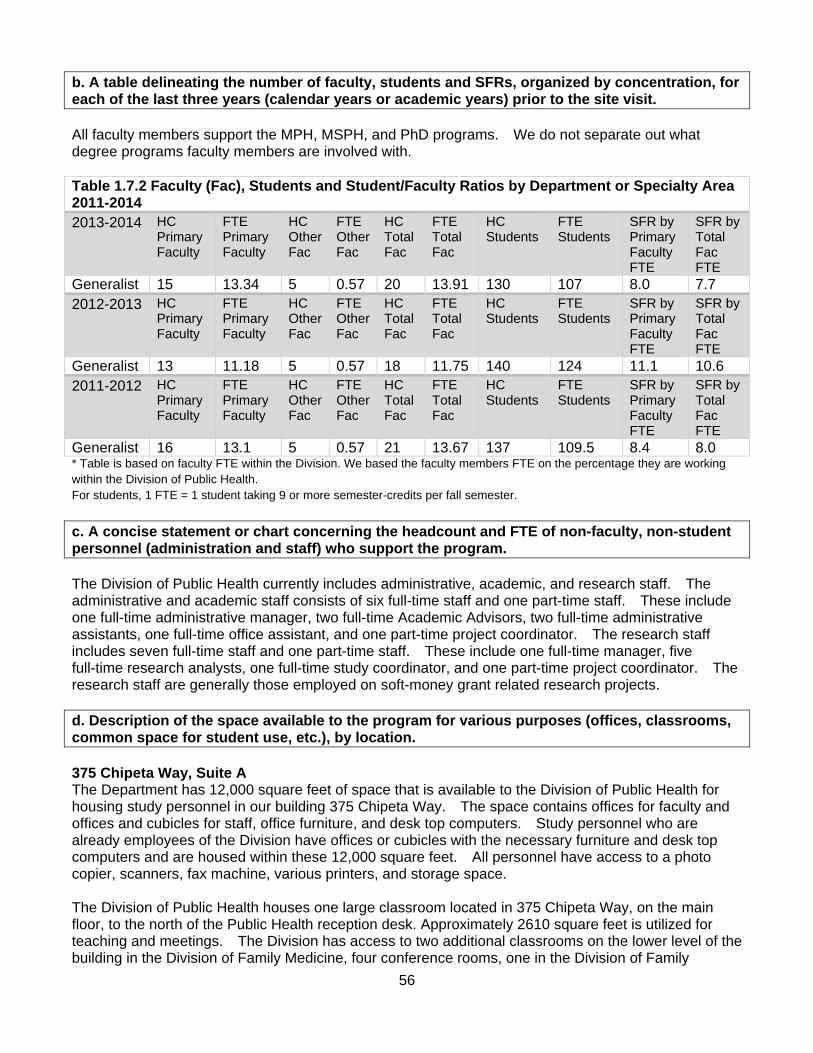
56
b. A table delineating the number of faculty, students and SFRs, organized by concentration, for each of the last three years (calendar years or academic years) prior to the site visit. All faculty members support the MPH, MSPH, and PhD programs. We do not separate out what degree programs faculty members are involved with. Table 1.7.2 Faculty (Fac), Students and Student/Faculty Ratios by Department or Specialty Area 2011-2014 2013-2014 HC
Primary Faculty
FTE Primary Faculty
HC Other Fac
FTE OtherFac
HC Total Fac
FTE Total Fac
HC Students
FTE Students
SFR by Primary Faculty FTE
SFR by Total Fac FTE
Generalist 15 13.34 5 0.57 20 13.91 130 107 8.0 7.7 2012-2013 HC
Primary Faculty
FTE Primary Faculty
HC Other Fac
FTE OtherFac
HC Total Fac
FTE Total Fac
HC Students
FTE Students
SFR by Primary Faculty FTE
SFR by Total Fac FTE
Generalist 13 11.18 5 0.57 18 11.75 140 124 11.1 10.6 2011-2012 HC
Primary Faculty
FTE Primary Faculty
HC Other Fac
FTE OtherFac
HC Total Fac
FTE Total Fac
HC Students
FTE Students
SFR by Primary Faculty FTE
SFR by Total Fac FTE
Generalist 16 13.1 5 0.57 21 13.67 137 109.5 8.4 8.0 * Table is based on faculty FTE within the Division. We based the faculty members FTE on the percentage they are working within the Division of Public Health. For students, 1 FTE = 1 student taking 9 or more semester-credits per fall semester.
c. A concise statement or chart concerning the headcount and FTE of non-faculty, non-student personnel (administration and staff) who support the program. The Division of Public Health currently includes administrative, academic, and research staff. The administrative and academic staff consists of six full-time staff and one part-time staff. These include one full-time administrative manager, two full-time Academic Advisors, two full-time administrative assistants, one full-time office assistant, and one part-time project coordinator. The research staff includes seven full-time staff and one part-time staff. These include one full-time manager, five full-time research analysts, one full-time study coordinator, and one part-time project coordinator. The research staff are generally those employed on soft-money grant related research projects. d. Description of the space available to the program for various purposes (offices, classrooms, common space for student use, etc.), by location. 375 Chipeta Way, Suite A The Department has 12,000 square feet of space that is available to the Division of Public Health for housing study personnel in our building 375 Chipeta Way. The space contains offices for faculty and offices and cubicles for staff, office furniture, and desk top computers. Study personnel who are already employees of the Division have offices or cubicles with the necessary furniture and desk top computers and are housed within these 12,000 square feet. All personnel have access to a photo copier, scanners, fax machine, various printers, and storage space. The Division of Public Health houses one large classroom located in 375 Chipeta Way, on the main floor, to the north of the Public Health reception desk. Approximately 2610 square feet is utilized for teaching and meetings. The Division has access to two additional classrooms on the lower level of the building in the Division of Family Medicine, four conference rooms, one in the Division of Family
57
Medicine and three in the Administrative area on the main floor. The Division of Public Health also has the ability to schedule classrooms at the Health Sciences Education Building on the main campus of the University of Utah. A quiet study and common study area has been created for students to meet and work, on the Garden level of 375 Chipeta Way. The quiet study area has mini cubicles and chairs with an attached desk. The common study area is found at the bottom of the stairs and has three tables with chairs around them. There is also a refrigerator, microwave, sink, and filtered water located throughout the building for students, faculty, and staff. e. A concise description of the laboratory space and description of the kind, quantity and special features or special equipment. Faculty members have laboratory space at the Huntsman Cancer Institute, a cancer research facility at the University of Utah. HCI is a six-level, 225,000 square foot facility, fifty percent of which is dedicated to basic and clinical research. The main labs on each of the laboratory floors are built on an open floor plan designed to encourage interaction between laboratory staff in different research groups and to encourage communal use of major equipment. When other laboratory space needs arise, the faculty partner with various labs across the University of Utah campus. f. A concise statement concerning the amount, location and types of computer facilities and resources for students, faculty, administration and staff. Faculty and staff at the University of Utah each have individual offices or modular space provided by the University of Utah with locking filing cabinets and networked password protected computers. All faculty and staff have access to the University’s computer facilities and computer support services. The computer system is supported by Departmental personnel. Computers of sufficient size are available to handle large amounts of data generated. The Department of Family and Preventive Medicine’s server connects to the Internet via a router on the University of Utah campus network. The University’s Network Communications department, in conjunction with the Institutional Security Office, controls access and monitoring of the campus network twenty-four hours a day, seven days a week. High threat ports are blocked at the edge of the University in order to keep worms and viruses from entering the University network. If a compromised system is found inside the University network, a block is placed on the machine at the router port until the problem is corrected. Computer resources for the Division are excellent. Faculty and staff members have personal computers that are current and provide necessary capacity. Network resources are readily available, including server space for large files and sophisticated statistical analyses, and are upgraded regularly to meet increasing demands. A computer lab with 11 stations is available for students, who also receive accounts with limited network storage space. A suite of common and specialized software is available on these computers. Wireless network connectivity is also available in all areas of building 375 Chipeta Way. University email accounts are provided for all faculty, staff, and students. For those students who bring their own laptops we have installed ground plugs every few feet in the main classroom. Additionally, students have access to computer labs in both the Marriott library on main campus or the Eccles Health Sciences library on upper campus. Students must use their designated University of Utah student identification number and personal password to access computers in all facilities.
58
g. A concise description of library/information resources available for program use, including a description of library capacity to provide digital (electronic) content, access mechanisms, training opportunities and document-delivery services. Faculty, staff, and students within the Division have access to and utilize the Spenser S. Eccles Health Science Library as well as the J. Willard Marriott Library that service the entire University of Utah campus. The libraries provide a full range of start-of-the-art services. Libraries can be accessed through the physical facilities or via the internet. In addition, librarians are actively involved in the education and research components of the Division by providing instruction in a variety of settings and providing assistance in accessing materials. Overall, there is convenient access to excellent library resources; students, faculty, and staff have access to over 9 e-journals related specifically to public health, 9 journals for epidemiology, 5 journals for environmental health, 4 for health policy and 21 for behavioral health. Articles from journals that the University does not have a subscription to can be ordered through an online system known as the Interlibrary Loan and Document Delivery (ILLiad). h. A concise statement of any other resources not mentioned above, if applicable. Center for Teaching and Learning Excellence (CTLE; http://ctle.utah.edu). CTLE aims to support the University's teaching community through a variety of services, such as courses, and evaluations with feedback. In addition, resource pages include links to promote the ongoing development of faculty, teaching assistants and anyone else involved in teaching at the University. Teaching and Learning Technologies (TLT; http://tlt.utah.edu/). Teaching & Learning Technologies provides technology support for University of Utah faculty working in both physical and virtual learning spaces. They have two offices to meet technology needs: Milton Bennion Hall (MBH) provides classroom technology and audio & video services for both academic and non-academic events. Marriott Library (MLIB Suite 1705) provides course consultation services for online class webpages and other online learning technologies, and provides proctored exam services for online courses. Center for Clinical and Translational Science (CCTS, http://medicine.utah.edu/ccts/). CCTS serves as an academic home for clinical and translational research, developing innovative health services for the community and researchers, and training a new generation of clinical and translational investigators. The CCTS is a collaborative partnership between the Utah Department of Health, University of Utah, Intermountain Healthcare, and the Department of Veteran Affairs. University Writing Center (http://writingcenter.utah.edu/). The University Writing Center champions the writer inside each person. Whether the individual is just starting college, working on a dissertation, or finalizing an article for publication, the Writing Center is a resource to help improve writing. In a collaborative atmosphere a student meets with a tutor to talk about a writing assignment. The tutors can work on anything from rhetorical analysis papers, to arguments, to lab reports and research results. Whether the student needs to brainstorm ideas, write or re-write, tutors help improve writing in practice.
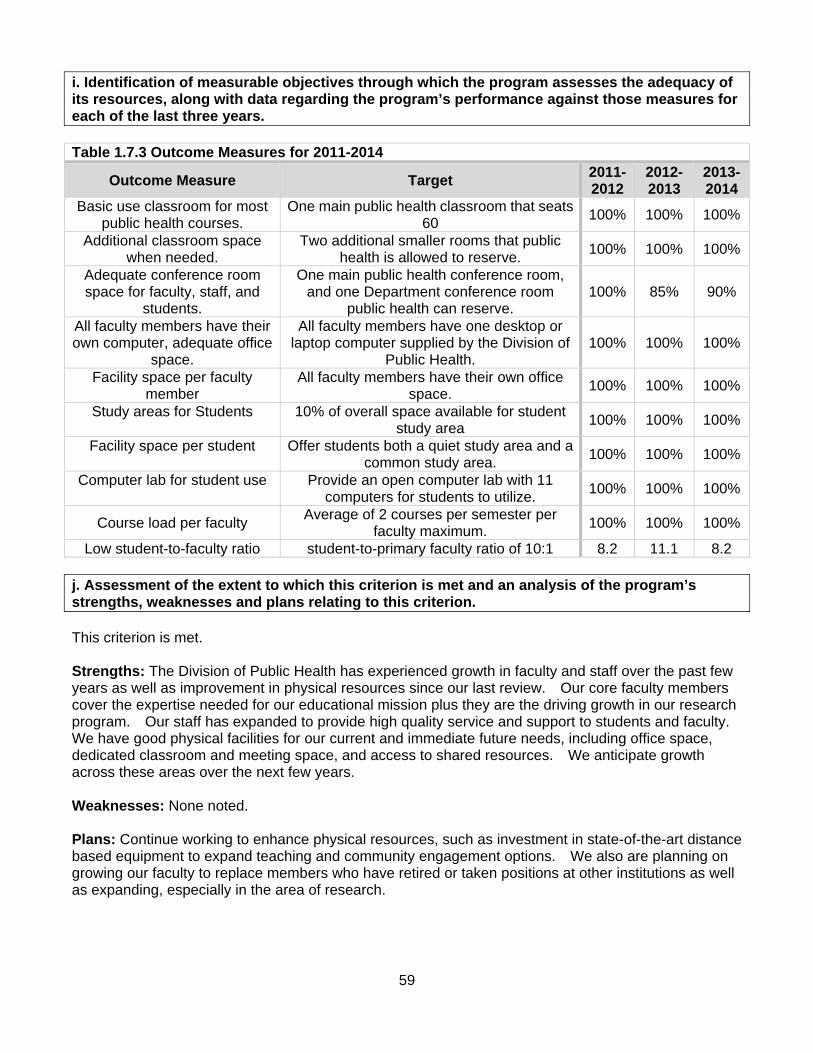
59
i. Identification of measurable objectives through which the program assesses the adequacy of its resources, along with data regarding the program’s performance against those measures for each of the last three years. Table 1.7.3 Outcome Measures for 2011-2014
Outcome Measure Target 2011-2012
2012-2013
2013-2014
Basic use classroom for most public health courses.
One main public health classroom that seats 60
100% 100% 100%
Additional classroom space when needed.
Two additional smaller rooms that public health is allowed to reserve.
100% 100% 100%
Adequate conference room space for faculty, staff, and
students.
One main public health conference room, and one Department conference room
public health can reserve. 100% 85% 90%
All faculty members have their own computer, adequate office
space.
All faculty members have one desktop or laptop computer supplied by the Division of
Public Health. 100% 100% 100%
Facility space per faculty member
All faculty members have their own office space.
100% 100% 100%
Study areas for Students
10% of overall space available for student study area
100% 100% 100%
Facility space per student
Offer students both a quiet study area and a common study area.
100% 100% 100%
Computer lab for student use
Provide an open computer lab with 11 computers for students to utilize.
100% 100% 100%
Course load per faculty Average of 2 courses per semester per
faculty maximum. 100% 100% 100%
Low student-to-faculty ratio student-to-primary faculty ratio of 10:1 8.2 11.1 8.2 j. Assessment of the extent to which this criterion is met and an analysis of the program’s strengths, weaknesses and plans relating to this criterion. This criterion is met. Strengths: The Division of Public Health has experienced growth in faculty and staff over the past few years as well as improvement in physical resources since our last review. Our core faculty members cover the expertise needed for our educational mission plus they are the driving growth in our research program. Our staff has expanded to provide high quality service and support to students and faculty. We have good physical facilities for our current and immediate future needs, including office space, dedicated classroom and meeting space, and access to shared resources. We anticipate growth across these areas over the next few years. Weaknesses: None noted. Plans: Continue working to enhance physical resources, such as investment in state-of-the-art distance based equipment to expand teaching and community engagement options. We also are planning on growing our faculty to replace members who have retired or taken positions at other institutions as well as expanding, especially in the area of research.
60
1.8 Diversity. The program shall demonstrate a commitment to diversity and shall evidence an ongoing practice of cultural competence in learning, research and service practices. a. A written plan and/or policies demonstrating systematic incorporation of diversity within the program.
i. Description of the program’s under-represented populations, including a rationale for the designation.
The program has identified rural residence and race/ethnicity minority groups as underrepresented populations in our student, staff, and faculty. The majority of the counties in Utah are rural, and public health issues such as medical care and access are important issues for rural communities in Utah. According to the US Department of Agriculture, for individuals living in census places with <50,000 people, 62.9% of the population in Utah is rural and 99% of the land is considered rural (http://www.ers.usda.gov/datafiles/Rural_Definitions/StateLevel_Maps/ut.pdf). The 2012 US census estimates for race/ethnicity distributions in Utah were: 79.9% non-Hispanic White, 1.3% Black, 1.5% American Indian or Alaska Native, 2.2% Asian, 1.0% Native Hawaiian or Other Pacific Islander, 2.4% two or more races, 13.3% Hispanic or Latino. Although the proportion of race/ethnic minority groups is small in Utah compared to other states, some groups such as Hispanics are largely under-represented in our student, staff, and faculty.
ii. A list of goals for achieving diversity and cultural competence within the program, and a description of how diversity-related goals are consistent with the university’s mission, strategic plan and other initiatives on diversity, as applicable.
The goals for achieving diversity and cultural competence within the program are:
Recruitment of a diverse student body Retaining a diverse faculty Immersion of students, faculty, and staff to a diverse environment through the global health
initiative (study abroad programs and international research projects) Continuing to offer courses that build competency in diversity and cultural considerations
The goals for achieving diversity and cultural competence within the program are consistent with those of the Office of Inclusion and Outreach (http://www.diversity.utah.edu/) within the University of Utah, School of Medicine. The goal of this office is: "to extend an open invitation to all embracing and supporting all values for the enrichment of the entire Utah community. Additionally, we seek to value and embrace all outreach in order to bridge the Utah Community and the School of Medicine through educational and healthcare partnerships." The goals of the Office are:
To create sustainable educational and health partnerships for the purpose of the School of Medicine’s student volunteer efforts to the entire Utah community
To support partnerships within the School of Medicine and the entire Utah community To maintain educational continuum through the School of Medicine educational programs To embrace all School of Medicine student volunteer efforts to serve the Utah community To lead efforts for cultural awareness and embrace and welcome cultural differences in the
School of Medicine and the Utah community
61
iii. Policies that support a climate free of harassment and discrimination and that value the contributions of all forms of diversity; the program should also document its commitment to maintaining/using these policies.
The Division not only continues to pursue diverse applicants, but also has made great efforts to establish an environment that supports diversity. Faculty members have worked to establish course expectations that are consistent with a diverse student body. Additionally, counseling is available to assist students from diverse backgrounds. Faculty advisors are encouraged to be especially vigilant in monitoring the academic performance and general life challenges of students who come from diverse backgrounds. With regards to policies and procedures implementing student diversity, the Division operates under the jurisdiction of mandates, established by the School of Medicine and the University of Utah as a whole. This means that criteria for admissions and faculty and staff hires are based upon explicit qualifications and procedures and that no exclusionary caveats exist with respect to age, sex, race, disability, religion, or national origin. University executive, administrative, academic, and supervisory officers exercising Employee management responsibilities are required to take vigorous and appropriate action to assure that all employment-related practices and decisions are made without discrimination, harassment, or prejudicial treatment because of race/ethnicity, color, religion, national origin, sex, sexual orientation, gender identity/expression, age, disability or protected veteran - external link's status. All employment-related practices and decisions within the University shall, to the maximum feasible extent, be instituted and administered in a fair and equitable manner, using only legally valid job-related criteria and standards, including but not limited to experience, training, education, skills, and potential for successful job performance and upward mobility. All University facilities used by or available to University employees or applicants for employment shall be maintained and operated on a nonsegregated and nondiscriminatory basis. The University of Utah complies with the Americans with Disabilities Act (ADA) by providing qualified individuals with disabilities access to University programs, services, and activities. Reasonable prior notice is needed to evaluate requests for accommodation and to implement them when appropriate. All the course syllabi from our Division include the ADA statement “The University of Utah seeks to provide equal access to its programs, services and activities for people with disabilities. If you will need accommodations in the class, reasonable prior notice needs to be given to the Center for Disability Services (CDS), 162 Union Building, 581-5020 (V/TDD). CDS will work with you and the instructor to make arrangements for accommodations.” Harassment and discrimination are handled like any other issues in misconduct with appropriate actions. Should any concerns or potential issues arise they are immediately referred to the Division Chief. The Division Chief takes all reports seriously and gives full consideration and due process. Although, we have not had any issues in recent years, we continue to use the University of Utah Policies as a resource. http://regulations.utah.edu/academics/guides/discrimination.php
iv. Policies that support a climate for working and learning in a diverse setting. The Division is deeply committed to enhancing the success of diverse faculty, students, and staff, as part of our broader goal to enrich the educational experiences and success of all members of our University community. The Division recognizes that a diverse and inclusive University enriches the educational experiences of all students, and enhances our excellence as a world-class institution for 21st Century learners. The Office for Equity and Diversity leads the University’s efforts to support the success and achievement of faculty, students, and staff who self-identify as African American, Latina/o or Chicana/o, Asian American, Pacific Islander, American Indian, members of the Lesbian, Gay, Bisexual, Transgender and Questioning community, and women in underrepresented fields.
62
In collaboration with community outreach, the Division collaborates with several programs outside of the University. Faculty, staff, and students are involved in research and educational experiences with organizations such as Center for Clinical and Translational Sciences, and Community Faces of Utah, which provides joint research for our community engaged scholarship. Specific programs and efforts to value the contributions of all forms of diversity are:
Coalition of a Healthier Community for Utah Women and Girls (UWAG) by using the principles of community-based participatory research is currently
o Studying the effect of Community Wellness Coaches in each community o Working with women to improve physical activity and diet to prevent obesity and its
associated co-morbidities o Comparing a high-intensive to a low-intensive intervention o Studying the associated cost effectiveness of the intervention
Utah Rural Outreach Program (UROP) is an outreach program that directly addresses the
issue of disproportionately low numbers of health care providers in rural and frontier Utah through the promotion of health care educational programs to rural high school students. Additional details were provided in section 1.4.
Community faces of Utah is a multi-cultural consortium that includes leadership from the
African, African American, American Indian, Hispanic, and Pacific Islander communities as well as the University of Utah and Utah Department of Health. In conjunction with Drs. Simonsen and Dr. Gren’s research work with Community Faces of Utah, we also have PhD student involvement.
Global Health Initiative. Our working and learning environment is particularly diverse in that our Division oversees the Global Health Initiative (GHI; http://www.globalhealth.utah.edu), which is a cross disciplinary, multi-partner collaboration to address the triad of global human development challenges – health, education, and economic sustainability. We provide student, professor, and doctor exchanges with partner universities and hospitals worldwide while providing all participants a deeper understanding of each other’s areas of expertise. The GHI programs are active in Armenia, China, Ghana, India, Peru, Thailand, and Uganda.
Songdo Global University partnership. The Division is engaged in a partnership with the
Songdo Global University in Incheon, Korea. The Division is planning for an exchange of students between the two universities.
v. Policies and plans to develop, review and maintain curricula and other opportunities
including service learning that address and build competency in diversity and cultural considerations.
We consider service learning as community engaged scholarship. All of our Learning Abroad programs are designated as community engagement by the University of Utah Lowell Bennion Community Service Center. Requirements for this designation are “formerly known as service-learning, the Community Engaged Learning designation distinguishes courses on campus. Students in community engaged learning courses connect classroom concepts, knowledge, and theories with real people and needs by collaborating on projects and service opportunities designed by the students, faculty, and community partners. Projects meet the course’s academic goals and advance the community partner’s mission.” http://bennioncenter.org/faculty/learning/index.php The Division is involved in multiple community engagement opportunities through UWAG, the Honors College and Global Scholars, Community engagement not only links us to students but it also helps link potential students to us.
63
The Curriculum Committee reviews the syllabi of the courses to assure that competency building in diversity and culture continues for the students. Relevant curricula include the following courses, syllabi from each course can be found in the Reference File, Course syllabus:
FP MD 5520 Public Health Perspective on Surgery in the Global Context FP MD 5530/6530 Global Health FP MD 5540 Refugee Health FP MD 6502 International Public Health Issues FP MD 6531 Learning Abroad - International Fieldwork in Public Health FP MD 6600 Social Context in Public Health FP MD 7640 Research and Evaluation of Health Behavior
The courses build competency by exposing students to public health issues faced by diverse populations from around the world. Service learning projects are incorporated in many of these courses, further enhancing the training of our students to diversity.
vi. Policies and plans to recruit, develop, promote and retain a diverse faculty. The Division recognizes through our self-study assessment that diversity in faculty, staff, and students is an area we need to target. Beyond policy recruitment of faculty, staff, and students the Division has developed initiatives to connect and recruit from the Hispanic population by actively working with our partners around campus such as the Office of Inclusion and Outreach. The University of Utah Office for Equity and Diversity “recognizes that diverse faculty, student, and staff populations benefit and enrich the educational experiences of the entire campus and greater community. To this end, the Office of the Associate Vice President for Diversity is committed to removing barriers that have been traditionally encountered by individuals from underrepresented groups; strives to recruit students, faculty, and staff who will further enrich our campus diversity; and makes every attempt to support their academic, professional, and personal success while they are here.” “The faculty hiring process at the University of Utah is supervised by different offices to ensure compliance with federal and state regulations and recruit diverse pools of candidates. For academic departments and programs that are not part of the health sciences, the Office for Equity and Diversity provides oversight for faculty job posting and advertising, recruitment and position offers. The Office for Equal Opportunity and Affirmative Action ensures that federal and state reporting requirements are met. The Office for Faculty provides oversight for the faculty appointment, hire, and tenure processes. For the School of Medicine and other health science academic departments and programs, oversight is provided by The Office of Faculty Administration in the School of Medicine.” The Office for Equity and Diversity strives to meet three goals in faculty recruitment:
Provide information to help departments recruit diverse pools of candidates. Ensure that federal and state regulations are followed in recruitment and job offers. Provide information and resources to assist departments in attracting and securing outstanding
candidates.
64
vii. Policies and plans to recruit, develop, promote and retain a diverse staff. http://regulations.utah.edu/human-resources/5-106.php The University of Utah is an "Equal Opportunity Employer," and is fully committed to the principle of nondiscrimination in all employment-related practices and decisions, including, but not limited to, recruitment, hiring, supervision, promotion, compensation, benefits, termination, and all other practices and decisions affecting university employment status, rights, and privileges.
viii. Policies and plans to recruit, admit, retain and graduate a diverse student body. The Office for Student Equity and Diversity (SED) at the University of Utah is the student programming and support Division of the University of Utah Office for Equity and Diversity. The office provides leadership, education, and coordination of all student diversity support programs, initiatives, and cultural events. Collectively the programs serve over 3,000 students annually who self-identify as LGBT and/or historically underrepresented students of color. The following programs are part of the Office for Student Equity and Diversity: the American Indian Resource Center, Center for Ethnic Student Affairs (CESA), the Lesbian Gay Bisexual Transgender Resource Center, and Scholarships & Grants. Part of our developing student recruitment plan is reviewing the under-represented communities throughout our state and our outreach involvement with AHEC, UROP, Office of Inclusion and Outreach and main campus. In addition, the Division has several minority scholarships aimed at recruiting and retaining diverse students, including:
The Senator Pete Suazo Memorial Endowed Hispanic Scholarship in Public Health: Established in honor of the late Utah State Senator Pete Suazo, who was a leader in public health issues for all Utahans. This scholarship is awarded to an applicant of Hispanic descent fully matriculated in the Division.
The Minority Endowed Scholarship in Public Health: Established to support qualified minority
students in the Division.
F. Marian Bishop Scholarship: Established to support a qualified female student who is fully matriculated and in good standing in the Public Health Program at the University of Utah.
ix. Regular evaluation of the effectiveness of the above-listed measures. We assess the following as evaluation of the effectiveness of the above-listed measures:
The number of students from minority groups and rural areas Number of faculty recruited from minority groups Partnerships with community groups Administration of the Hispanic and minority scholarships Global health summer programs completed successfully Courses completed that build competency in diversity and cultural considerations
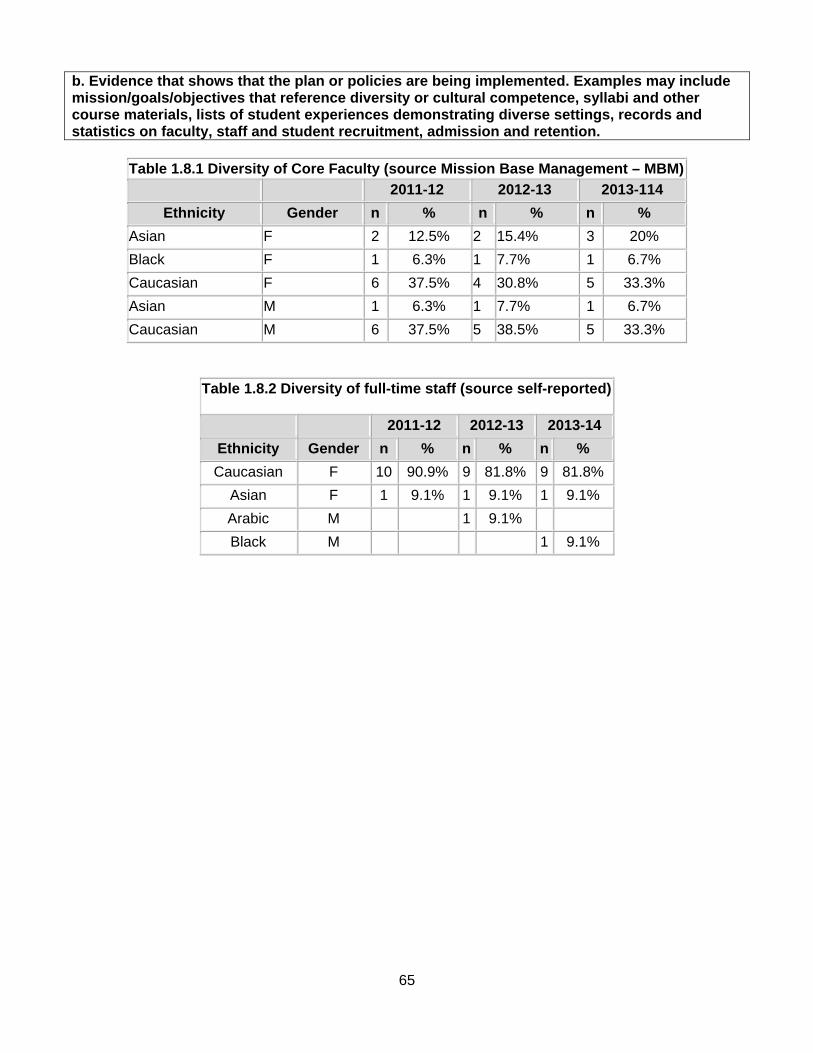
65
b. Evidence that shows that the plan or policies are being implemented. Examples may include mission/goals/objectives that reference diversity or cultural competence, syllabi and other course materials, lists of student experiences demonstrating diverse settings, records and statistics on faculty, staff and student recruitment, admission and retention.
Table 1.8.1 Diversity of Core Faculty (source Mission Base Management – MBM)
2011-12 2012-13 2013-114
Ethnicity Gender n % n % n %
Asian F 2 12.5% 2 15.4% 3 20%
Black F 1 6.3% 1 7.7% 1 6.7%
Caucasian F 6 37.5% 4 30.8% 5 33.3%
Asian M 1 6.3% 1 7.7% 1 6.7%
Caucasian M 6 37.5% 5 38.5% 5 33.3%
Table 1.8.2 Diversity of full-time staff (source self-reported)
2011-12 2012-13 2013-14
Ethnicity Gender n % n % n %
Caucasian F 10 90.9% 9 81.8% 9 81.8%
Asian F 1 9.1% 1 9.1% 1 9.1%
Arabic M 1 9.1%
Black M 1 9.1%
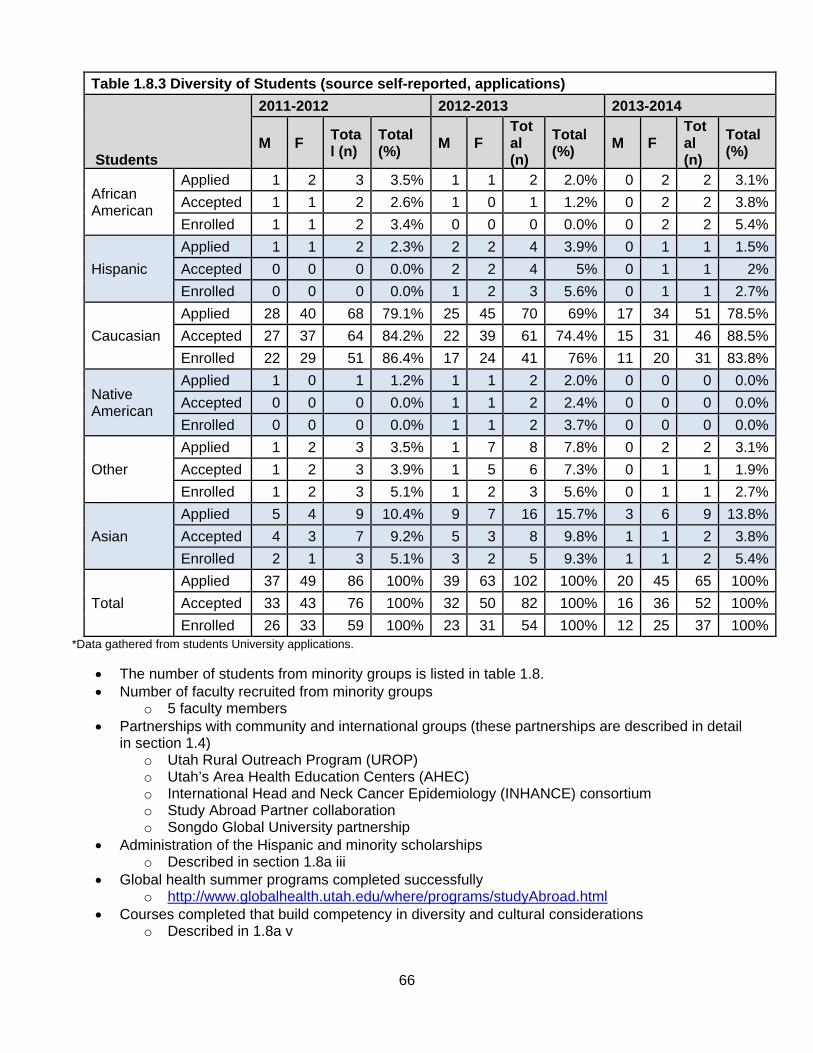
66
Table 1.8.3 Diversity of Students (source self-reported, applications)
Students
2011-2012 2012-2013 2013-2014
M F Total (n)
Total (%)
M F Total (n)
Total (%)
M F Total (n)
Total (%)
African American
Applied 1 2 3 3.5% 1 1 2 2.0% 0 2 2 3.1%
Accepted 1 1 2 2.6% 1 0 1 1.2% 0 2 2 3.8%
Enrolled 1 1 2 3.4% 0 0 0 0.0% 0 2 2 5.4%
Hispanic
Applied 1 1 2 2.3% 2 2 4 3.9% 0 1 1 1.5%
Accepted 0 0 0 0.0% 2 2 4 5% 0 1 1 2%
Enrolled 0 0 0 0.0% 1 2 3 5.6% 0 1 1 2.7%
Caucasian
Applied 28 40 68 79.1% 25 45 70 69% 17 34 51 78.5%
Accepted 27 37 64 84.2% 22 39 61 74.4% 15 31 46 88.5%
Enrolled 22 29 51 86.4% 17 24 41 76% 11 20 31 83.8%
Native American
Applied 1 0 1 1.2% 1 1 2 2.0% 0 0 0 0.0%
Accepted 0 0 0 0.0% 1 1 2 2.4% 0 0 0 0.0%
Enrolled 0 0 0 0.0% 1 1 2 3.7% 0 0 0 0.0%
Other
Applied 1 2 3 3.5% 1 7 8 7.8% 0 2 2 3.1%
Accepted 1 2 3 3.9% 1 5 6 7.3% 0 1 1 1.9%
Enrolled 1 2 3 5.1% 1 2 3 5.6% 0 1 1 2.7%
Asian
Applied 5 4 9 10.4% 9 7 16 15.7% 3 6 9 13.8%
Accepted 4 3 7 9.2% 5 3 8 9.8% 1 1 2 3.8%
Enrolled 2 1 3 5.1% 3 2 5 9.3% 1 1 2 5.4%
Total
Applied 37 49 86 100% 39 63 102 100% 20 45 65 100%
Accepted 33 43 76 100% 32 50 82 100% 16 36 52 100%
Enrolled 26 33 59 100% 23 31 54 100% 12 25 37 100%*Data gathered from students University applications.
The number of students from minority groups is listed in table 1.8. Number of faculty recruited from minority groups
o 5 faculty members Partnerships with community and international groups (these partnerships are described in detail
in section 1.4) o Utah Rural Outreach Program (UROP) o Utah’s Area Health Education Centers (AHEC) o International Head and Neck Cancer Epidemiology (INHANCE) consortium o Study Abroad Partner collaboration o Songdo Global University partnership
Administration of the Hispanic and minority scholarships o Described in section 1.8a iii
Global health summer programs completed successfully o http://www.globalhealth.utah.edu/where/programs/studyAbroad.html
Courses completed that build competency in diversity and cultural considerations o Described in 1.8a v
67
c. Description of how the diversity plan or policies were developed, including an explanation of the constituent groups involved. In reviewing the mission of the Division, in conjunction with our annual retreat and followed up with the Administrative and Leadership Committees commitment to stewardship, it was determined that the dimensions of urban and rural distributions, gender representation, race and ethnicity were lacking. In response to this development the Division has created a subcommittee to maintain focus on this issue. The committee will include faculty members Dr. Jessica Greenwood, Dr. Steve Alder, Dr. Yelena Wu, staff member Courtney DeMond, and Sharon Austin (student representation). Any proposed faculty appointment is publicly advertised in compliance with Office of Equal Opportunity and Affirmative Action (OEO/AA). It is the policy of the University of Utah to include members of minority groups, women, and members of other protected classes on Search Committees, to strive to increase the inclusion of women and minorities in the applicant pool as well as to pay particular attention to applicants that fall into those categories. The Division Chief appoints a new search committee per each faculty applicant. In an effort to ensure compliance with federal guidelines in hiring, effective July 1, 2005, departments that open new tenure track positions must meet with a representative from the OEO/AA. d. Description of how the plan or policies are monitored, how the plan is used by the program and how often the plan is reviewed. To monitor the policies and plan we have determined to follow the guidelines of 67% urban, 33% rural distribution. We aim for a balanced gender and racial distribution that reflects the under-representation of minority groups not only in public health, but in our community as well. Through the use of the Population by Race and Hispanic Origin: Utah Counties (2012), we recognize under-representation of Hispanic groups across students, faculty, and staff. In working with Community Faces of Utah and Utah Hispanic Health Alliance, our community partners directly connected to the Hispanic community as well as the Office of Inclusion and Outreach, we will create an effective strategy for recruitment support across these dimensions engaged in public health. Through these connections we are planning on making the review of our diversity an annual retreat topic.
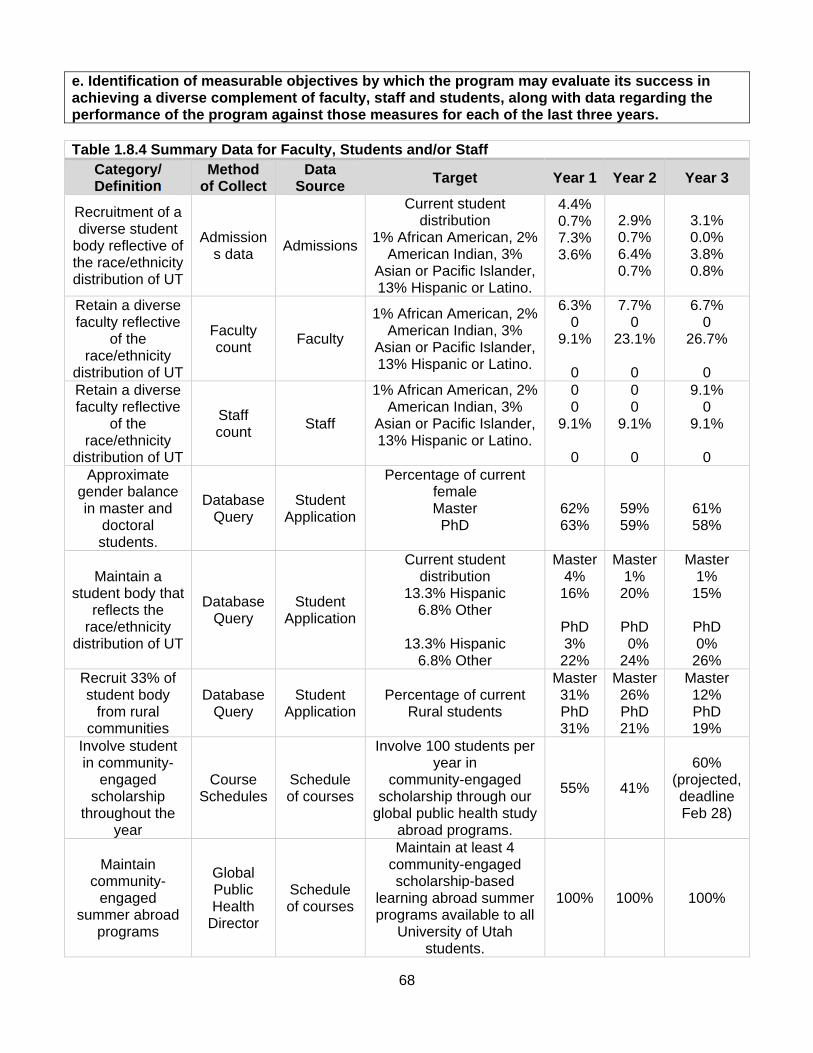
68
e. Identification of measurable objectives by which the program may evaluate its success in achieving a diverse complement of faculty, staff and students, along with data regarding the performance of the program against those measures for each of the last three years. Table 1.8.4 Summary Data for Faculty, Students and/or Staff
Category/ Definition
Method of Collect
Data Source
Target Year 1 Year 2 Year 3
Recruitment of a diverse student
body reflective of the race/ethnicity distribution of UT
Admissions data
Admissions
Current student distribution
1% African American, 2% American Indian, 3%
Asian or Pacific Islander, 13% Hispanic or Latino.
4.4% 0.7% 7.3% 3.6%
2.9% 0.7% 6.4% 0.7%
3.1% 0.0% 3.8% 0.8%
Retain a diverse faculty reflective
of the race/ethnicity
distribution of UT
Faculty count
Faculty
1% African American, 2% American Indian, 3%
Asian or Pacific Islander, 13% Hispanic or Latino.
6.3% 0
9.1%
0
7.7% 0
23.1%
0
6.7% 0
26.7%
0 Retain a diverse faculty reflective
of the race/ethnicity
distribution of UT
Staff count
Staff
1% African American, 2% American Indian, 3%
Asian or Pacific Islander, 13% Hispanic or Latino.
0 0
9.1%
0
0 0
9.1%
0
9.1% 0
9.1%
0 Approximate
gender balance in master and
doctoral students.
Database Query
Student Application
Percentage of current female Master PhD
62% 63%
59% 59%
61% 58%
Maintain a student body that
reflects the race/ethnicity
distribution of UT
Database Query
Student Application
Current student distribution
13.3% Hispanic 6.8% Other
13.3% Hispanic
6.8% Other
Master 4%
16%
PhD 3%
22%
Master1%
20%
PhD 0% 24%
Master 1%
15%
PhD 0%
26% Recruit 33% of student body
from rural communities
Database Query
Student Application
Percentage of current Rural students
Master 31% PhD 31%
Master26% PhD 21%
Master 12% PhD 19%
Involve student in community-
engaged scholarship
throughout the year
Course Schedules
Schedule of courses
Involve 100 students per year in
community-engaged scholarship through our
global public health study abroad programs.
55% 41%
60% (projected, deadline Feb 28)
Maintain community-
engaged summer abroad
programs
Global Public Health
Director
Schedule of courses
Maintain at least 4 community-engaged scholarship-based
learning abroad summer programs available to all
University of Utah students.
100% 100% 100%
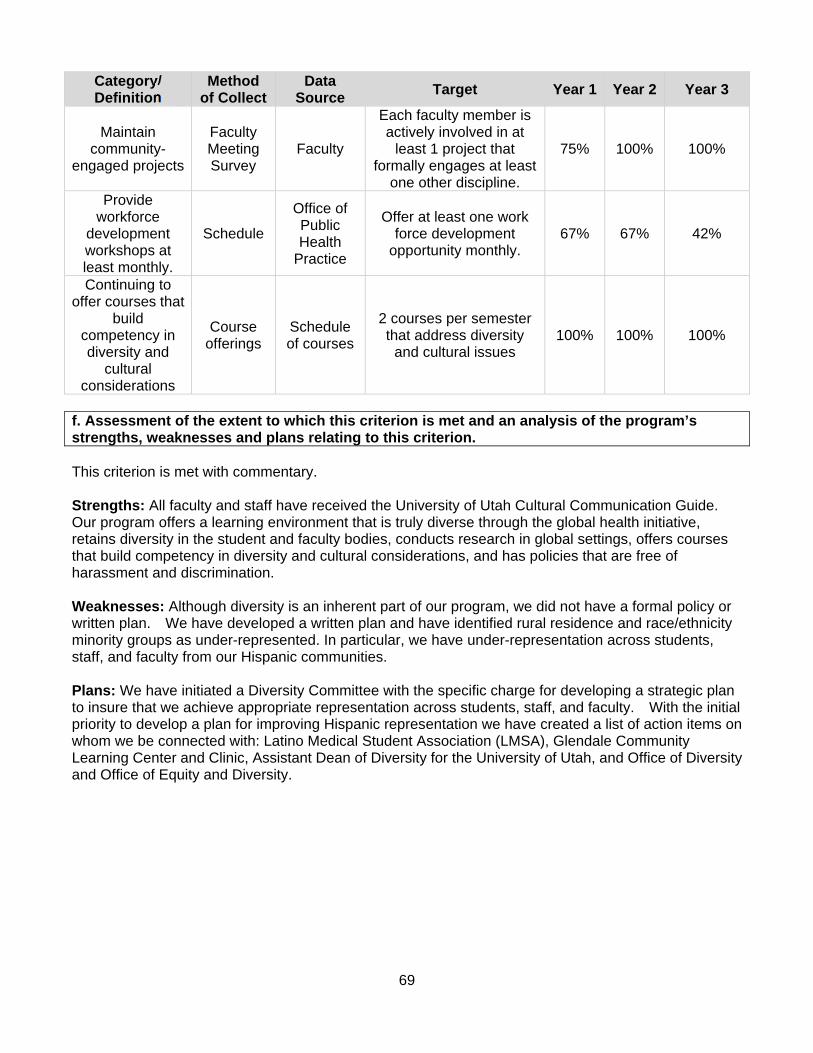
69
Category/ Definition
Method of Collect
Data Source
Target Year 1 Year 2 Year 3
Maintain community-
engaged projects
Faculty Meeting Survey
Faculty
Each faculty member is actively involved in at
least 1 project that formally engages at least
one other discipline.
75% 100% 100%
Provide workforce
development workshops at least monthly.
Schedule
Office of Public Health
Practice
Offer at least one work force development
opportunity monthly. 67% 67% 42%
Continuing to offer courses that
build competency in diversity and
cultural considerations
Course offerings
Schedule of courses
2 courses per semester that address diversity
and cultural issues 100% 100% 100%
f. Assessment of the extent to which this criterion is met and an analysis of the program’s strengths, weaknesses and plans relating to this criterion. This criterion is met with commentary. Strengths: All faculty and staff have received the University of Utah Cultural Communication Guide. Our program offers a learning environment that is truly diverse through the global health initiative, retains diversity in the student and faculty bodies, conducts research in global settings, offers courses that build competency in diversity and cultural considerations, and has policies that are free of harassment and discrimination. Weaknesses: Although diversity is an inherent part of our program, we did not have a formal policy or written plan. We have developed a written plan and have identified rural residence and race/ethnicity minority groups as under-represented. In particular, we have under-representation across students, staff, and faculty from our Hispanic communities. Plans: We have initiated a Diversity Committee with the specific charge for developing a strategic plan to insure that we achieve appropriate representation across students, staff, and faculty. With the initial priority to develop a plan for improving Hispanic representation we have created a list of action items on whom we be connected with: Latino Medical Student Association (LMSA), Glendale Community Learning Center and Clinic, Assistant Dean of Diversity for the University of Utah, and Office of Diversity and Office of Equity and Diversity.
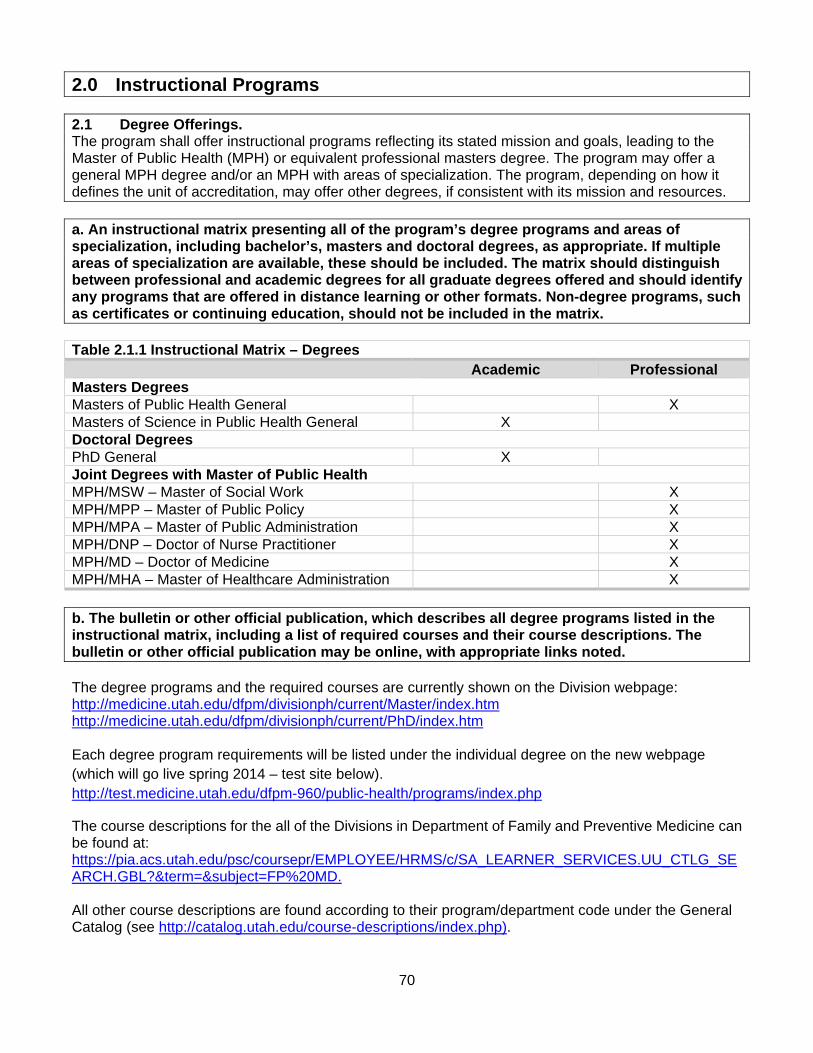
70
2.0 Instructional Programs 2.1 Degree Offerings. The program shall offer instructional programs reflecting its stated mission and goals, leading to the Master of Public Health (MPH) or equivalent professional masters degree. The program may offer a general MPH degree and/or an MPH with areas of specialization. The program, depending on how it defines the unit of accreditation, may offer other degrees, if consistent with its mission and resources. a. An instructional matrix presenting all of the program’s degree programs and areas of specialization, including bachelor’s, masters and doctoral degrees, as appropriate. If multiple areas of specialization are available, these should be included. The matrix should distinguish between professional and academic degrees for all graduate degrees offered and should identify any programs that are offered in distance learning or other formats. Non-degree programs, such as certificates or continuing education, should not be included in the matrix. Table 2.1.1 Instructional Matrix – Degrees Academic Professional Masters Degrees Masters of Public Health General X Masters of Science in Public Health General X Doctoral Degrees PhD General X Joint Degrees with Master of Public Health MPH/MSW – Master of Social Work X MPH/MPP – Master of Public Policy X MPH/MPA – Master of Public Administration X MPH/DNP – Doctor of Nurse Practitioner X MPH/MD – Doctor of Medicine X MPH/MHA – Master of Healthcare Administration X b. The bulletin or other official publication, which describes all degree programs listed in the instructional matrix, including a list of required courses and their course descriptions. The bulletin or other official publication may be online, with appropriate links noted. The degree programs and the required courses are currently shown on the Division webpage: http://medicine.utah.edu/dfpm/divisionph/current/Master/index.htm http://medicine.utah.edu/dfpm/divisionph/current/PhD/index.htm Each degree program requirements will be listed under the individual degree on the new webpage (which will go live spring 2014 – test site below). http://test.medicine.utah.edu/dfpm-960/public-health/programs/index.php
The course descriptions for the all of the Divisions in Department of Family and Preventive Medicine can be found at: https://pia.acs.utah.edu/psc/coursepr/EMPLOYEE/HRMS/c/SA_LEARNER_SERVICES.UU_CTLG_SEARCH.GBL?&term=&subject=FP%20MD. All other course descriptions are found according to their program/department code under the General Catalog (see http://catalog.utah.edu/course-descriptions/index.php).

71
c. Assessment of the extent to which this criterion is met and an analysis of the program’s strengths, weaknesses and plans relating to this criterion. This criterion is met. Strengths: Our degree programs are well established as general public health offerings for both professional (MPH) and academic (MSPH and PhD) education. In addition, the joint degree programming offers students the option of linking graduate work in Public Health with education in related disciplines, providing them with the option of strengthening their educational experience through these cross-disciplinary relationships. Weaknesses: Providing clear distinction between our professional and academic degrees is needed. Additionally, sequencing (MPH to DrPH and MSPH to PhD) needs refinement. Plans: We are currently developing a revised degree strategy that will enhance the distinction between professional and academic degrees. We are also developing the sequencing that will more closely align master-level and doctoral education. This will be the focus for our Spring 2014 faculty retreat.
72
2.2 Program Length. An MPH degree program or equivalent professional master’s degree must be at least 42 semester-credit units in length. a. Definition of a credit with regard to classroom/contact hours. Most classes offered through the Division are 3 credits and carry 96 contact hours. The Division’s general rule with regards to classroom/contact hours at the graduate level is for every (1) one hour of class during the week we expect (2) two hours of additional outside work per week. The Division is on semesters, with 16 weeks in spring (January – May), 12 weeks in summer (May – August), and 16 weeks in fall (August – December). b. Information about the minimum degree requirements for all professional public health master’s degree curricula shown in the instructional matrix. If the program or university uses a unit of academic credit or an academic term different from the standard semester or quarter, this difference should be explained and an equivalency presented in a table or narrative. The MPH degree offered by the Division requires completion of 45 credit hours, which includes 24 credits in core courses, 15 credits in electives and 6 credits in a practicum. Specific classes required for the MPH can be found in the Appendix 2.2A. c. Information about the number of professional public health master’s degrees awarded for fewer than 42 semester credit units, or equivalent, over each of the last three years. A summary of the reasons should be included. No MPH students have graduated with fewer than 42 credits in the last three years. d. Assessment of the extent to which this criterion is met and an analysis of the program’s strengths, weaknesses and plans relating to this criterion. This criterion is met. Strengths: The MPH program has required at least 45 semester hours of coursework since 2006. The content of these course requirements has achieved a successful balance between education and practice. Weaknesses: None noted. Plans: We will continue to evaluate curricular requirements and content on an annual basis.
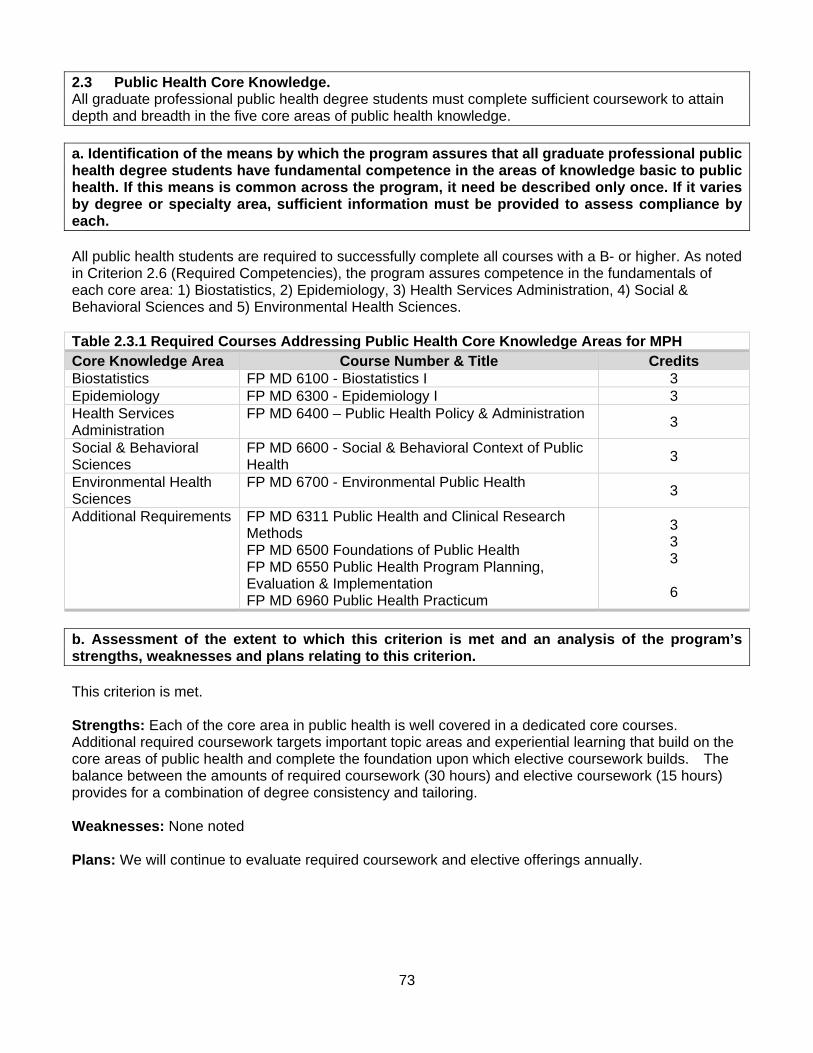
73
2.3 Public Health Core Knowledge. All graduate professional public health degree students must complete sufficient coursework to attain depth and breadth in the five core areas of public health knowledge. a. Identification of the means by which the program assures that all graduate professional public health degree students have fundamental competence in the areas of knowledge basic to public health. If this means is common across the program, it need be described only once. If it varies by degree or specialty area, sufficient information must be provided to assess compliance by each. All public health students are required to successfully complete all courses with a B- or higher. As noted in Criterion 2.6 (Required Competencies), the program assures competence in the fundamentals of each core area: 1) Biostatistics, 2) Epidemiology, 3) Health Services Administration, 4) Social & Behavioral Sciences and 5) Environmental Health Sciences. Table 2.3.1 Required Courses Addressing Public Health Core Knowledge Areas for MPH Core Knowledge Area Course Number & Title Credits Biostatistics FP MD 6100 - Biostatistics I 3 Epidemiology FP MD 6300 - Epidemiology I 3 Health Services Administration
FP MD 6400 – Public Health Policy & Administration 3
Social & Behavioral Sciences
FP MD 6600 - Social & Behavioral Context of Public Health
3
Environmental Health Sciences
FP MD 6700 - Environmental Public Health 3
Additional Requirements FP MD 6311 Public Health and Clinical Research Methods FP MD 6500 Foundations of Public Health FP MD 6550 Public Health Program Planning, Evaluation & Implementation FP MD 6960 Public Health Practicum
3 3 3
6
b. Assessment of the extent to which this criterion is met and an analysis of the program’s strengths, weaknesses and plans relating to this criterion. This criterion is met. Strengths: Each of the core area in public health is well covered in a dedicated core courses. Additional required coursework targets important topic areas and experiential learning that build on the core areas of public health and complete the foundation upon which elective coursework builds. The balance between the amounts of required coursework (30 hours) and elective coursework (15 hours) provides for a combination of degree consistency and tailoring. Weaknesses: None noted Plans: We will continue to evaluate required coursework and elective offerings annually.
74
2.4 Practical Skills. All graduate professional public health degree students must develop skills in basic public health concepts and demonstrate the application of these concepts through a practice experience that is relevant to students’ areas of specialization. a. Description of the program’s policies and procedures regarding practice placements, including the following: selection of sites, methods for approving preceptors, opportunities for orientation and support for preceptors, approaches for faculty supervision of students, means of evaluating student performance, means of evaluating practice placement sites and preceptor qualifications, criteria for waiving, altering or reducing the experience, if applicable Masters Practicum: All MPH students must complete 6 credit hours (270 hours fieldwork) of practicum prior to graduation. The practicum experience is meant to give students direct, hands-on experience comparable to a career position suitable for someone with an MPH. This will not only supplement the student’s coursework and enrich their academic experience, but also prepare the student for employment after completion of their degree. All Practicum forms can be found http://medicine.utah.edu/dfpm/divisionph/current/Master/MPH-MSPH_Forms.htm The goals of the practicum are:
1. To integrate foundational public health knowledge with a concrete experience of public health practice. In particular, to observe and report how the following concepts play out in real public health practice:
o the core functions of public health, o the core organizational practices necessary for governmental agencies to carry out the
mission of public health, and o the essential public health services, from a community-based perspective.
2. To identify and report the issues in cultural competence relevant to a specific practicum site and how they play out in real public health practice.
3. To identify emerging areas in the practice of public health. 4. To broaden knowledge and skills in public health practice. 5. To gain experience working with a mentor that has the academic credentials and experience to
oversee and evaluate masters level student goals and activities.
Masters students are not eligible to start their practicum until they have completed and passed with B- or above the prerequisite courses: FPMD 6100 Biostatistics I, FPMD 6300 Epidemiology I, FPMD 6400 Public Health Policy & Administration, FPMD 6500 Foundations of Public Health, FPMD 6600 Social & Behavioral Context of Public Health, and FPMD 6700 Environmental Public Health. A practicum site should expect that the students will come prepared to contribute as well as learn.
Selection of sites Master Practicum sites must be related to an area of public health the student is interested in. They may be public or private based and can be either clinical, community based or research in emphasis. They can be local, national, or international. A review of the site is completed before students receive approval to undertake the practicum experience.
Methods for approving preceptors
Master students preceptors must have a minimum of a Masters degree or higher in a field that matches or is closely related to the public health practicum topic that the student has chosen.
75
Our practicum coordinator and faculty advisor reviews and evaluates the preceptor’s qualifications by reviewing the Mentor Credentials and CV.
Opportunities for orientation and support for preceptors
The practicum coordinator provides support for preceptors on an ongoing basis throughout the practicum period. Preceptors have access to the practicum coordinator for any questions and issues. The Mentor Evaluations are submitted to the practicum coordinator and then used to evaluate the quality and amount of work completed by each student. Currently, there is not a process in place for support of first-time preceptors. We will create a handbook of criteria and expectations as well as have check-ins and possibly meetings by the practicum coordinator for our future first-time preceptors.
Approaches for faculty supervision of students
The student’s faculty advisor works with the student, in developing the student’s project. This meeting can happen either before and/or after the student has met with practicum mentor and practicum coordinator. Once the project is developed and Practicum Objectives form is completed it is reviewed by practicum coordinator to be sure it meets the program requirements. The practicum coordinator has the final sign off on the completed Objective form before the student is able to register for classes. The faculty advisor and practicum coordinator are available to students during their practicum to address issues that may arise that would affect the ability of the student in successful completion of the project.
Means of evaluating student performance
Each student is required to submit a written summary of his/her project. In addition the practicum mentor prepares a Mentor Evaluation form and submits it. The practicum coordinator then reviews each written report submitted, against the practicum objectives worksheet. A grade of Credit or No Credit is awarded following the practicum coordinator’s review with the consideration of the mentors evaluation.
Means of evaluating practice placement sites and preceptor qualifications
The preceptor qualifications are reviewed by the practicum coordinator and practicum instructor. Students submit two Student Evaluation forms which provide us with ongoing review of the site and the mentor. The first evaluation form contains student identifiers and the second student evaluation does not in order to allow the student to give candid responses. The second Student Evaluation form is found in a public binder in the Academic Advisors office (See Student Practicum Evaluations binder).
Criteria for waiving, altering or reducing the experience, if applicable We do not allow the practicum to be waived.
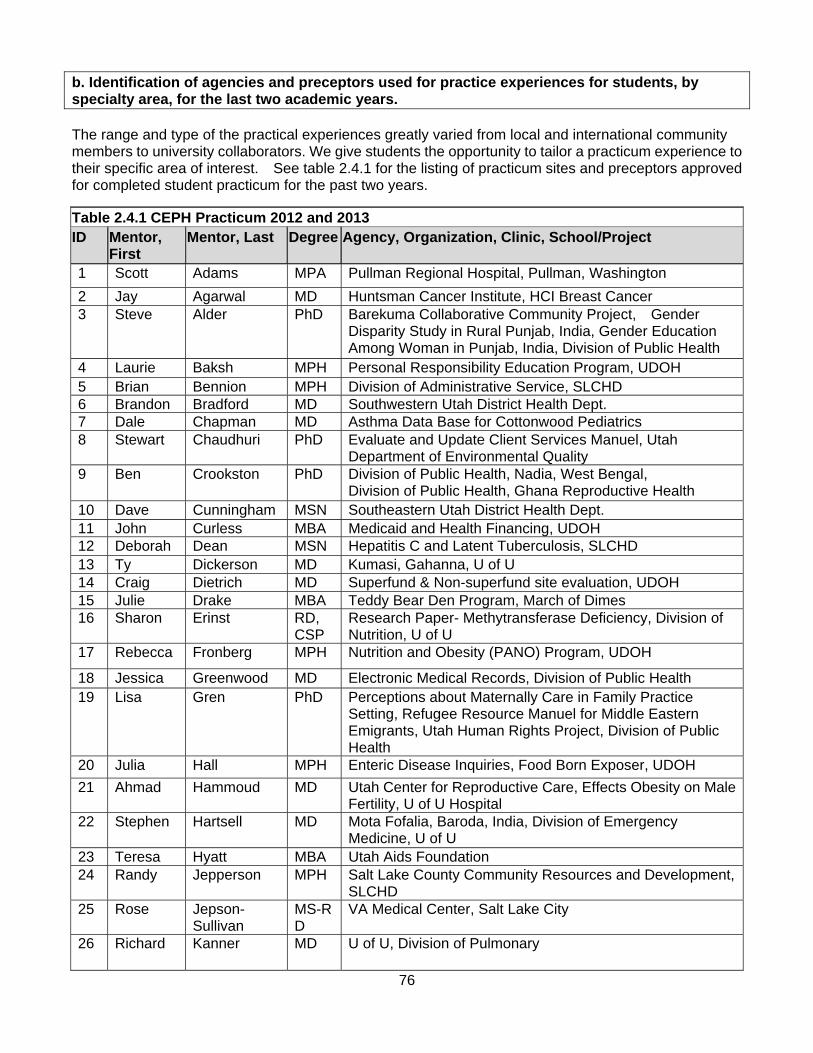
76
b. Identification of agencies and preceptors used for practice experiences for students, by specialty area, for the last two academic years. The range and type of the practical experiences greatly varied from local and international community members to university collaborators. We give students the opportunity to tailor a practicum experience to their specific area of interest. See table 2.4.1 for the listing of practicum sites and preceptors approved for completed student practicum for the past two years.
Table 2.4.1 CEPH Practicum 2012 and 2013 ID Mentor,
First Mentor, Last Degree Agency, Organization, Clinic, School/Project
1 Scott Adams MPA Pullman Regional Hospital, Pullman, Washington
2 Jay Agarwal MD Huntsman Cancer Institute, HCI Breast Cancer 3 Steve Alder PhD Barekuma Collaborative Community Project, Gender
Disparity Study in Rural Punjab, India, Gender Education Among Woman in Punjab, India, Division of Public Health
4 Laurie Baksh MPH Personal Responsibility Education Program, UDOH 5 Brian Bennion MPH Division of Administrative Service, SLCHD 6 Brandon Bradford MD Southwestern Utah District Health Dept. 7 Dale Chapman MD Asthma Data Base for Cottonwood Pediatrics 8 Stewart Chaudhuri PhD Evaluate and Update Client Services Manuel, Utah
Department of Environmental Quality 9 Ben Crookston PhD Division of Public Health, Nadia, West Bengal,
Division of Public Health, Ghana Reproductive Health 10 Dave Cunningham MSN Southeastern Utah District Health Dept. 11 John Curless MBA Medicaid and Health Financing, UDOH 12 Deborah Dean MSN Hepatitis C and Latent Tuberculosis, SLCHD 13 Ty Dickerson MD Kumasi, Gahanna, U of U 14 Craig Dietrich MD Superfund & Non-superfund site evaluation, UDOH 15 Julie Drake MBA Teddy Bear Den Program, March of Dimes 16 Sharon Erinst RD,
CSP Research Paper- Methytransferase Deficiency, Division of Nutrition, U of U
17 Rebecca Fronberg MPH Nutrition and Obesity (PANO) Program, UDOH
18 Jessica Greenwood MD Electronic Medical Records, Division of Public Health 19 Lisa Gren PhD Perceptions about Maternally Care in Family Practice
Setting, Refugee Resource Manuel for Middle Eastern Emigrants, Utah Human Rights Project, Division of Public Health
20 Julia Hall MPH Enteric Disease Inquiries, Food Born Exposer, UDOH
21 Ahmad Hammoud MD Utah Center for Reproductive Care, Effects Obesity on Male Fertility, U of U Hospital
22 Stephen Hartsell MD Mota Fofalia, Baroda, India, Division of Emergency Medicine, U of U
23 Teresa Hyatt MBA Utah Aids Foundation 24 Randy Jepperson MPH Salt Lake County Community Resources and Development,
SLCHD 25 Rose Jepson-
Sullivan MS-RD
VA Medical Center, Salt Lake City
26 Richard Kanner MD U of U, Division of Pulmonary
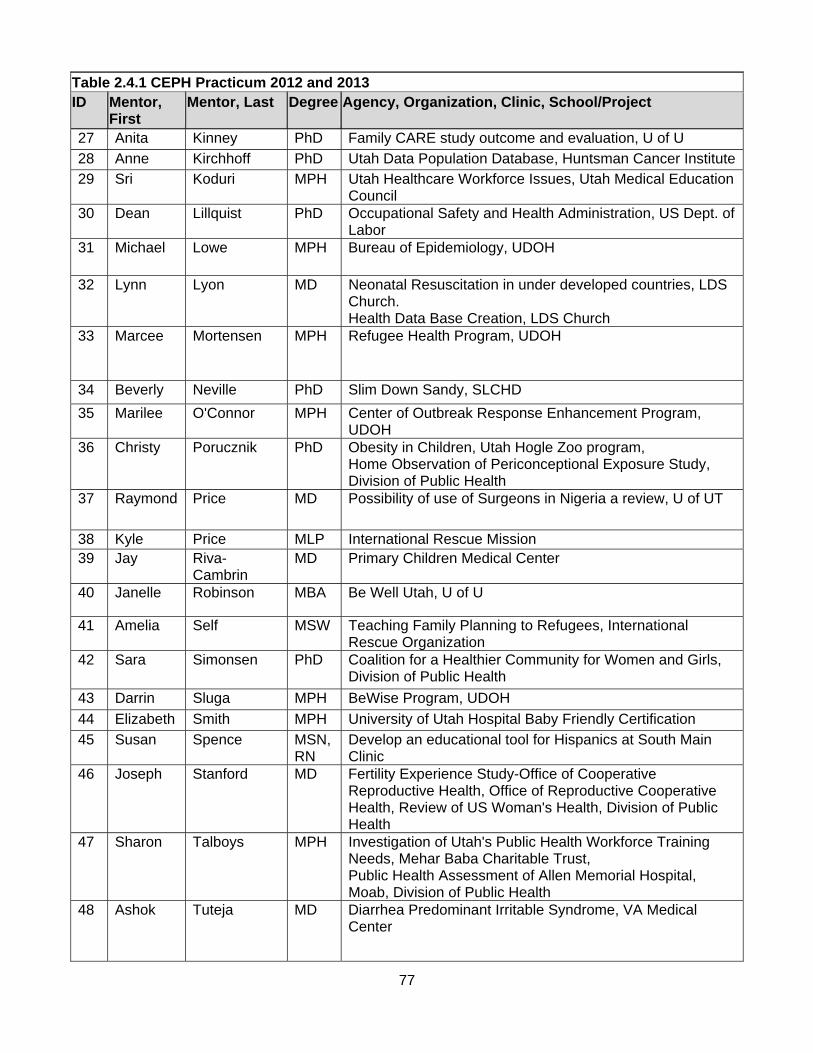
77
Table 2.4.1 CEPH Practicum 2012 and 2013 ID Mentor,
First Mentor, Last Degree Agency, Organization, Clinic, School/Project
27 Anita Kinney PhD Family CARE study outcome and evaluation, U of U
28 Anne Kirchhoff PhD Utah Data Population Database, Huntsman Cancer Institute29 Sri Koduri MPH Utah Healthcare Workforce Issues, Utah Medical Education
Council 30 Dean Lillquist PhD Occupational Safety and Health Administration, US Dept. of
Labor 31 Michael Lowe MPH Bureau of Epidemiology, UDOH
32 Lynn Lyon MD Neonatal Resuscitation in under developed countries, LDS Church. Health Data Base Creation, LDS Church
33 Marcee Mortensen MPH Refugee Health Program, UDOH
34 Beverly Neville PhD Slim Down Sandy, SLCHD
35 Marilee O'Connor MPH Center of Outbreak Response Enhancement Program, UDOH
36 Christy Porucznik PhD Obesity in Children, Utah Hogle Zoo program, Home Observation of Periconceptional Exposure Study, Division of Public Health
37 Raymond Price MD Possibility of use of Surgeons in Nigeria a review, U of UT
38 Kyle Price MLP International Rescue Mission 39 Jay Riva-
Cambrin MD Primary Children Medical Center
40 Janelle Robinson MBA Be Well Utah, U of U
41 Amelia Self MSW Teaching Family Planning to Refugees, International Rescue Organization
42 Sara Simonsen PhD Coalition for a Healthier Community for Women and Girls, Division of Public Health
43 Darrin Sluga MPH BeWise Program, UDOH
44 Elizabeth Smith MPH University of Utah Hospital Baby Friendly Certification
45 Susan Spence MSN, RN
Develop an educational tool for Hispanics at South Main Clinic
46 Joseph Stanford MD Fertility Experience Study-Office of Cooperative Reproductive Health, Office of Reproductive Cooperative Health, Review of US Woman's Health, Division of Public Health
47 Sharon Talboys MPH Investigation of Utah's Public Health Workforce Training Needs, Mehar Baba Charitable Trust, Public Health Assessment of Allen Memorial Hospital, Moab, Division of Public Health
48 Ashok Tuteja MD Diarrhea Predominant Irritable Syndrome, VA Medical Center
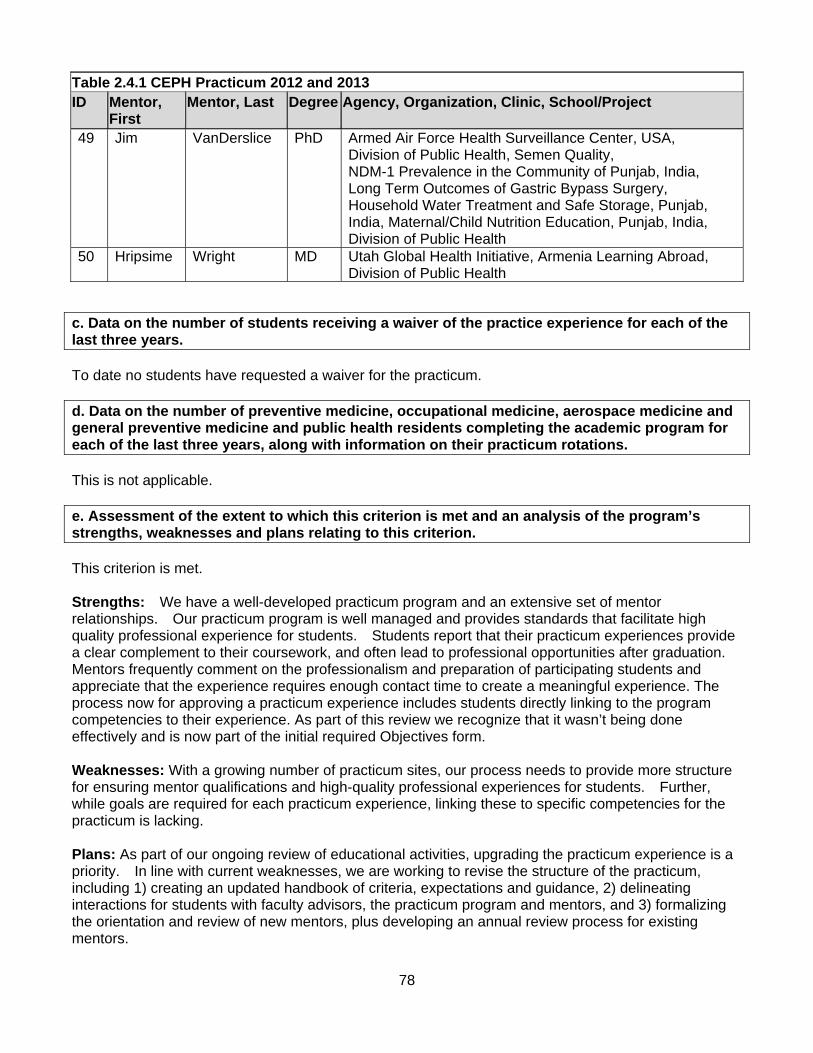
78
Table 2.4.1 CEPH Practicum 2012 and 2013 ID Mentor,
First Mentor, Last Degree Agency, Organization, Clinic, School/Project
49 Jim VanDerslice PhD Armed Air Force Health Surveillance Center, USA, Division of Public Health, Semen Quality, NDM-1 Prevalence in the Community of Punjab, India, Long Term Outcomes of Gastric Bypass Surgery, Household Water Treatment and Safe Storage, Punjab, India, Maternal/Child Nutrition Education, Punjab, India, Division of Public Health
50 Hripsime Wright MD Utah Global Health Initiative, Armenia Learning Abroad, Division of Public Health
c. Data on the number of students receiving a waiver of the practice experience for each of the last three years. To date no students have requested a waiver for the practicum. d. Data on the number of preventive medicine, occupational medicine, aerospace medicine and general preventive medicine and public health residents completing the academic program for each of the last three years, along with information on their practicum rotations. This is not applicable. e. Assessment of the extent to which this criterion is met and an analysis of the program’s strengths, weaknesses and plans relating to this criterion. This criterion is met. Strengths: We have a well-developed practicum program and an extensive set of mentor relationships. Our practicum program is well managed and provides standards that facilitate high quality professional experience for students. Students report that their practicum experiences provide a clear complement to their coursework, and often lead to professional opportunities after graduation. Mentors frequently comment on the professionalism and preparation of participating students and appreciate that the experience requires enough contact time to create a meaningful experience. The process now for approving a practicum experience includes students directly linking to the program competencies to their experience. As part of this review we recognize that it wasn’t being done effectively and is now part of the initial required Objectives form. Weaknesses: With a growing number of practicum sites, our process needs to provide more structure for ensuring mentor qualifications and high-quality professional experiences for students. Further, while goals are required for each practicum experience, linking these to specific competencies for the practicum is lacking. Plans: As part of our ongoing review of educational activities, upgrading the practicum experience is a priority. In line with current weaknesses, we are working to revise the structure of the practicum, including 1) creating an updated handbook of criteria, expectations and guidance, 2) delineating interactions for students with faculty advisors, the practicum program and mentors, and 3) formalizing the orientation and review of new mentors, plus developing an annual review process for existing mentors.
79
2.5 Culminating Experience. All graduate professional degree programs identified in the instructional matrix shall assure that each student demonstrates skills and integration of knowledge through a culminating experience.
a. Identification of the culminating experience required for each professional public health degree program. If this is common across the program’s professional degree programs, it need be described only once. If it varies by degree or specialty area, sufficient information must be provided to assess compliance by each. Comprehensive Examination (Master students) The comprehensive examination is the capstone of the master students in the Division of Public Health; here students apply their knowledge and skills learned in their coursework. The comprehensive examinations are offered the first two weeks of the semester. Students may sit for the examination once they have completed and passed the following Program required courses: Biostatistics I, Epidemiology I, Foundations of Public Health, Public Health Administration & Policy, Social and Behavioral Context of Public Health, Environmental Public Health. Starting in spring 2013, the Program Planning Implementation and Evaluation course will also be required. Students are not required to register for a specific course to sit for the exam, however, they are required to be registered for a minimum of three credits during the semester in which the examination is taken. The examination consists of complex questions based on a real-life public health issue. Groups of 4-6 qualifying students are divided into small random groups and assigned separate questions. The group must develop an in-depth report and presentation for the public health issue which includes literature review, and development of a public health project to address the issue. Both written and oral presentations are developed and presented to a Faculty Review Board of 3-5 members for evaluation (faculty selection of audience is based on available times). New questions are written each semester by faculty members and reviewed by the comprehensive exam committee. (Questions that have been used in the past can be found in the Reference File, Comprehensive Exam, Sample Questions.) The Faculty Review Boards are dependent on number of groups we have each semester. Once students sign up and are put into groups, a presentation sign-up sheet is passed around to faculty when available. When there are more than 5 groups each faculty member is asked to sign up for two groups. The Faculty Review Boards are usually different for each group. The determination of the contribution of each student member of the team is based on the groups Individual Students Contribution Forms as well as the Team Member Evaluation (Appendix 2.5A & 2.5B). The Faculty Review Boards also direct questions at individual team members to assess their knowledge of the project in full, as well as their contributions. They also review the students sections of their both written documents and presentation they are able to review the sections assigned to each student. Both written and oral presentations are developed and presented to a Faculty Review Board for evaluation. Measurable outcomes from the comprehensive examination are three-fold. First, to ascertain whether the student has both the specific and broad knowledge expected of someone holding a masters degree in public health and has met the core competencies of the public health program. Second, to determine whether the student has been able to integrate knowledge obtained from individual courses into unified concepts which link the student’s own interests to the other areas of public health. Third, to determine if this knowledge can be translated into solving a specific public health problem as part of a team. Students are assigned into teams and then provided approximately 1 week to develop a response, including deliverable items, to the issue. An interim report is required to be provided to an assigned
80
Academic Advisor via email to check each team’s progress. About two days after that each group will check in with designated faculty members. The purpose of this check in is to evaluate their progress and group dynamics and re-direct any efforts if necessary. It also serves as a useful interim deadline before which students must have something completed. About two days after that each group will be expected to submit the written component and Student Contribution (attached) to the Academic Advisor. Students will be notified of their status regarding the written and Contribution component approximately two days later. The possibilities are:
1. The written component has no more than minor problems. The group is cleared to prepare the final presentation and paper.
2. The written component has some deficiencies which will need to corrected, but the group will still present. Should the group fall into this category they will be required to complete revisions on the written component, due three days later to the Academic Advisor, using track changes feature. Students will either be cleared to continue with the presentation, or if they fail to address the deficiencies, the group will fail and be required to repeat the comprehensive exam.
3. The written component was insufficient. The group fails and must repeat the comprehensive exam during another semester.
Three days later five copies of the final version (hard copy and e-mailed) are due to the Academic Advisor by noon that includes, and is not limited to, final report, presentation materials, PowerPoint, handouts and Student Evaluation Worksheet. Two to three days later the students present. The final written documents are 20 pages in length, excluding appendices and references. The final presentation is 45 minutes in length and all students are required to present. After the students presentation, the Faculty Review Board takes 45 minutes to ask questions based on the students presentation and written report (Sample reports and PowerPoints Reference File Comprehensive Examination, Sample Report & Power Points). In the unlikely event students fail the Masters Comprehensive Exam, remediation will be provided as described below. Definition of failure: Any group whose composite score is below 70%. Remediation - When a group fails, they will be offered an opportunity for group remediation in the form of a single written document.
a. At the review following the oral presentation, the Faculty Adjudicators will discuss the presentation’s shortcomings with the students and propose specific steps that should be taken to address the shortcomings.
b. Within 24 hours, the Faculty Lead will summarize in writing the shortcomings and specific recommendations to be addressed in a written format by the student group. This memo (Memo #1) will be sent to the students in the group and the Faculty Adjudicators, with a copy to the Division Academic Advisor. In addition to the scientific considerations, the memo should contain any page limits, formatting or style requirements, and the deadline for re-submission of the students’ document (recommend 3-5 days).
c. The students will submit their document to the Division Academic Advisor, who will distribute the document to the Faculty Adjudicators.
d. The Faculty Adjudicators will review the document and evaluate whether the group passes, with reference to the specific recommendations given to the students. This step should be completed within 1 week.
e. A passing grade requires that, by the deadline, students satisfactorily address all of the
81
specific recommendations that were provided in Memo #1. f. If the group does not pass group remediation, students will be offered an opportunity for
individual remediation. i. Within 24 hours, the Faculty Lead will draft a second memo (Memo #2) that
outlines the outstanding issues with the remediation document. This memo will be addressed to the Division Chief, or his/her designee, with a copy to the Division Academic Advisor.
ii. Within 24 hours, the Division Chief (or designee) will draft a memo (Memo #3) to the students detailing the reason(s) for failure at the group remediation step. Each student will be offered a final opportunity for remediation by submission of an individual paper that addresses the requirements specified in Memo #1. The deadline for submission of the individual paper will be specified (recommend up to 1 week). A copy of this memo will be sent to the Division Academic Advisor.
iii. A passing grade requires that, by the deadline, the individual student satisfactorily addresses all of the specific recommendations that were provided in Memos #1 and #3. The faculty will have 1 week to review the individual remediation
iv. Failure of individual remediation will require that the student participate in the Comprehensive Exam during another semester. If the student is not registered for classes in that semester, s/he will need to register for 3 credit hours in the semester s/he plans to take the Comprehensive Exam.
b. Assessment of the extent to which this criterion is met and an analysis of the program’s strengths, weaknesses and plans relating to this criterion. This criterion is met. Strengths: The comprehensive examination provides a culminating learning experience and assessment for the student’s mastery of public health competencies included in their required coursework, and is augmented by elective coursework and the practicum experience. Given the professional focus of the MPH, projects are designed to simulate real-world and timely public health issues. The grading system is designed to assess both the collective team response as well as the contributions of each member. Weaknesses: With a refinement of the MPH competencies, the Comprehensive Exam needs to be refined to ensure that the competencies are well represented in each developed question and in the grading rubric. Plans: With newly adopted competencies, the Comprehensive Exam Committee is now responsible for appropriate revision of Comprehensive Exam guidelines to reflect alignment.
82
2.6 Required Competencies. For each degree program and area of specialization within each program identified in the instructional matrix, there shall be clearly stated competencies that guide the development of degree programs. The program must identify competencies for graduate professional, academic and baccalaureate public health degree programs. Additionally, the program must identify competencies for specializations within the degree programs at the all levels (bachelor’s, master’s and doctoral). a. Identification of a set of competencies that all graduate professional public health degree students and baccalaureate public health degree students, regardless of concentration, major or specialty area, must attain. There should be one set for each graduate professional public health degree and baccalaureate public health degree offered by the program (e.g., one set each for BSPH, MPH and DrPH). These competencies reflect knowledge in the core areas of public health, the ability to apply this knowledge at a high level (i.e., analysis, evaluation and synthesis), skills and attitudes underlying teamwork, appropriate community engagement and leadership, and specific technical skills in data use and analysis for assessment and program evaluation. Many of these competencies are derived from competencies developed by the Association of Schools and Programs in Public Health and the Council on Linkages. These Core Competencies apply to our MPH program, PhD, and MSPH students must meet these competencies as well as degree-specific competencies, described below. MPH Core Competencies At the time of graduation each MPH student should meet the following competencies: A. Principles of Public Health
1. Identify the behavioral determinants of complex public health issues, and apply behavioral theories to the development and implementation of program and policies.
2. Assess the impact of social, political, economic, and cultural forces on the development and implementation of health policy options and programs.
3. Discuss the inter-relationships between political and economic forces, technology, environmental processes and behaviors on exposures to environmental risk factors and subsequent health outcomes.
4. Evaluate the influence of behavioral, social, cultural, political, economic, environmental factors on the initiation and persistence of health disparities among sub-populations.
5. Describe the public health systems and structures at the local, region/state, national and international levels, and how their structure affects the development, delivery and quality of programs and policies.
B. Core Functions of Public Health: Assessment, Policy Development and Assurance
6. Utilize descriptive and inferential statistical methods and epidemiologic principles to:
a. Critically evaluate and interpret scientific evidence from published studies. b. Clearly articulate a public health issue and formulate relevant research questions. c. Design appropriate/effective methods for collecting health and risk factor data for community
needs assessments, surveillance, research, and program evaluation. d. Measure and compare the health status of populations. e. Evaluate public health interventions and f. provide a basis for making decisions and developing policy and recommendations.
83
7. Based on existing data and information, develop goals, measurable objectives, programmatic activities, and expected outcomes for a public health program.
C. Professionalism, Leadership and Community Engagement
8. Use team building, negotiation, and conflict management skills to achieve organizational and community health goals.
9. Demonstrate effective written and oral skills for communicating with a wide range of audiences and in a variety of public health practice settings.
10. Apply social justice and human rights principles and use the basic concepts and skills regarding culturally appropriate community engagement and empowerment when addressing community needs.
11. Recognize the ethical principles that underlie the values of integrity, respect, transparency, accountability and equity in public health practice.
MSPH Core Competencies At the time of graduation each MSPH student should meet the MPH Core Competencies, as well as competencies that reflect the skills to assist in and conduct public health assessment, evaluation and research. The addition Core Competencies for the MSPH degree are: 1. Synthesize existing research and develop a testable research hypothesis. 2. Be proficient in the use of a statistical programming language (SAS, STATA, R) for integrating
data, preparing data for analysis, managing databases and conducting descriptive and inferential statistics.
3. Describe the principles of the Human Subject Protection and apply these principles to the design and conduct of research.
PhD in Public Health Core Competencies PhD students are expected to meet not only the MPH Core Competencies described above, but to also meet a set of more advanced core competencies reflecting the skills and knowledge needed to conduct high quality public health research that reflects the ethical treatment of individuals and communities in the conduct of human research. At the time of graduation each PhD student should meet the following PhD Core Competencies:
1. Synthesize existing research and develop a testable research hypothesis. 2. Apply the basic tenets of public health to research problems. 3. Develop expertise in their area of study. 4. Create an appropriate study design to address a research question. 5. Describe the principles of the Human Subject Protection and apply these principles to the design
and conduct of research. 6. Demonstrate required skills for data collection, management and analysis. 7. Based on research findings, develop relevant programmatic and policy recommendations. 8. Effectively communicate research ideas and findings orally and in writing.
b. Identification of a set of competencies for each concentration, major or specialization (depending on the terminology used by the program) identified in the instructional matrix, including professional and academic graduate degree curricula and baccalaureate public health degree curricula. We do not currently offer concentrations or specializations in any of our degree programs.
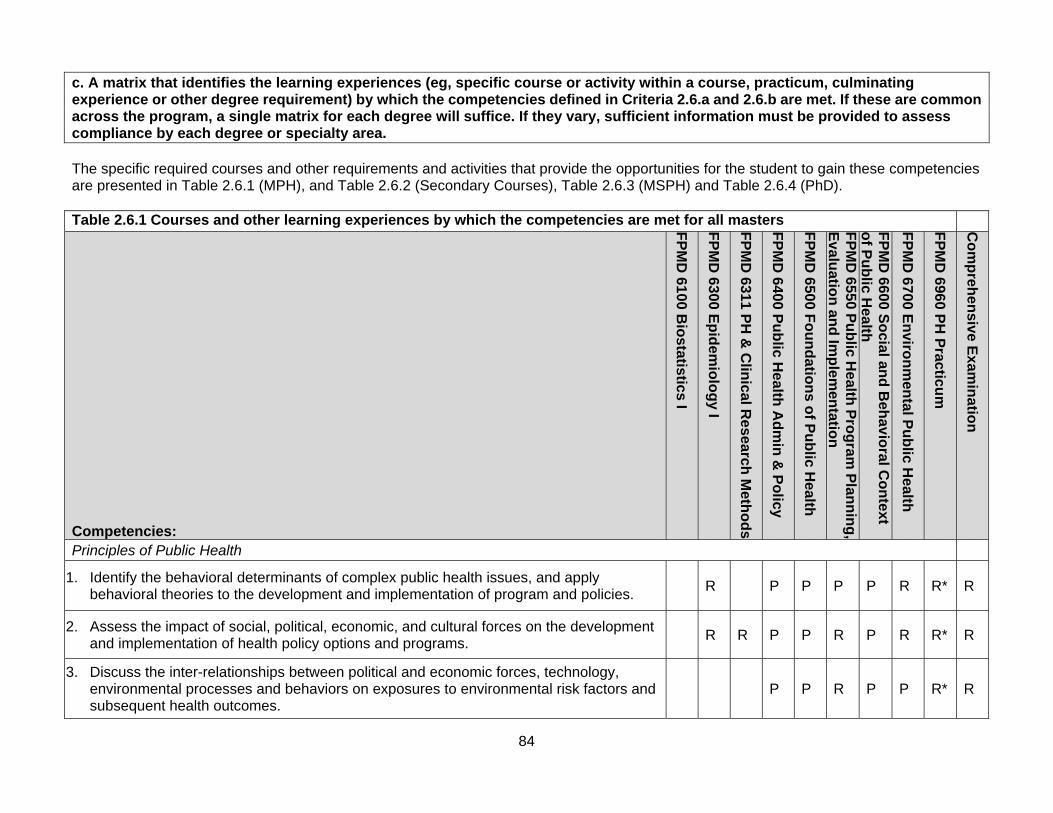
84
c. A matrix that identifies the learning experiences (eg, specific course or activity within a course, practicum, culminating experience or other degree requirement) by which the competencies defined in Criteria 2.6.a and 2.6.b are met. If these are common across the program, a single matrix for each degree will suffice. If they vary, sufficient information must be provided to assess compliance by each degree or specialty area. The specific required courses and other requirements and activities that provide the opportunities for the student to gain these competencies are presented in Table 2.6.1 (MPH), and Table 2.6.2 (Secondary Courses), Table 2.6.3 (MSPH) and Table 2.6.4 (PhD). Table 2.6.1 Courses and other learning experiences by which the competencies are met for all masters
Competencies:
FP
MD
6100 B
iostatistics I
FP
MD
6300 E
pid
emio
log
y I
FP
MD
6311 P
H &
Clin
ical Research
Meth
od
s
FP
MD
6400 P
ub
lic Health
Ad
min
& P
olicy
FP
MD
6500 F
ou
nd
ation
s of P
ub
lic Health
FP
MD
6550 Pu
blic H
ealth P
rog
ram P
lann
ing
,E
valuatio
n an
d Im
plem
entatio
n
FP
MD
6600 S
ocial an
d B
ehavio
ral Co
ntext
of P
ub
lic Health
FP
MD
6700 E
nviro
nm
ental P
ub
lic Health
FP
MD
6960 P
H P
racticu
m
Co
mp
rehen
sive Exam
inatio
n
Principles of Public Health
1. Identify the behavioral determinants of complex public health issues, and apply behavioral theories to the development and implementation of program and policies.
R
P P P P R R* R
2. Assess the impact of social, political, economic, and cultural forces on the development and implementation of health policy options and programs.
R R P P R P R R* R
3. Discuss the inter-relationships between political and economic forces, technology, environmental processes and behaviors on exposures to environmental risk factors and subsequent health outcomes.
P P R P P R* R

85
4. Evaluate the influence of behavioral, social, cultural, political, economic, environmental factors on the initiation and persistence of health disparities among sub-populations.
R R
R P R P R R* R
5. Describe the public health systems and structures at the local, region/state, national and international levels, and how their structure affects the development, delivery and quality of programs and policies.
R P P R R P R* R
Core Functions of Public Health: Assessment, Program Development and Assurance
6. Utilize descriptive and inferential statistical methods and epidemiologic principles to:
a. Critically evaluate and interpret scientific evidence from published studies P R R R P R R P R* R
b. Clearly articulate a public health issue and formulate relevant research questions. P P P P P P R R* R
c. Design appropriate/effective methods for collecting health and risk factor data for community needs assessments, surveillance, research, and program evaluation.
R P P R R P R R R* R
d. Measure and compare the health status of populations. P P R R R R P R* R
e. Evaluate public health interventions and R P R P R P R R R* R
f. provide a basis for making decisions and developing policy and recommendations. R R R P
R P R R* R
7. Based on existing data and information, develop goals, measurable objectives, programmatic activities, and expected outcomes for a public health program.
R P R P R
R* R
Professionalism, Leadership and Community Engagement
8. Use team building, negotiation, and conflict management skills to achieve organizational and community health goals.
R P R P R R R* R
9. Demonstrate effective written and oral skills for communicating with a wide range of audiences and in a variety of public health practice settings.
R R R P P P P P R* R
10. Apply social justice and human rights principles and use the basic concepts and skills regarding culturally appropriate community engagement and empowerment when addressing community needs.
R P
P P R R* R
11. Recognize the ethical principles that underlie the values of integrity, respect, transparency, accountability and equity in public health practice.
R P P P P R R* R
P=Primary, R=Reinforcing R* - Depending on practicum will depend on what competencies are reinforced.
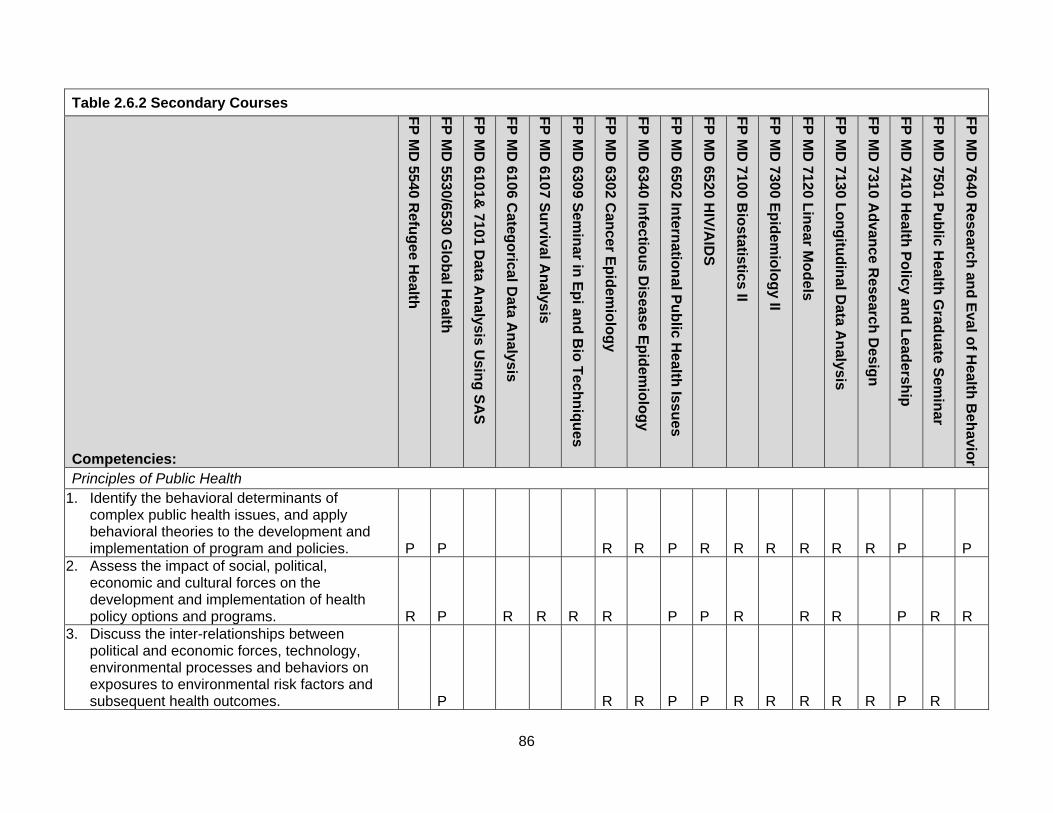
86
Table 2.6.2 Secondary Courses
Competencies:
FP
MD
5540 R
efug
ee Health
FP
MD
5530/6530 G
lob
al Health
FP
MD
6101&
7101 Data A
nalysis U
sing
SA
S
FP
MD
6106 C
atego
rical Data A
nalysis
FP
MD
6107 S
urvival A
nalysis
FP
MD
6309 S
emin
ar in E
pi an
d B
io T
echn
iqu
es
FP
MD
6302 C
ancer E
pid
emio
log
y
FP
MD
6340 In
fectiou
s Disease E
pid
emio
log
y
FP
MD
6502 In
ternatio
nal P
ub
lic Health
Issues
FP
MD
6520 H
IV/A
IDS
FP
MD
7100 B
iostatistics II
FP
MD
7300 E
pid
emio
log
y II
FP
MD
7120 L
inear M
od
els
FP
MD
7130 L
on
gitu
din
al Data A
nalysis
FP
MD
7310 A
dvan
ce Research
Desig
n
FP
MD
7410 H
ealth P
olicy an
d L
eadersh
ip
FP
MD
7501 P
ub
lic Health
Grad
ua
te Sem
inar
FP
MD
7640 R
esearch an
d E
val of H
ealth B
eh
avior
Principles of Public Health 1. Identify the behavioral determinants of
complex public health issues, and apply behavioral theories to the development and implementation of program and policies. P P R R P R R R R R R P P
2. Assess the impact of social, political, economic and cultural forces on the development and implementation of health policy options and programs. R P R R R R P P R R R P R R
3. Discuss the inter-relationships between political and economic forces, technology, environmental processes and behaviors on exposures to environmental risk factors and subsequent health outcomes. P R R P P R R R R R P R
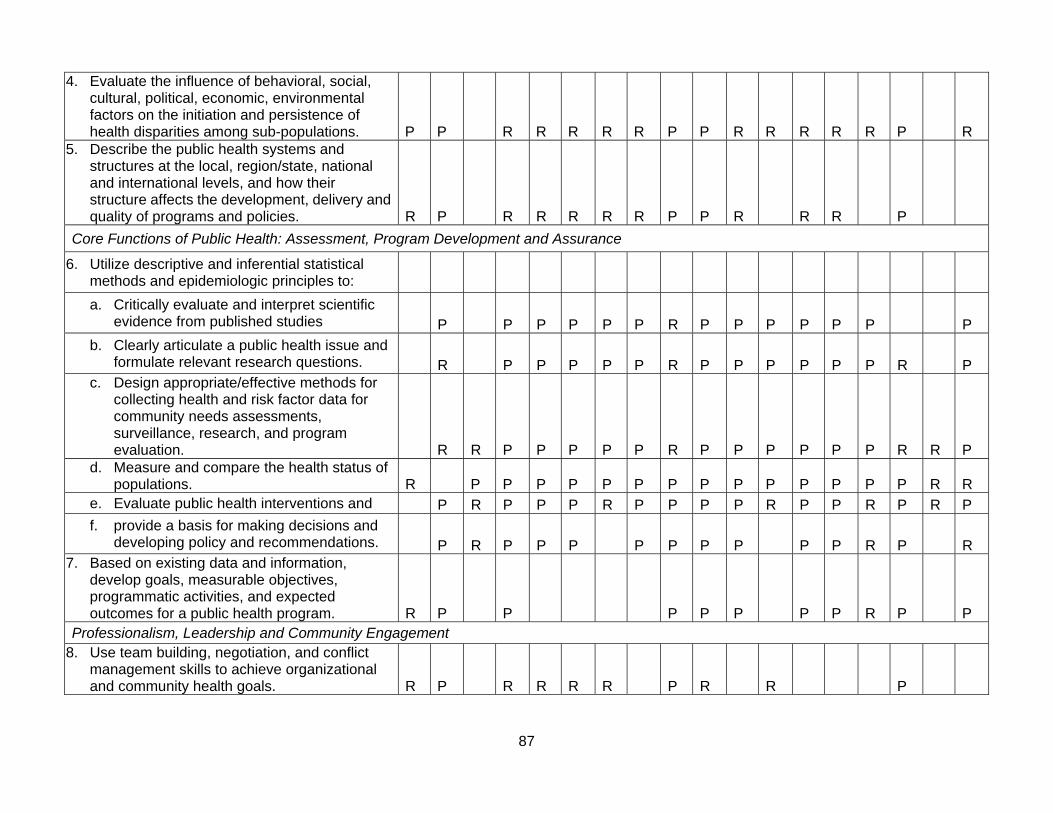
87
4. Evaluate the influence of behavioral, social, cultural, political, economic, environmental factors on the initiation and persistence of health disparities among sub-populations. P P R R R R R P P R R R R R P R
5. Describe the public health systems and structures at the local, region/state, national and international levels, and how their structure affects the development, delivery and quality of programs and policies. R P R R R R R P P R R R P
Core Functions of Public Health: Assessment, Program Development and Assurance
6. Utilize descriptive and inferential statistical methods and epidemiologic principles to:
a. Critically evaluate and interpret scientific evidence from published studies P P P P P P R P P P P P P P
b. Clearly articulate a public health issue and formulate relevant research questions. R P P P P P R P P P P P P R P
c. Design appropriate/effective methods for collecting health and risk factor data for community needs assessments, surveillance, research, and program evaluation. R R P P P P P R P P P P P P R R P
d. Measure and compare the health status of populations. R P P P P P P P P P P P P P P R R
e. Evaluate public health interventions and P R P P P R P P P P R P P R P R P
f. provide a basis for making decisions and developing policy and recommendations. P R P P P P P P P P P R P R
7. Based on existing data and information, develop goals, measurable objectives, programmatic activities, and expected outcomes for a public health program. R P P P P P P P R P P
Professionalism, Leadership and Community Engagement 8. Use team building, negotiation, and conflict
management skills to achieve organizational and community health goals. R P R R R R P R R P
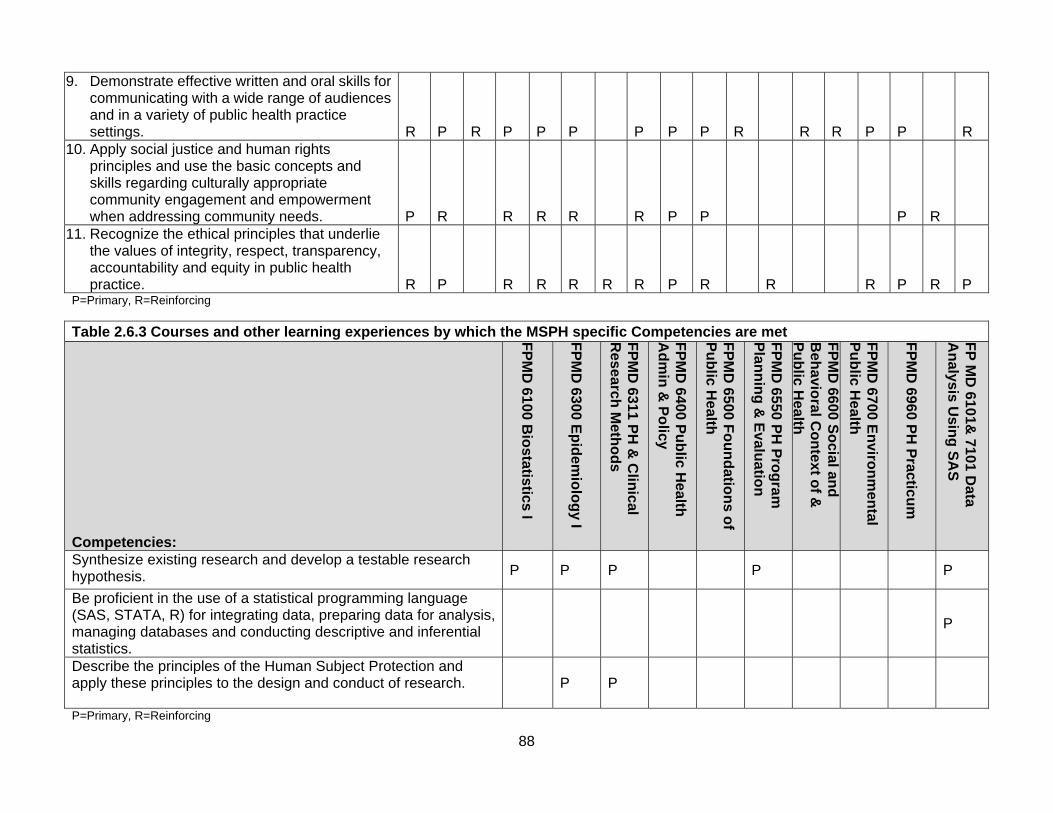
88
9. Demonstrate effective written and oral skills for communicating with a wide range of audiences and in a variety of public health practice settings. R P R P P P P P P R R R P P R
10. Apply social justice and human rights principles and use the basic concepts and skills regarding culturally appropriate community engagement and empowerment when addressing community needs. P R R R R R P P P R
11. Recognize the ethical principles that underlie the values of integrity, respect, transparency, accountability and equity in public health practice. R P R R R R R P R R R P R P
P=Primary, R=Reinforcing
Table 2.6.3 Courses and other learning experiences by which the MSPH specific Competencies are met
Competencies: F
PM
D 6100
Bio
statistics I
FP
MD
6300 E
pid
emio
log
y I
FP
MD
6311 P
H &
Clin
ical R
esearch M
etho
ds
FP
MD
6400 P
ub
lic Health
A
dm
in &
Po
licy
FP
MD
6500 F
ou
nd
ation
s of
Pu
blic H
ealth
FP
MD
6550 P
H P
rog
ram
P
lann
ing
& E
valuatio
n
FP
MD
6600 S
ocial an
d
Beh
avioral C
on
text of &
P
ub
lic Health
FP
MD
6700 E
nviro
nm
ental
Pu
blic H
ealth
FP
MD
6960 P
H P
racticu
m
FP
MD
6101&
7101 Data
An
alysis Usin
g S
AS
Synthesize existing research and develop a testable research hypothesis. P P P P P
Be proficient in the use of a statistical programming language (SAS, STATA, R) for integrating data, preparing data for analysis, managing databases and conducting descriptive and inferential statistics.
P
Describe the principles of the Human Subject Protection and apply these principles to the design and conduct of research.
P P
P=Primary, R=Reinforcing
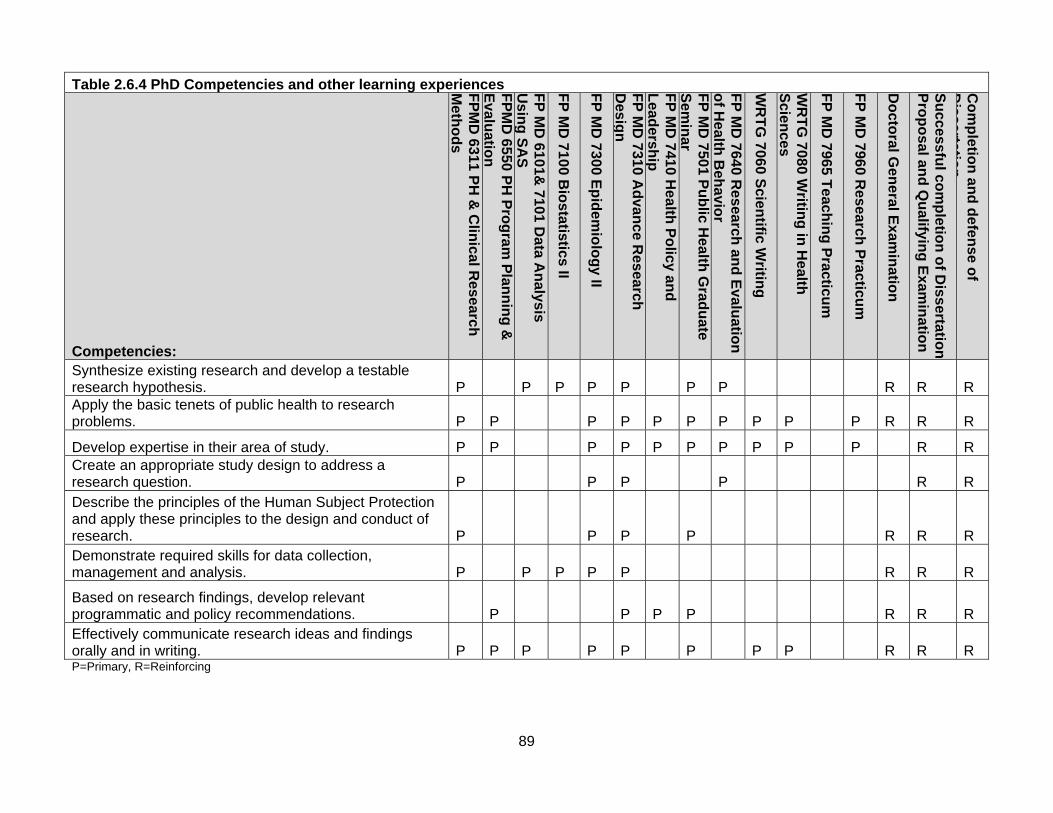
89
Table 2.6.4 PhD Competencies and other learning experiences
Competencies:
FP
MD
6311 P
H &
Clin
ical Research
M
etho
ds
FP
MD
6550 P
H P
rog
ram
Plan
nin
g &
E
valuatio
n
FP
MD
6101&
7101 Data A
nalysis
Usin
g S
AS
FP
MD
7100 B
iostatistics II
FP
MD
7300 E
pid
emio
log
y II
FP
MD
7310 A
dvan
ce Research
D
esign
FP
MD
7410 H
ealth P
olicy an
d
Lead
ership
FP
MD
7501 P
ub
lic Health
Grad
ua
te S
emin
ar
FP
MD
7640 R
esearch an
d E
valuatio
n
of H
ealth B
ehavio
r
WR
TG
7060 S
cientific W
riting
WR
TG
7080 W
riting
in H
ealth
Scien
ces
FP
MD
7965 T
eachin
g P
racticum
FP
MD
7960 R
esearch P
racticum
Do
ctoral G
eneral E
xamin
ation
Su
ccessful co
mp
letion
of D
issertation
P
rop
osal an
d Q
ualifyin
g E
xamin
ation
Co
mp
letion
and
defen
se of
Dissertatio
n
Synthesize existing research and develop a testable research hypothesis. P P P P P P P R R R Apply the basic tenets of public health to research problems. P P P P P P P P P P R R R
Develop expertise in their area of study. P P P P P P P P P P R R Create an appropriate study design to address a research question. P P P P R R Describe the principles of the Human Subject Protection and apply these principles to the design and conduct of research. P P P P R R R Demonstrate required skills for data collection, management and analysis. P P P P P R R R
Based on research findings, develop relevant programmatic and policy recommendations. P P P P R R R Effectively communicate research ideas and findings orally and in writing. P P P P P P P P R R R P=Primary, R=Reinforcing
90
d. Analysis of the completed matrix included in Criterion 2.6.c. If changes have been made in the curricula as a result of the observations and analysis, such changes should be described. We have used the data in Tables 2.6.1, to 2.6.4 to assess the degree to which our curriculum covers the program competencies. We reviewed our prior competency set in the 2010 Division faculty retreat and discussed areas where a competency was covered only partially. This lead to some changes in the material or depth of coverage of topics in specific courses, notably the Foundations of Public Health and Clinical Research Methods courses. e. Description of the manner in which competencies are developed, used and made available to students. In 2010 the Division adopted the ASPH competencies associated with the five core areas for all MPH, MSPH and PhD students. Additional competencies that focused on the conduct of research were developed for the PhD program. These competency sets were developed through a consensus process with the faculty. Existing competency sets from ASPH, the Council on Linkages, and other public health educational programs were compiled and reviewed by an ad hoc committee. They were presented to the full faculty for discussion at a series of faculty meetings. The faculty felt that the ASPH core competencies for the core areas were unambiguous and the most appropriate. An initial set of additional competencies for the PhD degree were drafted by the ad hoc committee. These were presented to the full faculty and extensively revised. Both competency sets were formally adopted by the faculty at the 2010 Faculty Retreat. We initiated a process of reviewing and revising our Core Competencies in March 2012, as a result of input during our CEPH consultation visit. The Core Competencies adopted in 2010 consisted of 48 competencies from the ASPPH core competencies for the five core areas of public health. While most of these competencies were very specific, it was difficult to adequately assess the competence of our students with such a long list. In addition, some of the competencies seemed much less important than others. The new competencies reflect a broader description organized into three areas: A) Principles of Public Health; B) Core Functions of Public Health: Assessment, Program Development and Assurance; and C) Professionalism, Leadership and Community Engagement. The competencies are first presented to the students in the Foundation of Public Health course, which is typically taken during the students’ first semester. Relevant competencies are listed on each course syllabus, and will be eventually be the updated website under Related Links. f. Description of the manner in which the program periodically assesses changing practice or research needs and uses this information to establish the competencies for its educational programs. There are several mechanisms whereby we obtain feedback regarding how well our graduates are prepared for the workforce. In our annual survey of graduates (Appendix 2.6A) we ask whether each graduate feels that they were adequately prepared for their position and in what ways they feel they could have been better prepared. We solicit input from key leaders at the state and local health departments through an informal gathering on how well our graduates are prepared and what new skills or knowledge they think we need to incorporate. Finally, through our work in the Office of Public Health Practice and our participation in the Utah-Nevada Public Health Workforce Alliance, we address workforce needs including workforce preparation and workforce development. This input is directed to the Curriculum committee, who periodically leads a discussion in faculty meetings. The faculty use this input to modify their course content, and the faculty use this input during our annual review of goals, objectives, and competencies.
91
g. Assessment of the extent to which this criterion is met and an analysis of the program’s strengths, weaknesses and plans relating to this criterion. This criterion is met with commentary.
Strengths: We have critically reviewed our competencies based on guidance received during the self-study process, and, as a result, have re-formulated them into a more succinct and targeted set. This was carried out through a collaborative process with direct input from the faculty. Feedback from employers and other stakeholders from criteria 2.7.e was also used as we formulated the new competencies.
Weaknesses: The recently developed set of competences was designed to reflect a more detailed set that have used over the past few years. However, due to this being a substantial change in our competencies, we have not yet been able to fully assess how well these operationalize across our educational programs. We also feel that it is important to be more systematic in our review of competencies, with a target of annual review by faculty, student representatives, community advisors and other stakeholders.
Plans: We will formally review competencies in conjunction with our annual retreat to insure that they continue to reflect the focus of our degree programs and are effectively operationalized. We will also be more effective in tracking competencies across the curriculum to ensure that they are guiding our educational efforts. Finally, we are more formally incorporating the competencies in our comprehensive examination process, which is now practical with the manageable number in our newly developed set.
92
2.7 Assessment Procedures. There shall be procedures for assessing and documenting the extent to which each student has demonstrated achievement of the competencies defined for his or her degree program and area of concentration. a. Description of the procedures used for monitoring and evaluating student progress in achieving the expected competencies, including procedures for identifying competency attainment in practice and culminating experiences. Student progress in achieving the expected competencies is monitored and evaluated by:
• Grades in classes. The Academic Advisor is informed when students do not get an adequate grade for the course to count toward their degree.
• Online tracking. Tracking of progress in required coursework, practicum, and comprehensive exam online. If students have not met policy requirements, a letter is sent to them.
• Faculty advisors. They are informed about students not doing well in class. Faculty advisors must also approve the students completed coursework, practicum and comprehensive exams online. Faculty advisors meet with students individually to discuss coursework or any difficulties the students encounter in the degree programs.
• Faculty meetings. Biannually, the faculty reviews the list of PhD students. The faculty chair of the PhD committee reports on the progress of the PhD student and brings up any issues the student may be having on completing their PhD.
• Coursework. When our competencies were developed in 2010, we asked each professor to identify which competencies were addressed in each course. This allowed us to identify gaps in our overall curriculum. We worked to identify the class(es) where additional material and activities should be added to cover competencies that were not adequately covered. As we revised our competencies, we noticed that in some cases the material in the course implies areas of competence that we felt were important and that should be covered in our new competencies. An example is competence in research design, data collection and data analysis. After our new competencies were finalized, each professor once again reviewed their courses to identify which competencies were primarily addressed or reinforced. This was then reviewed by the curriculum committee to ensure that all competencies were covered by the required curriculum.
• Assessment of culminating experience. The comprehensive exam, general exam, and qualifying exams are administered to assess integration of knowledge and skills (please see details in section 2.5)
• Practicum. Students final practicum reports include a section evaluating the project utilizing public health core competencies
• The number of students graduating each year. The number of students graduating from the masters and PhD programs are assessed by the Academic Advisor each year.
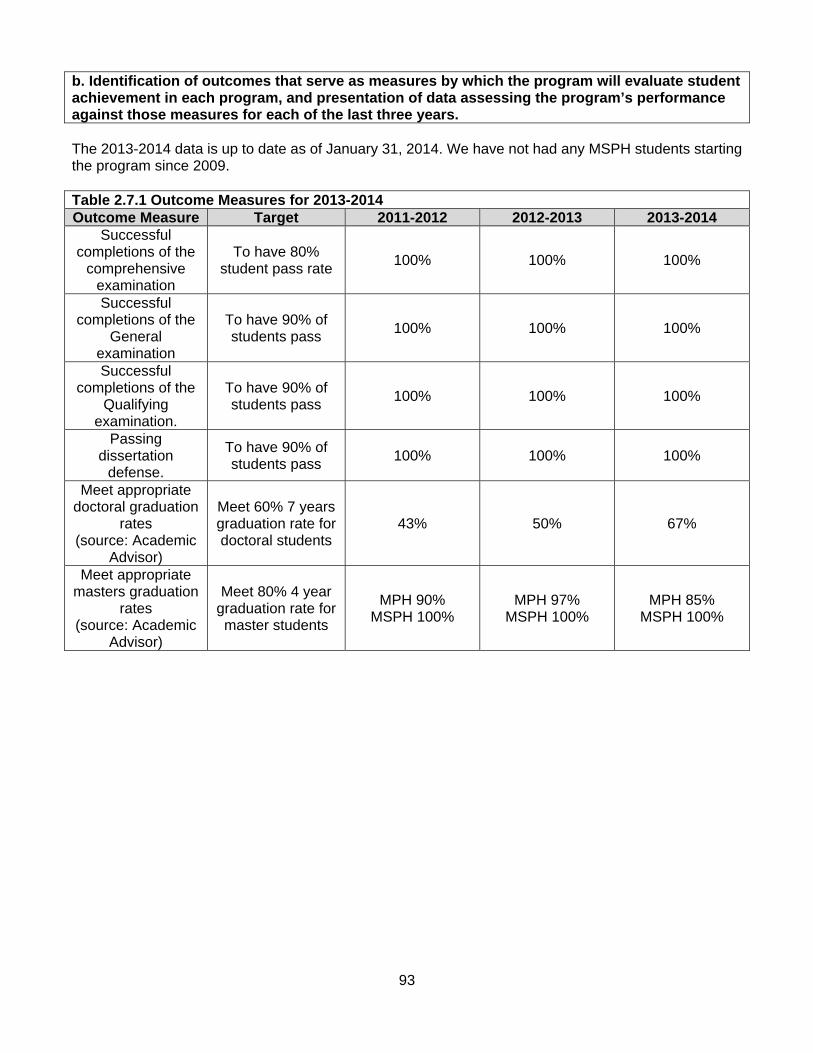
93
b. Identification of outcomes that serve as measures by which the program will evaluate student achievement in each program, and presentation of data assessing the program’s performance against those measures for each of the last three years. The 2013-2014 data is up to date as of January 31, 2014. We have not had any MSPH students starting the program since 2009. Table 2.7.1 Outcome Measures for 2013-2014 Outcome Measure Target 2011-2012 2012-2013 2013-2014
Successful completions of the
comprehensive examination
To have 80% student pass rate
100% 100% 100%
Successful completions of the
General examination
To have 90% of students pass
100% 100% 100%
Successful completions of the
Qualifying examination.
To have 90% of students pass
100% 100% 100%
Passing dissertation
defense.
To have 90% of students pass
100% 100% 100%
Meet appropriate doctoral graduation
rates (source: Academic
Advisor)
Meet 60% 7 years graduation rate for doctoral students
43% 50% 67%
Meet appropriate masters graduation
rates (source: Academic
Advisor)
Meet 80% 4 year graduation rate for master students
MPH 90% MSPH 100%
MPH 97% MSPH 100%
MPH 85% MSPH 100%
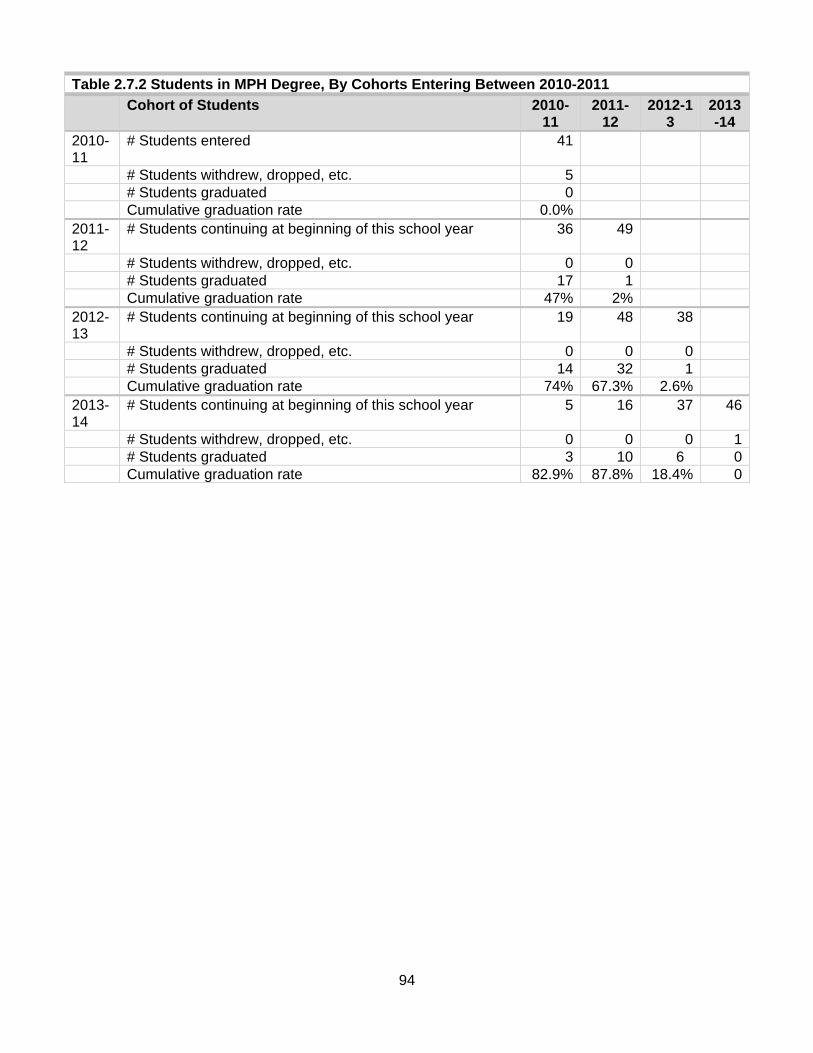
94
Table 2.7.2 Students in MPH Degree, By Cohorts Entering Between 2010-2011
Cohort of Students 2010-11
2011-12
2012-13
2013-14
2010-11
# Students entered 41
# Students withdrew, dropped, etc. 5 # Students graduated 0 Cumulative graduation rate 0.0% 2011-12
# Students continuing at beginning of this school year 36 49
# Students withdrew, dropped, etc. 0 0 # Students graduated 17 1 Cumulative graduation rate 47% 2% 2012-13
# Students continuing at beginning of this school year 19 48 38
# Students withdrew, dropped, etc. 0 0 0 # Students graduated 14 32 1 Cumulative graduation rate 74% 67.3% 2.6%2013-14
# Students continuing at beginning of this school year 5 16 37 46
# Students withdrew, dropped, etc. 0 0 0 1 # Students graduated 3 10 6 0 Cumulative graduation rate 82.9% 87.8% 18.4% 0

95
Table 2.7.3 Students in PhD Degree, By Cohorts Entering Between 2007-2008 and 2013-2014
Cohort of Students 2007-08
2008-09
2009-10
2010-11
2011-12
2012-13
2013-14
2007-08 # Students entered 11 # Students withdrew, dropped,
etc. 4
# Students graduated 0 Cumulative graduation rate 0.0% 2008-09 # Students continuing at
beginning of this school year 7 4
# Students withdrew, dropped, etc.
0 1
# Students graduated 0 0 Cumulative graduation rate 0.0% 0.0% 2009-10 # Students continuing at
beginning of this school year 7 3 2
# Students withdrew, dropped, etc.
0 0 1
# Students graduated 0 0 0 Cumulative graduation rate 0.0% 0.0% 0.0% 2010-11 # Students continuing at
beginning of this school year 7 3 1 6
# Students withdrew, dropped, etc.
0 0 0 0
# Students graduated 0 0 0 0 Cumulative graduation rate 0.0% 0.0% 0.0% 0.0% 2011-12 # Students continuing at
beginning of this school year 7 3 1 6 8
# Students withdrew, dropped, etc.
0 0 0 0 0
# Students graduated 4 0 0 0 0 Cumulative graduation rate 36.4% 0.0% 0.0% 0.0% 0.0% 2012-13 # Students continuing at
beginning of this school year 3 3 1 6 8 6
# Students withdrew, dropped, etc.
0 0 0 0 0 0
# Students graduated 1 0 0 1 0 0 Cumulative graduation rate 45.5% 0.0% 0.0% 0.0% 0.0% 0.0%2013-14 # Students continuing at
beginning of this school year 2 3 1 5 8 6 4
# Students withdrew, dropped, etc.
0 0 1 0 0 0 0
# Students graduated 0 3* 0 2* 0 0 0 Cumulative graduation rate 45.5% 75% 0.0% 0.0% 0.0% 0.0% 0.0%*Number of students planning to graduate May 2014

96
c. An explanation of the methods used to collect job placement data and of graduates’ response rates to these data collection efforts. The program must list the number of graduates from each degree program and the number of respondents to the graduate survey or other means of collecting employment data. The Academic Advisor sends out an Alumni survey after graduation (Appendix 2.6A). The Alumni Survey was created through Mission Base Management E-survey. The survey link has been sent out by the Academic Advisor to the Graduates for the past three years. Students are given two-three weeks to complete the survey. The Alumni Survey response rate is about 25%. When the survey closes the Academic Advisor pulls the reports to present to the Division Chief and Faculty members (Appendix 2.7A).
Table 2.7.4 Destination of MPH Graduates by Employment Type
2011-2012 2012-2013 Fall 2013*
Employed 18 29 6 Continuing education/training (not employed) 8 9 0 Actively seeking employment 3 5 1 Not seeking employment (not employed and not continuing education/training, by choice)
1 1 1
Unknown 2 4 0 Total 32 48 8
*As of fall 2013 graduation
Table 2.7.5 Destination of MSPH Graduates by Employment Type
2011-2012 2012-2013 2013-2014
Employed 1 0 0 Continuing education/training (not employed) 3 0 0 Actively seeking employment 0 0 0 Not seeking employment (not employed and not continuing education/training, by choice)
0 0 0
Unknown 0 0 0 Total 4 0 0
*We have not had any new MSPH students start the MSPH program since 2009.
Table 2.7.6 Destination of PhD Graduates by Employment Type
2011-2012 2012-2013 2013-2014 projected
Employed 7 1 5 Continuing education/training (not employed) 0 0 0 Actively seeking employment 1 0 0 Not seeking employment (not employed and not continuing education/training, by choice)
0 0 0
Unknown 0 0 0 Total 8 1 5
*Based on number of students planning to graduate May 2014 d. In fields for which there is certification of professional competence and data are available from the certifying agency, data on the performance of the program’s graduates on these national examinations for each of the last three years. Not applicable
97
e. Data and analysis regarding the ability of the program’s graduates to perform competencies in an employment setting, including information from periodic assessments of alumni, employers and other relevant stakeholders. Methods for such assessment may include key informant interviews, surveys, focus groups and documented discussions. The ability of the program’s graduates to perform competencies in an employment setting are collected by:
Employer survey / focus groups. We have often conducted informal surveys of our community leaders. This year we have begun holding formal focus groups with employers of our graduates (Appendix 1.2B). Their feedback has been essential in getting this critical perspective on our educational offerings. We have now scheduled these focus groups as a semi-annual activity. We will also be using this feedback to increase our systematic assessment of employers. Alumni Survey. We send out an alumni survey about seven months after graduation. The Alumni surveys are sent out through the Universities E-survey tool (Appendix 2.6A). From this survey we have received important feedback around important aspects of our educational programming, such as the need for more formal career advising. In response to this, we have now expanded the scope of our academic advising to include more formal career advising.
f. Assessment of the extent to which this criterion is met and an analysis of the program’s strengths, weaknesses and plans relating to this criterion.
The criterion is met with commentary. Strengths: We assess the extent to which each student has mastered the necessary skills, concepts, content and competencies attained through their educational experience. The procedures for measuring the attainment of competencies include intra-course assessment, practicum evaluation and the comprehensive exam. Feedback from employers and recent graduates complements these efforts to get a market perspective on the appropriate preparation of our graduates. We continue to look for ways to access input to guide educational programming for maximizing the success of our graduates for both market competitiveness and capacity for impact.
Weaknesses: Specific feedback from current students and graduates specific to our newly revised core competencies will help to improve our assessment of student attainment of competencies. This, combined with our improved efforts to create complementary feedback mechanisms to the assessments that are part of the standard educational activities, such as our newly developed employer focus group strategy, will help to increase our performance relative to this criterion.
Plans: Based on our revised competencies, we will work on connecting with current students and recent graduates to determine both the relevance of our competency list and our performance in preparing students. We are also working on more systematic feedback from employers and potential employers regarding the competency mastery.
98
2.8 Bachelor’s Degrees in Public Health. If the program offers baccalaureate public health degrees, they shall include the following elements.
This is not applicable.

99
2.9 Academic Degrees. If the program also offers curricula for graduate academic degrees, students pursuing them shall obtain a broad introduction to public health, as well as an understanding about how their discipline-based specialization contributes to achieving the goals of public health. a. Identification of all academic degree programs, by degree and area of specialization. The instructional matrix in Criterion 2.1.a may be referenced for this purpose. The two Academic degrees offered by the Division are the Master of Science of Public Health (MSPH), and the PhD in Public Health as shown in Criterion 2.1. The MSPH degree offered by the Division requires completion of 55 credit hours, which includes 24 core requirements, 15 elective, 10 hours of thesis/project of publishable quality and a 6 credit hour practicum and a comprehensive examination, not taken for credit. A breakdown of the specific classes required for the MSPH can be found in the Appendix 2.9A. The PhD degree offered by the Division requires completion of 74 credit hours, which include 29 core requirements, 25 electives, 3 credits for a research practicum, 3 credits for a teaching practicum and 14 credits of dissertations as well as the general examination and oral examination, not take for any credit. b. Identification of the means by which the program assures that students in academic curricula acquire a public health orientation. If this means is common across the program, it need be described only once. If it varies by degree or specialty area, sufficient information must be provided to assess compliance by each. MSPH students must successfully complete the same five courses required of MPH students. In addition, student research projects must integrate knowledge from the core areas of public health. Our policy indicates how this process works and that it is designed to insure that research conducted maintains a public health orientation. Through this process, we have been able to refocus students who have proposed projects that do not have this orientation.
Masters Practicum: All MSPH students must complete 6 credit hours (270 hours fieldwork) of practicum prior to graduation. The practicum experience is meant to give students direct, hands-on experience, which will tie into their research project. This will not only supplement the student’s coursework and enrich their academic experience, but also prepare the student with a start to their paper of publishable quality or thesis completion of their degree
Goal 1. To integrate foundational public health knowledge with a concrete experience of public health
practice. In particular, to observe and report how the following concepts play out in real public health practice:
o the core functions of public health, o the core organizational practices necessary for governmental agencies to carry out the
mission of public health, and o the essential public health services, from a community-based perspective.
2. To identify and report the issues in cultural competence relevant to a specific practicum site and how they play out in real public health practice.
3. To identify growth edges in public health practice. 4. To broaden knowledge and skills in public health practice. 5. To gain experience working with a mentor that has the academic credentials and experience to
oversee and evaluate masters level student goals and activities.
100
Master students are not eligible to start their practicum until they have competed and passed with B- or above without at least year one courses completed as prerequisites: FP MD 6100 Biostatistics I, FP MD 6300 Epidemiology I, FP MD 6400 Public Health Policy & Administration, FP MD 6500 Foundations of Public Health, FP MD 6600 Social & Behavioral Context of Public Health, and FP MD 6700 Environmental Public Health. Doctoral Research practicum http://medicine.utah.edu/dfpm/divisionph/current/PhD/ResearchPracticum.htm: All PhD students must complete 3 credit hours (135 hours fieldwork) of practicum prior to graduation. The practicum experience is meant to give students direct, hands-on research experience comparable to a career position suitable for someone with a PhD in Public Health. This will not only supplement the student’s coursework and enrich their academic experience, but also prepare the student for employment after completion of their degree. Goal The purpose of the PhD Research Practicum is two-fold.
1. To have the student form a working relationship with a member of the full time Public Health Program faculty who will serve as the chair of his/her dissertation committee
2. To identify, with the assistance of the same faculty member, a suitable topic about which to conduct his/her PhD dissertation project.
Evaluation By the end of this practicum the student should have identified a suitable topic for his/her PhD dissertation and have prepared a detailed proposal which can be submitted to the Public Health Program faculty for their approval as a dissertation topic.
Doctoral Teaching Practicum http://medicine.utah.edu/dfpm/divisionph/current/PhD/TeachingPracticum.htm: All PhD students must complete 3 credit hours (135 hours fieldwork) of practicum prior to graduation. The practicum experience is meant to give students direct, hands-on teaching experience comparable to a career position suitable for someone with a PhD in Public Health. This will not only supplement the student’s coursework and enrich their academic experience, but also prepare the student for employment after completion of their degree. Goal The goal of this practicum is to give the student experience in teaching within the Public Health Program. The student must work with the one of the full time faculty members of the Public Health Program. The practicum must include the presentation of lectures on part or the entire curriculum for a particular course. It should include the development of laboratory exercises, or other learning materials; the development, administration and grading of tests; the development and presentation of lectures for one or more parts of a course. c. Identification of the culminating experience required for each academic degree program. If this is common across the program’s academic degree programs, it need be described only once. If it varies by degree or specialty area, sufficient information must be provided to assess compliance by each. Comprehensive Exam (Master Students) The comprehensive exam for masters students was described in detail in section 2.5.
General Examination (Doctoral students) The examination is administered and graded by the core public health faculty. Students will not be allowed to take the Qualifying Examination (dissertation proposal defense) until the General Examination is successfully taken.
101
Objectives: The objective of the General Exam is to provide an opportunity for the faculty and the student, to assess the student’s knowledge and ability to conduct research, by having them consider a research question, analyze data, prepare a short manuscript for submission, and give a scientific presentation. Eligibility: A student will be eligible to take the General Exam after they have completed, with a B- or better, the following courses and their pre-requisites: Epidemiology II, Biostatistics II, Data Analysis Using SAS, Research and Evaluation of Health Behavior, Public Health and Clinical Research Methods, Scientific Communication or equivalent, and Advanced Research Design. Exam structure: The exam will consist of four parts: a short guided literature review on a topic new to the student, an analysis of a data set to answer specific research questions, preparation of a short manuscript based on this analysis, and a short presentation to a faculty committee. The students are given approximately 3 weeks to complete the draft the manuscript.
1. Literature review: Students are provided an orientation of the general topic area to be covered. Preparation guidelines for the entire manuscript (i.e. “guidelines for authors”) are provided, including word limits, and the maximum number of tables, figures, and references.
2. Data analysis: Students are provided a data set with full documentation (data dictionary), and a set of research questions/hypotheses. The dataset will be clean but will require processing (e.g. to create appropriate missing values, composite variables, re-coded variables). Each student will be expected to independently conduct an analysis of this data, both descriptive and analytical. This will include submission of analysis programs, output, tables and figures, with a brief interpretation of each result.
3. Manuscript preparation: Students will use their literature review and results to prepare a short manuscript, similar to a manuscript for submission to a peer-reviewed journal.
4. Oral Presentation. After they submit their manuscript, students will give a short (10-15 min) presentation of their results to a committee and answer questions. This presentation will be expected to be of the type and quality for an oral presentation at a national conference.
Students will be given comments at the presentation and a summary of the comments in writing. Students must address comments by writing a response to each comment and making corresponding changes in the manuscript draft, similar to addressing reviewer comments after manuscript submission to a scientific journal. All work completed by the students will be assessed by a committee and given a grade (pass with honors, pass, conditional pass, fail). Any student given a ‘conditional pass’ will be assigned additional work. Students who fail the exam must re-take the exam before proceeding. Expected Timeline: The exam is offered at the end of Fall and Spring semesters. Qualifying Examination (PhD students) The qualifying examination is taken after the 5-page concept proposal has been presented to the faculty, the full dissertation proposal has been presented to the supervisory committee and before dissertation research has begun. To be eligible to take the qualifying examination, a student should have petitioned the Graduate School to establish their supervisory committee at least four months prior to the examination and be registered for at least 3 credits in the semester in which the qualifying examination is taken. In addition, the student must have completed all the core course requirements. The qualifying examination, administered by the doctoral supervisory committee, deals with the topic of the student’s dissertation. It is designed to:
1. Measure the student’s ability to analyze and synthesize information.

102
2. Determine whether the student has sufficient breadth of knowledge of the topic of his/her dissertation, including a clear understanding of the background of the topic under study; and
3. Evaluate whether the student has adequate knowledge of recent advances and important public health issues, as well as other disciplines (e.g., biostatistics, health economics, etc.) relevant to the student’s research project.
The qualifying examination consists of two parts--written and oral. Written: The written examination is the first step of the qualifying examination, consisting of 1 or 2 questions from each committee member, tailored to the student’s individual dissertation proposal, with 1-2 weeks allowed to complete the written part. However, committees are free to depart from that model, if appropriate. A student who performs poorly on the written portion of the qualifying examination may be re-examined at the discretion of the committee before the oral portion is taken. The committee members may require additional course work to remedy perceived deficiencies in any relevant area. Oral: The oral portion of the qualifying examination includes a defense of the written examination, and is scheduled as soon as possible after the written examination is submitted. The oral examination should be taken a minimum of four months after the official date the committee is formed. A student must be registered for at least 3 credits during the semester they take the oral examination. At least four members of the committee must be present, including the chair. If the chair is not present, the examination must be rescheduled for a later date. Results of the Qualifying Examination After the qualifying examination, the supervisory committee indicates on the Report of the Qualifying Examination for the Ph.D., Ed.D., or M.Phil. Degree and Recommendation for Admission to Candidacy form whether the student passed or failed. All supervisory committee members who are present at the examination should sign the form. Students should make a copy of the signed form in case the original is lost. The student should make sure that the signed form reaches the Academic Advisor no later than the last day of the semester, at least two months proceeding the semester of graduation. If the student passes, they are formally appointed as candidates for doctoral degree, and the student can then begin research for their dissertation. If the student fails, they have one more chance to pass. In case of failure, the supervisory committee will make appropriate recommendations for further courses, reading or research to address the deficiencies. Students may not defend their dissertation in the same semester as the qualifying examination. d. Assessment of the extent to which this criterion is met and an analysis of the program’s strengths, weaknesses, and plans relating to this criterion. This criterion is met with commentary. Strengths: Our current academic degree offerings provide a strong foundation in the core disciplines of public health combined with meaningful academic-specific elements for demonstrating mastery of the science of public health (for the MSPH) or expanding the science of public health (for the PhD in Public Health). Weaknesses: Alignment between the MSPH and PhD, including more reasonable requirements for the MSPH, will help improve the academic graduate experience. Plans: We are currently working on a strategy for improving degree alignment (along both academic and professional lines) as well as the creation of emphases. With the continuing expansion of faculty resources, we are beginning the initial strategizing for this transition in anticipation that we will be in a position to meet the accreditation criteria for making these changes. Plans to align the MSPH and PhD to a more researched orientated degree will take place during the 2014-2015 academic year.
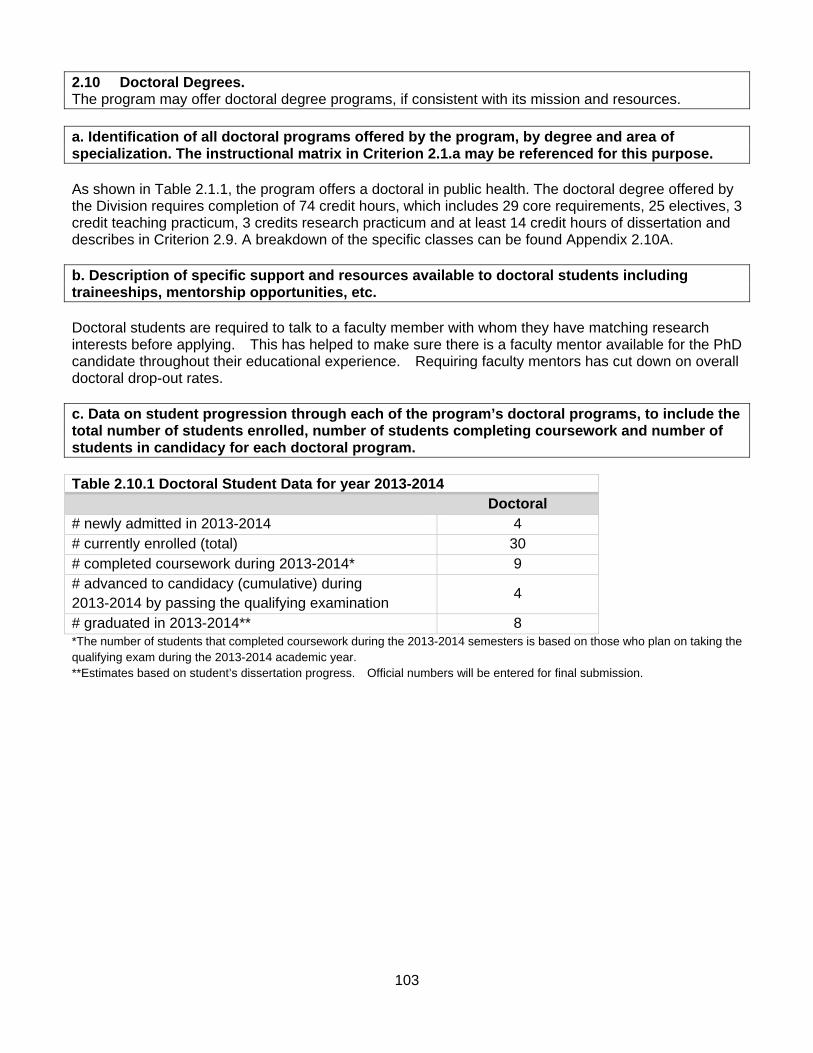
103
2.10 Doctoral Degrees. The program may offer doctoral degree programs, if consistent with its mission and resources. a. Identification of all doctoral programs offered by the program, by degree and area of specialization. The instructional matrix in Criterion 2.1.a may be referenced for this purpose. As shown in Table 2.1.1, the program offers a doctoral in public health. The doctoral degree offered by the Division requires completion of 74 credit hours, which includes 29 core requirements, 25 electives, 3 credit teaching practicum, 3 credits research practicum and at least 14 credit hours of dissertation and describes in Criterion 2.9. A breakdown of the specific classes can be found Appendix 2.10A. b. Description of specific support and resources available to doctoral students including traineeships, mentorship opportunities, etc. Doctoral students are required to talk to a faculty member with whom they have matching research interests before applying. This has helped to make sure there is a faculty mentor available for the PhD candidate throughout their educational experience. Requiring faculty mentors has cut down on overall doctoral drop-out rates. c. Data on student progression through each of the program’s doctoral programs, to include the total number of students enrolled, number of students completing coursework and number of students in candidacy for each doctoral program. Table 2.10.1 Doctoral Student Data for year 2013-2014 Doctoral # newly admitted in 2013-2014 4 # currently enrolled (total) 30 # completed coursework during 2013-2014* 9 # advanced to candidacy (cumulative) during 2013-2014 by passing the qualifying examination
4
# graduated in 2013-2014** 8 *The number of students that completed coursework during the 2013-2014 semesters is based on those who plan on taking the qualifying exam during the 2013-2014 academic year. **Estimates based on student’s dissertation progress. Official numbers will be entered for final submission.
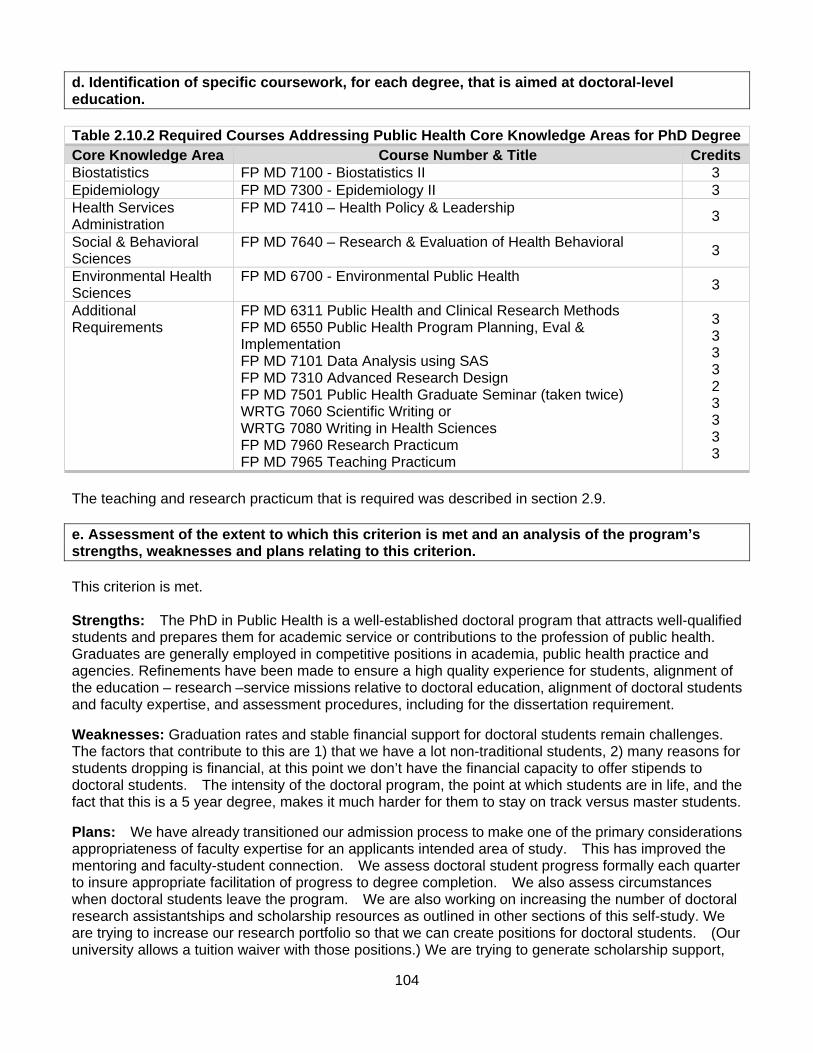
104
d. Identification of specific coursework, for each degree, that is aimed at doctoral-level education. Table 2.10.2 Required Courses Addressing Public Health Core Knowledge Areas for PhD Degree Core Knowledge Area Course Number & Title CreditsBiostatistics FP MD 7100 - Biostatistics II 3 Epidemiology FP MD 7300 - Epidemiology II 3 Health Services Administration
FP MD 7410 – Health Policy & Leadership 3
Social & Behavioral Sciences
FP MD 7640 – Research & Evaluation of Health Behavioral 3
Environmental Health Sciences
FP MD 6700 - Environmental Public Health 3
Additional Requirements
FP MD 6311 Public Health and Clinical Research Methods FP MD 6550 Public Health Program Planning, Eval & Implementation FP MD 7101 Data Analysis using SAS FP MD 7310 Advanced Research Design FP MD 7501 Public Health Graduate Seminar (taken twice) WRTG 7060 Scientific Writing or WRTG 7080 Writing in Health Sciences FP MD 7960 Research Practicum FP MD 7965 Teaching Practicum
3 3 3 3 2 3 3 3 3
The teaching and research practicum that is required was described in section 2.9. e. Assessment of the extent to which this criterion is met and an analysis of the program’s strengths, weaknesses and plans relating to this criterion. This criterion is met. Strengths: The PhD in Public Health is a well-established doctoral program that attracts well-qualified students and prepares them for academic service or contributions to the profession of public health. Graduates are generally employed in competitive positions in academia, public health practice and agencies. Refinements have been made to ensure a high quality experience for students, alignment of the education – research –service missions relative to doctoral education, alignment of doctoral students and faculty expertise, and assessment procedures, including for the dissertation requirement.
Weaknesses: Graduation rates and stable financial support for doctoral students remain challenges. The factors that contribute to this are 1) that we have a lot non-traditional students, 2) many reasons for students dropping is financial, at this point we don’t have the financial capacity to offer stipends to doctoral students. The intensity of the doctoral program, the point at which students are in life, and the fact that this is a 5 year degree, makes it much harder for them to stay on track versus master students.
Plans: We have already transitioned our admission process to make one of the primary considerations appropriateness of faculty expertise for an applicants intended area of study. This has improved the mentoring and faculty-student connection. We assess doctoral student progress formally each quarter to insure appropriate facilitation of progress to degree completion. We also assess circumstances when doctoral students leave the program. We are also working on increasing the number of doctoral research assistantships and scholarship resources as outlined in other sections of this self-study. We are trying to increase our research portfolio so that we can create positions for doctoral students. (Our university allows a tuition waiver with those positions.) We are trying to generate scholarship support,

105
yet that remains limited. As an example our Alumni Scholarship was designed to be big enough to have some impact but we are not currently able to support these students in a substantial way that would make it easier for them to go to school. We also continue to lobby for better financial support, which would allow for funded doctoral students.

106
2.11 Joint Degrees. If the program offers joint degree programs, the required curriculum for the professional public health degree shall be equivalent to that required for a separate public health degree.
a. Identification of joint degree programs offered by the program. The instructional matrix in Criterion 2.1.a may be referenced for this purpose. The program offers six joint degrees as shown in Table 2.1.1 in section 2.1. b. A list and description of how each joint degree program differs from the standard degree program. The program must explain the rationale for any credit-sharing or substitution as well as the process for validating that the joint degree curriculum is equivalent. The Division of Public Health offers the following joint degree programs described below. For the most part the joint degree students take the same 24 credits of required coursework as well as the 6-credit practicum and comprehensive examination. The joint degrees differ from the standalone MPH degree in the 15 credits of electives. All outside courses have been evaluated by the Curriculum Committee and are based on the previous competencies and deemed valuable substitutions (Reference File, Course Descriptions, Joint Degrees). The few exceptions to that rule are:
DNP/MPH - These joint degree students take two program planning and evaluation courses from the nursing department instead of the FP MD Public Health Program Planning, Evaluation and Implementation.
MD/MPH – These joint degree students have previously taken Social Medicine through the
medical school. Since the medical school has just gone through a massive curriculum revision, the social medicine and electives will now be reevaluated by the Curriculum committee.
Doctor of Medicine The Division of Public Health, in conjunction with the University of Utah School of Medicine, offers a joint MD/MPH degree. This is an ideal program for those medical students with an interest in clinical medicine as well as public health. MD/ MPH admission requirements and worksheet can be found in Appendix 2.11A. Interested students already accepted or enrolled into the University of Utah School of Medicine can apply to the MPH program. This combined degree program will require at least five years to complete. Students are required to take a one-year leave of absence from medical school to complete the public health degree requirements. This leave may be extended at the discretion of the dean for student affairs. The leave should be taken between the second and third years of medical school. In unusual circumstances this may occur between the first and second year or the third and fourth year at the discretion of the dean of student affairs. Table 2.11.1 Electives for the MD/MPH studentsMPH/MD elective credits below: INTMD 7580 International Health Elective INTMD 7650 Infectious Disease Clinical Clerkship INTMD 7780 Internal Medicine in the Community INTMD 7880 Research Problems in Infectious Disease INTMD 7990 International Health Preceptorship
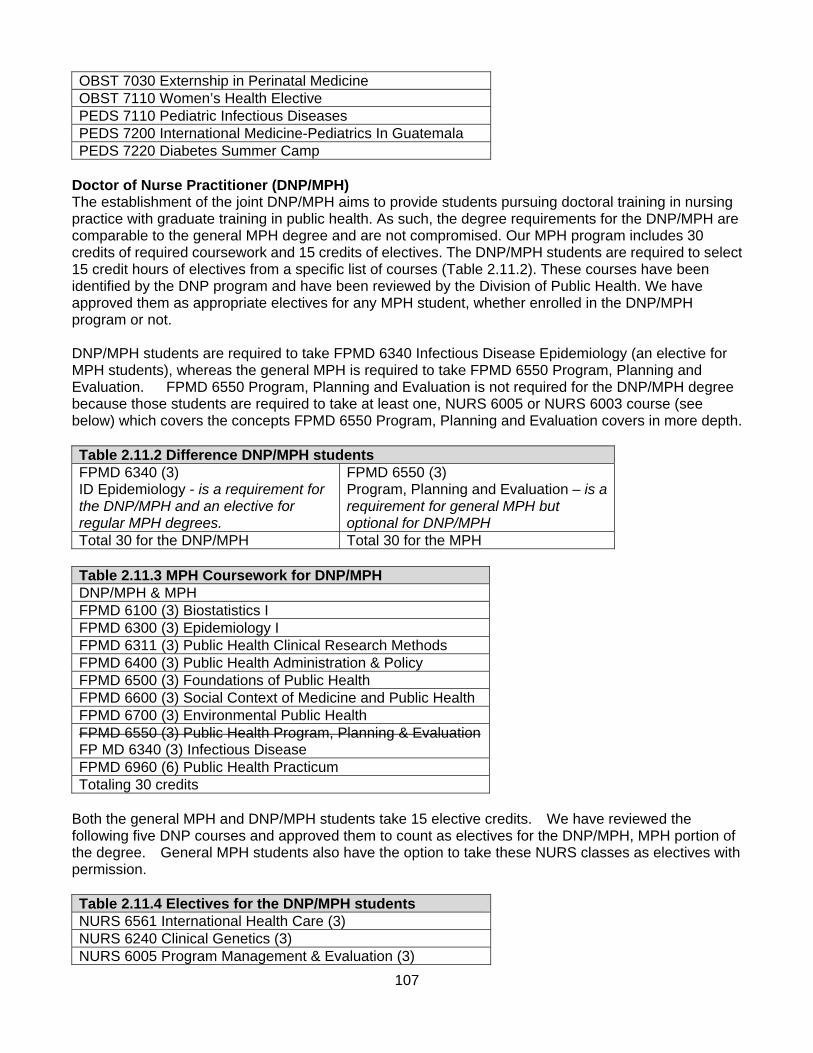
107
OBST 7030 Externship in Perinatal Medicine OBST 7110 Women’s Health Elective PEDS 7110 Pediatric Infectious Diseases PEDS 7200 International Medicine-Pediatrics In Guatemala PEDS 7220 Diabetes Summer Camp
Doctor of Nurse Practitioner (DNP/MPH) The establishment of the joint DNP/MPH aims to provide students pursuing doctoral training in nursing practice with graduate training in public health. As such, the degree requirements for the DNP/MPH are comparable to the general MPH degree and are not compromised. Our MPH program includes 30 credits of required coursework and 15 credits of electives. The DNP/MPH students are required to select 15 credit hours of electives from a specific list of courses (Table 2.11.2). These courses have been identified by the DNP program and have been reviewed by the Division of Public Health. We have approved them as appropriate electives for any MPH student, whether enrolled in the DNP/MPH program or not. DNP/MPH students are required to take FPMD 6340 Infectious Disease Epidemiology (an elective for MPH students), whereas the general MPH is required to take FPMD 6550 Program, Planning and Evaluation. FPMD 6550 Program, Planning and Evaluation is not required for the DNP/MPH degree because those students are required to take at least one, NURS 6005 or NURS 6003 course (see below) which covers the concepts FPMD 6550 Program, Planning and Evaluation covers in more depth. Table 2.11.2 Difference DNP/MPH students FPMD 6340 (3) ID Epidemiology - is a requirement for the DNP/MPH and an elective for regular MPH degrees.
FPMD 6550 (3) Program, Planning and Evaluation – is a requirement for general MPH but optional for DNP/MPH
Total 30 for the DNP/MPH Total 30 for the MPH Table 2.11.3 MPH Coursework for DNP/MPH DNP/MPH & MPH FPMD 6100 (3) Biostatistics I FPMD 6300 (3) Epidemiology I FPMD 6311 (3) Public Health Clinical Research Methods FPMD 6400 (3) Public Health Administration & Policy FPMD 6500 (3) Foundations of Public Health FPMD 6600 (3) Social Context of Medicine and Public Health FPMD 6700 (3) Environmental Public Health FPMD 6550 (3) Public Health Program, Planning & Evaluation FP MD 6340 (3) Infectious Disease FPMD 6960 (6) Public Health Practicum Totaling 30 credits
Both the general MPH and DNP/MPH students take 15 elective credits. We have reviewed the following five DNP courses and approved them to count as electives for the DNP/MPH, MPH portion of the degree. General MPH students also have the option to take these NURS classes as electives with permission. Table 2.11.4 Electives for the DNP/MPH students NURS 6561 International Health Care (3) NURS 6240 Clinical Genetics (3) NURS 6005 Program Management & Evaluation (3)

108
NURS 6003 Program Planning & Development (3) NURS 6772 Quality Improvement & Clinical Data Analysis (3)
Master of Healthcare Administration (MHA/MPH) This joint degree option prepares students for positions as program managers and health services researchers in state and local health departments, public health advocacy groups—such as HealthInsights, the state's healthcare quality improvement organization—and healthcare delivery organizations, such as the Veterans’ Administration Healthcare System and military healthcare facilities. The MHA/MPH joint degree program is a joint effort between the Department of Family and Preventive Medicine, Division of Public Health and the David Eccles School of Business (http://mha.business.utah.edu/page/mphmha-master-public-health); it gives students the option of earning an MHA degree in addition to a Master of Public Health, the two masters degrees being completed in approximately 66.5 credit hours. On average the joint degree will take students three years of full-time coursework; part-time students take an average of four years to complete the joint degree. Table 2.11.5 Electives for the MHA/MPH students ACCTG 6000 Financial Accounting (3)
ACCTG 6001 Managerial Accounting (1.5)
ECON 6190 Health Economics (3)
FINAN 6020 Financial Management (3)
FP MD 6600 Social and Behavioral Context of Public Health (3)
IS 6850 Healthcare Information Technology (1.5 credits)
MBA 6800 Field Study (5)
MGT 6051 Managing and Leading in Organizations (3)
Choose one option: MGT 6154 Competitive Advantage Through HR (1.5) OR PADMN 6360 Public Human Resource Management (3)
MHA 6550/MKTG 6550 Marketing for Health Professionals (3)
MHA 6551/MKTG 6551 (1.5) Environment of Healthcare I: Hospital Industry NOTE: Required 1st year of program MHA 6552/MKTG 6552 (1.5) Environment of Healthcare II: Leadership Principles and Practices NOTE: Required 2nd year of program MHA 6553/MKTG 6553 (1.5) Environment of Healthcare III: Healthcare Financial Management NOTE: Required final year of program MHA 6900/MKTG 6900 Healthcare Administration Internship (3) (Fall, Spring, Summer) Must be approved in advance by program director Choose one option: OIS 6060/6061 Production and Operations Management I & II (1.5 Fall & 1.5 Spring) OR OIS 6670 Managing Service Operations (3)
OIS 6420 Quality Management (1.5)
PADMN 6321 Health Policy (3)
Choose one: H EDU 5100 Health Care in the United States (3) H EDU 6790 Health Services Administration (3)

109
Choose one: LAW 7779 American Healthcare (3) LAW 7360 Health Care Regulation (3) MGT 6310 Business Law (3)
PADMN 6210 Public Administration & Law (3)
Choose one: MGT 6540 Ethics of Management (3) PADMN 6870 Public Administration and Ethics (3) PHIL 6520 Advanced Bioethics (3)
Master of Public Administration (MPA/MPH) The establishment of the joint MPA/MPH program is designed for students who seek advanced training in health policy analysis and program evaluation, as well as public health administration. Health issues are an area of priority within the public, nonprofit and private sectors. Students pursuing the MPA/MPH joint degree will acquire the skills needed to work in all three sectors. These skills include health policy analysis and program evaluation, government contracting with health agencies and nonprofits, aspects of managing health organizations, and law and ethics of health fields. Our MPH program includes 30 credits of required coursework, and 15 credits of electives. The MPA/MPH students will be required to select 15 credit hours of electives from the following list of courses (Table 2.11.6). These courses have been identified by the MPA program and have been reviewed by the Division of Public Health. We have approved them as appropriate electives for any MPH student, whether enrolled in the MPA/MPH program or not. Table 2.11.6 Electives for the MPA/MPH students PADMN 6300 Administrative Theory (3) PADMN 6550 Nonprofit/Nongovernmental Organizations (3) PADMN 6323 Policy Analysis (3) PADMN 6289 Research Design (3) PADMN 6210 Public Administration & Law (3) PADMN 6870 Public Administration & Ethics (3)
Master of Public Policy (MPP/MPH) The MPP/MPH program is designed for students who seek advanced training in the quantitative and qualitative methods of policy analysis as well as thorough preparation in the field of public health management and policy. Graduates will be prepared to develop policy-based approaches to improving and protecting the public’s health, in the public, non-profit and private sector. Through this joint degree program, graduates will also gain the skills needed to be effective in professional roles that involve health policy development, administration, and evaluation. Our MPH program includes 30 credits of required coursework, and 15 credits of electives. The MPP/MPH students will be required to select their electives from the following list of courses (Table 2.11.7). These courses were identified by the MPP program and have been reviewed by the Division of Public Health. We have approved them as appropriate electives for any MPH student, whether enrolled in the MPP/MPH program or not. Table 2.11.7 Electives for the MPP/MPH studentsPADMN 6320 Public Policy Theories (3) PADMN 6323 Policy Analysis (3) STAT 6003 Survey of Computer Software Packages (3) PUBPL 6900 Public Policy Research (3)
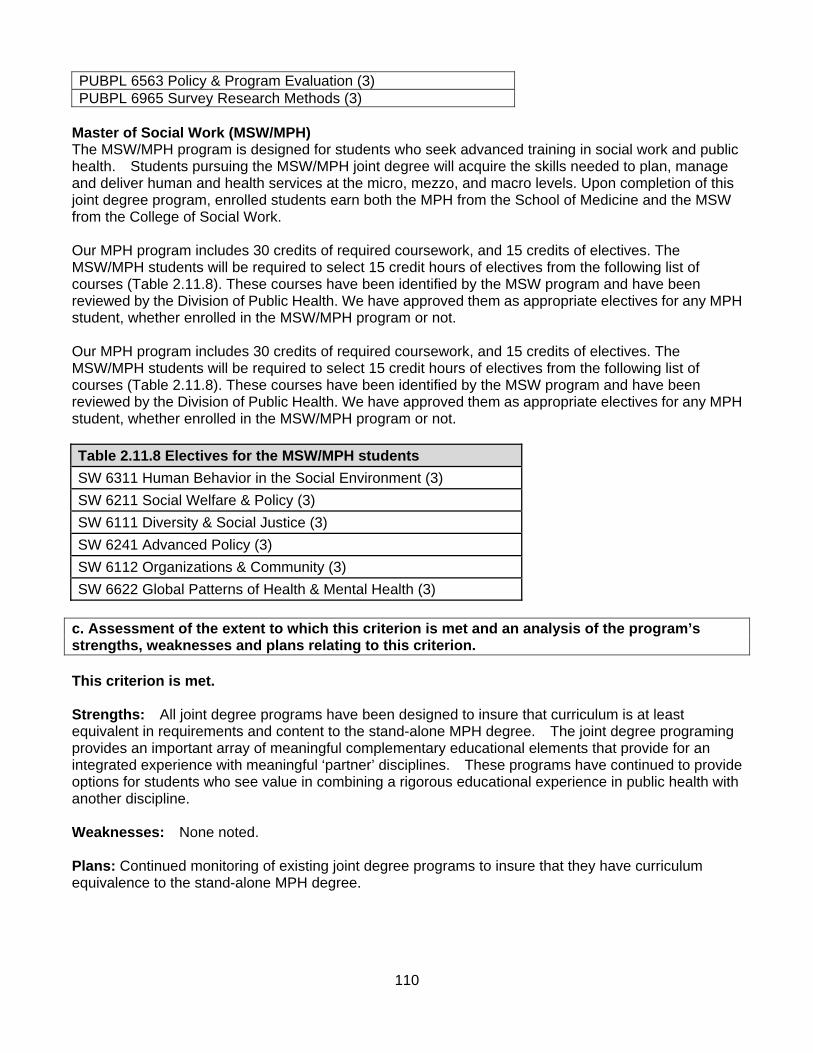
110
PUBPL 6563 Policy & Program Evaluation (3) PUBPL 6965 Survey Research Methods (3)
Master of Social Work (MSW/MPH) The MSW/MPH program is designed for students who seek advanced training in social work and public health. Students pursuing the MSW/MPH joint degree will acquire the skills needed to plan, manage and deliver human and health services at the micro, mezzo, and macro levels. Upon completion of this joint degree program, enrolled students earn both the MPH from the School of Medicine and the MSW from the College of Social Work. Our MPH program includes 30 credits of required coursework, and 15 credits of electives. The MSW/MPH students will be required to select 15 credit hours of electives from the following list of courses (Table 2.11.8). These courses have been identified by the MSW program and have been reviewed by the Division of Public Health. We have approved them as appropriate electives for any MPH student, whether enrolled in the MSW/MPH program or not. Our MPH program includes 30 credits of required coursework, and 15 credits of electives. The MSW/MPH students will be required to select 15 credit hours of electives from the following list of courses (Table 2.11.8). These courses have been identified by the MSW program and have been reviewed by the Division of Public Health. We have approved them as appropriate electives for any MPH student, whether enrolled in the MSW/MPH program or not. Table 2.11.8 Electives for the MSW/MPH students
SW 6311 Human Behavior in the Social Environment (3)
SW 6211 Social Welfare & Policy (3)
SW 6111 Diversity & Social Justice (3)
SW 6241 Advanced Policy (3)
SW 6112 Organizations & Community (3)
SW 6622 Global Patterns of Health & Mental Health (3) c. Assessment of the extent to which this criterion is met and an analysis of the program’s strengths, weaknesses and plans relating to this criterion. This criterion is met. Strengths: All joint degree programs have been designed to insure that curriculum is at least equivalent in requirements and content to the stand-alone MPH degree. The joint degree programing provides an important array of meaningful complementary educational elements that provide for an integrated experience with meaningful ‘partner’ disciplines. These programs have continued to provide options for students who see value in combining a rigorous educational experience in public health with another discipline. Weaknesses: None noted. Plans: Continued monitoring of existing joint degree programs to insure that they have curriculum equivalence to the stand-alone MPH degree.

111
2.12 Distance Education or Executive Degree Programs. If the program offers degree programs using formats or methods other than students attending regular on-site course sessions spread over a standard term, these degree programs must a) be consistent with the mission of the program and within the program’s established areas of expertise; b) be guided by clearly articulated student learning outcomes that are rigorously evaluated; c) be subject to the same quality control processes that other degree programs in the university are; and d) provide planned and evaluated learning experiences that take into consideration and are responsive to the characteristics and needs of adult learners. If the program offers distance education or executive degree programs, it must provide needed support for these programs, including administrative, travel, communication, and student services. The program must have an ongoing program to evaluate the academic effectiveness of the format, to assess learning methods and to systematically use this information to stimulate program improvements. The program must have processes in place through which it establishes that the student who registers in a distance education or correspondence education course or degree is the same student who participates in and completes the course or degree and receives the academic credit.
Not applicable.

112
3.0 Creation, Application and Advancement of Knowledge 3.1 Research. The program shall pursue an active research program, consistent with its mission, though which its faculty and students contribute to the knowledge base of the public health disciplines, including research directed at improving the practice of public health. a. Description of the program’s research activities, including policies, procedures and practices that support research and scholarly activities. Our main opportunity for growth is through the development of our research programs. We have implemented an Office of Public Health Research, directed by Dr. Christina Porucznik, that manages an ongoing tracking of grants being developed, submitted and funded (which is reviewed at each faculty meeting), a weekly Division faculty development meeting, increased focus at annual retreats, increased research-development support staffing, more investment in salary support for faculty research development, increased involvement in the School of Medicine K-award support programming, support for faculty member participation in national research development programs (such as the Grant Generating Program sponsored by the Society of Teachers of Family Medicine), and increased focus on mentoring for junior faculty members. The Division of Public Health’s research activities have grown over the past five years due to the growth and expansion of our faculty and collaborations with other faculty members both at the University of Utah and other institutions. We anticipate that our research activities will steadily increase in the years to come as we hire additional faculty members. Our research interests are broad and the opportunities that exist for growth in our research endeavors in an area that our faculty aims to make a top priority in the upcoming fiscal year. In addition to research being a major component of our mission, we are limited by other funding streams to keep our operation intact and therefore must rely on research generating activities in order to continue our operations as a Division. Our program follows the policies, procedures, and practices from these university entities:
Vice president for Research oversees all aspects of research at the university including the Office of Sponsored Projects, Conflict of Interest Committee, Institutional Review Board, University Research Committee, Research Instrumentation Committee, Funding Incentive Seed Grant Committee (http://research.utah.edu/)
Office of Sponsored Projects (OSP) assists our faculty and research staff with grant submissions and grant awards. The Division of Public Health follows all University of Utah research policies and procedures which includes negotiated federal F&A rates, budget accounting standards (including OMB Circular requirements/cost restrictions), standards for conduct of research, and other related regulations. Most of this information can be found in the research handbook: http://osp.utah.edu/policies/handbook/
Health Sciences Center Core operates a number of core facilities that offer both advanced technologies and equipment. The goal of the cores is to make technology and expertise available to all faculty members and students. The institutional view is that supporting core facilities is the single best way that institutional funds can be used to promote the University's research mission.
Funding Incentive Seed Grant Program sponsored by the University of Utah Research Foundation, supports new areas of research for a principal investigator. The investigator must clearly and convincingly demonstrate that the proposed project represents a new research direction in an area likely to generate extramural funding. http://www.research.utah.edu/funding/seed.html

113
University Tracking of Clinical Research (uTRAC) is a clinical research management system (CRMS) that builds comprehensive financial compliance assurance into the study management process, while also reducing duplicate data entry, facilitating non-financial study activities, and providing senior leadership with crucial institutional data.
Institutional Review Board protects the rights and welfare of human research participants. http://irb.utah.edu/
University Health Sciences Development Office fosters philanthropic opportunities in health care that support education, research, and community outreach. http://healthsciences.utah.edu/development/
Center for Clinical and Translational Science serves as an academic home for clinical and translational research, developing innovative health services for the community and researchers, and training a new generation of clinical and translational investigators. Their services include Bioinformatics, Clinical Services, Community Outreach & Collaboration, Patient-Centered Outcomes Research Methods, Recruitment, Retention & Safety, Research Education, Training & Career Development, Study Design & Biostatistics, and Translational Technologies & Resources. http://medicine.utah.edu/ccts/
REDCap is a secure, web-based application for building and managing online surveys and databases. Using REDCap's stream-lined process for rapidly developing projects, allows for creation and design of projects using 1) the online method from the web browser using the Online Designer; and/or 2) the offline method by constructing a 'data dictionary' template file in Microsoft Excel, which can be later uploaded into REDCap. https://redcap01.brisc.utah.edu/ccts/redcap/
FURTHeR assists the University of Utah research community with questions related to finding clinical cohorts for research purposes. This system is available to anyone with a University ID, is approved by the Institutional Review Board, and makes de-identified data available from the desktop via a web link. More data sources will become available as the system is expanded.
b. Description of current research activities undertaken in collaboration with local, state, national or international health agencies and community-based organizations. Formal research agreements with such agencies should be identified. We have several collaborative projects in process currently. Below is a brief statement on select projects.
We have partnered with Kirk Humanitarian; a charity that provides micronutrient supplements to at-risk women and children in less developed areas of the world. Specifically, we are working with women and children in Ghana, West Africa.
We also conduct research in other international regions of the world in conjunction with our study abroad programs. Our partnered sites include India, China, Ghana, Peru, Armenia, and Uganda.
International NaProTechnology Evaluation and Surveillance of Treatment (iNEST) Clinic-based study of outcomes of NaProTechnology treatment for infertility or miscarriage.
The Office of Cooperative Reproductive Health conducts research and education to increase understanding of normal human fertility and subfertility, the menstrual cycle, and the application of that knowledge by women, couples, clinicians, and researchers. Our philosophy is that knowledge regarding fertility can help couples achieve their pregnancy intentions in the healthiest ways possible, provide clinicians with powerful tools for restorative reproductive medicine, and aid researchers in understanding fecundity, pregnancy, and human development.
Home Observation of Periconceptional Exposures (HOPE): Study by identifying the date that pregnancy started, scientists can help determine when testing should occur during pregnancy in order to match important developmental milestones. Methods exist to determine the most fertile day using lab tests, but they are expensive and not practical for long-term use. The Home
114
Observation of Periconceptional Exposures (HOPE) Study will use a novel and simple method for determining ovulation/conception near the time that it occurs, known as the Peak Day method.
The Office of Public Health Practice in the Division of Public Health seeks to ensure a competent public health workforce in public and non-profit organizations in Utah, the Mountain West and globally. We strive to achieve this Mission by partnering with the region’s public health agencies and other academic and non-profit institutions to meet the following objectives: Gather and distribute information about the knowledge, competencies and training needs of the public health workforce. Facilitate and provide appropriate training and educational opportunities to meet the needs of the public health workforce by: Strategically develop systems that apply continuous quality improvement principles to workforce development.
Head and Neck Cancer Risk Prediction Model. The goals of the study are to estimate the attributable risks of a comprehensive list of head and neck cancer risk factors across world regions and utilize pooled data from the International Head and Neck Cancer Epidemiology Consortium in order to develop a risk prediction model for these cancers and to validate the risk prediction model.
Pilot study for a population-based cohort of ovarian cancer survivors in Utah: The goal of the project is to establish a population-based cohort of ovarian cancer patients and age-matched population-based controls in Utah to investigate the incidence of long-term health effects due to cancer treatment.
Epidemiology of testicular cancer in the Utah population: We are conducting a descriptive epidemiology, case-control and follow up study of testicular cancer patients in Utah, based on the Utah Population Database
Psychosocial outcomes of small bowel transplant recipients: Cincinnati Children’s Hospital Medical Center: The goal of this study is to document the longitudinal psychosocial and medical regimen adherence outcomes of children who received a small bowel or multivisceral transplant.
Coalition for a Healthier Community for Utah Women and Girls (UWAG):To evaluate the effectiveness of low vs. high intensity wellness coaching on lifestyle factors associated with obesity among women in 5 communities (African, African American, American Indian/Alaskan Native, Hispanic, Pacific Islander)
Utah AIDS Education and Training Center (several on-going quality improvement projects): To evaluate preventive health care received by HIV-positive women in Utah. To develop a model to estimate the mean clinic viral load among HIV-positive patients being seen at the University of Utah Infectious Diseases Clinic (Clinic 1A). To understand the characteristics of newly diagnosed HIV-positive patients who fail to present for their initial appointment at Clinic 1a.
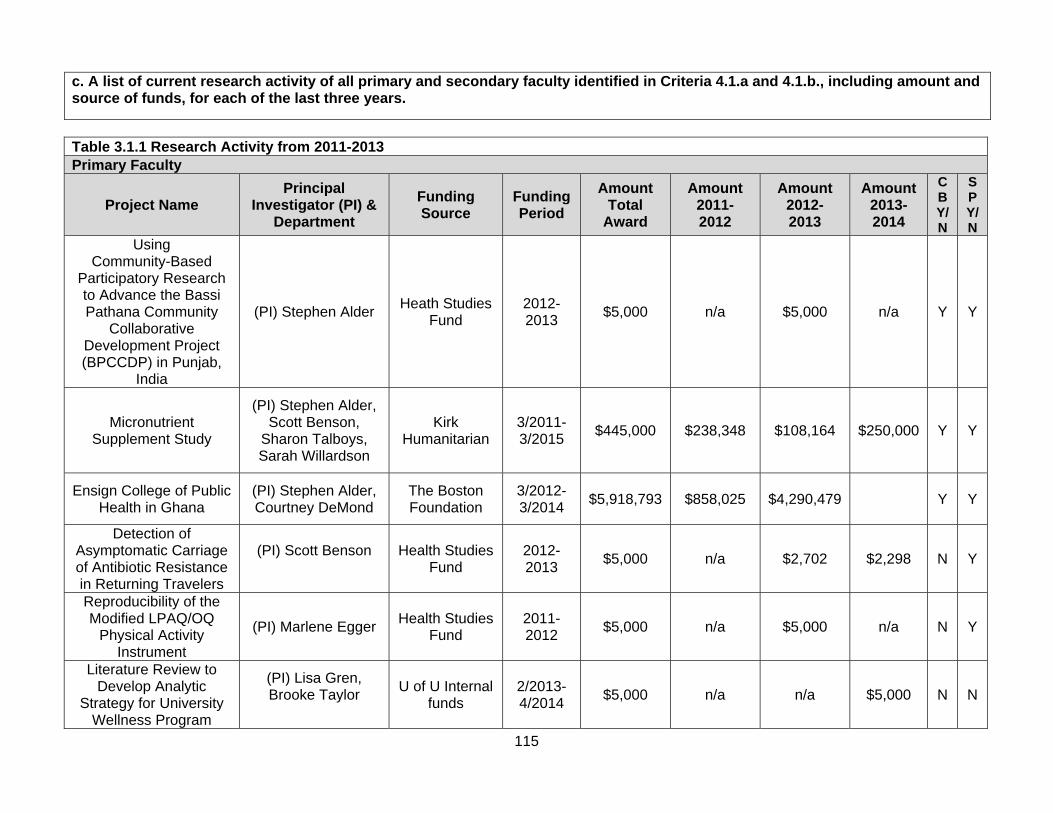
115
c. A list of current research activity of all primary and secondary faculty identified in Criteria 4.1.a and 4.1.b., including amount and source of funds, for each of the last three years.
Table 3.1.1 Research Activity from 2011-2013 Primary Faculty
Project Name Principal
Investigator (PI) & Department
Funding Source
Funding Period
Amount Total
Award
Amount 2011- 2012
Amount 2012- 2013
Amount 2013- 2014
CB Y/N
SP Y/N
Using Community-Based
Participatory Research to Advance the Bassi Pathana Community
Collaborative Development Project (BPCCDP) in Punjab,
India
(PI) Stephen Alder Heath Studies
Fund 2012- 2013
$5,000 n/a $5,000 n/a Y Y
Micronutrient Supplement Study
(PI) Stephen Alder, Scott Benson,
Sharon Talboys, Sarah Willardson
Kirk Humanitarian
3/2011- 3/2015
$445,000 $238,348 $108,164 $250,000 Y Y
Ensign College of Public Health in Ghana
(PI) Stephen Alder, Courtney DeMond
The Boston Foundation
3/2012- 3/2014
$5,918,793 $858,025 $4,290,479 Y Y
Detection of Asymptomatic Carriage of Antibiotic Resistance in Returning Travelers
(PI) Scott Benson
Health Studies Fund
2012- 2013
$5,000 n/a $2,702 $2,298 N Y
Reproducibility of the Modified LPAQ/OQ
Physical Activity Instrument
(PI) Marlene Egger Health Studies
Fund 2011- 2012
$5,000 n/a $5,000 n/a N Y
Literature Review to Develop Analytic
Strategy for University Wellness Program
(PI) Lisa Gren, Brooke Taylor
U of U Internal funds
2/2013- 4/2014
$5,000 n/a n/a $5,000 N N
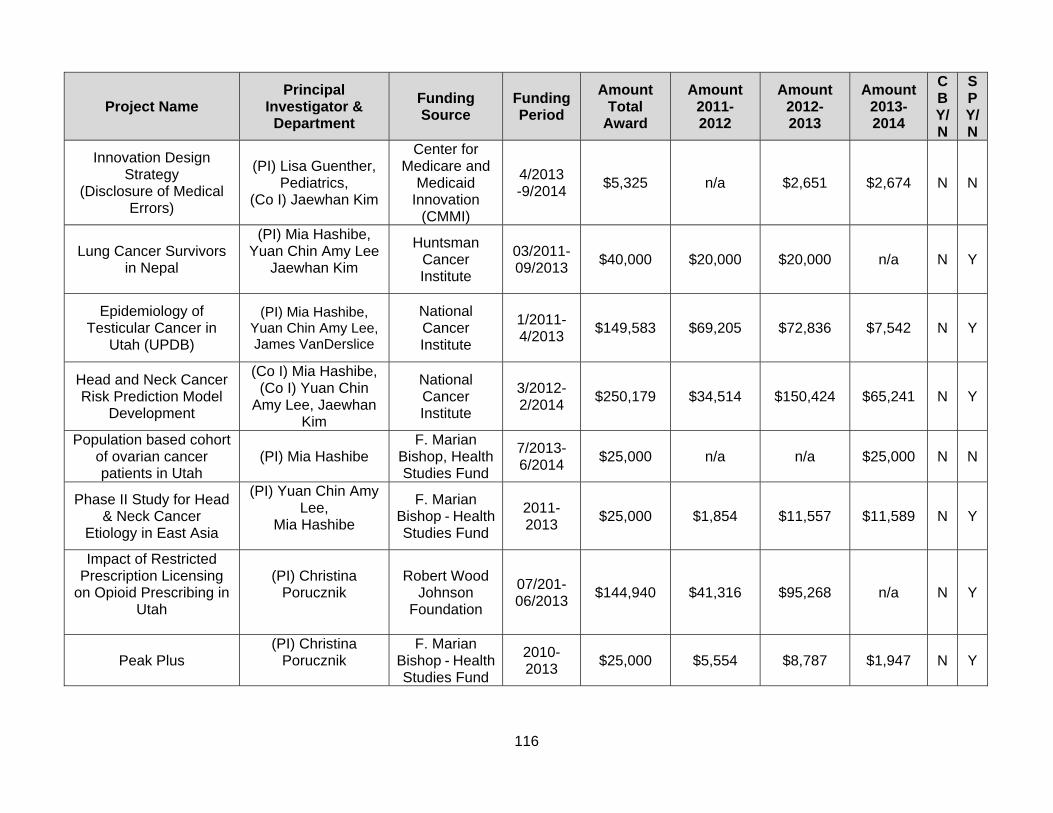
116
Project Name Principal
Investigator & Department
Funding Source
Funding Period
Amount Total
Award
Amount 2011- 2012
Amount 2012- 2013
Amount 2013- 2014
CB Y/N
SP Y/N
Innovation Design Strategy
(Disclosure of Medical Errors)
(PI) Lisa Guenther, Pediatrics,
(Co I) Jaewhan Kim
Center for Medicare and
Medicaid Innovation
(CMMI)
4/2013 -9/2014
$5,325 n/a $2,651 $2,674 N N
Lung Cancer Survivors in Nepal
(PI) Mia Hashibe, Yuan Chin Amy Lee
Jaewhan Kim
Huntsman Cancer Institute
03/2011- 09/2013
$40,000 $20,000 $20,000 n/a N Y
Epidemiology of Testicular Cancer in
Utah (UPDB)
(PI) Mia Hashibe, Yuan Chin Amy Lee, James VanDerslice
National Cancer Institute
1/2011- 4/2013
$149,583 $69,205 $72,836 $7,542 N Y
Head and Neck Cancer Risk Prediction Model
Development
(Co I) Mia Hashibe, (Co I) Yuan Chin
Amy Lee, Jaewhan Kim
National Cancer Institute
3/2012- 2/2014
$250,179 $34,514 $150,424 $65,241 N Y
Population based cohort of ovarian cancer patients in Utah
(PI) Mia Hashibe F. Marian
Bishop, Health Studies Fund
7/2013- 6/2014
$25,000 n/a n/a $25,000 N N
Phase II Study for Head & Neck Cancer
Etiology in East Asia
(PI) Yuan Chin Amy Lee,
Mia Hashibe
F. Marian Bishop - Health Studies Fund
2011- 2013
$25,000 $1,854 $11,557 $11,589 N Y
Impact of Restricted Prescription Licensing
on Opioid Prescribing in Utah
(PI) Christina Porucznik
Robert Wood Johnson
Foundation
07/201- 06/2013
$144,940 $41,316 $95,268 n/a N Y
Peak Plus (PI) Christina
Porucznik
F. Marian Bishop - Health Studies Fund
2010- 2013
$25,000 $5,554 $8,787 $1,947 N Y

117
Project Name Principal
Investigator & Department
Funding Source
Funding Period
Amount Total
Award
Amount 2011- 2012
Amount 2012- 2013
Amount 2013- 2014
CB Y/N
SP Y/N
Home Observation of Periconceptional
Exposures (HOPE) Periconceptionally
Timed Biomonitoring
(PI) Christina Porucznik,
Joseph Stanford, James VanDerslice,
Jaewhan Kim
National Institute of
Environmental Health
Sciences (NIEHS)
Outstanding New
Environmental Scientist (ONES)
8/2011- 4/2016
$2,127,996 $419,447 $411,077 $400,000 N Y
CDC Interagency Personnel Agreement
(IPA)
(PI) Christina Porucznik
Center for Disease Control
9/2013- 9/2014
$33,428 n/a n/a $25.072 N N
Assessing Child Developmental
Outcomes in the Fertility Experiences Study
(FES)
(PI) Sara Simonsen, (Co I) Joseph
Stanford
Marian Bishop Foundation
2012- 2013
$25,000 n/a $24,809 $191 N Y
International NaProTechnology
Evaluation and Surveillance of
Treatment - INEST
(PI) Joseph StanfordJaewhan Kim
Women's Reproductive Health Fund
10/2010- 9/2015
$236,451 $166,291 $18,541 n/a Y Y
Recovery of NDM-1 Plasmid Carrying
Bacteria from Tap Water
(PI) James VanDerslice
Health Studies Fund
2011- 2013
$5,000 n/a $5,000 n/a N Y
Integrating Spatial Data and Services into the
Utah Population Database
(PI) James VanDerslice,
(Co I) Ken Smith, HCI
Utah Population Database
7/2013- 6/2016
$15,000 n/a n/a $15,000 N N
Summary Totals $9,491,695 $1,854,554 $5,232,295 $786,507

118
Secondary Faculty
Project Name Principal
Investigator & Department
Funding Source
Funding Period
Amount Total
Award
Amount 2011- 2012
Amount 2012- 2013
Amount 2013- 2014
CB Y/N
SP Y/N
Translational Comparative
Effectiveness Research (T-Cer)
(PI) Carrie Byington, Pediatric,
Jaewhan Kim
Patient Care Research Network
6/2011- 5/2013
$95,560 $47,780 $45,513 n/a
Y
PA Training in Primary Care
(PI) Dan Crouse, Physician Assistant,
Lisa Gren
Department of Health and
Human Services
9/2011- 9/2016
$6,686 n/a n/a $6,686 N Y
Recurrent Gestational Diabetes Project
(PI) Jane Dyer, College of Nursing
(Co I) Sara Simonsen
University of Utah, College
of Nursing
7/2013- 6/2014
$3,000 n/a n/a $3,000 N N
Utah Area Health Education (AHEC)
(PI) Michael Magill, DFPM,
Stephen Alder, Sandra Marsh
Human Resources and
Services Administration
9/2012- 8/2013
$274,281 $300,387 $274,281 $275,000 Y Y
University of Utah, Center for Clinical &
Translational Sciences: CCTS Research &
Design & Biostatistics Core
(PI) Donald McClain, Division of
Endocrinology, Metabolism and
Diabetes, Jaewhan Kim
Marlene Egger
National Institute of
Health
3/2012- 7/2013
$51,206 $12,512 $12,982 $25,712 N N
University of Utah, Center for Clinical &
Translational Sciences: CTR Clinical Translation
Association
(PI) Donald McClain, Division of
Endocrinology, Metabolism and
Diabetes, Stephen Alder
National Institute of
Health
5/2008- 4/2014
$48,044 $15,000 $16,440 $16,604 Y Y
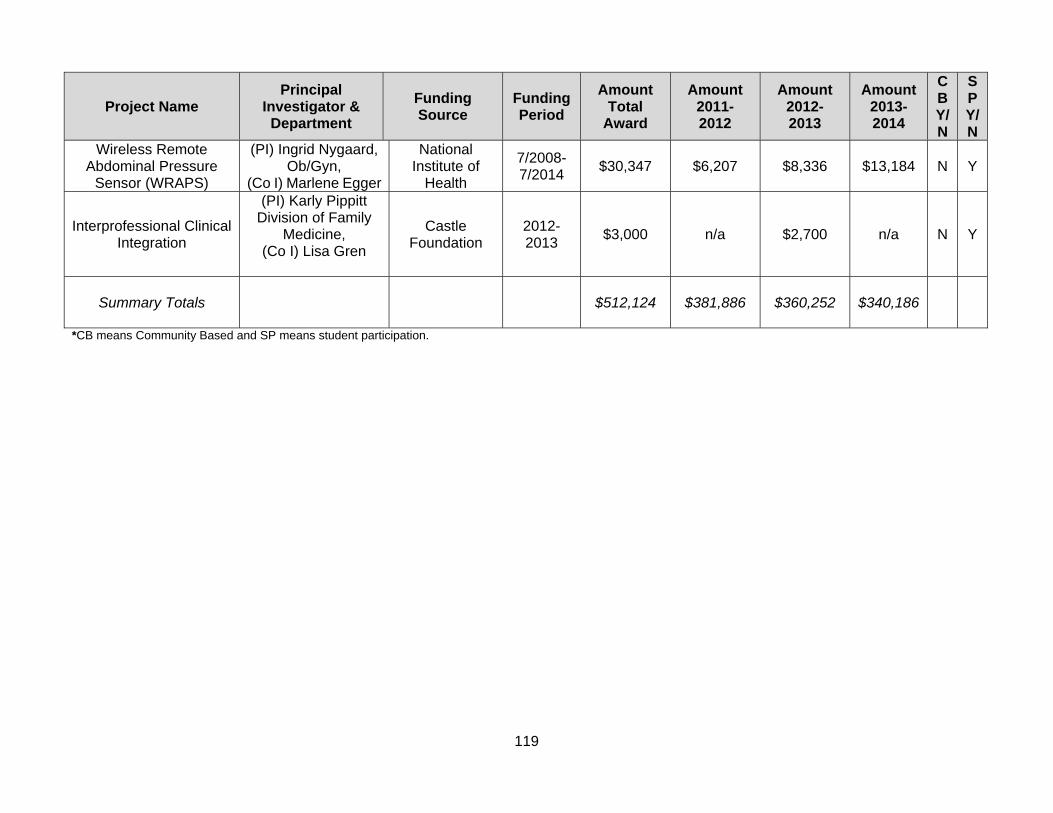
119
Project Name Principal
Investigator & Department
Funding Source
Funding Period
Amount Total
Award
Amount 2011- 2012
Amount 2012- 2013
Amount 2013- 2014
CB Y/N
SP Y/N
Wireless Remote Abdominal Pressure
Sensor (WRAPS)
(PI) Ingrid Nygaard, Ob/Gyn,
(Co I) Marlene Egger
National Institute of
Health
7/2008- 7/2014
$30,347 $6,207 $8,336 $13,184 N Y
Interprofessional Clinical Integration
(PI) Karly Pippitt Division of Family
Medicine, (Co I) Lisa Gren
Castle Foundation
2012- 2013
$3,000 n/a $2,700 n/a N Y
Summary Totals $512,124 $381,886 $360,252 $340,186
*CB means Community Based and SP means student participation.

120
d. Identification of measures by which the program may evaluate the success of its research activities, along with data regarding the program’s performance against those measures for each of the last three years. For example, programs may track dollar amounts of research funding, significance of findings (eg, citation references), extent of research translation (eg, adoption by policy or statute), dissemination (eg, publications in peer-reviewed publications, presentations at professional meetings) and other indicators. Table 3.1.2 Outcome Measures for Research activities
Outcome Measure Target 2011- 2012
2012- 2013
2013- 2014
Faculty members will publish their research findings in at least four peer-reviewed journals per year.
Average number per faculty member
2 4 1 (Feb. 2014)
An annual list of peer reviewed publications for each faculty will be
prepared
1 summary publication list per year
100% 100% 100%
Faculty members will support manuscript preparation and
submission with PhD, masters level and medical students.
1 published peer-reviewed publication per faculty member, per year with student co-author.
69% 100% 100%
Faculty members will attend and present at national meeting each year that aligns with their academic focus.
Present and attend at least one national meeting each year
93% 85% 95% (Feb 2014)
Each faculty member is actively involved in a project that formally
engages at least one other discipline.
Actively involved in at least 1 project.
75% 100% 100%
All faculty members will participate and present research in University of Utah
scholarly forum annually.
All faculty members will participate and present research in at least one University of Utah
scholarly forum annually.
69% 92% 69%
Maintain scholarly-productive community collaboration to ensure emphasis in community-engaged
scholarship.
Expect all faculty members to be formally engaged in at least one scholarly-productive community
collaboration.
56% 85% 80%
Incoming doctoral students will be matched to faculty for their research
expertise
All doctoral students matched for research interest to faculty
100% 100% 100%
Incoming master students will be matched to faculty for their research
expertise
All master students matched for research interest to faculty
80% 85% 90%
Involve doctoral and master students in faculty driven research.
1/4 doctoral students and 1/10 master students
PhD 63%
Master 100%
PhD 100% Master 100%
PhD 100% Master 100%
Tenure-line or research track faculty member will formally mentor or involve
clinical learner in scholarly activities (clinical student, medical student,
nursing students, pharmacy student, residents and fellows etc.).
one clinical learner per tenure-line or research track
faculty. 56% 100% 53%

121
e. Description of student involvement in research. Students within the Division are involved in research projects led by the faculty in the Division. Students are the main resource for research assistant positions available on faculty grants. The typical student research assistant would support the faculty in developing questionnaires for the project, coordinating the project, managing and analyzing data, writing scientific reports, and conducting literature reviews. A summary of students involved in the major projects conducted by our faculty are summarized below. 2011-12 Grants 1. International Napro Technology Evaluation and Surveillance of Treatment (Kaitlin Carruth, Michael
Lowe, Jessica Sanders, Nirupma Singh) 2. Multiple Micronutrient Supplement Study of Women of Reproductive Age (Steve Manortey) 3. Changes in Controlled Substance Prescribing Licensing Lead to Changes in Opiod Prescribing or
Adverse outcomes (Windy Tanner) 4. Effectiveness Intention in Behavior and Creighton Model NFP Use (Kaitlin Carruth, Daisy Krakowiak,
Nirupma Singh) 5. Outcomes of Infertility Treatments in Clinic and Population-Based Cohort (Scarlett Reeves, Jessica
Sanders, Melissa Sperry, Mandy Ward (MD student), Alessandra Zimmerman (MD student)) 6. HOPE - Peri-Conceptionally Timed Biomonitoring (Kyley Cox) 7. Advancing the Science Linkage Studies between Drinking Water Contaminants and Adverse Birth
outcomes (Mohammed Al-Temimi, Sam Allen, Alycia Parnell, Marissa Taddie, Windy Tanner) 8. Advancing the science linkage studies between drinking water contaminants and adverse birth
outcomes (Marissa Taddie, Windy Tanner, Alycia Parnell) 9. Epidemiology of testicular cancer in Utah (Mohammed Al-Temimi, Mei Wei) 2012-13 1. Multiple Micronutrient Supplement Study of Women of Reproductive Age (Steve Manortey) 2. Changes in Controlled Substance Prescribing Licensing Lead to Changes in Opiod Prescribing or
Adverse outcomes (Windy Tanner) 3. HOPE - Peri-Conceptionally Timed Biomonitoring (Lindsay Schmidt, Nicole Bailey) 4. Advancing the Science Linkage Studies between Drinking Water Contaminants and Adverse Birth
outcomes (Marissa Taddie, Windy Tanner, Alycia Parnell) 5. Epidemiology of testicular cancer in Utah (Mohammed Al-Temimi) 6. Environmental risk factors for lung cancer in Nepal (Rob Crosbie)
2013-14 1. Peri-conceptionally Times Biomonitoring (Nicole Bailey)
f. Assessment of the extent to which this criterion is met and an analysis of the program’s strengths, weaknesses and plans relating to this criterion. This criterion is met. Strengths: Our faculty is active in research, with a growing portfolio of funded research projects as demonstrated in Table 3.1.1. The research expertise of our faculty is both diverse and complementary, allowing for focused and collaborative, multi-disciplinary projects. Students are increasingly involved in the faculty research as research assistants and credit generating activities. The general trend of expansion is expected to continue consistent with our goals in having a competitive extramurally funded research program. Research remains a major priority for our institution. Our faculty is also active in collaborating with other investigators on campus in research generating projects and contracts. Our Research Inventory
122
provides a mechanism for tracking the development, submission and implementation of grant funded activities. Weaknesses: The major challenge in growing our research program is accessing funds for activities needed to develop competitive research proposals and supporting a growing grants management infrastructure. Plans: Expanding our research program includes two major strategies. The first is supporting the existing research program by actively seeking resources that will support faculty time for developing proposals and the grants support infrastructure. Secondly, we continue to pursue resources to support our research program, including intramural research development funds, supplemental funds for such activities as planning, and federal funds with higher indirect rates that will allow us more leverage institutionally to negotiate for investment funds.

123
3.2 Service. The program shall pursue active service activities, consistent with its mission, though which faculty and students contribute to the advancement of public health practice. a. Description of the program’s service activities, including policies, procedures and practices that support service. If the program has formal contracts or agreements with external agencies, these should be noted. Division faculty members are expected to have service as part of their academic activities. This is also required as part of the retention, promotion and tenure (RPT) process of the University (for additional details on the RPT process see website: http://medicine.utah.edu/facultyadmin/rpt/criteria/) Tracking each faculty members proportion of time spent in service activities is part the Health Sciences Center Mission-Based Management System (MBM). MBM helps the Health Sciences Center “understand the distribution of faculty’s commitments across research, education, clinical service, and academic/community service, and thereby understand the costs of our missions.” (Vivian Lee, MD, PhD, MBA - http://healthsciences.utah.edu/mbm/) Division faculty members provide service in a variety of ways. They serve as consultants to colleagues in health-related projects, both within the School of Medicine and other departments in the University. Clinical and other professional consultations are also provided to clinical groups in the region. Faculty members are involved in providing consultation to the Utah Department of Health and the Salt Lake County Health Department around issues of public health as well as serving in official capacities, such as membership on the Salt Lake County Board of Health. See table 3.2.1 for roles and organization. The Division has formal contracts; with the Utah Department of Health (UDOH) for the Utah Statewide Immunization System (USIIS), Utah’s Area Health Education Centers (AHEC), Utah Population Database (UPDB), described in 1.4 b. More specifically, Dr. Porucznik has an Interagency Personnel agreement with the CDC. Dr. VanDerslice has a contact to conduct research and prepare dissemination materials that identify areas with high potential for private well contamination with the CDC. Dr. Sundwall has an agreement with the Medicaid Commission (Medicaid and CHIP Payment and Access Commission – MACPAC). The Division is frequently approached to provide service. Given the breadth of discipline of public health, one of the challenges faced by the Division is to fulfill its service role with a limited number of faculty members. At an appropriate level, service activities can be part of a well-rounded faculty experience. However, the current high service demands can serve to distract from other faculty responsibilities. b. Description of the emphasis given to community and professional service activities in the promotion and tenure process. “Promotion in rank is the acknowledgement by the university of excellence in performance in teaching, research, and creative work, professional competence, activity, and responsibility, and university and public service.” http://medicine.utah.edu/facultyadmin/rpt/overview.htm Recognition is accorded faculty members for the quality and extent of their public service. Demonstration of effective service at a level appropriate to rank is essential for retention, promotion, and tenure. Our university is a Carnegie designated community engaged institution and light of that we look to the expectation is that every faculty will be involved in engaged service.

124
c. A list of the program’s current service activities, including identification of the community, organization, agency or body for which the service was provided and the nature of the activity, over the last three years. See CEPH Data Template 3.2.1. Projects presented in Criterion 3.1 should not be replicated here without distinction. Funded service activities may be reported in a separate table; see CEPH Template 3.2.2. Extramural funding for research or training/continuing education grants should be reported in Template 3.1.1 (research) or Template 3.3.1 (funded workforce development), respectively.
Table 3.2.1 Faculty Service from 2011 to 2014
Faculty Member
Role Organization Activity or Project Year (s)
Stephen Alder
Member Framing the Future Task Force: The Next 100 Years
2011- 2015
Board Member Salt Lake County Board of Health
2009- 2015
Chair Chair of the Finance Committee, Salt Lake County Board of Health
2009- 2015
President Association of Accredited Public Health Programs (President-Elect 2009-2011)
2011- 2014
Member Presidential Commission on the Status of Women
2013- 2014
Member Health System Innovation and Research Steering Committee
2013- Present
Member Institute for Health Care Transformation Inaugural Advisory Board
2013- Present
Member Utah Leaders For Health Coalition (sponsored by the Utah Department of Health)
2013- Present
Board of Trustees
Ensign College of Public Health, Kpong, Ghana
2012- Present
Member Utah Personalized Health Coalition
2012- Present
Member Community Faces of Utah (community coalition)
2008- Present
Member Barekuma Community Collaboration Coalition (community coalition in Kumasi, Ghana)
2006 – Present
L. Scott Benson
Board of Directors
Silver Fork Pipeline Corporation
2000- Present
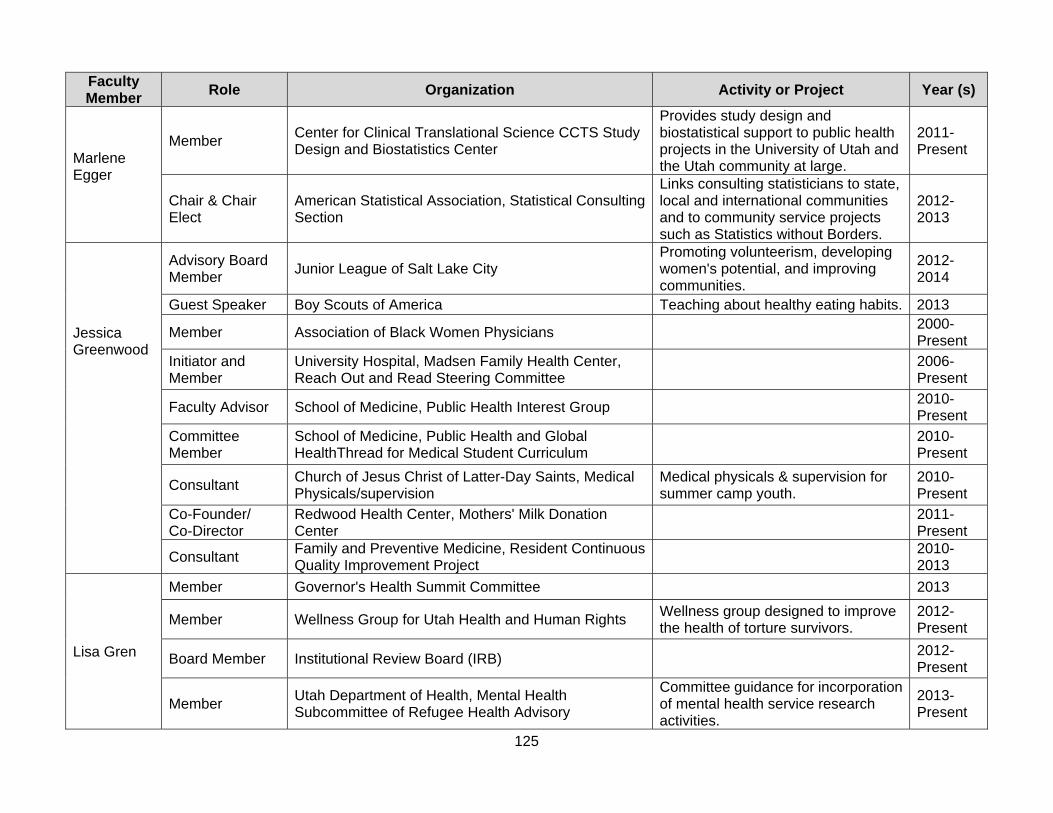
125
Faculty Member
Role Organization Activity or Project Year (s)
Marlene Egger
Member Center for Clinical Translational Science CCTS Study Design and Biostatistics Center
Provides study design and biostatistical support to public health projects in the University of Utah and the Utah community at large.
2011- Present
Chair & Chair Elect
American Statistical Association, Statistical Consulting Section
Links consulting statisticians to state, local and international communities and to community service projects such as Statistics without Borders.
2012- 2013
Jessica Greenwood
Advisory Board Member
Junior League of Salt Lake City Promoting volunteerism, developing women's potential, and improving communities.
2012- 2014
Guest Speaker Boy Scouts of America Teaching about healthy eating habits. 2013
Member Association of Black Women Physicians 2000- Present
Initiator and Member
University Hospital, Madsen Family Health Center, Reach Out and Read Steering Committee
2006- Present
Faculty Advisor School of Medicine, Public Health Interest Group 2010- Present
Committee Member
School of Medicine, Public Health and Global HealthThread for Medical Student Curriculum
2010- Present
Consultant Church of Jesus Christ of Latter-Day Saints, Medical Physicals/supervision
Medical physicals & supervision for summer camp youth.
2010- Present
Co-Founder/ Co-Director
Redwood Health Center, Mothers' Milk Donation Center
2011- Present
Consultant Family and Preventive Medicine, Resident Continuous Quality Improvement Project
2010- 2013
Lisa Gren
Member Governor's Health Summit Committee 2013
Member Wellness Group for Utah Health and Human Rights Wellness group designed to improve the health of torture survivors.
2012- Present
Board Member Institutional Review Board (IRB)
2012- Present
Member Utah Department of Health, Mental Health Subcommittee of Refugee Health Advisory
Committee guidance for incorporation of mental health service research activities.
2013- Present
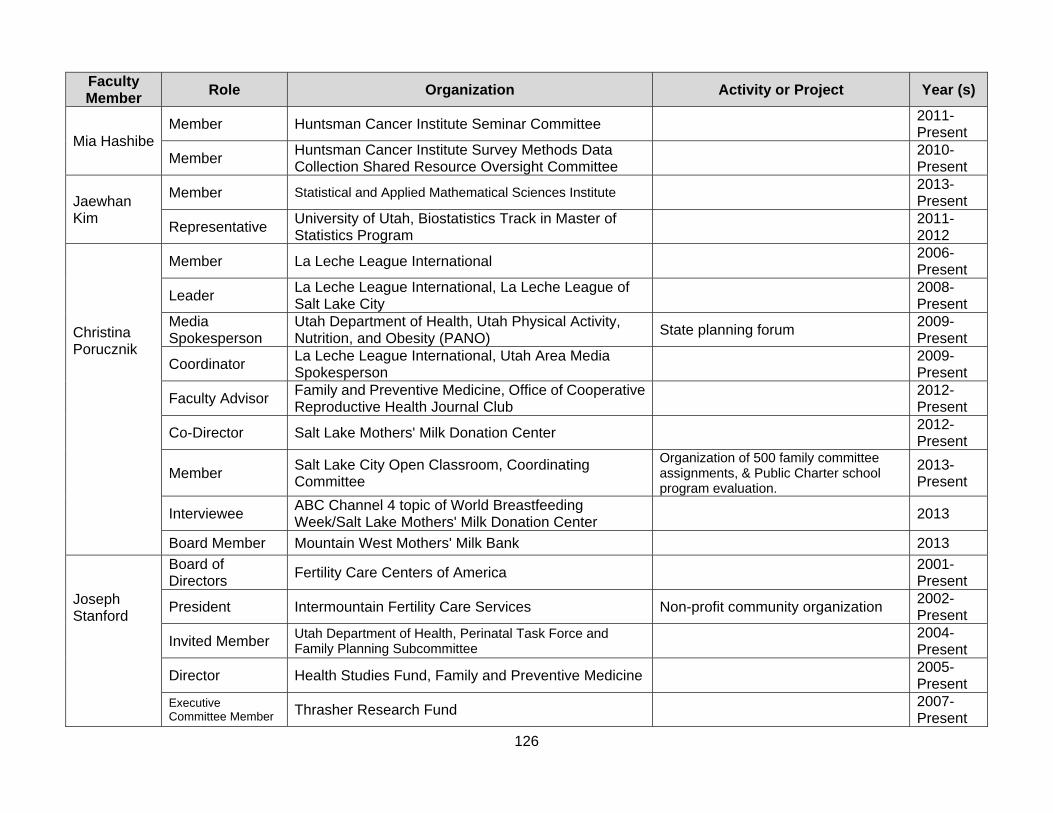
126
Faculty Member
Role Organization Activity or Project Year (s)
Mia Hashibe Member Huntsman Cancer Institute Seminar Committee
2011- Present
Member Huntsman Cancer Institute Survey Methods Data Collection Shared Resource Oversight Committee
2010- Present
Jaewhan Kim
Member Statistical and Applied Mathematical Sciences Institute
2013- Present
Representative University of Utah, Biostatistics Track in Master of Statistics Program
2011- 2012
Christina Porucznik
Member La Leche League International 2006- Present
Leader La Leche League International, La Leche League of Salt Lake City
2008- Present
Media Spokesperson
Utah Department of Health, Utah Physical Activity, Nutrition, and Obesity (PANO)
State planning forum 2009- Present
Coordinator La Leche League International, Utah Area Media Spokesperson
2009- Present
Faculty Advisor Family and Preventive Medicine, Office of Cooperative Reproductive Health Journal Club
2012- Present
Co-Director Salt Lake Mothers' Milk Donation Center 2012- Present
Member Salt Lake City Open Classroom, Coordinating Committee
Organization of 500 family committee assignments, & Public Charter school program evaluation.
2013- Present
Interviewee ABC Channel 4 topic of World Breastfeeding Week/Salt Lake Mothers' Milk Donation Center
2013
Board Member Mountain West Mothers' Milk Bank 2013
Joseph Stanford
Board of Directors
Fertility Care Centers of America 2001- Present
President Intermountain Fertility Care Services Non-profit community organization 2002- Present
Invited Member Utah Department of Health, Perinatal Task Force and Family Planning Subcommittee
2004- Present
Director Health Studies Fund, Family and Preventive Medicine 2005- Present
Executive Committee Member Thrasher Research Fund
2007- Present
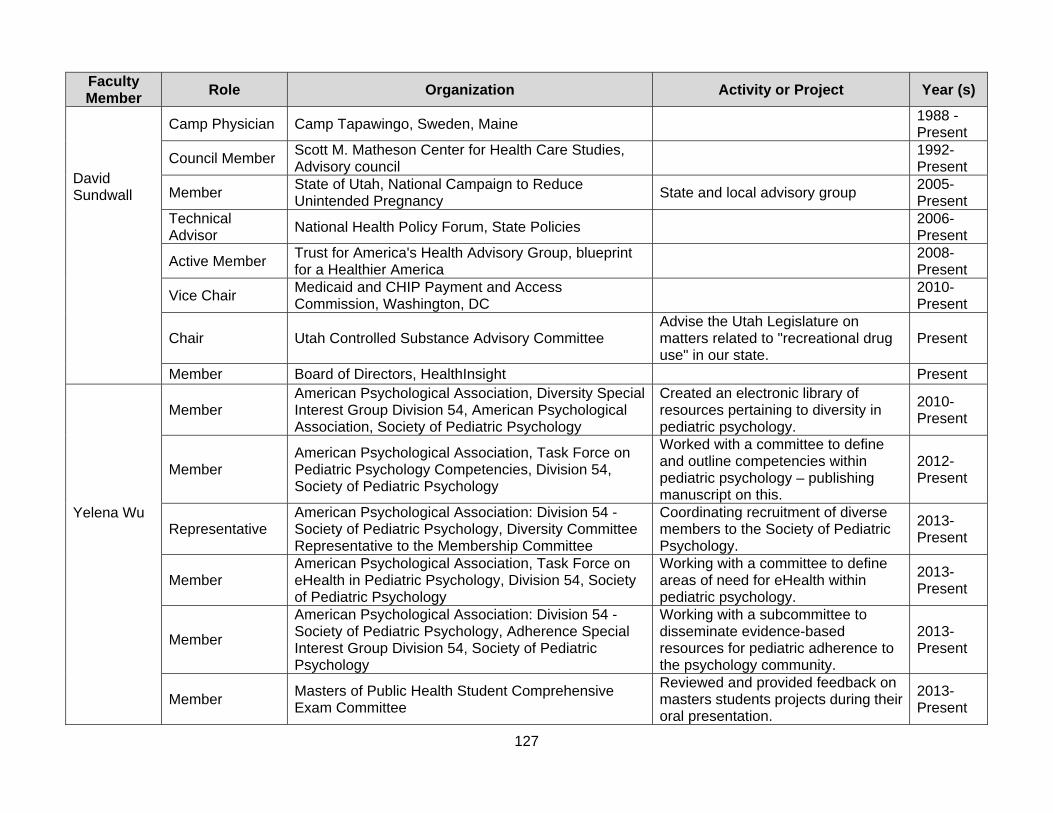
127
Faculty Member
Role Organization Activity or Project Year (s)
David Sundwall
Camp Physician Camp Tapawingo, Sweden, Maine 1988 - Present
Council Member Scott M. Matheson Center for Health Care Studies, Advisory council
1992- Present
Member State of Utah, National Campaign to Reduce Unintended Pregnancy
State and local advisory group 2005- Present
Technical Advisor
National Health Policy Forum, State Policies 2006- Present
Active Member Trust for America's Health Advisory Group, blueprint for a Healthier America
2008- Present
Vice Chair Medicaid and CHIP Payment and Access Commission, Washington, DC
2010- Present
Chair Utah Controlled Substance Advisory Committee Advise the Utah Legislature on matters related to "recreational drug use" in our state.
Present
Member Board of Directors, HealthInsight Present
Yelena Wu
Member American Psychological Association, Diversity Special Interest Group Division 54, American Psychological Association, Society of Pediatric Psychology
Created an electronic library of resources pertaining to diversity in pediatric psychology.
2010- Present
Member American Psychological Association, Task Force on Pediatric Psychology Competencies, Division 54, Society of Pediatric Psychology
Worked with a committee to define and outline competencies within pediatric psychology – publishing manuscript on this.
2012- Present
Representative American Psychological Association: Division 54 - Society of Pediatric Psychology, Diversity Committee Representative to the Membership Committee
Coordinating recruitment of diverse members to the Society of Pediatric Psychology.
2013- Present
Member American Psychological Association, Task Force on eHealth in Pediatric Psychology, Division 54, Society of Pediatric Psychology
Working with a committee to define areas of need for eHealth within pediatric psychology.
2013- Present
Member
American Psychological Association: Division 54 - Society of Pediatric Psychology, Adherence Special Interest Group Division 54, Society of Pediatric Psychology
Working with a subcommittee to disseminate evidence-based resources for pediatric adherence to the psychology community.
2013- Present
Member Masters of Public Health Student Comprehensive Exam Committee
Reviewed and provided feedback on masters students projects during their oral presentation.
2013- Present
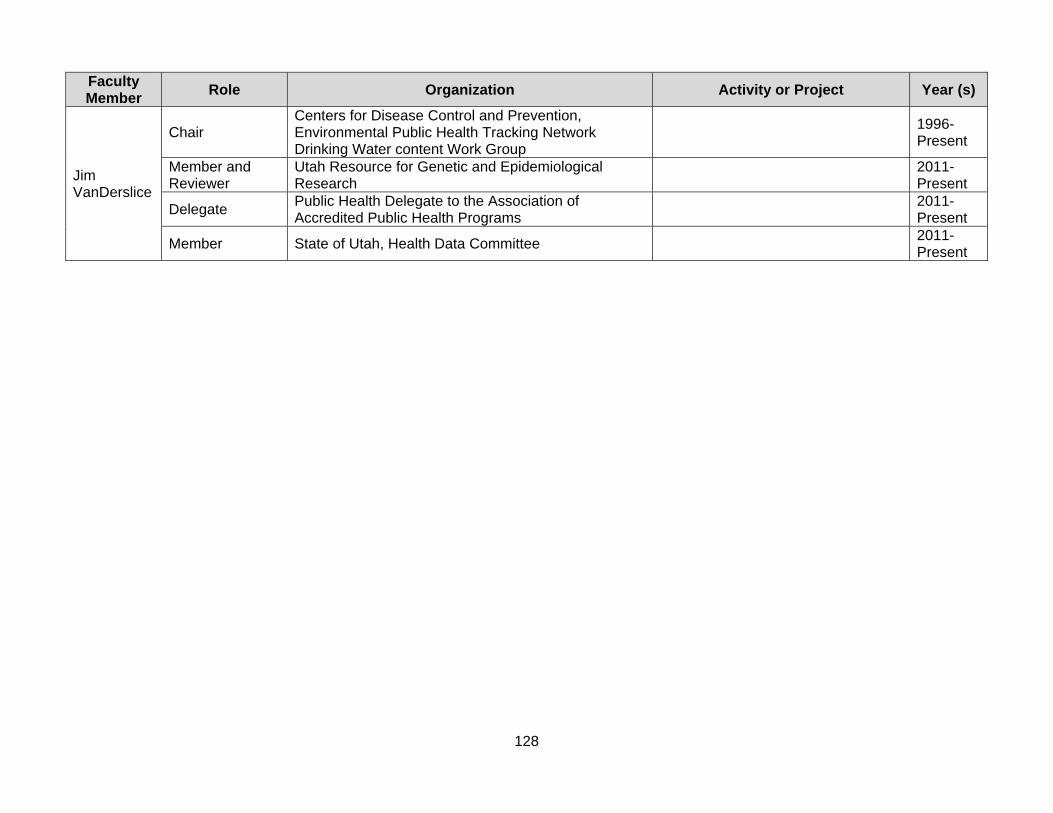
128
Faculty Member
Role Organization Activity or Project Year (s)
Jim VanDerslice
Chair Centers for Disease Control and Prevention, Environmental Public Health Tracking Network Drinking Water content Work Group
1996- Present
Member and Reviewer
Utah Resource for Genetic and Epidemiological Research
2011- Present
Delegate Public Health Delegate to the Association of Accredited Public Health Programs
2011- Present
Member State of Utah, Health Data Committee
2011- Present
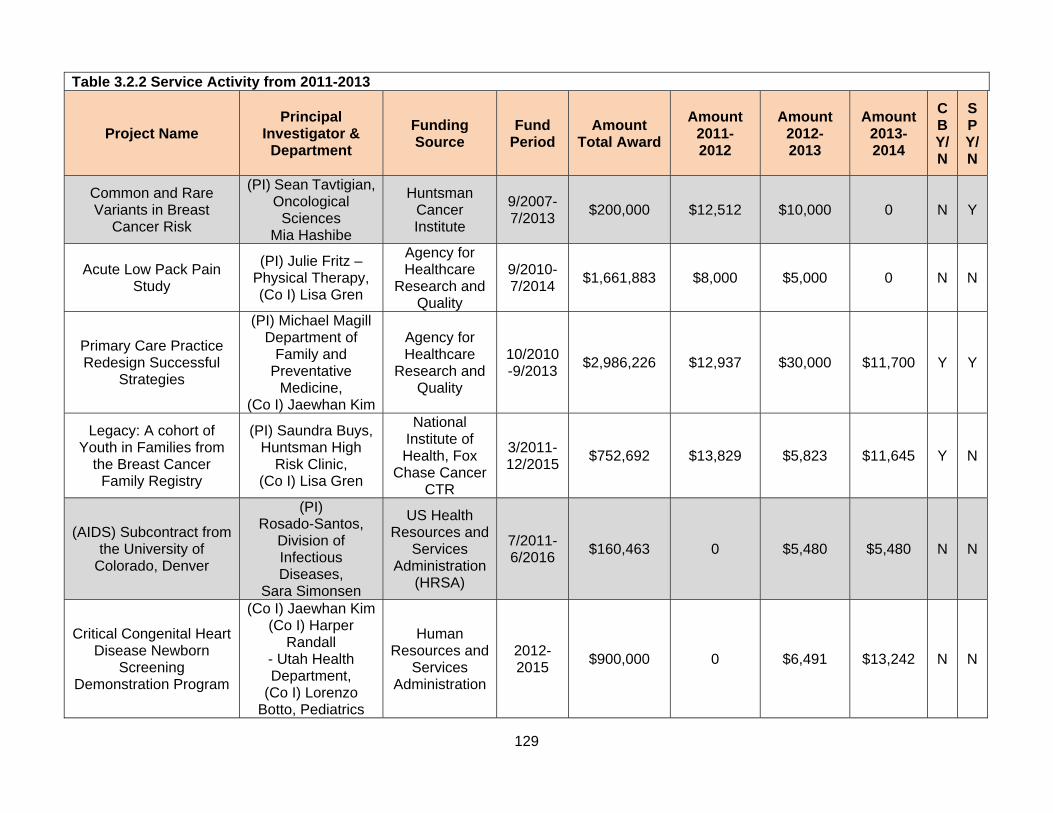
129
Table 3.2.2 Service Activity from 2011-2013
Project Name
Principal
Investigator & Department
Funding Source
Fund Period
Amount Total Award
Amount 2011- 2012
Amount 2012- 2013
Amount 2013- 2014
CB Y/N
SP Y/N
Common and Rare Variants in Breast
Cancer Risk
(PI) Sean Tavtigian,Oncological
Sciences Mia Hashibe
Huntsman Cancer Institute
9/2007- 7/2013
$200,000 $12,512 $10,000 0 N Y
Acute Low Pack Pain Study
(PI) Julie Fritz – Physical Therapy, (Co I) Lisa Gren
Agency for Healthcare
Research and Quality
9/2010- 7/2014
$1,661,883 $8,000 $5,000 0 N N
Primary Care Practice Redesign Successful
Strategies
(PI) Michael Magill Department of
Family and Preventative
Medicine, (Co I) Jaewhan Kim
Agency for Healthcare
Research and Quality
10/2010-9/2013
$2,986,226 $12,937 $30,000 $11,700 Y Y
Legacy: A cohort of Youth in Families from
the Breast Cancer Family Registry
(PI) Saundra Buys, Huntsman High
Risk Clinic, (Co I) Lisa Gren
National Institute of Health, Fox
Chase Cancer CTR
3/2011- 12/2015
$752,692 $13,829 $5,823 $11,645 Y N
(AIDS) Subcontract from the University of
Colorado, Denver
(PI) Rosado-Santos,
Division of Infectious Diseases,
Sara Simonsen
US Health Resources and
Services Administration
(HRSA)
7/2011- 6/2016
$160,463 0 $5,480 $5,480 N N
Critical Congenital Heart Disease Newborn
Screening Demonstration Program
(Co I) Jaewhan Kim(Co I) Harper
Randall - Utah Health Department,
(Co I) Lorenzo Botto, Pediatrics
Human Resources and
Services Administration
2012- 2015
$900,000 0 $6,491 $13,242 N N
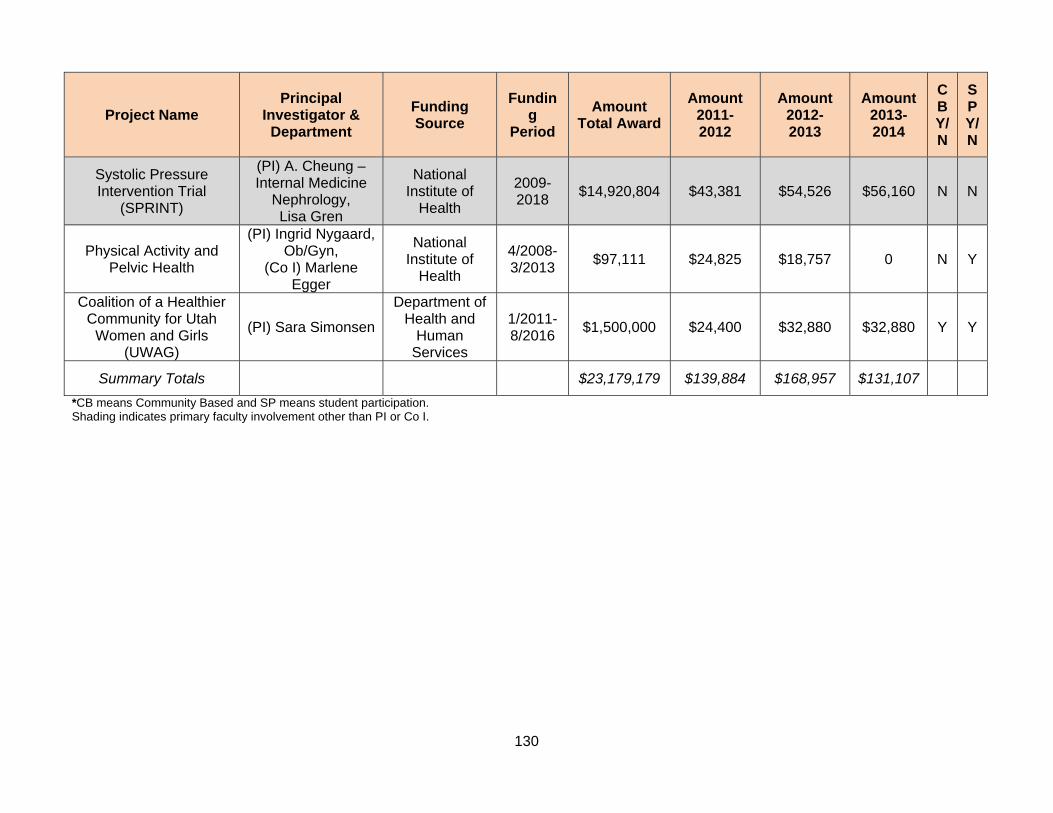
130
Project Name
Principal
Investigator & Department
Funding Source
Funding
Period
Amount Total Award
Amount 2011- 2012
Amount 2012- 2013
Amount 2013- 2014
CB Y/N
SP Y/N
Systolic Pressure Intervention Trial
(SPRINT)
(PI) A. Cheung – Internal Medicine
Nephrology, Lisa Gren
National Institute of
Health
2009- 2018
$14,920,804 $43,381 $54,526 $56,160 N N
Physical Activity and Pelvic Health
(PI) Ingrid Nygaard, Ob/Gyn,
(Co I) Marlene Egger
National Institute of
Health
4/2008- 3/2013
$97,111 $24,825 $18,757 0 N Y
Coalition of a Healthier Community for Utah
Women and Girls (UWAG)
(PI) Sara Simonsen
Department of Health and
Human Services
1/2011- 8/2016
$1,500,000 $24,400 $32,880 $32,880 Y Y
Summary Totals
$23,179,179 $139,884 $168,957 $131,107
*CB means Community Based and SP means student participation. Shading indicates primary faculty involvement other than PI or Co I.
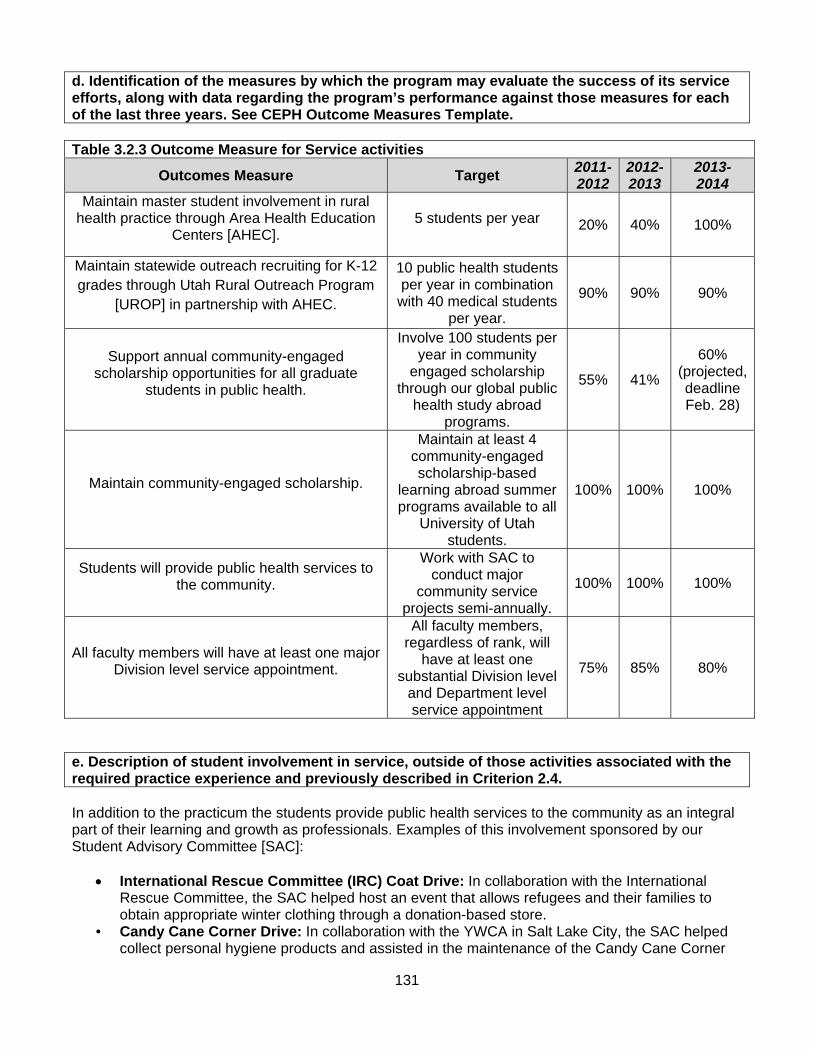
131
d. Identification of the measures by which the program may evaluate the success of its service efforts, along with data regarding the program’s performance against those measures for each of the last three years. See CEPH Outcome Measures Template.
Table 3.2.3 Outcome Measure for Service activities
Outcomes Measure Target 2011- 2012
2012-2013
2013- 2014
Maintain master student involvement in rural health practice through Area Health Education
Centers [AHEC]. 5 students per year 20% 40% 100%
Maintain statewide outreach recruiting for K-12 grades through Utah Rural Outreach Program
[UROP] in partnership with AHEC.
10 public health students per year in combination with 40 medical students
per year.
90% 90% 90%
Support annual community-engaged scholarship opportunities for all graduate
students in public health.
Involve 100 students per year in community
engaged scholarship through our global public
health study abroad programs.
55% 41%
60% (projected, deadline Feb. 28)
Maintain community-engaged scholarship.
Maintain at least 4 community-engaged scholarship-based
learning abroad summer programs available to all
University of Utah students.
100% 100% 100%
Students will provide public health services to the community.
Work with SAC to conduct major
community service projects semi-annually.
100% 100% 100%
All faculty members will have at least one major Division level service appointment.
All faculty members, regardless of rank, will
have at least one substantial Division level
and Department level service appointment
75% 85% 80%
e. Description of student involvement in service, outside of those activities associated with the required practice experience and previously described in Criterion 2.4. In addition to the practicum the students provide public health services to the community as an integral part of their learning and growth as professionals. Examples of this involvement sponsored by our Student Advisory Committee [SAC]:
International Rescue Committee (IRC) Coat Drive: In collaboration with the International Rescue Committee, the SAC helped host an event that allows refugees and their families to obtain appropriate winter clothing through a donation-based store.
• Candy Cane Corner Drive: In collaboration with the YWCA in Salt Lake City, the SAC helped collect personal hygiene products and assisted in the maintenance of the Candy Cane Corner

132
store, a donations-based store that the YWCA holds yearly around the holidays to allow their clients to shop for their families at no cost.
• UWAG Health Fair Interviews: In collaboration with the Utah Women and Girls Coalition, the SAC assisted in establishing a health fair and conducted survey interviews of attendees to gain a better understanding of gender roles in health behaviors.
• Division of Public Health Blood Drive: in recognition of National Public Health Week, the SAC hosted a blood drive for the School of Medicine.
• 4th Street Triathlon: The SAC helped organize this event, which is a fundraiser for the 4th Street Clinic in Salt Lake City, which provides medical care to homeless and impoverished individuals.
• Volunteer tutoring: The SAC committee worked with current students who volunteered their time to help tutor other students
• The Home Observation of Periconceptional Exposures (HOPE) collaborates with the Center for Human Toxicology in the College of Pharmacy, Division of Andrology and Carol Sweeney from Medicine.
f. Assessment of the extent to which this criterion is met and an analysis of the program’s strengths, weaknesses and plans relating to this criterion. This criterion is met. Strengths: As the Division of Public Health continues to mature, more opportunities arise for impact-driven service. Our faculty, staff, and students are actively engaged in service that is consistent with our mission. As our expertise becomes more recognized, invitations and opportunities are forthcoming that facilitate the provision of high quality service that complements our education and research missions. Weaknesses: None noted. Plans: Maintain a service ethic and continue to seek opportunities that allow for high quality service balanced with our research and education mission.
133
3.3 Workforce Development. The program shall engage in activities other than its offering of degree programs that support the professional development of the public health workforce.
a. Description of the ways in which the program periodically assesses the continuing education needs of the community or communities it intends to serve. The assessment may include primary or secondary data collection or data sources. The Division of Public Health established the Office of Public Health Practice (OPHP) in 2010 to assure a more focused approach to workforce development. Assessment of the continuing education needs of the public health workforce was among our top priorities, which included: (1) training needs assessment, (2) training development and delivery, (3) training evaluation, and (4) meaningful engagement with stakeholders. As such, OPHP works to assess knowledge, competence, training needs, and preferred training delivery methods among public health workers in Utah and Nevada. In August 2010, we joined with the University of California Los Angeles, Fielding School of Public Health (UCLA) to form the Southwest Regional Public Health Training Center (SRPHTC). This collaboration enhanced our ability to systematically assess training needs and to develop additional competency sets by which to assess needs in various specialty areas (Health education, environmental health, and epidemiology). All assessment activities were based on the Council on Linkages Core Public Health Competencies.
Since that time, the Division of Public Health has completed several needs assessments and built capacity to continue periodic assessment of continuing education needs. Input from representatives in Utah and Nevada’s state and local health departments was gathered in a variety of ways and are described below.
Local Health Officer Interviews - Key informant interviews were conducted with agency leaders in 92% of the local health departments in the state of Utah between July 2011 and January 2012. The context of these interviews were to: (1) build on existing relationships with health department administration; and, (2) to discuss their workforce composition, current training and methods, training needs/topics, delivery preferences, and recruitment/retention. Results of these discussions were published as an OPHP report and shared with the local health officers in Utah in January 2012. The full results of this survey can be found in the Appendix 3.3A.
Outputs: Face to Face meetings held with 10 of Utah’s 12 local health officers at their location “An Assessment of Utah’s Local Health Departments’ Training Needs” Verbal presentation of results at statewide local health officer meeting: January 19, 2012
Local Health Officer Survey - Health officers in Utah were also asked to complete a perceived needs assessment of their staff. A hard copy of this assessment was made available to health officers in January 2012, and an online version that went live shortly thereafter. Local health officers were asked to rate the competence of their Tier I and Tier II staff in the Council on Linkages Core Competencies for Public Health Professionals, and the importance of these competencies to specific job types. Seven of 12 (58%) health officers completed the assessment.
Outputs: Online assessment tool (REDCap survey) for use by upper level leadership at health
departments about employee needs
Nevada Workforce Needs Assessment Meeting - Training needs among Nevada’s workforce were assessed through a summit meeting we convened on May 31, 2012 in Reno with state and local health officials. These needs have been recorded in the minutes and served as a basis for the work pursued
134
through the Utah-Nevada Public Health Workforce Alliance, which we established based on assessment findings.
Outputs: Relationships developed via face to face meeting with 8 representatives from Nevada’s state and
local health departments and public health academic programs Documentation of training needs via meeting minutes
Local Health Department Employee Knowledge-based survey - A competency-based needs assessment was conducted at the Davis County Health Department in northern Utah in May – June 2012. Three knowledge-based needs assessment tools developed previously by the SRPHTC team were used, depending on the professional level of the employee: (1) Public Health Professional, (2) Public Health Foundations, and (3) Health Educator. The majority (64%) took the Foundations assessment and is considered to be pre-Tier I to Tier II professionals, while 25% took the Professional assessment and are considered to be Tier II to Tier III professionals. An aggregate report and individual reports for each employee were provided to the agency. This particular activity has resulted in further consultation with the Davis County Health Department on implementation strategies for both workforce development and a training plan. We plan to use a similar training framework for other state and local agencies across the state of Utah.
Outputs: 53 employees assessed Three Survey instruments developed: Foundations, Professional, and Health education Manuscript prepared for publication on the Foundations assessment tool Based on the results, input was provided to the local health department regarding their training
and development plan Utah-Nevada Public Health Workforce Alliance – In 2012 we initiated the Utah-Nevada Public Health Workforce Alliance with stakeholders from both academia and practice. The development of this alliance was modeled after the California Public Health Alliance for Workforce Excellence (CPHAWE). The purpose of the alliance is to create and maintain quality in the public health workforce in both states through a coordinated effort. The Utah-Nevada Public Health Workforce Alliance includes representation from state and local health agencies in Utah and Nevada, the Utah Public Health Association, the Nevada Public Health Association, the Nevada Public Health Foundation, the University of Utah, Brigham Young University, the University of Nevada-Reno, and the University of Nevada-Las Vegas. Next steps include seeking additional stakeholders from the region and prioritizing specific aims and activities.
Outputs: Two preliminary meetings held May 31, 2012 and October 5, 2012 and an inaugural meeting
held January 28, 2013 Organizational capacity to set regional workforce development priorities and pursue collaborative
projects Relationships developed via face to face meeting with representatives from 16 public health
organizations across Utah and Nevada Meeting minutes
135
b. A list of the continuing education programs, other than certificate programs, offered by the program, including number of participants served, for each of the last three years. As part of our collaboration with SRPHTC, we have offered several continuing education programs. This has included both face-to-face and distance-based training, in addition to the creation of a Learning Management System (LEARN) that houses additional web-based training. Emerging Leader Workshop Series The Emerging Leader Workshop Series is designed to address the need for leadership training for mid-level personnel in the face of a diminishing and a retiring workforce. All workshops are designed for public health professionals working in public health agencies, academic institutions, and/or non-profit organizations. The series is taught in face-to-face workshop settings in Utah and California locations and covers 12 important management and leadership topics. To date, we have developed and delivered the first six topics from the list below. All sessions are evaluated, including satisfaction and an assessment of knowledge gained.
Developing the Leader in You Understanding Public Health Systems and Change Stakeholders and Strategic Partnerships: Working with Community Partners Effective Strategic Planning Successful Grant Proposal Writing Ethical Decision Making Effective Program Management Practical Evaluation Time and Self-Management Finance and Budgeting Effective Communication Managing Change
Public Health Grand Rounds and Global Public Health Grand Rounds Additionally, the Division of Public Health holds monthly Public Health Grand Rounds and Global Public Health Grand Rounds where invited presenters lecture on their research or related public health work. OPHP has recently started to broadcast these presentations and have made them available to view in real-time in a distance-based format and are archived for later viewing. The UDOH also shows these sessions live at the health department each month for interested employees. Archived videos will soon be available to view on the OPHP website, which is currently in development. Learning Management System (LEARN) Through our partnership with SRPHTC, we have developed a LEARN which features knowledge-based Needs Assessments and allows participants to independently track their learning progress. Web-based or self-study training are also available to registered users. New training is currently in development and is continually being added to the LEARN Library. Training topics available include:
Public Health 101: Principles of Public Health Public Health Nursing Training Set Emergency Preparedness Training Set Public Health Law Ethical Decision-making in Public Health
Rapidly Conducting Community Health Needs Assessments We also conducted a distance-based series in partnership with the Utah Department of Health to provide just-in-time training regarding Qualitative Research Methods for Rapidly Conducting Community
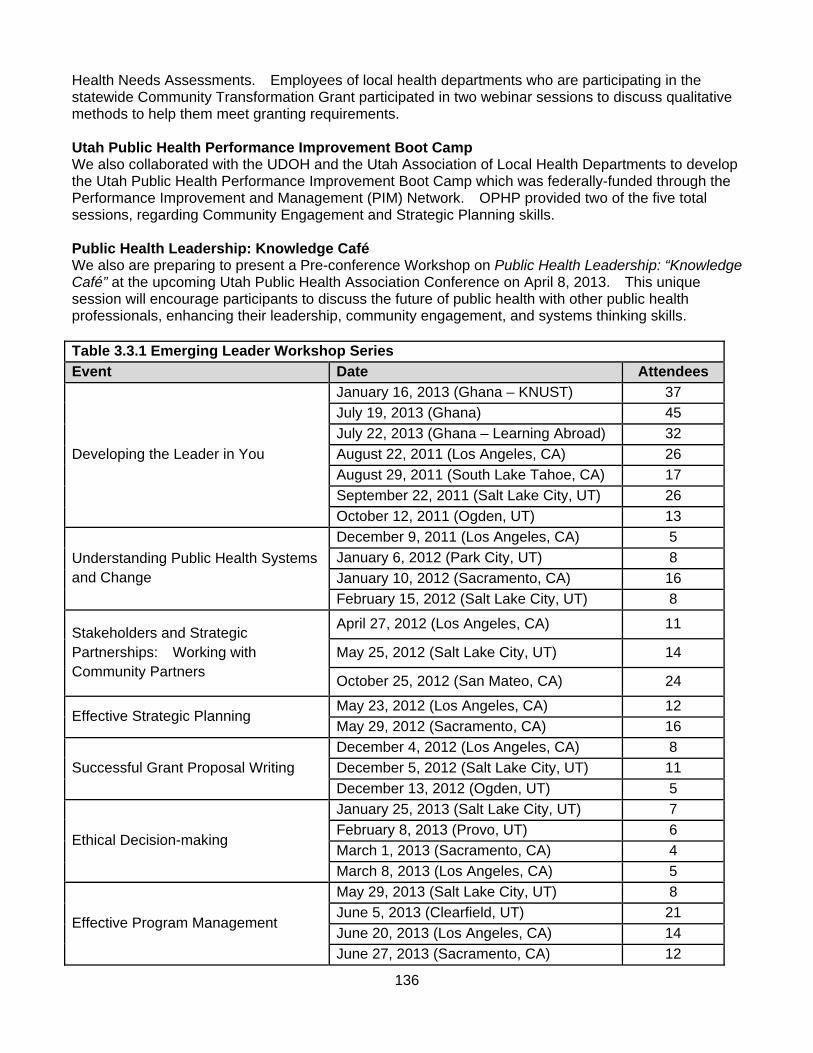
136
Health Needs Assessments. Employees of local health departments who are participating in the statewide Community Transformation Grant participated in two webinar sessions to discuss qualitative methods to help them meet granting requirements. Utah Public Health Performance Improvement Boot Camp We also collaborated with the UDOH and the Utah Association of Local Health Departments to develop the Utah Public Health Performance Improvement Boot Camp which was federally-funded through the Performance Improvement and Management (PIM) Network. OPHP provided two of the five total sessions, regarding Community Engagement and Strategic Planning skills. Public Health Leadership: Knowledge Café We also are preparing to present a Pre-conference Workshop on Public Health Leadership: “Knowledge Café” at the upcoming Utah Public Health Association Conference on April 8, 2013. This unique session will encourage participants to discuss the future of public health with other public health professionals, enhancing their leadership, community engagement, and systems thinking skills. Table 3.3.1 Emerging Leader Workshop Series
Event Date Attendees
Developing the Leader in You
January 16, 2013 (Ghana – KNUST) 37
July 19, 2013 (Ghana) 45
July 22, 2013 (Ghana – Learning Abroad) 32
August 22, 2011 (Los Angeles, CA) 26
August 29, 2011 (South Lake Tahoe, CA) 17
September 22, 2011 (Salt Lake City, UT) 26
October 12, 2011 (Ogden, UT) 13
Understanding Public Health Systems and Change
December 9, 2011 (Los Angeles, CA) 5
January 6, 2012 (Park City, UT) 8
January 10, 2012 (Sacramento, CA) 16
February 15, 2012 (Salt Lake City, UT) 8
Stakeholders and Strategic Partnerships: Working with Community Partners
April 27, 2012 (Los Angeles, CA) 11
May 25, 2012 (Salt Lake City, UT) 14
October 25, 2012 (San Mateo, CA) 24
Effective Strategic Planning May 23, 2012 (Los Angeles, CA) 12
May 29, 2012 (Sacramento, CA) 16
Successful Grant Proposal Writing
December 4, 2012 (Los Angeles, CA) 8
December 5, 2012 (Salt Lake City, UT) 11
December 13, 2012 (Ogden, UT) 5
Ethical Decision-making
January 25, 2013 (Salt Lake City, UT) 7
February 8, 2013 (Provo, UT) 6
March 1, 2013 (Sacramento, CA) 4
March 8, 2013 (Los Angeles, CA) 5
Effective Program Management
May 29, 2013 (Salt Lake City, UT) 8
June 5, 2013 (Clearfield, UT) 21
June 20, 2013 (Los Angeles, CA) 14
June 27, 2013 (Sacramento, CA) 12
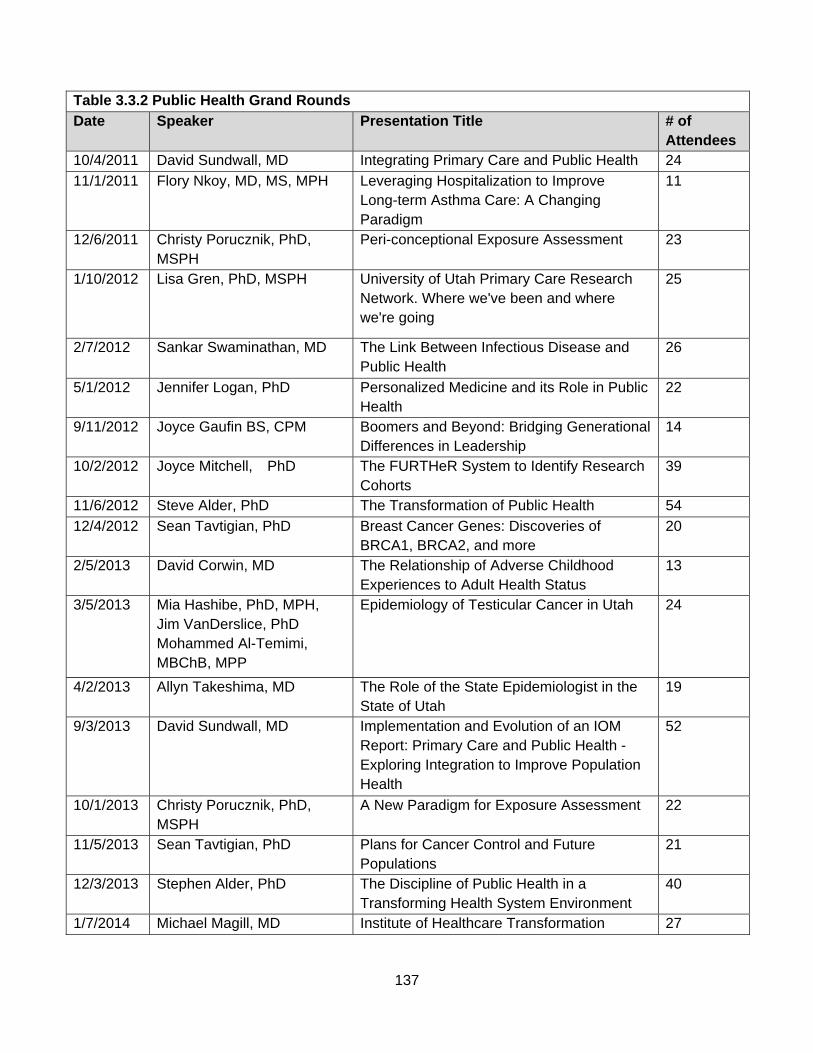
137
Table 3.3.2 Public Health Grand Rounds
Date Speaker Presentation Title # of Attendees
10/4/2011 David Sundwall, MD Integrating Primary Care and Public Health 24
11/1/2011
Flory Nkoy, MD, MS, MPH
Leveraging Hospitalization to Improve Long-term Asthma Care: A Changing Paradigm
11
12/6/2011 Christy Porucznik, PhD, MSPH
Peri-conceptional Exposure Assessment 23
1/10/2012 Lisa Gren, PhD, MSPH University of Utah Primary Care Research Network. Where we've been and where we're going
25
2/7/2012
Sankar Swaminathan, MD
The Link Between Infectious Disease and Public Health
26
5/1/2012 Jennifer Logan, PhD Personalized Medicine and its Role in Public Health
22
9/11/2012
Joyce Gaufin BS, CPM
Boomers and Beyond: Bridging Generational Differences in Leadership
14
10/2/2012 Joyce Mitchell, PhD The FURTHeR System to Identify Research Cohorts
39
11/6/2012 Steve Alder, PhD The Transformation of Public Health 54
12/4/2012 Sean Tavtigian, PhD Breast Cancer Genes: Discoveries of BRCA1, BRCA2, and more
20
2/5/2013 David Corwin, MD The Relationship of Adverse Childhood Experiences to Adult Health Status
13
3/5/2013
Mia Hashibe, PhD, MPH, Jim VanDerslice, PhD Mohammed Al-Temimi, MBChB, MPP
Epidemiology of Testicular Cancer in Utah
24
4/2/2013 Allyn Takeshima, MD The Role of the State Epidemiologist in the State of Utah
19
9/3/2013
David Sundwall, MD
Implementation and Evolution of an IOM Report: Primary Care and Public Health - Exploring Integration to Improve Population Health
52
10/1/2013 Christy Porucznik, PhD, MSPH
A New Paradigm for Exposure Assessment 22
11/5/2013 Sean Tavtigian, PhD Plans for Cancer Control and Future Populations
21
12/3/2013 Stephen Alder, PhD The Discipline of Public Health in a Transforming Health System Environment
40
1/7/2014 Michael Magill, MD Institute of Healthcare Transformation 27
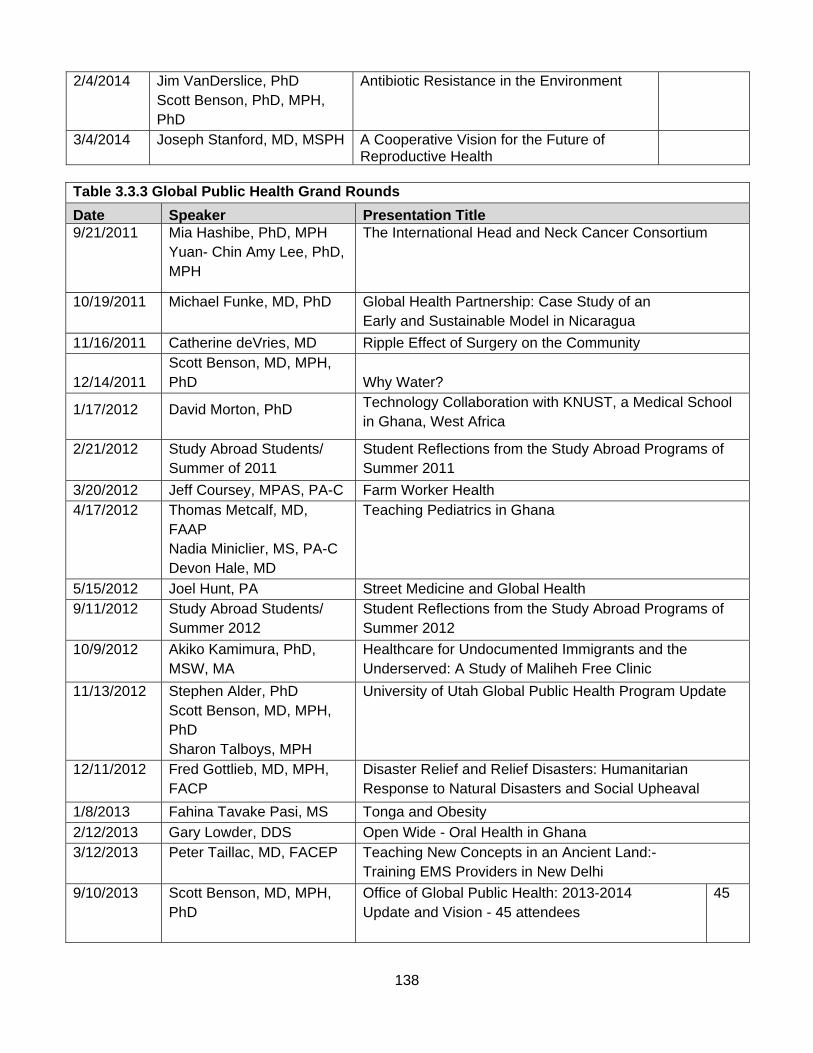
138
2/4/2014
Jim VanDerslice, PhD Scott Benson, PhD, MPH, PhD
Antibiotic Resistance in the Environment
3/4/2014 Joseph Stanford, MD, MSPH A Cooperative Vision for the Future of Reproductive Health
Table 3.3.3 Global Public Health Grand Rounds
Date Speaker Presentation Title 9/21/2011 Mia Hashibe, PhD, MPH
Yuan- Chin Amy Lee, PhD, MPH
The International Head and Neck Cancer Consortium
10/19/2011 Michael Funke, MD, PhD Global Health Partnership: Case Study of an Early and Sustainable Model in Nicaragua
11/16/2011 Catherine deVries, MD Ripple Effect of Surgery on the Community
12/14/2011 Scott Benson, MD, MPH, PhD Why Water?
1/17/2012
David Morton, PhD
Technology Collaboration with KNUST, a Medical School in Ghana, West Africa
2/21/2012
Study Abroad Students/ Summer of 2011
Student Reflections from the Study Abroad Programs of Summer 2011
3/20/2012 Jeff Coursey, MPAS, PA-C Farm Worker Health 4/17/2012
Thomas Metcalf, MD, FAAP Nadia Miniclier, MS, PA-C Devon Hale, MD
Teaching Pediatrics in Ghana
5/15/2012 Joel Hunt, PA Street Medicine and Global Health 9/11/2012
Study Abroad Students/ Summer 2012
Student Reflections from the Study Abroad Programs of Summer 2012
10/9/2012
Akiko Kamimura, PhD, MSW, MA
Healthcare for Undocumented Immigrants and the Underserved: A Study of Maliheh Free Clinic
11/13/2012
Stephen Alder, PhD Scott Benson, MD, MPH, PhD Sharon Talboys, MPH
University of Utah Global Public Health Program Update
12/11/2012 Fred Gottlieb, MD, MPH, FACP
Disaster Relief and Relief Disasters: Humanitarian Response to Natural Disasters and Social Upheaval
1/8/2013 Fahina Tavake Pasi, MS Tonga and Obesity
2/12/2013 Gary Lowder, DDS Open Wide - Oral Health in Ghana 3/12/2013
Peter Taillac, MD, FACEP
Teaching New Concepts in an Ancient Land:- Training EMS Providers in New Delhi
9/10/2013
Scott Benson, MD, MPH, PhD
Office of Global Public Health: 2013-2014 Update and Vision - 45 attendees
45
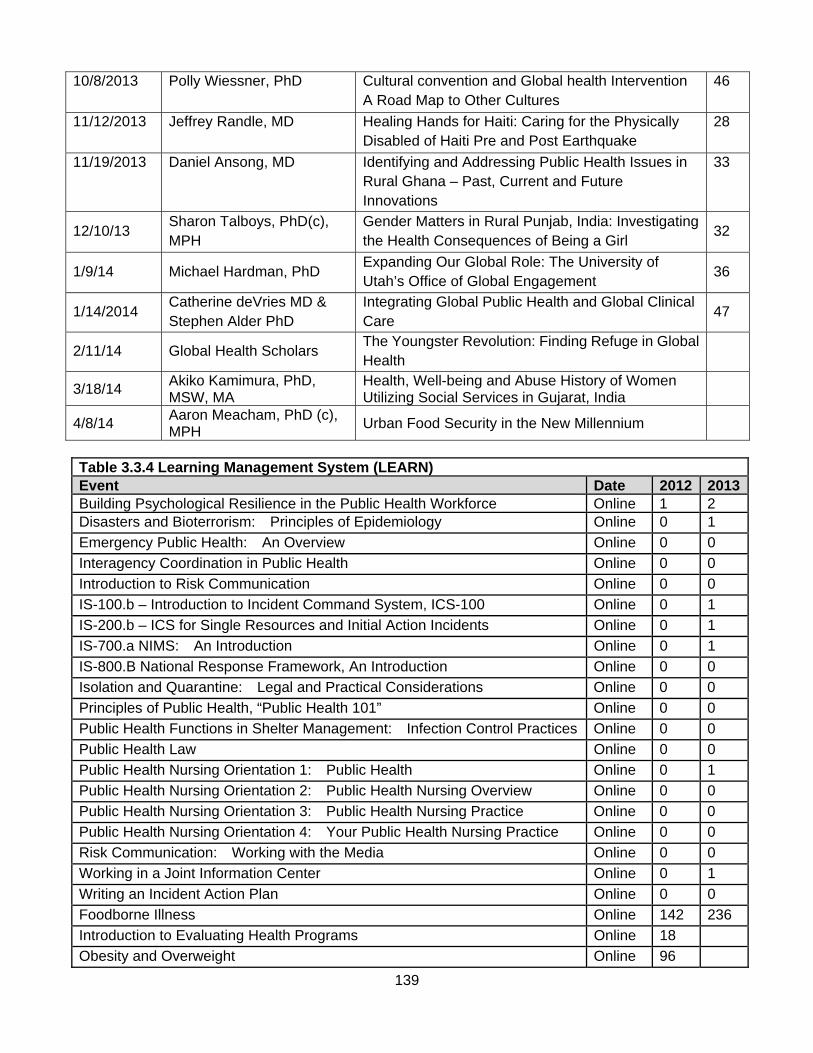
139
10/8/2013
Polly Wiessner, PhD
Cultural convention and Global health Intervention A Road Map to Other Cultures
46
11/12/2013
Jeffrey Randle, MD
Healing Hands for Haiti: Caring for the Physically Disabled of Haiti Pre and Post Earthquake
28
11/19/2013 Daniel Ansong, MD Identifying and Addressing Public Health Issues in Rural Ghana – Past, Current and Future Innovations
33
12/10/13 Sharon Talboys, PhD(c), MPH
Gender Matters in Rural Punjab, India: Investigating the Health Consequences of Being a Girl
32
1/9/14 Michael Hardman, PhD Expanding Our Global Role: The University of Utah’s Office of Global Engagement
36
1/14/2014 Catherine deVries MD & Stephen Alder PhD
Integrating Global Public Health and Global Clinical Care
47
2/11/14 Global Health Scholars The Youngster Revolution: Finding Refuge in Global Health
3/18/14 Akiko Kamimura, PhD, MSW, MA
Health, Well-being and Abuse History of Women Utilizing Social Services in Gujarat, India
4/8/14 Aaron Meacham, PhD (c), MPH
Urban Food Security in the New Millennium
Table 3.3.4 Learning Management System (LEARN) Event Date 2012 2013Building Psychological Resilience in the Public Health Workforce Online 1 2 Disasters and Bioterrorism: Principles of Epidemiology Online 0 1
Emergency Public Health: An Overview Online 0 0
Interagency Coordination in Public Health Online 0 0
Introduction to Risk Communication Online 0 0
IS-100.b – Introduction to Incident Command System, ICS-100 Online 0 1
IS-200.b – ICS for Single Resources and Initial Action Incidents Online 0 1
IS-700.a NIMS: An Introduction Online 0 1
IS-800.B National Response Framework, An Introduction Online 0 0
Isolation and Quarantine: Legal and Practical Considerations Online 0 0
Principles of Public Health, “Public Health 101” Online 0 0
Public Health Functions in Shelter Management: Infection Control Practices Online 0 0
Public Health Law Online 0 0
Public Health Nursing Orientation 1: Public Health Online 0 1
Public Health Nursing Orientation 2: Public Health Nursing Overview Online 0 0
Public Health Nursing Orientation 3: Public Health Nursing Practice Online 0 0
Public Health Nursing Orientation 4: Your Public Health Nursing Practice Online 0 0
Risk Communication: Working with the Media Online 0 0
Working in a Joint Information Center Online 0 1
Writing an Incident Action Plan Online 0 0
Foodborne Illness Online 142 236
Introduction to Evaluating Health Programs Online 18
Obesity and Overweight Online 96
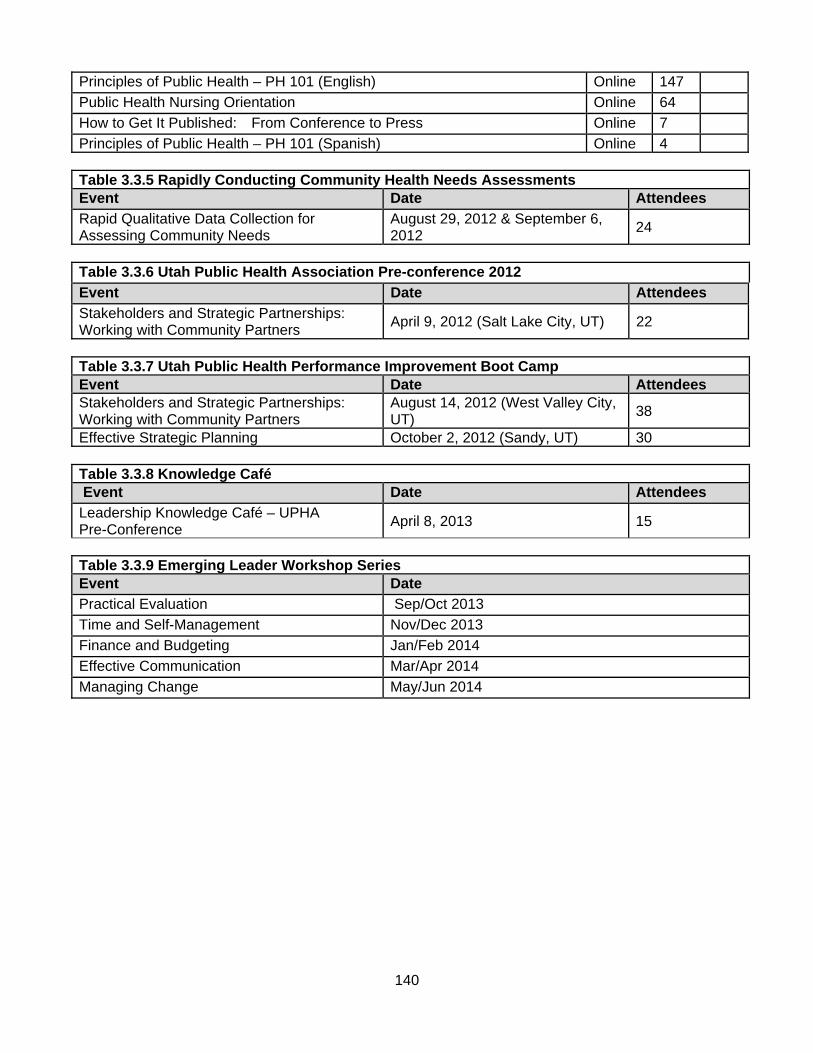
140
Principles of Public Health – PH 101 (English) Online 147
Public Health Nursing Orientation Online 64
How to Get It Published: From Conference to Press Online 7
Principles of Public Health – PH 101 (Spanish) Online 4 Table 3.3.5 Rapidly Conducting Community Health Needs Assessments Event Date Attendees
Rapid Qualitative Data Collection for Assessing Community Needs
August 29, 2012 & September 6, 2012
24
Table 3.3.6 Utah Public Health Association Pre-conference 2012
Event Date Attendees
Stakeholders and Strategic Partnerships: Working with Community Partners
April 9, 2012 (Salt Lake City, UT) 22
Table 3.3.7 Utah Public Health Performance Improvement Boot Camp Event Date Attendees Stakeholders and Strategic Partnerships: Working with Community Partners
August 14, 2012 (West Valley City, UT)
38
Effective Strategic Planning October 2, 2012 (Sandy, UT) 30 Table 3.3.8 Knowledge Café Event Date Attendees
Leadership Knowledge Café – UPHA Pre-Conference
April 8, 2013 15
Table 3.3.9 Emerging Leader Workshop Series Event Date
Practical Evaluation Sep/Oct 2013
Time and Self-Management Nov/Dec 2013
Finance and Budgeting Jan/Feb 2014
Effective Communication Mar/Apr 2014
Managing Change May/Jun 2014
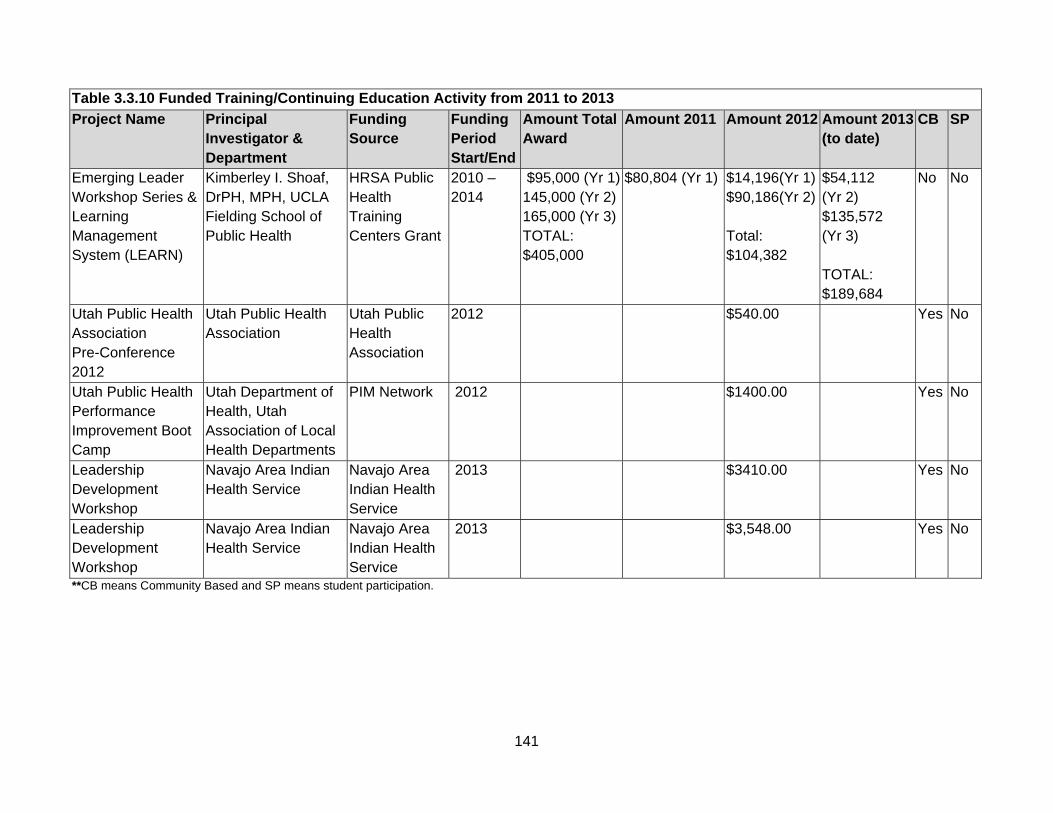
141
Table 3.3.10 Funded Training/Continuing Education Activity from 2011 to 2013
Project Name Principal Investigator & Department
Funding Source
Funding Period Start/End
Amount Total Award
Amount 2011 Amount 2012 Amount 2013 (to date)
CB SP
Emerging Leader Workshop Series & Learning Management System (LEARN)
Kimberley I. Shoaf, DrPH, MPH, UCLA Fielding School of Public Health
HRSA Public Health Training Centers Grant
2010 – 2014
$95,000 (Yr 1) 145,000 (Yr 2) 165,000 (Yr 3) TOTAL: $405,000
$80,804 (Yr 1) $14,196(Yr 1)$90,186(Yr 2) Total: $104,382
$54,112 (Yr 2) $135,572 (Yr 3) TOTAL: $189,684
No No
Utah Public Health Association Pre-Conference 2012
Utah Public Health Association
Utah Public Health Association
2012 $540.00 Yes No
Utah Public Health Performance Improvement Boot Camp
Utah Department of Health, Utah Association of Local Health Departments
PIM Network 2012 $1400.00 Yes No
Leadership Development Workshop
Navajo Area Indian Health Service
Navajo Area Indian Health Service
2013 $3410.00 Yes No
Leadership Development Workshop
Navajo Area Indian Health Service
Navajo Area Indian Health Service
2013 $3,548.00 Yes No
**CB means Community Based and SP means student participation.
142
c. Description of certificate programs or other non-degree offerings of the program, including enrollment data for each of the last three years Qualifications to enroll for each graduate certificate program are the same. If a student meets the admission requirements below they will be accepted into the respective graduate certificate program.
Admission requirements:
1. Have an undergraduate degree from an accredited college with a cumulative 3.0 or better GPA (transcripts may be required).
2. Complete an internal application https://rocky.utah.edu/pubhealth/PH_Certificate_Form.htm. 3. Either:
a. Enrolled in a Graduate Program, for which students must receive permission from their current program to earn the Certificate http://medicine.utah.edu/dfpm/divisionph/PDFs/Cert_Sig_Sheet.pdf or
b. Not enrolled in a graduate program you must apply through the Graduate School http://www.sa.utah.edu/admiss/ as an undergraduate, seeking second bachelors.
Application deadlines are (our deadline may be after the University of Utah and may incur late fees):
Fall admissions is July 1st
Spring admissions is December 1st
Summer admissions is April 1st
Students who wish to transition into the masters in public health degree must go through the regular admissions process in its entirety. Only if a student is admitted into the master of public health program can certificate credits count towards the degree. No special treatment is given to students who complete a certificate. Graduate Certificate in Public Health The Graduate Certificate in Public Health was approved by the Academic Senate Committee February 2012. (http://admin.utah.edu/wp-content/uploads/2012/01/Agenda02_09_2012_v2.pdf) The public health certificate gives students the potential to understand the opportunity and connection public health has in an array of fields such as biostatistics, social behavior, epidemiology, policy and administration and environmental public health through research, service and education. Also the Certificate will provide local professionals working in the field of public health an opportunity to seek training and certification that will directly impact how they address public health issues in their current professions. The following courses are required to earn the public health certificate: FPMD 6100 Biostatistics (3) FPMD 6300 Epidemiology (3) FPMD 6400 Public Health Policy & Administration (3) FPMD 6600 Social Context in Public Health (3) FPMD 6700 Environmental Public Health (3) Total: 15 credits We have admitted 5 students, of which 0 have graduated. Graduate Certificate in Global Health The Graduate Certificate in Global Health was approved by the Academic Senate Committee April 2010. http://admin.utah.edu/wp-content/uploads/2011/09/agenda_2010Apr5.pdf
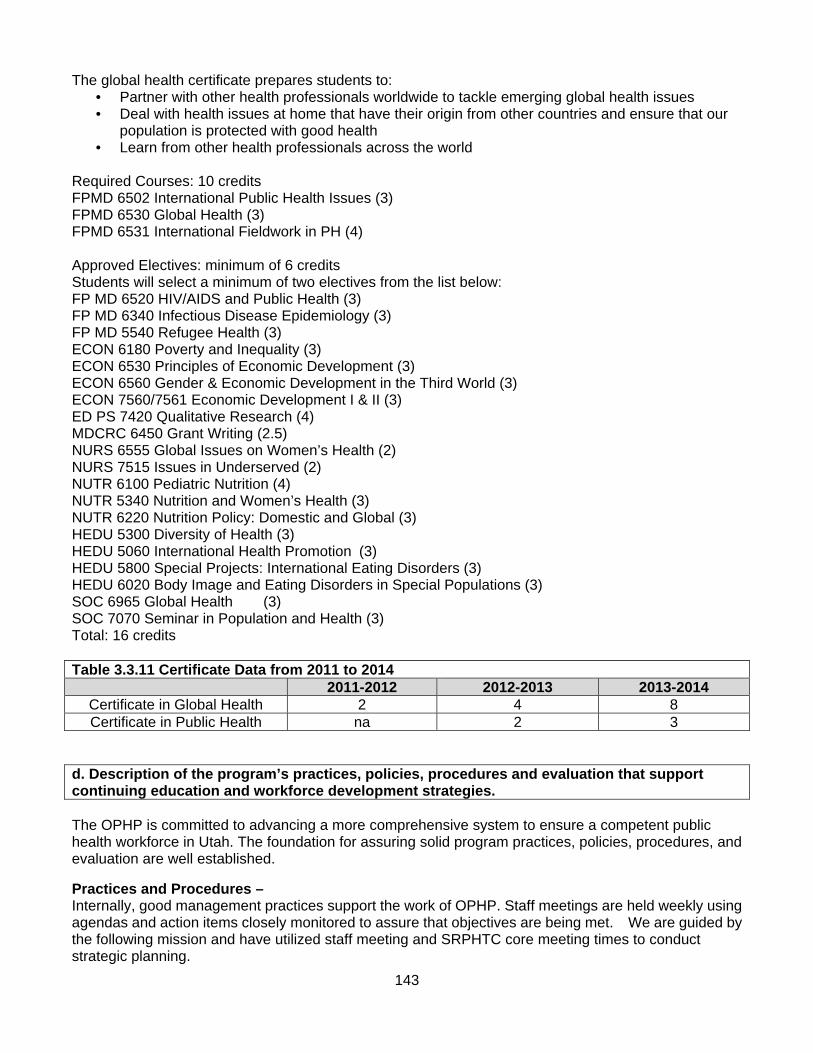
143
The global health certificate prepares students to: • Partner with other health professionals worldwide to tackle emerging global health issues • Deal with health issues at home that have their origin from other countries and ensure that our
population is protected with good health • Learn from other health professionals across the world
Required Courses: 10 credits FPMD 6502 International Public Health Issues (3) FPMD 6530 Global Health (3) FPMD 6531 International Fieldwork in PH (4) Approved Electives: minimum of 6 credits Students will select a minimum of two electives from the list below: FP MD 6520 HIV/AIDS and Public Health (3) FP MD 6340 Infectious Disease Epidemiology (3) FP MD 5540 Refugee Health (3) ECON 6180 Poverty and Inequality (3) ECON 6530 Principles of Economic Development (3) ECON 6560 Gender & Economic Development in the Third World (3) ECON 7560/7561 Economic Development I & II (3) ED PS 7420 Qualitative Research (4) MDCRC 6450 Grant Writing (2.5) NURS 6555 Global Issues on Women’s Health (2) NURS 7515 Issues in Underserved (2) NUTR 6100 Pediatric Nutrition (4) NUTR 5340 Nutrition and Women’s Health (3) NUTR 6220 Nutrition Policy: Domestic and Global (3) HEDU 5300 Diversity of Health (3) HEDU 5060 International Health Promotion (3) HEDU 5800 Special Projects: International Eating Disorders (3) HEDU 6020 Body Image and Eating Disorders in Special Populations (3) SOC 6965 Global Health (3) SOC 7070 Seminar in Population and Health (3) Total: 16 credits Table 3.3.11 Certificate Data from 2011 to 2014
2011-2012 2012-2013 2013-2014 Certificate in Global Health 2 4 8 Certificate in Public Health na 2 3
d. Description of the program’s practices, policies, procedures and evaluation that support continuing education and workforce development strategies. The OPHP is committed to advancing a more comprehensive system to ensure a competent public health workforce in Utah. The foundation for assuring solid program practices, policies, procedures, and evaluation are well established.
Practices and Procedures – Internally, good management practices support the work of OPHP. Staff meetings are held weekly using agendas and action items closely monitored to assure that objectives are being met. We are guided by the following mission and have utilized staff meeting and SRPHTC core meeting times to conduct strategic planning.
144
Our mission is to advance the development of a comprehensive system to ensure a competent public health workforce in public and non-profit organizations in Utah and the Mountain West.
Externally, our collaboration with SRPHTC is enhanced through consistent monthly meetings with the UCLA core team, as well as weekly contact with UCLA on joint projects. We attend the Utah Department of Health’s monthly meeting of their organizational development and performance improvement team, which helps us stay in touch with practical needs at health departments. We are also the convener of the Utah-Nevada Public Health Workforce Alliance.
We facilitate and provide appropriate training and educational opportunities to meet public health workforce needs by:
Identifying and/or creating existing high-quality public health training opportunities available through online sources.
Participating in and supporting training activities conducted by other organizations. Developing and implementing focused training designed to fill critical gaps and respond to
specific requests of public health agencies. Developing and delivering training to prepare emerging leaders in public health. Improving access to graduate-level education and certification in public health through distance
education. Providing graduate-level public health education that prepares students to meet the needs of
public health agencies. We strategically develop systems that apply continuous quality improvement principles to workforce development. All training offered by OPHP is formally evaluated. All grand rounds are evaluated through post-training questionnaires, and all workshops are evaluated with pre- and post-test questionnaires. In terms of program evaluation, we consistently set goals, such as number of trainings to offer, number of people to reach, rating of the quality of training provided, and demographic information to assure we are reaching a diverse audience. e. A list of other educational institutions or public health practice organizations, if any, with which the program collaborates to offer continuing education. Utah Public Health Association - As a collaborator with the Utah Public Health Association (UPHA), we have been an active member on its conference planning committee and have presented at the UPHA annual conference—in both pre-conference, breakout sessions, and exhibitor. Additionally, we have contributed as advisors to the UPHA Student Caucus which seeks opportunities for mentorship between students and public health professionals. We have a staff member who co-chairs the 2013 Utah Public Health Association conference and aim to assure annual representation on this committee. The UPHA conference is a primary source of continuing education for Utah public health professionals. Nevada Public Health Association - We have also participated in the Nevada Public Health Association conference as presenters and exhibitors. Utah Department of Health and the Utah Association of Local Health Departments - We have collaborated with the UDOH and the Utah Association of Local Health Departments to develop the Performance Improvement Boot Camp which was federally-funded through the PIM Network. We participate on their advisory council and present topics (Community Engagement and Strategic Planning) during the series. In addition, we serve as an advisor to the Office of Organizational Development and Performance Improvement at UDOH, which assesses state-level training needs. We have also provided just-in-time training regarding qualitative data collection methods for UDOH and local health departments participating with Utah’s Community Transformation Grant (funded through the Centers for Disease Control and Prevention).

145
Various health departments hosted training - We have partnered with UDOH, Weber-Morgan, Summit County, Davis County, Utah County, and Salt Lake County Health Departments to host sessions of our ELWS. Various health departments and hospitals hosted interns - We have also partnered with Davis County Health Department, Allen Memorial/Moab Regional Hospital, Beaver Valley Hospital, and Milford Valley Memorial Hospital to place students in a summer practicum experience. Area Health Education Centers – We also collaborate with Utah Area Health Education Centers (AHEC) to provide housing and logistical support for students participating in rural field placements. f. Assessment of the extent to which this criterion is met and an analysis of the program’s strengths, weaknesses and plans relating to this criterion. This criterion is met. Strengths: OPHP has been successful in meeting its goals and objectives, as well as the activities required in the SRPHTC collaboration. Our Emerging Leader Workshop Series has presented six topics over the last two years, which have been well received—as reported by participants’ evaluations. This office is active and effective. Its strengths include collaborative and profitable partnerships where mutual needs of both parties have been met. For example, our partnerships with UDOH and Utah’s local health departments have led to additional plans to study the Utah public health system and the services it provides. Based on our success, we have been invited to submit a full proposal to the Robert Wood Johnson Foundation to fund this project. Weaknesses: Because workforce development is a prominent and significant issue in the public health system today, there isn’t much OPHP could do. However, due to limited resources in key personnel and available funding, OPHP is limited in the number of opportunities we can accept or to which we can provide acceptable service. Plan: Thus to continue the success of OPHP, we plan to employ additional staff to support the office’s future activities. We plan to broaden our activities to include development of additional web-based training courses (available on LEARN), installment of a completely distance-based Certificate in Public Health for working professionals, full operation of the Utah-Nevada Public Health Workforce Alliance, formation of a Public Health Leadership Institute to serve public health professionals in Utah and Nevada, and further research into Utah’s public health services and system.
146
4.0 Faculty, Staff and Students 4.1 Faculty Qualifications. The program shall have a clearly defined faculty which, by virtue of its distribution, multidisciplinary nature, educational preparation, practice experience and research and instructional competence, is able to fully support the program’s mission, goals and objectives.
a. A table showing primary faculty who support the degree programs offered by the program.
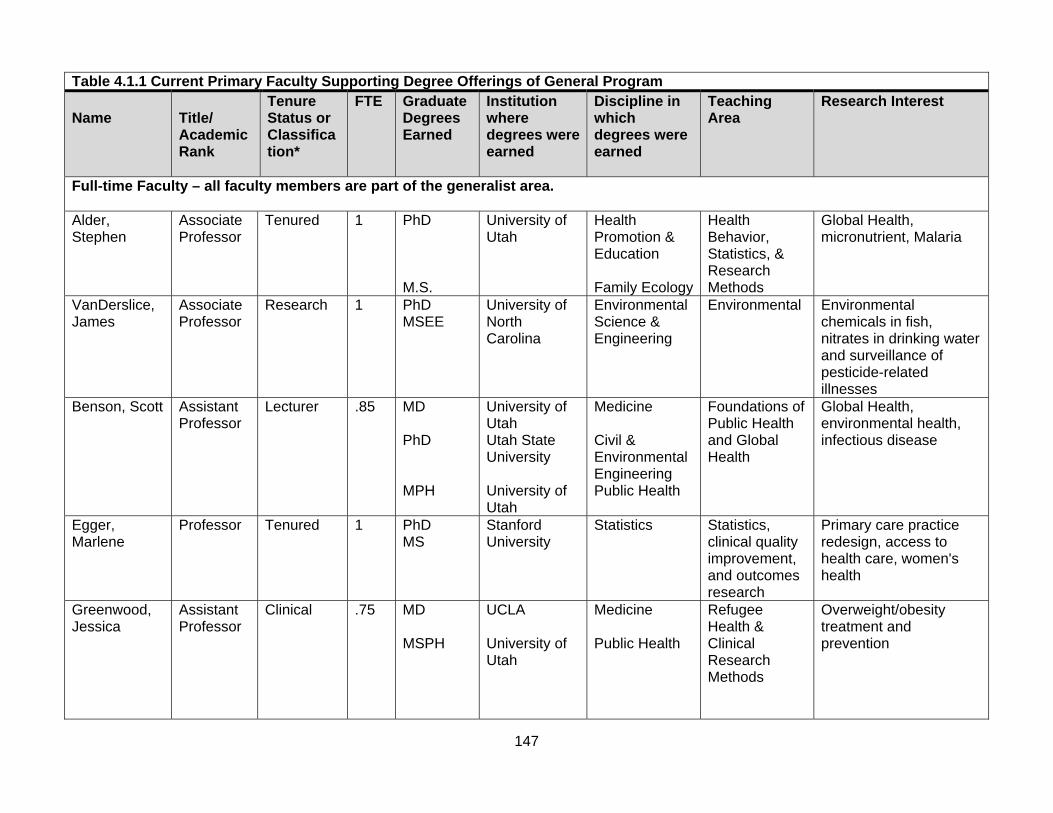
147
Table 4.1.1 Current Primary Faculty Supporting Degree Offerings of General Program Name
Title/ Academic Rank
Tenure Status or Classification*
FTE Graduate Degrees Earned
Institution where degrees were earned
Discipline in which degrees were earned
Teaching Area
Research Interest
Full-time Faculty – all faculty members are part of the generalist area. Alder, Stephen
Associate Professor
Tenured 1 PhD M.S.
University of Utah
Health Promotion & Education Family Ecology
Health Behavior, Statistics, & Research Methods
Global Health, micronutrient, Malaria
VanDerslice, James
Associate Professor
Research 1 PhD MSEE
University of North Carolina
Environmental Science & Engineering
Environmental Environmental chemicals in fish, nitrates in drinking water and surveillance of pesticide-related illnesses
Benson, Scott Assistant Professor
Lecturer .85 MD PhD MPH
University of Utah Utah State University University of Utah
Medicine Civil & Environmental Engineering Public Health
Foundations of Public Health and Global Health
Global Health, environmental health, infectious disease
Egger, Marlene
Professor Tenured 1 PhD MS
Stanford University
Statistics Statistics, clinical quality improvement, and outcomes research
Primary care practice redesign, access to health care, women's health
Greenwood, Jessica
Assistant Professor
Clinical .75 MD MSPH
UCLA University of Utah
Medicine Public Health
Refugee Health & Clinical Research Methods
Overweight/obesity treatment and prevention
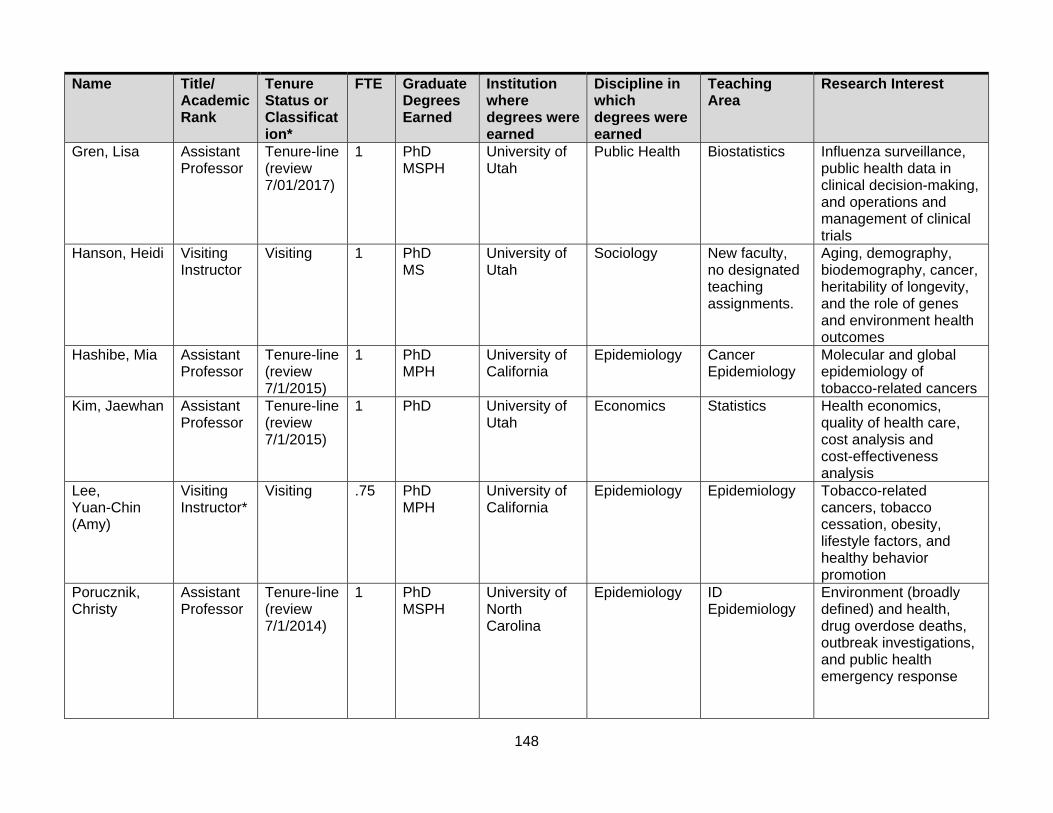
148
Name Title/ Academic Rank
Tenure Status or Classification*
FTE Graduate Degrees Earned
Institution where degrees were earned
Discipline in which degrees were earned
Teaching Area
Research Interest
Gren, Lisa Assistant Professor
Tenure-line (review 7/01/2017)
1 PhD MSPH
University of Utah
Public Health Biostatistics Influenza surveillance, public health data in clinical decision-making, and operations and management of clinical trials
Hanson, Heidi Visiting Instructor
Visiting 1 PhD MS
University of Utah
Sociology New faculty, no designated teaching assignments.
Aging, demography, biodemography, cancer, heritability of longevity, and the role of genes and environment health outcomes
Hashibe, Mia Assistant Professor
Tenure-line (review 7/1/2015)
1 PhD MPH
University of California
Epidemiology Cancer Epidemiology
Molecular and global epidemiology of tobacco-related cancers
Kim, Jaewhan Assistant Professor
Tenure-line (review 7/1/2015)
1 PhD University of Utah
Economics Statistics Health economics, quality of health care, cost analysis and cost-effectiveness analysis
Lee, Yuan-Chin (Amy)
Visiting Instructor*
Visiting .75 PhD MPH
University of California
Epidemiology Epidemiology Tobacco-related cancers, tobacco cessation, obesity, lifestyle factors, and healthy behavior promotion
Porucznik, Christy
Assistant Professor
Tenure-line (review 7/1/2014)
1 PhD MSPH
University of North Carolina
Epidemiology ID Epidemiology
Environment (broadly defined) and health, drug overdose deaths, outbreak investigations, and public health emergency response

149
Name Title/ Academic Rank
Tenure Status or Classification*
FTE Graduate Degrees Earned
Institution where degrees were earned
Discipline in which degrees were earned
Teaching Area
Research Interest
Simonsen, Sara
Visiting Instructor*
Visiting .62 PhD CMN MSPH
University of Utah
Public Health Nursing Public Health
Epidemiology Community-based wellness coaches for the prevention of obesity in diverse underserved communities, preterm birth, & infertility
Stanford, Joseph
Professor Tenured 1 MD MSPH
University of Minnesota University of Missouri
Medicine Public Health
Advanced Research Design
Family planning, & infertility
Sundwall, David
Professor Clinical .54 MD University of Utah
Medicine Social Context & Policy & Administration
Healthcare policy & advocacy
Wu, Yelena Assistant Professor
Tenure-line (review 7/1/2019)
.83 PhD MA
University of Kansas
Clinical Child Psychology
Health Behavior
Pediatric chronic illness self-management and adherence to medical regimens
*Visiting Instructors are considered full-time employees by the University of Utah.
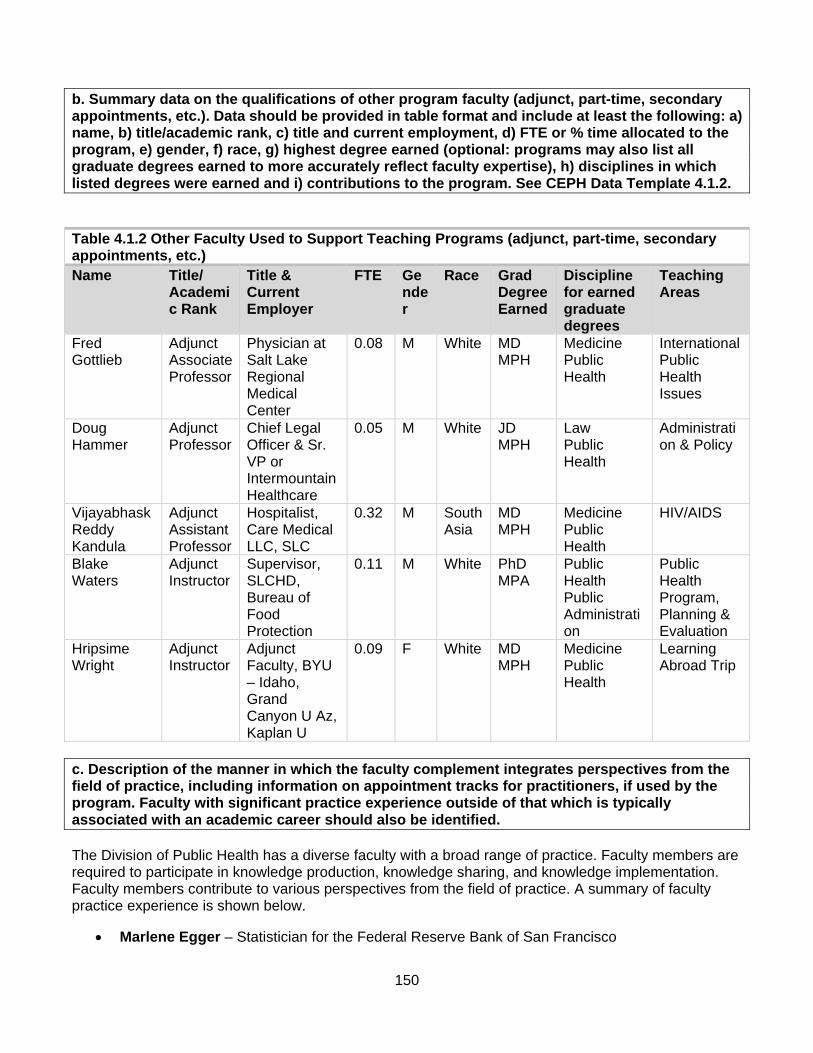
150
b. Summary data on the qualifications of other program faculty (adjunct, part-time, secondary appointments, etc.). Data should be provided in table format and include at least the following: a) name, b) title/academic rank, c) title and current employment, d) FTE or % time allocated to the program, e) gender, f) race, g) highest degree earned (optional: programs may also list all graduate degrees earned to more accurately reflect faculty expertise), h) disciplines in which listed degrees were earned and i) contributions to the program. See CEPH Data Template 4.1.2. Table 4.1.2 Other Faculty Used to Support Teaching Programs (adjunct, part-time, secondary appointments, etc.) Name Title/
Academic Rank
Title & Current Employer
FTE Gender
Race Grad Degree Earned
Discipline for earned graduate degrees
Teaching Areas
Fred Gottlieb
Adjunct Associate Professor
Physician at Salt Lake Regional Medical Center
0.08 M White MD MPH
Medicine Public Health
International Public Health Issues
Doug Hammer
Adjunct Professor
Chief Legal Officer & Sr. VP or Intermountain Healthcare
0.05 M White JD MPH
Law Public Health
Administration & Policy
Vijayabhask Reddy Kandula
Adjunct Assistant Professor
Hospitalist, Care Medical LLC, SLC
0.32 M South Asia
MD MPH
Medicine Public Health
HIV/AIDS
Blake Waters
Adjunct Instructor
Supervisor, SLCHD, Bureau of Food Protection
0.11 M White PhD MPA
Public Health Public Administration
Public Health Program, Planning & Evaluation
Hripsime Wright
Adjunct Instructor
Adjunct Faculty, BYU – Idaho, Grand Canyon U Az, Kaplan U
0.09 F White MD MPH
Medicine Public Health
Learning Abroad Trip
c. Description of the manner in which the faculty complement integrates perspectives from the field of practice, including information on appointment tracks for practitioners, if used by the program. Faculty with significant practice experience outside of that which is typically associated with an academic career should also be identified. The Division of Public Health has a diverse faculty with a broad range of practice. Faculty members are required to participate in knowledge production, knowledge sharing, and knowledge implementation. Faculty members contribute to various perspectives from the field of practice. A summary of faculty practice experience is shown below.
Marlene Egger – Statistician for the Federal Reserve Bank of San Francisco
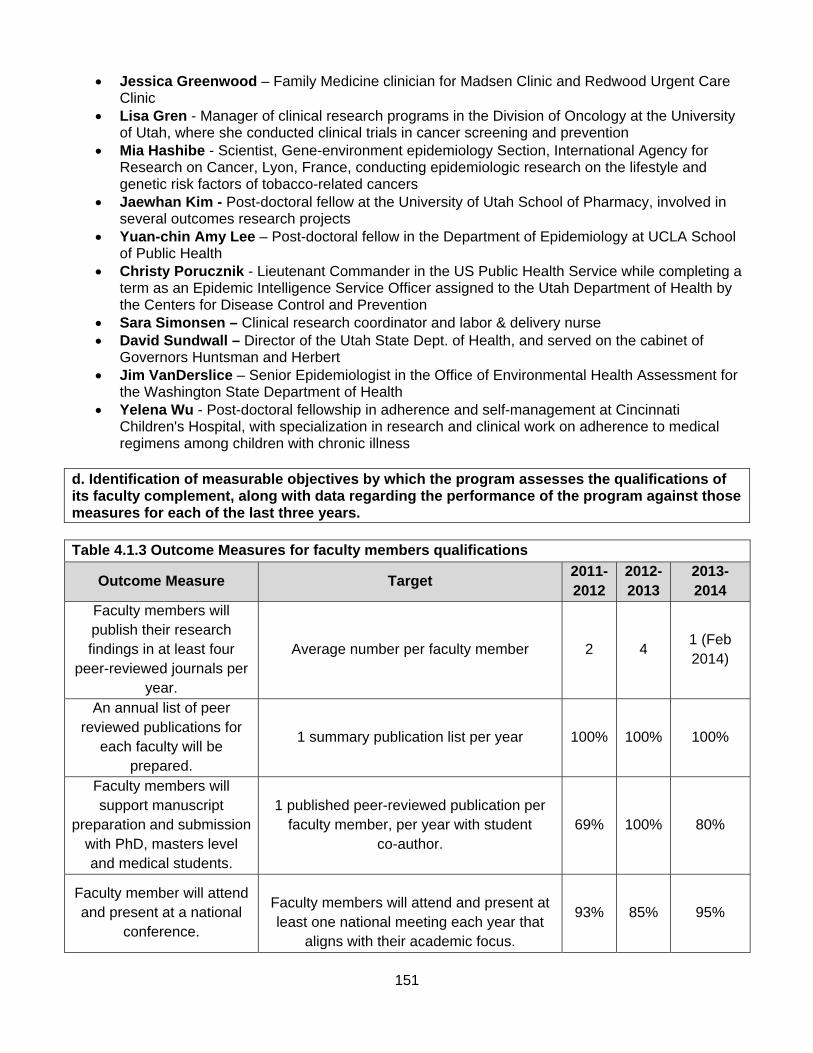
151
Jessica Greenwood – Family Medicine clinician for Madsen Clinic and Redwood Urgent Care Clinic
Lisa Gren - Manager of clinical research programs in the Division of Oncology at the University of Utah, where she conducted clinical trials in cancer screening and prevention
Mia Hashibe - Scientist, Gene-environment epidemiology Section, International Agency for Research on Cancer, Lyon, France, conducting epidemiologic research on the lifestyle and genetic risk factors of tobacco-related cancers
Jaewhan Kim - Post-doctoral fellow at the University of Utah School of Pharmacy, involved in several outcomes research projects
Yuan-chin Amy Lee – Post-doctoral fellow in the Department of Epidemiology at UCLA School of Public Health
Christy Porucznik - Lieutenant Commander in the US Public Health Service while completing a term as an Epidemic Intelligence Service Officer assigned to the Utah Department of Health by the Centers for Disease Control and Prevention
Sara Simonsen – Clinical research coordinator and labor & delivery nurse David Sundwall – Director of the Utah State Dept. of Health, and served on the cabinet of
Governors Huntsman and Herbert Jim VanDerslice – Senior Epidemiologist in the Office of Environmental Health Assessment for
the Washington State Department of Health Yelena Wu - Post-doctoral fellowship in adherence and self-management at Cincinnati
Children's Hospital, with specialization in research and clinical work on adherence to medical regimens among children with chronic illness
d. Identification of measurable objectives by which the program assesses the qualifications of its faculty complement, along with data regarding the performance of the program against those measures for each of the last three years. Table 4.1.3 Outcome Measures for faculty members qualifications
Outcome Measure Target 2011-2012
2012-2013
2013- 2014
Faculty members will publish their research findings in at least four
peer-reviewed journals per year.
Average number per faculty member 2 4 1 (Feb 2014)
An annual list of peer reviewed publications for
each faculty will be prepared.
1 summary publication list per year 100% 100% 100%
Faculty members will support manuscript
preparation and submission with PhD, masters level and medical students.
1 published peer-reviewed publication per faculty member, per year with student
co-author. 69% 100% 80%
Faculty member will attend and present at a national
conference.
Faculty members will attend and present at least one national meeting each year that
aligns with their academic focus.
93% 85% 95%

152
Outcome Measure
Target
2011-2012
2012-2013
2013- 2014
Each faculty member is actively involved in at least
1 project that formally engages at least one other
discipline.
List project and other discipline 75% 100% 100%
Faculty members will participate and present research in at least one University of Utah forum
each year to insure intra-institutional
networking.
All faculty members will participate and present research in at least one University of
Utah scholarly forum annually. 69% 92% 69%
Maintain scholarly-productive
community collaboration to ensure emphasis in community-engaged
scholarship.
Expect all faculty members to be formally engaged in at least one scholarly-productive community collaboration to ensure emphasis
in community-engaged scholarship. (Reference File, Faculty CV)
56% 85% 80%
Annual faculty reviews ensure academic focus alignment with teaching
responsibility.
Faculty members meet with Division Chief once a year to review teaching expectations
and expertise. 100% 100% 100%
Students recognize expertise as illustrated by
faculty members knowledge of the subject.
Course evaluations reflect that 80% of the faculty demonstrated thorough knowledge of
the subject (Appendix 1.2A, Surveys line 1.1).
96% 97% 94%
Course and faculty evaluations are reviewed
by the Division Chief at the end of every semester.
If courses overall rating falls below 80%, a specific plan is developed which includes;
using course evaluations to guide correcting of deficiencies and instructors are provided guidance from the Center for Teaching and
Learning Excellence (CTLE) (Appendix 1.2A, Surveys lines 1.3).
94% 93% 88%
Faculty members will present their research results in grand rounds (minimum of 3 faculty members per year)
(source: faculty CVs)
3 faculty members will present in grand rounds per year per series, Public Health
and Global Public Health. 100% 100% 100%
All faculty members will have Division and
Department service
All faculty members, regardless of rank, will have at least one substantial Division level and Department level service appointment.
75% 85% 80%
On average all faculty members will have
community public health service appointment.
On average, all faculty members will have at least one community public health service
appointment. 44% 54% 47%
153
e. Assessment of the extent to which this criterion is met and an analysis of the program’s strengths, weaknesses and plans relating to this criterion.
This criterion is met. Strengths: We have grown our core faculty, since our last Self Study,. Our faculty has a growing breadth and depth of knowledge that facilitates successful accomplishment of our mission. Courses are taught by faculty members with in depth expertise in subject matter, our research capacity has grown due in part to the competitiveness of our faculty expertise, and students are better aligned with faculty members with expertise in their areas of interest. Weaknesses: Growth and transitions in our faculty has resulted in a high proportion of junior faculty members at the instructor and assistant professor ranks. Mentoring and career development have been challenging because of this high proportion of junior faculty. Plans: We have increased our mentoring activities by becoming more proactive with our internal mentoring, and by accessing external resources. We continue to work with junior faculty members to help protect their time by limiting service obligations and providing funds to assist in developing research activities. We are also working on linking them to institutional resources for career development, and prioritizing recruitment of mid-career faculty members as future hiring opportunities arise.

154
4.2 Faculty Policies and Procedures. The program shall have well-defined policies and procedures to recruit, appoint and promote qualified faculty, to evaluate competence and performance of faculty, and to support the professional development and advancement of faculty. a. A faculty handbook or other written document that outlines faculty rules and regulations. The faculty handbook contains links to policies and procedures that apply to faculty appointments at the University of Utah, as well as additional information about the University, its campus, and surroundings that may be of interest to the faculty. The Faculty Handbook provides faculty members with direct links to University policies and other sources of information, many of which are located online on University web pages or are provided by departmental and collegiate administrative offices. http://admin.utah.edu/faculty-handbook b. Description of provisions for faculty development, including identification of support for faculty categories other than regular full-time appointments. The University of Utah School of Medicine mission statement on faculty development is as follows: “To help faculty chart a course for career success, in the areas of teaching, clinical care, scholarship, and administration.” The Office of Faculty Administration oversees and supports faculty development for the School of Medicine (http://medicine.utah.edu/facultyadmin/index.htm). They provide workshops on faculty mentoring and professional development, oversee the Faculty Club with various social events. Additional resources for faculty development, which are available to all faculty members including part time faculty, are shown below.
Human resource training and development. The Human Resources Training & Development
Department is committed to helping the faculty and staff to cultivate the skills and knowledge necessary for success by providing numerous professional learning opportunities. The Training and Development Department has workshops on management essentials, professional development, onsite trainings, facilitations and inclusion in the workplace. Faculty professional development workshop topics include ‘Working with challenging students’, ‘How to run a meeting’, ‘Taking care of yourself’, ‘Leading change’, “Working with international students’, ‘Expanding your classroom’, ‘Writing effective letters of recommendation’, ‘Time management’. https://www.hr.utah.edu/training/
Center for Teaching and Learning Excellence provides a wide range of services to support classroom and on-line teaching and learning excellence
Financial and Business Services for financial management resources for Business Officers, Principal Investigators, Deans, and Department Directors
Human Resources – Training and Development (University, Health Sciences, excluding Hospitals, and Clinics) provides a range of workshops for faculty, staff, and post docs, meeting and retreat facilitations and customized training options
University Healthcare – Education and Development provide a range of workshops and services to support staff in university hospitals and clinics
Office of Equity and Diversity has resources to support faculty and students on the main campus
The Mentoring network for faculty, staff, post docs, and students http://research.utah.edu/mentoring/
University Training Consortium is a campus wide organization which brings together training professionals and the range of classes available at the university
Women in Medicine and Science (WIMS) Program is sponsored by the Dean, School of Medicine, and Faculty Administration. The goal of the program is to bring women faculty,
155
residents, and students together for networking, and to provide programs to assist in their professional and personal development
Research Education provides professional development opportunities for all faculty, staff, postdoctoral scholars and members of the University research community
Continuing Education offers credit, noncredit, and professional courses covering a wide range of topics from art to sports to writing. Areas within Continuing Education include Lifelong Learning, Independent Study, Telecourses, Youth Education, Preparatory Courses, Professional Education and Certificate Programs, the English Language Institute, and Technology Education, as well as credit courses
Staff Diversity provides hiring managers with tools and resources for the recruitment of diverse applicant pools for staff positions. It is also intended to inform staff of the University opportunities available to them through University offices and committees, including Human Resources as they identify and pursue their individual career goals. http://staffdiversity.utah.edu/
The Lowell Bennion Community Service Center fosters lifelong service and civic participation by engaging the university with the greater community in action, change and learning http://bennioncenter.org/about/index.php
Intramural funding opportunities are available for faculty to apply for seed grants, research instrumentation, creative awards, and community based research grants
c. Description of formal procedures for evaluating faculty competence and performance. Within the School of Medicine appointment, promotion retention and tenure guidelines are established to assure that the School of Medicine appropriately recognizes the contributions made by individual members of the faculty. The following points clarify the School of Medicine guidelines: Faculty members are appointed through a process directed by the School of Medicine. The appointment process is designed to assess appropriateness for hire only. Subsequent formal reviews for RPT are performed according to guidelines that are distinct from the appointment process. All faculty members, except those on the research track, are expected to teach and bear some of the administrative burden in the School of Medicine. Some faculty positions are eligible for tenure and some are not. Only one tenure track exists. Faculty members in the tenure track are described by University regulations as “Regular Faculty.” The School of Medicine recognizes two types of tenure track faculty positions that can be differentiated by the amount of time and effort devoted to the clinical mission. The two types of tenure generating positions are called “scientist-scholars” and “clinician-scholars.” The non-tenure generating faculty positions are designated “clinical”, “research”, and “lecturer”, and are encompassed by the term “Auxiliary Faculty” in University regulations. The School of Medicine RPT Committee will consider the relative time and effort spent on the scholarship mission of the School when evaluating the scholarly attainment of an individual. This consideration will involve the volume of scholarship produced, the impact of the scholarship produced, and the type of scholarship produced. The scientist-scholars are expected to produce a greater volume of scholarship, a greater impact of scholarship, and a more tightly defined type of scholarship than the clinician-scholar and the clinical faculty member. Moreover, the scientist-scholars are expected to be Principal Investigator of extramurally funded grants and/or contracts. The clinician-scholar (is similarly expected to produce a greater volume of scholarship, a greater impact of scholarship, and a more tightly refined type of scholarship than the clinical faculty member.
156
Review Promotion and Tenure (RPT) http://medicine.utah.edu/facultyadmin/rpt/criteria/ http://medicine.utah.edu/facultyadmin/rpt/overview.htm Within the Division of Public Health the formal procedure for evaluating faculty competence and performance is annual with the Division Chief. The annual review between the faculty member and Division Chief includes the letter that goes out to all faculty members letting them know what they need to bring to this meeting, Appendix 4.2A. During this meeting they discuss those items as part of that review, and then that review is formalized at the designated steps of Faculty Administration and Retention, Promotion, and Tenure. This is designed so that this annual review will make sure faculty members are on pace for success for the next formal review and that any concerns or deficiency as well as opportunities for success are assessed on a more regular basis so that early intervention can be intimated. d. Description of the processes used for student course evaluation and evaluation of instructional effectiveness. CTLE (http://ctle.utah.edu/scf/instructors.php) manages the student course feedback program to incorporate the student perspective into its services to improve instruction at the University of Utah. While student course feedback is not a stand-alone measure of teaching effectiveness, it can be a valuable resource for identifying teaching strengths and areas for improvement. CTLE has created a comprehensive resource for instructors regarding the student course feedback program. The information has been organized into three sections, corresponding to the time periods before evaluations begin, during the evaluation session, and after evaluations are complete when feedback reports become available. CTLE also provides instructor consultations and observations on an individual basis. They offer consultations before, during, and after each semester. They offer observations of teaching throughout the semester. Instructors benefit from individual consultations regarding their syllabus, lesson plans, rubrics, or other class materials. Additionally, instructors can request CTLE's in-class observations and/or mid-semester student feedback to obtain feedback that is very rewarding and valuable for their individual teaching strategies and goals. Within the Division, the chief reads each evaluation of each class, every semester. The teaching evaluations are also reviewed during the annual review meetings between the Division Chief and individual faculty member. The areas of evaluation are: objectives clearly stated, objectives met, content well-organized, course materials helpful, assignments and exams covered the course, learned a great deal, overall effective course, instructor was organized, instructor presented effectively, instructor created respectful environment, instructor demonstrated thorough knowledge, instructor encouraged questions/opinions, and over effective instructor. Students responses range from strongly disagree, disagree, mild disagree, mild agree, agree, and strongly agree.
157
e. Assessment of the extent to which this criterion is met and an analysis of the program’s strengths, weaknesses and plans relating to this criterion. This criterion is met. Strengths: Policies, procedures, and operational guidelines related to the conditions of the employment are established and available to all faculty members. Retention, promotion, and tenure criteria are also available. Faculty development is supported via numerous departments and organizations within the University. The annual faculty review provides a thorough review of each faculty member’s career focus and aspirations compared against past, current, and future activities. This review also checks the progression of each faculty member through the retention, promotion, and tenure process. Weaknesses: None noted. Plans: Continue to actively support faculty development by close monitoring of the policies, procedures, and practices. We are also working closely with our Faculty Administration office to insure that our support of effective faculty recruitment and development. In the School of Medicine it is important for us to ensure that the needs of the public health faculty members are considered as policy advances and procedures are updated. Part of our working closely with faculty administration is to ensure that any updates continue to make this an attractive place for recruitment of qualified new faculty members and that this process is designed to facilitate successful retention and promotion of faculty members.

158
4.3 Student Recruitment and Admissions. The program shall have student recruitment and admissions policies and procedures designed to locate and select qualified individuals capable of taking advantage of the program’s various learning activities, which will enable each of them to develop competence for a career in public health.
a. Description of the program’s recruitment policies and procedures. If these differ by degree (eg, bachelor’s vs. graduate degrees), a description should be provided for each. The Division distributes newsletters (Appendix 4.3A) and frequently asked questions (FAQ) (Appendix 4.3B), which includes admission requirements, sample coursework outlines, and faculty research projects for specific degrees. Academic Advisors respond to numerous telephone, e-mail, and written requests for information. Information on the webpage is updated and serves as a resource for both current and prospective students to find the most current program guidelines and information. We are currently revising our entire webpage and hope to have a more informative and user friendly site by spring 2014. MSPH. All accepted students are initially admitted into our MPH program, and once they have completed some coursework, usually a semester or two, and have a Division of Public Health faculty member sign on as their mentor to a specific research project, and have a started a research project, they can then request to transfer into the MSPH program. Faculty members and staff connect with other universities within Utah (i.e. BYU, Utah State University, Weber State University, Utah Valley State University, Southern Utah University, etc.) as well an nationally where applicants who are interested in a graduate degree in public health are recruited. The Academic Advisors exhibit/recruit during the following: American Public Health Association (APHA) – APHA is the oldest and most diverse organization of public health professionals in the world and has been working to improve public health since 1872. The Association aims to protect all Americans, their families and their communities from preventable, serious health threats and strives to assure community-based health promotion and disease prevention activities and preventive health services are universally accessible in the United States. APHA represents a broad array of health professionals and others who care about individual health and the health of communities. Utah Public Health Association Conference (UPHA) – UPHA is a leader in public health advocacy, improving public health practice, and providing professional development opportunities for members and the public health community. Founded in 1916, UPHA is the largest public health organization in Utah and is an affiliate of the American Public Health Association. Our members include public health professionals, health educators, doctors, nurses, community leaders, and citizens committed to improving the health of Utahns. Utah Graduate School Fair – We exhibit with several other programs across the State of Utah. Brigham Young University (BYU) Global Family Health and Development Conference – The Global Family Health and Development Conference focuses on current solutions and best practices that can be used by families and communities to address the multi-dimensional aspects of poverty. Participants learn about new family and community-based solutions and interventions, plus leading local, national, and global experts share perspectives related to issues such as building self-reliance through education, women's empowerment, and economic development; addressing hunger; and understanding health equity and the social determinants of health.
159
b. Statement of admissions policies and procedures. If these differ by degree (eg, bachelor’s vs. graduate degrees), a description should be provided for each. Decisions are based on an evaluation of the applicant’s:
Pre-Requisites – o Masters - college algebra (1050) or equivalent with a grade of B or better is required. A
course in statistics is highly recommend, but not required. o PhD – students entering the doctoral program without an accredited Master of Public
Health or Master of Science in Public Health degree will be required to complete, with the minimum grade of B-, the course work covering the five core areas identified by CEPH (Epidemiology I, Biostatistics I, Social Context of Medicine and Public Health, Environmental Public Health, and Public Health Policy and/or Public Health Administration).
Transcripts, GPA – Undergraduate and graduate grades of at least a cumulative 3.0. o **It is necessary for a candidate with an undergraduate GPA below 3.0 to also submit a
justification letter. This letter should detail why the candidate's GPA is lower than 3.0 and why they feel that they are prepared to pursue the Public Health degree in spite of their lower GPA. This letter is different than the Statement of Purpose and will be included with the candidates application file. **
General Graduate Record Examination (GRE) – Performance on the GRE is an important indicator of a student's ability to be successful in graduate study. (school code 4853, department code 0616). Although we do not have a minimum GRE score the goal for master applicants is verbal and quantitative in the 40% and an analytical score 3.5. For doctoral applicants verbal and quantitative in the 60% and analytical score of 3.5.
o Masters applicants without a terminal degree (MD or PhD) earned in the U.S. must submit the GRE, scores older than 5 years will not be considered. The MCAT scores may be substituted only if the applicant has been accepted into
the University of Utah medical school and plans to seek the MD/MPH. The Medical school letter of acceptance must be attached to MCAT scores.
o All PhD applicants must submit General Test of the GRE, scores older than 10 years, will not be considered, no exceptions.
TOEFL scores. International students – must submit TOEFL scores. We use the guidelines of the University of Utah for the minimum TOEFL scores of 80 iBT (550 pBT) or better, or a minimum IELTS band score of 6.5 or better.
Three letters of recommendation – required for each masters or PhD applicant. o The recommendation letters should come from persons familiar with the applicant's
academic and professional capabilities, achievements, work experience, and/or personal qualities, not family or friends. There is no specific format for these letters.
Statement of Purpose – The statement should include comments relevant to public health degree(s), reasons for choosing public health as a future career area, any previous relative work experience, and how the training will facilitate the student’s career goals.
o Masters not to exceed 500 words o PhD not to exceed 1000 words
If appropriate, copies of an applicant's publication abstracts should be included in the Writing Sample-Essay-Publication section.
Personal interview may be required, including international applicants. Telephone interviews may be conducted and will be considered on a case-by-case basis.
PhD applicants must also submit a Curriculum Vitae (CV) Self-Identify a faculty mentor – Doctoral applicants must identify a faculty mentor from within the
Division of Public Health
160
The process for evaluating applications has several steps. The fall and summer deadline for applicants is February 1 and for spring applicants it is October 1. Incomplete or late applications are not considered. The transcripts are processed, the GPA is determined, and the degree information is verified by the Graduate Admission Office. Once an online Application is submitted the Division prints the application packet and enters it into the database. As the Academic Advisor reviews the applications they will contact each applicant who has an incomplete file, informing them of what is missing and working with them to complete the file before the deadline. Formal review of the applications begins mid-February. Given faculty constraints on time it has been helpful to have the Admission Committee review the competed applications for those who meet the program goals. The Admission Committee provides recommendation on each application to the rest of the Division faculty. Actions that can be taken are to ‘admit’, ‘deny’, ‘interview’ or defer the decision. The number of applicants admitted is dependent on multiple factors, including current student enrollment, number of graduates, anticipated funding, and the number and capacity of Division faculty. Applicants are notified via e-mail that the Division has recommended their acceptance to the University. An official letter of acceptance is sent from the University Admissions office and posted through the students Apply Yourself account. The university defers to the program for recommendations, and although could overrule the program to date has not done so. Students who are rejected will receive an e-mail from the Division and a posting to their online application account. Denied Students are welcome to discuss the decision with the Academic Advisor and/or Admissions Chair. Joint degree students must apply to each degree program separately, and must be admitted into each program separately before beginning the joint degree program. Students are held to each individual degree programs admissions process and requirements it is possible for a student to be admitted into one program and not the other. c. Examples of recruitment materials and other publications and advertising that describe, at a minimum, academic calendars, grading and the academic offerings of the program. If a program does not have a printed bulletin/catalog, it must provide a printed web page that indicates the degree requirements as the official representation of the program. In addition, references to website addresses may be included. To view the course catalog visit: https://pia.acs.utah.edu/psc/coursepr/EMPLOYEE/HRMS/c/SA_LEARNER_SERVICES.UU_CTLG_SEARCH.GBL?&term=&subject=FP%20MD On the new webpage we will post videos of the grand rounds, newsletters, degree FAQ’s, and Student project opportunities http://medicine.utah.edu/dfpm/Research/spo.pdf. d. Quantitative information on the number of applicants, acceptances and enrollment, by concentration, for each degree, for each of the last three years. We do not admit students directly into the MSPH program; while the program outline is the same for the MPH and MSPH, we try to ensure that students requesting the MSPH are really interested in research and have talked to a public health faculty member about signing on as their MSPH faculty advisor.
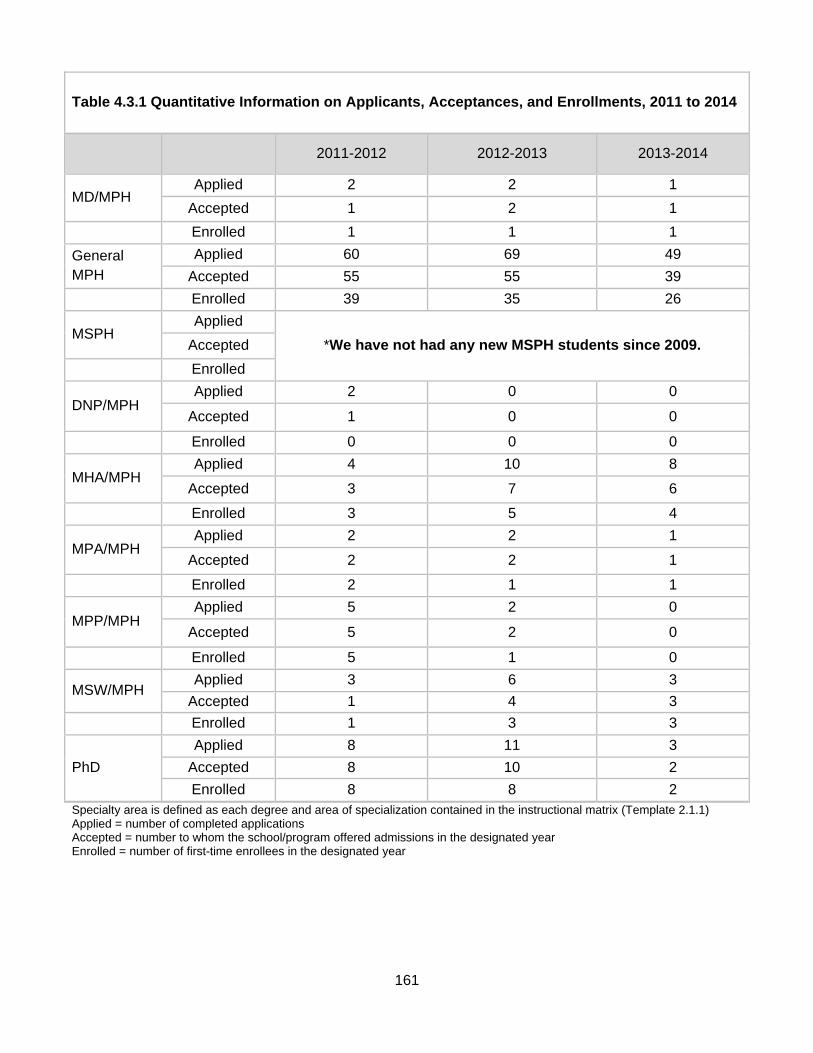
161
Table 4.3.1 Quantitative Information on Applicants, Acceptances, and Enrollments, 2011 to 2014
2011-2012 2012-2013 2013-2014
MD/MPH Applied 2 2 1
Accepted 1 2 1
Enrolled 1 1 1
General MPH
Applied 60 69 49
Accepted 55 55 39
Enrolled 39 35 26
MSPH Applied
*We have not had any new MSPH students since 2009. Accepted
Enrolled
DNP/MPH Applied 2 0 0
Accepted 1 0 0
Enrolled 0 0 0
MHA/MPH Applied 4 10 8
Accepted 3 7 6
Enrolled 3 5 4
MPA/MPH Applied 2 2 1
Accepted 2 2 1
Enrolled 2 1 1
MPP/MPH Applied 5 2 0
Accepted 5 2 0
Enrolled 5 1 0
MSW/MPH Applied 3 6 3
Accepted 1 4 3
Enrolled 1 3 3
PhD
Applied 8 11 3
Accepted 8 10 2
Enrolled 8 8 2 Specialty area is defined as each degree and area of specialization contained in the instructional matrix (Template 2.1.1) Applied = number of completed applications Accepted = number to whom the school/program offered admissions in the designated year Enrolled = number of first-time enrollees in the designated year
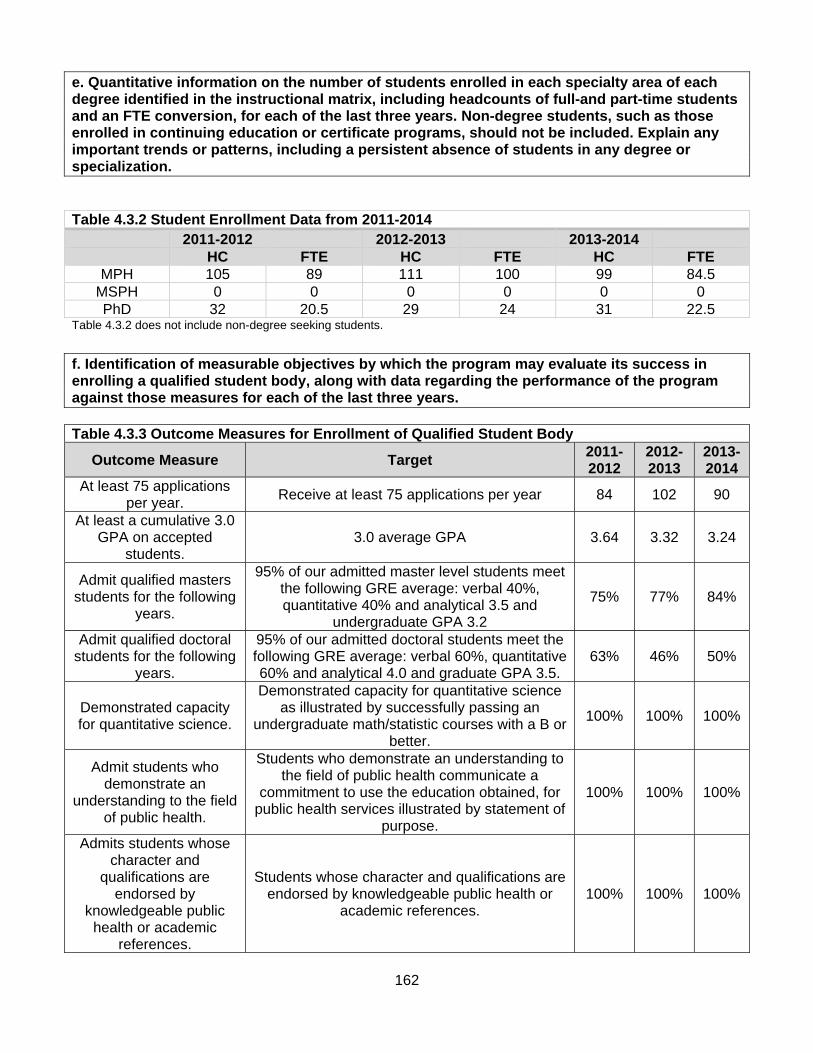
162
e. Quantitative information on the number of students enrolled in each specialty area of each degree identified in the instructional matrix, including headcounts of full-and part-time students and an FTE conversion, for each of the last three years. Non-degree students, such as those enrolled in continuing education or certificate programs, should not be included. Explain any important trends or patterns, including a persistent absence of students in any degree or specialization. Table 4.3.2 Student Enrollment Data from 2011-2014
2011-2012 2012-2013 2013-2014 HC FTE HC FTE HC FTE
MPH 105 89 111 100 99 84.5 MSPH 0 0 0 0 0 0 PhD 32 20.5 29 24 31 22.5
Table 4.3.2 does not include non-degree seeking students.
f. Identification of measurable objectives by which the program may evaluate its success in enrolling a qualified student body, along with data regarding the performance of the program against those measures for each of the last three years. Table 4.3.3 Outcome Measures for Enrollment of Qualified Student Body
Outcome Measure Target 2011-2012
2012-2013
2013-2014
At least 75 applications per year.
Receive at least 75 applications per year 84 102 90
At least a cumulative 3.0 GPA on accepted
students. 3.0 average GPA 3.64 3.32 3.24
Admit qualified masters students for the following
years.
95% of our admitted master level students meet the following GRE average: verbal 40%, quantitative 40% and analytical 3.5 and
undergraduate GPA 3.2
75% 77% 84%
Admit qualified doctoral students for the following
years.
95% of our admitted doctoral students meet the following GRE average: verbal 60%, quantitative 60% and analytical 4.0 and graduate GPA 3.5.
63% 46% 50%
Demonstrated capacity for quantitative science.
Demonstrated capacity for quantitative science as illustrated by successfully passing an
undergraduate math/statistic courses with a B or better.
100% 100% 100%
Admit students who demonstrate an
understanding to the field of public health.
Students who demonstrate an understanding to the field of public health communicate a
commitment to use the education obtained, for public health services illustrated by statement of
purpose.
100% 100% 100%
Admits students whose character and
qualifications are endorsed by
knowledgeable public health or academic
references.
Students whose character and qualifications are endorsed by knowledgeable public health or
academic references. 100% 100% 100%

163
g. Assessment of the extent to which this criterion is met and an analysis of the program’s strengths, weaknesses and plans relating to this criterion. This criterion is met. Strengths: We continue to recruit well-qualified students who are both academically capable and committed to pursuing advanced education in public health. We implement mechanisms by which we can build interest in the discipline of public health and attract potential students to our graduate programs. Weaknesses: As indicated in our self-assessment of diversity, we have not connected effectively with some segments of our community. We currently are experiencing underrepresentation of students of Hispanic/Latino ethnicity and those from rural communities. Plans: We have established our Diversity Committee to proactively seek to achieve diversity reflective of our constituent communities. We also plan to become more proactive about recruitment of students in contrast to the passive recruitment that we have relied on for several years.
164
4.4 Advising and Career Counseling. There shall be available a clearly explained and accessible academic advising system for students, as well as readily available career and placement advice. a. Description of the program’s advising services for students in all degrees and concentrations, including sample materials such as student handbooks. Include an explanation of how faculty are selected for and oriented to their advising responsibilities. When an interested applicant contacts the Division by email or phone, the Academic Advisor answers their immediate questions and talks to them about admission procedures. Follow-up is done by e-mailing a sheet of FAQ’s, which includes a sample worksheet for the particular degree in which they are inquiring, which includes links to the Division website and tuition information. If the interested applicant has more specific questions, they are encouraged to make an appointment so that adequate time is available to meet with them. Before new students start in the program, the Academic Advisor meets with each student individually to review policies, guidelines, deadlines, program webpage navigation, semester schedules, certificates, and how to register when applicable. During that meeting, students are assigned an initial faculty advisor with whom their interest areas align and are reassured the Academic Advisor will be available for their entire program. For those students who do not meet with the Academic Advisor before school starts, they are assigned a faculty member based on availability. Once the student has started the program we continue to encourage meeting with the Academic Advisor, as well as having a faculty mentor whose interests are aligned with their own. If they would like to change their faculty advisor they are allowed to do so, but they need to visit with the Academic Advisor first. Students are encouraged to interact with their faculty advisors as soon as they are accepted into a degree program and then meet regularly thereafter. Faculty members are also asked to meet with their advisees and participate in administrative matters relevant to these students. If a student feels their interest area may be more in-line with a different faculty member than they were assigned, they are encouraged to talk to the new faculty member and ask if they would be their mentor. When the faculty member agrees, either party can let the Academic Advisor know for the official change. Doctoral students are now required before submitting their application to identify and talk to a faculty member who they would potentially like to work with on their dissertation. An orientation for all incoming students is held in August of the academic year. During orientation each student is given an orientation packet which includes topics such as Division structure, requirements, procedures, resources, newsletter, worksheet for their specific degree, and other relevant material as discussed. At the end of orientation we break the students into groups to meet with their faculty advisor for initial introductions. Upon formal acceptance into the Division each student is assigned to a faculty member who serves as his/her initial advisor. By Graduate School requirements, within the first year all students must nominate a committee to provide advising and guidance functions. Usually the person initially assigned as a faculty advisor becomes the chair of the graduate committee (officially labeled ‘Supervisory Committee’). While the Graduate School requires formation of a Supervisory Committee for all graduate students, the extent and scope of advising duties are different for each degree:
For the PhD student, the committee chair is their primary contact for advising and functions to guide the student in choosing elective courses that are relevant to their dissertation. We follow
165
the rules of the University Graduate School as they relate to the Supervisory Committee. “Each supervisory committee consists of five faculty members. The committee chair and the majority of the committee must be regular (tenured or tenure track) faculty in the student’s department. One member of the committee must be appointed from outside the student’s major department. The outside member is normally from another University of Utah department. However, the dean of the Graduate School may approve requests to appoint a committee member from another university where appropriate justification and supporting documentation is provided. The supervisory committee is responsible for approving the student’s academic program, preparing and judging the qualifying examinations, approving the dissertation subject and final dissertation, and administering and judging the final oral examination (dissertation defense).” http://gradschool.utah.edu/graduate-catalog/degree-requirements/
For the MSPH student, a Supervisory Committee not only functions to guide in choice of elective courses (and offer advice on other relevant curricular and career matters), but also to help the student plan and conduct a research project or thesis of publishable quality.
The MPH student Supervisory Committee functions to provide the student with faculty resources to call upon for electives and focused discussions around career issues.
For both the MPH and MSPH we follow the rules of the University Graduate School as they relate to the Supervisory Committee. “Unless otherwise approved by the dean of The Graduate School, a supervisory committee consisting of three faculty members, the majority of whom must be regular (tenured or tenure track) faculty in the student’s major department, is appointed no later than the second semester of graduate work. If a graduate student’s preliminary work is deficient, the supervisory committee may require supplementary undergraduate courses for which no graduate credit is granted.” http://gradschool.utah.edu/graduate-catalog/degree-requirements/
Our goal for graduate students is to meet with his/her Committee or Faculty Advisor at least twice per academic year as a matter of routine; other meetings are arranged as called for by emerging issues. That schedule is not always regularly attained. The Degree Course Worksheet such as Appendix F, K or L has become invaluable in helping the student and advisor plan the student’s academic progression. b. Description of the program’s career counseling services for students in all degree programs. Include an explanation of efforts to tailor services to meet specific needs in the program’s student population. All students receive career counseling form a variety of sources:
FP MD 6500 Foundation of Public Health introduces students to career planning by inviting staff from the University of Utah Career Services to come and present as well as meet with students individually to review resumes, cover letters, or for mock interviews. This course has also implemented a Career Fair for all students at the end of the semester. We invite community partners attend and discuss opportunities for jobs or practicum experiences. We hope to continue to expand this opportunity as it has been well received.
Practicum Mentorship – students not only work with their practicum mentors to earn credit for their practicum but they are also receiving career counseling.
Supervisory Committee/Faculty Advisor – available as resources for discussion on career tracks.
Job Announcements – the Academic Advisor e-mails all job announcements received, posts them on the job board, as well as on the webpage: http://medicine.utah.edu/dfpm/divisionph/current/JobOpportunities/index.htm.

166
c. Information about student satisfaction with advising and career counseling services. Students have had high satisfaction rates with the Academic Advisors. In the past, career counseling has been an area of weakness, and although we have implemented aspects of career counseling services listed above, we still have opportunity for improvement. The latest Alumni survey of 2012, still states improvements can be made. We have created a detailed “Job Opportunity” webpage (http://medicine.utah.edu/dfpm/divisionph/current/JobOpportunities/index.htm) that links to several other career websites. We hope that a more established working relationship between students and their Faculty Advisors will help students receive appropriate career counseling. We have also been in discussion with University of Utah, Career Services about holding a seminar towards the students graduating semester to help them start the job search and let them know what job opportunities are out there. d. Description of the procedures by which students may communicate their concerns to program officials, including information about how these procedures are publicized and about the aggregate number of complaints and/or student grievances submitted for each of the last three years. All students are expected to “adhere to generally accepted standards of academic honesty, including but not limited to refraining from cheating, plagiarizing, research misconduct, misrepresenting one’s work, and/or inappropriately collaborating (The Code of Student Rights and Responsibilities, Policy 6-400).” Such violations are subject to disciplinary action, up to and including expulsion. Please refer to the student code for details on student academic performance action and appeals processes at http://regulations.utah.edu/academics/6-400.php. We have not had any complaints and/or student grievances submitted in the last three years. e. Assessment of the extent to which this criterion is met and an analysis of the program’s strengths, weaknesses and plans relating to this criterion. This criterion is met with commentary. Strengths: Students in the program receive extensive advising services in all degrees and concentrations through courses, Academic Advisors, and Faculty Advisors. Weaknesses: We feel that a lot of students may not be getting all that they could out of the career services experience. Plans: The major step we have taken to address career advising is to transition our Academic Advising Office to an Academic Advising and Career Counseling Office. We are working with our major employers and connecting to employment resources to create more support for students as they seek employment. We have also implemented a career services seminar to provide an active way for students to create strategies for successfully entering and progressing in the workforce.




![GSMA RCS IOT Self-accreditation handbook (RCS 3.2 · [8] - UX self-assessment matrix 2 Self-accreditation process overview 2.1 Licensing and Accreditation Framework summary The accreditation](https://img.dokumen.tips/doc/110x75/5f0a8ed67e708231d42c38db/gsma-rcs-iot-self-accreditation-handbook-rcs-32-8-ux-self-assessment-matrix.jpg)




![GSMA RCS IOT Self-accreditation handbook. joyn Hot Fixes ... · [8] - UX self-assessment matrix 2 Self-accreditation process overview 2.1 Licensing and Accreditation Framework summary](https://img.dokumen.tips/doc/110x75/5f0a8ed67e708231d42c38da/gsma-rcs-iot-self-accreditation-handbook-joyn-hot-fixes-8-ux-self-assessment.jpg)



















