Embed Size (px)
Citation preview

368 ORTHOPEDICS | Healio.com/Orthopedics
n trauma updateSection Editors: David J. Hak, MD, MBA & Philip F. Stahel, MD
Long Bone Osteomyelitis in Adults: Fundamental Concepts and Current TechniquesJulia Sanders, MD; Cyril Mauffrey, MD, FRCS
Osteomyelitis is a chal-lenge for orthopedic sur-
geons. Bone provides a unique harbor for microorganisms that produce biofilms, allow-ing them to attach resiliently to biologic and implanted surfaces while remaining in-susceptible to host defenses. Acute and chronic phases of osteomyelitis are differenti-
ated by both pathophysiol-ogy and treatment algorithms. Hippocrates first described the disease, recommending splint-ing and clean dressings for open fractures and highlight-ing the risk of bone infection.1 Ambroise Paré, a French sur-geon, described his own open tibia fracture that developed an infection, and attributed this
to retained humor.2 Warfare in the 20th century spurred advances in plastic and ortho-pedic surgery and, along with the introduction of penicillin in the 1940s, pointed the treat-ment of osteomyelitis in the direction that has taken today.3
Unfortunately, the man-agement of osteomyelitis has been given too little attention to date, and quality clinical trials to support treatment practice are scarce. The vari-ability in practice and lack of standardization highlights the latter statement. A treatment algorithm that is based on a classification scheme with a poor interobserver variability can contribute to this difficul-ty. Furthermore, few centers treat a high volume of patients that would be sufficient to develop evidence-based algo-rithms. Finally, surgical meth-ods aimed at local excision of the lesion are bound to failure; the infected tissue within bone has the potential to spread, and wide excision with clear margins is the most valid treat-ment philosophy. In this arti-cle, the fundamental concepts
behind the disease process are reviewed and the current tech-niques for the management of osteomyelitis are discussed. An algorithm for treatment based on these concepts and techniques is presented and illustrated using clinical ex-amples.
EpidEmiologyAlthough many break-
throughs have been made in the field of infectious disease over the past decades, osteo-myelitis remains a difficult problem for the orthopedic community, particularly in busy trauma centers that care for open and complex frac-tures. Infection rates in open long bone fractures range from 4% to 64%.4 A recent study showed that even in patients receiving state-of-the-art or-thopedic and plastic surgical care, 23% of patients devel-oped infections after an aver-age of 3 procedures per limb.5 Chronic infections are both expensive and challenging to treat and cure rates are still not optimal. Ideally, treatment methods should offer complete
The authors are from the Department of Orthopaedics, Denver Health Medical Center, Denver, Colorado.
The authors have no relevant financial relationships to disclose.Correspondence should be addressed to: Cyril Mauffrey, MD, FRCS,
Department of Orthopedics, Denver Health Medical Center, 777 Bannock St, Denver, CO 80204 ([email protected])
doi: 10.3928/01477447-20130426-07
Abstract: Osteomyelitis is challenging for orthopedic sur-geons. The fundamental basis of osteomyelitis treatment is wide surgical debridement. A variety of operative techniques exist for soft tissue coverage and segmental bony stabilization; however, extensive resection remains the crucial starting point in a comprehensive treatment plan. Antibiotic therapy con-tinues to be a cornerstone of adjuvant therapy; nevertheless, the length of treatment is still debated. With ever-increasing antimicrobial resistance rates, targeted therapy based on ac-curate cultures has become imperative. Osteomyelitis requires a multidisciplinary team prepared to formulate an individual-ized surgical and medical plan for each patient. The aim of the current article is to highlight and summarize the current concepts in the management of long bone osteomyelitis.
S P OT L I G H T O N
infectionErratum
This article has been amended to include a factual correction. An error was identified subsequent to its original
printing (2013; 36[5]:368-375), which was acknowledged in an erratum printed in 2014; 37(1):16. The online
article and its erratum are considered the version of record.

MAY 2013 | Volume 36 • Number 5 369
n trauma update
resolution of infection and op-timized function and mobil-ity of the affected extremity. Currently, despite advances in both surgical and chemical treatment, recurrence rates fol-lowing bony infection are be-tween 20% and 30%.6
ClassifiCationSeveral classification sys-
tems have been devised for osteomyelitis, but the Cierny-Mader system remains the most clinically relevant. This system stratifies hosts into 3 categories (A-C) based on physiologic comorbidities and designates 4 anatomic stages of infection (1-4), which are combined to pro-duce 12 classifications.7 This system assists in clinical deci-sion making for the extent of surgical debridement, as well as antibiotic therapy.
Host factors are impor-tant in determining treat-ment algorithms. According to the Cierny-Mader system, a type A host is a healthy pa-tient without comorbidities that might affect their ability to heal. Type B hosts have 1 or more comorbidities that increase their risk of treat-ment failure, including local (eg, vascular disease, chronic edema, fibrosis from radiation or scarring, and obesity) and systemic factors (eg, drug use, age, diabetes mellitus, malig-nancy, immune deficiencies, and malnutrition).8 Type C hosts are compromised to the point that the benefits of treat-ment are outweighed by the possible risks. These patients are offered palliation or treated expectantly while their comor-bidities are addressed.
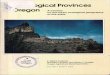
The Cierny-Mader system identifies 4 anatomic types of osteomyelitis (Figure 1): med-ullary (type I), superficial (type II), localized (type III), and diffuse (type IV). Medullary disease involves the internal surface of the bone only, often associated with intramedul-lary hardware. Superficial os-teomyelitis is often associated with soft tissue infections that spread down to bone, such as the base of an open pressure ulcer. Localized disease in-volves the full thickness of the cortex and is essentially a deep extension of a superficial pro-cess. These lesions are limited enough that surgical resec-tion of involved bone leaves a stable segment. In contrast, diffuse osteomyelitis is a full-thickness infection extensive enough to require fixation following debridement due to instability.7 This classifica-tion system still guides treat-ment despite having a poor interobserver variability. It is often difficult to differentiate between a medullary and a su-perficial or localized infection. Magnetic resonance imaging often shows a diffuse appear-ance, which is a more accurate and realistic representation of the infectious process.
EtiologyOsteomyelitis can arise sec-
ondary to hematogenous spread or from a contiguous source of infection. Hematogenous infec-tion is more common in those younger than 20 years and older than 60 years and is the least common form of the disease. It rarely causes osteomyelitis of the long bones in adults.9
Contiguous spread of infection can be caused by surgery, partic-ularly the placement of prosthe-ses or hardware, and trauma or other foreign body introduction. Osteomyelitis can also arise sec-ondary to vascular insufficiency, commonly from a soft tissue in-fection in patients with diabetes mellitus.
In the hematogenous form, a single pathogen is usu-ally isolated, with the most common organism being Staphylococcus aureus.10 In contrast, osteomyelitis sec-ondary to contiguous spread or direct inoculation is usu-ally caused by multiple organ-isms. Polymicrobial infection was responsible for approxi-mately 30% of infections in one series.11 Staphylococcus aureus is the most common isolate in polymicrobial infec-tions, but anaerobes and gram-
negative bacilli are also iso-lated. Antimicrobial-resistant organisms have become more common, and a recent study of approximately 200 patients noted that no single antibiotic regimen would adequately treat the infections.11 Rarely, tuberculosis, other atypical mycobacterium, and fungi may also cause osteomyelitis.
pathogEnEsisAt the onset of infection
in osteomyelitis, immediate vascular changes occur that compromise blood flow to the bone. If the infection is not eradicated before the bone dies, a sequestrum develops and provides a base for the formation of a microbial bio-film. Biofilms are comprised of exopolysaccharide poly-mers forming a protective fibrous matrix around host
Figure 1: Cierny and Mader classification showing the 4 anatomic types of osteomyelitis known as medullary (A), superficial (B), localized (C), and diffuse (D).
1A 1B
1C 1D

370 ORTHOPEDICS | Healio.com/Orthopedics
n trauma update
cells, as well as bacteria.12 Necrotic bone is resorbed, with cancellous bone requir-ing a few weeks to disappear. Cortical bone may take longer, even up to months, to erode. Inflammatory cells in granu-lation tissue are responsible for the destruction of infected bone. Microorganisms freely propagate, and the biofilm ex-pands within the cavity formed by this resorption. As osteo-myelitis progresses, new bone forms around the sequestrum from the neighboring pieces of intact periosteum and end-osteum. As it begins to sur-round the area of infection, it is known as the involucrum. The involucrum is often ir-regular with perforating sinus tracts and may increase in den-sity and thickness with time.13
diagnosisDiagnosis is based on clini-
cal examination, tissue cul-tures, laboratory studies, and imaging. Symptoms of chron-ic osteomyelitis are not always obvious and may include low-grade fever and chronic pain.
Swelling, skin changes, and drainage over the site may be present. Acute infection in adults and particularly chil-dren may present with more systemic signs, such as chills, night sweats, erythema, and severe pain.13 Sinus tracts are often present over the area of chronically infected bone. If these become obstructed, they may form abscesses.
laboratoryInitial workup should in-
clude basic complete blood count, inflammatory markers, cultures, and gram stain. Gram stain is a reflexive addition to any workup but may not lend any diagnostic value except to potentially guide early tai-loring of antibiotic therapy. Cultures are necessary to iden-tify the microbial offender responsible for the infection. Bone biopsies should be taken at the time of surgical debride-ment and should be carefully evaluated for sensitivities. Cultures taken from sinus tract drainage are not reliable for determining the microorgan-
ism responsible for deep infec-tion.14 Cierny8 recommended using polymerase chain reac-tion DNA pyrosequencing to detect and characterize micro-organisms. Prolonged culture (up to 14 days) has also been recommended to increased sensitivity for low-virulence organisms because 7-day cul-tures only provided evidence of infection in 64% of patients in a recent series.11
Surprisingly, leukocyte count may be normal; how-ever, elevated erythrocyte sedimentation rate and noncar-diac C-reactive protein are key signs of infection. The eryth-rocyte sedimentation rate and C-reactive protein will both decrease with successful treat-ment; therefore, their values should be followed closely dur-ing the pre- and postoperative phases. C-reactive protein is known to increase and decrease faster in response to physio-logic changes than erythrocyte sedimentation rate. In addition to inflammatory markers, labo-ratory studies, including albu-min, prealbumin, creatinine, and blood glucose should be followed to ensure optimiza-tion of host factors.10 Blood cultures are positive only in the acute hematogenous form of osteomyelitis and generally do not assist with the diagno-sis of chronic infection in long bones.1
imagingCommon imaging tech-
niques for detecting osteomy-elitis include plain radiography (Figure 2), computed tomogra-phy, magnetic resonance imag-ing, and radionuclide labeled
scans (Figure 3). Often, more than 1 type of imaging is needed for adequate diagnosis and sur-gical planning. Radiographic changes are visible approxi-mately 2 weeks after the physi-ologic process of infection be-gins. The classic signs on plain radiographs include periosteal reaction and osteopenia.10 As the infection progresses, radio-graphic signs (in order of ap-pearance) are soft tissue swell-ing, solid periostitis, lysis and lucencies, surrounding sclero-sis, and sinus tracts.15
Computed tomography scan can assist in visualizing soft tis-sue changes surrounding a bony infection but is impractical to use for infections with local hardware due to resultant arti-fact. It is best used for detailed surgical planning because it clearly identifies sequestra and devascularized bone. Magnetic resonance imaging offers high-er resolution and easily dif-ferentiates between bone and soft tissue involvement. It has high sensitivity and specificity for diagnosing osteomyelitis, which typically appears as a decreased local marrow signal on T1 and an increased local marrow signal on T2.16 Sinus tracts are also well visualized on magnetic resonance imag-ing but often require gadolini-um enhancement.15
Radionuclide labeled scans are useful, especially in clini-cal situations where a clear diagnosis has not been made and in acute settings when radiographs are not helpful. However, they do not offer high-resolution delineation of anatomical involvement. Bone scans with methylene diphos-
2AFigure 2: Anteroposterior (A) and lateral (B) radiographs of a distal femur highlighting the features of diffuse osteomyelitis, which include regional os-teopenia, periosteal reaction with aggressive features (including Codman’s triangle), peripheral sclerosis, sequestrum, and involucrum.
2B

MAY 2013 | Volume 36 • Number 5 371
n trauma update
phonate are highly sensitive and specific for osteomyelitis when increased activity is seen on initial and delayed images but becomes less accurate in the setting of recent surgery or trauma. White blood cell la-beled scans may be performed with several different labels and require longer testing time but offer improved specific-ity.15 Gallium citrate and in-dium may also be used as la-beling compounds to identify areas of inflammation but are less popular due to cost and technical requirements.10
trEatmEntDefinitive management of
long bone osteomyelitis re-quires a multidisciplinary ap-proach involving aggressive surgical debridement and re-construction followed by an-tibiotic therapy.10 Antibiotic therapy alone leads to high failure rates. The current au-thors believe that osteomyelitis should be surgically treated as a malignancy, with wide clear margins ensuring adequate soft tissue coverage. High recur-rence rates are seen with con-servative debridement.1 Soft tissue coverage and dead space management after extensive debridement is paramount be-cause spaces left unmanaged may contribute to ongoing in-fection. All efforts should be made to optimize the host prior to treatment, such as smoking cessation and close control of blood glucose in patients with diabetes mellitus.9
AntibioticsTradition has dictated that
antibiotic therapy should last
4 to 6 weeks, based largely on animal studies and the knowledge that it takes ap-proximately 4 weeks for bone to revascularize after surgical debridement.10 Haidar et al17 proposed that a shorter duration of antibiotic treatment could be feasible following aggressive surgical debridement and well-vascularized flap placement. Antibiotic therapy alone fails because the infection site has a poor vascular supply. Without adequate blood flow to the area, adequate concentrations of an-timicrobials cannot be attained. Levels of antibiotics in bone are less than 20% of serum lev-els, even in healthy bone,1 and are theoretically even lower in diseased tissue. The biofilms formed in osteomyelitis may further decrease the penetration of antimicrobials.
Once adequate surgical de-bridement has occurred, both the offending biofilm and the vascular deficiency should have been addressed, and in-travenous antibiotics should be effective. Shorter courses of intravenous antibiotics would save the health care system a significant amount of money considering the cost and logistical barriers to out-patient intravenous therapy. A recent Cochrane review attempted to summarize the evidence for systemic anti-biotic treatment after surgi-cal debridement for chronic osteomyelitis.6 The authors found few quality studies, but those chosen demonstrated no significant difference between recurrence rates 12 months after oral and parenteral anti-biotic treatment.6
Antibiotics can also be delivered locally rather than systemically. Alternate routes of antibiotic delivery include antibiotic-impregnated cement beads, which provide both high local antibiotic concentrations and dead space management. The effectiveness of this treat-ment, both alone and in con-junction with intravenous anti-biotics, has been demonstrated in animal models and human trials.17 However, local anti-biotic strategies have not been proven superior to intravenous administration and require sur-gical removal.
Biodegradable antibiotic delivery systems obviate the need for a second surgical pro-cedure for removal and several systems are being developed. Collagen fleece is a nontoxic, biocompatible antibiotic car-
3A 3B
3C
Figure 3: Features of diffuse tibial osteomyelitis as shown on coronal T1- (A) and T2-weighted (B) magnetic resonance images. Axial computed to-mography scan revealing diffuse proxi-mal femoral osteomyelitis (C) and axial magnetic resonance image showing type II osteomyelitis of the tibia (D).
3D

372 ORTHOPEDICS | Healio.com/Orthopedics
n trauma update
rier that offers a triphasic anti-biotic release and strong clini-cal results to date. Polyesters are another alternative for biodegradable delivery, offer-ing a slower breakdown and some evidence of intracellular action. Calcium-based carri-ers, including Plaster of Paris, calcium sulphate, and calcium hydroxyapatite, are promis-ing because they allow tissue and bone ingrowth as they de-grade. Other potential delivery systems not requiring surgical removal are polyanhydrides, amylose starch, and composite carriers.
Surgical InterventionThe extent of surgical de-
bridement should be planned to account for the host type, area of involvement, and likely need for soft tissue coverage and stabilization. Adequate debridement is the key to treatment success, and all dead and ischemic tissues and sinus
tracts should be removed.7 Simpson et al18 prospectively studied the effect of extent of surgical debridement on cure rates and found 100% cure rates with wide excision and 100% recurrence rates with intralesional biopsy and local debulking. Marginal resection with less than 5-mm margins exhibited a 28% recurrence rate, all of which were found in type B hosts.18
When debriding, healthy bleeding tissue should be visu-alized at all boundaries of the surgical site, followed by thor-ough irrigation.19 At this point, the need for stabilization and soft tissue coverage can be assessed. Stage I infections limited to the medullary canal may be treated with intramed-ullary reaming and occasional-ly very localized unroofing and curettage.7 If evidence exists of metaphyseal involvement or endosteal scalloping, a longi-tudinal trough should be made
to access the canal for curet-tage, which minimizes effects on bony stability.20 Primary closure can usually be attained because the dead space is lim-ited to the intramedullary ca-nal.8 Stage II infections can be addressed with soft tissue de-bridement and decortication of the bone adjacent to the infec-tion. Coverage with a flap has been described both simulta-neously and during a second-stage procedure,7 either with local or free flap mobilization. Stage III osteomyelitis usually requires debridement of soft tissue, sequestrum, and cortex, as well as decompression of the involved medullary canal. Cierny et al7 referred to this process as saucerization, al-luding to the shape of the bone left untouched. Stabilization, soft tissue coverage, and grafting may all be necessary depending on the extent of involvement, with more than 70% of the cortex required for
absolute stability.20 Stage IV infections are the most chal-lenging to treat surgically be-cause they most often require multiple staged procedures and necessitate osseous sta-bilization. Staged procedures address the need for eradica-tion of infection followed by osseous reconstruction aiming for union and stability once the tissue is healthy. In Figure 4, the current authors present their treatment algorithm.
For extensive involvement with significant segmental bone loss, several methods of staged treatment have been described, with no current consensus on a gold standard. A wide variety of studies ex-ist, with many combinations of early and late stabilization, coverage, structural support, and antibiotic delivery. Some weaknesses in the literature include a paucity of long-term follow-up data and a lack of a universal definition of cure.
The Papineau, or open air, technique and its various per-mutations have been widely cited in the treatment of os-teomyelitis. This method in-volves radical debridement, staged bone grafting, and de-layed soft tissue coverage with either natural granulation or skin grafting.21 This technique is often used in type III infec-tions following saucerization because the bone graft does not offer significant structural support.22 Meticulous wound care is needed because the de-brided area is left open with the bone graft exposed. This technique has somewhat fallen out of favor in light of newer plastic surgery techniques for
Figure 4: Algorithm of the authors’ preferred treatment methodology for the management of stage 4 osteomyelitis.
4

MAY 2013 | Volume 36 • Number 5 373
n trauma update
tissue transfer and grafting but remains a foundational approach to the surgical treat-ment of osteomyelitis.
McNally et al23 first de-scribed a staged procedure, known as the Belfast tech-nique, comprised of radical debridement, early soft tissue coverage (with or without an-tibiotic beads) to eliminate dead space, and delayed bone grafting, if necessary. This decreased the hospitalization time necessary for treatment compared with previous meth-ods and led to a cure rate of 92%. They emphasized wide resection of infected areas with no attempt to salvage dis-eased tissue as a key compo-nent of treatment.23
The Ilizarov technique in-volves placing a circular exter-nal fixation device for the long-
term treatment of bone defects. It is both time- and cost- intensive but has had success in the treatment of osteomyelitis. Marsh et al24 reported a 100% cure rate at 1-year follow-up using an Ilizarov frame on in-fected long bones, although 3 patients failed to unite their fractures in this time. This tech-nique allows stabilization with concurrent soft tissue treatment as well as distraction osteo-genesis to close a segmental gap and can be combined with other forms of treatment for op-timal outcomes.
Vacuum-assisted closure of soft tissue defects has been used in many settings, and recent evidence has demonstrated its efficacy in the treatment of stage II, III, and IV infections after de-bridement and the initiation
of antibiotic therapy. One study compared vacuum-assisted closure therapy to conventional wound care and found a significant reduction in infection recurrence, the rate of necessary subsequent flap treatment, and the in-
cidence of positive cultures after treatment completion.25 Vacuum-assisted closure therapy has also been imple-mented in combination with the Papineau technique in lieu of wet-to-dry dressings with good results.26
Figure 5: Photographs showing the first stage of the Masquelet technique used to excise a large segment of the affected tibia. The skin is marked based on magnetic resonance imaging findings and extension of the infectious pro-cess (A). Photograph showing the application of a monotube external fixator and resection of the affected segment with clear margins on the intraoperative frozen section (B). Fluoroscopic imaging showing the affected bony segment resection (C, D).
5A 5B
5C 5D
Figure 6: Clinical photograph of the tibial segment affected by the infection that has been cut in half to show the involvement of both the cortex and the medullary cavity (A). Clinical photograph showing that the sinus tract is clearly visible. Anteroposterior (C) and lateral (D) radiographs of the tibia with the cement spacer in situ.
6A 6B
6C 6D
7A 7BFigure 7: Anteroposterior (A) and lateral (B) radiographs of the tibia following the second stage of reconstruction using Masquelet technique. The bone graft (30 mL) was harvested using a reamer-irrigator-aspirator from the ipsilateral femur and inserted into the defect after removal of the antibiotic spacer.

374 ORTHOPEDICS | Healio.com/Orthopedics
n trauma update
Masquelet pioneered a technique for the treatment of segmental bony defects in-volving initial wide debride-ment and the placement of an antibiotic-loaded cement spac-er with temporary stabilization with intramedullary nailing, plating, or external fixation. This is followed 8 weeks later by removal of the spacer and careful placement of autograft into the induced membrane rich in growth factors (Figures 5-7).27 However, this tech-nique has not been specifically studied in the treatment of os-teomyelitis.
For infections that per-sist despite debridement and antibiotics, the Lautenbach technique has been offered as an alternative treatment. This procedure was first de-scribed in patients with total hip arthroplasty infections and involves intramedullary ream-ing and placement of a closed endosteal irrigation system.28 This system allows for the lo-cal delivery of antibiotics and continuous sampling of the in-fected cavity for cultures and narrowing of antibiotic ther-apy. Hashmi et al29 reported using this technique in 17 pa-tients with chronic osteomy-elitis. Therapy was continued until 3 consecutive negative cultures were obtained and the endosteal cavity was filled with granulation tissue, with a mean treatment length of 27 days. They reported only 1 re-currence, which resolved with repeat treatment.29
Beals and Richard30 com-pared the treatment of chronic osteomyelitis of the tibia with antibiotics and one of several
surgical techniques by the same surgeon. They found good results with debridement and muscle flap, bone graft, bone transport, the Papineau technique, and an Ilizarov frame. Twenty-seven of 30 patients had good outcomes, suggesting that optimal results can be obtained with any well-planned surgical procedure.31
ConClusionA plethora of reconstruc-
tive techniques exist, none of which has been proven superi-or in the setting of osteomyeli-tis, but the key remains eradi-cation of infection with wide resection and adjuvant antibi-otics. Failure of infection elimination appears to be di-rectly related to the extent of resection.18 The philosophy guiding the management of long bone osteomyelitis should be early aggressive management along with opti-mization of the host medical and nutritional status, with a focus on wide margins exci-sion and debridement of all af-fected tissues. Necessary length of antibiotic treatment is still debatable; however, in-creasing rates of resistance un-derscore the importance of ac-curate cultures and targeted therapy. New methods for soft tissue coverage and bony re-construction continue to be in-troduced, and it is important to refer patients to centers spe-cialized in bone infection. An algorithm, such as the one sug-gested here (Figure 4), should be used to guide management. Future research should ideally address the lack of prospec-tive, controlled, randomized
trials comparing techniques and identify a gold standard of treatment for antibiotic length and delivery.
rEfErEnCEs 1. Lew DP, Waldvogel FA.
Osteomyelitis. Lancet. 2004; 364:369-379.
2. Perry CR. A historical per-spective. In: Bone and Joint Infections. London: Martin Dunitz; 1996:1-8.
3. Klenerman L. A history of os-teomyelitis from the Journal of Bone Joint Surg. 1948-2006. J Bone Joint Surg Br. 2007; 89:667-670.
4. Schenker ML, Yannascoli S, Baldwin KD, Ahn J, Mehta S. Does timing to operative debridement affect infectious complications in open long bone fractures? A systematic review. J Bone Joint Surg Am. 2012; 94:1057-1064.
5. Penn-Barwell JG, Bennett PM, Fries CA, Kendrew JM, Midwinter MJ, Rickard RF. Severe open tibial fractures in combat trauma: management and preliminary outcomes. Bone Joint J. 2013; 95:101-105.
6. Conterno LO, da Silva Filho CR. Antibiotics for treating chronic osteomyelitis in adults. Cochrane Database Syst Rev. 2009; 3:1-30.
7. Cierny G, Mader JT, Penninck JJ. A clinical staging for adult osteomyelitis. Clin Orthop Relat Res. 2003; (414):7-24.
8. Cierny G. Surgical treatment of osteomyelitis. Plast Reconstr Surg. 2011; 127:190S-204S.
9. Mader JT, Calhoun JH, Lazzarini L. Adult long bone osteomyeli-tis. In: Calhoun JH, Mader JT, eds. Musculoskeletal Infections. New York, NY: Marcel Dekker; 2003:149-182.
10. Lazzarini L, Mader JT, Calhoun JH. Osteomyelitis in long bones. J Bone Joint Surg Am. 2004; 86:2305-2318.
11. Sheehy SH, Atkins BA, Bejon P, et al. The microbiology of chronic osteomyelitis: preva-lence of resistance to common empirical antimicrobial regi-mens. J Infect. 2010; 60:338-343.
12. Gristina AG, Oga M, Webb LX, Hobgood CD. Adherent bacteri-al colonization in the pathogen-esis of osteomyelitis. Science. 1985; 228:990-993.
13. Calhoun JH, Manring MM, Shirtliff M. Osteomyelitis of the long bones. Semin Plast Surg. 2009; 23(2):59-72.
14. Perry CR, Pearson RL, Miller GA. Accuracy of cultures of material from swabbing of the superficial aspect of the wound and needle biopsy in the pre-operative assessment of osteo-myelitis. J Bone Joint Surg Am. 1991; 73:745-749.
15. Pineda C, Vargas A, Rodriguez AV. Imaging of osteomyelitis: current concepts. Infect Dis Clinic N Am. 2006; 20:789-825.
16. Ma LD, Frassica FJ, Bluemke DA, Fishman EK. CT and MRI evaluation of musculoskeletal in-fection. Crit Reb Diagn Imaging. 1997; 38:535-568.
17. Haidar R, Boghossian AD, Atiyeh B. Duration of post-surgical anti-biotics in chronic osteomyelitis: empiric or evidence-based? Int J Inf Dis. 2010; 14:e752-e758.
18. Simpson AH, Deakin M, Lathan JM. The effect of the extent of surgical resection on infection-free survival. J Bone Joint Surg Br. 2001; 83:403-407.
19. Forsberg JA, Potter BK, Cierny G, Webb L. Diagnosis and man-agement of chronic infection. J Am Acad Orthop Surg. 2011; 19:S9-S19.
20. Parsons B, Strauss E. Surgical management of chronic os-teomyelitis. Am J Surg. 2004; 188:S57-S66.
21. Papineau LJ. Excision-graft with deliberately delayed clos-ing in chronic osteomyelitis [in French]. Nouv Presse Med. 1973; 2:2753-2755.
22. Papineau LJ, Allfageme A, Dalcourt JP, Pilon L. Chronic osteomyelitis: open excision and grafting after saucerisation. Int Orthop. 1979; 3:165-176.
23. McNally MA, Small JO, Tofighi HG, Mollan RAB. Two-stage management of chronic os-teomyelitis of the long bones. J Bone Joint Surg Br. 1993; 75:375-380.
24. Marsh DR, Shah S, Elliott J, Kurdy N. The Ilizarov method in nonunion, malunion, and in-

MAY 2013 | Volume 36 • Number 5 375
n trauma update
fection of fractures. J Bone Joint Surg Br. 1997; 79:273-279.
25. Tan Y, Wang X, Li H, Zheng Q, Li J, Feng G, Pan Z. The clinical efficacy of the vacuum-assisted closure therapy in the manage-ment of adult osteomyelitis. Arch Orthop Trauma Surg. 2011; 131:255-259.
26. Archdeacon MT, Messerschmitt P. Modern Papineau technique with vacuum-assisted closure. J Orthop Trauma. 2006; 20:134-137.
27. Karger C, Kishi T, Schneider L, Fitoussi F, Masquelet AC. Treatment of posttraumatic bone defects by the induced mem-
brane technique. Orthop Traum Surg Res. 2012; 98:97-102.
28. Weber FA, Lautenbach EEG. Revision of infected total hip arthroplasty. Clin Orthop Relat Res. 1986; (211):108-115.
29. Hashmi MA, Norman P, Saleh M. The management of
chronic osteomyelitis using the Lautenbach method. J Bone Joint Surg Br. 2004; 86:269-275.
30. Beals RK, Richard EB. The treatment of chronic open os-teomyelitis of the tibia in adults. Clin O rthop Relat Res. 2005; (433):212-217.