Embed Size (px)
Citation preview

208� Vol�4�No�4�•�Journal�of�Paramedic�Practice
Clinical
Prehospital improvised bronchodilator therapy of a patient on Bi-level Positive
Airway Pressure therapy
On the 15th of June 2011 the Medical Director of the Scottish Ambulance Service approved the use of a T-piece in-line nebulizer device
(Figure 1) for use by paramedics and emergency medical technicians (Scottish Ambulance Service, 2011). This internal communication indicated that instruction on its use would follow during mandatory updates and after such training, staff would then be deemed competent and authorised to use this device. Shortly after this directive, a call to attend a forty year old male having breathing difficulties was received
Anthony Haley is a Paramedic Team Leader for the Scottish Ambulance Service, Anthony Forbes is a Paramedic for the
Scottish Ambulance Service
Email for correspondence: [email protected]
Abstract Patients�suffering�acute�breathlessness�is�a�common�emergency�situation,�many�patients�with�airways�disease�require�bronchodilator�therapy�with�β-agonists.�To�assist�the�management�of�these�cases�paramedics�are�guided�by�guidelines�drawn�up�by�the�Joint�Royal�Colleges�Ambulance�Liaison�Committee�(JRCALC).�They�provide�guidance�on�the�management�of�most�situations�paramedics�are�likely�to�encounter.�However,�there�will�be�occasions�when�paramedics�are�called�to�deal�with�a�situation�which�is�outside�of�their�experience�and�the�JRCALC�guidelines�do�not�provide�the�appropriate�guidance�required�to�fully�inform�clinical�decision�making.�In�the�UK�telephone�support�from�a�physician�skilled�in�the�specific�discipline�they�require�is�generally�not�available,�so�paramedics�have�become�skilled�at�improvising.�This�case�study�describes�such�an�improvisation,�in�the�management�of�acute�breathlessness�in�a�patient�who�is�on�home�Bi-level�Positive�Airway�Pressure�(BiPAP)�therapy.
Key wordsl�COPD�l�Nebuliser�l�BiPAP�l�Paramedic�l�Non-invasive�positive�pressure�ventilation�
Accepted�for�publication�28�November�2011�
by the Emergency Medical Dispatch Centre (EMDC) and was subsequently attended by the authors. Both authors had not yet attended the mandatory update referred to above and consequently did not carry the T-piece in-line nebulizer device.
On arrival it was found that the patient had a patent airway supported by a non-invasive Ventilation (NIV) device via nasal mask, was breathing at a rate of 30 breaths per minute, had a heart rate of 160 beats per minute with full, regular radial pulses and was ‘alert’ on the AVPU scale (AVPU: Alert, responds to Verbal stimulus, responds to Pain, Unresponsive).
He had increased the inspiratory pressure on the device from 18cmH20 (his normal day time inspiratory pressure) to 21cmH20 in an attempt to improve oxygen delivery. The patient’s medical history cannot be described fully to ensure patient confidentiality, but he had been receiving Bi-level Positive Airway Pressure (BiPAP) therapy (Figure 2) via this device for many years because of a neuromuscular condition and chronic obstructive pulmonary disease (COPD). BiPAP has been shown to improve ventilatory parameters in COPD whilst decreasing the work of breathing and transdiaphragmatic work (Vanpee et al, 2002) and has been shown to be effective in the treatment of acute respiratory failure in the emergency setting when used with other therapies (Goss, 2008). Supplemental oxygen is recommended in conjunction with BiPAP in cases of hypoxaemia (Scala, 2004).
DiscussionFurther assessment found that the patient had bilateral inspiratory and expiratory wheezes and crepitations on auscultation of his anterior and posterior chest,

Journal�of�Paramedic�Practice�•�Vol�4�No�4 209�
Clinical
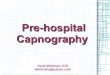
via a standard nebulizer device and mask, but this was impossible due to the patient’s reliance on BiPAP. The solution was to connect the oxygen connector from a standard oxygen mask (usually discarded when setting up such a mask to attach a nebulizer chamber) to the top of a nebulizer chamber and connecting this via a small length of oxygen tubing (about 10cms) to a connector on the BiPAP nasal mask (Figure 3). The inferior connector on the nebulizer was connected to an oxygen cylinder in the usual way and the oxygen delivered to the nebulizer at the required rate (6–8 litres per minute) ( JRCALC, 2006a). Again, consideration was given to the BiPAP inspiration and expiration pressures. These showed no change (inspired: 21–14cmH20 and expired: 4–4.1cmH20). Mild expiratory and inspiratory wheezes were still audible on auscultation. Ipratropium bromide is an antimuscarinic bronchodilator and is indicated for patients suffering exacerbation of COPD (JRCALC, 2006a), 500mcg of ipratropium bromide was delivered using the same improvised method. A short time after commencing ipatropium Bromide therapy SpO2 rose to 91% and respiratory rate reduced further. Supplemental oxygen into the BiPAP nasal mask was reduced to 2 litres per minute after complete delivery of nebulized ipratropium bromide. On arrival at hospital the BiPAP inspiration pressure was further increased to 24cmH20. The improvised device was replaced with
Figure 1: T-Piece Nebulizer
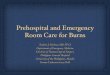
Fig. 2 - Non-invasive positive pressure ventilation via nasal
mask
Use of this image is made with kind permission of ResMed Limited who own the copyright. All rights reserved.
Figure 2: Non-invasive pressure ventilation via nasal maskUse�of�this�image�is�made�with�kind�permission�of�ResMed�Limited�who�own�the�copyright.�All�rights�reserved
saturation of peripheral oxygen (SpO2) measured by pulse oximetry at 76% on room air, as well as being pyrexic; normotensive and denying pain. He was being treated with antibiotic therapy by his General Practitioner for a suspected chest infection. This clinical presentation suggested critical illness and that the patient needed supplemental oxygen therapy to reverse hypoxaemia (preferably Fractional Inspired Oxygen (Fi O2) of 0.85) while a bronchodilator therapy device (nebulizer) was prepared. However, the British Thoracic Society guidelines (O’Driscoll, 2008) and the JRCALC guidelines ( JRCALC, 2009) also advise that patients with COPD or who are at risk of hypercapnoeic respiratory failure should be placed on a nasal cannula with oxygen delivery set at 2–6 litres per minute or standard mask with an appropriate venturi adapter with oxygen flow set to 4 litres per minute in with a target SpO2 of 88–92%. None of these oxygen delivery methods was appropriate in this case as the patient required respiratory support via the BiPAP circuit and was unable to remove the nasal mask. Instead, standard oxygen tubing was connected to a connector on the nasal mask (Figure 3) and oxygen delivered into the nasal mask at 2 litres per minute. SpO2 was observed whilst a solution to delivering effective bronchodilator therapy was sought.
BiPAP mask pressures were monitored whilst supplemental oxygen therapy was attached. The BiPAP control panel displayed both inspired and expired pressures (pre-set and actual pressures) and these did not change during supplemental oxygen therapy in this way (inspired: 21–14 cmH20 and expired: 4–4.1 cmH20). Within a short time, SpO2 rose to 85%, so the oxygen delivery rate was increased to 4 litres per minute and the same inspired and expired pressures were noted.
Consideration was given to bronchodilator therapy

30� Vol�4�No�1�•�Journal�of�Paramedic�Practice
Clinical
a T-piece in-line nebulizer and further salbutamol was administered. His symptoms improved further and on last seeing the patient his respiratory rate was 20 breaths per minute, heart rate was 146 beats per minute and SpO2 was93%. He reported a significant easing of his symptoms.
ConclusionThis improvised method delivered moderately
effective relief of the patient’s symptoms. Increased SpO2, decreased respiratory rate and decreased heart rate were observed, as well as a reduction in audible signs on auscultation. The authors recommend this method of improvised nebulization in the absence of a T-piece in-line nebulizer or similar device, but ambulance staff should make sure inspiratory and expiratory pressures are not adversely affected and that all decisions, actions, oxygen delivery rates and BiPAP pressures are recorded in clinical records. High priority should be placed on returning oxygen supplementation to a lower controlled level as soon as practicable after the delivery of nebulized drugs.
All�reasonable�steps�have�been�taken�to�ensure�patient�confidentiality.
Figure 3: Improvised nebuliser device
Goss JF (2008) How non-invasive ventilation helps patients in respiratory failure. JEMS 33(2): 78–83
Joint Royal Colleges Ambulance Liaison Committee (2006a) UK Ambulance Service Clinical Practice Guidelines: Salbutamol (Ventolin) Available at: www2.warwick.ac.uk/fac/med/research/hsri/emergencycare/prehospitalcare/jrcalcstakeholderwebsite/guidelines/salbutamol_ventolin_slb.pdf (Accessed 20 October 2011)
Joint Royal Colleges Ambulance Liaison Committee (2006b) UK Ambulance Service Clinical Practice Guidelines: Ipratropium Bromide (Atrovent) Available at: www2.warwick.ac.uk/fac/med/research/hsri/emergencycare/prehospitalcare/jrcalcstakeholderwebsite/guidelines/ipratropium_bromide_atrovent_ipr.pdf (Accessed 20 October 2011)
Joint Royal Colleges Ambulance Lwwiaison Committee (2009) UK Ambulance Service Clinical Practice Guidelines: Oxygen — update. Available at: jrcalc.org.uk/newjrcalcguidance/oxygen_guideline_combined220409.pdf (Accessed 20 October 2011)
O’Driscoll BR, Howard LS, Davison AG et al (2008) Guideline for emergency oxygen use in adult patients. Thorax 63(Supp): vi1-vi68
Scala R (2004) Bi-level home ventilators for non-invasive positive pressure ventilation. Monaldi Arch Chest Dis 61(4): 213-–21
Scottish Ambulance Service (2011) Clinical National Bulletin No.09/11: T-Piece In-Line Nebulisers, Scottish Ambulance Service Internal Communication, Edinburgh, Scottish Ambulance Service
Vanpee D, El Khawand C, Rousseau L et al (2002) Effects of nasal pressure support on ventilation and inspiratory work in normocapnic and hypercapnic patients with stable COPD, Chest 122(1): 75–83
Key points�l British�Thoracic�Society�guidelines�and�JRCALC�guidelines�advise�that�patients�with�COPD�or�who�are�at�risk�of�hypercapnoeic�respiratory�failure�should�be�placed�on�a�nasal�cannula�or�standard�mask�with�an�appropriate�venturi�adapter�with�a�target�SpO2�of�88-92%.�This�is�impossible�with�patients�on�BiPAP�and�alternatives�must�be�sought.
�l Patients�with�an�Spo2�of�less�than�85%�are�suffering�critical�levels�of�hypoxaemia�and�should�be�placed�on�high�flow�supplemental�oxygen�therapy�to�improve�blood�oxygen�levels.�Again�this�will�be�impossible�with�patients�reliant�on�BiPAP�and�alternatives�must�be�sought.
�l The�improvised�method�of�oxygen�supplementation�and�delivery�of�nebulised�drugs�in�this�case�did�not�appear�to�adversely�affect�the�inspiratory�and�expiratory�pressures�delivered�by�the�BiPAP�unit.
�l If�using�this�improvised�method,�ambulance�staff�should�make�sure�inspiratory�and�expiratory�pressures�are�not�adversely�affected�and�that�all�decisions,�actions,�oxygen�delivery�rates�and�BiPAP�pressures�are�recorded�in�clinical�records.