Embed Size (px)
Citation preview

SCI and Co-Occurring TBISCI and Co-Occurring TBI
Janet P. Niemeier, Ph.D., ABPPJanet P. Niemeier, Ph.D., ABPPProfessor, Director of ResearchProfessor, Director of Research
Carolinas RehabilitationCarolinas Rehabilitation
Charlotte, NCCharlotte, NC

Disclosure of PI-RRTC GrantDisclosure of PI-RRTC Grant
James S. Krause, PhD, Holly Wise, PhD; PT, and James S. Krause, PhD, Holly Wise, PhD; PT, and Elizabeth Walker, MPA have disclosed a Elizabeth Walker, MPA have disclosed a research research grantgrant with the National Institute of Disability and with the National Institute of Disability and Rehabilitation ResearchRehabilitation Research
The contents of this presentation were developed The contents of this presentation were developed with support from an educational grant from the with support from an educational grant from the Department of Education, NIDRR grant number Department of Education, NIDRR grant number H133B090005. However, those contents do not H133B090005. However, those contents do not necessarily represent the policy of the Department necessarily represent the policy of the Department of Education, and you should not assume of Education, and you should not assume endorsement by the Federal Government.endorsement by the Federal Government.

AccreditationAccreditation
The Medical University of South Carolina is accredited by the The Medical University of South Carolina is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to Accreditation Council for Continuing Medical Education (ACCME) to provide continuing medical education for physicians. The Medical provide continuing medical education for physicians. The Medical University of South Carolina designates this live activity for a University of South Carolina designates this live activity for a maximum of maximum of 1.0 AMA PRA Category 1 Credit(s)™1.0 AMA PRA Category 1 Credit(s)™. Physicians . Physicians should claim only the credit commensurate with the extent of their should claim only the credit commensurate with the extent of their participation in the activity.participation in the activity.
In accordance with the ACCME Essentials &Standards, anyone In accordance with the ACCME Essentials &Standards, anyone involved in planning or presenting this educational activity will be involved in planning or presenting this educational activity will be required to disclose any relevant financial relationships with required to disclose any relevant financial relationships with commercial interests in the healthcare industry. This information is commercial interests in the healthcare industry. This information is listed below. Speakers who incorporate information about off-label listed below. Speakers who incorporate information about off-label or investigational use of drugs or devices will be asked to disclose or investigational use of drugs or devices will be asked to disclose that information at the beginning of their presentation.that information at the beginning of their presentation.
The Center for Professional Development is an approved provider of The Center for Professional Development is an approved provider of the continuing nursing education by the South Carolina Nurses the continuing nursing education by the South Carolina Nurses Association, an accredited approver by the American Nurses Association, an accredited approver by the American Nurses Credentialing Center’s Commission on AccreditationCredentialing Center’s Commission on Accreditation

Disclosure of PresenterDisclosure of Presenter
Dr. Janet Niemeier does not have any Dr. Janet Niemeier does not have any financial disclosures.financial disclosures.

Continuing EducationContinuing EducationContinuing Nursing Education (CNE) credit:Continuing Nursing Education (CNE) credit:
The Center for Education and Best Practice is an The Center for Education and Best Practice is an approved provider of continuing nursing education approved provider of continuing nursing education by the South Carolina Nurses Association, an by the South Carolina Nurses Association, an accredited approver by the American Nurses accredited approver by the American Nurses Credentialing Center’s Commission on Credentialing Center’s Commission on Accreditation.Accreditation.
Only RNs are eligible to receive nursing contact Only RNs are eligible to receive nursing contact hourshours
Each participant will receive two forms for CNEEach participant will receive two forms for CNE Verification of attendanceVerification of attendance Individual evaluation formIndividual evaluation form
For all CNE sessions, in order to receive full contact For all CNE sessions, in order to receive full contact hour credit for the CNE activities, you must:hour credit for the CNE activities, you must:
Be present no later than five minutes Be present no later than five minutes after starting timeafter starting time
Remain until the scheduled ending timeRemain until the scheduled ending time Complete and return the evaluation Complete and return the evaluation
form at the end of the sessionform at the end of the session
Conflict of Interest Conflict of Interest
A conflict of interest occurs when an individual has an A conflict of interest occurs when an individual has an opportunity to affect educational content about health care opportunity to affect educational content about health care products or services of a commercial interest with which products or services of a commercial interest with which she/he has a financial relationship.she/he has a financial relationship.
The planners and presenters of this CNE activity have The planners and presenters of this CNE activity have disclosed relevant financial relationships with any commercial disclosed relevant financial relationships with any commercial interests pertaining to this activity. A list of event sponsors interests pertaining to this activity. A list of event sponsors and vendors may be found in your handouts or and vendors may be found in your handouts or disclosure slide.disclosure slide.
The Center for Education and Best Practice has conflict of The Center for Education and Best Practice has conflict of interest disclosures on file for all presenters and planners.interest disclosures on file for all presenters and planners.
Non-endorsement of ProductsNon-endorsement of Products
Provision of this education activity by the Center for Education Provision of this education activity by the Center for Education and Best Practice does not imply endorsement by the Center and Best Practice does not imply endorsement by the Center or SCNA of any commercial products displayed in conjunction or SCNA of any commercial products displayed in conjunction with this activity. Commercial support does not influence the with this activity. Commercial support does not influence the design and scientific objectivity of any Center educational design and scientific objectivity of any Center educational activity.activity.

Learning ObjectivesLearning Objectives
Attendees will be able to discuss:Attendees will be able to discuss:
1.1. The epidemiology of co-occurring SCI The epidemiology of co-occurring SCI and TBIand TBI
2.2. TBI symptoms and challenges and how TBI symptoms and challenges and how these complicate recovery from SCIthese complicate recovery from SCI
3.3. Best practices for identification and Best practices for identification and treatment of patients with both SCI and treatment of patients with both SCI and TBITBI

Separate EpidemiologySeparate Epidemiology
Traumatic Brain Injury 1.7 million a yearTraumatic Brain Injury 1.7 million a year
SCI 11,000 a yearSCI 11,000 a year– 82% male, 82% male, – Average age 31Average age 31– 52% paraplegic, 47% quadriplegic52% paraplegic, 47% quadriplegic
Military study, OIF/OEF -- Military study, OIF/OEF -- 10%, from 10%, from blasts (Bell et al., 2009) and combat blasts (Bell et al., 2009) and combat injuriesinjuries
(CDC)(CDC)

Causes of SCICauses of SCI(LeGrand, 10/16/10, C3/C4)(LeGrand, 10/16/10, C3/C4)
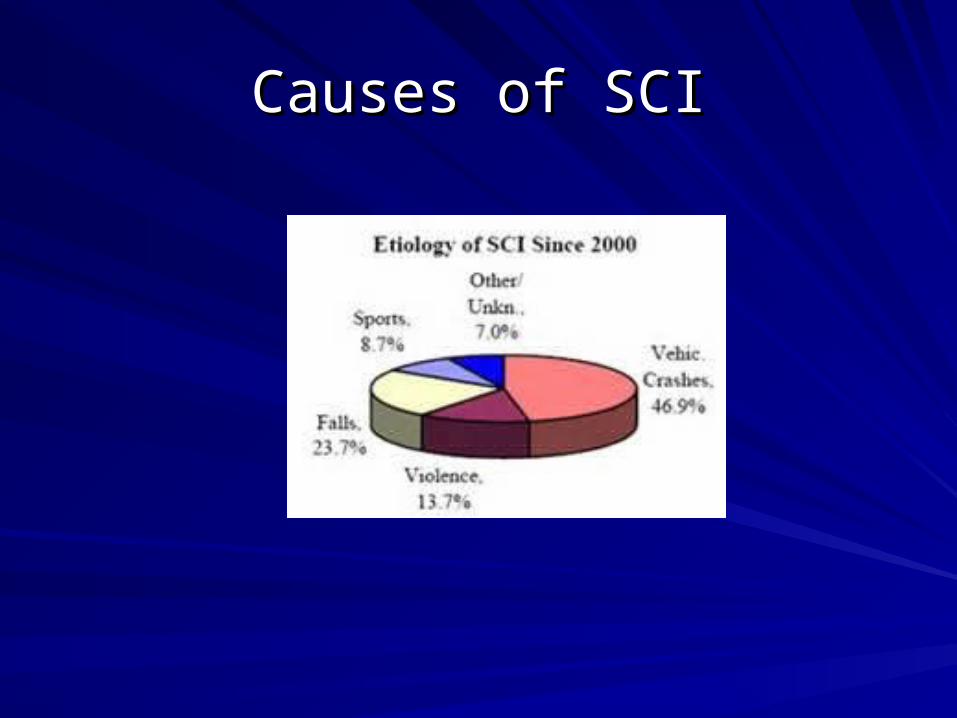
Causes of SCICauses of SCI

SCI/TBI EpidemiologySCI/TBI Epidemiology
Estimates vary depending on method of data Estimates vary depending on method of data collection, i.e., ICD-9 codes, neuroimaging, length of collection, i.e., ICD-9 codes, neuroimaging, length of comacoma
24-59% 24-59% (Sommer & Witkiewicz, 2004)(Sommer & Witkiewicz, 2004)
25% GCS 25% GCS (Wagner et al., 1984)(Wagner et al., 1984)
42% PTA/LOC 42% PTA/LOC (Davidoff et al., 1992)(Davidoff et al., 1992)
46.7%; most mild46.7%; most mild (Hagen et al., 2010) (Hagen et al., 2010)
56% Neuropsychological test data 56% Neuropsychological test data (Wilmot et al., 1985)(Wilmot et al., 1985)
60% GCS 60% GCS NIDRR diagnostic criteria, neurocognitive tests, PTA NIDRR diagnostic criteria, neurocognitive tests, PTA (Macchiocchi et al., (Macchiocchi et al., 2008) 2008)
74% ACRM diagnostic criteria, diagnostic imaging 74% ACRM diagnostic criteria, diagnostic imaging (Telenon et al., 2007) (Telenon et al., 2007)
Incidence is increasingIncidence is increasing
Injury Variables Associated with Co-Injury Variables Associated with Co-Occurrence of TBI & SCIOccurrence of TBI & SCI
CauseCause –MVAs, falls, assaults, sports, combat –MVAs, falls, assaults, sports, combat
SCI LevelSCI Level--Most common --Most common – C5-8, Asia Grade A-C C5-8, Asia Grade A-C – T 1-8, Asia Grade A-C T 1-8, Asia Grade A-C – T 9-12, Asia Grade A-CT 9-12, Asia Grade A-C– Completeness of injuryCompleteness of injury
SeveritySeverity – Many with SCI have – Many with SCI have mild mild TBITBI
Length of PTA, long is worseLength of PTA, long is worse(Macchiocchi et al., 2008)(Macchiocchi et al., 2008)

Injury Variables Associated with Co-Injury Variables Associated with Co-Occurrence of TBI & SCIOccurrence of TBI & SCI
NIDRR classifications: NIDRR classifications: – Mild (GCS = 13 – 15)**Mild (GCS = 13 – 15)**– mild complicated (cerebral pathology, contusion, mild complicated (cerebral pathology, contusion,
hemorrhage, skull fx)hemorrhage, skull fx)– Moderate (GCS = 9 – 12)Moderate (GCS = 9 – 12)– Severe (GCS = 3 – 8)Severe (GCS = 3 – 8)
GenderGender male male
Ethnicity Ethnicity WhiteWhite
Significant problem: Lack of ER, acute recordsSignificant problem: Lack of ER, acute records

CLASSIFICATIONS OF TBICLASSIFICATIONS OF TBI
Mild – GCS 13 – 15, ? To Min. LOC, Mild – GCS 13 – 15, ? To Min. LOC, ≤≤12 12 hours PTA, “post concussive syndrome” hours PTA, “post concussive syndrome” Symptom overlap with PTSDSymptom overlap with PTSDModerate – GCS 9 – 12, Moderate – GCS 9 – 12, ≤≤ 30 minutes 30 minutes LOC, ≤ 24 hours PTALOC, ≤ 24 hours PTASevere – GCS 3 – 8, > 30 minutes LOC, Severe – GCS 3 – 8, > 30 minutes LOC, >24 hours PTA>24 hours PTA

Co-Occurrence Risk FactorsCo-Occurrence Risk Factors
ETOHETOHCompleteness of Traumatic SCICompleteness of Traumatic SCIGender maleGender maleInvolvement in sportsInvolvement in sportsProfessions or occupations requiring work Professions or occupations requiring work at significant heightsat significant heightsCombat exposureCombat exposure

Early Assessment ToolsEarly Assessment Toolsand TBI Factsand TBI Facts
TBIMS Definition: : Damage to brain tissue caused by an external mechanical force as evidenced by loss of consciousness or post traumatic amnesia (PTA) due to brain trauma, or by objective neurological findings

Causes of TBICauses of TBI

TBI FactsTBI Facts
Annual incidence >1.5 millionAnnual incidence >1.5 million““Signature Wound” of global war on Signature Wound” of global war on terrorism, >1,700 U.S. military (64%) since terrorism, >1,700 U.S. military (64%) since beginning of Middle Eastern conflictbeginning of Middle Eastern conflict$4 million lifetime costs per person$4 million lifetime costs per personGreatest risk ages <5 and > 85 Greatest risk ages <5 and > 85 MVAs cause most severe injuriesMVAs cause most severe injuries

TBI Research TimelineTBI Research Timeline
First review of literature on TBI rehabilitation in First review of literature on TBI rehabilitation in 1998 (Cicerone, et al.)1998 (Cicerone, et al.)– Very little clinically useful work on efficacy of Very little clinically useful work on efficacy of
treatmenttreatment
– We need tested interventions, but most of We need tested interventions, but most of the research studies and articles have the research studies and articles have focused on impairments, course of focused on impairments, course of recovery, and ways to measure post-TBI recovery, and ways to measure post-TBI function.function.

Early Assessment ToolsEarly Assessment Tools
Length of coma*Length of coma*Time to commands*Time to commands*GCS*GCS*Admission FIMAdmission FIMTM *InterD baseline evals
Lots of challenges for examiners of acute patientsWiser make long-term recs based on evals completed during post acute phase*Assessment of Severity.
Inpatient Baseline EvaluationsInpatient Baseline Evaluations
Discipline specific:Discipline specific:SpeechSpeechVisionVisionHearing Hearing Practic functions/Sensory motor abilitiesPractic functions/Sensory motor abilitiesBalanceBalanceGross motor/walking/wheel chairGross motor/walking/wheel chairEnduranceEnduranceCognitive status:Cognitive status:Level of AgitationLevel of AgitationSocial and emotional statusSocial and emotional status

Common Symptoms and Issues after TBICommon Symptoms and Issues after TBI
SymptomsSymptoms IssuesIssues
PhysicalPhysical Pain Pain
PerceptualPerceptual PremorbidPremorbid
EmotionalEmotional Comorbid Comorbid
BehavioralBehavioral PsychosocialPsychosocial
SocialSocial
CognitiveCognitive
The Scientific TBI Literature Tells Us…The Scientific TBI Literature Tells Us…
Primary Needs after TBI:Primary Needs after TBI:
MildMild—Injury and coping Knowledge, —Injury and coping Knowledge, reassurance, time, rehab for disruptive deficits, reassurance, time, rehab for disruptive deficits, counseling (especially if PTSD)counseling (especially if PTSD)
Moderate, SevereModerate, Severe—Early and intensive rehab, —Early and intensive rehab, knowledge, compensatory skills, opportunity for knowledge, compensatory skills, opportunity for purpose and QOL, community and family purpose and QOL, community and family supportssupports

The Scientific TBI Literature Tells Us…The Scientific TBI Literature Tells Us…
Factors in Long-term outcome:Factors in Long-term outcome:AgeAge LOCLOC
GenderGender early rehabearly rehab
EthnicityEthnicity GCS on admitGCS on admit
Level of educationLevel of education Site of injurySite of injury
ViolenceViolence Premorbid factorsPremorbid factors
SeveritySeverity ER careER care
Support networkSupport network Relationship stabilityRelationship stability
Family involvementFamily involvement

The Scientific TBI Literature Tells Us…The Scientific TBI Literature Tells Us…
Evidence-Based, Effective Interventions:Evidence-Based, Effective Interventions:
In General:In General: Early, Early, comprehensivecomprehensive
Cognitive RehabilitationCognitive Rehabilitation: :
Visual scanning trainingVisual scanning training
Speech language therapySpeech language therapy
Problem Solving trainingProblem Solving training
Memory RetrainingMemory Retraining
Electronic Assistive DevicesElectronic Assistive Devices
Outcomes assessed with real world tasks practice Outcomes assessed with real world tasks practice

The Scientific TBI Literature Tells Us…The Scientific TBI Literature Tells Us…
Post Injury employment outcomes affected Post Injury employment outcomes affected most by:most by:Premorbid employment statusPremorbid employment statusEthnicityEthnicityFunctional status at rehab D/CFunctional status at rehab D/CCognitive functioningCognitive functioningVocational rehabilitationVocational rehabilitationSupportive employmentSupportive employment
No “gold standard” for defining productivityNo “gold standard” for defining productivity

The Scientific TBI Literature Tells Us…The Scientific TBI Literature Tells Us…
Variables Associated with Quality of Life Variables Associated with Quality of Life Outcomes:Outcomes:
Being employedBeing employed
ActivityActivity
Social integrationSocial integration
Less severe injuryLess severe injury

Challenges to InterD EvaluationsChallenges to InterD Evaluations
Polytrauma, medical problemsPolytrauma, medical problemsPainPainReduced enduranceReduced enduranceReduced time for assessmentReduced time for assessmentLess insurance coverageLess insurance coverageSymptom overlapSymptom overlapMedication EffectsMedication EffectsAgitation, behavior problemsAgitation, behavior problemsCultural IssuesCultural IssuesSetting prioritiesSetting prioritiesPerceptual, language, and motor deficitsPerceptual, language, and motor deficits

Limited Literature about Dual DxLimited Literature about Dual Dx
Studies looking at long-term consequences of Studies looking at long-term consequences of TBI and SCITBI and SCI
Moderate/severe TBI + SCI = more personal and family Moderate/severe TBI + SCI = more personal and family adjustment difficulties than mild TBI and SCI adjustment difficulties than mild TBI and SCI ((Richards et al., Richards et al., 1991)1991)
Fewer functional gains from pre- to post-treatment on Fewer functional gains from pre- to post-treatment on FIM for SCI + TBI vs. SCI only FIM for SCI + TBI vs. SCI only (Macchiocchi et al., 2004)(Macchiocchi et al., 2004)
Worse neuropsychological test performance, more Worse neuropsychological test performance, more psychopathology and behavioral problems, greater psychopathology and behavioral problems, greater demands on clinician resources, increased rehab demands on clinician resources, increased rehab costs (costs (Bradbury et al., 2008)Bradbury et al., 2008)

Limited LiteratureLimited Literature
Small sample sizesSmall sample sizes
Variation in methodologiesVariation in methodologies
Mostly epidemiological and descriptiveMostly epidemiological and descriptive
Need more research on variables associated Need more research on variables associated with outcome, best interventionswith outcome, best interventions
Inconsistent information in acute or ER recordsInconsistent information in acute or ER records—true of military records as well—true of military records as well
Persons with mild TBI often do not recall being Persons with mild TBI often do not recall being injured or losing consciousnessinjured or losing consciousness

Military Co-OccurrenceMilitary Co-Occurrence
Military Study of Impact Blast and Military Study of Impact Blast and military grade weaponry on CNS (Bell military grade weaponry on CNS (Bell et al., 2009)et al., 2009)
n = 40/408 (9.8% co-occurring SCI and n = 40/408 (9.8% co-occurring SCI and TBI)TBI)
No stratification in looking at outcomes, No stratification in looking at outcomes, level of injurylevel of injury

Challenges to Dual DiagnosisChallenges to Dual Diagnosis
Often missed in EROften missed in ER
Acute charts often have no informationAcute charts often have no information
Motor performance is required on many Motor performance is required on many cognitive testscognitive tests
Cognitive deficits can impair ability to Cognitive deficits can impair ability to follow test instructionsfollow test instructions

Challenges to Treatment of DDChallenges to Treatment of DD
Cognitive deficits Lead to:Cognitive deficits Lead to:– Poor recall of therapists’ instructions and Poor recall of therapists’ instructions and
teaching/trainingteaching/trainingForgetting to do critical self care:Forgetting to do critical self care:
– Pressure releasesPressure releases– Exercise Exercise – TLSO complianceTLSO compliance– Forgetting precautions, getting up impulsively, and risking Forgetting precautions, getting up impulsively, and risking
further injuryfurther injury

Challenges to Treatment of DDChallenges to Treatment of DD
Inability to retain vital educational portions of Inability to retain vital educational portions of rehabilitation of the SCI due to cognitive rehabilitation of the SCI due to cognitive deficits: deficits: B&BB&B NutritionNutrition SexualitySexuality Avoidance of medical complicationsAvoidance of medical complications

Challenges to TreatmentChallenges to Treatment
Behavioral issues Behavioral issues AgitationAgitationAggressionAggressiondisinhibitiondisinhibitioninitiationinitiationSocial pragmaticsSocial pragmaticsTreatment disruptedTreatment disruptedPoor problem solvingPoor problem solving
Aphasia—hard to make needs and feelings knownAphasia—hard to make needs and feelings knownHard to understand therapistsHard to understand therapists

Challenges to TreatmentChallenges to Treatment
Mood and coping issues are common in SCIMood and coping issues are common in SCI– Depression, suicidal ideationDepression, suicidal ideation– lethality worse after TBIlethality worse after TBI
Impaired self-awarenessImpaired self-awareness endangering self with impulsive behaviorendangering self with impulsive behavior
Losses doubledLosses doubled– Grief further complicate emotional responses to Grief further complicate emotional responses to
disabilitydisability– Patients overwhelmed with 2 disorders to acceptPatients overwhelmed with 2 disorders to acceptMajor Issue: Psychotherapy helps with adjustment Major Issue: Psychotherapy helps with adjustment
but is a talking enterprise – conceptually complexbut is a talking enterprise – conceptually complex

Challenges to TreatmentChallenges to Treatment
Failure to educate staff, patients, and family Failure to educate staff, patients, and family about cognitive assessment findingsabout cognitive assessment findings
Cognitive disability is overshadowed due to Cognitive disability is overshadowed due to paralysis paralysis
Patients can be labeled unmotivated, Patients can be labeled unmotivated, noncomplaint -- misinterpretation of their noncomplaint -- misinterpretation of their neurobehavioral symptomsneurobehavioral symptoms
Therapists frustrated by need to repeat infoTherapists frustrated by need to repeat info

Variables Affecting OutcomesVariables Affecting Outcomes
Type, severity, and number of Type, severity, and number of neurobehavioral deficitsneurobehavioral deficits
Location of injuryLocation of injury
CauseCause
Family supportFamily support
Social adjustmentSocial adjustment

Treatment RecommendationsTreatment Recommendations
NEED SPECIALIZED TREATMENTNEED SPECIALIZED TREATMENTNeuropsychological assessmentNeuropsychological assessmentCarefully check acute and ICU record to confirm TBI, type and Carefully check acute and ICU record to confirm TBI, type and severityseverity– Some biomarkers identified that can distinguish TBI + Some biomarkers identified that can distinguish TBI +
polytrauma from polytrauma alonepolytrauma from polytrauma aloneEducate team, family and patientEducate team, family and patientNormalize TBI symptoms, feelingsNormalize TBI symptoms, feelingsFamily hands-on trainingFamily hands-on trainingBehavior managementBehavior managementChemical restraintsChemical restraints

Treatment RecommendationsTreatment Recommendations
POA and decision-making issues clarifiedPOA and decision-making issues clarified
Train patient in purposive and consistent use of Train patient in purposive and consistent use of compensatory cognitive strategiescompensatory cognitive strategies
Repeat instructions and provide written backupRepeat instructions and provide written backup
Use of schedule, calendar, memory log (if able)Use of schedule, calendar, memory log (if able)
Link patient and family with community Link patient and family with community resourcesresources
Manage pain effectivelyManage pain effectively

Treatment RecommendationsTreatment Recommendations
Reduce size of education and support groups—Reduce size of education and support groups—two leaderstwo leadersIf possible, match group members by cognitive If possible, match group members by cognitive levellevelSimplify languageSimplify languageConsider education on an individual basisConsider education on an individual basisVisual aidsVisual aidsOpportunities to practice, apply concepts and Opportunities to practice, apply concepts and skillsskillsDry Erase boardDry Erase board

Treatment RecommendationsTreatment Recommendations
Gently redirect if attention wandersGently redirect if attention wanders
Awards/incentives for complianceAwards/incentives for compliance
TBI focus in education first….as cognition TBI focus in education first….as cognition improves, then start SCI edimproves, then start SCI ed
Have Dual Dx patients attend educational Have Dual Dx patients attend educational series more than onceseries more than once
Use of task analysis to trainUse of task analysis to train
Use consulting experts on both diagnosesUse consulting experts on both diagnoses

Predictors of OutcomesPredictors of Outcomes
Length of Post traumatic amnesia (PTA) Length of Post traumatic amnesia (PTA) >14 days, or time to commands>14 days, or time to commandsSeverity of cognitive deficitsSeverity of cognitive deficitsViolence associated with InjuryViolence associated with InjuryEarly rehabilitationEarly rehabilitationVocational rehabilitationVocational rehabilitationGenderGenderEthnicityEthnicity
(Heineman et al., 2002; Macchiocchi et al., 2008; Williams-Gary et al., 2009; )(Heineman et al., 2002; Macchiocchi et al., 2008; Williams-Gary et al., 2009; )

Clinical and Economic Clinical and Economic ConsequencesConsequences
Economic as well as clinical burdenEconomic as well as clinical burdenIncreased rehabilitation costsIncreased rehabilitation costsIncreased burden on clinician resources Increased burden on clinician resources and timeand timeMore nursing careMore nursing careLonger LOS-More time needed to achieve Longer LOS-More time needed to achieve comparable gainscomparable gains
(Bradbury et al., 2008)(Bradbury et al., 2008)

Further ResearchFurther Research
Intervention studiesIntervention studiesTranslational researchTranslational researchProtocol or manualization/critical path with Protocol or manualization/critical path with specialized assessment and interventionsspecialized assessment and interventionsPreventionPreventionImproved informatics to track trends and Improved informatics to track trends and associations that will help us learn moreassociations that will help us learn moreCare at ERs and in the field to carefully Care at ERs and in the field to carefully assess for and note both disordersassess for and note both disorders






























