Embed Size (px)
Citation preview

Clinical Breast Cancer October 2004 • 269
commentary
The adequate management of indi-viduals who carry a high lifetime riskfor breast cancer is still an unsettledissue. This holds especially true forsubjects with documented or suspectedgermline mutation of a breast cancersusceptibility gene. These women facea lifetime risk of breast cancer as highas 80%, which is of course significant.But this still means that about onefifth of these women will never developthe disease. Also, it is impossible topredict at which time in a woman’s lifethe threat comes true, from her thir-ties to many years after menopause.This, together with the perceived mu-tilating effects of mastectomy, makesthe decision for surgical preventionvery difficult for most women. Under-standably, in their search for alterna-tives to surgical measures, patientsurge their health care providers tooffer screening for familial breast can-cer, with the underlying assumptionthat early diagnosis is a synonym for(or ensures) an excellent prognosis.However, this concept is debatable inmany aspects.
Breast ScreeningIt is important to realize that there
is only very limited evidence regardingthe effectiveness of screening pro-grams in women at high genetic risk.As Robson correctly summarizes in hisreview in this issue of Clinical BreastCancer, there are a number of thor-oughly conducted clinical screeningtrials under way that investigate theefficacy of imaging studies for screen-ing women with familial breast can-cer.1 Although there is some evidenceto suggest that intensified screeningallows an early diagnosis of familialbreast cancer, the long-term efficacy ofall screening efforts are unclear interms of actual patient outcome. Theremay be some evidence suggesting thatscreening, particularly with breast
magnetic resonance imaging (MRI),may allow diagnosis of tumors in theirearly stages, but whether or this willtranslate into reduced mortality re-mains to be seen. The positive predic-tive value (PPV), number of detectedcancers, or tumor stage at diagnosisare only surrogate markers for the effi-cacy of screening. It is important tocommunicate this lack of long-termoutcome data to the patient and to ex-plain that the only intervention forwhich an effect on mortality has beendocumented so far is preventive mas-tectomy.2,3 In this context, anotherproblematic issue needs to be dis-cussed: today, breast cancer awarenessis high, in particular among familieswith several affected individuals. Prob-ably more than in the past, today,women tend to actively seek independ-ent information resources, such as viathe media or the Internet. The verylimited published evidence regardingscreening MRI has been closely fol-lowed by many of these women, andthis seems sufficient to make aprospective randomized clinical trialvirtually impossible. Already, basedon the limited evidence that existstoday on the use of MRI for screeningfamilial breast cancer, it would be dif-ficult to withhold MRI from womenat increased risk for study purposes.Accordingly, it will be increasinglydifficult to set up a randomizedscreening trial that would be neededto investigate the efficacy of intensi-fied screening in terms of mortality.
Imaging TechniquesRobson carefully explains that there
is uncertainty as to which of the avail-able imaging techniques (mammogra-phy, high-frequency breast ultra-sonography [US], and MRI) should beused for screening (Figure 1). Even ifcost-effectiveness issues are disregard-ed, the question that remains is whichtechnique is most suitable for thistask. Surprisingly, and despite the ob-vious lack of scientific evidence, anumber of guidelines already exist forthe surveillance of women at high ge-netic risk of breast cancer.4-7 Yet these
Screening of Women with Hereditary Risk of Breast Cancer
Christiane K. Kuhl, MD
Department of Radiology University of BonnGermany
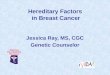
Images from a Patient with Hereditary Risk of Breast Cancer
Figure 1
Images from a 32-year-old patient with a strong family history of early-onset breast cancer and documented BRCA1 mutation. Screening mammogram and screening US were negative. MRI reveals a suspicious lesion in the lower outer quadrant of her right breast. MRI-guided localization and excisional biopsy confirmed presence of a 5-mm duct-invasive breast cancer, G3. Patient underwent breast-conserving therapy and uneventful follow-up for 6 years. A. Mammogram, mediolateral view. B. Mammogram, CC view. C: Non-enhanced MRI of the breast. D. Contrast material–enhanced MRI of the breast. E. Contrast material–enhanced subtracted MRI. Note that the mammogram is normal and that the breast parenchyma is only intermediately dense (ACR 3). Note the small enhancing lesion in the MRI.
C
A
D
E
B

270 • Clinical Breast Cancer October 2004
guidelines in the majority of cases arebased on “expert opinion” alone. First,systematic comparative screening tri-als suggested that mammography is oflimited value in the young patient athigh risk.8-16 Nevertheless, virtuallyall the existing guidelines recommendyearly bilateral 2-view mammographicscreening to start at age 30 or evenyounger. However, the dense parenchy-ma in young women tends to cause di-agnostic difficulties. This leads to addi-tional mammographic burden causedby short-term follow-up studies; addi-tional views and spot magnificationviews can be predicted to occur. It isimportant to realize that the long-termeffects of such an intensified mammo-graphic screening are unknown, par-ticularly in BRCA mutation carriers.BRCA-regulated gene products havebeen implicated directly or indirectlyin cell cycle regulation and DNA re-pair.17-19 Thus, there is evidence tosuggest that carriers of pathogenic mu-tations of the BRCA1 or BRCA2 genesmay be more susceptible to mutageniceffects of even low-dose irradiation,such as that used for mammography.So although the potentially increasedradiation sensitivity should caution usto use as little ionizing radiation aspossible, current guidelines recom-mend that we expose mutation carriersto a cumulative lifetime organ dosethat will be substantially higher thanthat recommended for a woman at av-erage risk.
These guidelines are justifiable inview of the very high lifetime risk ofbreast cancer in mutation carriers, andit should be well understood that, evenin the worst-case scenario, the attrib-utable risk induced by mammographicscreening will be slight. Still, if therewere imaging studies at hand that of-fered a diagnostic accuracy equivalentto a mammogram, but without ioniz-ing radiation, the possibly increasedradiation sensitivity would be a goodreason to prefer these imaging studiesover mammography in this specificsubset of patients.
The results of several multimodalityscreening studies are impressively con-cordant in that MRI seems to be notonly equivalent to mammography, buteven substantially more accurate for di-
agnosing early familial breast cancer.Still, MRI is only rarely offered forscreening women at high genetic risk.
Apart from cost, the most importantreason why MRI is only reluctantly ac-cepted for screening is probably its re-ported low specificity and PPV. Particu-larly in young women, hormonal stimu-lation and proliferative changes (ie,adenosis) are notorious causes of false-positive diagnoses on MRI. These areeven more problematic than false-posi-tive mammographic or sonographic di-agnoses, because any MRI-only suspi-cious finding would require an MRI-guided intervention for clarification, orat least an additional MRI study for fol-low-up. Given the very low number ofinstitutions that offer MRI-guided in-terventions at this time, the issue ofmere availability of this type of patientcare becomes a major concern.
So despite the well-recognized andunprecedented sensitivity, the allegedlylow PPV (high rate of false-positiveMRI diagnoses) seems to outweigh thebenefits. However, it is important tonote that this reported low PPV is notan inherent feature of breast MRI.Rather, it is a side effect of the relativeunderuse of this technique comparedwith mammography.
It is well established that the accuracyof any diagnostic imaging modality de-pends heavily on the experience of theinterpreting radiologist. Specifically re-garding mammographic screening, thishas led to the recommendation to re-quire a certain number of mammogramsto be read each year by radiologists whowish to participate in screening (the cur-rent guidelines of the European Unionrequire a minimum of 5000 mammo-grams to be read per year). There is noreason to assume that reading screeningbreast MRI or breast US would requireless expertise with these imaging modal-ities. However, although > 40,000,000screening mammograms are read eachyear in the United States, the total num-ber of breast MRI studies is estimated torange between 6000 and 9000 per year;ie, 0.02% of the number of mammo-grams.20 This wide gap between the pre-sumed average expertise in readingmammograms compared with the re-spective expertise in reading breast MRIstudies is probably the single most im-
portant reason for the reported low PPVfor breast MRI. One may even speculatethat if mammograms were read with thesame level of expertise as the averagebreast MRI study is read, the PPV ofmammographic screening would in turnbe considered inappropriate.
Evidence suggests that with increas-ing practical experience, screening MRIhas not only equivalent, but in facthigher, PPV compared with mammo-graphic or US screening. Our own de-partment sees approximately 5000breast MRI studies per year; this trans-lated into a PPV of 57% for MRIscreening in women at high risk, com-pared with PPVs of 38% for mammog-raphy and only 16% for breast US inthe same patients.8
So it seems that the allegedly lowPPV of breast MRI is simultaneously acause and an effect of the continued un-deruse of this technique, thus perpetu-ating the current situation.
It is certainly true that false-positivediagnoses may still occur even with themost experienced readers and may im-pair the quality of life (QOL) of womenundergoing screening. Yet the majorityof women still appreciate having accessto screening with MRI, because QOL iscertainly worse with a diagnosis of ad-vanced-stage breast cancer. If ourscreening efforts proved effective interms of survival, then another impor-tant contribution of screening to QOLwould be the fact that screening mayallow women to avoid mastectomy andlive their lives with their body imageuntouched.
Our current concept is to offer yearlybreast MRI together with single-view(mediolateral oblique) mammographyto offer maximum sensitivity for intra-ductal and invasive cancer and still re-duce radiation dose. Breast US is thenperformed between screening rounds toensure timely surveillance of women athigh risk.
With this it is hoped, but not yetproven, that we do more good than harm.
1. Robson M. Breast cancer surveillance inwomen with hereditary risk of breast cancerwith BRCA1 or BRCA2 mutations. ClinBreast Cancer 2004; 5:260-268.
2. Hartmann LC, Schaid DJ, Woods JE, et al.Efficacy of bilateral prophylactic mastecto-my in women with a family history of breastcancer. N Engl J Med 1999; 340:77-84.

Clinical Breast Cancer October 2004 • 271
3. Meijers-Heijboer H, van Geel B, van PuttenWL, et al. Breast cancer after prophylacticbilateral mastectomy in women with aBRCA1 or BRCA2 mutation. N Engl J Med2001; 345:159-164.
4. Burke W, Daly M, Garber J, et al. Recom-mendations for follow-up care of individu-als with an inherited predisposition to can-cer. II. BRCA1 and BRCA2. Cancer Genet-ics Studies Consortium. JAMA 1997;277:997-1003.
5. Eisinger F, Alby N, Bremond A, et al. Rec-ommendations for medical management ofhereditary breast and ovarian cancer: theFrench National Ad Hoc Committee. AnnOncol 1998; 9:939-950.
6. Pichert G, Bolliger B, Buser K, et al. Evi-dence-based management options forwomen at increased breast/ovarian cancerrisk. Ann Oncol 2003; 14:9-19.
7. Vasen HF, Haites NE, Evans DG, et al. Cur-rent policies for surveillance and manage-ment in women at risk of breast and ovari-an cancer: a survey among 16 Europeanfamily cancer clinics. European FamilialBreast Cancer Collaborative Group. Eur JCancer 1998; 34:1922-1926.
8. Kuhl CK, Schmutzler RK, Leutner CC, etal. Breast MR imaging screening in 192women proved or suspected to be carriers ofa breast cancer susceptibility gene: prelimi-
nary results. Radiology 2000; 215:267-279.9. Stoutjesdijk MJ, Boetes C, Jager GJ, et al.
Magnetic resonance imaging and mammog-raphy in women with a hereditary risk ofbreast cancer. J Natl Cancer Inst 2001;93:1095-1102.
10. Tilanus-Linthorst MM, Obdeijn IM, BartelsKC, et al. First experiences in screeningwomen at high risk for breast cancer withMR imaging. Breast Cancer Res Treat 2000;63:53-60.
11. Tilanus-Linthorst MM, Bartels CC, ObdeijnAI, et al. Earlier detection of breast cancerby surveillance of women at familial risk.Eur J Cancer 2000; 36:514-519.
12. Tilanus-Linthorst M, Verhoog L, ObdeijnIM, et al. A BRCA1/2 mutation, high breastdensity and prominent pushing margins ofa tumor independently contribute to a fre-quent false-negative mammography. Int JCancer 2002; 102:91-95.
13. Warner E, Plewes DB, Shumak RS, et al.Comparison of breast magnetic resonanceimaging, mammography, and ultrasoundfor surveillance of women at high risk forhereditary breast cancer. J Clin Oncol2001; 19:3524-3531.
14. Kriege M, Brekelmans CT, Boetes C, et al.Efficacy of MRI and mammography forbreast cancer screening in women with a fa-milial and genetic predisposition. N Engl J
Med 2004; 351:427-437.15. Kuhl CK, Schrading S, Leutner CC, et al.
Surveillance of “high risk” women withproven or suspected familial (hereditary)breast cancer: First mid-term results of amulti-modality clinical screening trial. ProcAm Soc Clin Oncol 2003; 22:2 (Abstract #4).
16. Podo F, Sardanelli F, Canese R, et al. TheItalian multi-centre project on evaluation ofMRI and other imaging modalities in earlydetection of breast cancer in subjects athigh genetic risk. J Exp Clin Cancer Res2002; 21(3 suppl):115-124.
17. Zhou C, Smith JL, Liu J. Role of BRCA1 incellular resistance to paclitaxel and ionizingradiation in an ovarian cancer cell line car-rying a defective BRCA1. Oncogene 2003;22:2396-2404.
18. Somasundaram K. Breast cancer gene 1(BRCA1): Role in cell cycle regulation andDNA repair-perhaps through transcription.J Cell Biochem 2003; 88:1084-1091.
19. Deng CX, Wang RH. Roles of BRCA1 inDNA damage repair: a link between devel-opment and cancer. Hum Mol Genet 2003;12(suppl 1):R113-R123.
20. United States General Accounting Office,Report to the Chairman of the Special Com-mittee on Aging, US Senate; GAO-02-532Mammography, Capacity Generally Existsto Deliver Services; April 2002.