Embed Size (px)
Citation preview

Difficult Cases
Scottsdale Headache Symposium 2016
• Alex Sinclair• NIHR Clinician Scientist & Honorary
Consultant Neurologist • [email protected]
• No conflicts of interest
Presenting complaint • 21 year old woman referred for an opinion on whether to site a shunt

Headache History• No headaches as child or during most of her adult life
• Continous headaches for 13 months
• Worse in morning and increases on valsalva and bending
• Continous tinnitus over the same time period
• Excerbations of the headache are linked to blurred vision, obscurations, occasional diplopia
• Since summer 2015 increase in weight by 1 stone (8 weeks)

• Asthma• Increased BMI• Hypothyroid• Heartburn• Cholecystectomy 2014• Appendectomy 2012
Social history• Nursery nurse at risk of loosing job due
to time off work• Married no children
Allergies• Dystonic reaction to prochlorperazine
Family history• Grandmother glaucoma
Drug historyPast medical history• Topiramate 50mg OD (6/12)• Acetazolamide 500mg BD• Celebrex 100mg BD• Co-Codamol up to 8 daily• Salbutamol inhaler• Levothyroxine 50mcg• Lansoprazole 30mg

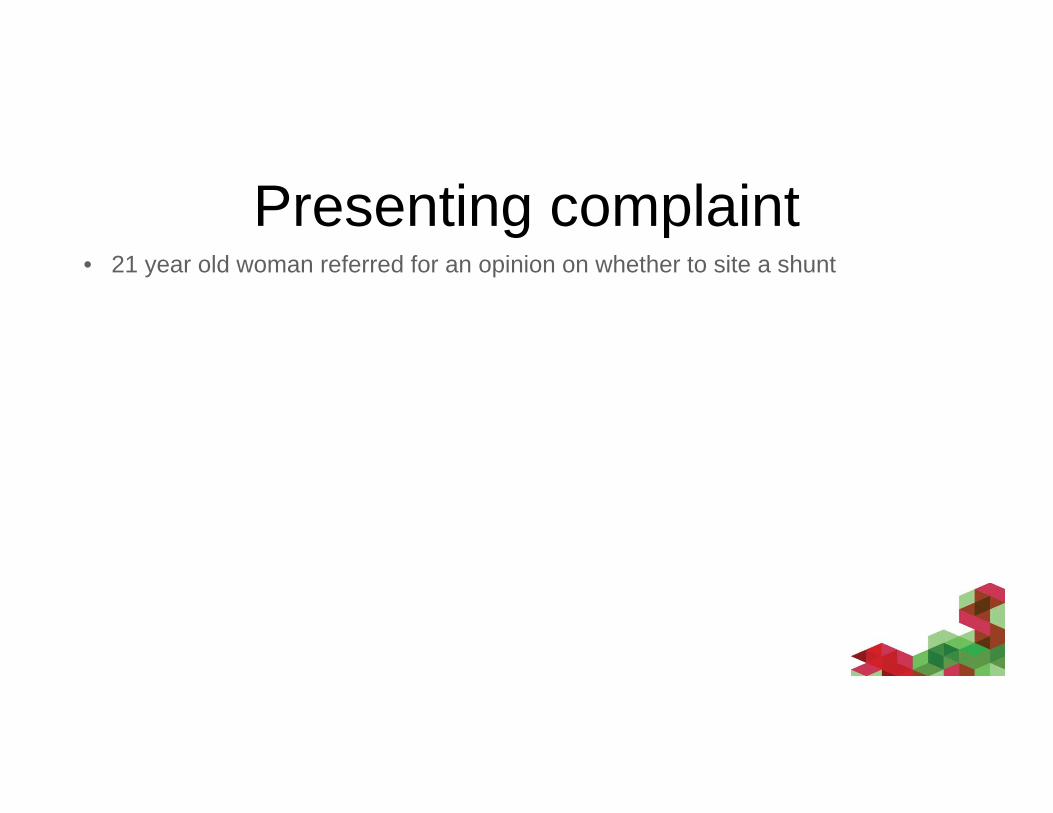
First presentation• No papilloedema
• MRI brain - normal
• CT brain –normal
• CT venogram – normal
• LP – 32cm CSF; normal constituents

MRI imaging
Post contrastPre contrast

Referred to the IIH clinic• Noted one stone weight gain in 8 weeks prior to
presentation, in conjunction with new diagnosis of hypothyroidism
• No antibiotic use• No steroid use• No Vit A analogues• No Vit A supplementation• Not anaemic• No history of sleep apnoea• No venous thrombosis

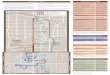
Summary of LP’s in regional hospital
Relief of tinnitus and headaches after LP
32
45
25
30
MAR APR MAY JUN JUL AUG SEPT OCT NOV DEC JAN FEB MAR APR MAY JUN JUL AUG SEPT OCT
3130
25
45
32
2015 2016
1 stone weight gain

ExaminationRight Left
Acuity Un-aided 6/36 6/18
Acuity Corrected 6/18 6/9Ishihara colour vision Full fast Full fast
Pupils Normal, no RAPD
EOM Left VI nerve palsy
BMI 40.4
Full neurological exam otherwise normal

Right eye Left Eye

No fix losses, false pos false neg 5%No correction put upMD ‐5.92 DBPSD 6.66 DB
No fix losses, false pos or false negMD ‐1.97 DB PSD 1.83 DB

Could it be IIHWOP?• IIH With Out Papilloedema• Typically have a phenotype of obesity and
female gender• Debated area
• May have been over diagnosed in some studies
• New Diagnostic criteria*Friedman DI et al. Neurology 2013;81:1159–65

IIHWOP Diagnostic criteria
• Fulfil the criteria B-E above +• Unilateral or bilateral sixth nerve palsy• Or 3 neuro-imaging findings suggestive of raised ICP
• Empty sella, flattening of the posterior aspect of the globe, distention of the perioptic subarachnois space ±a tortuous optic nerve and transverse sinus stenosis
• Venous stenosis.
Diagnostic criteria for adult IIH* (Friedman 2013 Neurology)
A. Papilloedema
B. Normal neurological examination except for cranial nerve abnormalities
C. Neuroimaging: Normal brain parenchyma without evidence of hydrocephalus, mass or structural
lesion and no abnormal meningeal enhancement or venous sinus thrombosis on MRI and magnetic
resonance venography; if MRI is unavailable or contraindicated, contrast-enhanced CT may be
used.
D. Normal cerebrospinal fluid (CSF) composition
E. Elevated lumbar puncture opening pressure (≥ 25cmH2O) in a properly performed lumbar puncture

IIHWOP case 2Chronic daily headache 3 yearsNo papilloedemaNo 6th nerve palsy
LP 52 cmCSFBMI 49
LP 37 cmCSFBMI 49
LP 54 cmCSFBMI 49
Only imaging finding was empty sella
• LP shunt inserted
• Referred to Tier 3 Weight management program
Challenging diagnosisDon’t all have the classic imaging findings or 6th
Nerve palsy

IIHWOP – practical approach•• Chronic headaches• Obese female• No papilloedema
•
Consider • Repeat interval LP • ICP monitoring
• Raised ICP on separate occasions is increasingly supportive of diagnosis• Caution about interpreting improvement post LP
± Any evidence of Raised ICP on MRI? LP
Baseline OCT
IIHWOP increasingly likely
IIH WOP likely INCREASING LIKELIHOOD OF PATHOLOGICALLY RAISED ICP
15 20 25 30 35 40 4510 50 55 60

IIHWOP – Vision
Clover leaf appearance of functional visual fields can occur
• No papilloedema• Don’t develop papilloedema• Do not lose vision• Functional visual loss can occur• Visual phenomenon from migraine aura may occur

IIHWOP management1.Manage
conservatively Facilitate weight loss
2.Ongoing disability
Phenotype headachePhenotype headache
Any evidence of medication overuse?
Any evidence of medication overuse? Withdrawal
Any evidence of migraine
Any evidence of migraine Acute and preventative strategies
Consider shunting