Embed Size (px)
Citation preview

� 2006 Wiley-Liss, Inc. American Journal of Medical Genetics Part A 140A:1854–1858 (2006)
Clinical Report
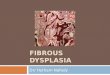
Sedaghatian SpondylometaphysealDysplasia With Pachygyria and Absence
of the Corpus Callosum
Sharon J. English,1* Neti Gayatri,2 Rosemary Arthur,3 and Yanick J. Crow4
1Department of Neonatal Medicine, Leeds General Infirmary, Leeds, United Kingdom2Department of Paediatric Neurology, Leeds General Infirmary, Leeds, United Kingdom
3Department of Radiology, Leeds General Infirmary, Leeds, United Kingdom4Department of Clinical Genetics, St. James’s University Hospital, Leeds, United Kingdom
Received 25 November 2005; Accepted 26 May 2006
We report on a female infant with a metaphyseal dysplasiaand a neuronal migration abnormality consistent with adiagnosis of Sedaghatian spondylometaphyseal dysplasia.This child, born to nonconsanguineous Caucasian parents,was hypotonic from birth and experienced recurrentcyanotic episodes within a few hours of delivery. Cerebralimaging revealed absence of the corpus callosum andmarked frontotemporal pachygyria. She developed seizureson day 14 of life and died at the age of 17 days. Our case
highlights the possibility for neuronal migration abnormal-ities in Sedaghatian spondylometaphyseal dysplasia andsuggests a novel association of the disorder with agenesis ofthe corpus callosum. � 2006 Wiley-Liss, Inc.
Key words: Sedaghatian; spondylometaphyseal dysplasia;pachygyria; neuronal migration disorder; agenesis of thecorpus callosum
How to cite this article: English SJ, Gayatri N, Arthur R, Crow YJ. 2006. Sedaghatian spondylometaphysealdysplasia with pachygyria and absence of the corpus callosum. Am J Med Genet Part A 140A:1854–1858.
INTRODUCTION
Sedaghatian spondylometaphyseal is a rare,perinatally lethal osteochondrodysplasia comprisingmetaphyseal cupping and irregularity with platy-spondyly. A number of extra-skeletal manifestationshave been described including cardiac and cerebralabnormalities. Although only two of 14 reportedcases have been female [Sedaghatian, 1980; Fouldset al., 2003], consanguinity in two of 9 families [Opitzet al., 1987; Kerr et al., 2000] suggests autosomalrecessive inheritance.
Despite the presence of an apparently normalthorax and only relatively minor rhizomelic short-ness, the disease is uniformly fatal due to a com-bination of unexplained hypotonia and respiratoryfailure. Herein, we describe a female infant demon-strating a clinical phenotype consistent with adiagnosis of Sedaghatian spondylometaphyseal dys-plasia. This case further highlights the association ofSedaghatian spondylometaphyseal dysplasia withneuronal migration abnormalities and suggests apreviously unrecorded association with agenesis ofthe corpus callosum.
CLINICAL REPORT
A female infant was delivered by emergencycaesarean at 37 weeks of gestation for undiagnosedbreech presentation following spontaneous onset oflabor. She was the first baby of nonconsanguineousCaucasian parents. Mother was 29 years old withunremarkable past medical history. Pregnancy hadbeen entirely normal, including a 20-week anomalyscan. Birth weight was 2.83 kg (50th centile) andhead circumference 35 cm (91st centile). Apgarscores were 9 at 1 min and 9 at 5 min. However,she was floppy from birth, fed poorly, and experi-enced several unprovoked cyanotic episodes withinthe first 3 hr of life.
She had plagiocephaly, mild micrognathia, andminor proximal limb shortness. She was grossly
*Correspondence to: Dr. Sharon J. English, Department of NeonatalMedicine, Leeds General Infirmary, Leeds LS1 3EX, United Kingdom.E-mail: [email protected]
DOI 10.1002/ajmg.a.31376

hypotonic with absent reflexes although she demon-strated some antigravity movement of all limbs(Fig. 1). She had an irregular breathing pattern withmoderate recession. Saturations were 96% in air butshe desaturated profoundly on handling, requiringfacial oxygen, and demonstrated stridor with respira-tory distress when agitated. She had a clinicallydislocated right hip and dislocatable left hip.
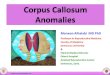
She was monitored and commenced on nasogas-tric feeds. Cranial ultrasound scan showed an absentcorpus callosum. MRI confirmed agenesis of thecorpus callosum and demonstrated pachygyriaparticularly affecting the frontal and temporallobes (Fig. 2). Skeletal survey documented a severemetaphyseal dysplasia (Fig. 3) with platyspondylyandV-shapednotchingof theposterior ribs. EEGwasnormal. An ECG was also unremarkable but echo-cardiogram demonstrated a small muscular VSD.Ophthalmological findings were normal. Endocrine,metabolic, and congenital infection screens yieldednormal results.
The baby remained profoundly hypotonic withfew antigravity movements. She had a weak gagreflex and no suck. She continued to desaturate onhandling and had episodes of hypoventilation.Following diagnosis, she was discharged home atage 12 days on full nasogastric feeds. At the time of
discharge she had shown no abnormal movements.However, on day 14 she experienced a tonic-clonicseizure lasting approximately 15 min. On day 16 shestarted to experience prolonged apnoeic episodeswhich became increasingly frequent. She died athome on day 17 of life. Autopsy was not performed.
DISCUSSION
The clinical and radiological findings of the childwe present are consistent with Sedaghatian spondy-lometaphyseal dysplasia. Despite only mild rhizo-melic limb shortness on examination, radiographs
FIG. 1. Patient at age 12 days with hypotonia and minimal rhizomelicshortness. [Color figure can be viewed in the online issue, which is available atwww.interscience.wiley.com.]
FIG. 2. a and b: MRI showing frontotemporal pachygyria (neuronalmigration disorder) and absence of the corpus callosum.
SEDAGHATIAN SPONDYLOMETAPHYSEAL DYSPLASIA WITH PACHYGYRIA 1855
American Journal of Medical Genetics Part A: DOI 10.1002/ajmg.a

FIG. 3. a: Plain radiograph of legs demonstrating marked metaphyseal Dysplasia.b: Plain radiograph of chest demonstrating platyspondyly, bell-shaped thorax, thinribs, and V-shaped notching of the posterior ribs. c: Lateral radiograph of spine demonstrating platyspondyly. d: Plain radiograph of hand.
1856 ENGLISH ET AL.
American Journal of Medical Genetics Part A: DOI 10.1002/ajmg.a

showed more dramatic findings including platy-spondyly and severe metaphyseal dysplasia. Astriking observation in all patients described is thepresence of normal birth weights and normal or nearnormal intrauterine growth (Table I). Consequently,although rhizomelic shortness has been identified onprenatal ultrasound scan performed in the thirdtrimester [Peeden et al., 1992; Elcioglu and Hall,1998], other infants had normal antenatal scanseven where careful monitoring was undertakenbecause of the known risk of recurrence [Kerret al., 2000].
All cases with this rare osteochondrodysplasiareported to date have exhibited profound neonatalhypotonia, an onset of respiratory problems withinthe first few hours of life and a dramatic postnatalcourse to deathdespite nomajor disproportionof thethorax. Our case is consistent with these observa-tions. The exact cause of the uniform fatality so farremains unexplained.
It is of note that five cases have demonstratedcardiac conduction defects [Sedaghatian, 1980;Peeden et al., 1992; Kerr et al., 2000; Koutoubyet al., 2000] and/or a structural cardiac lesion [Peedenet al., 1992; Koutouby et al., 2000]. However, allaffected infants have died in spite of intensivecardiorespiratory support and cardiac lesions haveonly been described in a few cases. We wereunable to document an electrical cardiac abnormalityalthough a very small muscular VSD was present.
Three previous reports have mentioned findings ofa neuronal migration disorder [Peeden et al., 1992;Koutouby et al., 2000; Foulds et al., 2003]. Brainimaging was provided in only one of these[Koutouby et al., 2000] and showed cerebral atrophywithmarkedpachygyria in the absence of anobviousfronto-occipital gradient. Peeden et al. [1992] pro-vided limited autopsy findings of what they term‘partial lissencephaly’ of the inferior frontal andtemporal lobes. These changes were associatedwith nonspecific EEG abnormalities. Additionally,cerebral ultrasonography in case 2 reported byElcioglu and Hall [1998] was said to show porence-phaly although no further details or imageswere provided. MRI of the child we present demon-strated agenesis of the corpus callosum and pachy-gyria particularly affecting the frontal and temporallobes. Such abnormalities may be related to thehypotonia and to the onset of seizures on day 14of life.
The combination of pachygyria with an epiphysealdysplasia is also seen in Wollcott–Rallison syndrome[Iyer et al., 2004] and microcephalic osteodyplasticprimordial dwarfism [Klinge et al., 2002;Ozawaet al.,2005]. Additionally, filamin A mutations have beenassociated with a bone/brain phenotype [Zenkeret al., 2004]. However, all of these disorders showclinical differences from Sedaghatian spondylome-taphyseal dysplasia.
TABLE
I.Se
lect
ed
Man
ifest
atio
ns
inPublish
ed
Cas
esofSe
dag
hat
ian
Spondylo
meta
phys
eal
Dysp
lasi
a
Refe
rence
Sex
Consa
nguin
ity
Birth
weig
ht(K
g)
(gest
atio
nin
weeks)
OFC
(cm
)O
nse
tofre
spirat
ory
pro
ble
ms
Age
atdeat
h(d
ays)
Car
dia
cab
norm
ality
Bra
inab
norm
alitie
s
Sedag
hat
ian
[1980]
Mal
eN
o3.3
(40)
35
Birth
3W
ide
QRS;
Bundle
bra
nch
blo
ckn.s
.
Mal
en.s
.(n
.s.)
n.s
.n.s
.3
n.s
.n.s
.Fem
ale
3.8
(n.s
.)40
Birth
1n.s
.n.s
.O
pitz
etal
.[1
987]
Mal
eY
es
3.2
8(n
.s.)
35
Birth
4N
on.s
.Cam
pbell
etal
.[1
992]
Mal
en.s
.n.s
.(n
.s.)
n.s
.IU
Dat
30
weeks
IUD
at30
weeks
n.s
.Aqueduct
stenosi
sM
ale
n.s
.n.s
.(4
1)
n.s
.Birth
1D
ilat
ed
hear
tN
one
on
post
-mortem
Peeden
etal
.[1
992]
Mal
eN
o3.1
2(3
6)
33.5
Birth
2ASD
;CH
BFoca
lliss
ence
phal
yElc
ioglu
and
Hal
l[1
998]—
Fam
ily
1M
ale
No
2.9
(36)
31
Stillb
irth
Stillb
irth
n.s
.n.s
.
Elc
ioglu
and
Hal
l[1
998]—
Fam
ily
2M
ale
No
n.s
.(n
.s.)
n.s
.Birth
30
n.s
.Se
izure
s;pore
nce
phal
y
Kerr
etal
.[2
000]
Mal
eY
es
2.6
(36)
31
Stillb
irth
Stillb
irth
n.s
.n.s
.M
ale
3(3
8)
35
Birth
1CH
Bn.s
.M
ale
2.9
5(3
8)
34.2
12
hours
1A-V
dis
soci
atio
nn.s
.K
outo
uby
etal
.[2
000]
Mal
eN
o3.4
(40)
34.5
Birth
161
(with
full
resp
irat
ory
support)
ASD
Seiz
ure
s;ce
rebra
lat
rophy
and
pac
hygyria
Fould
setal
.[2
003]
Fem
ale
No
3.3
4(3
8)
34
2hours
30
No
‘Im
mat
ure
sulc
aldevelo
pm
entan
da
degre
eof
hypopla
sia
thro
ughout’
on
MRI
OFC,occ
ipitofr
onta
lci
rcum
fere
nce
;n.s
.,notst
ated;IU
D,in
tra
ute
rine
deat
h;ASD
,at
rial
septa
ldefe
ct;CH
B,co
mple
tehear
tblo
ck.
SEDAGHATIAN SPONDYLOMETAPHYSEAL DYSPLASIA WITH PACHYGYRIA 1857
American Journal of Medical Genetics Part A: DOI 10.1002/ajmg.a

ACKNOWLEDGMENTS
We like to thank the family for permission toproduce this report. We gratefully acknowledgeProfessor Christine Hall for reviewing the skeletalroentgenograms and suggesting the diagnosis ofSedaghatian spondylometaphyseal dysplasia.
REFERENCES
Campbell RSD, Ireland M, Bloxham CA, Chippindale AJ. 1992.Platyspondylic lethal osteochondrodysplasia: Shiraz typewithradiological-pathological correlation. Pediatr Radiol 22:90–92.
Elcioglu N, Hall CM. 1998. Spondylometaphyseal dysplasia—Sedaghatian type. Am J Med Genet 76:410–414.
Foulds N, Fairhurst J, Temple IK, Cade S, Groves C, LancasterT. 2003. A female case of Sedaghatian type spondylometa-physeal dysplasia. Am J Med Genet Part A 118A:377–381.
Iyer S, Korada M, Rainbow L, Kirk J, Brown RM, Shaw N,Barrett TG. 2004. Wolcott–Rallison syndrome: A clinicaland genetic study of three children, novel mutation inEIF2AK3 and a review of the literature. Acta Paediatr 93:1195–1201.
Kerr B, Smith V, Patel R, Ladusans E, Sillence DO. 2000.Spondylometaphyseal dysplasia Sedaghatian type associated
with lethal arrhythmia andnormal intrauterine growth in threesiblings. Clin Dysm 9:167–172.
Klinge L, Schaper J, Wieczorek D, Voit T. 2002. Microlissence-phaly in microcephalic osteodysplastic primordial dwarfism:A case report and review of the literature. Neuropediatrics33:309–313.
Koutouby A, Habibullah J, Moinuddin FA. 2000. Spondylometa-physeal dysplasia: Sedaghatian type. Am J Med Genet 90:199–202.
Opitz JM, Spranger JW, Stoss HR, Pesch HJ, Azadeh B. 1987.Sedaghatian congenital lethal metaphyseal chondrodysplasia:Observation in a second Iranian family and histopathologicalstudies. Am J Med Genet 26:583–590.
Ozawa H, Takayama C, Nishida A, Nagai T, Nishimura G,Higurashi M. 2005. Pachygyria in a girl with microcephalicosteodysplastic primordial short stature type II. Brain Dev27:237–240.
Peeden JN Jr, RimoinDL, LachmanRS,DyerML,GerardD,GruberHE. 1992. Spondylometaphyseal dysplasia, Sedaghatian type.Am J Med Genet 44:651–656.
Sedaghatian MR. 1980. Congenital lethal metaphyseal chondro-dysplasia: A newly recognised complex autosomal recessivedisorder. Am J Med Genet 6:269–274.
Zenker M, Rauch A, Winterpacht A, Tagariello A, Kraus C,Rupprecht T, Sticht H, Reis A. 2004. A dual phenotype ofperiventricular nodular heterotopia and frontometaphysealdysplasia in one patient caused by a single FLNA mutationleading to two functionally different aberrant transcripts. Am JHum Genet 74:731–737.
1858 ENGLISH ET AL.
American Journal of Medical Genetics Part A: DOI 10.1002/ajmg.a